Embed Size (px)
Citation preview

Birth Control:what works best for
YOU?
Slides adapted from Ruth Lesnewski MD; FMDRL.org
Katy Kropf DOHeritage College of Osteopathic Medicine
November 28, 2012For The Birth Circle, Athens, OH

Nearly half of pregnancies in the United States are unintended.
52 % Intended
25 % Unintended
Used Contraception
23 % Unintended
No Contraception
Henshaw SK. Fam Plann Perspect. 1998;30(1):24-9, 46.Rosenberg MJ, Waugh MS, Long S. J Reprod Med. 1995;40(5):355-60.Potter L, et al. Fam Plann Perspect. 1996;28(4):154-8.

If no method is used to prevent pregnancy, what is
the typical risk of pregnancy after 1 year?

Emergency Contraception:
Levonorgestrel (Plan B One-Step)
Take at once
up to 5 days after unprotected sex.
Lowers risk of pregnancy by 58-89%

Levonorgestrel EC:Mechanism of Action
Inhibits ovulation
Does NOT cause abortion

Ulipristal acetate: Ellaa new emergency contraceptive option
Decreases risk of pregnancy by about 90%
Nearly full efficacy up to 5 days after unprotected intercourse
Requires Prescription

Why do women experience unintended pregnancies?

Half of women at risk are not fully protected from unintended pregnancy.

Fertility Awareness Methods (aka natural family planning)
As commonly used: approx. 25 pregnancies per 100 women using this method.
BUT with correct and consistent use, pregnancy rates can range from 1-9 per 100 women using this method.
•Calendar based methods (tracking your cycles)•Symptom based methods (cervical secretions, temperature)


Cyclebeads.com

Highly Effective Methods
0.3%0.3%Hormone shot
Perfect-Use Rate of Pregnancy
Typical-Use Rate of Pregnancy
Family Planning Method
0.6%-1.5%0.8%-2%Intrauterine
devices
0.1%0.1%Implants
0.1%-0.5%0.2%-0.5%Male and female
sterilization
NOT USER DEPENDENT
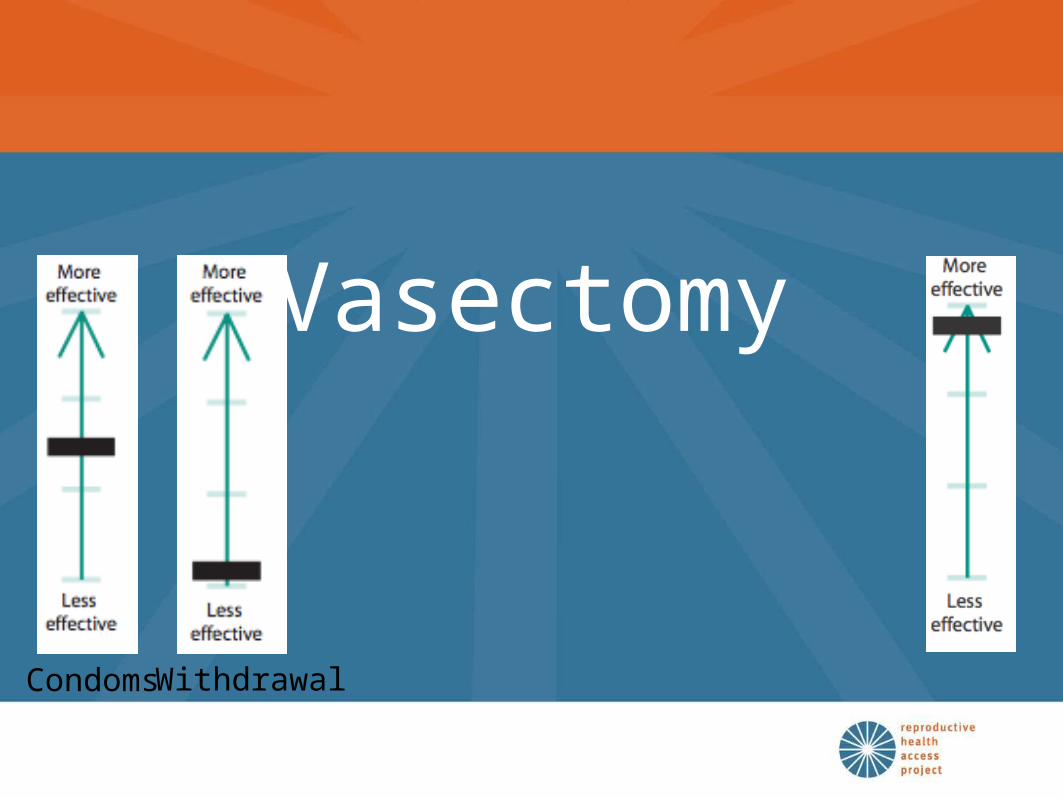
Vasectomy
Condoms Withdrawal

Tubal Ligation - “tubes tied”
Essure

Intrauterine Devices

IUD Myths Debunked
IUDs DO NOT raise risk of Pelvic infection
IUDs DO NOT raise risk of infertility.
IUDs DO NOT raise risk of ectopic pregnancy.
IUDs can be used safely by women who’ve never been pregnant and teens

IUD Myths Debunked
IUDs DO NOT cause abortion.
OK to insert IUD at any point in the menstrual cycle.
OK to insert immediately after delivery (post-partum) or following surgical abortion

Progestin IUD (MIRENA)

Progestin Implant: Nexplanon
• Highly effective and rapidly reversible• Discreet• Not user-dependent• Contain no estrogen• Can be used during lactation

Features of Progestin Implants
Can cause spotting
Requires certified clinician visits for insertion and removal

Progestin-Only Injection
Hatcher, R et al. A Pocket Guide to Managing Contraception, 2007-2008

Depo Provera & Bone Density
“No need to restrict Depo Provera use because of bone density concerns”
-ACOG

LAM: Lactational Amenorrhea Method
A woman can use LAM if:1. Her period has NOT returned
2. She is breastfeeding on demand (at least every 4 hours during the day, every 6 hours at night) and not pumping
3. Her baby is less than 6 months old
•If any of these factors are not in place, risk of pregnancy increases and additional methods should be used
•Risk of pregnancy < 2% (and may be lower)

Hormonal Contraceptives What is needed before prescribing?
Medical historyREQUIRED
Blood pressureRECOMMENDED
Pap smear
Pelvic/breast exam
STI testing
Hemoglobin
NOT REQUIRED

Progesterone Only: Mini Pill
• ONE pill every day – No breaks between packs
• Safe for breastfeeding women & babies
• Adds to the contraceptive effect of breastfeeding – Together, they provide effective pregnancy
protection
• Bleeding changes are common but not harmful

Hormonal Contraception: Benefits
• Birth Control• Decreased bleeding• Decreased anemia• Decreased menstrual pain• Decreased PMS• Decreased ACNE
• Decreased endometrial and ovarian cancer
• Decreased benign breast conditions
• Decreased ectopic pregnancies

Hormonal ContraceptivesWho can’t use estrogen?
Estrogen contraindications: • Migraine with aura• Uncontrolled high blood pressure• Postpartum < 6 weeks• History of blood clot
Smoking: NOT a contraindication in women/teens under age 35

When can you start the pill?

Extended Cycle Regimens

Estrogen/progestin vaginal ring
• Active for at least 3 weeks
• May remove for up to 3 hours
• Can do “QuickStart” same as with pills

Estrogen / Progestin Patch
• 1 patch weekly for 3 weeks, then one week off
• OK to shower, swim, exercise with patch on
• Failures in trials were in women over 198 pounds, but still rare
Gallo MF, et al. Cochrane Reviews. 2003, Issue 1. Art. No. CD003552.Jick S, et al. Contraception 73 (2006)

Getting the most out of your next provider visit
Start thinking about and discussing your next method of birth control before your baby is born
Do some research (ex. My Method at Planned Parenthood) http://www.plannedparenthood.org/all-access/my-method-26542.htm
Come prepared: •Write down what you want from your birth control•Write down your questions•Ask about side effects•Ask your provider for a full year prescription

References and Resources
• Hatcher et al, Contraceptive Technology 2007• Managing Contraception – book online @
www.managingcontraception.org• Medical Eligibility Criteria for Contraceptive Use 2010 by WHO
www.who.int/reproductive-health • Association of Reproductive Health Professionals www.arhp.org • Alan Guttmacher Institute www.agi-usa.org• Planned Parenthood www.plannedparenthood.org• The Cochrane Collaboration www.cochrane.org• www.Not-2-Late.com• Reproductive Health Access Project www.reproductiveaccess.org