Embed Size (px)
Citation preview

a
J Oral Maxillofac Surg70:1903-1908, 2012
Bite Force Evaluation of MandibularFractures Treated With Microplates
and MiniplatesAnand Gupta, MDS, MFDS,* Vibha Singh, MDS,† and
Shadab Mohammad, MDS‡
Purpose: The purpose of this study was to determine the clinical stability and efficacy of 1microplate combined with 1 miniplate in the management of mandibular fractures of the interfo-raminal region compared with the standard 2-miniplate treatment using bite force measurements.
Materials and Methods: Twenty patients were treated for isolated mandibular fractures of theinterforaminal region. They were randomly divided into group A (test group) and group B (controlgroup), with 10 patients per group. Group A underwent osteosynthesis using the combination of 1microplate (subapical) and 1 miniplate (at the lower border). Group B underwent osteosynthesisusing the standard 2-miniplate protocol. The bite force measurements were performed preopera-tively and postoperatively at each follow-up using a bite force recorder. As a secondary outcome, thepatients also were assessed for complications, such as infection, that might interfere with successfulosteosynthesis at the fracture site.
Results: A statistically significant increase in incisor bite force was found in the 2 groups comparedwith the preoperative bite force measurements. No statistically significant difference was seen in theincisor bite force of either group at the different follow-up visits. No statistically significantdifference was seen in the molar bite force (right vs left) of the test and control groups duringfollow-up. Molar bite force on the nonfractured side was greater than on the fractured side in the 2groups. Infection was seen in 1 patient (ie, 10%) in each group. On surgical exploration, the fracturehad united and the infection was resolved in the 2 patients, with no further complications.
Conclusions: The replacement of an upper miniplate by a microplate in the management of mandibularfractures is stable and adequately efficacious to withstand the masticatory loads and torsional forcesacting in the anterior region of the mandible.Crown Copyright © 2012 Published by Elsevier Inc on behalf of the American Association of Oral andMaxillofacial Surgeons. All rights reserved.
J Oral Maxillofac Surg 70:1903-1908, 2012btotp
i
The management of mandibular fractures includes therestoration of the pre-existing anatomic form, withassociated esthetics and functions. An evolution hasoccurred in fixation techniques from the historical eraof external fixation to internal fixation. Miniplate os-teosynthesis, introduced by Michelet et al1 in 1973nd further developed by Champy et al2 in 1978, has
Received from the Department of Oral and Maxillofacial Surgery,
CSM Medical University, Lucknow, India.
*Assistant Professor (Oral and Maxillofacial Surgery), Department
of Dentistry Government Medical College and Hospital, Chandi-
garh, India.
†Associate Professor.
‡Professor and Head.
Address correspondence and reprint requests to Dr Gupta: De-
partment of Dentistry (Oral and Maxillofacial Surgery), Government
1903
ecome the standard treatment of mandibular frac-ures. Champy et al2 determined the ideal lines ofsteosynthesis and described a 2-level zone betweenhe mental foramina in which 2 plates must be ap-lied to resist torsional forces.Thicker compact bone, the difficulty in identify-
ng the course of dental roots in the mandibles, and
Medical College and Hospital, Sector 32 B, Chandigarh, India
160030; e-mail: [email protected]
Crown Copyright © 2012 Published by Elsevier Inc on behalf of the
American Association of Oral and Maxillofacial Surgeons. All rights reserved.
0278-2391/12/7008-0$36.00/0
http://dx.doi.org/10.1016/j.joms.2012.03.036

il
GM
1904 BITE FORCE OF MICROPLATES AND MINIPLATES
the probability of injuring teeth are 3 times higherin the mandible than in the maxilla.3 The recentmedical literature has reported more and morecases in which metal depositions are found in thedirect neighborhood of the titanium microplate andminiplate or in peripheral organs after osteosynthe-sis. Therefore, the size and amount of the osteosyn-thesis material used should be minimized.4,5
Previously, microplates were used in nonstress-bearing areas such as the midface, but recent exper-imental and clinical studies have shown that micro-plates can be used efficiently in stress-bearing areassuch as the mandible.6-10
An experimental study was carried out in 60 acrylicmodels by Feller et al11 to examine the load-carryingstability and torsional strength of 2-piece acrylic mod-els connected by 2 titanium miniplates or 1 titanium
FIGURE 1. A, Intraoperative photograph showing the fixation of aparasymphysis fracture with a microplate at the subapical level anda miniplate at the lower border. B, Postoperative radiograph show-ng a microplate close to the mental foramen and a miniplate at theower border.
upta, Singh, and Mohammad. Bite Force of Microplates andiniplates. J Oral Maxillofac Surg 2012.
microplate and 1 miniplate. Their results suggested
that the combination of a microplate and a miniplatein the treatment of mandibular fracture in the inter-foraminal region is stable enough for early mobiliza-tion. However, they did not confirm the clinical sta-bility of the microplate in the management ofmandibular fractures.
The purpose of the present study was to determinethe clinical stability and efficacy of the microplate andminiplate combination in the management of mandib-ular fractures of the interforaminal region comparedwith the standard 2-miniplate treatment using biteforce measurements.
Materials and Methods
This study was conducted at the Department ofOral and Maxillofacial Surgery, CSM Medical Univer-sity, where 20 patients were treated for isolated man-dibular fractures of the interforaminal region. Thesepatients were randomly assigned to the test group(group A; 10 patients) or the control group (group B;10 patients) using sealed opaque envelopes with thetreatment allocation inside each envelope. Approvalwas obtained from the institutional ethical committeebefore starting this prospective study. Group A under-went osteosynthesis using the combination of 1 mi-croplate (Liebinger 1.2-mm titanium system [Stryker,Freiburg, Germany], subapical) and 1 miniplate(Liebinger 2.0-mm titanium system [Stryker, Freiburg,Germany], at the lower border; Figs 1A,B). Group Bunderwent osteosynthesis using 2 miniplates (Liebin-ger 2.0-mm titanium system [Stryker, Freiburg, Ger-many]; Figs 2A,B). Patients with a comminuted frac-ture of the mandible and infections were excluded.Patients with concomitant midface and dentoalveolarfractures also were excluded. Informed consent wastaken to participate in the study.
A standard surgical protocol was followed for allcases. Patients were evaluated using conventionalradiographs and bite force recordings before sur-gery. They underwent surgery under general orlocal anesthesia within 10 days after the trauma. Allfracture sites were exposed through an intraoralroute. Fracture fragments were reduced and fixa-tion was performed using the combination of 1subapical microplate and 1 miniplate at the lowerborder in group A (test) or 2 miniplates in group B(control). All patients were given similar postoper-ative antibiotics and analgesics.
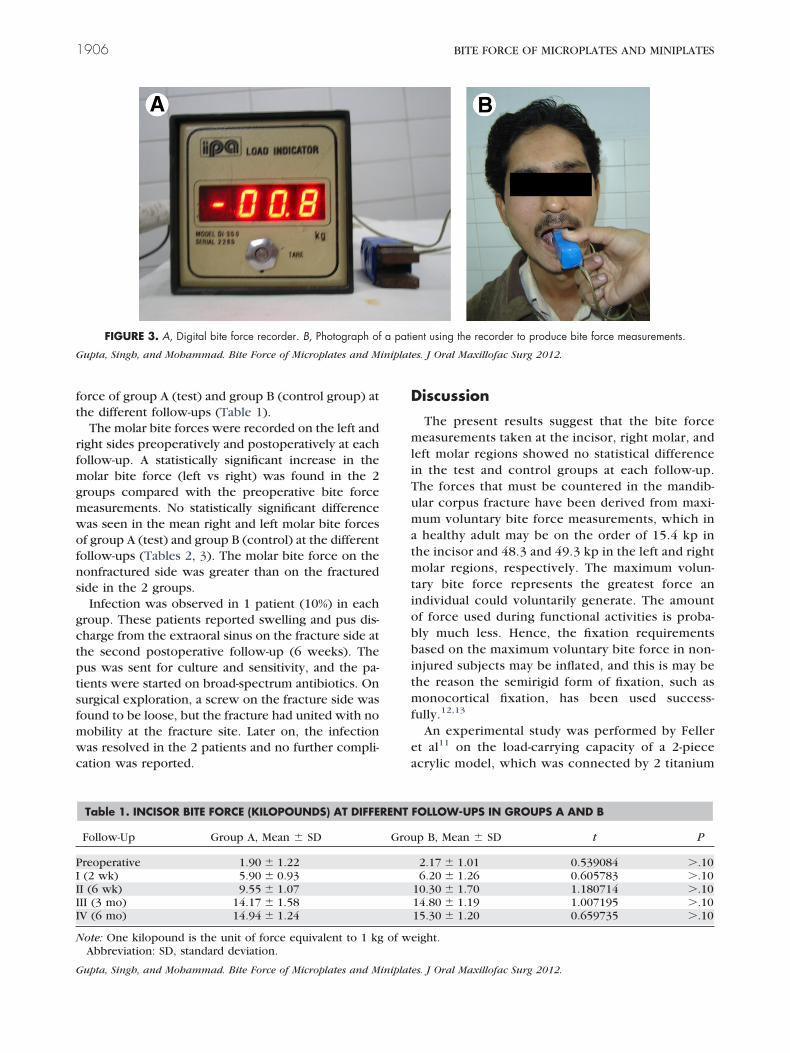
The assessment of the patients was performedusing bite force measurements. The measurementswere obtained preoperatively and postoperativelyin kilopounds (kp) at each follow-up using a biteforce recorder. The recorder was designed at a
reputable research center (Research Designs and
amtdt
2y(dg
iniplat
GUPTA, SINGH, AND MOHAMMAD 1905
Standards Organization, Lucknow, India) that con-sisted of 4 strain gauges mounted on 2 stainlesssteel bars forming a Wheatstone bridge, based onthe principles of Tate et al12 (Figs 3A,B).
As a secondary outcome, the patients also weressessed for complications such as infection thatight interfere with successful osteosynthesis at
he fracture site. Follow-up was performed at 14ays, 6 weeks, 3 months, and 6 months postopera-ively.
The data of all patients were entered in Excel007 (Microsoft, Redmond, WA) and statistical anal-sis was performed using EpiInfo version 3.4.3CDC, Atlanta). The Student t test was applied toetermine the difference among the parameters of
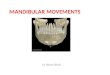
FIGURE 2. A, Intraoperative photograph showing fixation of a pathe lower border. B, Postoperative radiograph showing adequate
Gupta, Singh, and Mohammad. Bite Force of Microplates and M
roups A and B.
Results
This study was conducted for 1 year, during which30 patients reported to the outpatient departmentand trauma center with isolated mandibular fracturesof the interforaminal region.
Of these, 6 were excluded because of associatedmidface injuries and 4 did not consent to partici-pate in the study. Therefore, 20 patients were in-cluded in this study. These patients were randomlyassigned to group A (test group) or group B (con-trol group). All defined parameters were comparedin the 2 groups.
The incisor bite force was recorded preoperativelyand postoperatively at each follow-up. No statistically
hysis fracture with 2 miniplates, 1 at the subapical level and 1 atwith 2 miniplates.
es. J Oral Maxillofac Surg 2012.
rasympfixation
significant difference was seen in the incisor bite
a
iniplat
1906 BITE FORCE OF MICROPLATES AND MINIPLATES
force of group A (test) and group B (control group) atthe different follow-ups (Table 1).
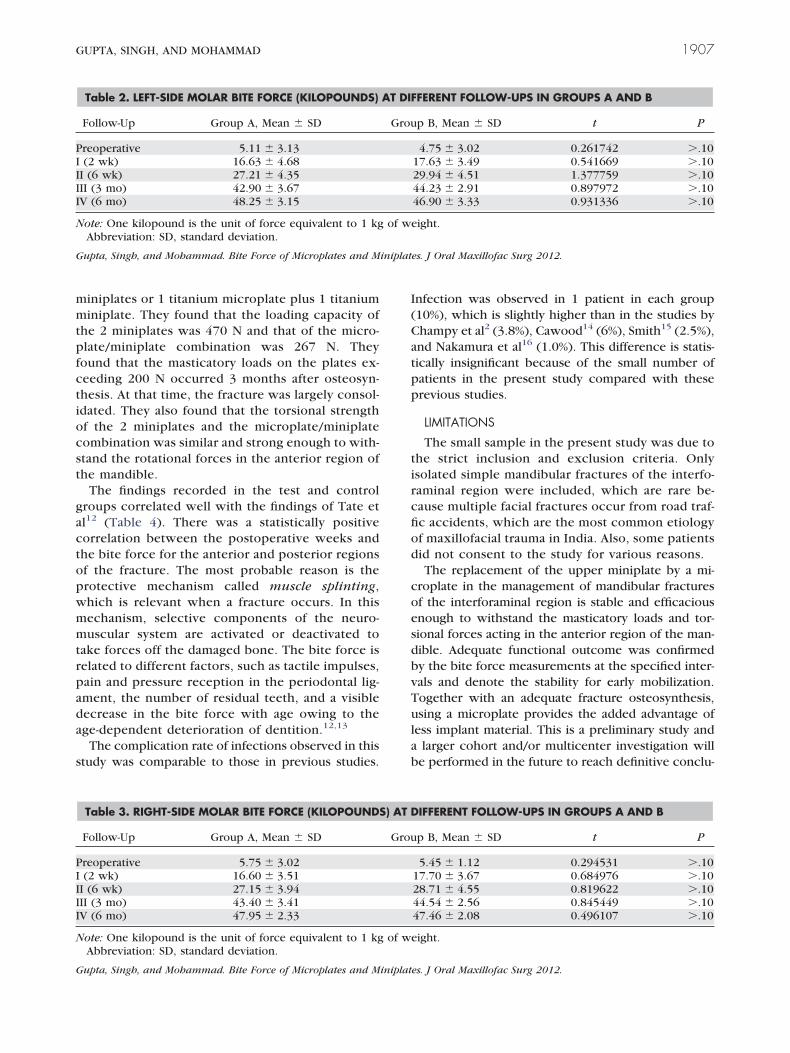
The molar bite forces were recorded on the left andright sides preoperatively and postoperatively at eachfollow-up. A statistically significant increase in themolar bite force (left vs right) was found in the 2groups compared with the preoperative bite forcemeasurements. No statistically significant differencewas seen in the mean right and left molar bite forcesof group A (test) and group B (control) at the differentfollow-ups (Tables 2, 3). The molar bite force on thenonfractured side was greater than on the fracturedside in the 2 groups.
Infection was observed in 1 patient (10%) in eachgroup. These patients reported swelling and pus dis-charge from the extraoral sinus on the fracture side atthe second postoperative follow-up (6 weeks). Thepus was sent for culture and sensitivity, and the pa-tients were started on broad-spectrum antibiotics. Onsurgical exploration, a screw on the fracture side wasfound to be loose, but the fracture had united with nomobility at the fracture site. Later on, the infectionwas resolved in the 2 patients and no further compli-cation was reported.
FIGURE 3. A, Digital bite force recorder. B, Photograph of
Gupta, Singh, and Mohammad. Bite Force of Microplates and M
Table 1. INCISOR BITE FORCE (KILOPOUNDS) AT DIFFE
Follow-Up Group A, Mean � SD
Preoperative 1.90 � 1.22I (2 wk) 5.90 � 0.93II (6 wk) 9.55 � 1.07III (3 mo) 14.17 � 1.58IV (6 mo) 14.94 � 1.24
Note: One kilopound is the unit of force equivalent to 1 kgAbbreviation: SD, standard deviation.
Gupta, Singh, and Mohammad. Bite Force of Microplates and Miniplat
Discussion
The present results suggest that the bite forcemeasurements taken at the incisor, right molar, andleft molar regions showed no statistical differencein the test and control groups at each follow-up.The forces that must be countered in the mandib-ular corpus fracture have been derived from maxi-mum voluntary bite force measurements, which ina healthy adult may be on the order of 15.4 kp inthe incisor and 48.3 and 49.3 kp in the left and rightmolar regions, respectively. The maximum volun-tary bite force represents the greatest force anindividual could voluntarily generate. The amountof force used during functional activities is proba-bly much less. Hence, the fixation requirementsbased on the maximum voluntary bite force in non-injured subjects may be inflated, and this is may bethe reason the semirigid form of fixation, such asmonocortical fixation, has been used success-fully.12,13
An experimental study was performed by Felleret al11 on the load-carrying capacity of a 2-piececrylic model, which was connected by 2 titanium
ent using the recorder to produce bite force measurements.
es. J Oral Maxillofac Surg 2012.
FOLLOW-UPS IN GROUPS A AND B
p B, Mean � SD t P
2.17 � 1.01 0.539084 �.106.20 � 1.26 0.605783 �.10
10.30 � 1.70 1.180714 �.1014.80 � 1.19 1.007195 �.1015.30 � 1.20 0.659735 �.10
eight.
a pati
RENT
Grou
of w
es. J Oral Maxillofac Surg 2012.
a
iniplat
GUPTA, SINGH, AND MOHAMMAD 1907
miniplates or 1 titanium microplate plus 1 titaniumminiplate. They found that the loading capacity ofthe 2 miniplates was 470 N and that of the micro-plate/miniplate combination was 267 N. Theyfound that the masticatory loads on the plates ex-ceeding 200 N occurred 3 months after osteosyn-thesis. At that time, the fracture was largely consol-idated. They also found that the torsional strengthof the 2 miniplates and the microplate/miniplatecombination was similar and strong enough to with-stand the rotational forces in the anterior region ofthe mandible.
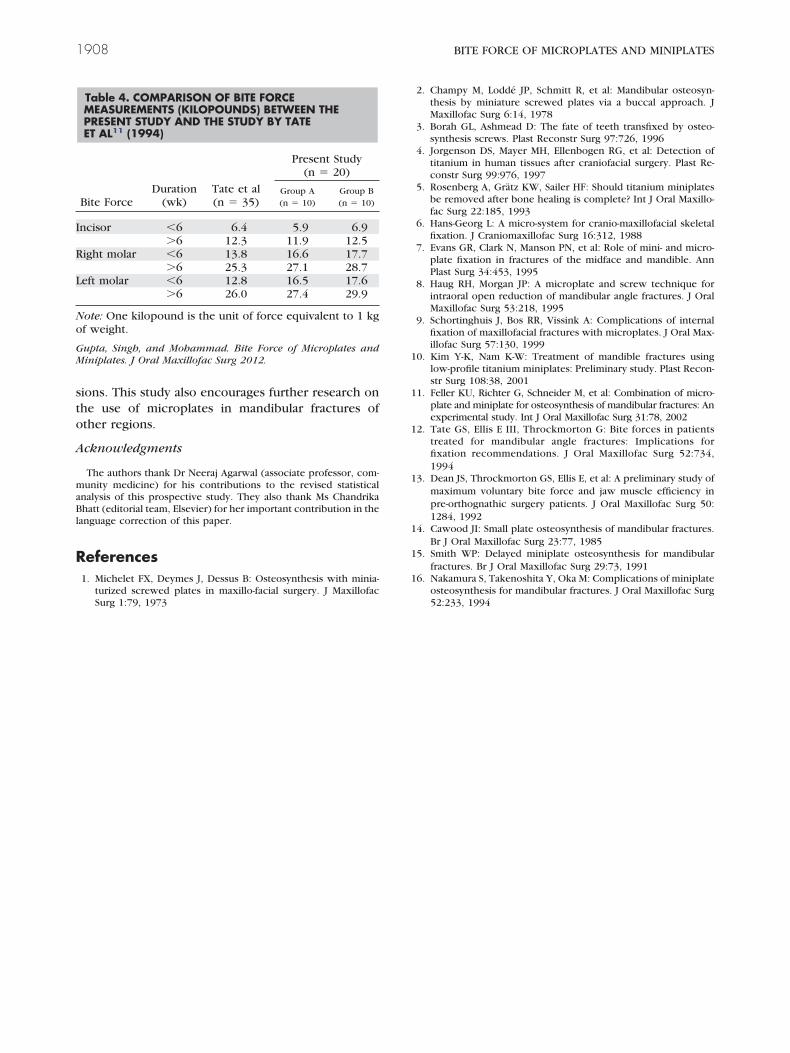
The findings recorded in the test and controlgroups correlated well with the findings of Tate etal12 (Table 4). There was a statistically positivecorrelation between the postoperative weeks andthe bite force for the anterior and posterior regionsof the fracture. The most probable reason is theprotective mechanism called muscle splinting,which is relevant when a fracture occurs. In thismechanism, selective components of the neuro-muscular system are activated or deactivated totake forces off the damaged bone. The bite force isrelated to different factors, such as tactile impulses,pain and pressure reception in the periodontal lig-ament, the number of residual teeth, and a visibledecrease in the bite force with age owing to theage-dependent deterioration of dentition.12,13
The complication rate of infections observed in thisstudy was comparable to those in previous studies.
Table 2. LEFT-SIDE MOLAR BITE FORCE (KILOPOUNDS)
Follow-Up Group A, Mean � SD
Preoperative 5.11 � 3.13I (2 wk) 16.63 � 4.68II (6 wk) 27.21 � 4.35III (3 mo) 42.90 � 3.67IV (6 mo) 48.25 � 3.15
Note: One kilopound is the unit of force equivalent to 1 kgAbbreviation: SD, standard deviation.
Gupta, Singh, and Mohammad. Bite Force of Microplates and M
Table 3. RIGHT-SIDE MOLAR BITE FORCE (KILOPOUND
Follow-Up Group A, Mean � SD
Preoperative 5.75 � 3.02I (2 wk) 16.60 � 3.51II (6 wk) 27.15 � 3.94III (3 mo) 43.40 � 3.41IV (6 mo) 47.95 � 2.33
Note: One kilopound is the unit of force equivalent to 1 kgAbbreviation: SD, standard deviation.
Gupta, Singh, and Mohammad. Bite Force of Microplates and Miniplat
Infection was observed in 1 patient in each group(10%), which is slightly higher than in the studies byChampy et al2 (3.8%), Cawood14 (6%), Smith15 (2.5%),nd Nakamura et al16 (1.0%). This difference is statis-
tically insignificant because of the small number ofpatients in the present study compared with theseprevious studies.
LIMITATIONS
The small sample in the present study was due tothe strict inclusion and exclusion criteria. Onlyisolated simple mandibular fractures of the interfo-raminal region were included, which are rare be-cause multiple facial fractures occur from road traf-fic accidents, which are the most common etiologyof maxillofacial trauma in India. Also, some patientsdid not consent to the study for various reasons.
The replacement of the upper miniplate by a mi-croplate in the management of mandibular fracturesof the interforaminal region is stable and efficaciousenough to withstand the masticatory loads and tor-sional forces acting in the anterior region of the man-dible. Adequate functional outcome was confirmedby the bite force measurements at the specified inter-vals and denote the stability for early mobilization.Together with an adequate fracture osteosynthesis,using a microplate provides the added advantage ofless implant material. This is a preliminary study anda larger cohort and/or multicenter investigation willbe performed in the future to reach definitive conclu-
FERENT FOLLOW-UPS IN GROUPS A AND B
p B, Mean � SD t P
4.75 � 3.02 0.261742 �.1017.63 � 3.49 0.541669 �.1029.94 � 4.51 1.377759 �.1044.23 � 2.91 0.897972 �.1046.90 � 3.33 0.931336 �.10
eight.
es. J Oral Maxillofac Surg 2012.
IFFERENT FOLLOW-UPS IN GROUPS A AND B
p B, Mean � SD t P
5.45 � 1.12 0.294531 �.1017.70 � 3.67 0.684976 �.1028.71 � 4.55 0.819622 �.1044.54 � 2.56 0.845449 �.1047.46 � 2.08 0.496107 �.10
eight.
AT DIF
Grou
of w
S) AT D
Grou
of w
es. J Oral Maxillofac Surg 2012.
1908 BITE FORCE OF MICROPLATES AND MINIPLATES
sions. This study also encourages further research onthe use of microplates in mandibular fractures ofother regions.
Acknowledgments
The authors thank Dr Neeraj Agarwal (associate professor, com-munity medicine) for his contributions to the revised statisticalanalysis of this prospective study. They also thank Ms ChandrikaBhatt (editorial team, Elsevier) for her important contribution in thelanguage correction of this paper.
References1. Michelet FX, Deymes J, Dessus B: Osteosynthesis with minia-
turized screwed plates in maxillo-facial surgery. J Maxillofac
Table 4. COMPARISON OF BITE FORCEMEASUREMENTS (KILOPOUNDS) BETWEEN THEPRESENT STUDY AND THE STUDY BY TATEET AL11 (1994)
Bite ForceDuration
(wk)Tate et al(n � 35)
Present Study(n � 20)
Group A(n � 10)
Group B(n � 10)
Incisor �6 6.4 5.9 6.9�6 12.3 11.9 12.5
Right molar �6 13.8 16.6 17.7�6 25.3 27.1 28.7
Left molar �6 12.8 16.5 17.6�6 26.0 27.4 29.9
Note: One kilopound is the unit of force equivalent to 1 kgof weight.
Gupta, Singh, and Mohammad. Bite Force of Microplates andMiniplates. J Oral Maxillofac Surg 2012.
Surg 1:79, 1973
2. Champy M, Loddé JP, Schmitt R, et al: Mandibular osteosyn-thesis by miniature screwed plates via a buccal approach. JMaxillofac Surg 6:14, 1978
3. Borah GL, Ashmead D: The fate of teeth transfixed by osteo-synthesis screws. Plast Reconstr Surg 97:726, 1996
4. Jorgenson DS, Mayer MH, Ellenbogen RG, et al: Detection oftitanium in human tissues after craniofacial surgery. Plast Re-constr Surg 99:976, 1997
5. Rosenberg A, Grätz KW, Sailer HF: Should titanium miniplatesbe removed after bone healing is complete? Int J Oral Maxillo-fac Surg 22:185, 1993
6. Hans-Georg L: A micro-system for cranio-maxillofacial skeletalfixation. J Craniomaxillofac Surg 16:312, 1988
7. Evans GR, Clark N, Manson PN, et al: Role of mini- and micro-plate fixation in fractures of the midface and mandible. AnnPlast Surg 34:453, 1995
8. Haug RH, Morgan JP: A microplate and screw technique forintraoral open reduction of mandibular angle fractures. J OralMaxillofac Surg 53:218, 1995
9. Schortinghuis J, Bos RR, Vissink A: Complications of internalfixation of maxillofacial fractures with microplates. J Oral Max-illofac Surg 57:130, 1999
10. Kim Y-K, Nam K-W: Treatment of mandible fractures usinglow-profile titanium miniplates: Preliminary study. Plast Recon-str Surg 108:38, 2001
11. Feller KU, Richter G, Schneider M, et al: Combination of micro-plate and miniplate for osteosynthesis of mandibular fractures: Anexperimental study. Int J Oral Maxillofac Surg 31:78, 2002
12. Tate GS, Ellis E III, Throckmorton G: Bite forces in patientstreated for mandibular angle fractures: Implications forfixation recommendations. J Oral Maxillofac Surg 52:734,1994
13. Dean JS, Throckmorton GS, Ellis E, et al: A preliminary study ofmaximum voluntary bite force and jaw muscle efficiency inpre-orthognathic surgery patients. J Oral Maxillofac Surg 50:1284, 1992
14. Cawood JI: Small plate osteosynthesis of mandibular fractures.Br J Oral Maxillofac Surg 23:77, 1985
15. Smith WP: Delayed miniplate osteosynthesis for mandibularfractures. Br J Oral Maxillofac Surg 29:73, 1991
16. Nakamura S, Takenoshita Y, Oka M: Complications of miniplateosteosynthesis for mandibular fractures. J Oral Maxillofac Surg
52:233, 1994