Embed Size (px)
Citation preview

Intensive Care Med (1996) 22:324-328 �9 Springer-Verlag 1996
M. Singer C. Millar R. Stidwill R. Unwin
Bladder epithelial oxygen tension - a new means of monitoring regional perfusion? Preliminary study in a model of exsanguination/fluid repletion
Received: 9 December 1994 Accepted: 14 July 1995
Support for this study was provided by Biomedical Sensors
M. Singer (~) - C. Millar R. Stidwill �9 R.Unwin Bloomsbury Institute of Intensive Care Medicine and Division of Nephrology University College London Medical School, Rayne Institute, University Street, London WC1E 6JJ, UK
Abstract Objective: To assess whether monitoring of bladder epi- thelial oxygen tension (BEOT) would provide an indication of regional (renal) organ perfusion in an exsanguination/fluid repletion animal model. Design: Prospective non-random- ized laboratory study. Setting." Research laboratory. Interventions." Eight anaesthetised, spontaneously breathing Sprague- Dawley male rats weighing approx- imately 200 g were instrumented. They received 1-ml aliquots of fluid until no further haemodynamic improvement was seen, followed by removal of 1-ml aliquots of blood until renal blood flow fell by 50%. The animal was then resuscitated with repeated 1 to 2-ml aliquots of fluid until no further improvement was achieved and, finally, progressively exsanguinated to cardiovascular collapse.
Measurements and results." A con- tinuous Clark-type oxygen elec- trode lying in contact with the inside wall of the bladder measured changes in BEOT during these exsanguination and fluid repletion manoeuvres. Changes in BEOT closely mirrored both systemic (blood pressure and aortic blood flow) and regional (renal blood flow) haemodynamic changes. A di- rect correlation existed between percentage change in BEOT and base deficit, and an indirect correla- tion was seen with arterial oxygen tension. Conclusions: Measurement of BEOT may be a useful and relative- ly non-invasive means of monitor- ing regional organ perfusion. Fur- ther studies are warranted.
Key words Bladder epithelium �9 Oxygen tension " Tissue oxygenation �9 Regional organ perfusion
Introduction
Despite the relative ease of measuring global cardiac output in the clinical situation by either invasive or non-invasive techniques, continuous monitoring of re- gional blood flow and organ perfusion still presents considerable difficulty. A knowledge of the adequacy of
flow in organ beds would prove highly useful in patient management and may potentially provide more appro- priate treatment endpoints. If organ hypoperfusion and impending dysfunction could be revealed at an earlier stage, prophylactic or corrective measures could be instituted more promptly and perhaps more effectively.
The development of techniques measuring regional perfusion in the critically ill or high-risk patient is still

325
in its relative infancy. Invasive access to myocardial, splanchnic, hepatic and renal circulations is not gener- ally applicable for long-term monitoring. Tonometric measurement of gut mucosal pH via a balloon placed in either the stomach or the sigmoid colon has been advanced as a relatively non-invasive means of assess- ing splanchnic mucosal hypoperfusion [1] and predict- ing multi-organ failure and outcome [2, 3]. However, this technique is still used predominantly as a research tool for a variety of reasons, including its inability to provide continuous on-line measurement.
The oxygen tension (PO2) of urine has been suggest- ed as a potential means of monitoring renal perfusion. Previous studies have shown a relationship between renal blood flow and PO2 in both renal medullary and cortical tissue [4] and urine PO2 measured at the renal pelvis [5]. However, an early study by Rennie et al. [6] suggested that this relationship could not be extended to the PO2 of urine in the bladder as urine itself may consume oxygen, and that gaseous exchange may take place between the urine and the walls of the extra-renal urinary tract. Nevertheless, re-investigation was felt to be worthwhile, particularly as measurement of urinary PO2 could now be facilitated by an accurate, continu- ously measuring oxygen electrode sited within a blad- der being continually drained through a catheter. How- ever, a pilot experiment in a rat model revealed almost immediate changes in PO2 following intravascular vol- ume repletion or depletion, allowing for the 90% cath- eter response time of 90 s. The rapidity of change in bladder PO2 following such a manoeuvre, in the face of negligible urine output, suggested that the electrode was measuring the PO2 of the epithelial lining of the bladder rather than that of the urine. An experiment was thus designed to measure changes in bladder epi- thelial PO2 with concurrent measurement of renal blood flow, aortic blood flow, and systemic blood pres- sure during staged exsanguination and volume reple- tion in a rat model.
Materials and methods
This experiment was performed in accordance with the principles of laboratory animal care and under Home Office project licence. Male Sprague-Dawley rats weighing approximately 200 g were anaesthe- tised with 60 mg/kg thiobutabarbitone (Trapanal, BYK Guilden, Germany) injected intraperitoneally. The animal was maintained in a supine position on a thermostatically controlled heating table (Effenberger, Essen, Germany) to maintain rectal temper- ature at approximately 37~ and continued to breathe room air spontaneously.
The right internal jugular vein was exposed and cannulated with Portex tubing of 0.58 mm internal diameter (ID) through which a continuous infusion of 4 ml/h isotonic saline solution was adminis-
tered. The left carotid artery was also cannulated with 0.58 mm ID Portex tubing; this was kept patent by heparinised saline and connected to an external pressure transducer system (BLPR, WPI, Miami, Fla.) to enable continuous monitoring of mean arterial blood pressure. Portex tubing of ID 1.57 mm was inserted into the trachea to enable removal of secretions by absorbent tissue paper.
A midline laparotomy was performed. The bladder was exposed and cannulated with Portex tubing of ID 1.14 and 0.58 mm, respec- tively. Urine was allowed to drain freely from both tubes. The intestines were lifted from the abdominal cavity, covered in saline- soaked swabs, and placed in a plastic bag to reduce fluid and heat loss, The left renal artery was exposed and dissected clear of the renal vein and any significant amounts of connective or adipose tissue. A 1-gauge perivascular Doppler flow probe was placed around the artery and connected to a self-calibrating dual-channel Doppler ftowmeter (Model T206, Transonic Systems, Ithaca, N.Y. A similar procedure was performed on the abdominal aorta distal to the renal arteries around which a 2-gauge perivascular Doppler flow probe was placed and then connected to the other channel of the flowmeter. This measured flow predominantly to the pelvis, tail and hindlimbs. Acoustic gel was applied to both probes, and good coupling was confirmed by the signal strength displayed on the flowmeter. The accuracy of the internal self-calibration was also confirmed. Outputs for both Doppler probes and the pressure trans- ducer measuring systemic blood pressure were connected to a Mac- Lab recording system (ADI Instruments, Milford, Mass.).
A continuous oxygen-measuring modified Clark electrode of Ag-AgC1 design and 0.5 mm in diameter (Continucath 1000, Bio- medical Sensors, High Wycombe, U.K.) was advanced through the larger of the bladder cannulae. The 1 cm exposed length of the electrode at the catheter tip was coiled within and in contact with the epithelial lining of the bladder; the catheter was connected to its monitor. After a minimum period of 10 min to allow for catheter stabilisation during which haemodynamic stability was mandatory, the electrode was calibrated against the PO2 of a fresh urine speci- men draining into a heparinized capillary tube placed over the distal end of the smaller bladder catheter. The POz of the urine specimen was measured on a previously calibrated pH/blood gas analyser (Model 178, Ciba-Corning, Halstead, Essex, UK) which was also suitable for urine oxygen measurement. Blood gas was also analysed on the same machine using arterial blood samples drawn from the carotid artery cannula into heparinized capillary tubes after suffi- cient volume had been removed to account for dead-space in the tubing. This dead-space volume was then returned to the animal to prevent fluid depletion as a consequence of blood sampling.
After calibration of the oxygen electrode to urine PO2, baseline recordings of renal and aortic blood flow, systemic BP, body temper- ature, arterial blood gas analysis and bladder epithelial POz were taken.
A 1-ml bolus of isotonic saline was given over 30-45 s. The above recordings were repeated at 1, 3, 5 and 10 min (other than arterial blood gas analysis which was performed only at 10 min) following completion of the bolus. Unless no change was seen in either sys- temic arterial pressure or renal flow, a further fluid challenge was administered and recordings made as above. This procedure was repeated until no further increase was seen in either systemic blood pressure, aortic or renal blood flow, at which point adequate intra- vascular fluid repletion was assumed. Then 1 ml blood was slowly drawn off the carotid artery line over 30-45 s into a heparinized syringe. A small amount was used for blood gas analysis while the remainder was stored for later return to the animal. Measurements of aortic and renal blood flow, arterial pressure, bladder PO2 and temperature were taken at 1, 3, 5 and 10 min. This procedure was repeated until renal blood flow fell by at least 50% from the value obtained at the end of the fluid repletion phase. Repeat arterial gas analysis was then performed.

326
The animal was then volume-repleted with 1 to 2-ml aliquots of stored blood (or isotonic saline if all the blood had been returned). The size of aliquot was determined by the general circulatory status of the animal. Measurements were made at 1, 3, 5 and 10 rain following each fluid challenge, and the procedure was repeated until intravascular fluid repletion was achieved, as judged by no further increase in systemic arterial pressure or renal blood flow. After the second fluid repletion phase, the animal was progressively exsan- guinated by 1-ml aliquots until cardiovascular collapse. Measure- ments were taken at 1, 3, 5 and 10 min following each withdrawal, including arterial blood gas analysis at each 10 min sample.
Statistical analysis was performed by repeated measures analysis of variance with post hoc Fisher PLSD tests, and the Spearman rank correlation coefficient test was used to determine whether a signifi- cant relationship existed between percentage changes from baseline values in bladder 02 and percentage changes in blood pressure, PaO2 and PaCO2, renal and aortic blood flow, and base deficit.
Results
Eight rats were studied with weights of 164-238 g (mean 209 g). The bladder PO2 reading changed within 30 s of fluid removal/addition. Systemic blood pressure and renal and aortic blood flow fluctuated over the first three rain while intra- and extravascular fluid com- partments were re-equilibrating; however, cardiovascu- lar stability was generally achieved by 5 min. The 10- min readings were used for subsequent analysis of results.
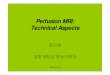
Figure 1 shows the changes in bladder epithelial PO2, aortic and renal blood flow, and systemic blood pressure at (1) baseline, (2) the end of the first fluid repletion phase, (3) the end of the first exsanguination phase, (4) the end of the second fluid repletion phase and, (5) at three evenly spaced time intervals during the final exsanguination phase. Changes from baseline were significant for bladder PO2, aortic and renal blood flow, and systemic BP, even at the end of the first exsanguination phase (p < 0.001 for all except aortic blood flow where p < 0.05). An obvious relationship was seen throughout between changes in bladder PO2, aortic and renal blood flow and systemic blood pres- sure. A significant relationship was seen between per- centage changes in bladder PO2 and mean blood pres- sure (p = 0.79, p = 0.05), aortic blood flow and renal blood flow (p = 0.74, p = 0.05).
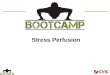
Figure 2 shows the relationship between bladder PO2 and arterial blood measurements of PaO2, PaCO2 and standard base deficit. As the animal became hy- povolaemic, it hyperventilated in an attempt to com- pensate for the increasing metabolic acidosis. Despite an increase in arterial PO2 on exsanguination, the bladder epithelial PO2 progressively fell. A significant relationship existed between percentage change in bladder PO2 and both base deficit (p = 0.64, p = 0.05),
Bladder PO 2 (kPa) renal/aortic blood flow (mL/min)
20~
15-
10-
mean BP (mmHg)
125
"100
?
al
"_~
I I I ] I
.c
kl.l t.U
-75
-50
-25
0
Fig. 1 Changes in bladder epithelial PO 2 (white diamonds), aortic blood flow (black triangles) renal blood flow (squares) and systemic mean blood pressure (circles) at (1) baseline, (2) the end of the first fluid repletion phase, (3) the end of the first exsanguination phase, (4) the end of the second fluid repletion phase and, (5) three evenly spaced time intervals dmZing the final exsanguination phase. Results expressed as mean _+ SE
and arterial PaCO2 (p = 0.74, p = 0.05). However, an inverse correlation was seen with arterial PaO2 (p = - 0.65, p = 0.05).
Discussion
In this acute exsanguination/fluid repletion model, changes in PO2 measured inside the bladder promptly reflected systemic as well as regional circulatory changes. However, no relationship was seen between bladder and arterial PO2, suggesting that bladder PO2 is independent of arterial blood PO2, at least in the normoxaemic range. Metabolic acidosis as determined by the increasing base deficit did not become marked until the terminal stages of the experiment. To prevent excessive haemodilution by blood sampling we used base deficit rather than lactate as a surrogate marker of tissue ischaemia. Indeed, a recent study in a dog model by Waisman et al. [7] showed that the base deficit was superior to lactate as a measure of the quantity of haemorrhage.

327
-10-
-15
Bladder PO 2 (kPa) Pa02, PaCO 2 (kPa) BE
20
15-
10-
5 -
0
-5-
I l I l I
n l n l
Fig. 2 Relationship between bladder epithelial PO 2 (white dia- monds) and arterial blood measurements of PaO 2 (black triangles), PaCO 2 (white squares) and standard base deficit (white circles) at baseline and at the end of each fluid repletion and exsanguination phase. Results expressed as mean _+ SE
Nelimarkka et al. [4] found that changes in renal blood flow are correlated with PO2 within the renal medulla and cortex. Kainuma et al. [-5] measured changes in urine PO2 using an indwelling oxygen elec- trode introduced through the ureter and positioned at the renal pelvis and found that these also correlated with changes in renal blood flow. This approach is obviously impractical in human subjects, but no studies have examined the relationship, if any, between the PO2 of bladder urine and renal blood flow. The use of a continuously measuring oxygen electrode sited within the bladder in our experiment revealed changes in PO2 within 30 s of a manoeuvre. The rapidity of change implies that urinary PO2 is not being measured, parti- cularly as urine production in this rat model was only 1-2 ml/h. By virtue of being constantly drained the bladder is collapsed, thus the oxygen electrode is in permanent contact with its epithelial lining. It is thus reasonable to assume that the electrode is measuring the PO2 within the epithelial layer.
The close relationship found in this model between bladder PO2 and both the systemic and renal circula- tions suggests that the bladder PO2 acts as a marker of circulatory status. Whether these changes in PO2 re-
flect alterations in perfusion of the bladder lining microvasculature and/or increased tissue oxygen ex- traction remains open to question. Nelimarkka and Niinikoski [8] showed that the oxygen extraction ratio of the kidney increases with graded haemorrhage in a dog model but is especially marked (from 22% to 58%) when total withdrawn blood volume increases from 30% to 40%. At the same time, however, renal blood flow fell from 50 + 4 to 12 + 2 ml/min and mean arterial pressure from 72 _+ 3 to 39 _+ 2 mmHg.
It can be hypothesised that the epithelial layer of the bladder wall is compromised by reductions in or- gan perfusion in similar fashion to the mucosal lining of the gut being first affected during splanchnic hypoper- fusion [9]. The early development of gut mucosal is- chaemia is the basis for the gut tonometric measure- ment of gastric mucosal pH being promoted as an early indicator of inadequate tissue perfusion. This technique utilises equilibration of intramucosal pCO2 with saline within an intraluminal balloon; however, a time delay is introduced as CO2 must first diffuse across the semi- permeable membrane of the balloon. A minimum 30- min equilibration period is recommended by the manu- facturers of the commercially available tonometer for optimal accuracy (Instruction Leaflet, Trip catheter, Tonometrics, Worcester, Mass.). Measurement of blad- der epithelial PO2 may potentially provide similar in- formation though with the advantages of no major time delay, patient comfort and constant updating with no operator effort required.
Further studies are obviously needed in which blad- der PO2 is measured in different situations of circula- tory instability. Reliability must be assessed over longer periods, particularly with regard to electrode drift. The relationship between changes in PO2 occurring within the bladder epithelium to splanchnic, other regional and systemic circulations requires study. If these condi- tions are satisfied, attention could turn to patient stud- ies. Correlation must be sought between low values and subsequent clinically apparent multiple organ dysfunc- tion and complications. The sensitivity and degree of histological change of the bladder wall epithelium to systemic insults such as hypovolaemic and sepsis is unknown. Though microscopic haematuria is a com- mon finding in critically ill patients, it is often ascribed to bladder catheter trauma rather than epithelial is- chaemia. Frank haematuria is a much rarer event. Furthermore, though trends were utilised in this experi- ment, knowledge of absolute values of bladder epi- thelial PO2 would be useful. In this study the oxygen electrode was calibrated against urine PO2 obtained while the animal was in a steady state at the beginning of the experiment. These values were similar to those

328
obtained from urine in the renal pelvis by Ka inuma et al. [5]. Ongoing studies utilising preinsertion calibration of the electrode in degassed saline are pro- ducing approximately similar values and may be more accurate.
In conclusion, measurement of bladder epithelial PO2 may offer a quick, simple and cont inuous means of moni tor ing regional organ perfusion. Global circula- tory variables such as lactate and mixed venous oxygen
saturat ion do not necessarily exclude or confirm re- gional organ hypoperfusion [-10, 11]. This new ap- proach could prove to be a valuable moni tor ing tool and may potentially provide useful early warning of organ hypoperfusion and, possibly, an appropriate treatment endpoint.
Acknowledgements We would like to acknowledge the support of Biomedical Sensors.
References
1. Antonsson JB, Boyle CC, KursthoffKL, Wang HL, Sacristan E, Rothschild HR, Fink MP (1990) Validation of tonomet- ric measurement of intramural pH during endotoxemia and mesenteric occlusion in pigs. Am J Physiol 259: G519-G524
2. Doglio GR, Pusajo JF, Egurrola MA, Bonfigli GC, Parra C, Vetere L, Hernandez MS, Fernandez S, Palizas F, Gutierrez G (1991) Gastric mucosal pH as a prognostic index of mortality in critically ill patients. Crit Care Med 19: 1037-1040
3. Mythen MG, Webb AR (1994) Intra- operative gut mucosal hypoperfusion is associated with increased post-operative complications and cost. Intensive Care Med 20:105-108
4. Nelimarkka O, Halkola L, Niinikoski J (1984) Renal hypoxia and lactate metabolism in hemorrhagic shock in dogs. Crit Care Med 12:656-660
5. Kainuma M, Kimura N, Shimada Y (1990) Effect of acute changes in renal arterial blood flow on urine oxygen tension in dogs. Crit Care Med 18:309-312
6. Rennie DW, Reeves PB, Pappenheimer JR (1958) Oxygen pressure in urine and its relation to intrarenal blood flow. Am J Physiol 195:120-132
7. Waisman Y, Eichacker PQ, Banks SM, Hoffman WD, MacVittie TJ, Natanson C (1993) Acute hemorrhage in dogs: construction and validation of models to quantify blood loss. J AppI Physiol 74:510-519
8. Nelimarkka O, Niinikoski J (t984) Oxygen and carbon dioxide tensions in the canine kidney during arterial occlu- sion and hemorrhagic hypotension. Surg Gynecol Obstet 158:27-32
9. Gilmour DG, Aitkenhead R, Hothersall AP, Ledingham IM (1980) The effect of hypovolaemic on colonic blood flow in the dog. Br J Surg 67:82-85
10. van Lambalgen AA, Runge HC, van den Bos GC, Thijs LG (1988) Regional lactate production in early canine endotoxin shock. Am J Physiol 254: E45-51
11. Kyff JV, Vaughn S, Yang SC, Raheja R, Puri VK (1989) Continuous monitoring of mixed venous oxygen saturation in patients w i t h acute myocardial infarction. Chest 95:607-611