Embed Size (px)
Citation preview

Coavriwht Acta AnurJthesz~l SLand I99S Artu Anuesthrsiol Scand 1995: 39: Supplementum 107, 77-80 Printed in Denmark ~ all rights reserved Acta Anaesthesiologica
Scandinavica ISSN 0515-2720
ISBN 87- 16.151 73-9
Bladder epithelial oxygen tension as a marker of organ perfusion M. SINGER, D. ROSSER AND R. STIDWILL Bloomsbury Institute of Intensive Care Medicine, University College London Medical School, Rayne Institute, London, UK
Key words: Bladder; hemodynamics; oxygen tension; organ pertusion; tissue oxygenation.
A tissue oxygen deficit can be both precursor and endpoint of multiple organ dysfunction. Shoemaker et al. (1) demonstrated how persistence and severity of a post- operative tissue oxygen debt correlated with subsequent complications. This group and others (2, 3) have shown how postoperative maintenance of adequate levels of global perfusion had a clearly demonstrable benefit on mortality, morbidity, hospital stay and costs. Circulatory manipulations were performed by fluid and dobutamine (I) , fluid and dopexamine (2), or fluid alone (3). Once the oxygen debt is established and the patient is critically ill, belated attempts to improve global blood flow and oxygen transport caused, if anything, a poorer outcome (4). Tissue hypoxia is a potent stimulator of inflamma- tory mediators including nitric oxide (5-7) while activa- tion of inflammatory cascades causing (i) microvascular obstruction by aggregated neutrophils and platelets, (ii) vasoconstriction from local release of vasoactive media- tors such as endothelins and thromboxanes, (iii) endo- thelial leak and interstitial oedema all contribute to tissue hypoxia. The high mixed venous oxygen saturation seen in sepsis in the face of a coexisting metabolic deficit is often ascribed to shunting of oxygenated blood away from nutrient capillaries (8- 10). However, definitive evidence for this hypothesis is lacking.
A further problem lies in monitoring of tissue hypoxia. Covert tissue hypoxia often passes unrecognised, despite a seemingly adequate circulation (1 1) while current means of early identification are also limited. Global indices of anaerobic respiration such as an increasing base deficit (acidaemia) or hyperlactataemia are used but, in terms of sensitivity and specificity, neither are perfect. High blood lactate levels may be found in accelerated aerobic glycolysis, liver dysfunction, post-seizures, and
with the use of lactate-buffered renal replacement fluid (12-14) while an elevated base deficit may reflect, for example, deteriorating renal function. A further problem arises when the area of ischaemia is localised, e.g., a segment of bowel or bowel mucosa. Lactate and hydro- gen ions draining from this region will be diluted in the central blood stream and only when hepatorenal and blood buffering mechanisms for clearing these ions are overwhelmed will abnormal blood levels be detected.
The Holy Grail of circulatory monitoring is to have a device that can monitor simply, reliably, with minimal invasiveness, and with a high degree of sensitivity, speci- ficity ... and affordability. It should be able to assess the adequacy of perfusion at a regional level and should also reflect the adequacy of perfusion of the vital organs. This detection should be as early as possible and it should serve as an appropriate treatment endpoint.
Tissue hypoxia can be measured locally either by as- sessing the level of substrate, i.e., oxygen, or by measur- ing of one or more of the consequences of altered metab- olism, e.g., intracellular acidosis, redox status, high energy phosphate status or C02 production. The latter is the principle underlying gut tonometry whereby acid production from anaerobic gut mucosal metabolism is buffered by tissue bicarbonate with subsequent release of carbon dioxide. The PCO, equilibrates with saline within the tonometer; this can be measured and used in a mod- ified Henderson-Hasselbalch equation to provide the gut mucosal pHi, a low value of which is indicative of local ischaemia (15, 16). As the splanchnic circulation is claimed to be the first area undergoing ischaemia during decreased blood flow (e.g., haemorrhage) (17, 18), the tonometer is touted as an early warning device though this has yet to be validated in clinical practice. Further-
0 Acta Anaesthesiologica Scandinavica 39 (1995)

78 M. SINGER ET AL.
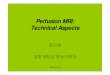
renal a,- Doppler flow probo 1
urlnc drainage
Fig. 1
more, the derivation of pHi relies upon substitution of arterial bicarbonate for tissue bicarbonate, an assumption which appears to be seriously flawed (19, 20).
Studies involving oxygen tension measurement within tissue beds are numerous and include brain, skin, subcu- taneous tissue, conjunctiva, liver, kidney and gut (21-3 1). These are taken from serosal or mucosal surfaces, from a direct intra-parenchymal approach or from effluent drainage, e.g., urine, venous blood (34-36). Relationships have been shown experimentally between the adequacy of blood flow and tissue oxygen tension while in both patient studies and animal models, tissue oxygen tension appears to be a good and early indicator of the degree of blood loss. It has also been used to assess the viability of tissue grafts (37).
In performing studies in a rat model to evaluate changes in urine oxygen tension during various circulatory insults, a continuously monitoring Clark-type oxygen electrode was sited in the bladder lumen to facilitate monitoring. Changes in PO, occurred within seconds of a manoeuvre making it more likely that bladder rather than urine PO, was being measured, particularly as the bladder lumen was collapsed (urine was being drained continuously) and the active tip of the electrode (1 cm . 0.55 mm) was in direct contact with the bladder epithelium. As the data are contemporaneous and currently undergoing peer review, only a description of the model and an overview of results will be given to not jeopardise subsequent publication.
Male Sprague-Dawley rats are anaesthetized, tracheo- stomised and left spontaneously breathing on room air. In our initial experiments intraperitoneal thiobuta- barbitone was used for anaesthesia though, latterly, this has been replaced by halothane which was found to provide better haemodynamic stability. The animal is
b... I
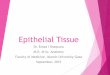
Fig. 2.
placed on a heating table to maintain core temperature at 37 "C and instrumented with carotid and internal jugular lines for arterial and central venous pressure monitoring, intermittent sampling for blood gas analysis and infusion of drugs and fluid. A baseline fluid infusion of 2 mL/lOO g body wt/hr is commenced. A midline ab- dominal laparotomy is then performed for placement of Doppler flow probes around the left renal artery and infrarenal abdominal aorta. The bladder is cannulated directly to allow continuous free drainage of urine and to keep the bladder in a collapsed state. A continuous Clark-type electrode of Ag/AgCl design (Continucath, Biomedical Sensors, High Wycombe, UK) is introduced alongside the bladder cannula and coiled within the collapsed bladder lumen such that the active tip of the electrode is in contact with the bladder wall (Fig. 1). The abdominal cavity is then covered with clingfilm to decrease any evaporative and thermal losses. After a stabilisation period of at least 60 minutes and confirma- tion of cardiorespiratory stability, the rat undergoes one of a variety of manoeuvres. These have included haem- orrhage, hypoxaemia, vasoactive drugs (dobutamine, noradrenaline), and endotoxin (20 mgkg bolus and

BLADDER EPITHELIAL OXYGEN TENSION AS A MARKER OF ORGAN PERFUSION 79
10 mgkg infusion over 30 minutes to create hypo- and hyperdynamic models, respectively).
Fig. 2 shows a summary of findings to date. The oxy- gen tension in the bladder epithelium appears to be a very sensitive indicator of circulatory disturbance, chang- ing in line with arterial base deficit in all conditions other than sepsis. In this situation, creation of both hypo- and hyperdynamic endotoxaemic models produced a consistent rise in bladder epithelial oxygen tension des- pite marked metabolic acidosis. This implies that the tissue oxygen debt seen in sepsis may be related more to defects in utilization of oxygen at celluladmitochondrial level rather than microcirculatory oxygen delivery. More work is obviously needed and studies are currently ongoing in our laboratory.
CONCLUSION
Tissue hypoperfusion is often difficult to detect, especial- ly at an early stage where prompt correction may result in maintenance of organ function and an improved out- come. Current methodologies in clinical use for deter- mining the adequacy of organ perfusion all have limita- tions. Monitoring of tissue oxygenation has shown poten- tial for a number of years; perhaps the bladder epithelial approach may prove to be a clinically useful tool as it is relatively non-invasive and easily accessible in critically ill or high-risk patients via a Foley catheter. The finding of an increase in bladder epithelial oxygen tension in sepsis despite apparent anaerobic tissue metabolism war- rants further investigation.
REFERENCES
I .
2.
3.
4.
5.
6.
Shoemaker W C, Appel P L, Kram H B. Tissue oxygen debt as a determinant of lethal and nonlethal postoperative organ failure. Crit Cure Med 1988: 16: 1117-1120. Boyd 0, Grounds R M, Bennett E D. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA 1993: 270: 2699-2707. Mythen M G , Webb A R. Per-operative plasma volume expan- sion reduces the incidence of gut mucosal hypoperfusion in cardiac surgery. Ann Surg 1995 (in press). Hayes M A, Timmins A C, Yau E H, Palazzo M, Hinds C J, Watson D. Elevation of systemic oxygen delivery in the treat- ment of critically ill patients. N Engl J Med 1994: 330: 1717- 1722. Gerlach H, Gerlach M, Clauss M. Relevance of tumour necrosis factor-alpha and interleukin- I-alpha in the pathogenesis of hypoxia-related organ failure. Eur J Anuesthesiol 1993: 10: 273- 285. Ghezzi P, Dinarello C A. Bianchi M, Rosandich M E, Repine J E, White C W. Hypoxia increases production of interleukin-1 and tumor necrosis factor by human mononuclear cells. Cyro- kine 1991: 3: 189-194.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
Yu L, Gengaro P E, Niederberger M, Burke T J, Scrier R W. Nitric oxide: a mediator in rat tubular hypoxidreoxygenation injury. Proc Natl Acad Sci 1994: 91: 1691-1695. Powell R J, Machiedo G W, Rush B F Jr. Decreased red blood cell deformability and impaired oxygen utilization during human sepsis. Am Surg 1993: 59: 65-68. Rogers F, Dunn R, Barett J, Merlotti G, Sheaff C, Nolan P. Alterations of capillary flow during sepsis. Circ Shock 1985: 15: 105-110. Dantzker D. Oxygen delivery and utilization in sepsis. Crit Cure Clin 1989: 5: 81-98. Bihari D, Smithies M, Gimson A, Tinker J . The effects of vasodilatation with prostacyclin on oxygen delivery and uptake in critically ill patients. N Engl J Med 1987: 317: 397-403. Curtis S E, Cain S M. Regional and systemic oxygen deliv- eryhptake relations and lactate flux in hyperdynamic, endo- toxin-treated dogs (see comments). Am Rev Respir Dis 1992: 145: 348-354. Cerra F B. Multiple organ failure: Is it only hypoxia? In: Gutierrez G, Vincent JL, eds. Tissue oxygen utilization. Berlin, Heidelberg: Springer Verlag 1991: 242-251. Nimmo G R, Mackenzie S J, Walker S, Nicol M, Grant I S. Acid-base responses to high-volume haemofiltration in the criti- cally ill. Nephrol Dial Transplant 1993: 8: 854-857. Antonsson J B, Boyle C C, Kruithoff K L, et al. Validation of tonometric measurement of gut intramural pH during endotox- emia and mesenteric occlusion in pigs. Am J Physiol 1990: 259:
Marik P E. Gastric intramucosal pH. A better predictor of multi- organ dysfunction syndrome and death than oxygen-derived variables in patients with sepsis. Chest 1993: 104: 225-229. Price H L, Deutsch S, Marshall B E, Stephen G W, Behar M G, Neufeld G R. Hemodynamic and metabolic effects of hemor- rhage in man with particular reference to the splanchnic circula- tion. Circ Res: 18: 469-474. Reilly P M, Bulkley G B. Vasoactive mediators and splanchnic perfusion. Crit Care Med 1993: 21, Suppl 2: S55-68. Schlichtig R, Bowles S A. Distinguishing between aerobic and anaerobic appearance of dissolved C0, in intestine during low flow. JAppl Physiol 1994: 76: 2443-2451. Desai V S, Weil M H, Tang W. Yang G, Bisera J. Gastric intra- mural PCO, during peritonitis and shock. Chest 1993: 104: 1254-1258. Shoemaker W C, Fink S, Ray C W, McCartney S. Effect of hemorrhagic shock on conjunctival and transcutaneous oxygen tensions in relation to hemodynamic and oxygen transport changes. Cn't Care Med 1984: 12: 949-952. Makisalo H J, Soini H 0, Tapani Lalla M I, Hockerstedt K A. Subcutaneous and liver tissue oxygen tension in hemorrhagic shock: an experimental study with whole blood and two colloids. Crit Care Med 1988: 16: 857-861. Gottmp F, Gellett S, Kirkegaard L, Hansen E S, Johansen G . Effect of hemorrhage and resuscitation on subcutaneous, conjunctival, and transcutaneous oxygen tension in relation to hemodynamic variables. Crit Care Med 1989: 17: 904-907. Dahn M S, Wilson R F, Lange P, Stone A, Jacobs L A. Hepatic parenchymal oxygen tension following injury and sepsis. Arch Surg 1990: 125: 441-443. Soini H 0, Takala J, Nordin A J, Makisalo H J, Hockerstedt K A. Peripheral and liver tissue oxygen tensions in hemorrhagic shock. Crit Care Med 1992: 20: 1330-1334. Hartmann M, Montgomery A, Jonsson K, Haglund U. Tissue oxygenation in hemorrhagic shock measured as transcutaneous oxygen tension, subcutaneous oxygen tension, and gastrointestinal intramucosal pH in pigs. Crit Care Med 1991: 19: 205-210.
G5 19-523.

M. SINGER ET AL. 80
27.
28.
29.
30.
31.
32.
33.
34.
Sheridan W G, Lowndes R H, Williams G T, Young H L. De- termination of a critical level of tissue oxygenation in acute intestinal ischaemia. Cut 1992 33 762-766. Nelimarkka 0, Halkola L, Niinikoski J. Effect of graded hemor- rhage on renal cortical perfusion in dogs. Am J Surg 1981: 141:
Nelimarkka 0, Halkola L, Niinikoski J. Renal hypoxia and lactate metabolism in hemorrhagic shock in dogs. Crit Care Med 1984: 12: 656-660. Kram H B, Appel P L, Fleming A W, Shoemaker W C. Assess- ment of intestinal and renal perfusion using surface oximetry. Crit Care Med 1986: 1 4 707-713. Gullichsen E, Nelimarkka 0, Halkola L, Niinikoski J. Renal oxygenation in endotoxin shock in dogs. Crit Care Med 1989:
Boekstegers P, Weidenhofer S, Pilz G, Werdan K. Peripheral oxygen availability within skeletal muscle in sepsis and septic shock comparison to limited infection and cardiogenic shock. J hfect 1991: 19: 317-323. Gutierrez G, Lund N, Palizas F. Rabbit skeletal muscle PO2 during hypodynamic sepsis. Chest 1991: 9 9 224-229. Kainuma M, Kimura N, Shimada Y. Effect of acute changes in
235-239.
17: 547-550.
renal arterial blood flow on urine oxygen tension in dogs. Crit Care Med 1990: 18: 309-312. Wong D H, Weir P D, Wesley R C, Gordon I L, Weber E C, Zaccari J, Ferraro L M, Tremper K K. Changes in renal vein, renal surface, and urine oxygen tension during hypoxia in pigs. J Clin Monit 1993: 9: 1-4. Hurtado F J, Gutierrez A M, Silva N, Fernandez E, Khan A E, Gutierrez G. Role of tissue hypoxia as the mechanism of lactic acidosis during E. coli endotoxemia. J AppZ Physior 1992: 72:
Hofer S 0, Timmenga E J, Christian0 R, Bos K E. An intra- vascular oxygen tension monitoring device used in myocutaneous transplants: a preliminary report. Microsurgery 1993: 19: 304-309.
35.
36.
1895-1901. 37.
Address: Metvyn Singer, M.D. Bloomsbury Institute of Intensive Care Medicine University College London Medical School Rayne Institute University Street London WClE 6JJ, UK