Embed Size (px)
Citation preview

BLITZ Heart Failure (HF)
Protocol Number K15
Version 4.0 – August 1, 2016
Study promoted by Heart Care Foundation-ANMCO
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 2
TABLE OF CONTENTS
Signature page for Study Chairman and Co-Chairmen ............................................................................................... 3
Signature Page for Principal Investigator ...................................................................................................................... 4
LIST OF ABBREVIATION ............................................................................................................................................ 5
SUMMARY ....................................................................................................................................................................... 6
1. BACKGROUND AND RATIONALE ........................................................................................................................ 8
2. STUDY OBJECTIVES ................................................................................................................................................ 9
2.1 Primary objectives .................................................................................................................................................... 9
2.2 Secondary objectives ................................................................................................................................................ 9
3. STUDY POPULATION ............................................................................................................................................... 9
3.1 Inclusion criteria ....................................................................................................................................................... 9
3.2 Exclusion criteria .................................................................................................................................................... 10
4. STUDY OUTCOME MEASURES ............................................................................................................................ 10
4.1 Primary end-points ................................................................................................................................................. 10
4.2 Secondary end-points ............................................................................................................................................. 12
5. INVESTIGATIONAL PLAN .................................................................................................................................... 13
5.1 Study Design .......................................................................................................................................................... 13
5.2 Study Phases ........................................................................................................................................................... 13
5.3 Certification ............................................................................................................................................................ 15
5.4 Data Collection ....................................................................................................................................................... 15
6. STUDY VARIABLES ................................................................................................................................................ 15
6.1 Baseline data .......................................................................................................................................................... 15
6.2 Follow-up data ........................................................................................................................................................ 16
7. STATISTICAL CONSIDERATIONS ...................................................................................................................... 16
8. SAFETY ASPECTS .................................................................................................................................................... 17
9. STUDY ORGANIZATION ........................................................................................................................................ 17
9.1 Study sponsor ......................................................................................................................................................... 17
9.2 Steering Committee ................................................................................................................................................ 17
9.3 Executive Committee ............................................................................................................................................. 17
9.4 Participating Centers .............................................................................................................................................. 17
9.5 Monitoring Procedures ........................................................................................................................................... 18
9.6 Publication Policy................................................................................................................................................... 18
10. ETHICAL ISSUES ................................................................................................................................................... 18
11. STUDY DURATION ................................................................................................................................................ 19
REFERENCES ............................................................................................................................................................... 20
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 3
Dott. Michele Massimo Gulizia
Dott. Andrea Di Lenarda
August 1st, 2016
Dott. Fabrizio Oliva
August 1st, 2016
August 1st, 2016
Signature page for Study Chairman and Co-Chairmen
Protocol:
BLITZ Heart Failure (HF)
Approved by:
__________________________________ _______________________ ____________
Chairman Signature Date
__________________________________ _______________________ _____________
Co-Chairman Signature Date
__________________________________ _______________________ _____________
Co-Chairman Signature Date
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 4
Signature Page for Principal Investigator
Protocol:
BLITZ Heart Failure (HF)
I have read this protocol and I agree to conduct this study in accordance with all stipulations of the
protocol and in accordance with the current regulations.
(Principal Investigator) Signature date
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 5
LIST OF ABBREVIATION
AF Atrial fibrillation
ANMCO Associazione Nazionale Medici Cardiologi Ospedalieri
(Italian Association of Hospital Cardiologists)
CRT-D Cardiac Resynchronization Therapy with ICD
CRT-P Cardiac Resynchronization Therapy
EF Ejection Fraction
HCF Heart Care Foundation
HF Heart Failure
HFmrEF mid range LV ejection fraction (EF 40-49%)
HFpEF preserved LV ejection fraction (EF ≥50%)
HFrEF reduced LV ejection fraction (EF <40%)
ICD Implantable Cardioverter Defibrilaltor
MRA Mineralocorticoid Antagonist
NSAIDS Non steroidal anti-inflammatory drugs
OAC Oral Anticoagulants
SBP Systolic Blood Pressure
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 6
SUMMARY
Project Title BLITZ Heart Failure (HF)
Sponsor Fondazione per il Tuo cuore – HCF Onlus
Principal Investigator Dott. Michele Massimo Gulizia – Dott. Andrea Di Lenarda –
Dott. Fabrizio Oliva
Rationale and aims of
the study
Observational studies and administrative data indicate that diagnostic
and therapeutic pathways in heart failure (HF) are still inadequate both
in the hospital and after discharge and that the use of recommended
treatments is at least sub-optimal. The implementation of a structured
network for the management of patients with HF, with shared objectives
and integrated between hospital and territory, has yet to be implemented.
The main aim of this project is to reduce, if needed, the possible gap
between guidelines recommendations and the daily clinical practice in
each participating centre.
Population Patients admitted for acute heart failure (AHF) and outpatient with
chronic heart failure (CHF).
Study Design Multicentre, cross-sectional, prospective, non-interventional,
observational study.
Main Study Objective To improve the level of adherence to current ESC guidelines
recommendations in both acute and chronic HF patients enrolled in each
participating center.
To verify if a specific HF educational intervention composed by an
educational web based program of data collection and face to face
meetings is able to improve adherence to guidelines recommendations
evaluated during a second enrollment period.
Inclusion Criteria ‐ All consecutive patients with chronic HF and those admitted for
acute (de novo or worsening) HF. The diagnosis of HF (both acute
and chronic) will be defined locally following the current ESC
guidelines.
‐ Chronic HF: any NYHA class (I-IV).
‐ Acute HF: Only patients in NYHA class III or IV, or with
pulmonary edema or cardiogenic shock treated with an IV infusion
(inotropes, vasodilators or vasopressor) will be included.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 7
‐ Any gender.
‐ Any etiology of HF.
‐ Any level of EF.
‐ Written informed consent.
Exclusion Criteria ‐ Age <18 years
‐ Inclusion in registries or trials that can influence, by protocol, the
clinical management of patients.
‐ Patients already enrolled in the BLITZ HF (by another participating
centre or in the first enrollment period).
Data Collection Data will be collected in two different enrollment phases lasting 3
months (or for at least 50 patients per center); the second phase will be
done 6 months after the first phase.
Follow-up period All patients with chronic HF and acute HF included in the study in the
first and second enrolling phase will enter a longitudinal follow-up visit
at 6 and 12 months.
Data collected at 12 months will include mortality and morbidity
outcomes, and assessment of applicable indicators to derive individual
and composite adherence measures.
Participating Centers Approximately 160 Italian Cardiology Centers
Sample size Considering the explorative and observational nature of the current
study, no formal sample size calculation has been performed. However,
the current study is aiming at a sample of at least 5000 patients from 160
centers to allow the evaluation of patients hospitalized for acute HF and
of those with chronic HF and with different levels of ejection fraction
(EF): reduced, mid range and preserved.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 8
1. BACKGROUND AND RATIONALE
Heart Failure (HF) is associated with a high burden of mortality and morbidity, poor quality of life
and elevated healthcare costs in both US and Europe. Despite significant advances in diagnosis and
therapy over the past 20 years, patients with HF continue to have a poor long-term prognosis;
recurrent hospital admissions are common and contribute to progression of HF and escalating
expenditures (1-2). Registries and surveys describing clinical characteristics of patients with both
chronic HF and acute HF, demonstrated that adherence to evidence-based medicine, as proxy for
high-quality care and appropriate pharmacological/non-pharmacological management, remains
suboptimal (3-5). However implementation of current guidelines (6) in real world clinical practice
has been infrequently targeted. One such example is the Get With the Guidelines® (GWTG) initiative
by the American Heart Association (7).
In Italy, as well as in other developed countries, prevalence of HF is increasing due to ageing of the
population and progress in the treatment of cardiovascular disease. However both observational
studies and administrative data point out that incorporation of international guidelines
recommendations and targets set by the national document "Struttura e Organizzazione Funzionale
della Cardiologia" (8) lags behind during both the in-hospital and post-discharge transition phases (3-
4). Diagnostic pathways are often poorly defined, the use of evidence-based pharmacological
therapies and device treatments is suboptimal (5,9), the vulnerable phase of post-discharge transition
to home and patient empowerment through education is often inadequately addressed (10-11). An
integrated professional network supported by shared targets between community and hospital care is
far from being implemented.
Knowledge gaps include identification of patient profiles that might benefit from specific treatments
(12) and information on the prevalence, clinical characteristics and prognosis of HF-associated valve
heart disease, that may worsen the syndrome or precipitate acute exacerbations and might benefit
from novel, non surgical correction options (13-14).
The large experience accumulated in Italy in web-based observational studies in patients with both
acute and chronic HF represents an ideal setting to conduct a quality improvement initiative in
cardiology centers during routine clinical care of HF patients with the aim of disseminating and
certifying updated multidisciplinary knowledge among health professionals devoted to the care of
patients with HF.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 9
2. STUDY OBJECTIVES
2.1 Primary objectives
- To improve the level of adherence to the most relevant recommendations reported by the current
ESC guidelines (6) in both acute and chronic HF patients enrolled in each participating center.
- To verify if a specific HF educational intervention composed by an educational web based
program of data collection and face to face meetings is able to improve adherence of participating
cardiologists to guidelines recommendations evaluated during a second enrollment period (see
section 5.2 for details) in each participating center.
2.2 Secondary objectives
- To describe the clinical characteristics and the outcomes of patients with HFmrEF, the new HF
category of patients recently introduced in the ESC guidelines
- To describe the organization of HF care at each center and at national level.
- To evaluate the impact of adherence to guidelines on patients’ outcomes at the National level.
- To describe how cardiologists manage valvular abnormalities associated with HF, such as aortic
stenosis or functional mitral regurgitation.
3. STUDY POPULATION
3.1 Inclusion criteria
‐ All consecutive patients with chronic HF and those admitted for acute (de novo) or worsening
chronic HF. The diagnosis of HF (both acute and chronic) will be defined locally following the
ESC guidelines (6).
‐ Chronic HF: any NYHA class (I-IV).
‐ Acute HF Only patients in NYHA class III or IV, or with pulmonary edema or cardiogenic shock
for whom an IV therapy specific for HF (diuretic, vasodilators, vasopressors) is administered.
‐ Any gender.
‐ Any etiology of HF.
‐ Any level of EF.
‐ Written informed consent.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 10
3.2 Exclusion criteria
‐ Age <18 years.
‐ Inclusion in registries or trials that can influence, by protocol, the clinical management of patients.
‐ Patients already enrolled in the BLITZ HF (by another participating centre or in the first
enrollment period).
4. STUDY OUTCOME MEASURES
4.1 Primary end-points
At the center level: To describe the level of adherence to the specific performance measures as
detailed in the Table considering the different clinical presentations (acute HF, chronic HFrEF,
chronic HFmrEF, chronic HFpEF).
At the National level: to compare the level of adoption of current ESC guidelines before and after
the use of the educational web based program of data collection and the educational face to face
meetings.
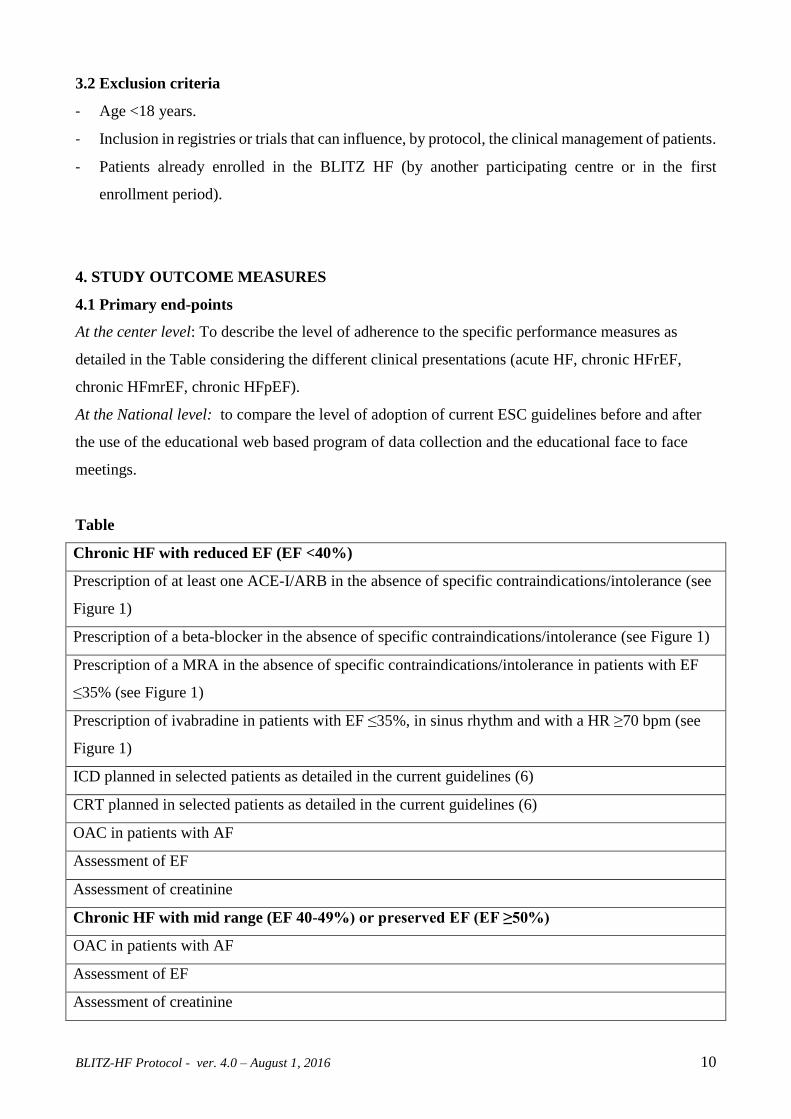
Table
Chronic HF with reduced EF (EF <40%)
Prescription of at least one ACE-I/ARB in the absence of specific contraindications/intolerance (see
Figure 1)
Prescription of a beta-blocker in the absence of specific contraindications/intolerance (see Figure 1)
Prescription of a MRA in the absence of specific contraindications/intolerance in patients with EF
≤35% (see Figure 1)
Prescription of ivabradine in patients with EF ≤35%, in sinus rhythm and with a HR ≥70 bpm (see
Figure 1)
ICD planned in selected patients as detailed in the current guidelines (6)
CRT planned in selected patients as detailed in the current guidelines (6)
OAC in patients with AF
Assessment of EF
Assessment of creatinine
Chronic HF with mid range (EF 40-49%) or preserved EF (EF ≥50%)
OAC in patients with AF
Assessment of EF
Assessment of creatinine
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 11
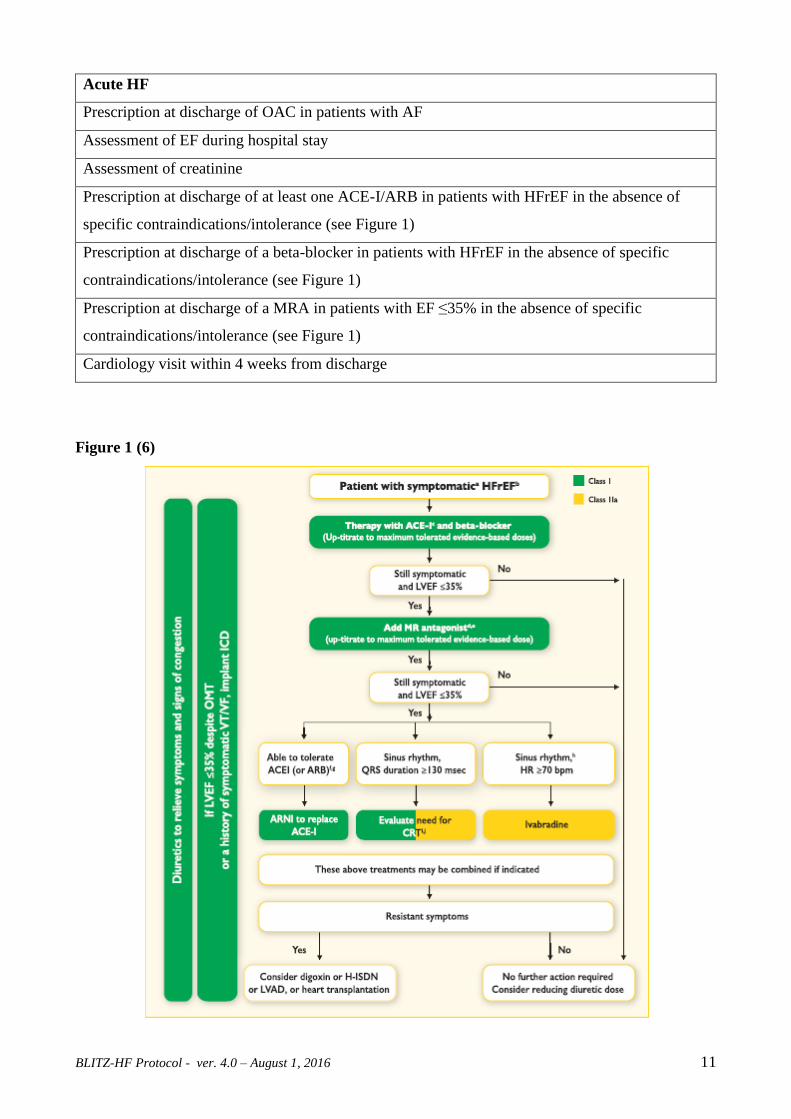
Acute HF
Prescription at discharge of OAC in patients with AF
Assessment of EF during hospital stay
Assessment of creatinine
Prescription at discharge of at least one ACE-I/ARB in patients with HFrEF in the absence of
specific contraindications/intolerance (see Figure 1)
Prescription at discharge of a beta-blocker in patients with HFrEF in the absence of specific
contraindications/intolerance (see Figure 1)
Prescription at discharge of a MRA in patients with EF ≤35% in the absence of specific
contraindications/intolerance (see Figure 1)
Cardiology visit within 4 weeks from discharge
Figure 1 (6)
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 12
4.2 Secondary end-points
At the National level:
4.2.1 The rate of patients with HFrEF receiving all the drugs recommended by current guidelines:
ACE-Is/ARBs, betablockers and MRAs, in the absence of specific contraindications/intolerance.
4.2.2 The rate of patients with chronic HFrEF with an indication to ICD and/or CRT planned in
clinical practice.
4.2.4 The rate of patients treated with oral anticoagulants in case of AF.
4.2.4 The rate of chronic HFrEF in patients with EF ≤35%, in sinus rhythm and with an HR ≥70
bpm treated with ivabradine.
4.2.5 The rate of implementation of a new drug approach (ARNI) for patients with HF and EF ≤35%
(see Figure 1);
4.2.6 The rate of patients with acute HF with a measure of EF and of creatinine performed during
the hospital stay and, if discharged alive, with a clinical visit planned and performed within 4 weeks
after discharge.
4.2.7 The rate of CHF patients with an available measure of EF and of creatinine from the visit.
4.2.7 Other analyses
The rate of adherence to other guideline recommendations will be evaluated:
‐ dosages of recommended treatments (ACE-I/ARBs, beta-blockers, MRAs, ivabradine);
‐ influenza vaccination;
‐ description of the modalities of diagnosis and management of the most relevant comorbidities
(COPD, diabetes, renal dysfunction, anemia, iron deficiency);
‐ inotropes in acute HF if SBP >90 mmHg;
‐ prescription of treatments that can cause harm in patients with HF: glitazones, dronedarone, class
I anti-arrhythmics, NSAIDS, COX2 inhibitors, Alpha receptor antagonists.
4.2.8 Mortality and morbidity outcomes
4.2.8.1 Mortality
Death from all-causes, for cardiovascular causes, for HF:
Acute HF: in-hospital, at 1 and 12 months from index admission date.
Chronic HF: at 12 months from index enrolment visit.
4.2.8.2 Morbidity
Hospital admissions from all-causes, for cardiovascular causes, for HF:
Acute HF: at 1, 6, 12 months from index admission date.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 13
Chronic HF: at 6, 12 months from index enrolment visit.
In each participating center:
4.2.9. Indicators of the organization of HF care
Presence of the following at center level, if formally recognized:
- integrated care pathways for HF within the hospital,
- integrated care pathways shared between hospital and community care,
- adequately staffed (physician-nurse personnel) outpatient clinic,
- feed-back available from the Administrative Office of the hospital on activity volumes (HF
admissions, HF outpatient visits), length of stay, in-hospital mortality in general and for HF
patients.
A questionnaire regarding these characteristics of the participating structures will be collected at the
beginning of phase 1 and 3 of the study.
At the National level:
4.2.10. Management of valvular abnormalities
To measure the rate of use of the diagnostic and therapeutic procedures implemented in patients with
valvular abnormalities associated with HF, such as aortic stenosis or functional mitral regurgitation.
5. INVESTIGATIONAL PLAN
5.1 Study Design
Multicentre cross-sectional and prospective national observational study to evaluate the impact of a
guideline implementation intervention.
No specific protocols for evaluation, management, and/or treatment besides guideline
recommendations will be put forth during the study. Standard management will be the diagnostic and
therapeutic interventions performed at each centre for patients presenting with signs and symptoms
of acute HF or chronic HF. Indications to perform diagnostic or therapeutic procedures will be left to
participating cardiologists’ decision.
5.2 Study Phases
Four study phases are foreseen.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 14
Phase 1. First cross-sectional data collection
Prospective cross-sectional survey. Educational web program during data collection in patients with
HF to improve the awareness regarding the contents and the implementation of current guidelines,
with particular attention to diagnostic issues, drug and device treatment (See Table). Data collection
will last for a period of 3 months (or for at least 50 patients) of all consecutive subjects with chronic
HF or admitted for acute HF at participating centers (see inclusion and exclusion criteria).
Phase 2. Educational intervention
Face-to-face educational sessions during investigators’ meeting held at macro-regional level with a
final test to document achievement of learning objectives (before the study starts and during the 5
months following the phase 1 completion). A specific focus on the results of phase 1 data collection
and the gaps/obstacles in applying guidelines in clinical practice will be also implemented.
Phase 3. Second cross-sectional data collection
A second educational web program during data collection will be conducted for a period of 3 months
(or for at least 50 patients) in all consecutive patients with chronic HF or admitted for acute HF at
participating centers (see inclusion and exclusion criteria); patients who have been enrolled in phase
1, either as acute or chronic HF, will not be eligible for enrolment in Phase 3. Phase 3 will be carried
out 6 months after the end of Phase 1 recruitment.
During phase 1 and 3 a specific decision support system module will be added to of the web-based
case report form. Pop-up reminders will appear during fill-in whenever recommended diagnostic-
therapeutic procedures applicable to the individual patient (see Table) are not reported as
implemented.
Phase 4. Longitudinal Follow-up
All patients (AHF and CHF) included in the study in Phase 1 and 3 will enter a longitudinal follow-
up with a clinical visit at 6 and 12 months.
Data collected at 12 months will include mortality and morbidity outcomes, and assessment of
applicable indicators to derive individual and composite adherence measures.
Benchmark reports will be available online describing changes over time (phase 3 vs phase 1) of the
guideline adherence in the same center, and comparisons across predefined subgroups of centers (by
region, by typology of hospitals etc).
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 15
5.3 Certification
A final certification of expertise in the management of patients with HF will be provided to the
participating centers, based on their performance in the conduction of this project.
Requirements for center certification (all of the following):
- Inclusion of at least 30 patients in both phase 1 and 3 with a complete (>95%) follow-up visits.
- Documented attendance at the face-to-face session of all health care professionals dealing with
this project in each participating center.
- Presence of a HF Outpatient Clinic.
Each center will be provided online with its own rate of adherence to the relevant recommended
treatments (see Table) in comparison with the centers of its geographical area (North, Center, South
of Italy) and the whole country.
5.4 Data Collection
Data will be collected using the web based system IN-HF on line Software (HCFSCOL), used in
Italian centers from 1995. Participating Centers will be divided in two categories:
Old (O) Centers already using IN-HF on line (e.g. IN-HF on line protocol has been already
approved by local IRB);
New (N) Centers not already using IN-HF on line.
For center of type O, only BLITZ-HF protocol will have to be approved by local IRB. For center of
type N, both BLITZ-HF and IN-HF on line protocol will have to be approved by local IRB.
For patients already enrolled in the IN-HF on line registry, time zero for the BLITZ HF study is the
date of the visit/hospital admission occurring for the first time during the BLITZ HF enrollment
period. For patients never enrolled in the IN-HF on line registry time zero is the date of the first
visit/hospital admission that will be recorded in the IN-HF online database.
6. STUDY VARIABLES
Data to be collected are reported in detail in the Case Report Form (eCRF, Annex 1).
6.1 Baseline data
In both phase 1 and 3 of the study, information on demographic characteristics, clinical features, past
history, laboratory examinations, diagnostic procedures, pharmacological and not-pharmacological
treatments will be collected.

BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 16
6.2 Follow-up data
Adverse events (fatal and non fatal) occurring during the follow-up period will be collected together
with information on the use of resources. Specifically information on survival status, causes of death,
need for hospitalization/re-hospitalization and related causes, pharmacological and not-
pharmacological treatments will be collected.
7. STATISTICAL CONSIDERATIONS
Considering the explorative and observational nature of the current study, no formal sample size
calculation has been performed. However, the current study is aiming at a sample of at least 5000
patients from 160 centers to allow for a representative national cohort.
Based on the study objectives, data analysis will be mainly descriptive and will assess the degree of
adhesion to guidelines recommendations. In addition, comparisons can be made between hospital
types and geographical distribution.
A sample of at least 30 patients per participating center and a total of 5000 patients has been estimated
as a minimum number to fulfill the level of quality to assess the adherence to guidelines in the setting
of the Italian participating centres dealing with the different presentations of HF. The inclusion in the
survey of such a number of patients should allow to have sufficient information on a few subgroups
of patients for whom a specific focus can be considered of interest (i.e. patients with preserved EF,
patients with the different clinical profiles at hospital admission, patients with COPD or diabetes).
Moreover, at the National level, this number of patients should allow to evaluate in a sufficient
number of patients with chronic HF and reduced EF the increase in the appropriate rate of use of
ACE-I/ARBs and beta-blockers and MRAs which are recommended in all patients with HF and
reduced EF, unless specific contraindications or intolerance are present. According to the most recent
Italian epidemiological data, about 40% of patients with HF and reduced EF are receiving all the 3
recommended treatments. If we assume that this quality improvement initiative can increase the rate
of patients prescribed in those treatments by 25% (from 40% to 50%), the number of patients needed
to demonstrate this assumption is 1000 with a power of 90% and a p value <0.05.
All patients enrolled will be included in the analysis.
Each center will be provided with descriptive summaries of their level of adherence to current
guidelines (6) both in the 1 and 3 phases of the study.
At the National level, descriptive summaries of level of adherence to guidelines will be presented for
all patients, and for the following specified subgroups of patients:
‐ Females versus males,
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 17
‐ elderly (>70 years versus ≤70 years),
‐ acute HF versus chronic HF,
‐ HFrEF (<40%) versus HFmrEF (40-49) versus HFpEF (≥50%),
‐ prevalence of AF and related treatment,
‐ implanted CRT-P – ICD – CRT-D patients versus indicated ones,
‐ valvular heart disease: aortic stenosis, mitral regurgitation,
‐ number of patients included in the study (above/below the median value).
8. SAFETY ASPECTS
In agreement with the current rules regarding pharmaco-vigilance (Good pharmacoVigilance
Practice, GVP), regarding non-interventional studies, the responsible of the study has the duty to
promptly communicate to the competent Authorities all adverse reactions occurring during this
observational study according with the rules of spontaneous reporting (post-marketing). In any case,
the sponsor of the study should be informed by the Investigator of those adverse reactions.
9. STUDY ORGANIZATION
9.1 Study sponsor
ANMCO - Heart Care Foundation.
9.2 Steering Committee
The Steering Committee acts as the Sponsor of the study, and has the full responsibility for planning,
conduct, analysis, and publication of study protocol and results.
9.3 Executive Committee
The Executive Committee will be responsible for the formulation of the study protocol and to oversee
its implementation.
9.4 Participating Centers
All cardiology centers managing HF patients will be invited to participate. The expectation is that
approximately 150 centers will participate at the project.
Representativeness with respect to the geographical distribution of centers and their clinical facilities
technological level will be assessed.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 18
9.5 Monitoring Procedures
The study will be monitored to ensure overall quality of data.
The Steering Committee of the study delegates the monitoring aspects to the monitoring group of the
Coordinating Centre (ANMCO Research Centre). All centers participating in the study will be
monitored according to monitoring procedures set out by HCF for observational studies.
A centralized Web monitoring of eCRF entries will be conducted with periodical emission of queries
to the participating centers.
On site monitoring could be conducted following a risk-based approach.
The investigator must maintain source documents for each patient in the study, including
documentation of HF, notes containing demographic and medical information, copies of laboratory
and clinical tests. The investigator must also keep the original informed consent form signed by the
patient. In the case of on-site monitoring visit, the investigator must give the monitor access to all
relevant source documents to confirm their consistency with (e)CRF entries.
9.6 Publication Policy
The study will be published anyhow, independently of the final results, on the behalf of the study
group. An appropriate Appendix will include the names of the members of the study committees, of
the coordinating center and of representatives from each individual study site. Manuscripts and
abstracts will be prepared through cooperation between the Steering Committee and the ANMCO
Research Centre.
Ancillary analyses can be proposed by the member of the Steering and Executive Committee and by
each Investigator. The Steering Committee has the commitment to evaluate these proposal, to approve
them if scientifically sound and prioritize the analysis of the database. The Steering Committee must
receive a copy of any presentation, manuscript, or abstract prior to any outside submission. A period
of 5 working days for presentational materials and abstracts and 15 working days for a journal
submission will be required for the Steering Committee review. Authorship of the ancillary analyses
will be determined according to the current medical community rules. The author must have (a)
contributed substantially to the conception and design of the study, the acquisition of data, or their
analysis and interpretation and (b) drafted or provided a critical revision of the article.
10. ETHICAL ISSUES
The survey is an observational study that does not dictate the manner in which patients are evaluated
or treated for HF. Physicians may decide to evaluate and manage-patients with HF in any way they
deem appropriate according to the local standard of care.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 19
The protocol will be submitted to local Ethical Committees according to current national regulations.
Each patient shall sign an informed consent to the study. Personal data will be encrypted to be
transferred anonymously to the central served and patients will be identified in the eCRF by numerical
codes. The main database will be secured according to current standards to ensure both ethical and
integrity requirements of the data. In order to maintain strict security, each investigator/study
personnel will have a unique login and password to enter patient’s information.
11. STUDY DURATION
Overall study duration will be 36 months:
M0-M6: preparation of protocol, CRF, regulatory procedures.
M7-M9: phase 1.
M9-M15: phase 2.
M16-M18: phase 3.
M30: end of follow-up of the last patient included in the study.
M31-M32: data cleaning, database locking.
M33-M34: statistical analysis.
M35-M36: preparation of the final report and diffusion of the results of the study.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 20
REFERENCES
1. Roger VL. Epidemiology of heart failure. Circ Res 2013;113:646-59.
2. Braunwald E. The war against heart failure: the Lancet lecture. Lancet 2015;385:812-24.
3. Nieminen MS, Brutsaert D, Dickstein K, et al; EuroHeart Survey Investigators; Heart Failure
Association, European Society of Cardiology. EuroHeart Failure Survey II (EHFS II): a survey
on hospitalized acute heart failure patients: description of population. Eur Heart J 2006;27:2725-
36.
4. Tavazzi L, Senni M, Metra M, et al; INHF (Italian Network on Heart Failure) Outcome
Investigators. Multicenter prospective observational study on acute and chronic heart failure: one-
year follow-up results of IN-HF (Italian Network on Heart Failure) outcome registry. Circ Heart
Fail 2013;6:473-81.
5. Maggioni AP, Anker SD, Dahlström U, et al; Heart Failure Association of the ESC. Are
hospitalized or ambulatory patients with heart failure treated in accordance with European Society
of Cardiology guidelines? Evidence from 12,440 patients of the ESC Heart Failure Long-Term
Registry. Eur J Heart Fail 2013;15:1173-84.
6. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey
JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B,
Riley JP, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Authors/Task Force Members;
Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic
heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of
the European Society of Cardiology (ESC) Developed with the special contribution of the Heart
Failure Association (HFA) of the ESC. Eur Heart J. 2016 May 20. pii: ehw128. [Epub ahead of
print]
7. Allen LA, Fonarow GC, Liang L, et al; American Heart Association’s Get With The Guidelines
Heart Failure (GWTG-HF) Investigators. Medication initiation burden required to comply with
heart failure guideline recommendations and hospital quality measures. Circulation
2015;132:1347-53.
8. Struttura ed Organizzazione Funzionale della Cardiologia. G Ital Cardiol 2009;10(Suppl 3-6):81S-
84S.
9. Fonarow GC, Yancy CW, Hernandez AF, et al. Potential impact of optimal implementation of
evidence-based heart failure therapies on mortality. Am Heart J 2011;161:1024-30.
10. Fonarow Gc, Petereson ED. Heart failure performance measures and outcome: real or illusory
gains. JAMA 2009;302:792-94.
BLITZ-HF Protocol - ver. 4.0 – August 1, 2016 21
11. Au AG, McAlister FA, Bakal JA, Ezekowitz J, Kaul P, van Walraven C. Predicting the risk of
unplanned readmission or death within 30 days of discharge after a heart failure hospitalization.
Am Heart J 2012;164:365-72.
12. Teixeira A, Parenica J, Park JJ, et al; GREAT (Global Research on Acute Conditions Team)
Network. Clinical presentation and outcome by age categories in acute heart failure: results from
an international observational cohort. Eur J Heart Fail 2015;17:1114-23.
13. Joint Task Force on the Management of Valvular Heart Disease of the European Society of
Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS), Vahanian A,
Alfieri O, Andreotti F et al. Guidelines on the management of valvular heart disease (version
2012). Eur Heart J 2012;33:2451-96.
14. Candreva A, Maisano F, Taramasso M. MitraClip and Transcatheter Aortic Valve Implantation
(TAVI): State of the Art 2015. Curr Heart Fail Rep 2015;12:379-88.





























