Embed Size (px)
Citation preview

DOCUMENT CONTROL:
Version: 7
Ratified by: Clinical Quality and Standards Group
Date ratified: 8 December 2015
Name of originator/author: Senior Clinical Nurse Specialist - Infection Prevention and Control
Name of responsible committee/individual:
Infection Prevention and Control Quality & Standards Committee
Date issued: 16 December 2015
Review date: December 2018
Target Audience All clinical staff
BLOOD AND BODY FLUID
SPILLAGES POLICY
Page 2 of 18
CONTENTS
SECTION PAGE NO
1. INTRODUCTION 4
2.
2.1
PURPOSE
DEFINITIONS/EXPLANATIONS OF TERMS USED
4
3. SCOPE 4
4. RESPONSIBILITIES, ACCOUNTABILITIES AND DUTIES 4
4.1 Board of Directors 4
4.2
4.3
Chief Executive
Director of Infection Prevention and Control (DIPC) (Director of Nursing and Quality)
5
5
4.4 Infection Prevention and Control Quality & Standards Committee (IPCQ&SC)
5
4.5 Infection Control Doctors/Consultant Microbiologists 6
4.6 Clinical Nurse Specialists Infection Prevention and Control Quality & Standards (CNSIPCQ&S)
6
4.7 Consultant Medical Staff/Medical Staff 6
4.8 Modern Matrons/Service Managers 6
4.9 Staff 6
5. PROCEDURE/IMPLEMENTATION 7
5.1 Management of Spillages 7
5.2 Small blood and visibly blood stained body fluid spillages 8
5.3 Large blood and visibly blood stained body fluid spillages 8
5.4 Use of Guest Medical or GV blood spillage kits 9
5.5 Blood and Body Fluid Spillages to Walls and Vertical Surfaces 9
5.6 Body fluid spillages inclusive of urine/vomit/excreta in the healthcare setting
9
5.7 Spillages of blood and blood stained body fluids on carpets and soft furnishings in the healthcare setting
10
5.8 Management of Blood and Body Fluid Spillages in the Patient’s Home 10
5.9 Spillages of body fluids on carpets and soft furnishings in the healthcare setting
11
5.10 Spillages of Blood and Body Fluids in Vehicles 12

Page 3 of 18
6. TRAINING IMPLICATIONS 12
7. MONITORING ARRANGEMENTS 12
8. EQUALITY IMPACT ASSESSMENT SCREENING 13
8.1
8.2
Privacy, Dignity and Respect
Mental Capacity Act
13
13
9. LINKS TO OTHER TRUST PROCEDURAL DOCUMENTS 13
10. REFERENCES 14
11. APPENDICES 14
Appendix 1 - High and Low Risk Body Fluids 15
Appendix 2 - Clinell Universal Wipes – Instructions for use 16
Appendix 3 - Clinell Spill Wipes; Instructions for use
Appendix 4 – Poster – Use of Biohazard spill kit for blood & blood stained body fluid spills
17
18

Page 4 of 18
1. INTRODUCTION Blood and body fluid spillages (Appendix 1) should be considered potentially infectious (Lawrence, 2003). Healthcare personnel dealing with spills of blood and body fluids may be exposed to blood borne viruses and other pathogens. For the management of spillages to be undertaken safely pathogens in the spillage must first be destroyed by a disinfectant (Wilson, 2006). Employers have a duty to protect healthcare personnel from hazards encountered during their work inclusive of microbiological hazards (COSHH 2002).
2. PURPOSE The purpose of this policy is to direct staff on the appropriate management of blood and body fluid spillages to reduce the risk of cross infection. This policy aims to provide guidance for staff to safely manage spillages in a variety of care settings including patient’s homes, healthcare environments and the transport of specimens’ service. The policy content is based on sound infection prevention and control principles and national guidance on the appropriate management of blood and body fluid spillages.
2.1 DEFINITIONS/EXPLANATIONS OF TERMS USED Blood borne viruses – includes such organisms as Hepatitis B, C or Human Immunodeficiency Virus (HIV) Pathogens – a microbe capable of causing infection and/or disease
3. SCOPE This policy applies to all staff providing care to all patients under the care of the Trust, whether in a direct or indirect patient care role regardless of the care environment. This policy should be read in conjunction with other infection prevention and control policies, particularly Hand Hygiene, Standard Infection Prevention and Control Precautions, Decontamination, Cleaning Systems and Processes for the Environment, Patient Equipment and Medical Devices, Pathology Specimens and Waste (Estates & Facilities policy).
4. RESPONSIBILITIES, ACCOUNTABILITIES AND DUTIES
All staff working on Trust premises, outreach clinics and community settings including Trust employed staff, contractors, agency and locum staff are responsible for adhering to this policy.
4.1
Board of Directors The Board of Directors are responsible for having policies and procedures in place to support best practice, effective management, service delivery, management of
Page 5 of 18
associated risks and meet national and local legislation and/or requirements.
4.2 Chief Executive The Chief Executive is responsible for establishing and maintaining infection prevention and control (IPC) arrangements across the organisation, but delegates the responsibilities to the Trust Board and the Director of Infection Prevention & Control. The Director with the lead responsibility is the Deputy Chief Executive and Lead Nurse.
4.3 Director of Infection Prevention and Control (DIPC) (Director of Nursing and Quality) The DIPC directly reports to the Chief Executive and the Board:
Any identified cases of infections/alert organisms and conditions, including outbreaks of infection
The organisations performance in relation to healthcare associated infections (HCAIs) providing regular reports including an annual report and IPC programme
Acts on legislation, national policies and guidance ensuring effective policies are in place and audited
Reports all incidents requiring post infection review
4.4 Infection Prevention and Control Quality & Standards Committee (IPCQ&SC) The main duties of the IPCQ&SC are:
To oversee compliance with national standards/targets in relation to the prevention and control of HCAIs including the Health and Social Care Act 2008, NHS Litigation Authority (NHSLA), and the Care Quality Commission (CQC).
To oversee key IPC issues in relation to:
o Policy development and review
o Audit
o Education & training
o Communication with staff patients and the public
o Monitoring of infection control incidents
o Review of post infection review reports , identify lessons learnt, develop and monitor action plans
o Agreeing the annual IPC report and work programme prior to its submission to Clinical Governance Group.
To inform the Clinical Governance Group of clinical risk issues relating to the Trust.
To monitor compliance for IPC training
To oversee the Trust’s compliance with the CQC Fundamental Standards

Page 6 of 18
4.5 Infection Control Doctors/Consultant Microbiologists These are medical microbiologists hosted within the local provider acute Trusts whose main duties are to:
Be available for 24 hour access, arrangements made through service agreements
Provide expert microbiology advice
Support and provide education to all grades and all disciplines as appropriate
4.6 Clinical Nurse Specialists Infection Prevention & Control Quality & Standards Team (CNSIPCQ&ST) The CNSIPCQ&ST:
Provide expert professional advice and education on the prevention and control of infection to other professionals, multi-disciplinary groups, patients and carers
Report findings to the DIPC
Give advice on complex issues relating to the management of multi-resistant organisms and control measures, delegating responsibility to Trust staff as appropriate
4.7 Consultant Medical Staff/Medical Staff Consultant medical staff are responsible for the supervision of junior staff and must:
Ensure compliance with IPC policies
Liaise with the Consultant Microbiologist for advice in relation to IPC issues
4.8 Modern Matrons/Service Managers All Service Managers and Modern Matrons are responsible for:
Membership at the IPCQ&S Committee.
On-going compliance with this policy within their clinical areas and reporting non-compliance to the DIPC
Reporting all matters relating to IPC to the Deputy Director of Nursing
Facilitating feedback of information related to surveillance data and identified cases of infection/alert organisms & conditions
Ensuring that situation reports are completed to deadline as requested
4.9 Staff All staff must comply with this policy and related guidance. Only staff who are fully vaccinated against Hepatitis B and who are competent to do so should deal with blood and/or body fluid spillages. It is the responsibility of all staff to ensure that their immunisation status for Hepatitis B is up to date. This can be obtained by contacting Occupational Health services. For spillages, whether caused by patients, staff or visitors, the responsibility

Page 7 of 18
is as follows:
Wards and departments – nursing or departmental staff
Main entrance, main corridors, communal areas outside ward and departments – domestic services
Outdoor areas, waste trolleys, vans – relevant department e.g Estates, Logistics staff
5. PROCEDURE / IMPLEMENTATION
5.1
Management of Spillages For effective management of spillages in the healthcare setting, surfaces such as walls, floors and upholstery should be smooth, wipeable, and impervious to moisture. Recommended products for the safe management of blood and body fluid spillages include quaternary ammonium compounds, peracetic acid and hydrogen peroxide, and chlorine releasing agents such as sodium dichloroisocyanurate (NaDCC) and sodium hypochlorite. The products used within the Trust are:
Clinell Universal wipes (for spillages no greater than the size of a 2p coin)
Clinell Spill Wipes (for spillages greater than the size of a 2p coin)
Guest Medical or GV blood spillage kit
Haz Tabs (for vertical surfaces)
Hospec detergent
Infectious agents can survive for long periods in spillages and the person witnessing the event should deal with the spillage immediately if competent to do so. If the spillage cannot be dealt with immediately the area must be cordoned off and not left unattended whilst assistance is obtained. Chlorine-releasing agents are a chemical disinfectant which are effective against blood borne viruses and act rapidly. In order to be effective they must be used in accordance with manufacturer’s instructions and at the appropriate strength. All solutions made from tablets should be prepared only as and when needed. COSHH assessments must be carried out on all chemical disinfectants used. Staff must be aware of the implications of these products for storage, usage and first aid in the event of exposure e.g. splashing to the eye. Chlorine releasing agents can damage the skin and mucous membranes, therefore appropriate personal protective equipment (PPE) should be worn for contact with these chemicals i.e. gloves, aprons, face and eye protection.
Staff must always cover cuts and lesions with a waterproof dressing whilst on duty. Chlorine releasing agents are corrosive to many materials including metals and will bleach/damage soft furnishings, fabrics and carpets.

Page 8 of 18
When using/preparing chlorine releasing agents the area must be well ventilated. Never use hot water to dilute the chemicals. Cold water must be used. CHLORINE CONCENTRATIONS:
Strength Usage
10,000 parts per million (ppm)
To render blood and blood stained body fluid spillages safe to deal with (before cleaning)
1,000 parts per million (ppm)
Decontamination of surfaces contaminated with body fluids e.g. commodes (after cleaning)
Spillage Kits Biohazard spillage kits are available in many clinical settings including clinics and wards. These are kits that have the required equipment ready in a pack. Equipment in the kit generally contains:
Gloves and apron
Paper towels
Waste bag
Chlorine releasing granules/tablets and measured container
Scoop
Instructions for use are depicted on the outer packaging. Staff are responsible for ensuring that the equipment in the spill kit is replenished and in date. Kits must be stored in a locked cupboard in accordance with COSHH regulations.
5.2 Small blood and visibly blood stained body fluid spillages (surface area smaller than a 2p coin)
Ensure all cuts and lesions are covered with a waterproof dressing
Put on personal protective equipment (PPE) e.g. disposable gloves and apron
If there is a risk of splash wear eye/face protection
Remove blood spillage using a Clinell Universal wipe (Appendix 2)
Dispose of wipe into appropriate waste stream followed by PPE
Decontaminate hands using soap and water/hand wipes or hand rub
5.3 Large blood and visibly blood stained body fluid spillages (surface area larger than a 2p coin)
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE

Page 9 of 18
If there is a risk of splash wear eye/face protection
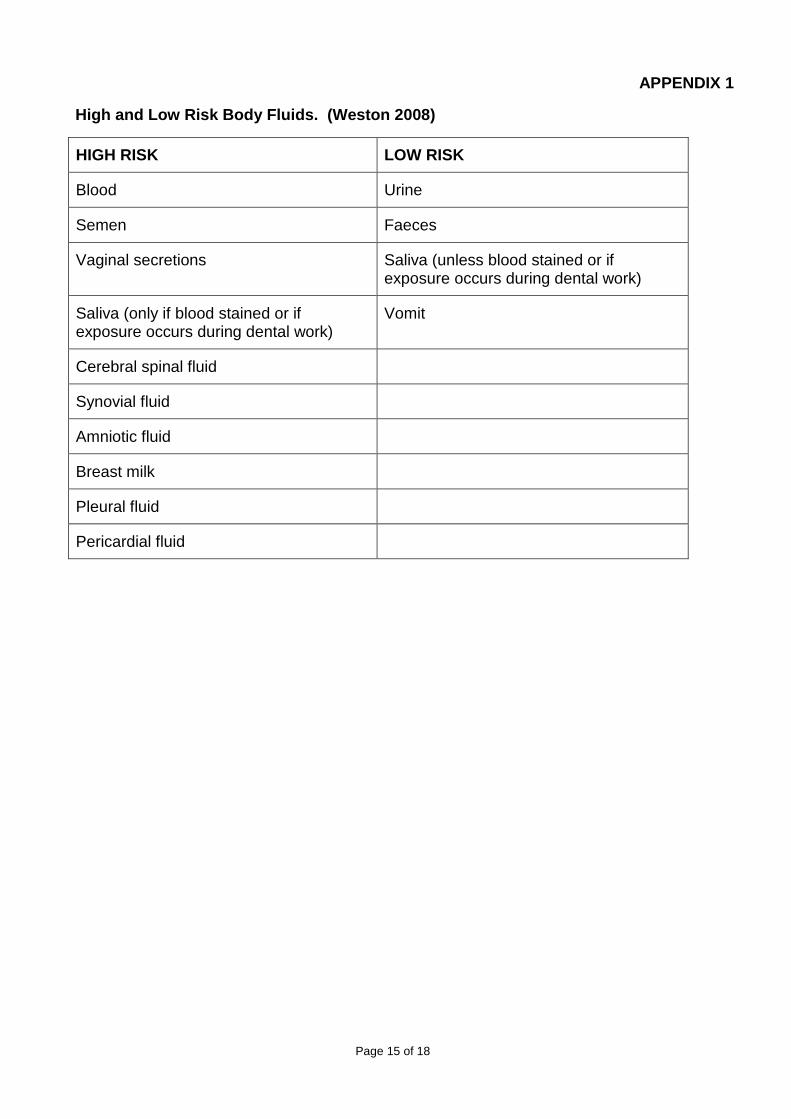
Absorb spill using Clinell Spill Wipe(s). Follow manufacturer’s instructions as illustrated on packet (Appendix 3)
Clean area with Clinell Universal wipes
Dispose of Spill Wipe and Universal wipes in to appropriate waste stream followed by PPE
Decontaminate hands using soap and water/hand wipes or hand rub
5.4 Alternatively use a Guest Medical or GV blood spillage kit:
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection
Follow manufacturer’s instructions for use as illustrated on packet (Appendix 4)
Dispose of waste including PPE in to appropriate waste stream
Decontaminate hands with soap and water/ hand wipes or hand rub
Replace spill kit
These kits must never be mixed with acids or used on spillages of urine or vomit, as a chlorine vapour will be released. Refer to sections 5.6 and 5.7 for managing urine and vomit spillages.
5.5 Blood and Body Fluid Spillages to Walls and Vertical Surfaces
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection
For small splashes use Clinell Universal wipe(s)
For large splashes prepare Haz Tab solution (10,000 parts per million) as directed by manufacturer’s instructions
Use the solution on disposable paper towels to remove the spill
Clean area, once spillage removed, with Clinell Universal wipe(s)
Discard remaining chlorine solution by flushing down the sink or sluice hopper
Dispose of paper towels, wipes and PPE into appropriate waste stream
Decontaminate hands with soap and water/ hand wipes followed by hand rub
For blood and body fluid spillages on equipment manufacturers’ instructions must be followed.
5.6 Body fluid spillages inclusive of urine/vomit/excreta in the healthcare setting (no visible blood)
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE

Page 10 of 18
If there is a risk of splash wear eye/face protection
Absorb spill using Clinell Spill Wipes. Follow manufacturer’s instructions as illustrated on packet
Dispose of Spill Wipe in to appropriate waste stream followed by PPE
Decontaminate hands with soap and water/ hand wipes followed by hand rub
Alternatively cover spillage with paper towels to absorb spill
Discard paper towels directly into appropriate waste stream
Clean area with Clinell Universal wipes or use hot water and neutral detergent using a disposable cloth or mop. Use colour appropriate equipment according to where the spill is located. Rinse and dry area
Dispose of cloth/mop head into appropriate waste stream. If reusable mop heads are used they must be sent to the laundry in a red alginate bag
Clean bucket with hot water and neutral detergent, rinse and dry
Discard PPE into appropriate waste stream
Decontaminate hands with soap and water/ hand wipes followed by hand rub
5.7 Spillages of blood and blood stained body fluids on carpets and soft furnishings in
the healthcare setting
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection
Absorb spill using Clinell Spill wipe(s)
Dispose of wipe(s) in to appropriate waste stream followed by PPE
Decontaminate hands with soap and water/ hand wipes followed by hand rub
Carpets and soft furnishings should be cleaned at the earliest opportunity using a carpet cleaner and/or steam cleaned
Haz Tabs should not be used except where chlorine resistant fabrics are specified. Soft furnishings such as cushions/covers, curtains etc must be laundered according to Laundry policy.
5.8 Spillages of body fluids (no visible blood) on carpets and soft furnishings in the healthcare setting
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection

Page 11 of 18
Absorb spill using Clinell Spill Wipes. Follow manufacturer’s instructions as illustrated on packet
Dispose of Spill Wipe in to appropriate waste stream followed by PPE
Decontaminate hands with soap and water/ hand wipes followed by hand rub
Alternatively cover spillage with paper towels to absorb spill
Discard paper towels directly into appropriate waste stream
Decontaminate hands with soap and water/ hand wipes followed by hand rub
Carpets and soft furnishings should be cleaned at the earliest opportunity using a carpet cleaner and/or steam cleaned
Soft furnishings such as cushions/covers, curtains etc must be laundered according to Laundry policy.
5.9 Management of Blood and Body Fluid Spillages in the Patient’s Home
For hard surfaces e.g. vinyl flooring, follow guidance in sections 5.2 and 5.3
If Clinell Universal wipes and Spill wipes are not available use a good quality bleach e.g. Domestos, diluted to 1 part bleach to 10 parts cold water
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection
Cover area with kitchen roll and gently pour on diluted solution
Leave for 2 minutes
Discard kitchen roll into plastic bag or bin liner
Wipe area with diluted solution and discard as above
Clean area with hot water and neutral detergent using a disposable cloth. Rinse and dry the area
Clean bucket/container with hot water and neutral detergent, rinse and dry
Discard PPE and cloth into plastic bag or bin liner and tie securely
Discard plastic bag or bin liner into domestic waste stream with patients permission
Decontaminate hands with liquid soap and water/ hand wipes and dry on kitchen roll followed by hand rub
For carpets and soft furnishings
Ensure all cuts and lesions are covered with a waterproof dressing
Put on PPE
If there is a risk of splash wear eye/face protection

Page 12 of 18
Absorb spill using Clinell Spill wipe(s) if available. Follow manufacturer’s instructions as illustrated on packet
Clean the area with Clinell Universal wipe(s)
Discard PPE and wipes into plastic bag or bin liner and tie securely
Discard plastic bag or bin liner into domestic waste stream with patients permission
Decontaminate hands with liquid soap and water/ hand wipes followed by hand rub
5.10 Spillages of Blood and Body Fluids in Vehicles
All vehicles transporting specimens must carry a spillage kit or Clinell Spill Wipes and Clinell Universal wipes. Drivers must be trained in the management of blood and body fluid spillages as outlined within this policy. Drivers are responsible for ensuring that the equipment in the spill kit is replenished and in date.
6. TRAINING IMPLICATIONS There are no specific training needs in relation to this policy, but all staff will need to be aware of its contents. Staff will be made aware through:
Line Manager
Team Brief
Team meetings
One to one meetings/supervision
Trust policy web site
7. MONITORING ARRANGEMENTS
Area for Monitoring
How
Who by
Reported to
Frequency
Non-compliance to policy
Via IR1 reports
Managers/ Matrons & IPC Team
Infection Prevention and Control Quality & Standards Committee (IPCQ&SC)
Bi monthly
Staff knowledge of procedure
IPC audit IPCQ&S team (IPCQ&SC) Annually

Page 13 of 18
8. EQUALITY IMPACT ASSESSMENT SCREENING
The completed Equality Impact Assessment for this Policy has been published on the Equality and Diversity webpage of the RDaSH website click here
8.1 Privacy, Dignity and Respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, ‘not just clinically but in terms of dignity and respect’. As a consequence the Trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
Indicate how this will be met
No issues have been identified in relation to this policy.
8.2 Mental Capacity Act
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals capacity to participate in the decision making process. Consequently, no intervention should be carried out without either the individuals informed consent, or the powers included in a legal framework, or by order of the Court
Therefore, the Trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act. For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act 2005 to ensure that the interests of an individual whose capacity is in question can continue to make as many decisions for themselves as possible.
Indicate How This Will Be Achieved.
All individuals involved in the implementation of this policy should do so in accordance with the Guiding Principles of the Mental Capacity Act 2005. (Section 1)
9. LINKS TO OTHER TRUST PROCEDURAL DOCUMENTS
Hand Hygiene Policy
Standard Infection Prevention and Control Precautions Policy
Use and Disposal of Sharps and Management of Contamination Injuries
Cleaning Systems and Processes for the Environment, Patient Equipment and Medical Devices
Decontamination Policy
Pathology Specimens Policy
Waste (Estates & Facilities policy).

Page 14 of 18
10. REFERENCES
1. Lawrence, J (2003) Infection Control in the Community, Churchill Livingstone, London.
2. Wilson, J (2006) Infection Control in Clinical Practice 3rd Edition, Bailliere Tindall, London.
3. Department of Health (1974) Health and Safety at Work Act, HMSO, London.
4. COSHH (2002) Control of Substances Hazardous to Health Regulations.
5. Department of Health (2006). The Health Act: a code of practice for the reduction of healthcare associated infections. London. Crown Copyright.
6. Department of Health (2015). The Health & Social Care Act 2008: Code of Practice on the prevention and control of infections and related guidance.
7. UK Health Departments (1998). Guidance for Clinical Health Care Workers: Protection against infection with blood borne viruses. Recommendations of the Expert Advisory Group on Hepatitis.www.dh.gov.uk/assetRoot/04/01/17/12/04011712.pdf.
8. Department of Health (2002) Keep Safe; Practical, everyday advice for HIV-infected people and their carers. www. Advisorybodies.dh.gov.uk/eaga/keepsafe1.htm
9. National Institute for Health and Clinical Excellence (2012) Prevention and control of healthcare associated infections in primary and community care. NICE clinical guideline 139
10. Ayliffe GAJ, Coates D and Hoffman PN (1993) Chemical Disinfection in Hospitals. Second edition. PHLS. London.
11. Weston, D (2008) Infection Prevention and Control. Theory and Practice for Healthcare Professionals. Wiley and Sons, England
11. APPENDICES
APPENDIX 1 - High and Low Risk Body Fluids. (Weston 2008)
APPENDIX 2 – Clinell Spill Wipes – Instructions for use
APPENDIX 3 - Clinell Universal wipes; Instructions for use
APPENDIX 4 – Use of Bio Hazard Spill Kit
Page 15 of 18
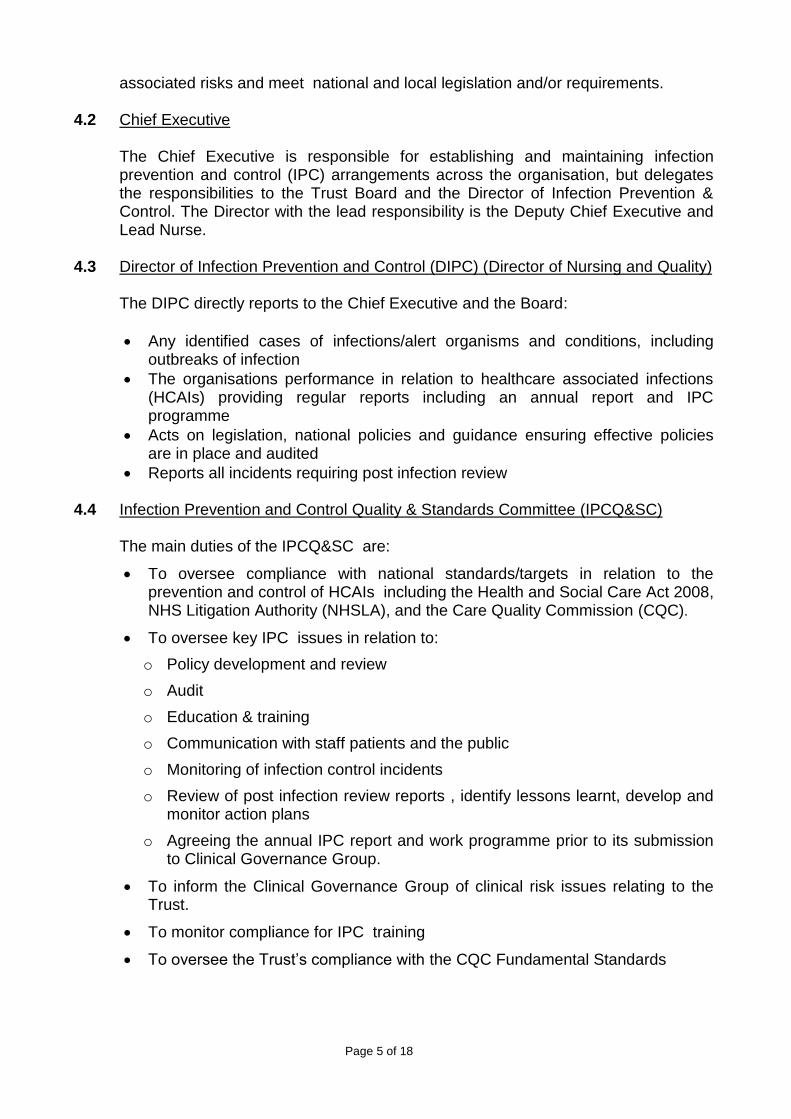
APPENDIX 1
High and Low Risk Body Fluids. (Weston 2008)
HIGH RISK LOW RISK
Blood Urine
Semen Faeces
Vaginal secretions Saliva (unless blood stained or if exposure occurs during dental work)
Saliva (only if blood stained or if exposure occurs during dental work)
Vomit
Cerebral spinal fluid
Synovial fluid
Amniotic fluid
Breast milk
Pleural fluid
Pericardial fluid

Page 16 of 18
APPENDIX 2
Clinell Universal wipes - Instructions for use
Page 17 of 18
APPENDIX 3
Clinell Spill Wipes – Instructions for use

Page 18 of 18
APPENDIX 4





























