Embed Size (px)
Citation preview
BLOOD TRANSFUSION
POLICY
Version 6.2.3
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
1
Policy Title:
Blood Transfusion Policy
Executive Summary:
To ensure safe, effective, timely and appropriate transfusion of blood components and blood products. This policy identifies individual roles and ensures the process is focused on patient safety.
Supersedes: Blood Transfusion Policy version 6.2.2
Description of Amendment(s):
Policy version number
Partial Review November 2007 for full review March 2008 Reviewed April 2008 Reviewed August 2011
Version 6.0
Reviewed January 2016 as Bloodhound included for fridge lockdown.
Version 6.1
July 2016 Included single nurse check
Version 6.2 - New request form added to policy and as appendix 7. - Information added to PCC, appendix 3. - Jehovah’s witness care plan added to appendix 4 for reference.
Version 6.2.2 -Procedure 3 point 3.10 wording amended. -New flowchart added for PCC – appendix 3 page 20
Version 6.2.3 New Massive Haemorrhage protocol added with telephone prompt card. December 2017
This policy will impact on: All clinical staff to ensure the safety of all inpatients in the Trust.
RELATES TO: PATIENT IDENTIFICATION POLICY (July 2007) INFECTION CONTROL POLICY (2007)
Policy Area: Clinical Practice Document Reference:
ECT002719
Version Number: V6.2.3 Effective Date: December 2017
Issued By: Medical Director Review Date: December 2018
Author: Transfusion Practitioner
Impact Assessment:
March 2018
APPROVAL RECORD
Committees / Group Date
Consultation: Hospital Transfusion Team
Hospital Transfusion Committee
4th December 2017
9th October 2017
Approved by Committees: Hospital Transfusion Committee
Medicines Management Group
Hospital Transfusion Committee
25th April 2016
13th Dec 2016
9th October 2017

Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
2
Received for information: Safety, Quality and Standards
Committee
July 2017
Approved by Director: Medical Director September 2011
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
3
CONTENTS PAGE PAGE INDEX
4 1.0 Policy Statement 4 2.0 Scope 4 3.0 Organisational Responsibilities 6 4.0 Planning and Implementation 7 5.0 Training 7 6.0 Monitoring Performance 8 7.0 Audit 8 8.0 Review 8 9.0 Bloodhound electronic tracking 9-12 Procedure 1: Identification of the patient, collection of the blood sample, completion of the request form and requesting blood components/blood products. 13 Procedure 2: Release, storage and collection of blood components 15 Procedure 3: Administration of Blood Components
17 References 18 Appendix 1 Massive Haemorrhage Protocol 20 Appendix 2 Investigation of an apparent transfusion reaction 21-26 Appendix 3 PCC – Warfarin Reversal 27-34 Appendix 4 Emergency protocol for treating Jehovah’s Witnesses 35 Appendix 5 Supplying blood to alternative hospitals 36 Appendix 6 Safety Sample 37 Appendix 7 Completion of the transfusion request form 38 Equality and Human Rights Policy Screening Tool
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
4
1.0 POLICY STATEMENT East Cheshire NHS Trust is committed to patient safety and as such will ensure that it has robust policies and procedures in place to reduce the likelihood of transfusion related incidents. It is essential to ensure safe, effective, timely and appropriate transfusion of blood components ie. Right Blood, Right Patient, Right Time. Errors in the requesting, supply, and administration of blood components leads to significant risks to patients and are completely avoidable. Failure to comply with the policy may result in disciplinary action.
2.0 SCOPE This policy applies to all staff involved in blood transfusion practice in all patient areas, including all wards, clinics, in-patients, out-patients, and critical care areas. The stages of the transfusion procedure can be divided up into:
Identification of the patient, collection of the blood sample and completion of the request form (procedure 1).
Pre-transfusion compatibility procedures which are the responsibility of the Blood Transfusion Department and are covered by their own internal protocols.
Release, storage and collection of blood components (procedure 2).
Administration of blood components and blood products into the correct patient (procedure 3).
Bloodhound electronic tracking is used within the trust and is mentioned within this policy. The bloodhound user guide is a separate document available on the East Cheshire Trust intranet. 3.0 ORGANISATIONAL RESPONSIBILITIES
Chief Executive Has overall responsibility for the policies and procedures in use in the Trust.
Medical Director Is responsible for the reporting to the Trust Board any risk issues or serious incidents relating to the blood transfusion process in the Trust.
Designated representative This term includes all suitably trained staff.
The above staff grades who participate in the Transfusion Procedure are responsible for following this policy to manage the risks associated with the blood transfusion procedure. They are responsible for attending training as set out in this policy to ensure patient safety.
Matrons/Departmental Managers Are responsible for ensuring that this policy and procedure is implemented within their area and that all staff attend training as appropriate
Blood Transfusion Practitioner Responsible for training all staff for example: clinicians, nurses, healthcare assistants and porters (but excluding staff in the transfusion laboratory) in the transfusion policy and procedures. Reports to the trust’s Hospital Transfusion Committee (HTC) on:
Training and competency of personnel in Blood Transfusion procedure
Audits carried out (national and local)
Proposes changes to practice accordingly
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
5
Reports on risks identified through the incident reporting process and lessons to be learned and changes implemented
Blood Bank Manager Responsible for all the technical issues which support the transfusion procedure. This includes:
The implementation of Blood Safety and Quality Regulations, equipment monitoring, maintaining blood component and blood product storage, laboratory staffing levels and staff training.
Initiating reports to SABRE of any Serious Adverse Event (SAE) or Serious Adverse Reactions (SAR) and any other event or near miss to SHOT.
Representing the HTC on the Regional (North West and North Wales) Transfusion Committee.
Laboratory Staff Perform the technical aspects of pre-transfusion compatibility testing. All staff working in the blood transfusion laboratory are fully trained, HCPC (Health and Care Professions Council) registered and competency assessed in the procedure. State Registered Biomedical Scientists (BMS) and supervised trainees are responsible for:
Ordering and correct storage of blood components and products
Correct identification of samples against request form
Checking patients’ historical data for special blood component requirements
Accurate and timely testing of samples
Ensuring suitability of issued components
Ensuring integrity of the blood components and products
Providing correctly labelled blood components which correlate with the details on the sample that was used for the testing purposes
Maintaining records of blood component and product usage to facilitate audit trails, patient transfusion records and provide statistical information
Investigation and reporting of transfusion incidents Receipt of samples and arrangement of appropriate laboratory tests
Issuing blood components and products
Managing blood stocks to minimise wastage
Offering advice and support to clinical staff
Identifying patient information correctly
Accurate documentation
All procedures will be in compliance with approved laboratory Standard Operating Procedures (SOPs)
Medical Laboratory Assistants (MLA) are responsible for:
Receipt and identification of samples in accordance with SOPs Data entry and/or filing of patient and blood component and product information. Porters
Are responsible for moving blood components and blood products in an appropriate and timely fashion to the remote issue blood bank refrigerators outside the main and orthopaedic theatre areas, and to other appropriate clinical areas within the Macclesfield District General Hospital site as directed by laboratory staff.
Hospital Transfusion Committee Has a responsibility to ensure a safe transfusion procedure by:
Monitoring performance in Clinical transfusion practice throughout the Trust
Monitoring the performance of the hospital transfusion service throughout the Trust
Monitoring the performance of the hospital transfusion service as a provider
Promoting education & readily available information on blood components & blood product transfusions
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
6
This will involve:
The timely review of all appropriate transfusion documentation and polices
Adopting best practice according to Regional and National guidance
Making recommendations on the appropriate use of blood components and blood products
Instigate training and education of staff and patients in the transfusion procedure Ensuring participation in audit
Ensuring an up to date Risk Register relating to all aspects of Blood Transfusion practice is maintained
Reporting the above to the committee for Safety, Quality and Standard Committee East Cheshire NHS Trust, the North West Regional Transfusion Committee (NWRTC); the Hospital Liaison Team National Blood Transfusion Service and the NHS Blood and Transplant (NHSBT) according to the HTC Terms of Reference.
Hospital Transfusion Team (HTT) This team is the operational arm of the Hospital Transfusion Committee and its main function is to:
Assists the HTC in the implementation of the HTC’s objectives
Promotes and provides advice and support to clinical teams on the appropriate and safe use of blood components and blood products
Actively promotes the implementation of good transfusion practice
Be a source of training for all hospital staff involved in the procedures of blood transfusion This will involve:
Interpreting National guidelines and assisting in the process of their implementation
Reviewing all adverse events relating to transfusion procedures
Establishing and maintaining an up to date Risk Register relating to all aspects of Blood Transfusion practice
Reporting the above to the Hospital Transfusion Committee on a quarterly basis 4.0 Planning and Implementation
4.1 The Blood Transfusion Policy will comply with:
NBTC Requirements for training and Assessment 2016 NICE Guidelines 24 Blood Transfusion 2015 Guidelines on the Administration of Blood Components 2009 Blood Safety and Quality Regulations 2005 (SI 2005 No.50) Handbook of Transfusion Medicine - United Kingdom Blood Services, 5th Edition. McClelland, DBL. London, the Stationery Office Better Blood Transfusion 3 (HSC 2007/001)
4.2 Blood samples for pre-transfusion compatibility testing may only be taken by a Medical
Officer or a Designated Representative that has been trained in this task. 4.3 Any clinician involved in the blood transfusion procedure must ensure they follow the
trust policy for correct identification of the patient 4.4 The Blood Transfusion Policy must be followed for each procedure 4.5 Any member of staff involved in the blood transfusion procedure must have received initial training in the process with statutory annual updates (SI 2005
No.50) and further competency based refresher training every 2 years NBTC Requirements for training and Assessment 2016
4.6 All clinical staff that care for patients in areas that provide blood transfusions or blood
products must be appropriately trained, competent and familiar with the trust blood transfusion procedures.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
7
4.7 Clinical staff must report any incident relating to the blood transfusion policy and procedure, or any incident from the administration of blood components and/or blood products to a patient on the Datix reporting system.
4.8 Full guidance that must be followed can be found in procedures 1, 2 and 3
4.9 In all clinical areas where any stage of the transfusion procedure takes place, patient
information leaflets on transfusion must be made available. 5.0 TRAINING
Statutory and Mandatory training – Annually all medical staff, ODP’s, midwives and nursing staff receive training on blood administration through annual updates on clinical statutory and mandatory training day.
Bloodhound training is in two forms: phlebotomy training and blood administration. All staff attending bloodhound training will have a practical assessment. 5.1 Phlebotomy training is provided to anyone who is taking blood samples via
venepuncture. 5.2 Training in transfusion administration is required for all staff involved in
the transfusion process including collection, checking and administration of a transfusion.
Porters: Receive initial training and competency assessment which is reassessed
every 2 years, or earlier if any circumstance dictate that further training and assessment is required.
Nursing staff/ODP/Midwives:
All must complete a transfusion administration competency. The competency follows the guidance set out in the NBTC Requirements for training and Assessment 2016.
Records will be completed for all training sessions and held by the Transfusion Practitioner.
Training is facilitated by the Transfusion Practitioner and designated senior nursing staff who have undertaken training to become blood transfusion link staff.
6.0 Monitoring Performance
6.1Key performance indicators (KPIs) identified relating to this policy are as follows:
An annual audit of compliance with this policy will be carried out by the Transfusion Practitioner following the National Blood Service National Comparative Audit In ‘Blood Transfusion Bed Side Practice’. This audit will include: o The process for the administration of blood components and products o The care of patients during transfusion o Training records of annual and competency based assessments in line with
national guidance, this policy and the NPSA alert ‘right patient, right blood’.
6.2 These KPIs will be reviewed during the policy review exercise to check that the Trust is performing and improving
6.3 Bloodhound generates alerts for any issues with blood administration. These will be
investigated by the transfusion practitioner and reported to the HTC or externally to SHOT (Serious Hazards of Transfusion) if indicated.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
8
7.0 Audit This policy will be audited in line with the KPI’s identified in section 6 on an annual basis by the Transfusion Practitioner and reported to the Hospital Transfusion Committee. Any action plans developed from this audit will be agreed by the Hospital Transfusion Committee with a quarterly review of progress. The transfusion practitioner will facilitate the involvement with any national or regional audits in force during each year and report the findings and any subsequent action plans back to The Hospital Transfusion Committee. 8.0 Review
This policy will be reviewed by the Hospital Transfusion Committee on a three yearly basis or earlier if required. 9.0 Bloodhound Bloodhound is an electronic system used in the transfusion process that enhances safety within transfusion. The process follows all national transfusion guidelines. Bloodhound is used for:
Phlebotomy
Lab issue of blood components
Tracking and scanning of each blood component through a kiosk on the blood bank fridge, or handheld machine on the ward area.
Ward receipt – to identify the ward where transfusion is taking place.
To record the transfusion start and end times and provide traceability of the use of blood components.
For individual procedures please read the separate Bloodhound user guide which is separate to this policy.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
9
PROCEDURE 1: All patients requiring transfusion must have a blood sample taken for pre-transfusion compatibility testing which can only be taken by a Medical Officer or a Designated Representative who has been trained in this task by the transfusion practitioner. The following procedure must be followed in all cases: 1 PATIENT IDENTIFICATION Positive identification of the patient is essential and the National policy for correct Patient Identification (HSC 2007/001) must be followed. The practitioner should: a) Question the patient to confirm their full name and date of birth. If they are not able or willing
then refer to ‘Patient Identification Policy and Procedures’ via the trust intranet.
b) Ensure the patient has a valid printed wristband attached to them with the correct patient details.
2 PROCEDURE FOR THE COLLECTION OF THE BLOOD SAMPLE 2.1 Informed Consent The patient must be informed of the indication for blood transfusion; the risks (especially nvCJD), alternatives and benefits of the transfusion and should be given an information leaflet and given the opportunity to ask any questions. Transfusion leaflets can be obtained via the transfusion practitioner. It must be written in the medical notes that the patient has had this information. This may be done by the prescribing doctor or nurse / midwife caring for the patient. The patient has the right to refuse a transfusion and this must be documented appropriately. 2.2 Venepuncture Using the bloodhound system and relevant checks, provides a safer process for taking phlebotomy samples and labelling appropriately. For training contact the transfusion practitioner bleep 5164. Take the sample from one patient at a time. Do not take the sample from an arm with an ongoing intravenous infusion. 2.3 Sample Type For patients requiring a transfusion that have no historic blood group available on our database, a second ‘safety’ sample must be obtained to verify their blood group prior to the issue of blood components. This sample provides an important safety check.
6 ml pink topped EDTA sample is required for blood group and antibody screen and/or crossmatch. If the patient is difficult to bleed and 6 ml is not obtainable contact the laboratory when sending the sample. For paediatric patients use the lavender topped EDTA sample bottles.
PROCEDURE 1:
Identification of the patient, collection of the blood sample and completion of the request form.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
10
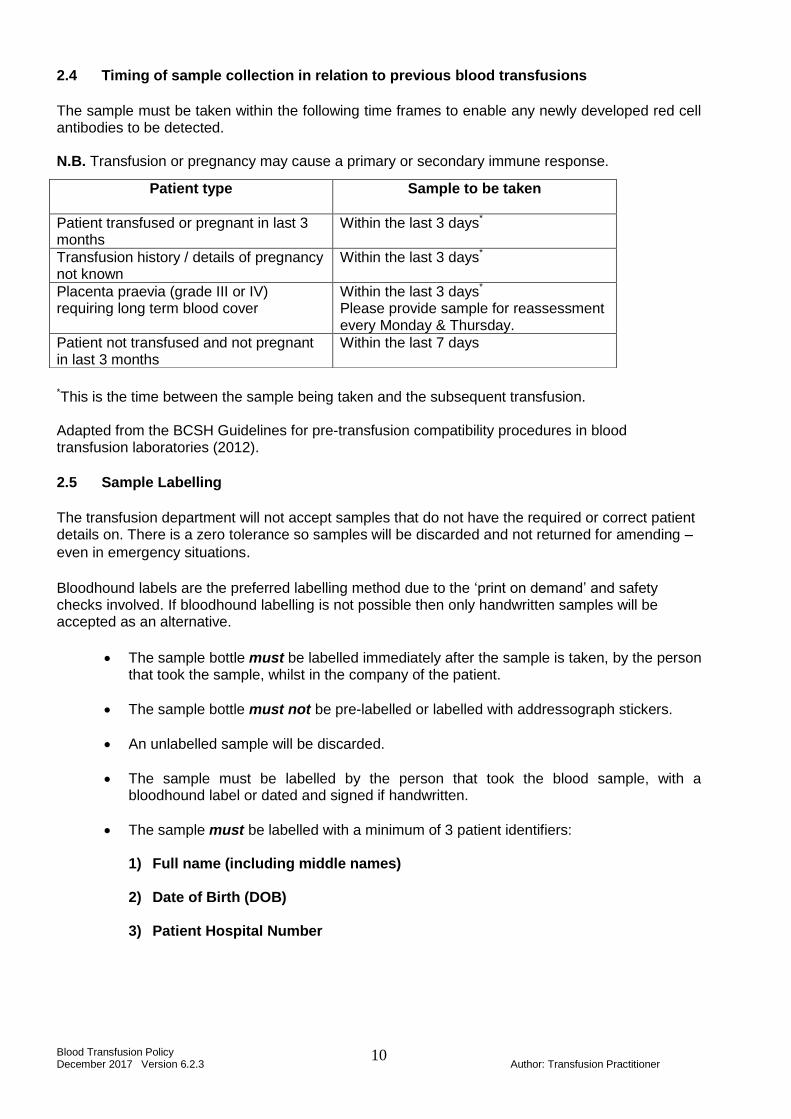
2.4 Timing of sample collection in relation to previous blood transfusions
The sample must be taken within the following time frames to enable any newly developed red cell antibodies to be detected. N.B. Transfusion or pregnancy may cause a primary or secondary immune response.
*This is the time between the sample being taken and the subsequent transfusion. Adapted from the BCSH Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories (2012).
2.5 Sample Labelling
The transfusion department will not accept samples that do not have the required or correct patient details on. There is a zero tolerance so samples will be discarded and not returned for amending –
even in emergency situations. Bloodhound labels are the preferred labelling method due to the ‘print on demand’ and safety checks involved. If bloodhound labelling is not possible then only handwritten samples will be accepted as an alternative.
The sample bottle must be labelled immediately after the sample is taken, by the person that took the sample, whilst in the company of the patient.
The sample bottle must not be pre-labelled or labelled with addressograph stickers.
An unlabelled sample will be discarded.
The sample must be labelled by the person that took the blood sample, with a bloodhound label or dated and signed if handwritten.
The sample must be labelled with a minimum of 3 patient identifiers: 1) Full name (including middle names)
2) Date of Birth (DOB)
3) Patient Hospital Number
Patient type
Sample to be taken
Patient transfused or pregnant in last 3 months
Within the last 3 days*
Transfusion history / details of pregnancy not known
Within the last 3 days*
Placenta praevia (grade III or IV) requiring long term blood cover
Within the last 3 days*
Please provide sample for reassessment every Monday & Thursday.
Patient not transfused and not pregnant in last 3 months
Within the last 7 days
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
11
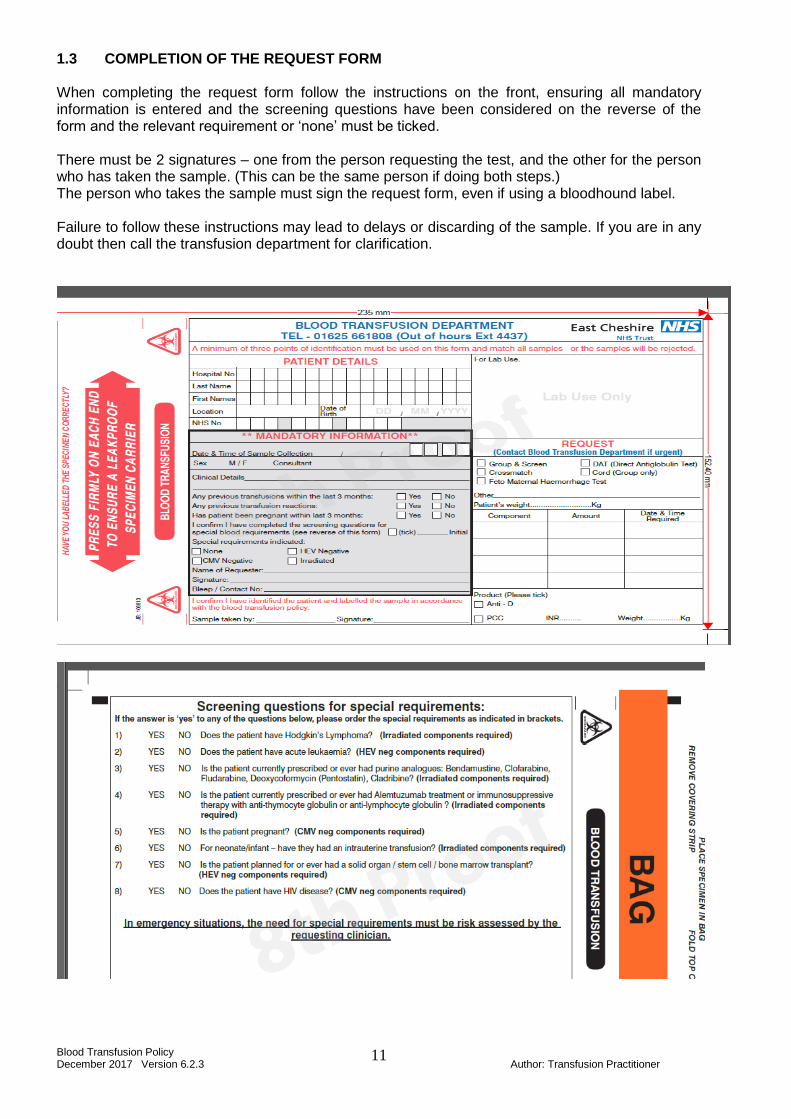
1.3 COMPLETION OF THE REQUEST FORM When completing the request form follow the instructions on the front, ensuring all mandatory information is entered and the screening questions have been considered on the reverse of the form and the relevant requirement or ‘none’ must be ticked. There must be 2 signatures – one from the person requesting the test, and the other for the person who has taken the sample. (This can be the same person if doing both steps.) The person who takes the sample must sign the request form, even if using a bloodhound label. Failure to follow these instructions may lead to delays or discarding of the sample. If you are in any doubt then call the transfusion department for clarification.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
12
1.4 REQUESTING BLOOD COMPONENTS A routine request for blood components requires 24 hour notice. If the requirement is within 24 hours then please notify the laboratory by telephone.
Monday to Friday during core hours telephone ext. 1808 Transfusion Laboratory All other times – short code 4437 – laboratory “out of hours” service or contact through switchboard.
On receipt of the telephone call, the laboratory staff will ask a number of questions to confirm the patient details and component requirements for the safe transfusion of the patient. HSC 2007/001 empowers the laboratory staff to ensure that a transfusion request is appropriate.
Send the sample with its request form immediately to the Pathology Reception
A telephone request for a crossmatch can be accepted from clinicians or delegated individuals who must be able to relay the appropriate information from the requesting clinician.
A blood group and antibody screen request can be upgraded to a crossmatch, by contacting the laboratory as above.
A sample for blood group and antibody screen is normally stored in the laboratory for 7 days.
Timings of blood components:
2 units of emergency group O RhD Negative red cells are available for immediate dispatch from the laboratory.
These timings are only valid at the point where the patient‘s blood group has been confirmed. If a second ‘safety sample’ is requested then this must be received in the transfusion department as soon as possible in order to confirm the blood group of the patient.
Group specific red cell units take a minimum of 15 minutes
A full crossmatch takes a minimum of 45 minutes In emergency situations, where the patient’s blood group has not been confirmed then universal donor groups will be issued until this confirmation has been obtained. 1.5 URGENT REQUESTS for UNCONSCIOUS PATIENTS In an emergency, a sample from an unconscious A&E patient must be labelled with at least one unique identifier, this is usually the hospital PAS (Patient Administration System) number. An unlabelled sample will be discarded even in an emergency situation. Failure to comply with the Blood Transfusion policy or provide the required information may delay the provision of blood components.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
13
2.1 Blood components are collected from the laboratory by the portering staff and transported in boxes with the appropriate documentation enclosed to the designated blood fridges or other areas as described below.
2.2 Units of red cells and fresh frozen plasma (FFP) issued to ward 5 and the Orthopaedic
Theatre are transported to the Orthopaedic Theatre Blood Bank refrigerator. 2.3 Units of red cells and FFP issued to all other ward areas are transported to the Main
Theatre Blood Bank refrigerator. The documentation is filed in the appropriate place of the Blood Bank Register alphabetically by surname.
2.4 Blood components issued to the Regency Hospital are transported to the Regency Blood
Bank refrigerator. The documentation is filed, alphabetically by surname, in the Blood Bank Register kept next to the refrigerator.
2.5 Red cells issued to the East Cheshire Hospice are transported in a validated insulated box
which maintains the components environment for 5 hours.
2.6 Cryoprecipitate will be issued directly to the ward for immediate use. 2.7 Platelets are ordered on a named patient basis from the NHS Blood and Transplant in
Manchester. Depending upon the availability of platelets and transportation time, it can take a number of hours before this component is on site. Platelets will be issued directly to the ward when the patient is ready for the infusion to begin. The bloodhound PDA’s should be used for products that arrive on the ward in the same process as for a blood transfusion. Never put platelets in the refrigerator.
2.8 In an emergency - two units of red cells may be delivered directly to the ward area where
the patient is being treated. 2.9 The person trained to collect the components from the designated Blood Bank Refrigerator
must use bloodhound to collect the blood from the fridge appropriately and complete the required checks.
2.10 The details that require checking are as follows:
The label containing all patient details: surname of patient, forename(s) of patient, date of birth, hospital unit number and patient’s blood group.
Expiry date of the component
Unique donation number of component
Donor unit blood group
General condition of the component – no leaks or clots within the bag
NEVER STORE BLOOD COMPONENTS IN A WARD OR DOMESTIC BLOOD FRIDGE
2.11 If a unit of red cells is removed from the blood bank refrigerator and transfusion is not
commenced within 30 minutes of removal, the unit of red cells is no longer suitable for further clinical use.
PROCEDURE 2:
RELEASE, STORAGE AND COLLECTION OF BLOOD COMPONENTS
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
14
Ensure that the Transfusion Department is contacted on extension 1808 if there are any problems prior to any transfusion. If the unit is within the 30 mins from fridge removal, then it can be scanned back into the blood bank fridge using bloodhound. (See separate bloodhound User guide) If more than 30 mins has passed, the blood unit MUST be labelled with marker pen: “OUT OF FRIDGE > 30 MINUTES DO NOT USE” and returned to the lab via a porter for disposal. The unit must be returned to the transfusion laboratory as soon as possible for disposal, in a sealed bag by a porter.
2.12 TRANSFER OF BLOOD COMPONENTS TO OTHER HOSPITALS
DO NOT transfer units of red cells without contacting the Blood Transfusion department Ext. 1808 during normal working hours or Ext. 4437 out of hours. Blood requested for transfer will always be despatched from the Blood Transfusion Department. The laboratory staff will ensure that the blood is packaged correctly and supply the necessary transfer documentation.
All transfers will be a maximum of 2 units of red cells.
Blood for transfer must NOT be removed from the blood bank refrigerator by anyone other than laboratory staff.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
15
Ensure the patient has been counselled on the risks/benefits of transfusion and has been provided with the appropriate information leaflets. 3.1 It must be stated in the notes that the transfusion has been discussed with the patient.
3.2 The patient’s notes, front of the blood component and patient’s wristband must be checked
against all other documents. All must agree or the transfusion should not be started. If the patient is able, they must always give verbal confirmation of their name and date of birth.
3.3 Prior to administering blood components, examine the component for any signs of
discoloration, clumps of material or fatty deposits. Check for leaks by squeezing it firmly. Check that the expiry date on the blood component has not been exceeded. Contact the Blood Transfusion Department (ext 1808 or via the switchboard if out of hours) if there are any anomalies.
3.4 Each component transfused must be recorded in the patient’s notes on the blood transfusion integrated pathway. One nurse and a bloodhound PDA can perform the safety checks on a component and begin the transfusion. If a PDA is not available or bloodhound is not available then 2 registered nurses must check the component and complete the relevant paperwork.
As the transfusion is commenced:
A minimum of one registered nurse must sign, date and time the blood transfusion integrated pathway and
scan with bloodhound handheld PDA
OR (if unable to use bloodhound PDA)
complete the white transfusion register form (in the folder at the frige) and
complete the red/white blood component traceability form (return to the lab) and
complete the blood transfusion integrated pathway (file in patient notes).
On the red/white documents record the following:
The date and time at which the component was connected to the patient
The signature of the two people checking it
The time the component finished transfusing. Place the signed blood component traceability form in the empty plastic bag and return to the Blood Transfusion Department as soon as possible.
3.5 Medications MUST NOT be added to blood components under any circumstances.
PROCEDURE 3:
ADMINISTRATION OF BLOOD
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
16
DO NOT WARM BLOOD COMPONENTS ON RADIATORS OR MICROWAVE, IN HOT WATER OR NEAR UNCONTROLLED HEAT SOURCES. Only approved blood warming devices must be used. The use of blood warmers will be indicated by the laboratory and are available from main theatre.
3.6 Monitoring of transfused patients
A full set of observations must be carried out within the hour prior to beginning the transfusion. The patient must be observed for the first 15 mins after commencing the transfusion, if possible the first 50ml should be given slowly. A full set of observations must be taken at 15 mins. A full set of observations must be done at the end of the transfusion. Further observations are at the discretion of the nurse / doctor caring for the patient. Transfusion of red cells must be started within 30 minutes of removal of the unit of red cells from the blood bank refrigerator. The transfusion must be completed at 4 hours of removal of the component from the fridge.
3.7 ANY ADVERSE EFFECTS, including shivering, rashes, flushing, shortness of breath or pain in the extremities or in the loins MUST be reported immediately to the Medical Officer in charge of the patient or the on-call medical team.
Adverse effects can include: Fever Low urine output Hypotension Agitation Rash Flushing Jaundice Breathlessness Shivering Pain in abdomen, flank or chest Haemoglobinurea Pain at infusion site If a transfusion reaction is suspected stop the infusion immediately, call the medical officer. Seek advice from the Blood Transfusion Department concerning which samples to take, and for clinical advice contact the Consultant Haematologist.
3.10 After disconnection dispose of as clinical waste. ONLY RETURN A COMPONENT TO THE LABORATORY IF A TRANSFUSION REACTION IS SUSPECTED. Component must be returned with giving set attached in a sealed bag, to the transfusion department by a porter.
3.11 Unless the transfusion is an emergency, components should be transfused to the patient
during the normal working day (08:00 to 20:00hrs) when appropriate monitoring can take place. Avoid transfusion over-night where possible.
3.12 The explicit reason for transfusing the patient must be recorded in the patient’s notes together with the full outcome of the transfusion event
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
17
REFERENCES McClelland, D.B.L. ed. (2007). Handbook of Transfusion Medicine - United Kingdom Blood Services, 5th Edition. London, The Stationary Office. British Committee for Standards in Haematology (BCSH) Guidelines on the administration of blood components Dec 2009 British Committee for Standards in Haematology (BCSH) (2012) Pre-transfusion compatibility procedures. BCSH website British Committee for Standards in Haematology (BCSH) (2004) Guidelines for the use of Fresh Frozen Plasma, Cryoprecipitate and Cryosupernatant. British Journal of Haematology; 126, 11-28. British Committee for Standards in Haematology (BCSH) (2014) Guidelines for the use of prophylactic Anti-D immunoglobulin. BCSH website. Blood Safety and Quality Regulations 2006 (Statutory Instrument (SI) 2006 No.50) Better Blood Transfusion 3 (Health Services Circular (HSC) 2007/001) NBTC Requirements for Training and Assessment 2016 NICE Guideline 24, Blood transfusion 2015 NPSA safer practice notice 14/2007 “Right Patient, Right Blood”
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
18
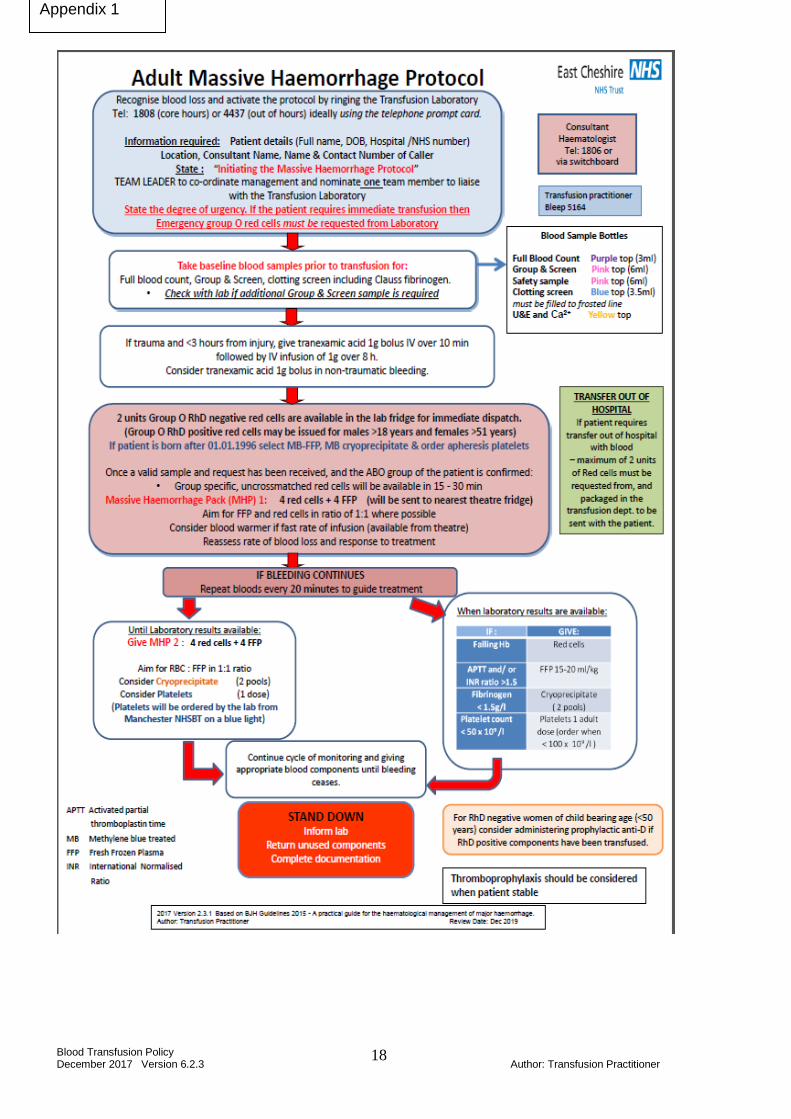
Appendix 1
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
19
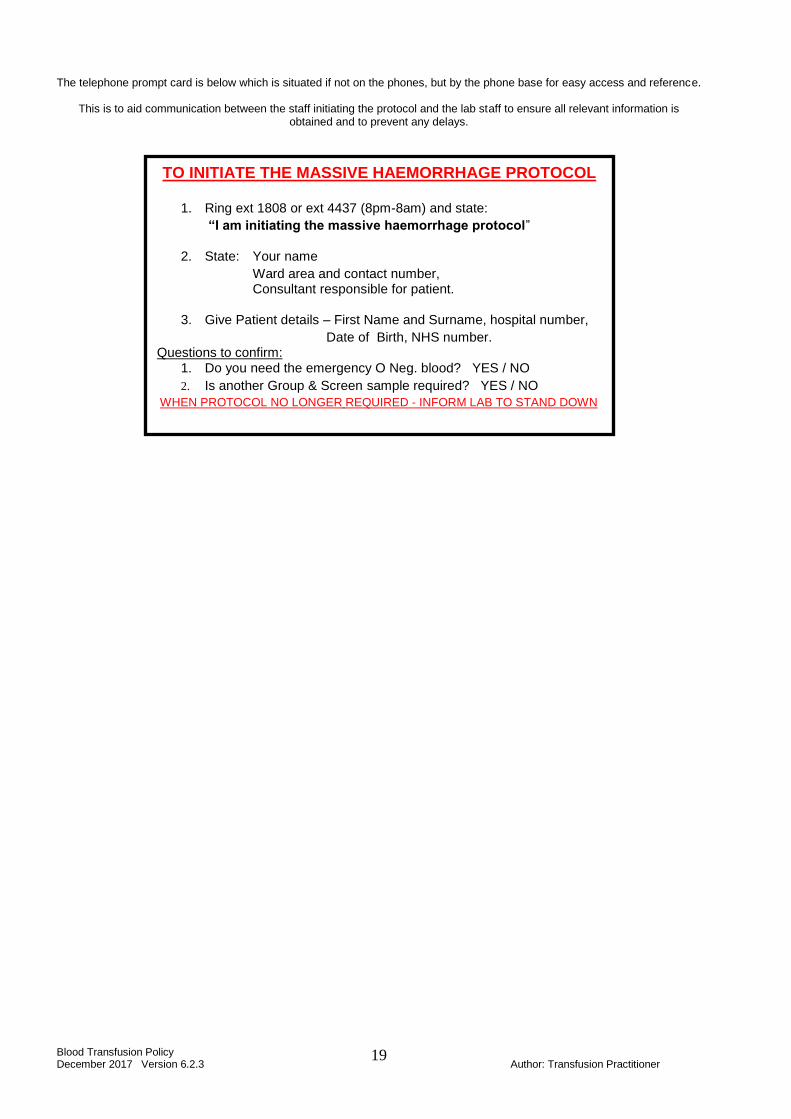
The telephone prompt card is below which is situated if not on the phones, but by the phone base for easy access and reference.
This is to aid communication between the staff initiating the protocol and the lab staff to ensure all relevant information is
obtained and to prevent any delays.
TO INITIATE THE MASSIVE HAEMORRHAGE PROTOCOL
1. Ring ext 1808 or ext 4437 (8pm-8am) and state:
“I am initiating the massive haemorrhage protocol”
2. State: Your name
Ward area and contact number, Consultant responsible for patient.
3. Give Patient details – First Name and Surname, hospital number,
Date of Birth, NHS number. Questions to confirm:
1. Do you need the emergency O Neg. blood? YES / NO
2. Is another Group & Screen sample required? YES / NO
WHEN PROTOCOL NO LONGER REQUIRED - INFORM LAB TO STAND DOWN
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
20
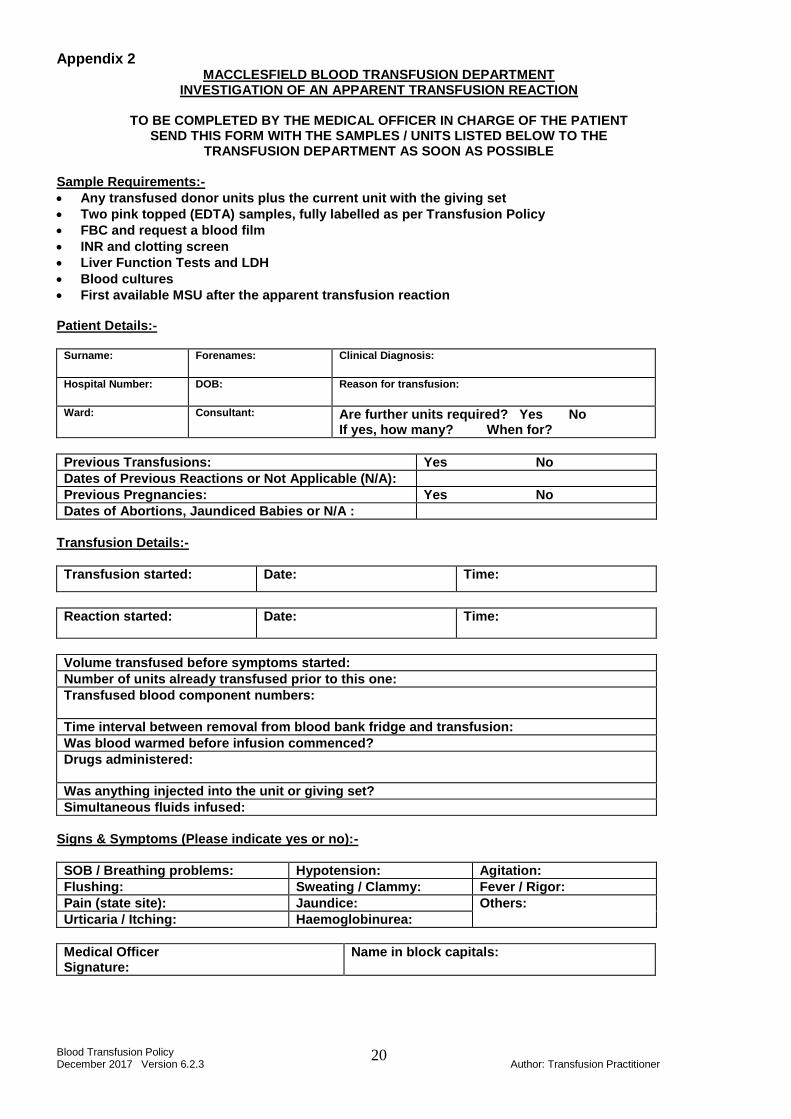
Appendix 2 MACCLESFIELD BLOOD TRANSFUSION DEPARTMENT
INVESTIGATION OF AN APPARENT TRANSFUSION REACTION
TO BE COMPLETED BY THE MEDICAL OFFICER IN CHARGE OF THE PATIENT SEND THIS FORM WITH THE SAMPLES / UNITS LISTED BELOW TO THE
TRANSFUSION DEPARTMENT AS SOON AS POSSIBLE
Sample Requirements:-
Any transfused donor units plus the current unit with the giving set
Two pink topped (EDTA) samples, fully labelled as per Transfusion Policy
FBC and request a blood film
INR and clotting screen
Liver Function Tests and LDH
Blood cultures
First available MSU after the apparent transfusion reaction Patient Details:-
Surname:
Forenames: Clinical Diagnosis:
Hospital Number:
DOB: Reason for transfusion:
Ward: Consultant:
Are further units required? Yes No If yes, how many? When for?
Previous Transfusions: Yes No
Dates of Previous Reactions or Not Applicable (N/A):
Previous Pregnancies: Yes No
Dates of Abortions, Jaundiced Babies or N/A :
Transfusion Details:-
Transfusion started: Date: Time:
Reaction started: Date: Time:
Volume transfused before symptoms started:
Number of units already transfused prior to this one:
Transfused blood component numbers:
Time interval between removal from blood bank fridge and transfusion:
Was blood warmed before infusion commenced?
Drugs administered:
Was anything injected into the unit or giving set?
Simultaneous fluids infused:
Signs & Symptoms (Please indicate yes or no):-
SOB / Breathing problems: Hypotension: Agitation:
Flushing: Sweating / Clammy: Fever / Rigor:
Pain (state site): Jaundice: Others:
Urticaria / Itching: Haemoglobinurea:
Medical Officer Signature:
Name in block capitals:
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
21
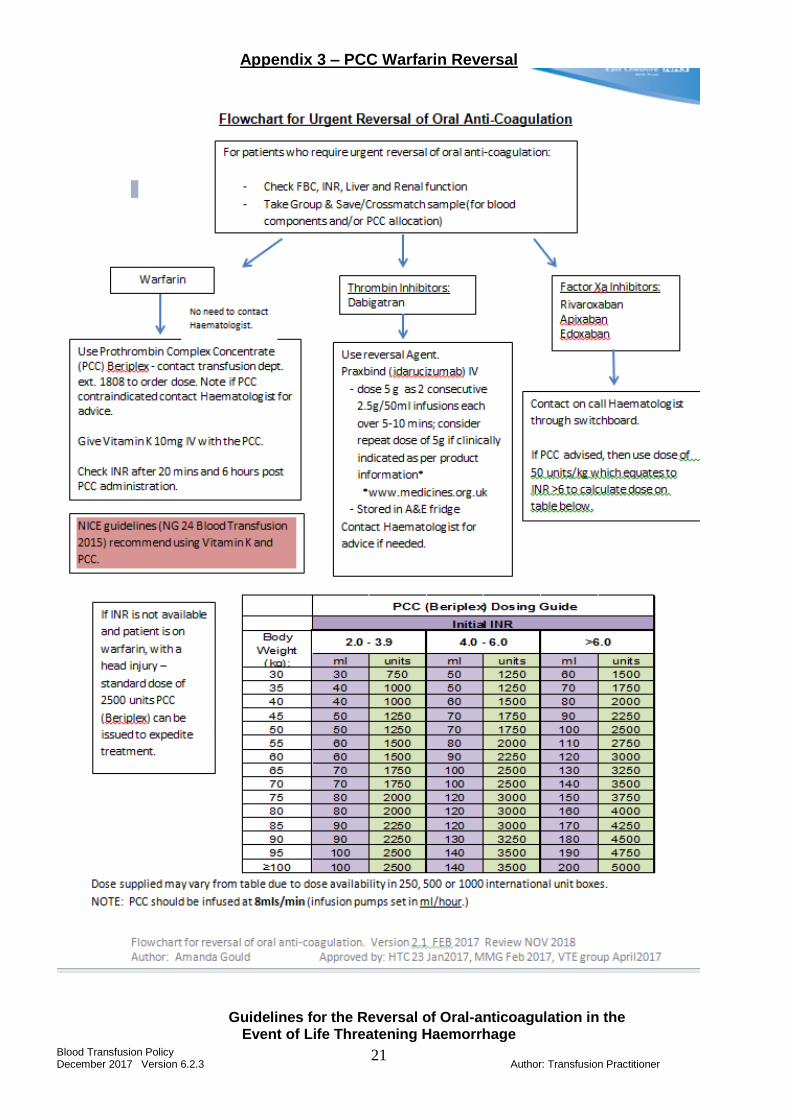
Appendix 3 – PCC Warfarin Reversal
Guidelines for the Reversal of Oral-anticoagulation in the
Event of Life Threatening Haemorrhage
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
22
Reversal of Warfarin and Analogues
1. Principle of Procedure
Prothrombin Complex Concentrate (PCC) is made from human plasma and it contains the human coagulation factors II, VII, IX and X, plus Protein C and Protein S. The coagulation factors II, VII, IX and X are vitamin K-dependent and are important for blood clotting. Lack of any of these factors will lead to an increased tendency to bleed. The replacement of factors II, VII, IX and X with PCC (brand name Beriplex P/N at this Trust) will repair the coagulation mechanisms. Beriplex P/N is presented as powder and solvent. The reconstituted solution is to be given by injection into a vein.
2. Indications for use
Prothrombin Complex Concentrates (PCC) such as the brands Beriplex P/N are used for the prevention and treatment of bleeds caused by the acquired or congenital lack of vitamin K-dependent coagulation factors. Fresh Frozen Plasma (FFP) has usually been used in cases of excessive bleeding or to prevent bleeding in patients with abnormal coagulation tests that are undergoing an invasive procedure. It has now been recognised that FFP is not the optimal form of coagulation factor replacement and in the case of a life threatening haemorrhage as a consequence of warfarin or other coumarin therapy. FFP should only be used when PCC is not available or is contraindicated.
3. Sample Requirements
Prior to the issue of PCC the following samples must be screened:
Full blood count (FBC)
Coagulation screen: PT, APTT and Clauss fibrinogen (not derived – this is only viable for normal results)
Baseline renal and liver function tests
A current sample must be available for group and screen to allow the allocation of the product to the patient’s record.
Any patient on warfarin with a strong suspicion of intracerebral haematoma after a clear head injury should have PCC made available prior to laboratory testing. This decision must be consultant lead. The INR must be checked 20-30 mins after the PCC has been administered to confirm suitable reversal. The laboratory will issue a standard dose of 2500IU of PCC for these patients.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
23
4. Reversal of Oral anti-coagulants (alternatives to WARFARIN) Reversal of thrombin inhibitors Dabigatran - Reversal agent Praxbind (5g Dose) available in A&E fridge. Not life threatening haemorrhage Stop anticoagulant Life threatening haemorrhage Stop anticoagulant Measure Thrombin time to verify if patient anticoagulated Discuss with consultant haematologist for appropriate measures Reversal of factor Xa inhibitors – No reversal agent available Rivaroxaban Apixaban Edoxaban Not life threatening haemorrhage: Stop the anticoagulant Life threatening haemorrhage: Stop the anticoagulant Prescribe PCC (Beriplex) 50IU / kg (use INR - above 6) Measure the Thrombin time pre and post to verify reversal Discuss with consultant haematologist for other appropriate measures Note Factor Xa and Thrombin inhibitors are new anticoagulants and there is little evidence in the appropriate reversal in the event of a life threatening haemorrhage so discussion with the consultant haematologist is strongly advised
5. Dose and Administration
Stop warfarin and reverse anticoagulation
Give vitamin K1 5 – 10 mg IV slowly (over 10 – 15 minutes). This can cause anaphylaxis if given too quickly.
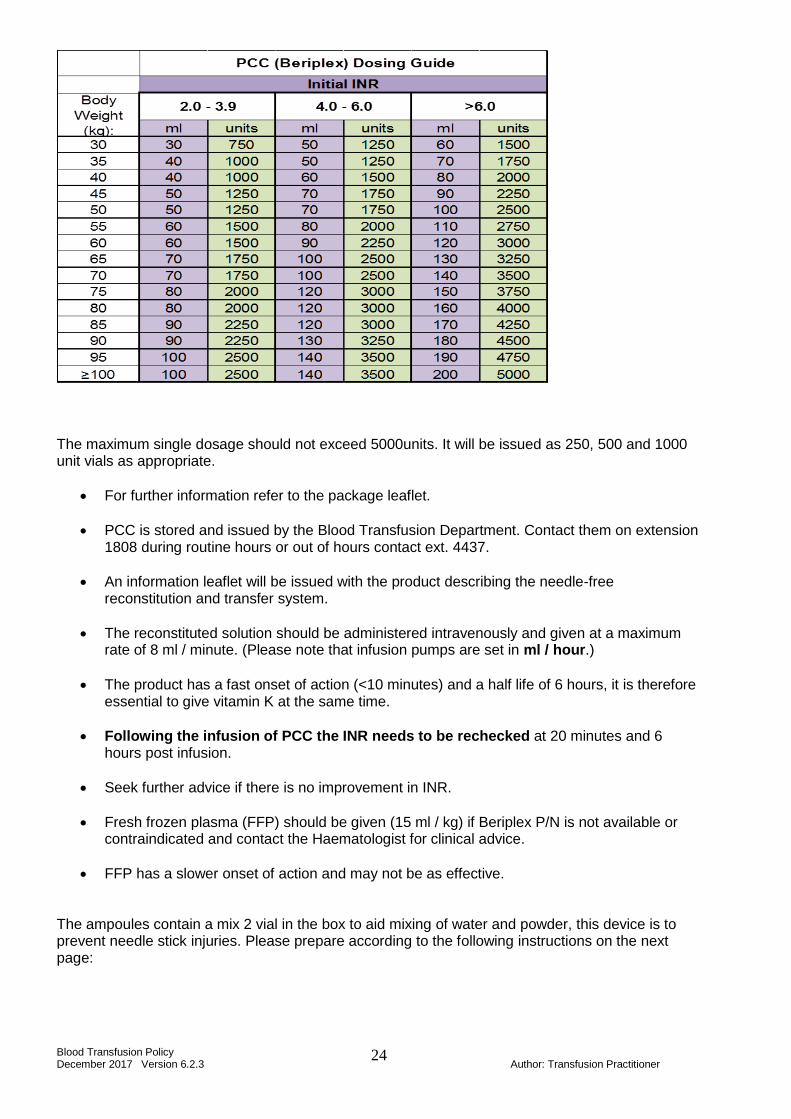
Give Beriplex P/N (Prothrombin Complex Concentrate). Calculate the dose according to the INR and weight in kg as per table below:
Patient’s INR Recommended dose of Beriplex P/N
2.0 – 3.9 25 units / kg body weight
4.0 – 6.0 35 units / kg body weight
Above 6.0 50 units / kg body weight
This is incorporated into the following dosage guide:
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
24
The maximum single dosage should not exceed 5000units. It will be issued as 250, 500 and 1000 unit vials as appropriate.
For further information refer to the package leaflet.
PCC is stored and issued by the Blood Transfusion Department. Contact them on extension 1808 during routine hours or out of hours contact ext. 4437.
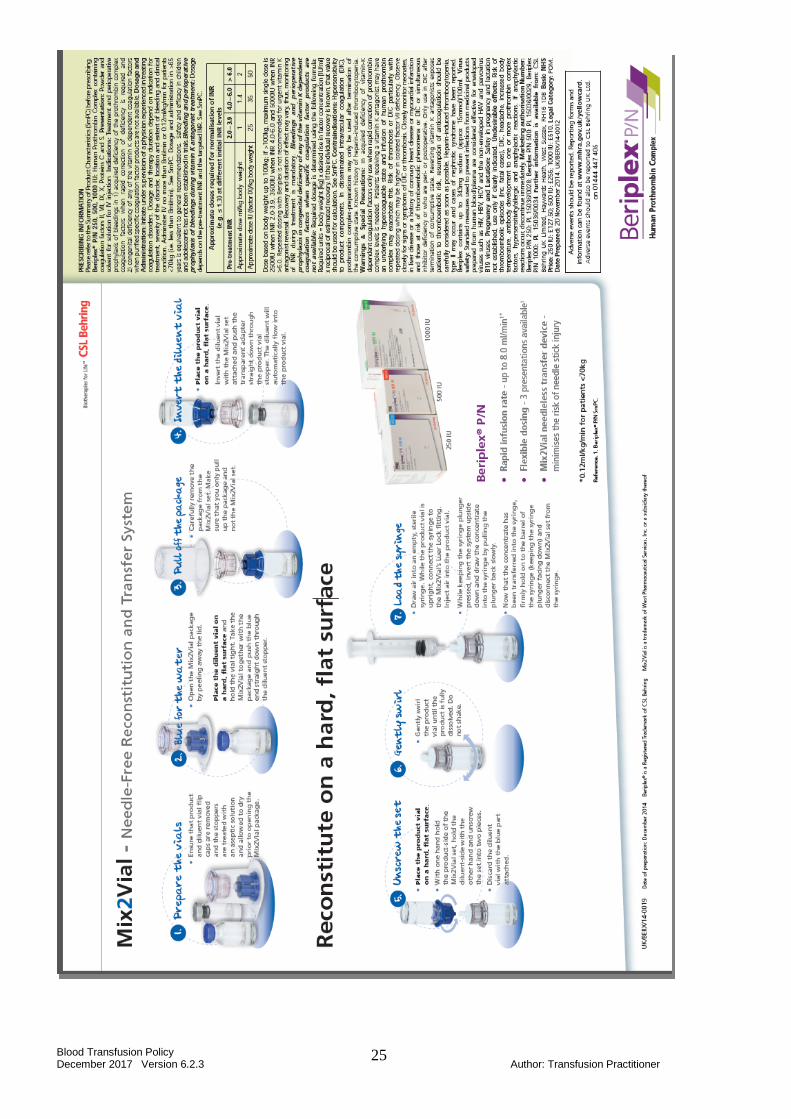
An information leaflet will be issued with the product describing the needle-free reconstitution and transfer system.
The reconstituted solution should be administered intravenously and given at a maximum rate of 8 ml / minute. (Please note that infusion pumps are set in ml / hour.)
The product has a fast onset of action (<10 minutes) and a half life of 6 hours, it is therefore essential to give vitamin K at the same time.
Following the infusion of PCC the INR needs to be rechecked at 20 minutes and 6 hours post infusion.
Seek further advice if there is no improvement in INR.
Fresh frozen plasma (FFP) should be given (15 ml / kg) if Beriplex P/N is not available or contraindicated and contact the Haematologist for clinical advice.
FFP has a slower onset of action and may not be as effective.
The ampoules contain a mix 2 vial in the box to aid mixing of water and powder, this device is to prevent needle stick injuries. Please prepare according to the following instructions on the next page:
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
25
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
26
6. Contraindications to use of Beriplex P/N
Known hypersensitivity to any of the components of the product.
Risk of thrombosis, angina pectoris, recent myocardial infarction (exception: life-threatening haemorrhages following overdose of oral anticoagulants, and before induction of fibrinolytic therapy).
In the case of disseminated intravascular coagulation, prothrombin complex preparations may only be applied after termination of the consumptive state.
Known history of heparin-induced thrombocytopenia. For further information see product SPC accessible on www.medicines.org.uk
7. Audit
FFP is a blood component and PCC is a plasma product. It is important that they are used Appropriately, and their prescription and rationale for use are recorded in the patient’s notes. Ensure that the white crossmatch sheet is signed and returned to the Blood Transfusion Department and that the red/white transfusion report is filed in the patient case notes. Use wisely: Beriplex P/N typically costs £1500 for a typical adult. If further clinical advice is required regarding this product please contact the Haematologist. 7. Related BCSH Guidelines British Committee for Standards in Haematology. Guidelines on oral anticoagulation fourth edition. British Journal of Haematology; 154, 311-324. British Committee for Standards in Haematology. Guidelines on oral anticoagulation (warfarin): third edition 2005 update. British Society for Haematology; 132, 277-285. British Committee for Standards in Haematology 2004 a) Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. British Journal of Haematology; 126, 11-28.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
27
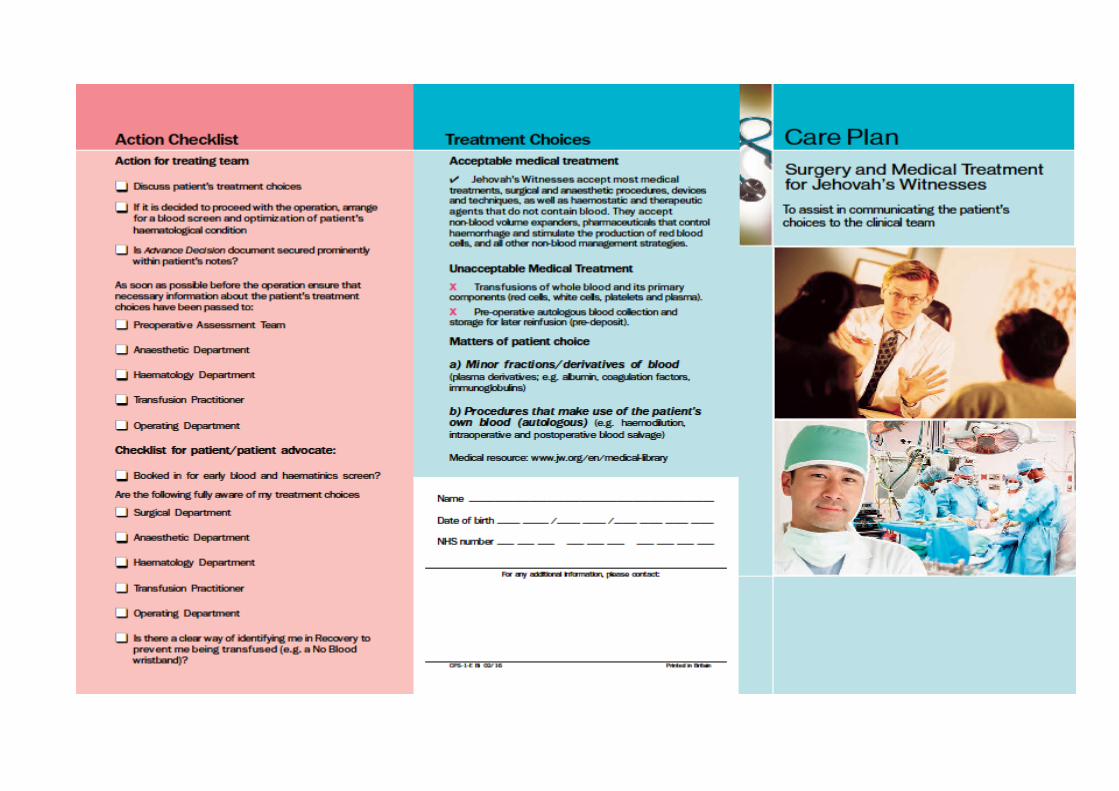
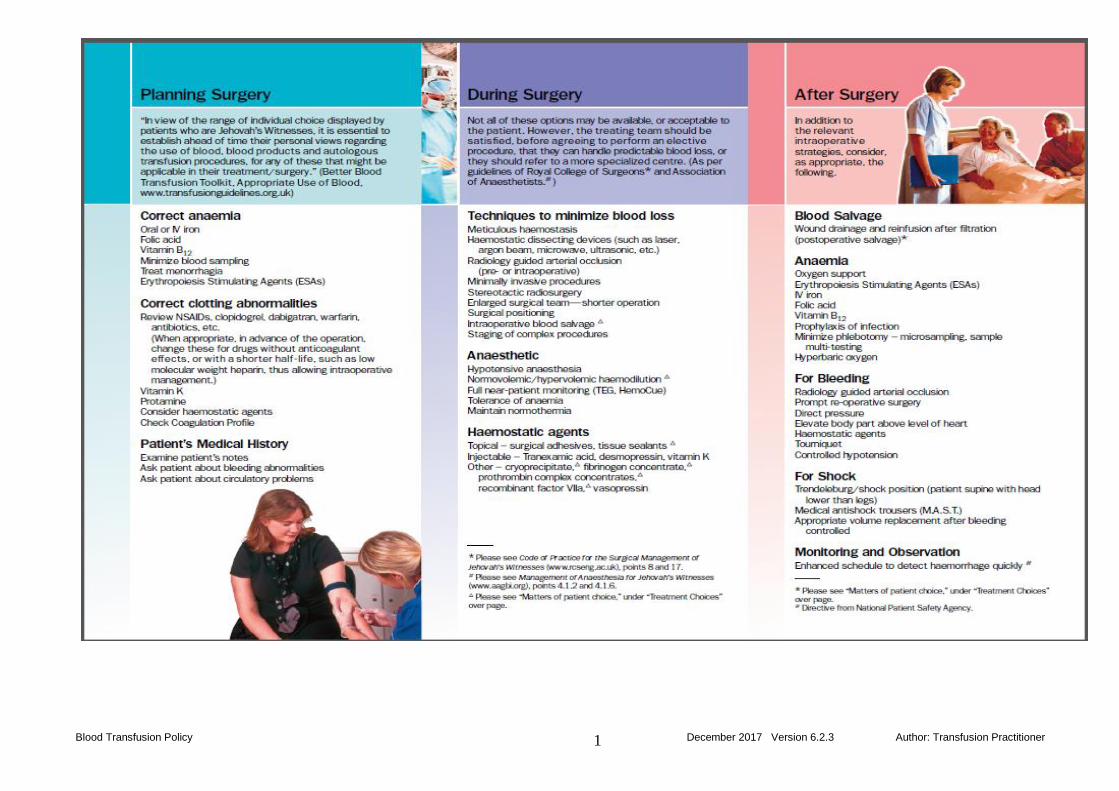
Appendix 4
EMERGENCY PROTOCOL FOR TREATING JEHOVAH'S WITNESSES Jehovah’s Witnesses carry an Advance Medical Directive that directs that no donor blood be administered under any circumstances, and releases doctors and hospitals from liability for any damages that might be caused by the patient’s refusal of blood. The card is also carried by Witness children. The card contains other pertinent information that may be helpful to an emergency team. In an emergency, if information is required regarding consent issues, treatment alternatives etc, please telephone the number below: EMERGENCY PHONE NUMBER (24 HOUR) 07831 343 895 If a Jehovah's Witness patient comes into the Trust for emergency treatment the following is advised:
1. Ask for/look for an Advance Medical Directive or in the case of a child an identity card. Information is available on the reverse of the card.
2. Review non-blood medical alternatives and treat the patient without using homologous
blood. 3. Consult with colleagues experienced in non-blood alternative management at the same
facility and treat without using homologous blood. 4. Contact local Hospital Liaison Committee of Jehovah's Witnesses for co-operative
consultants at other facilities to confer with regarding alternative care (see above for emergency phone number).
5. If necessary, transfer the patient to a co-operative consultant or facility before the patient's
condition deteriorates. 6. In a rare situation, if court assistance is deemed necessary, the patient, or parents, should
be notified as soon as possible of such intended action. This is in harmony with natural justice and enables the court to hear both sides, including alternative non-blood medical management of the case, so as to weigh all the factors before reaching a decision.
7. Consent Form: The East Cheshire Trust ‘General Consent Form Excluding Blood
Transfusion’ (print code number CPY 734 2/05) is a supplementary form to be used alongside the trust consent forms and may also be used for any patient refusing a blood transfusion regardless of their spiritual beliefs.
8. Guidance relating to the treatment of Witness children is below.
CHILDREN - LEGAL AND CONSENT ISSUES.
The children of Jehovah's Witnesses requiring blood transfusion present the most difficult management problem. The wellbeing of the child is paramount and if, after full parental consultation, blood is refused, the surgeon should make use of the law to protect the child's interests.
In England and Wales, a Specific Issue Order may be applied for to provide legal sanction for a specific action, such as the administration of blood, without removing all parental authority. The order should be limited to the specific medical condition requiring treatment, and the parents
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
28
should be kept informed at each stage of the application. Advice and assistance in obtaining this action should be sought from a medical social worker.
If a child needs blood in an emergency, despite the surgeon's best efforts to contain haemorrhage, it should be given. The surgeon who stands by and allows a 'minor' patient to die in circumstances where blood might have avoided death may be vulnerable to criminal prosecution.
Children of 16 can give legally valid consent for medical treatment and children under this age can consent if they understand the issues involved. However, the courts have proved willing to overrule the refusal of specific procedures by children.
The High Court is the most appropriate forum to achieve a fair and impartial hearing when conflict arises between religious, medical and ethical opinions.
PREOPERATIVE CONSIDERATIONS
For elective surgery in children, a full and frank discussion should take place between the surgeon and the parents of the child; the relevant anaesthetist may also need to be directly involved at this stage. Either parent may sign a consent form permitting a transfusion.
Most operations on children do not require or involve blood transfusion. If, in the opinion of the surgeon, the child is extremely unlikely to need transfusion as a result of the procedure, the usual arrangements should be made to proceed with the operation. The parents should be invited to sign the appropriate forms signifying their objection to blood transfusion.
Recognising that misjudgements will occur and that occasionally a transfusion will unexpectedly become necessary, the surgeon may choose to say to the parents, 'I will not allow your child to die for want of a blood transfusion'; unless it is, indeed, an intention to withhold blood under all circumstances. Most parents find this acceptable.
Some operations carry a significant risk of needing blood transfusion. These can be divided into three groups:
Group 1 - Those which are absolutely indicated and urgent.
Group 2 - Those which are absolutely indicated and non-urgent.
Group 3 - Those which are not absolutely indicated.
In group 1, if the surgeon feels it would be unreasonable to proceed without the freedom to transfuse, the help of the medical social worker should be sought in obtaining a Specific Issue Order from the courts. In an emergency, when there is no time to obtain a Specific Issue Order, the use of blood components and blood products in life-threatening situations should be based on the judgement of the clinician in charge of the patient.
In group 2, the patient could be transferred to the care of a surgeon who is prepared to operate even under these constraints.
In group 3, a non-operative choice may be appropriate.
In groups 2 and 3, if these alternatives are not clinically appropriate, the surgeon should proceed as in group1.
At times, it may be judged that the patient is competent to make the necessary decisions, in which his/her wishes must be respected. A child may not be competent to make the necessary independent decisions if unduly influenced by another person.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
29
At all times, the surgeon must respect the beliefs of the family. Every effort should be made to avoid the perioperative use of blood components or blood products. Nevertheless, the wellbeing of the child is paramount.
References:
Medical Management for Jehovah’s Witnesses, Hospital Liaison Committee (documents held by Nursing and Quality)
Code of Practice for the Surgical Management of Jehovah’s Witness (2002), RCS (attached to this protocol)
The Law of Consent to Medical Treatment (2002), Hockton, A,
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
30
GENERAL CONSENT FORM EXCLUDING BLOOD TRANSFUSION Patient’s Full Name ……………………………………………….……………………...
Date of Birth ………………………..……………. Male Female Unit Number …………………………….……….. DOCTOR – Please see overleaf (this part to be completed by Registered Medical Practitioner) TYPE OF OPERATION, INVESTIGATION OR TREATMENT: I confirm that I have explained the operation, investigation or treatment, and such appropriate options as are available and the type of anaesthetic, if any (general/regional/sedation) proposed, to the patient in terms which my judgement are suited to the understanding of the patient and/or to one of the parents, or guardians of the patient. I further confirm that I have emphasised my clinical judgement of the potential risks to the patient and/or person who non-the-less understood and imposed the limitation of consent listed below. I acknowledge that this limited consent will not be over-ridden unless revoked or modified in writing. Signature ……………………………………………………………………………………………..… Date ………………….……… Name of Registered Medical Practitioner ……………………………………………………………………………………………… PATIENT/PARENT/GUARDIAN – Please see overleaf I am the patient / parent / guardian (delete as necessary) I agree:
to what is proposed, which has been explained by the doctor, named above
to the use of the type of anaesthetic that I have been told about
to the use of non-blood volume expanders; pharmaceuticals that control haemorrhage and/or stimulate the production of red blood cells:
(Subject to the exclusions below) I have told the doctor:
I am / am not one of Jehovah’s Witnesses with firm religious convictions and that I have decided resolutely: to obey the Bible command “keep abstaining from … blood”(Acts 15:28, 29). With full
realisation of the implications of this position, and exercising my own choice, free from any external influence, I expressly WITHOLD MY CONSENT to the transfusion of ALLOGENEIC BLOOD OR PRIMARY BLOOD COMPONENTS (RED CELLS, WHITE CELLS, PLASMA & PLATELETS), and to the use of any sample of my blood for cross-matching.
That this limitation of consent shall remain in force and bind all those treating me unless and until I expressly revoke it in writing.
About any additional procedures I would NOT wish to be carried out straightaway without my having the opportunity to consider them first. I understand:
That the procedure might not be done by the doctor who has been treating me so far.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
31
That my express refusal of allogeneic blood or primary blood components will be regarded as absolute and WILL NOT be over-ridden in ANY circumstances by a purported consent of a relative or other person or body.
Such refusal will be regarded as remaining in force even though I may be unconscious and/or affected by medication, stroke or other condition rendering me incapable of expressing my wishes and consent to treatment options, and the doctor(s) treating me consider that SUCH REFUSAL MAY BE LIFE THREATENING.
That any procedure in addition to the investigation or treatment described on this form, but with the exclusion of the transfusion of allogeneic blood or primary blood components, will only be carried out if it is necessary and in my best interests and can be justified for medical reasons.
That details of my treatment, and any consequences resulting, will not be disclosed to any source without my express consent or that of my instructed agent(s), unless required by law.
Signature …………………………………………………………………………………………. Date …………………………………
1. Please read this form and the notes below very carefully.
2. If there is anything that you don’t understand about the explanation, or if you want more
information you should ask the doctor.
3. Please check that all the information on the form is correct. If it is, and you understand the explanation, then sign the form.
NOTES TO DOCTORS
This form is a supplementary form to be used alongside the trust consent forms.
A patient has a legal right to grant or withhold consent prior to examination or treatment. Patients should be given sufficient information, in a way they can understand, about the proposed treatment and the possible alternatives. Patients must be allowed to decide whether they will agree to the treatment and they may refuse or withdraw consent at any time. A Jehovah’s Witness patient’s limited consent to treatment should be recorded on this form.
Further guidance is given in HC (90)22 A Guides to Consent for Examination or Treatment and the trust policy for consent to examination or treatment.
PATIENTS
The doctor is here to help you. He or she will explain the proposed treatment and what the alternatives are. You can ask any questions and seek further information. You can refuse the treatment.
You may ask for a relative, or friend, or Hospital Liaison Committee member, or a nurse to be present.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
32
Training health professionals is essential to the continuation of the health service and improving the quality of care. Your treatment may provide an important opportunity for such training, where necessary under the careful supervision of a senior doctor. You may refuse any involvement in a formal training programme without this adversely affecting your care and treatment.
FORMS
Blank copies of this form are available from the Print Room, code CPY734 2/05. Model form taken from the Code of Practice for the surgical management of Jehovah’s Witnesses. The Royal College of Surgeons of England (2002)
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner 1
Appendix 5
OUT OF HOSPITAL – BLOOD TRANSFUSION PROTOCOL
This protocol acts as a supplement to the East Cheshire NHS Trust Blood Transfusion
Policy and is designed to facilitate blood transfusion at designated centres outside of the main hospital, with agreement between Clinicians responsible for that Centre and the
Transfusion Department. At least 24 hours’ notice needs to be given for crossmatching and component selection. Procedure 1. Identification of patient, taking of blood sample and completion of request form to be
performed as described in the Blood Transfusion Policy 2. Release, collection and storage of blood. The patient notes are to be brought to the
Transfusion Laboratory to identify the blood required. Transfusion staff to provide a maximum of two units in the dedicated insulated container. The container will guarantee temperature stability for four hours. The person designated to collect the blood must travel directly from the Transfusion Laboratory to the Centre where the blood transfusion is occurring.
3. Administration of blood. The prescription of the blood is the responsibility of the Medical
Officer in charge of the patient. Each unit of blood must only be removed immediately prior to administration, remaining units must be kept in the insulated box. The box must be closed immediately following the removal of each unit to ensure adequate temperature control of remaining units. It is strongly recommended that each unit is transfused over two hours unless there are medical reasons to prolong this.
4. At the point of administration of each unit of blood complete the enclosed documentation
regarding the date and time of transfusion. Place the red report form in the patient's notes and after completion of all of the units return the white copy and the red traceability forms with the insulated box to the Transfusion Department.
5. On completion, the empty unit should be placed in an appropriate sharps bin (if administration
set attached) or clinical waste (if empty bag only). The empty insulated blood container must be returned to the Transfusion Laboratory within twenty four hours of completion of transfusion.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
1
Appendix 6
Safety samples For patients’ requiring a transfusion that have no historic blood group available on our database, then a second ‘safety’ sample is obtained to verify their blood group prior to the issue of blood components. This second sample should only be taken when requested to do so by the laboratory. It is important that the two samples are taken independently of one another. Two samples must not be taken at the same time and one ’saved’ to send to the transfusion laboratory at a later time. Taking of the safety sample should never compromise the patient who needs blood components urgently. The recommendation of this safety sample is based on the evidence from the BEST studies as referenced in 7.2, and on data from the IBCT and the Near Miss chapters in recent SHOT reports (SHOT, 1996 to 2010) – 386 cases of wrong blood in tube (WBIT) were reported as near misses in 2010. By taking a safety sample the risk of WBIT goes from approximately 1 in 14,000 to 1 in 500,000. Appendix 7 - COMPLETION OF THE REQUEST FORM
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
2
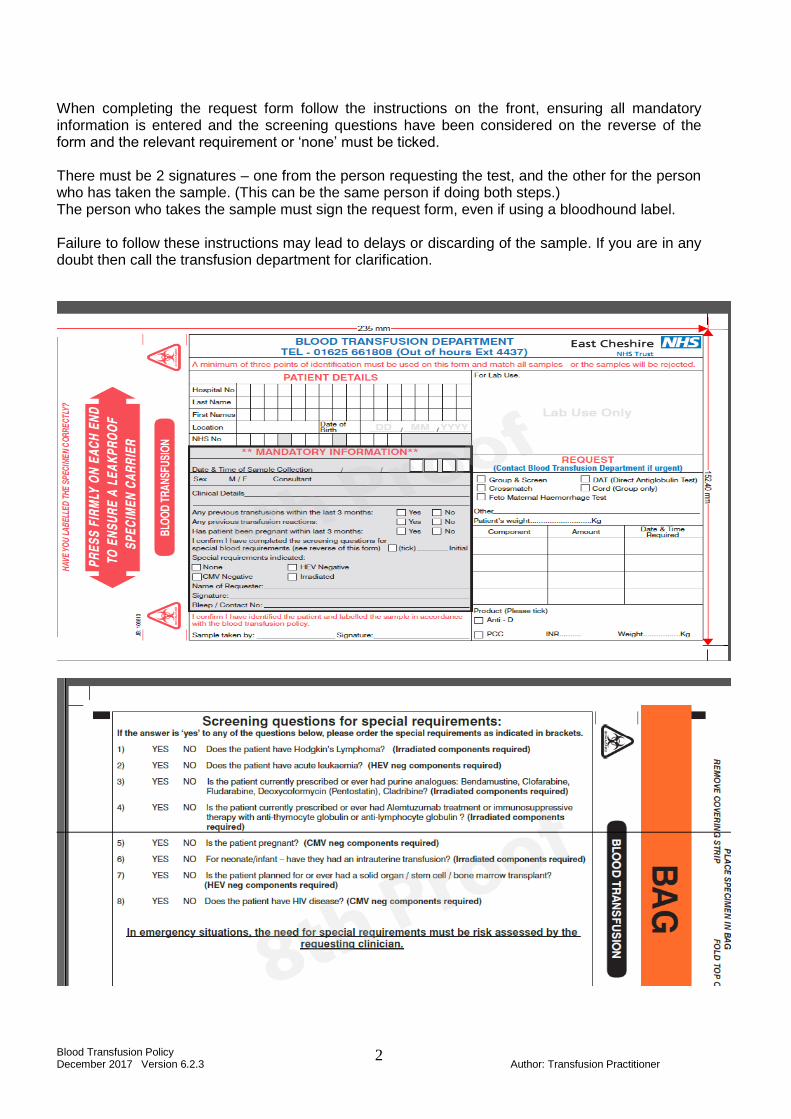
When completing the request form follow the instructions on the front, ensuring all mandatory information is entered and the screening questions have been considered on the reverse of the form and the relevant requirement or ‘none’ must be ticked. There must be 2 signatures – one from the person requesting the test, and the other for the person who has taken the sample. (This can be the same person if doing both steps.) The person who takes the sample must sign the request form, even if using a bloodhound label. Failure to follow these instructions may lead to delays or discarding of the sample. If you are in any doubt then call the transfusion department for clarification.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
3
Equality Analysis (Impact assessment)
1. What is being assessed?
Blood transfusion policy
Details of person responsible for completing the assessment:
Name: Amanda Gould
Position: Transfusion Practitioner
Team/service: Clinical Support Service
State main purpose or aim of the policy, procedure, proposal, strategy or service: (usually the first paragraph of what you are writing. Also include details of legislation, guidance, regulations etc which have shaped or informed the document)
To ensure safe, effective, timely and appropriate transfusion of blood components and blood products. This policy identifies individual roles and ensures the process is focused on patient safety.
2. Consideration of Data and Research
To carry out the equality analysis you will need to consider information about the people who use the service and the staff that provide it.
2.1 Give details of RELEVANT information available that gives you an understanding of who will be affected by this document
Cheshire East (CE) covers Eastern Cheshire CCG and South Cheshire CCG. Cheshire West & Chester (CWAC) covers Vale Royal CCG and Cheshire West CCG. In 2011, 370,100 people resided in CE and 329,608 people resided in CWAC.
Age: East Cheshire and South Cheshire CCG’s serve a predominantly older population than the national average, with 19.3% aged over 65 (71,400 people) and 2.6% aged over 85 (9,700 people). Vale Royal CCGs registered population in general has a younger age profile compared to the CWAC average, with 14% aged over 65 (14,561 people) and 2% aged over 85 (2,111 people). Since the 2001 census the number of over 65s has increased by 26% compared with 20% nationally. The number of over 85s has increased by 35% compared with 24% nationally. Race:
In 2011, 93.6% of CE residents, and 94.7% of CWAC residents were White British
5.1% of CE residents, and 4.9% of CWAC residents were born outside the UK – Poland and India being the most common
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
4
3% of CE households have members for whom English is not the main language (11,103 people) and 1.2% of CWAC households have no people for whom English is their main language.
Gypsies & travellers – estimated 18,600 in England in 2011. Gender: In 2011, c. 49% of the population in both CE and CWAC were male and 51% female. For CE, the assumption from national figures is that 20 per 100,000 are likely to be transgender and for CWAC 1,500 transgender people will be living in the CWAC area. Disability:
In 2011, 7.9% of the population in CE and 8.7% in CWAC had a long term health problem or disability
In CE, there are c.4500 people aged 65+ with dementia, and c.1430 aged 65+ with dementia in CWAC. 1 in 20 people over 65 has a form of dementia
Over 10 million (c. 1 in 6) people in the UK have a degree of hearing impairment or deafness.
C. 2 million people in the UK have visual impairment, of these around 365,000 are registered as blind or partially sighted.
In CE, it is estimated that around 7000 people have learning disabilities and 6500 people in CWAC.
Mental health – 1 in 4 will have mental health problems at some time in their lives. Sexual Orientation:
CE - In 2011, the lesbian, gay, bisexual and transgender (LGBT) population in CE was estimated at18,700, based on assumptions that 5-7% of the population are likely to be lesbian, gay or bisexual and 20 per 100,000 are likely to be transgender (The Lesbian & Gay Foundation).
CWAC - In 2011, the LGBT population in CWAC is unknown, but in 2010 there were c. 20,000 LGB people in the area and as many as 1,500 transgender people residing in CWAC.
Religion/Belief: The proportion of CE people classing themselves as Christian has fallen from 80.3% in 2001 to 68.9% In 2011 and in CWAC a similar picture from 80.7% to 70.1%, the proportion saying they had no religion doubled in both areas from around 11%-22%.
Christian: 68.9% of Cheshire East and 70.1% of Cheshire West & Chester
Sikh: 0.07% of Cheshire East and 0.1% of Cheshire West & Chester
Buddhist: 0.24% of Cheshire East and 0.2% of Cheshire West & Chester
Hindu: 0.36% of Cheshire East and 0.2% of Cheshire West & Chester
Jewish: 0.16% of Cheshire East and 0.1% of Cheshire West & Chester
Muslim: 0.66% of Cheshire East and 0.5% of Cheshire West & Chester
Other: 0.29% of Cheshire East and 0.3% of Cheshire West & Chester
None: 22.69%of Cheshire East and 22.0% of Cheshire West & Chester
Not stated: 6.66% of Cheshire East and 6.5% of Cheshire West & Chester
Carers: In 2011, nearly 11% (40,000) of the population in CE are unpaid carers and just over 11%
(37,000) of the population in CWAC.
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
5
2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints or concerns raised either from patients or staff (grievance) relating to the policy, procedure, proposal, strategy or service or its effects on different groups?)
No
2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result of this document?
No
3. Assessment of Impact Now that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy or service (part 1) and looked at the data and research you have (part 2), this section asks you to assess the impact of the policy, procedure, proposal, strategy or service on each of the strands listed below.
RACE: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, racial groups differently? Yes No
Explain your response:
All groups are equally likely to require blood products. For patients or NOK/carers whose foirst language is not English and where information/explanation is required, eg around consent, staff will follow the trust interpretation policy.
GENDER (INCLUDING TRANSGENDER): From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, different gender groups differently? Yes No
Explain your response: All groups are equally likely to require blood products.
DISABILITY From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, disabled people differently? Yes No
Explain your response: All groups are equally likely to require blood products. For patients with senory disabilities such as hearing or visual impairment, staff will follow the trust interpretation policy to ensure information and explanation is understood. For patients with learning disabilities there are picture communication books and health facilitators can be involved.
AGE: From the evidence available does the policy, procedure, proposal, strategy or service, affect, or have the potential to affect, age groups differently? Yes No
Explain your response: All groups are equally likely to require blood products and there is no discrimination on the basis of age. . Good explanation and guidance is included in the policy around the management of children of parents who are Jehovah’s Witnesses to ensure the safety of the child is paramount.
LESBIAN, GAY, BISEXUAL: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, lesbian, gay or bisexual groups differently? Yes No
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
6
Explain your response: All groups are equally likely to require blood products.
RELIGION/BELIEF:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, religious belief groups differently? Yes No
Explain your response:
The policy identifies contact numbers for advice for Jehovah’s witness patients who may decline blood components for religious belief.
Policy does state that consent must be obtained for all patients as any patient can refuse blood components if they have capacity.
The policy contains clear guidance for the management of children of parents who are Jehovah’s Witnesses to ensure the safety of the child is paramount.
CARERS: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, carers differently? Yes No
Explain your response: All groups are equally likely to require blood products. For parents who are Jehovah’s Witnesses and are carers for children there is clear guidance on the management of the child to ensure their safety and on communicating with and informing parents.
OTHER: EG Pregnant women, people in civil partnerships, human rights issues. From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect any other groups differently? Yes No
Explain your response: All groups are equally likely to require blood products.
4. Safeguarding Assessment - CHILDREN
a. Is there a direct or indirect impact upon children? Yes No
b. If yes please describe the nature and level of the impact (consideration to be given to all children; children in a specific group or area, or individual children. As well as consideration of impact now or in the future; competing / conflicting impact between different groups of children and young people:
Children receive blood components and Jehovah witness children may decline components in which case legal advice may be required to proceed.
c. If no please describe why there is considered to be no impact / significant impact on children
5. Relevant consultation
Having identified key groups, how have you consulted with them to find out their views and that the made sure that the policy, procedure, proposal, strategy or service will affect them in the way that you intend? Have you spoken to staff groups, charities, national organisations etc?
No
Blood Transfusion Policy December 2017 Version 6.2.3 Author: Transfusion Practitioner
7
6. Date completed: 16/2/17 Review Date: November 2018
7. Any actions identified: Have you identified any work which you will need to do in the
future to ensure that the document has no adverse impact? NO
Action Lead Date to be Achieved
8. Approval – At this point, you should forward the template to the Trust Equality and
Diversity Lead [email protected]
Approved by Trust Equality and Diversity Lead: Date: 8.3.18