Embed Size (px)
Citation preview

BLT/GUI/03210/CAN
1
BARTS AND THE LONDON NHS TRUST
GUIDELINES FOR THE USE AND MANAGEMENT OF IMPLANTABLE PORT CENTRAL VENOUS CATHETERS
TRUST CORE GUIDELINES
REVIEW April 2013 APPROVAL/ADOPTED Clinical Practice Validation Committee 20th
April 2010 DISTRIBUTION Policy Liaison Officers for distribution
All clinical wards and departments RELATED POLICIES Prevention of Infection And Management
Of Long-Term Central Venous Catheters and Ports (BLT/GUI/34510/IC) Policy No. 10 Standard Precautions including Hand Hygiene and Use of Protective Equipment and Management of Inoculation and Contamination Incidents. BLT/POL/25708/IC Prevention of Central Venous Catheter and Peripheral Cannula Related Infection. BLT/GUI/27008/IC Guidelines for the use and management of Cuffed Tunnelled Central Venous Catheter (CVC) (Hickman / Groshong lines) Guidelines for the use and management of Peripherally Inserted Central Venous Catheter (PICC) Policy for the Administration of Injectable Medicines in Clinical Areas BLT/POL/12709/PHA Policy for Consent for Examination and Treatment” BLT/POL/10910/HGC

BLT/GUI/03210/CAN
2
North East London Cancer Network Guidelines for the Safe Prescribing, Handling and Administration of Cytotoxic Drugs BLT/POL/13305/NQA
AUTHOR/FURTHER INFORMATION
Matthew Johnson, Consultant Nurse Chemotherapy 15-8605
THIS DOCUMENT REPLACES First version CONTENTS INTRODUCTION 3 Insertion of Implantable Ports 4 General care of implantable ports 7 Infection Prevention and Management 8 Inserting the Non-Coring Needle 9 Maintaining patency 10 Patient Education 12 Removal 12 Systemic infection 13 Local Infection 13 Catheter patency problems 14 Pain Swelling or leakage at port site 17 Pain or swelling in arm neck or shoulder 18 Palpitation / abnormal ECG 18 Acknowledgements 19 References 20 Apendixes 21
BLT/GUI/03210/CAN
3
INTRODUCTION/PURPOSE OF THE GUIDEINES 1. The term Central Venous Catheter (CVC) refers to an intravenous catheter whose internal tip
lies in a large central vein. There are various different types of CVC. These Guidelines relate to implantable ports. For other types of CVC refer to the relevant device Guideline. The Guidelines must be read in conjunction with the Trust Core Guidelines for the Prevention of Infection and Management of Long Term CVCs and Ports (BLT/GUI/34510/IC).
2. The aim of the guideline is to ensure that the implanted port is managed appropriately and risk
of infection relating to the CVC is minimised. The Guidelines are written to ensure compliance with the Department of Health “Saving Lives” programme and are compliant with epic2 Guidelines (Pratt et al 2007).
APPLICATION : TO WHOM THIS GUIDELINES APPLIES 3. These Guidelines must be adhered to by doctors and all intravenous (IV) accredited nursing
staff caring for a patient with an implanted port. These guidelines are also intended to be used by any staff who are caring for a patient who is contemplating having an implanted port to aid with patient decision making. The Guidelines apply to patients in all clinical areas of the Trust. Failure to comply with these guidelines will result in increased risk of complications and infection related to the CVC.
Implantable Ports: 4. Implantable Ports are similar to tunnelled lines but instead of protruding from the patient’s
chest, the catheter terminates in a self-sealing injection port which is implanted under the skin. There are therefore no external parts. The port is accessed through the skin using a dedicated non-coring needle (see diagram)
5. Some patients find an Implantable Port more discreet and less intrusive than a tunnelled CVC
(Camp-Sorrell 1992, 2004). Ports require less maintenance when not in use than other types of catheter. They may also offer a lower risk of infection (Krzywda, et al 1999).
6. Implantable Ports are suitable for patients who require long-term frequent and intermittent
venous access. Arguably they are less than ideal for long-running continuous infusions because of the risk of needle dislodgement (Camp-Sorrell 2004). The patient may return home with the port in situ, and therefore patient education regarding the recognition and reporting of complications is of great importance.

BLT/GUI/03210/CAN
4
7. Dual lumen devices are available. These are equipped with two access ports side-by-side which
can be accessed separately using two different needles. Each lumen provides independent access to the venous circulation, so that incompatible drugs/fluids may be administered simultaneously (RCN 2010).
8. Ports may also be used as an alternative to subcutaneous administration of long-term
maintenance therapies when the subcutaneous route has become unacceptable to the patient or unreliable – e.g. due to subcutaneous nodule formation.
9. Placement is not recommended in obese or cachexic patients, before or after chest irradiation,
or at mastectomy sites (Camp-Sorrell 2004). Insertion of implantable ports
10. Prior to placing an implantable Port under supervision a doctor must:
• Be competent in the insertion of Cuffed tunnelled CVCs • Hold a certificate to demonstrate training in the use and safety of medical x-rays (IR(M)ER
Ionising Radiation (Medical Uses) Exposure Regulations) • Be fully conversant with the Trust’s Central Venous Catheter Guidelines
11. Prior to placing an implantable port unsupervised a doctor must:
• Have placed at least 20 tunnelled CVCs successfully under close supervision by an experienced doctor and be deemed competent by that doctor.
• Have received training in the use of diathermy and surgical techniques for Port insertion as well as being trained in tunnelled CVC insertion
Diagram: Implantable Port

BLT/GUI/03210/CAN
5
12. Preparation for line insertion Prior to the procedure, the patient’s suitability must be assessed (Gabriel et al 2005) – • Whether an implantable Port is the best option for this patient:
o Could the treatment be given peripherally? o Will treatment be of short duration so manage with a non tunnelled CVC o Would a PICC be preferable?
• The patient’s anxiety levels: would they benefit from sedation prior to line insertion? • The patient’s vital signs and general status. If sepsis is present treatment should be
commenced prior to port placement. • The patient’s central venous catheter history including any problems, reasons for previous
line removal. • Any relevant past medical history, specifically taking note of any -
o History of thrombosis. An implantable port must not be attempted where there is an existing thrombosis in a vein. If the patient has experienced previous CVC-related thrombosis, anticoagulation should be considered for this patient. An examination of the central venous system by a radiologist may be needed if there are multiple venous thromboses and there is a risk of Superior Vena Cava (SVC) obstruction
o History of axillary lymph node clearance, lymphoedema, and/or axillary radiotherapy (eg for breast cancer. An implantable port should ideally not be placed on the side of the affected arm).
o Past (or present) fracture of clavicle could alter venous patency o Cellulitis near the insertion site o Allergies to any of the materials used in tunnelled CVC placement o Cardiac history. If the patient has unstable cardiac rhythms, X-Ray guidance will help
avoid causing further arrhythmias during insertion. If the patient has a mechanical heart valve the guidewire or line tip must not enter the heart during insertion
• The patient’s haematological profile: o FBC and coagulation screen must be done if there are reasons to think it will be
abnormal (eg haematological cancer, chemotherapy, warfarin) o Platelets: If the platelet count is below 50, give a dose of platelets prior to line insertion.
If platelet count has been falling, levels should be checked on the day of insertion o INR/ APTTR should ideally be 1.5 or below
• Patients on Warfarin should be carefully managed. Discussion with the patient’s medical team is essential, but management will usually entail: o Stopping Warfarin four days prior to insertion o Starting low-molecular weight heparin (LMWH eg Fragmin) three days prior to
insertion o Checking INR on the morning of line insertion. o Recommencing Warfarin (if prescribed) following successful line insertion. Patients on
LMWH will need to continue until target INR is reached. o For outpatients this will require careful coordination between the medical team,
anticoagulation clinic, community nurses and GP. The inpatient team requesting the CVC will be responsible for coordinating this care
• Patients on Heparin o If on a prophylactic dose of LMWH, there is no need to carry out a clotting screen. o If on a therapeutic dose of LMWH no clotting screen is necessary but the CVC should
be inserted 24 hours after the last dose, if given daily dose or after12 hours of a BD dose. If the patient is on IV heparin discuss management with patient’s medical team. This can be stopped 4 – 6 hours prior to CVC insertion.
BLT/GUI/03210/CAN
6
13. Consent Formal written consent for line insertion should be obtained. Please refer to Trust Core Policy “Policy for Consent for Examination and Treatment” BLT/POL/10910/HGC
14. Choice of line
The line with the smallest practical diameter should be chosen for insertion. This is to minimise the risk of venous thrombosis. It is usual to use a single lumen line for solid tumours (excepting germ cell) and dual lumen lines for haemato-oncology. The number of lumens should be appropriate to the patient’s clinical needs (Pratt et al 2007).
15. Line insertion
Implantable Port insertion must occur in an aseptic environment eg theatre suite or radiology suite. A ward area or on a patients bed is not acceptable
16. Vein selection and preparation
The Subclavian vein is first choice, Internal jugular vein second choice and femoral vein only if there are reasons to avoid the SVC (eg thrombosis). CVC infections are lowest in subclavian lines.
17. Asepsis
Lines must be inserted using optimum aseptic technique (Pratt et al 2007). Skin site must be cleaned with 2% chlorhexidine gluconate in 70% isopropyl alcohol prior to CVC insertion. Use an alcoholic povidone-iodine solution for patients with a history of chlorhexidine sensitivity.
18. Port site
The anterior chest wall is the preferred site for siting implantable ports which can be buried where there is sufficient overlying skin to minimise the chance of port erosion through the skin. The axilla should be avoided as the chance of infection is greatly enhanced.
19. Catheter tip It is recommended that x-ray fluoroscopy is used during insertion to optimise line tip position to the lower superior vena cava (SVC). The tip should lie parallel to the vein wall, reducing the risk of migration and also reducing the risk of damage to the vein walls, which might lead to an increased risk of thrombosis and vessel perforation. During insertion the line needs to be cut to the appropriate length to allow for tip position and tunnel length. If the patient experiences palpitations following line insertion there is a high probability that this is the result of atrial stimulation by the catheter and the line may need to be retracted by 1cm at a time until the palpitation ceases. ECG should be used to confirm this along with a chest x-ray (CXR) to confirm catheter tip position.
20. Flushing There should be a final flush of each lumen with 4mls Heparinised Saline (100 units/ml) and the gripper needle removed. If the port is to be used within 24 hours flush with 0.9% Sodium Chloride leaving the gripper needle in situ.
21. Imaging
This is rarely required post insertion as fluoroscopy will have confirmed line tip position. A CXR may be required if there is a suspected or increased risk of pneumothorax.

BLT/GUI/03210/CAN
7
22. Documentation The following must be clearly documented in the patient’s Health Care Record: • Name of Clinician inserting line • Where line was inserted • Date of insertion • Make, type and serial number of Line • Skin Prep used • Any complications or difficulties during insertion. • Final tip position • Amount of local anaesthetic administered • Amount of sedation medication administered • Line flush • Sutures used and if any removal is required • That the line is ready for use • Complete any audit documentation: database and audit card • Complete Insertion and Removal Device Record
General Care of implantable ports NB Always use aseptic non-touch technique when caring for the wound sites of an implanted port
23. Sutures: • To side of port: remove at 7-10 days (unless dissolvable) • Venepuncture site: Remove at 7 - 10 days (unless dissolvable) (Bishop et al 2007)
24. Frequency of needle change:
• If port in constant use for more than a week, change needle weekly using different puncture site.
25. Dressings • Non-accessed ports:
o No dressing or exit site care required (except immediately following insertion of the port when wound should be kept covered with a transparent dressing - with or without gauze - until stitches removed and wound healed.)
• Accessed ports:
o Pad needle with sterile gauze if necessary and cover with semi-permeable transparent IV dedicated dressing. Needle site should be visible for inspection.
o Tape tubing firmly to skin to prevent pulling on the needle. o Inspect needle entry site at least twice daily. o Advise patient to report any discomfort or swelling at the puncture site immediately.
26. Bathing, showering and swimming • Non-accessed ports:
o Patient may bath, shower or swim freely once wound has healed. • Accessed ports:
o Bathing: Patient should not submerge exit site in bathwater.
BLT/GUI/03210/CAN
8
o Showering: Patient may shower if needle site is completely covered with an occlusive dressing, taking care not to dislodge needle.
o Swimming: not allowed while needle is in situ.
27. General Points relating to implantable port care:
Action Rationale
Only access port using a dedicated non-coring needle with integral extension set with clamp / stopcock
Conventional needles will degrade the port diaphragm
Following insertion of the port there may be oedema and tenderness around the site. This may make accessing port painful and more difficult than usual.
Ideally port should be accessed while patient is in Theatres / Interventional Radiology if it is to be used immediately afterwards
If patient undergoes MRI scan, inform scanning personnel about the port
Nature of the port may impact scan or degrade the image
If patient requires defibrillation do not place paddles directly over the port
To reduce the risk of damage to Port and reduce risk of cardiac conduction related problems
The port should never be used for power-injection of contrast medium
This may cause the catheter to split
Infection Prevention and Management 28. Infection is the most common complication associated with all types of CVC’s and one of the
most serious.
• You must be familiar with the latest Trust Infection Control Policy Number 10 and Trust Guidelines for the Prevention of Infection and Management of Long Term CVCs and Ports when caring for patients with an implantable port.
• Decontaminate hands before and after each patient contact using correct hand hygiene procedure.
• Always use aseptic non-touch technique when accessing the implanted port.
• Inspect the skin around the port and needle exit site for signs of infection (at least once per shift if patient is in hospital with the port accessed, or whenever the port is used)
• Take action immediately if there are signs of CVC-related infection. These include:
o Tenderness, inflammation and or pain at port site o Clinical evidence of Systemic Inflammatory Response Syndrome criteria (SIRS)
- Temperature >38°C or <36°C - Heart Rate >90 bpm - Respiratory Rate >20 bpm - WCC >12 x 10*9/L or <4 x 10*9/L - Malaise
o Document all findings in the Health Care Record See section on managing complications

BLT/GUI/03210/CAN
9
Inserting the Non-coring Needle in order to access implantable ports
29. Which needle should be used?
• Style: For infusions, a 90o non-coring needle with extension set should be used. For boluses, blood-taking and flushing, a straight non-coring needle with extension set may be used instead if preferred.
• Gauge: A 20 or 22-gauge needle will suffice for most uses including blood administration and withdrawal.
• Length: Where a 90o needle is used, the length will depend on the amount of subcutaneous tissue between the skin surface and the port. The external part of the needle should not exert pressure on the skin but equally it should not stand too proud. Hint: a 1" needle is suitable for most adult patients. Deeper or more superficial ports will require longer or shorter needles.
30. Equipment • Clean plastic tray • Non-coring needle (Huber needle) (1 inch or 2 inch depending on patient size) • Gloves and apron • 2%Chlorhexidine in 70% Isopropyl Alcohol • 18 gauge needle (for drawing up sodium chloride) • 10 ml syringe • 10 ml 0.9% Sodium Chloride • Semi-permeable transparent dressing • 10cm x 10cm gauze • Bionector® • Appropriate IV administration set if required
31. Technique:
Action Rationale
Always use aseptic non-touch technique when accessing the port
To minimise the risk of contamination and line infection
Numb skin over the port if required using topical anaesthetic (before skin prep) or prescribed subcutaneous Lignocaine 1% (after skin prep).
Some patients find the process of accessing painful
Prepare skin over the port using 2% Chlorhexidine in 70% Isopropyl alcohol and using a 30-second back and forth friction rub. Allow to dry. Do not touch the proposed needle insertion site again except with totally sterile gloves
To reduce the chance of contamination of the line with the patient’s own skin flora
Prime needle and/or giving set with 0.9% sodium chloride
To reduce risk of air embolus

BLT/GUI/03210/CAN
10
Put on sterile gloves if you need to palpate the port (otherwise you can wear non-sterile gloves)
To ensure you are confident of its position
Hold port firmly (eg with thumb and two fingers) and stretch skin taut during insertion of the needle.
To prevent the port sliding out of the way of the needle and to reduce the risk of the port becoming dislodged within the subcutaneous pocket
Insert needle swiftly and firmly until it is felt to contact the back of the port
Reduces patient discomfort
Verify correct position by flushing with 10 mls 0.9% sodium chloride and checking for aspiration of blood
To ensure port correctly accessed
If there is any local discomfort and/ or oedema in the tissues around or over the port this may indicate incorrect position of the needle. In this case needle should be removed and a fresh attempt made. (You can use the same needle for up to 2 further attempts if it has not become contaminated or damaged.)
An incorrectly positioned needle will result in local infiltration of fluid around port site
If the port flushes easily without any local discomfort/oedema but there is no flashback of blood, this suggests that needle position is correct but that the catheter itself is not fully functional. See Managing Patency Problems
The CVC may be incorrectly positioned, or a fibrin sheath may be developing at the end of the line
Maintaining patency 32. Assessing Patency of implantable ports NB Always use aseptic non-touch technique when accessing the port
• Do not administer drugs fluids or chemotherapy unless the line is fully patent. By fully patent it is meant that: o There is flashback of blood o The line can be flushed easily
• If the port is not fully patent see Patency Problems. • Testing for patency:
o Test for flashback of blood before administering IV medication but note that you should not discard blood unnecessarily. To assess for flashback you can either:
- attach a syringe containing 10mls 0.9% sodium chloride to the giving set, flush 2mls into the line and then withdraw. As soon as you see a trace of blood in the catheter or syringe just flush the rest of the sodium chloride into the line.
- or use a gravity technique (ie with all clamps open briefly hold an attached infusion below the level of the patient’s heart until you see flashback of blood).

BLT/GUI/03210/CAN
11
33. Flushing implantable ports
NB Always use an aseptic non-touch technique when accessing the CVC
Action Rationale
Non-accessed ports:
• Flush at least every four weeks with 10mls 0.9% sodium chloride and lock with 4mls prescribed Heparinised Saline 100 U/ml.
Flushing with 10ml sodium chloride helps to clear the line of any debris. Locking the line with heparin helps to prevent intra-lumenal clots.
Accessed ports:
Wipe clean the needle-free bung (Bionector®) with Chlorhexidine 2% in 70% Isopropyl alcohol (eg Sanicloth 2% ®) and allow to dry for 30 seconds
Decontaminate the bung and reduce risk of introducing infection into the blood stream
Before flushing
If there are vasoactive drugs in the lumen, withdraw prior to flushing.
To avoid giving bolus of the drug.
Using a brisk push-pause technique flush with:
• 10 mls 0.9% sodium chloride between incompatible drugs / infusions or after blood sampling
If needle to be removed: lock with 4mls prescribed Heparinised Saline 100 U/ml
If needle to remain in situ: lock with a further 10mls 0.9% sodium chloride. Needle should be removed as soon as it is no longer required.
Heparin is not required if the line is being accessed at least daily.
34. Removing the Non-coring Needle from implantable ports
NB Always use an aseptic non-touch technique when removing the needle
Action Rationale
Lock port with 4mls prescribed Heparinised Saline 100 U/ml. Ideally, remove needle while injecting last ml but use gauze to prevent spray. (NB you will need to ask the patient or a third party to inject because you will need two hands for removing the needle. If this is not possible, you can achieve a positive pressure finish by clamping the infusion set while injecting the final ml of flush and then remove needle.)
To achieve positive pressure finish and prevent back-flow of blood into line
Stabilise the port with one hand during needle withdrawal. Take care to avoid a needle-stick injury
To avoid trauma to tissues

BLT/GUI/03210/CAN
12
Apply gentle pressure to needle site with sterile gauze until minor bleeding has ceased. A plaster may be applied if necessary / desired
There should only be minimal bleeding at site
Patient Education
35. If patient is discharged with port in situ:
• Make arrangements for the port to be flushed every 4 weeks if not in use. This is best done in the hospital setting, such as a day care unit.
• Patients may wish to learn to flush their own ports. Education should be given by nurses competent in this technique.
• Ensure patient has copy of relevant patient information leaflet
• Ensure patient is aware of care required
• Ensure patient is aware of the importance of reporting complications and has a contact number for this purpose (RCN 2010).
Removal 36. Implantable ports are usually removed in Theatres or Interventional Radiology.

BLT/GUI/03210/CAN
13
Managing Complications of implanted ports Systemic infection 37. Pyrexia plus or minus: rigor after flushing, sore throat, generally feeling unwell, hypotension,
tachycardia, shock, port pocket / tunnel infection (Krzywda 1999). • Possible cause:
o Catheter Related Blood Stream Infection
• Management:
Action Rationale • Urgently refer to medical staff. May be
treatable without catheter removal depending on patient’s clinical status and colonising organism. Microbiology opinion must be sought.
Early detection and management can reduce severity of infection
• Take line and peripheral blood cultures as per Trust guidelines.
Cultures taken from both line and peripheral stab can help to identify the source of infection
• TPR & BP. Frequency will depend on patient’s clinical status.
Monitor vital signs for possible deterioration
• If there are signs of port pocket site infection see below.
Local infection
38. Inflammation and tenderness at the needle exit site / port pocket plus or minus exudates
• Possible cause:
• Infection • Local skin irritation or sensitivity
• Management:
Action Rationale
• Take a swab To help identify organism if present
• Change dressing to alternative (or no dressing if implantable port not in use and insertion sutures removed), if irritation appears to be dressing related
Irritation maybe due to dressing
• Refer to medical staff. Microbiology opinion must be sought regarding which antibiotic line lock to use when appropriate. The CVC may need to be removed if unable to treat infection.
Infections involving the tunnel or the port pocket are very difficult to treat.

BLT/GUI/03210/CAN
14
• Increase frequency of dressing change & cleaning depending on amount of exudate.
To decrease microbial load at site of infection
• 4 hourly TPR & BP if patient in hospital To detect deterioration in condition
• If patient also shows signs of systemic infection, see above.
Catheter patency problems
39. The catheter is sluggish, or there is no flashback of blood, or there is complete blockage. • Possible causes:
• Clotted blood in catheter
• Fibrin sheath (which may be diagnosed using fluoroscopy)
• Malpositioned catheter
• Build up of lipids (eg Parenteral Nutrition)
• Drug Precipitation
• NB: In Implantable Ports needle may be incorrectly positioned: check before taking any other action
(RCN 2010, Baskin et al 2009, Camp Sorrell 2004).
Management No flashback of blood or catheter flow is sluggish
Action Rationale Ask the patient to take deep breaths and try different positions. Flush briskly using 10mls 0.9% sodium chloride. If this fails use a thrombolytic.
Deep breathing creates pressure changes in the chest and position changes will move the line position which may be sufficient to allow flash-back of blood.
If lipids/drug precipitation suspected consult pharmacy advice for suitable agent to dissolve occlusion.
Precipitated drugs can block catheters and can potentially be dissolved by altering the chemical environment of the drugs.
40. Catheter is completely blocked or sluggish line fails to respond
• Use a 3-way tap technique to instil thrombolytic into catheter. • What is a thrombolytic?
o A thrombolytic is a drug capable of breaking up a thrombus.
o Urokinase is a commonly used thrombolytic for unblocking CVCs. An alternative drug used is Alteplase (t-PA).
o A thrombolytic must always be prescribed.
o Heparin and Heparinised Saline are NOT thrombolytics: they are capable only of inhibiting thrombus formation.

BLT/GUI/03210/CAN
15
• When should you use a thrombolytic? Use a thrombolytic to improve patency in the following situations:
o flashback of blood is absent
o free-flow of fluids is sluggish or intermittent
o resistance is felt when flushing
o the catheter/lumen is completely blocked
41. How to use a thrombolytic (Baskins 2009, Mayo 1989)
Management: Action Rationale
Arrange prescription. (Caution if patient’s clotting is severely deranged or if high doses of an anticoagulant are being given concurrently.)
Thrombolytics are prescription only medications
Draw up the thrombolytic as per the Trust drug monograph
To ensure correct concentration and dose
Instil the thrombolytic into the catheter and wait for 20 to 60 minutes. Do NOT force the thrombolytic into the catheter if the lumen is completely blocked: see Using a Thrombolytic in a Completely Blocked Catheter (below).
Forcing the agent into the line risks fracturing the line or dislodging the port
Assess the catheter again. It is best to flush the catheter with 0.9% sodium chloride prior to attempting to obtain flashback, otherwise there is a risk of creating a further blockage in the line before you have cleared it.
There is no need to worry that you are flushing the thrombolytic into the patient: small doses can be flushed into the patient without danger unless the patient has exceptionally deranged clotting
If full function has not returned instil the thrombolytic again and leave in for longer – several hours or overnight if possible.
The fact that Urokinase has a half life of 20 minutes once it is in the patient’s system is irrelevant to how long it carries on working while still in the catheter. This explains why leaving it in longer is often more effective.
If the procedure fails to restore function consider whether lipids / drug precipitation could be causing a blockage. If not, refer to medical staff: a chest x-ray may reveal malposition of the line.

BLT/GUI/03210/CAN
16
42. Using a Thrombolytic in a Completely Blocked Catheter
Action Rationale
Attach 3-way-tap & syringe. (NB 3-way taps are now contraindicated for routine IV use but are still available for this procedure. Always use a 3-way tap without an extension set)
Diagram 1. • Three-way Tap Technique
Attempting to create a vacuum in the catheter will cause the thrombolytic drug to be pulled down further into the catheter, increasing the chance that it will come in contact with the clot blocking the line.
Open clamp (if there is one).
Open stopcock to the empty syringe and the blocked catheter.
Pull back on the plunger of the empty syringe. You will need to pull quite forcibly.
To create a vacuum in the empty syringe
Maintain suction with one hand and with the other hand turn stopcock so it is closed to the empty syringe and open to the syringe containing thrombolytic, which will be sucked into the catheter.
Opening the stopcock between the vacuum and the line creates vacuum in the line and draws in thrombolytic into the line. Don’t worry if it seems that very little thrombolytic is sucked in: even a tiny volume will reach several cm into the catheter.
Leave for several hours or overnight. Do not clamp catheter as this will prevent the thrombolytic from penetrating into the line.
BLT/GUI/03210/CAN
17
After this time, assess the catheter by attempting to flush the catheter using 0.9% sodium chloride in a 10ml syringe. Do not use excessive force.
It is best NOT to try aspirating before flushing at this stage as you may block the catheter again.
If the catheter is still completely blocked, repeat the procedure: this may need repeating up to three times before it works.
Sometimes leaving the thrombolytic in overnight seems to help. Don’t worry about overdosing the patient: if the catheter is blocked none of the drug will actually have been flushed into the blood stream.
Once the catheter can be flushed, and only then, check for flashback. If flashback is absent, administer thrombolytic as described.
Drawing back on the line first can cause further blockage
If the procedure fails despite three attempts, consult medical team with a view to removing the catheter
43. What if the thrombolytic fails to restore function? Management:
Action Rationale
If a thrombolytic used correctly fails to restore function, contact medical team. Consider the possibility of Pinch Off Syndrome (Bakins 2009)
A chest x-ray may need to be carried out to check the position of the line. If a chest x-ray shows that the catheter is correctly placed, it may be worth investigating further using fluoroscopy which may reveal a fibrin sheath
If the cause could be a build up of lipids from Parenteral Nutrition or drug precipitation consult pharmacy advice for a suitable agent to dissolve occlusion.
Thrombolytic drugs will be ineffective against drug precipitation
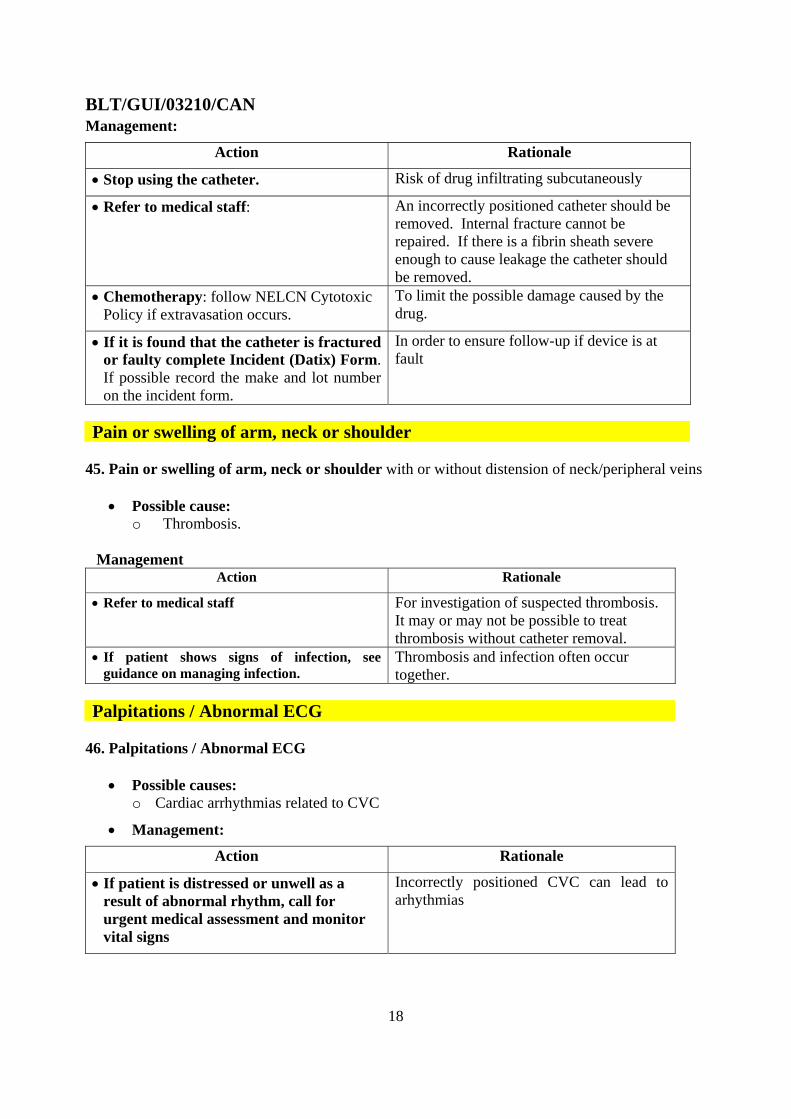
Pain, swelling or leakage at port site
44. Pain or visible swelling when port is used or fluid leaks from needle site when port is flushed.
• Possible causes:
NB: In Implantable Ports needle may be incorrectly positioned: check before taking any other action
o Malposition of catheter
o Internal catheter fracture
o Fibrin Sheath (which may be diagnosed using fluoroscopy)
o Separation of port and catheter
BLT/GUI/03210/CAN
18
Management:
Action Rationale
• Stop using the catheter. Risk of drug infiltrating subcutaneously
• Refer to medical staff:
An incorrectly positioned catheter should be removed. Internal fracture cannot be repaired. If there is a fibrin sheath severe enough to cause leakage the catheter should be removed.
• Chemotherapy: follow NELCN Cytotoxic Policy if extravasation occurs.
To limit the possible damage caused by the drug.
• If it is found that the catheter is fractured or faulty complete Incident (Datix) Form. If possible record the make and lot number on the incident form.
In order to ensure follow-up if device is at fault
Pain or swelling of arm, neck or shoulder
45. Pain or swelling of arm, neck or shoulder with or without distension of neck/peripheral veins
• Possible cause: o Thrombosis.
Management
Action Rationale
• Refer to medical staff
For investigation of suspected thrombosis. It may or may not be possible to treat thrombosis without catheter removal.
• If patient shows signs of infection, see guidance on managing infection.
Thrombosis and infection often occur together.
Palpitations / Abnormal ECG
46. Palpitations / Abnormal ECG
• Possible causes: o Cardiac arrhythmias related to CVC
• Management:
Action Rationale
• If patient is distressed or unwell as a result of abnormal rhythm, call for urgent medical assessment and monitor vital signs
Incorrectly positioned CVC can lead to arhythmias

BLT/GUI/03210/CAN
19
47. Cardiopulomonary symptoms These may include any of the following: respiratory distress / apnoea, reduced O2 saturation levels, tachycardia, bradycardia, hypotension, pallor, cyanosis, anxiety, chest pain, loss of consciousness • Possible causes:
o Pneumothorax o Air or catheter embolism o Pulmonary embolism o Cardiac tamponade / pericardial effusion
Management: Action Rationale
• Call for medical assistance / Critical Care Outreach Team / resuscitation team
Medical emergency
• Administer O2 First line drug in emergency situation
• Monitor vital signs As baseline and to monitor effects of any treatment.
Name of Author: Matthew Johnson Designation: Consultant Nurse (Chemotherapy) Date: May 2010

BLT/GUI/03210/CAN
20
References: Baskin, J., Pui, C., Reiss, U., Wilimas, J., Metzger, M., Ribeiro, R., Howard, S. (2009) Management of occultion and thrombosis associated with long-term indwelling central venous catheters. The Lancet 374 159-169 Bishop, L., Dougherty, L., Bodenham, A., Mansi, J., Crowe, P., Kibbler, C., Shannon, M., Treleaven, J. (2007) Guidelines on the insertion and management of central venous access devices in adults. International Journal of Laboratory Hematology 29, 261-278 Camp-Sorrell, D., (1992) Implantable Ports - Everything you Always Wanted to Know. Journal of Intravenous Nursing 15(5) 262 – 272 Camp Sorrell, D (2004) Access Device Guidelines, recommendations for nursing practice and education. 2nd Edition. Pittsburgh, Philadelphia: Oncology Nursing Society. Gabriel, J., Bravery, K., Dougherty, L., Malster, M., Scales, K. (2005) Vascular access: indications and implications for patient care. Nursing Standard 19, 26 45 - 52 Krzywda, E., Andris, D., Edmiston, C.,(1999). Catheter Infections: Diagnosis, Etiology, Treatment, and Prevention. Nutrition in Clinical Practice. 14(4) 178 - 90 Mayo, D., (1989) Administering Urokinase: Clearing the Way. Nursing98, 28(11) 50-52 Pratt, R., Pellowe, C., Wilson, J., Loveday, H., Harper, P., Jones, S., McDougall, C., Wilcox, M., (2007). epic2: National evidence based guidelines for preventing healthcare acquired infections in NHS hospitals in England. J Hosp Infection, 65S: S1-S64 Royal College of Nursing (RCN) (2010) Standards for Infusion Therapy. Third edition. London: RCN Publishing.

BLT/GUI/03210/CAN
21
Acknowledgement We are grateful for the considerable support that we have received from colleagues both within and from outside of Barts and the London NHS Trust. Some of those with substantial involvement in the development of this policy are listed below - . Liz Simcock Clinical Nurse Specialist for Venous Access University College London Hospitals NHS Foundation Trust who willingly shared the guidelines from UCLH upon which we based our own guidelines Dr Alastair Mulcahy Consultant Anaesthetist /Vascular Access Device Group BLT Aldine Thomas Clinical Nurse Specialist Cancer Services BLT Dr Aubrey Bristow Consultant Anaesthetist /Vascular Access Device Group BLT Claire Murrell Head of Nursing Cancer, I&I, Cutaneous BLT Daniel Lawrence Senior Charge Nurse Ward 7B BLT Eilidh Stewart Infection Control Nurse BLT Emma Riley Matron Cancer Services BLT Dr Ian Renfrew Lead Interventional Radiologist /Vascular Access Device Group BLT Ita O'Connor Lead Vascular Access Device Nurse BLT Mark Butler Clinical Nurse Specialist, Cystic Fibrosis, BLT Mary O'Leary Nutrition Clinical Nurse Specialist BLT Matthew Johnson Nurse Consultant (Chemotherapy) Dr. Michael Millar Consultant Microbiologist Chair of Vascular Access Device Group BLT Raquel Villanueva Senior Sister, Ward 7A BLT Rashida Jiva Tower Hamlets Adult Community IV Service Coordinator Stewart Elaine Clinical Nurse Specialist Cancer Services BLT

BLT/GUI/03210/CAN
22
Appendix 1: Patient information sheet about ports “Information: advice to patients who have an implantable port




![[Blt] 2014년 정부지원사업10월](https://img.pdfslide.net/doc/110x75/558e65901a28ab92218b458e/blt-2014-10.jpg)

![[BLT] 브랜드 네이밍 사례 - BLT 브랜드 네이밍 연구소 (엄정한 변리사)](https://img.pdfslide.net/doc/110x75/58a3fc3b1a28ab64528b57fd/blt-blt-.jpg)


![[BLT] 특허제도소개_김성현_20160824_v2](https://img.pdfslide.net/doc/110x75/589e54581a28ab1c7f8b6b49/blt-20160824v2.jpg)

![[Blt] 2014년 정부지원사업12월](https://img.pdfslide.net/doc/110x75/559cebdc1a28ab2b708b4788/blt-2014-12.jpg)

![[BLT] 특허권의내용과명세서의이해_김성현_20160824_v2](https://img.pdfslide.net/doc/110x75/58735df41a28abe7648b4f7b/blt-20160824v2-58bd808549376.jpg)



![[BLT] 창업과 지식재산](https://img.pdfslide.net/doc/110x75/5592e7321a28ab1f698b4701/blt-5592e7321a28ab1f698b4701.jpg)





![[Blt] 2014년 정부지원사업11월](https://img.pdfslide.net/doc/110x75/5592e5c81a28ab33698b4637/blt-2014-11.jpg)




![[BLT] 6HA 발명기법](https://img.pdfslide.net/doc/110x75/559af70b1a28ab8c458b45cf/blt-6ha--559c094e2d7ea.jpg)