Embed Size (px)
Citation preview

1
Blue Meadow Family Clinic
Case Study

2
short time ago, in land not far away…
BLUE MEADOW
FAMILY CARE

3
The Blue Meadow Team…

4
Next Step….
• Provider Enrollment• Sandee is your CPA
5
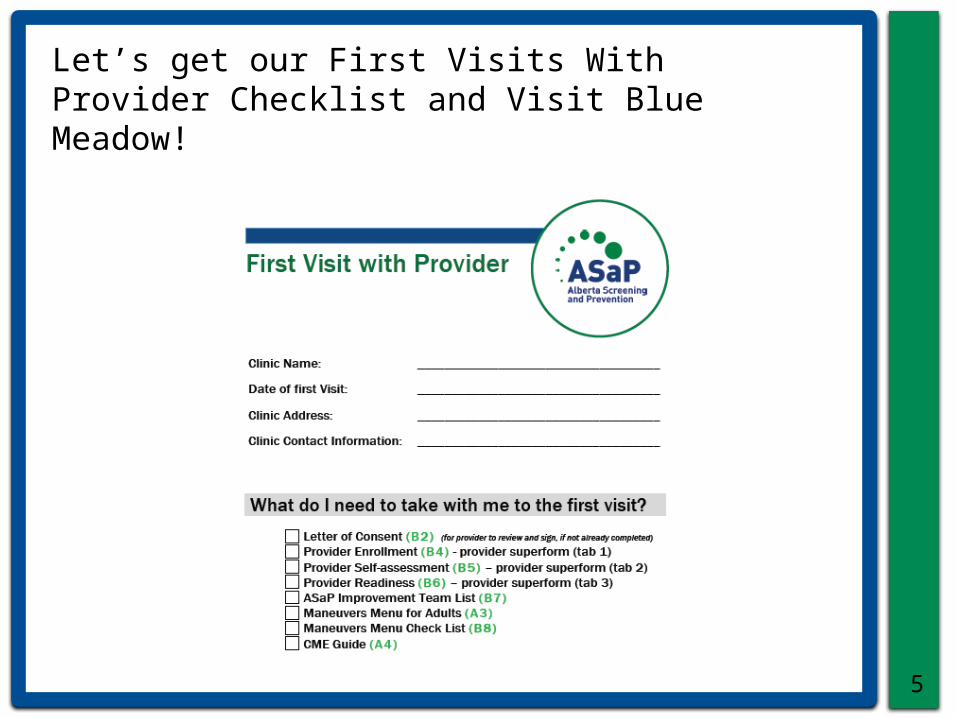
Let’s get our First Visits With Provider Checklist and Visit Blue Meadow!
6
BMFC Meeting #1…with Provider(s)
Dr. Doe (physician)
Dr. Green (physician)
Your Name Here (IF)

Enrolling Providers
• First we ensure the Letter of Consent is complete

Registering Drs. Doe & Green – The SuperForm
• For provider registration and chart review
• Complete one for each provider• Latest version available on TOP website• You can take a printed hard copy or
softcopy on laptop to your meeting to complete the form
• Let’s take a closer look at the form!

Provider SuperForm Highlights
• Must use Windows based PC• Must be using MS Excel 2003 or later• Macros must be enabled• You can only work in yellow fields• Saving: Macro-enabled format• Refer to video links on first tab of
SuperForm• More information in SuperForm User
Guide on TOP website

10
Blue Meadow Improvement Team

11
BMFC Meeting #2…with Improvement Team
Dr. Doe (physician)
Dr. Green (physician)
Doreen (receptionist)
Maureen (office
manager)Chris
(MOA)
• Panel Discussion• Maneuvers
Selections
Your Name Here (IF)
12
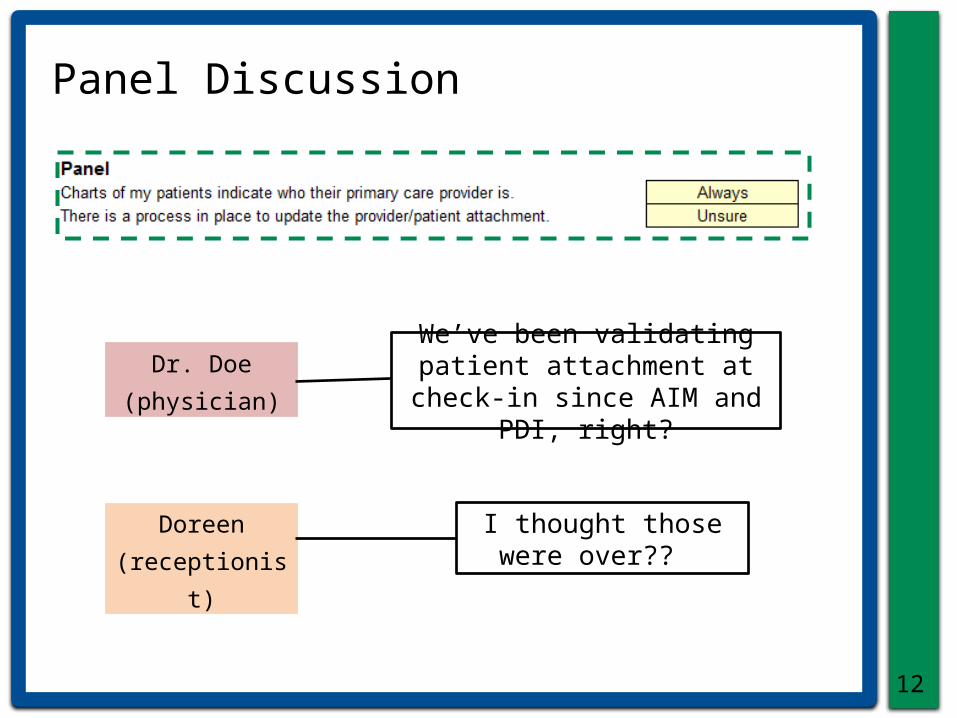
Panel Discussion
Dr. Doe (physician)
Doreen (receptionist)
We’ve been validating patient attachment at check-in since AIM
and PDI, right?
I thought those were over??

13
Panel Process Development Checklist

14
Panel Process Assessment Tool
15
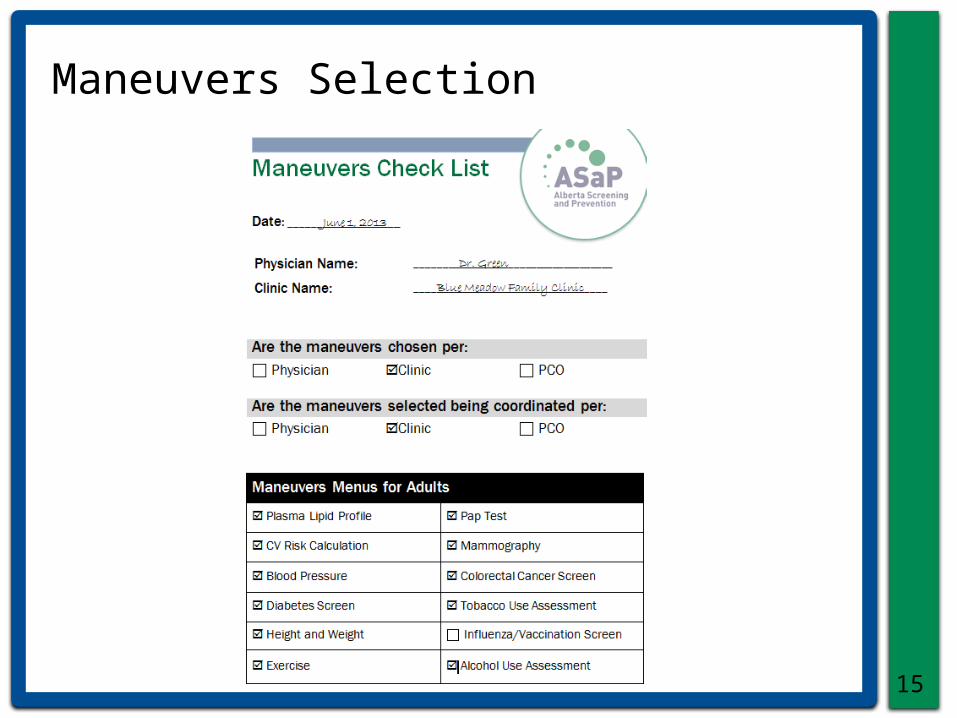
Maneuvers Selection

16
Screening Offers Documentation

17
BMFC Meeting #3
Dr. Doe (physician)
Dr. Green (physician)
Doreen (receptionist)
Maureen (office
manager)Chris
(MOA)
Your Name Here (IF)
• Current Screening Processes
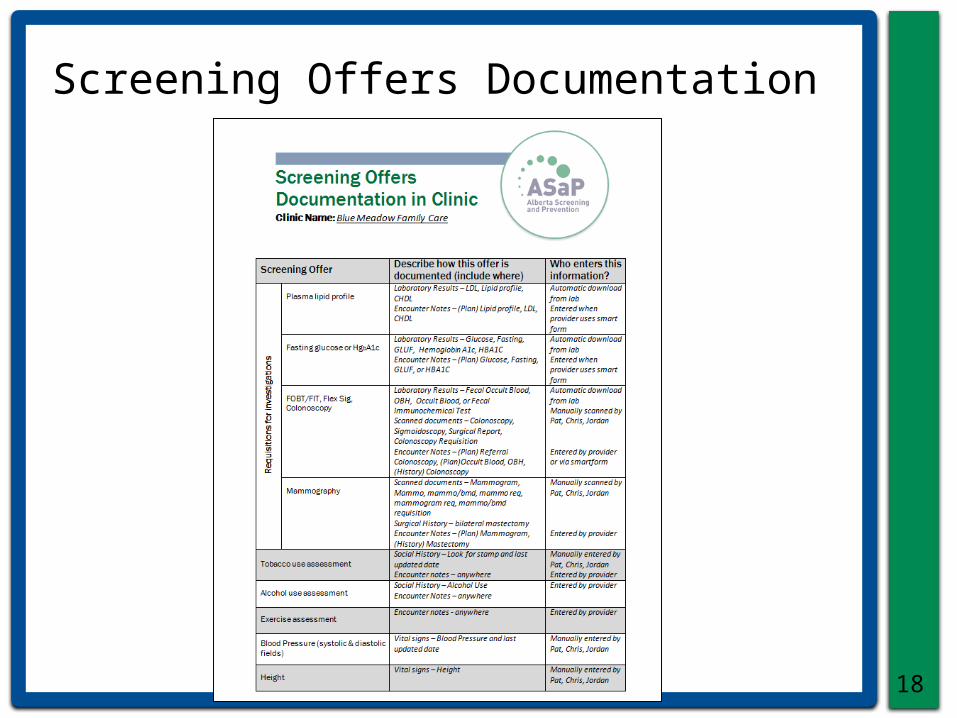
18
Screening Offers Documentation

19
Screening Discussion – Guided Interview
Dr. Doe (physician)
Dr. Green (physician)
Doreen (receptionist)
Maureen (office
manager)Chris
(MOA)
Your Name Here (IF)
In reality, I only screen patients when they book a
PHE. Otherwise, I generally don’t think of it
unless prompted…We have room for improvement - even some patients who are here frequently aren’t getting screened.
Sometimes I discuss screening with patients, but I don’t always chart
what I’ve offered – especially if they decline.

20
Map Current Screening Process
Patient greeted by reception
PHE?
Screening if patient
requests (physician)
MOA brings up
CPX template
MOA enters Ht/Wt
MOA measures
Ht/Wt
MOA rooms patient
Address confirmed
MOA leaves
Physician enters
Physician completes
CPX maneuvers
Completes exam, closes chart
No
Yes
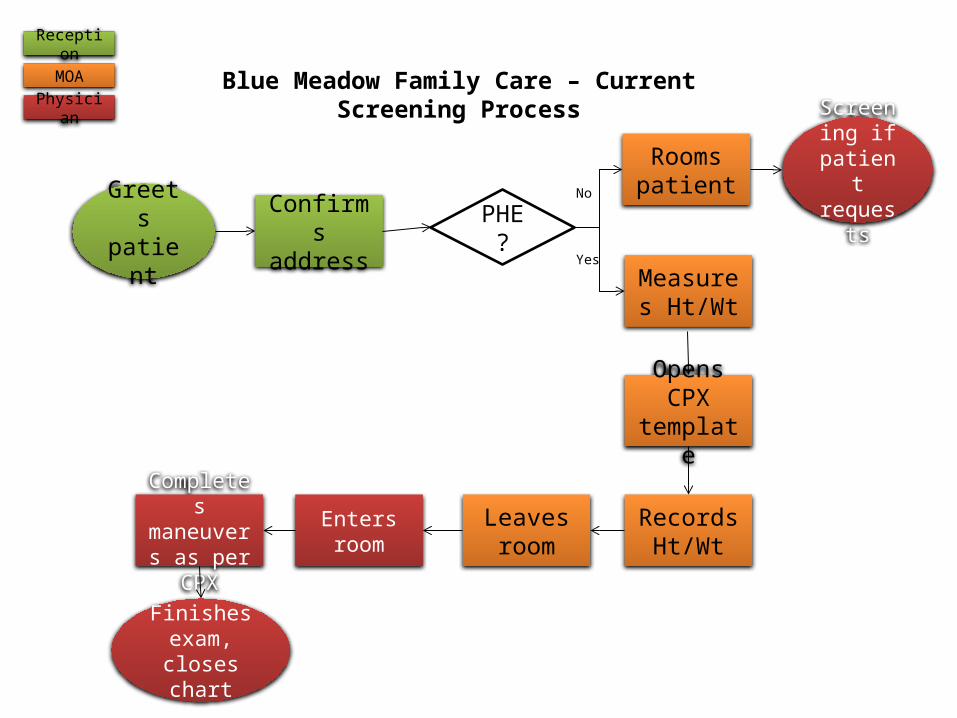
Blue Meadow Family Care – Current Screening Process
Greets patient
Confirms address
PHE?
Rooms patient
Screening if patient requests
Measures Ht/Wt
Opens CPX template
Records Ht/Wt
Leaves room
Enters roomCompletes maneuvers as per CPX
Finishes exam,
closes chart
No
Yes
Reception
MOA
Physician

22
Meeting #3 Discussion
Dr. Doe (physician)
Dr. Green (physician)
Doreen (receptionist)
Maureen (office
manager)Chris
(MOA)
Your Name Here (IF)
I tried running a report on height & weight and got low numbers of screens.
I’m not really sure where to chart height and weight. There’s more than one place where they can go.
I think I only see a height and weight on about ½ of
my patients - I end up doing it myself!

EMR “Intervention”
• BMFC sought out help from an experienced Wolf EMR user to observe how they were using Wolf for panel and screening processes to make recommendations for moving ahead with ASaP
• Experienced user observed Dr. Doe, Dr. Green and the care team working with them:– Receptionists– MOAs
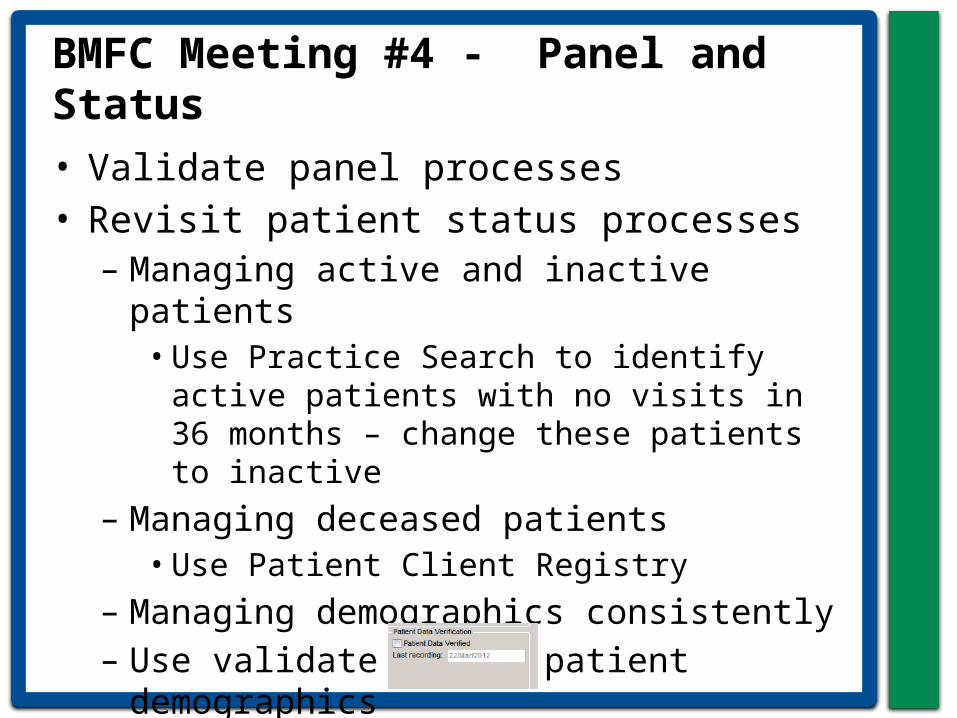
BMFC Meeting #4 - Panel and Status• Validate panel processes• Revisit patient status processes
– Managing active and inactive patients• Use Practice Search to identify active
patients with no visits in 36 months – change these patients to inactive
– Managing deceased patients• Use Patient Client Registry
– Managing demographics consistently– Use validate box in patient
demographics

Meeting #4 Continued - Screening Offers• Decide:
– How important are Run Charts on all offers?
• Stop: Documenting offers in Notes• Start: To use Templates or Manual Lab
Result to document offers that do not involve a lab requisition
• Agree on documentation outside of the Complete Physical eXam (CPX)

EMR Tips
• EMR and reliable processes need to work together– Ask: What work do we want to make the
EMR do?• Create processes for active, panelled
patients in the EMR– Manage demographics to contact the
patients– Processes to maintain patient status so
that Practice Search is accurate and reliable
• Document screening offers in Templates or Manual Lab Results
BMFC Meeting #5
27
Dr. Doe (physician)
Dr. Green (physician)
Doreen (receptionist)
Maureen (office
manager)Chris
(MOA)
• Applying QI ToolsYour Name Here (IF)
28
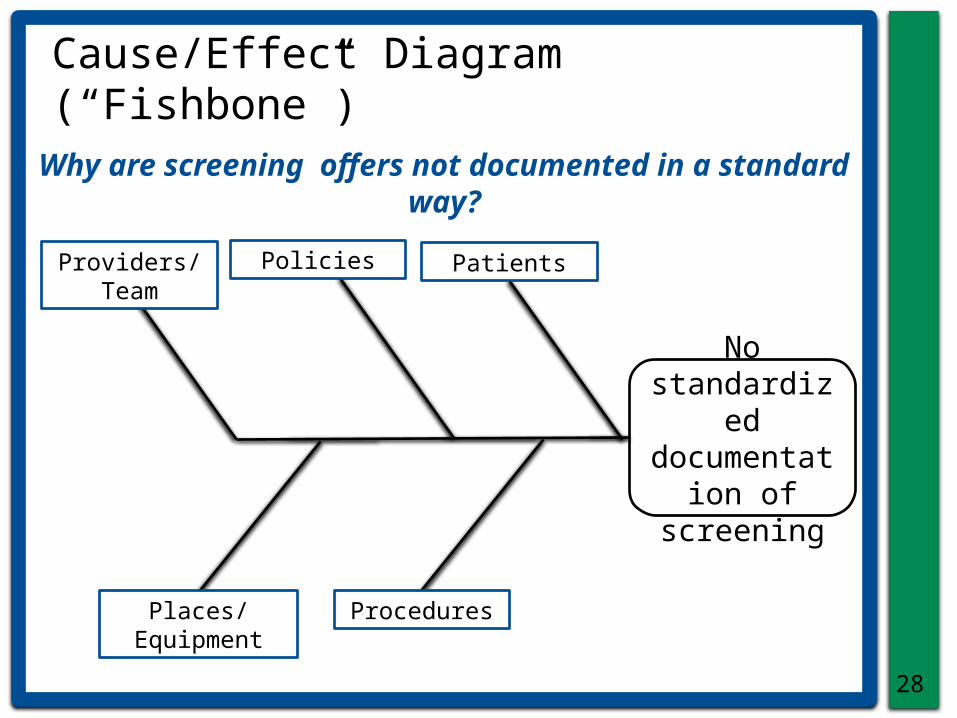
Why are screening offers not documented in a standard way?
No standardized
documentation of screening
Patients
Procedures
Providers/Team Policies
Places/Equipment
Cause/Effect Diagram (“Fishbone”)

29
MFI/PDSA • Read both sides of the BMFC plan

30
Future State Process Maps
• BMFC decided to adapt the sample processes you showed them for Opportunistic and Outreach Screening
• They understand that this is only a proposed process, and revisions will likely be made

Physician
Completes encounter
BMFC Future State Process (Opportunistic)
Escorts Patient to Exam Area
Mammogram Due?
• prints req for pt• enters in EMR
PAP Due? • offers • enters in EMR
MOA
Checks Reminders in Patient Chart
Colorectal Due?• provides FOBT kit &/OR makes colonoscopy referral, as needed• updates EMR
Greets patient
Validates in EMR:• Address/phone• Primary provider• Status (active)
Reception
Patient >18?
Checks Height & Weight
Rooms Patient• opens EMR chart
• enters Ht & Wt
BP Due?• check BP• enters in EMR
Exercise Due?• # minutes/week• enters in EMR
Tobacco Use Due?• check status• enters in EMR
Alcohol Use Due?• drinks/week• enters in EMR
Patient >40?
DM & Plasma Lipid Profile Due
• prints lab req and instructions
•enters in EMR
Patient >50?
Addresses primary reason
for visit
CV Risk Due? • enters values into Framingham Risk Calculator• enters in EMR
D5
D6
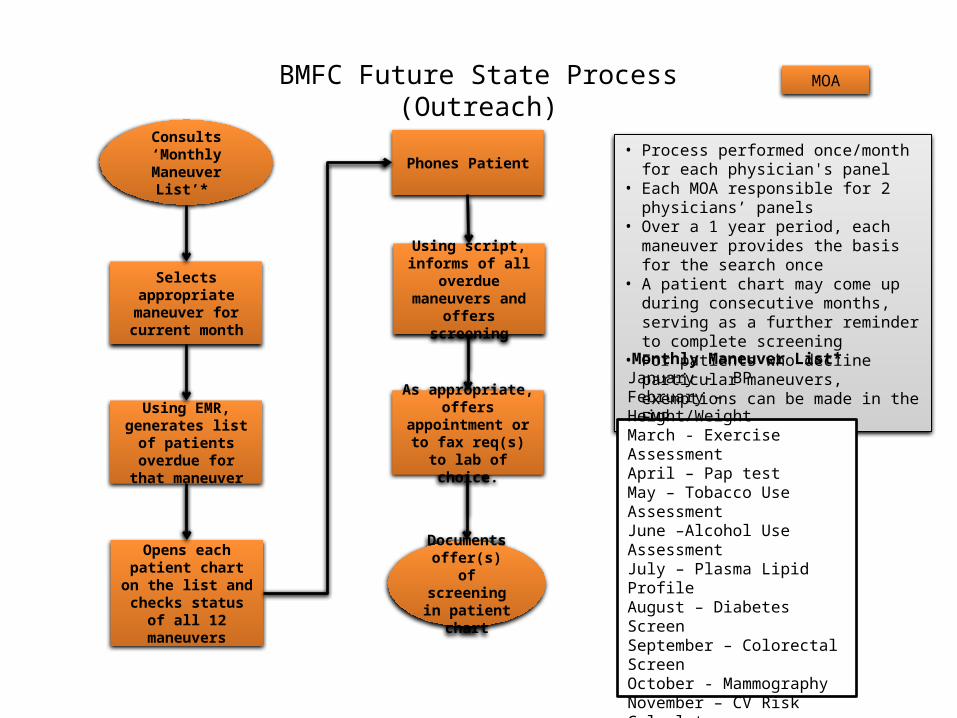
• Process performed once/month for each physician's panel
• Each MOA responsible for 2 physicians’ panels
• Over a 1 year period, each maneuver provides the basis for the search once
• A patient chart may come up during consecutive months, serving as a further reminder to complete screening
• For patients who decline particular maneuvers, exemptions can be made in the EMR
BMFC Future State Process (Outreach)
Consults ‘Monthly Maneuver
List’*
MOA
Opens each patient chart on
the list and checks status of all 12
maneuvers
Selects appropriate
maneuver for current month
Using EMR, generates list of patients overdue for that maneuver
Phones Patient
Using script, informs of all
overdue maneuvers and offers screening
As appropriate, offers
appointment or to fax req(s) to lab of
choice.
Documents offer(s) of
screening in patient chart
Monthly Maneuver List*January - BPFebruary – Height/WeightMarch - Exercise AssessmentApril – Pap testMay – Tobacco Use AssessmentJune –Alcohol Use AssessmentJuly – Plasma Lipid ProfileAugust – Diabetes ScreenSeptember – Colorectal ScreenOctober - MammographyNovember – CV Risk CalculatorDecember – Influenza Vaccine

ABC Clinic Improvement Board for “Topic”Names of People Working on this Improvement
What are we trying to accomplish?The NAME clinic will improve (increase/reduce) by 50% the percentage of our patients on 5 or more medications, seen weekly, who have been referred for a poly-pharmacy review for optimal care., by DATE 3 MONTHS FROM NOW, from current rate of x % to 1.5x %.
Provider/Staff
Procedures
Person/Patients
Policies
Place/Equipment
Effect
1 2 3 4 5 6 7 80
5
10
15
20
25
Series 1Target
What changes are we making that will lead to an improvement?
Patient Awareness :Placing posters in rooms promoting pharmacist reviews for patients on 5 or more medications.
Provider Reminders: Each day, attaching a pharmacist brochure to charts of patients on 5 or more medications who are scheduled.
What have we learned about the way we currently do things?
Insert ‘cause & effect diagram’ OR ‘process map’ OR ‘pareto diagram’ OR ‘5 whys’

EXTENDICARE FALCONBRIDGE- PUAP COLLABORATIVE WOUND WARRIORS TEAM CASE FOR ACTION
WHAT WE DID TEAM
RESULTS
Kim Lapierre, KinesiologistSylvie Clark RN ADOC
Angela Perreault PSW
Nicole Viel, DietitianStefanie Lavallee RN

36
Discussion & Questions




























