-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
1/11
Acupuncture point injection treatmentof primary dysmenorrhoea:a
randomised, double blind,
controlled studyC Wade,1,2 L Wang,3 W J Zhao,3 F Cardini,4 F
Kronenberg,1,5 S Q Gui,3 Z Ying,6
N Q Zhao,7 M T Chao,1,8 J Yu3
To cite:Wade C, Wang L,
Zhao WJ,et al. Acupuncture
point injection treatment of
primary dysmenorrhoea:
a randomised, double blind,
controlled study. BMJ Open
2016;6:e008166.doi:10.1136/bmjopen-2015-
008166
Prepublication history for
this paper is available online.
To view these files please
visit the journal online
(http://dx.doi.org/10.1136/
bmjopen-2015-008166 ).
Received 13 March 2015
Revised 25 November 2015
Accepted 26 November 2015
For numbered affiliations see
end of article.
Correspondence to
C Wade;
[email protected]
ABSTRACTObjective:To determine if injection of vitamin K3 inan
acupuncture point is optimal for the treatment ofprimary
dysmenorrhoea, when compared with 2 other
injection treatments.
Setting:A Menstrual Disorder Centre at a publichospital in
Shanghai, China.
Participants:Chinese women aged 1425 years withsevere primary
dysmenorrhoea for at least 6 monthsnot relieved by any other
treatment were recruited.
Exclusion criteria were the use of oral
contraceptives,intrauterine devices or anticoagulant drugs,
pregnancy,history of abdominal surgery, participation in other
therapies for pain and diagnosis of secondarydysmenorrhoea.
Eighty patients with primarydysmenorrhoea, as defined on a 4-grade
scale,
completed the study. Two patients withdrew
afterrandomisation.
Interventions:A double-blind, double-dummy,randomised controlled
trial compared vitamin K3acupuncture point injection to saline
acupuncture pointinjection and vitamin K3 deep muscle
injection.Patients in each group received 3 injections at a
single
treatment visit.
Primary and secondary outcome measures: Theprimary outcome was
the difference in subjectiveperception of pain as measured by an 11
unit Numeric
Rating Scale (NRS). Secondary measurements wereCox Pain
Intensity and Duration scales and theconsumption of analgesic
tablets before and after
treatment and during 6 following cycles.
Results:Patients in all 3 groups experienced painrelief from the
injection treatments. Differences in NRSmeasured mean pain scores
between the 2 active
control groups were less than 1 unit (0.71, CI1.37to0.05) and
not significant, but the differences inaverage scores between the
treatment hypothesised to
be optimal and both active control groups (1.11, CI0.45 to 1.78)
and (1.82, CI 1.45 to 2.49) werestatistically significant in
adjusted mixed-effects
models. Menstrual distress and use of analgesics werediminished
for 6 months post-treatment.
Conclusions:Acupuncture point injection of vitaminK3 relieves
menstrual pain rapidly and is a useful
treatment in an urban outpatient clinic.
Trial registration number: NCT00104546;Results.
INTRODUCTIONDysmenorrhoea is highly prevalent and amajor cause
of activity restriction and school
absence among young women worldwide.1 2
Primary dysmenorrhoea is a painful men-strual cramping of the
uterus without identi-able organic pathology that affects as manyas
85% of women, 20% of whom describetheir pain as severe.3 4 The
initial onset ofprimary dysmenorrhoea is usually shortlyafter
menarche, 612 months after ovulatorycycles begin. High levels of
uterine prosta-glandins, a hormone associated with uterinecramping,
abdominal pain and contractionof muscular tissue, have been
identied as asubstantial contributing factor to the pain
Strengths and limitations of this study
The results of this trial document the efficacy ofa treatment in
use for over 40 years at a high-volume Menstrual Disorder Centre
and provide
important information about a treatment for acommon condition of
women worldwide.
The design is rigorous: a double-blind, double-
dummy, randomised controlled trial powered tocompare three
active treatments.
The primary outcome effect size of the differencebetween groups
is robust.
Owing to funding limitations, the study wasimplemented in two
phases under two differentrandomisation schemes and data from the
first
phase were analysed prior to the implementationof the second
phase.
Stratified analyses were conducted to account for
any differences between the results of the twophases of the
trial.
Wade C,et al.BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166 1
Open Access Research
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://dx.doi.org/10.1136/bmjopen-2015-008166http://dx.doi.org/10.1136/bmjopen-2015-008166http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://crossmark.crossref.org/dialog/?doi=10.1136/bmjopen-2015-008166&domain=pdf&date_stamp=2016-01-05http://dx.doi.org/10.1136/bmjopen-2015-008166http://dx.doi.org/10.1136/bmjopen-2015-008166
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
2/11
and distress that are the major symptoms of dysmenor-rhoea.5 6
The pain duration is commonly 872 h and isusually associated with
the onset of menstrual ow.1
The condition often results in activity restriction over13 days
of each menstrual cycle,3 and therefore theannual costs in terms of
disability, in addition to treat-ment, are high.
The two most common treatments in the USA for dys-
menorrhoea are non-steroidal anti-inammatory drugs(NSAIDs) and
oral contraceptives (OCs).7 NSAIDs areeffective for some but not
all women, with a failure rateof up to 25%.8 Both treatments
require multiple or dailydosing and have side effects. In China,
common treat-ments for dysmenorrhoea include acupuncture andherbal
preparations, with increased use of NSAIDs inrecent years; OCs are
seldom prescribed for thecondition.
Injection of an agent, usually a herbal extract or drug,into an
acupuncture pointisan innovation in TraditionalChinese Medicine
(TCM)6 9 and has been used in China
over the past 40 years.
10
Classical and modern acupunc-ture usually involves needles
inserted at multiple pointsand left in place for 2060 min. In
contrast, acupuncturepoint injection is easily administered and
standardised,and requires less time at the clinical
encounter.11
Acupuncture point injection of vitamin K3 has beenused as a
standard of care treatment for dysmenorrhoeaat the Menstrual
Disorder Centre at the Obstetrics andGynecology Hospital in
Shanghai, Peoples Republic ofChina, since at least 1985,12 and
several uncontrolledstudies of the treatment have been conducted
inChinaand Italy with various forms of vitamin K.1315 Whilevitamin
K3 has been administered consistently at the
clinic where this study was conducted,16 this form ofvitamin K
is not typically used in the USA and Europe.Vitamin K1, however, is
routinely administered to new-borns shortly after birth to augment
coagulation and isconsidered to be safe. A pilot study of the
acupuncturepoint injection treatment with a cross-over design
substi-tuted vitamin K1 for vitamin K3 and explored
theacceptability of the treatment in the USA and theabsorption of
vitamin K1.17 18
While the positive results of these prior studies arepromising,
it was unknown whether vitamin K as anagent and the acupuncture
point as the site of injection
were essential to the treatments effect and whether
together they were an optimal treatment for pain reliefof
primary dysmenorrhoea as compared with otherinjection treatments.
To address this question, theprimary objective of this study was to
compare: (1) theeffects of vitamin K injection in a
non-acupuncturepoint, (2) the effects of injection of a non-active
sub-stance in the acupuncture point, and (3) the combinedeffects of
vitamin K injected in the acupuncture point.In addition, we sought
to evaluate whether the treat-ments, given only once, relieve
menstrual pain at avariety of time points; and to evaluate the
feasibility ofconducting an international randomised trial with
a
comparative effectiveness design. Our secondary out-comes were
whether the treatments administered in asingle cycle had a
carryover effect and decreased men-strual pain, distress and the
need for medications oversix cycles.
MATERIALS AND METHODS
Written informed consent was obtained from youngwomen, and
assent and parental consent from girls andtheir families. The study
was conducted in accordancewith the requirements of Good Clinical
Practice.We conducted a double-blind, double-dummy, rando-mised
controlled trial with three parallel groups:
Group A saline acupuncture point injection: Study partici-pants
randomised to this group received normal salineinjection at the San
Yin Jiao or Spleen 6 (SP6) acu-puncture point (both legs) and
saline in the rightbuttock. This served as an active control for
vitamin K.Group B vitamin K deep muscle injection: Study
partici-
pants randomised to this group received a vitamin K3injection in
the right buttock and saline at a non-acupuncture point near but
not SP6 (both legs). Theclinicians located the sham point at 1 cm
above Sp6,1 cm towards the back of the leg from Sp6, and
pene-trated the needle 1 cm beneath the skin. This served asan
active control for the acupuncture point injectionsite and ensured
that the patients in this group hadthe same dose of vitamin K3 as
group C, albeit at a dif-ferent injection site.Group C vitamin K
acupuncture point injection: Study parti-cipants randomised to this
group received a vitamin K3injection at the SP6 point (both legs)
and saline in the
right buttock. A third injection of saline in the buttockwas
administered to maintain uniformity of treatmentwith groups A and
B.
The treatments were administered only once.The alternative
hypothesis to all treatments having
similar effects on pain of primary dysmenorrhoea is thatpain
relief in group Cthe treatment most closelyaligned with TCM theory
and clinical innovations at theMenstrual Disorder Centrewas optimal
compared withthe other two treatments.
Young Chinese women aged 1425 years with severeprimary
dysmenorrhoea for at least 6 months that had
not been relieved, or only partially relieved, by any
othertreatment were recruited for this study. A four-gradescale
which grades dysmenorrhoea as absent, mild, mod-erate or severe
based on the presence of cramps,whether or not the cramps were very
painful or causedpatients to sometimes or always cut back on
activities,19
was used to screen prospective participants to
determineeligibility. Young women enrolled in the study were
nul-liparous, Mandarin or Shanghainese speaking, withregular
menstrual cycles for the past 6 months, and whohad a working
phone.
Exclusion criteria were diagnosis of secondary dysmen-orrhoea,
the use of OCs, intrauterine devices or
2 Wade C,et al. BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166
Open Access
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
3/11
anticoagulant drugs, pregnancy, history of abdominalsurgery,
participation in other therapies for acute orchronic pain and
diagnosis of dysmenorrhoea due toany recognised cause, such as
pelvic inammatorydisease. In addition, women who had had previous
injec-tion treatment with vitamin K in SP6 for any reason orwho
were intolerant to NSAIDs or who planned to beout of the area
during the course of the 7-month study
were excluded.Study participants were recruited from patients
who
presented with pelvic pain at the Menstrual DisorderCentre at
the Obstetrics and Gynecology Hospital,Fudan University, in
Shanghai, China. Information ses-sions were conducted at Fudan
University to let youngwomen and providers know about the study at
the clinic.Study physicians and staff screened prospective womenand
girls for eligibility and interest, described the studydetails and
obtained consent. For women under the ageof 18, parental consent
was also obtained. Diagnosis ofprimary dysmenorrhoea was conrmed by
the study phy-
sicians on the basis of history and physical
examination.Prospective participants who were not currently in
painsigned consent forms and were told to return at theonset of
their next painful menstrual cycle. Participantscould also consent
and receive the treatment on theirinitial visit if they were
currently in pain due to menses.Participants were informed that
they could withdrawfrom the study at any time.
Treatments were administered only once by medicaldoctors who
were also experienced acupuncturists. Painmeasurement was conducted
by clinic staff and not thestudy physicians. Participants were
followed for 6 monthswith follow-up phone interviews by clinic
staff.
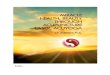
Treatment consisted of an injection at each of three sitesas per
group assignment. A single injection of vitaminK3 is 4 mg/mL, so
since participants were injected oncein each leg, the total dose
was 8 mg of vitamin K3 or2 mL of saline solution. The SP6
acupuncture point islocated on the lower leg, 3 cun or four widths
of themiddle phalange of the index nger on the patient,proximal to
the peak of the medial malleolus, just alongthe posterior aspect of
the tibial bone. The muscleinjected was m. soleus (see gure 1). An
injection of8 mg of vitamin K3 or 2 mL saline (depending on
thegroup) was administered as a deep intramuscular injec-
tion in the glutaeal muscle of the right buttock. NSAIDswere
available in case any patient was not satised withpain relief from
the treatment after 1 h.
Vitamin K3 was used because it is and has been theagent used in
the Menstrual Disorder Centre at theObstetrics and Gynecology
Hospital for treatment ofprimary dysmenorrhoea. Vitamin K3 ampoules
were pre-pared by the Shanghai #1 Biochemical andPharmaceutical
Company, Ltd. The investigators visitedthe company in January 2004
to specify a design forblinding (packaging, coding and labelling)
of theampoules. Vitamin K3 and saline ampoules looked iden-tical.
The injection site was specied on the ampoules.
The randomisation list was created by a biostatistician,who went
to the certied research pharmacy, whichencapsulated the agents to
blind the treatment and thensent the ampoules to the research site.
Eligible consent-
ing participants were assigned to a group at the treat-ment
visit according to a randomly permuted blockdesign with blocks of
size 6 to ensure equal allocation ofpatients to each treatment
group. The randomisationscheme was generated and held by the
studybiostatisticians.
Physicians were blinded as to saline and vitamin K3,but they
knew whether they were injecting into the acu-puncture point or
near the acupuncture point. Thus,study physicians knew when they
were administering togroup B, but they could not differentiate the
treatmentsin groups A and C. Patients presumably did not know
the difference between the acupuncture point and nearthe
acupuncture point and were blinded as to the agentin all three
groups. Evaluators (study staff collectingpain measures and other
study data) did not know thegroup assignment of participants.
Baseline data were collected following consent andprior to
treatment. The primary outcome, change inpain intensity at 0 and 60
min, was recorded on an11-unit Numeric Rating Scale (NRS) from 0 to
10 with 0being no pain and 10 being the worst pain the partici-pant
could imagine. Pain scores were obtained at base-line and at 2, 5,
30 and 60 min post-injection. Asecondary outcome was the
consumption of analgesic
Figure 1 In two of the groups injections were in the Spleen
6 (SP6)/San Yin Jiao (SYJ) acupuncture point near the ankle
on both legs. In the third group the injection site was near
but
not on SP6.
Wade C,et al. BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166 3
Open Access
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
4/11
tablets during the menstrual cycle before and after theinjection
treatment. Menstrual-related symptoms, suchas hours in bed and time
lost from school or work, wererecorded at baseline and after
treatment. Participantsmenstrual distress was evaluated after each
menstrualcycle on two different scales: Cox RetrospectiveSymptom
Scale (over 6 cycles) and Moos MenstrualDistress Questionnaire
(MMDQ) (over 2 cycles).20 21
The Cox scale included 17 symptoms commonly asso-ciated with
menstrual distress. Each of these was rated bythe participant on
both intensity and duration with arange from 0 (not perceptible) to
4 (extremely upset-ting). The MMDQ assessed six symptoms: muscle
stiff-ness, headache, cramps, backache, fatigue and generalaches
and painseach on a range of 0 (not present) to4 (severe). A
questionnaire to assess patients expect-ation about group
assignment and attitude towards par-ticipation in the research
study was also administered.
The trial was conducted in two phases. The rst phasewas
conducted as an exploratory pilot with 12 partici-
pants randomised to each of the three groups. Theresults of the
pilot were positive, with the effect size forgroup C exceeding the
hypothesised clinical effect whencompared with the other groups.
For the second phase,the investigators conducted a power
calculation basedon the effect sizes of the primary outcome from
thepilot phase. Using a Bonferroni correction for multipletesting,
we estimated that with 26 patients in each group,we could detect
change in mean pain scores of 2 unitswith SDs of 2.0 between groups
at =0.05 and 95%power. A stratied analysis was planned to
accommodatethe two phases of the randomised study.
Continuous variables were summarised by descriptive
statistics: mean, SD, median and range. Categorical vari-ables
were summarised in terms of frequencies and per-centages and groups
were tested to see if they differedon population characteristics.
Initially, results from thetwo phases of the trial were tested in
stratied analyses,however, the results were parallel and
homogeneouswith no signicant difference between the stratied
andunstratied results, so the data were then combined inthe
analysis for reporting. Treatment differencesbetween the three
groups were compared both inmarginal-effect and mixed-effect models
using Stata V.11(College Station, Texas, USA). A linear
mixed-effects
model was applied for the primary outcome, where painscores at
time 0 (baseline) and 60 min were the tworesponse variables (per
participant), each of which hadits own interceptor representing the
average pain levelat that time point.22 23 The observed covariates
weretreatment modalities and each individual was assignedwith an
unobserved random effect. The treatment effectis the difference at
the 60 min time point between thetwo arms under consideration.
Signicance levels wereobtained and adjusted for multiple
comparisons usingScheffe and Tukey-Kramer methods.22 Analysis of
vari-ance (ANOVA) was used to compare mean differencesboth (1)
BETWEEN and (2) WITHIN groups on the
secondary outcomes of the Cox and MMDQ scores forcycles 1 and 2
and also for cycles 1 and 7.
RESULTSBaseline dataThe study initiated in October 2004 and
ended in June2010. Phase I was completed in 2 years as it was
National
Institutes of Health (NIH) funded and physicians hadrelease time
to conduct the study: phase II took fouradditional years to
complete. Young Chinese women pre-senting with severe pelvic pain
to an urban hospitalclinic who were willing to be randomised to
active treat-ments were screened for eligibility and signed
consentforms. The parents of girls under 18 also consented tohave
their children participate. Of the 124 womenscreened, 82 enrolled
in the study and were randomised,80 of whom completed all study
visits (see gure 2). Twowomen withdrew after they signed consent
forms andwere randomised, because they or their parents changed
their minds about participation in a research study. Thebaseline
demographic characteristics and menstrualcycle proles of the women
did not differ between thethree groups (seetable 1).
Reduction of pain: When treated with an acupuncturepoint
injection of vitamin K3 in SP6 (group C), partici-pants had an
average 6.6 point decrease in pain on theNRS ( from 8.0 to 1.5,
p
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
5/11
not observed between groups (cycles 1 and 2 and cycles1 and 7)
on the Cox Duration and Intensity measures. Asignicant difference
however ( p
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
6/11
indicated that they did not know which treatment theyreceived
(68.8% and 57.5%) and the majority of theremainder thought they had
received injection at thetrue acupuncture point (30.0%) as well as
vitamin K3(36.3%). Only a small proportion thought they hadreceived
a control treatment: 1.3% thought they hadreceived an injection
near the acupuncture point and6.3% thought they had received
saline. These resultssuggest that the blinding procedures were
effective.
DISCUSSIONAll three active treatments reduced menstrual cycle
painrapidly (within an hour) with minimal side effects, but
acupuncture point injection with vitamin K3 in SP6 wasfound to
be optimal, producing a greater clinical andstatistically signicant
reduction in pain. One to twounits on the NRS for pain has been
described as clinic-ally signicant by studies designed to evaluate
unitscores with clinical improvement.24 25 Acupuncturepoint
injection with vitamin K3 provided rapid relief ofsevere as well as
moderate pain due to dysmenorrhoea.Effective treatment can be
administered in a high-volume hospital clinic and may be especially
useful towomen whose pain is unmitigated by other methods. No
differences between groups were found on long-termeffects, but
at the end of the study, participants in allactive treatment groups
endured signicantly less painover a reduced duration and reported
fewer activityrestrictions, fewer hours in bed and the consumption
offewer drugs for menstrual pain over the course of sixcycles than
at baseline, indicating the value of injectiontreatments for
primary dysmenorrhoea. All three treat-ments reduced pain rapidly
during the treatment cycle,yet the treatment in standard use at the
clinic, injectionof vitamin K3 in SP6, was clearly more effective
than theother two treatments on the primary short-termoutcome.
The pattern of reduction of menstrual distress overthe follow-up
cycles is consistent. Women in all of thetreatment groups
experienced long-term relief.Differences between the three groups
on the secondarylong-term outcomes of menstrual distress were not
sig-nicant. Patterns of analgesic use may interact withscores of
menstrual distress. In this study, group B, forexample, consumed
more analgesics than the other twogroups. Future research should
take this into accountwhen building analytic models. The
sensitivity of theCox and MMDQ scales over the long follow-up
period is
Figure 3 Pain intensity at
baseline and in the first hour after
treatment (SP6, Spleen 6).
Table 2 Pain intensity at baseline and in the first hour after
treatment
Overall model F-value=14.47 (p
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
7/11
unknown. Both instruments were administered with theidea of
validating results from one to the other anddetermining the best
instrument for future research.The MMDQ scale may be more sensitive
than the Coxscale for long-term follow-up assessment.
The overall reduction of menstrual distress and thedecrease in
the need for analgesics across groups duringthe follow-up period is
notable. Whether these effectsare due to the treatment or to the
natural course of dys-menorrhoea over 6 months is unknown, but
meritsfurther study. Differences between the effects of thethree
treatments on menstrual distress in subsequentcycles were more
variable than the short-term painoutcome and may be obscured by the
use of pain medi-cations and other home remedies which
participantswere free to employ during the long follow-up
period.
The three-arm study was designed to control for mul-tiple effect
pathways, and therefore the results supportthe injection site (an
acupuncture point) as a crucial
aspect of optimal pain relief. Little information existsabout
any specic mechanism of acupunctures effect onmenstrual pain, and
while acupunctures interruption ofpain pathways has been
investigated since 1979,26 muchremains unknown about the cause and
magnitude of theeffects of acupuncture, as placebo-controlled
trials ofmanual treatments are difcult to evaluate. Many studiesof
acupuncture do not nd signicant difference ofeffects for off-point
and on-point stimulation with acu-puncture needles.27 28 Point
injection may have differenteffects than classical acupuncture, and
measurement ofoutcomes may not have been sensitive enough in
someprevious studies to determine optimal effects.29 Benetsof
acupuncture point injection may include rapid andsubstantial pain
relief and prolonged effects across avariety of pain
conditions.3032 The three injection treat-ments administered in
this study worked rapidly,perhapsquicker than NSAIDs, which
optimises at 12 h,33 34 andour study indicates that the treatment
may have long-term
Table 3 Menstrual distress before and after injection treatment
and during follow-up cycles
Cox duration* Cox intensity* MMDQ*
Daily activity
restriction
Increased
hours in bed
Study period Mean Mean Mean Per cent Mean SD
Baseline cycle 1
Group A (control for vitamin K) 1.42 1.19 1.20 96.30 6.52
3.95
Group B (control for point location) 1.40 1.18 1.38 100.00 6.67
4.26
Group C (standard) 1.29 1.18 1.34 100.00 7.58 5.38Treatment
cycle 2
Group A (control for vitamin K) 0.84 0.68 0.69 59.26 3.60
1.35
Group B (control for point location) 0.93 0.68 0.82 74.07 5.40
2.80
Group C (standard) 0.83 0.69 0.69 61.54 4.57 1.81
Cycle 3
Group A (control for vitamin K) 0.85 0.66 n/a 65.38 4.33
1.30
Group B (control for point location) 0.93 0.76 n/a 62.96 5.00
1.85
Group C (standard) 0.73 0.57 n/a 50.00 5.13 2.47
Cycle 4
Group A (control for vitamin K) 0.90 0.65 n/a 42.31 7.50
5.73
Group B (control for point location) 0.82 0.67 n/a 55.56 5.00
1.61
Group C (standard) 0.76 0.64 n/a 46.15 5.11 1.76
Cycle 5
Group A (control for vitamin K) 0.77 0.52 n/a 42.31 7.67
5.99Group B (control for point location) 0.78 0.66 n/a 55.56 5.11
1.76
Group C (standard) 0.76 0.57 n/a 57.69 3.60 0.52
Cycle 6
Group A (control for vitamin K) 0.84 0.66 n/a 61.54 8.14
3.18
Group B (control for point location) 0.93 0.77 n/a 66.67 5.45
1.81
Group C (standard) 0.87 0.63 n/a 57.69 4.91 1.38
Cycle 7
Group A (control for vitamin K) 0.79 0.60 n/a 57.69 4.89
2.03
Group B (control for point location) 0.98 0.78 n/a 59.26 5.25
1.82
Group C (standard) 0.77 0.61 n/a 50.00 5.50 2.39
*Although all three groups experienced reduction in menstrual
distress on the Cox and MMDQ scales between baseline and cycle 2
andbetween baseline and cycle 7, the only significant difference in
group means was on the MMDQ scale between baseline and cycle
2.Standard treatment at the Menstrual Disorders Centre, Obstetrics
and Gynecology Hospital, Shanghai.Significant difference (p
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
8/11
effects on menstrual distress of up to 6 months. An effectof up
to 3months has been observed in at least one previ-ous study.14
Although this treatment cannot be self-
administered, it does not require dosing prior to theonset of
worst symptoms, as NSAIDs do, and nor does itrequire daily dosing
as OCs do.
Our results also indicate that vitamin K3 may havesome role in
amelioration of menstrual pain, althoughthe mechanism is as yet
unclear, as none of the forms ofvitamin K are known to have
analgesic effects. At leastone form of vitamin K is absorbed
through this treat-ment: increased concentrations of vitamin K1
(phyllo-quinone) following injection at SP6 were observed in astudy
of four participants with primary dysmenor-rhoea.18 Analysis of
plasma phylloquinone indicatednon-detectable concentrations before
acupuncture point
injection with vitamin K1, which increased up to425 nmol/L, 2048
h following injection. The vitamin Kprole of women with menstrual
cycle disorders may beworth exploring in a nutritional approach to
dysmenor-rhoea prevention.
The use of vitamin K3 (menadione) for this treatmentis routine
at the Menstrual Disorder Centre at theObstetricsand Gynecology
Hospital where this study wasconducted.1 4 1 6 Studies in the USA
and Europe havetested alternate forms of vitamin K. Vitamin K1
(phyl-loquinone) and K4 (menaquinone-4) were chosen overvitamin K3
because of availability in the clinical setting
and becausevitamin K1 has a better safety prole thanvitamin
K3.35 These studies also found that menstrualpain and distress were
relieved.14 15 17 Little is knownabout vitamin Ks role in
ameliorating symptoms of dys-menorrhoea or difference in effect in
the administrationof the various forms of vitamin K. NSAIDs
alleviate thepain of menstrual cramps through their effect on
prosta-glandin levels. One study that measured prostaglandinlevels
after acupuncture using the point SP6 did notnd that the treatment
reduced them.6 To the bestof our knowledge, studies of vitamin K
and prostaglan-din levels have not been reported. However, vitamin
Kis being explored for its potential role in reducing
proinammatory cytokines.36 Vitamin K is typically usedclinically
to abet blood clotting and, recently, has beenstudied in relation
to bone health. Animal studies haveshown that ovary concentrations
of vitamin K are higherthan in other organs,37 and researchers have
suggestedthat vitamin K may play a role in
reproductiveendocrinology.38
Our overarching goal was to create a research agenda
leading to a larger comparative effectiveness study con-ducted
by international collaborators in three countries,and the study
reported here was conceived as necessarypreliminary research to an
international trial of acupunc-ture point injection of vitamin K in
SP6 vs NSAIDs, whichwould be executed in the three countries where
pilotresearch had been successfully conducted. Studies inEurope,
North America and Asia have indicated that thistreatment reduces
menstrual pain in young women withprimary dysmenorrhoea, in a
variety of outpatient set-tings in diverse cultures. The results of
these studies as agroup indicate that various forms of vitamin K
(K1, K4
and K3) can produce pain relief when utilised with acu-puncture
point injection and have also indicated that thetreatment is
adaptable to various clinical settings (publichealth clinics,
private practice, hospital outpatient facil-ities) and acceptable
to young women in North Americaand Europe, as well as in China.1417
The study reportedhereisone of two known randomised studies of the
treat-ment17 and has the largest sample size and most
rigorousdesign of all known studies on the treatment.
Resultsreported here also suggest that both the agent and site
ofinjection inuence the effect size of the short-term painreduction
measures.
Study limitationsThe study setting may limit generalising the
results.Expectation by Chinese women that acupuncture willprovide
pain relief may have inuenced reports of painreduction. However,
this limitation is mitigated by theresearch efforts of
international collaborators who haveimplemented the clinical
protocol in a variety of coun-tries and settings. The hypothesised
optimal treatmentin this study has been tested on Chinese, American
andItalian women with primary dysmenorrhoea and hasreduced
menstrual pain in young women in publichealth clinics, private
practice and hospitals.14 15 17 The
study was implemented in two phases under two differ-ent
randomisation schemes and data from the rstphase were analysed
prior to the implementation of thesecond phase of the study.
Initially, the study team com-pleted a pilot study of 36 patients
and analysed the data.Since the hypothesised results were positive
and theeffect size was robust, the study was powered and datawere
collected for another 44 patients for more stableresults. We
performed analysis stratied by the twophases and found no signicant
differences in results byphase, which supports our methodological
approach ofanalysing and reporting the combined results.
Menstrualdistress scores on two different scales were compared
Table 4 Analgesic tablet consumption at baseline and six
follow-up cycles
Group B
Group A
(Control for
vitamin K)
(Control for
point
location)
Group C
(Standard)
Mean (SD) Mean (SD) Mean (SD)
Baseline 0.93 0.82 0.82 0.56 0.89 0.77Cycle 2 0.22 0.42 0.41
0.57 0.27 0.45
Cycle 3 0.11 0.32 0.33 0.48 0.35 0.49
Cycle 4 0.22 0.42 0.41 0.5 0.27 0.45
Cycle 5 0.22 0.42 0.48 0.5 0.35 0.49
Cycle 6 0.33 0.48 0.48 0.58 0.23 0.43
Cycle 7 0.22 0.42 0.33 0.48 0.23 0.43
8 Wade C,et al. BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166
Open Access
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
9/11
with Student t tests and not in an adjusted model formultiple
comparisons.
The study took over 6 years to complete in a very busyoutpatient
clinic. Recruitment during the second phaseof the study became ever
more challenging. Whereasthe rst phase received external funding,
in the secondphase the funding was greatly reduced, limiting
therelease time of the study physicians and making the
6 months of follow-up data collection difcult.Scheduling
difculties also affected recruitment, as it isimportant for
participants to be treated within 2 days ofonset of menses and at
the height of their pain.However, this was not always possible, and
this limitedparticipation in the study.
CONCLUSIONOur study reports the effect of acupuncture point
injec-tion of vitamin K3 on the pain of dysmenorrhoea inyoung
Chinese women. It extends the work of previoussingle-arm and
cross-over studies through the implemen-
tation of a randomised parallel group design, and pro-vides
substantial evidence that the treatment providespain relief for
women with painful periods who have notbeen able to obtain
satisfactory relief by any othermethod. Study results also indicate
that the site of injec-tion and the specic agent of vitamin K,
specicallyvitamin K3, are crucial to the optimal treatment of
paindue to primary dysmenorrhoea.
Author affiliations1Richard & Hinda Rosenthal Center for
Complementary and Alternative
Medicine Research, College of Physicians and Surgeons, Columbia
University,
New York, New York, USA2
Institute of East West Medicine, New York, New York,
USA3Obstetrics and Gynecology Hospital, Fudan University, Shanghai,
Shanghai,
China4Agenzia Sanitaria e Sociale Regionale dellEmilia Romagna,
(Healthcare and
Social Agency of Emilia Romagna Region), Viale Aldo Moro, 21,
40127
Bologna, Italy5Department of Anesthesiology, Pain and
Perioperative Medicine, Stanford
University School of Medicine, Palo Alto, California,
USA6Department of Statistics, Columbia University, New York, New
York, USA7Department of Statistics, School of Public Health, Fudan
University,
Shanghai, Shanghai, China8Osher Center for Integrative Medicine,
University of California at
San Francisco, San Francisco, California, USA
Contributors CW contributed to the study design, project
management, data
analysis and interpretation, and wrote the first draft of the
manuscript. LW,WJZ and SQG contributed to the study design and
procedures, data
acquisition and quality, study administration and interpretation
of results. FC
contributed to the study design and interpretation of results.
FK obtained the
study funding and participated in the administration and data
acquisition. ZY
was responsible for the power calculation, statistical analysis
and
interpretation and data monitoring. NQZ was responsible for
the
randomisation, blinding, statistical analysis and interpretation
and data
monitoring. MTC performed the statistical analysis and
interpretation. JY
developed the treatment protocol and provided the pilot
data.
Funding Funding was provided by an NIH/NCCAM Planning Grant
for
International Research on Chinese Medicine and Womens Health
(R21-AT01957), the Obstetrics and Gynecology Hospital, Shanghai,
China and
the Institute of East/West Medicine, New York, New York, USA.
Additional
funding was received through NIH/NCCAM (K01AT006545).
Disclaimer The contents of this paper are solely the
responsibility of the
authors and do not necessarily represent the official views of
the NIH or
NCCAM or other funders.
Competing interests None declared.
Ethics approval Columbia University Medical Center IRB, New
York, USA:
Obstetrics and Gynecology Hospital Medical Ethics Board,
Shanghai, China.
Provenance and peer review Not commissioned; externally peer
reviewed.
Data sharing statement No additional data are available.
Open Access This is an Open Access article distributed in
accordance with
the Creative Commons Attribution Non Commercial (CC BY-NC 4.0)
license,
which permits others to distribute, remix, adapt, build upon
this work non-
commercially, and license their derivative works on different
terms, provided
the original work is properly cited and the use is
non-commercial. See: http://
creativecommons.org/licenses/by-nc/4.0/
REFERENCES1. Harlow SD, Park M. A longitudinal study of risk
factors for the
occurrence, duration and severity of menstrual cramps in a
cohort ofcollege women. Br J Obstet Gynaecol 1996;103:113442.
2. Klein JR, Litt IF. Epidemiology of adolescent
dysmenorrhea.Pediatrics 1981;68:6614.
3. Dawood MY. Dysmenorrhea.Clin Obstet Gynecol1990;33:16878.
4. Latthe PM, Champaneria R, Khan KS. Dysmenorrhoea.BMJ
ClinEvid2011;2011:pii: 0813.5. Marjoribanks J, Proctor ML, Farquhar
C. Nonsteroidal anti-inflammatory
drugs for primary dysmenorrhoea.Cochrane Database Syst
Rev2003;(4):CD001751.
6. Shi GX, Liu CZ, Zhu J,et al. Effects of acupuncture at
Sanyinjiao(SP6) on prostaglandin levels in primary dysmenorrhea
patients. ClinJ Pain 2011;27:25861.
7. Davis AR, Westhoff CL. Primary dysmenorrhea in adolescent
girlsand treatment with oral contraceptives.J Pediatr Adolesc
Gynecol2001;14:38.
8. Dawood MY. Ibuprofen and dysmenorrhea.Am J
Med1984;77:8794.
9. Liu CZ, Xie JP, Wang LP,et al. Immediate analgesia effect of
singlepoint acupuncture in primary dysmenorrhea: a randomized
controlledtrial. Pain Med 2011;12:3007.
10. Chen CH. Acupuncture: a comprehensive text, Shanghai college
oftraditional medicine. Shanghai: Eastland Press, 1981.
11. Strudwick MW, Hinks RC, Choy STB. Point injection as
analternative acupuncture techniquean exploratory study ofresponses
in healthy subjects. Acupunct Med 2007;25:16674.
12. Yu J. Clinical and experimental study of dysfunctional
dysmenorrheatreated by Vit K.New Drugs Clin Rem 1985;5:146.
13. Zhao WJ, Weng JE, Yu J. Clinical study of vitamin K3
acupointinjection in treating pelvic pain. Chinese acupuncture
& moxibustion2000;20:3934.
14. Wang L, Cardini F, Zhao W,et al. Vitamin K acupuncture
pointinjection for severe primary dysmenorrhea: an international
pilotstudy.Med Gen Med 2004;6:45.
15. Lesi G, Gramenzi A, Gammi L,et al. Vitamin K injection in
San YinJiao acupoint (SP6) to treat severe primary dysmenorrhoea:
resultsof a pilot study. Eur J Integr Med 2012;4:S51.
16. Zhao WJ, Wang L, Weng JE,et al. Clinical study of vitamin
K3acupoint injection in treating pelvic pain.Chin J Integr
Med2003;9:1368.
17. Chao M, Wade C, Abercombie P, et al. An innovative
acupuncturetreatment for primary dysmenorrhea: a randomized,
crossover pilotstudy.Altern Ther 2014;20:4552.
18. Chao M, Wade C, Booth SL. Plasma phylloquinone
concentrationsincrease following acupoint injection for primary
dysmenorrhea.J Acupunct Meridian Stud 2014;7:1514.
19. Robinson JC, Plichta S, Weisman CS,et al. Dysmenorrhea and
useof oral contraceptives in adolescent women attending a
familyplanning clinic.Am J Obstet Gynecol 1992;166:57883.
20. Cox DJ. Menstrual symptom questionnaire: further
psychometricevaluation. Behav Res Ther 1977;15:5068.
21. Moos RH. The development of a menstrual distress
questionnaire.Psychosom Med 1968;30:85367.
22. Scheffe H.The analysis of variance. New York: Wiley,
1959.23. Fitzmaurice GM, Laird NM, Ware JH.Applied longitudinal
analysis.
New York: Wiley, 2004.24. Todd KH. Clinical versus statistical
significance in the assessment of
pain relief. Ann Emerg Med 1996;27:43941.
Wade C,et al. BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166 9
Open Access
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://creativecommons.org/licenses/by-nc/4.0/http://creativecommons.org/licenses/by-nc/4.0/http://dx.doi.org/10.1111/j.1471-0528.1996.tb09597.xhttp://dx.doi.org/10.1097/00003081-199003000-00023http://dx.doi.org/10.1097/AJP.0b013e3181fb27aehttp://dx.doi.org/10.1097/AJP.0b013e3181fb27aehttp://dx.doi.org/10.1016/S1083-3188(00)00076-0http://dx.doi.org/10.1016/S0002-9343(84)80025-Xhttp://dx.doi.org/10.1111/j.1526-4637.2010.01017.xhttp://dx.doi.org/10.1136/aim.25.4.166http://dx.doi.org/10.1002/jgm.511http://dx.doi.org/10.1007/BF02838571http://dx.doi.org/10.1016/j.jams.2014.01.004http://dx.doi.org/10.1016/0002-9378(92)91676-2http://dx.doi.org/10.1016/0005-7967(77)90009-2http://dx.doi.org/10.1097/00006842-196811000-00006http://dx.doi.org/10.1016/S0196-0644(96)70226-3http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/http://dx.doi.org/10.1016/S0196-0644(96)70226-3http://dx.doi.org/10.1097/00006842-196811000-00006http://dx.doi.org/10.1016/0005-7967(77)90009-2http://dx.doi.org/10.1016/0002-9378(92)91676-2http://dx.doi.org/10.1016/j.jams.2014.01.004http://dx.doi.org/10.1007/BF02838571http://dx.doi.org/10.1002/jgm.511http://dx.doi.org/10.1136/aim.25.4.166http://dx.doi.org/10.1111/j.1526-4637.2010.01017.xhttp://dx.doi.org/10.1016/S0002-9343(84)80025-Xhttp://dx.doi.org/10.1016/S1083-3188(00)00076-0http://dx.doi.org/10.1097/AJP.0b013e3181fb27aehttp://dx.doi.org/10.1097/AJP.0b013e3181fb27aehttp://dx.doi.org/10.1097/00003081-199003000-00023http://dx.doi.org/10.1111/j.1471-0528.1996.tb09597.xhttp://creativecommons.org/licenses/by-nc/4.0/http://creativecommons.org/licenses/by-nc/4.0/
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
10/11
25. Farrar JT, Young JP Jr, LaMoreaux L, et al. Clinical
importance ofchanges in chronic pain intensity measured on an
11-pointnumerical pain rating scale. Pain 2001;94:14958.
26. Pomeranz B, Cheng R. Suppression of noxious responses
insingle neurons of cat spinal cord by electroacupuncture and
itsreversal by the opiate antagonist naloxone. Exp
Neurol1979;64:32741.
27. McManus CA, Schnyer RN, Kong J,et al. Sham
acupuncturedevicespractical advice for researchers.Acupunct
Med2007;25:3640.
28. Park J, Linde K, Manheimer E,et al. The status and future
of
acupuncture clinical research. J Altern Complement
Med2008;14:87181.29. Vickers AJ, Cronin AM, Maschino AC,et al.
Acupuncture for chronic
pain: individual patient data meta-analysis.Arch Intern
Med2012;172:144453.
30. Kwon YB, Kang MS, Kim HW, et al. Antinociceptive effects of
beevenom acupuncture (apipuncture) in rodent animal models:
acomparative study of acupoint versus non-acupoint
stimulation.Acupunct Electrother Res 2001;26:5968.
31. Lee MS, Pittler MH, Shin BC,et al. Bee venom acupuncture
formusculoskeletal pain: a review. J Pain 2008;9:28997.
32. Park JM, Park SU, Jung WS,et al. Carthami-Semen
acupuncturepoint injection for chronic daily headache: a pilot,
randomised,double-blind, controlled trial.Complement Ther Med
2011;19(Suppl1):S1925.
33. Marjoribanks J, Proctor M, Farquhar C,et al.
Nonsteroidalanti-inflammatory drugs for dysmenorrhoea. Cochrane
DatabaseSyst Rev 2010;(1):CD001751.
34. Milsom I, Minic M, Dawood MY,et al. Comparison of the
efficacyand safety of nonprescription doses of naproxen and
naproxensodium with ibuprofen, acetaminophen, and placebo in the
treatmentof primary dysmenorrhea: a pooled analysis of five
studies. Clin
Ther 2002;24:1384
400.35. Bennett MI, Smith BH, Torrance N,et al. The S-LANSS
score foridentifying pain of predominantly neuropathic origin:
validation foruse in clinical and postal research. J Pain
2005;6:14958.
36. Booth SL. Roles for vitamin K beyond coagulation.Annu Rev
Nutr2009;29:89110.
37. Huber AM, Davidson K, OBrien-Morse ME,et al.
Tissuephylloquinone and menaquinones in rats are affected by age
andgender. J Nutr 1999;129:103944.
38. Truong JT, Booth SL. Emerging issues in vitamin K research.J
EvidBased Complement Altern Med 2011;16:739.
10 Wade C,et al. BMJ Open2016;6:e008166.
doi:10.1136/bmjopen-2015-008166
Open Access
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://dx.doi.org/10.1016/S0304-3959(01)00349-9http://dx.doi.org/10.1016/0014-4886(79)90273-5http://dx.doi.org/10.1136/aim.25.1-2.36http://dx.doi.org/10.1089/acm.2008.SAR-4http://dx.doi.org/10.1001/archinternmed.2012.3654http://dx.doi.org/10.1016/j.jpain.2007.11.012http://dx.doi.org/10.1016/j.ctim.2010.09.004http://dx.doi.org/10.1002/14651858.CD001751.pub2http://dx.doi.org/10.1002/14651858.CD001751.pub2http://dx.doi.org/10.1016/S0149-2918(02)80043-1http://dx.doi.org/10.1016/S0149-2918(02)80043-1http://dx.doi.org/10.1016/j.jpain.2004.11.007http://dx.doi.org/10.1146/annurev-nutr-080508-141217http://dx.doi.org/10.1177/1533210110392953http://dx.doi.org/10.1177/1533210110392953http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/http://dx.doi.org/10.1177/1533210110392953http://dx.doi.org/10.1177/1533210110392953http://dx.doi.org/10.1146/annurev-nutr-080508-141217http://dx.doi.org/10.1016/j.jpain.2004.11.007http://dx.doi.org/10.1016/S0149-2918(02)80043-1http://dx.doi.org/10.1016/S0149-2918(02)80043-1http://dx.doi.org/10.1002/14651858.CD001751.pub2http://dx.doi.org/10.1002/14651858.CD001751.pub2http://dx.doi.org/10.1016/j.ctim.2010.09.004http://dx.doi.org/10.1016/j.jpain.2007.11.012http://dx.doi.org/10.1001/archinternmed.2012.3654http://dx.doi.org/10.1089/acm.2008.SAR-4http://dx.doi.org/10.1136/aim.25.1-2.36http://dx.doi.org/10.1016/0014-4886(79)90273-5http://dx.doi.org/10.1016/S0304-3959(01)00349-9
-
7/23/2019 BMJ Acupuncture point injection treatment of primary
dysmenorrhoea
11/11
double blind, controlled studyprimary dysmenorrhoea: a
randomised,Acupuncture point injection treatment of
Q Zhao, M T Chao and J YuC Wade, L Wang, W J Zhao, F Cardini, F
Kronenberg, S Q Gui, Z Ying, N
doi: 10.1136/bmjopen-2015-0081662016 6:BMJ Open
http://bmjopen.bmj.com/content/6/1/e008166Updated information
and services can be found at:
These include:
References#BIBLhttp://bmjopen.bmj.com/content/6/1/e008166
This article cites 33 articles, 5 of which you can access for
free at:
Open Access
http://creativecommons.org/licenses/by-nc/4.0/non-commercial.
See:provided the original work is properly cited and the use
isnon-commercially, and license their derivative works on different
terms,permits others to distribute, remix, adapt, build upon this
work
Commons Attribution Non Commercial (CC BY-NC 4.0) license,
whichThis is an Open Access article distributed in accordance with
the Creative
serviceEmail alerting
box at the top right corner of the online article.Receive free
email alerts when new articles cite this article. Sign up in
the
CollectionsTopic Articles on similar topics can be found in the
following collections
(207)Obgyn(97)Complementary medicine
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo
request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go
to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.comon January 9, 2016 - Published
byhttp://bmjopen.bmj.com/Downloaded from
http://bmjopen.bmj.com/content/6/1/e008166http://bmjopen.bmj.com/content/6/1/e008166http://bmjopen.bmj.com/content/6/1/e008166#BIBLhttp://bmjopen.bmj.com/content/6/1/e008166#BIBLhttp://creativecommons.org/licenses/by-nc/4.0/http://creativecommons.org/licenses/by-nc/4.0/http://bmjopen.bmj.com//cgi/collection/bmj_open_obgynhttp://bmjopen.bmj.com//cgi/collection/bmj_open_complementary_medicinehttp://bmjopen.bmj.com//cgi/collection/bmj_open_obgynhttp://bmjopen.bmj.com//cgi/collection/bmj_open_complementary_medicinehttp://group.bmj.com/group/rights-licensing/permissionshttp://group.bmj.com/group/rights-licensing/permissionshttp://journals.bmj.com/cgi/reprintformhttp://journals.bmj.com/cgi/reprintformhttp://group.bmj.com/subscribe/http://group.bmj.com/subscribe/http://group.bmj.com/http://bmjopen.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/http://bmjopen.bmj.com/http://group.bmj.com/subscribe/http://journals.bmj.com/cgi/reprintformhttp://group.bmj.com/group/rights-licensing/permissionshttp://bmjopen.bmj.com//cgi/collection/bmj_open_obgynhttp://bmjopen.bmj.com//cgi/collection/bmj_open_complementary_medicinehttp://creativecommons.org/licenses/by-nc/4.0/http://bmjopen.bmj.com/content/6/1/e008166#BIBLhttp://bmjopen.bmj.com/content/6/1/e008166