Embed Size (px)
Citation preview

For peer review only
Immunogenicity and safety of early vaccination with two doses of a combined measles-mumps-rubella-varicella
vaccine in healthy Indian children from 9 months of age: a phase III, randomized, non-inferiority trial.
Journal: BMJ Open
Manuscript ID: bmjopen-2014-007202
Article Type: Research
Date Submitted by the Author: 14-Nov-2014
Complete List of Authors: Lalwani, Sanjay; Bharati Vidyapeeth Medical College, Pediatrics Chatterjee, Sukanta; Medical College Kolkata, Department of Pediatrics Balasubramanian, Sundaram; Kanchi Kamakoti Childs Trust Hospital, Bavdekar, Ashish; KEM Hospital, Mehta, Shailesh; GSK Pharmaceuticals, Datta, Sanjoy; GSK Vaccines, Povey, Michael; GSK Vaccines, Henry, Ouzama; GSK Vaccines,
<b>Primary Subject Heading</b>:
Paediatrics
Secondary Subject Heading: Paediatrics
Keywords: immunogenicity, India, measles-mumps-rubella-varicella vaccine, safety, vaccination schedule
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on January 4, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-007202 on 11 S
eptember 2015. D
ownloaded from

For peer review only
1
14 Nov 2014
Title page
Title: Immunogenicity and safety of early vaccination with two doses of a combined measles-
mumps-rubella-varicella vaccine in healthy Indian children from 9 months of age: a phase III,
randomized, non-inferiority trial.
Authors: Sanjay Lalwani, Vice Principal, Professor and Head of Departmenta, Sukanta
Chatterjee, Professor of Pediatricsb, Sundaram Balasubramanian, Senior Pediatric Consultant
c,
Ashish Bavdekar, Associate Professor and Consultant Pediatric Gastroenterologistd, Shailesh
Mehta, Area Medical Leader (South Asia)e, Sanjoy Datta, VP, Clinical R&D and Medical Affairs
f,
Michael Povey, Biostatisticianf, Ouzama Nicholson, Clinical Research Development Lead
g
Affiliations: aDepartment of Pediatrics, Bharati Vidyapeeth Deemed University, Pune 411043,
India
bDepartment of Pediatrics, Medical College Kolkata, 88 College street, Kolkata 700073, India
cKanchi Kamakoti Childs Trust Hospital, 12-A, Nageswara Road, Nungambakkam, Chennai
600034, India
dDepartment of Pediatrics, KEM Hospital, 489 Rasta Peth, Sardar Moodliar Road, Pune 411011,
India
eGSK Pharmaceuticals Ltd., Dr. Annie Besant Road, Worli, Mumbai 400030, India
fGSK Vaccines, Avenue Fleming 20, B-1300 Wavre, Belgium
gGSK Vaccines, 2301 Renaissance Boulevard, RN 0220, P.O. Box 61540, King of Prussia, PA
19406-2772, USA
Correspondence to: Sanjay Lalwani
Page 1 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
2
14 Nov 2014
Contact Details: +91 9822051716
Fax: +91 20 24364308
Email: [email protected]
Short title: Combined MMRV vaccine in Indian children
Abbreviations
ATP–according-to-protocol; CCID50–median cell culture infective dose; CI–confidence interval;
CRS–congenital rubella syndrome; ELISA–enzyme-linked immunosorbent assay; GMT–
geometric mean titer; IAP–Indian Academy of Pediatrics; mIU/mL–milli international unit per
milliliter; MMR–combined measles-mumps-rubella vaccine; MMR+V–coadministration of MMR
and V; MMRV–combined measles-mumps-rubella-varicella vaccine; pfu–plaque forming units;
SAE–serious adverse event; TVC–total vaccinated cohort; V–varicella; VZV–varicella zoster-
virus; WHO–World Health Organization
Keywords: immunogenicity, India, measles-mumps-rubella-varicella vaccine, safety, vaccination
schedule
Word count: 3521
Page 2 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
3
14 Nov 2014
Abstract
Objective: This study (NCT00969436) compared the immunogenicity and safety of measles-
mumps-varicella (MMR) followed by MMR+varicella (V) vaccines to (1) two doses of combined
MMRV and (2) MMR followed by MMRV, in Indian children.
Design: Phase III, open, randomized, non-inferiority study.
Setting: Six tertiary care hospitals located in India.
Participants: Healthy subjects aged 9–10 months not previously vaccinated against/exposed to
measles, mumps, rubella and varicella or without a history of these diseases.
Interventions: Subjects were randomized (2:2:1) to receive two doses of either MMRV
(MMRV/MMRV group) or MMR followed by MMRV (MMR/MMRV group) or MMR followed by
MMR+V (MMR/MMR+V, control group) at 9 and 15 months of age. Antibody titers against
measles, mumps and rubella were measured using ELISA and against varicella using an
immunofluorescence assay.
Main outcome measures: To demonstrate non-inferiority of the two vaccination regimens vs.
the control in terms of seroconversion rates, defined as a group difference with a lower bound
of the 95% confidence interval >-10% for each antigen, 43-days post-dose-2. Parents/guardians
recorded solicited local and general symptoms for a 4-day and 43-day period after each vaccine
dose, respectively.
Results: The seroconversion rates post-dose-1 ranged from 87.5%–93.2% for measles, 83.3%–
86.1% for mumps and 98.7%–100% for rubella across the three vaccine groups. Seroconversion
rates post-dose-2 for measles, mumps and rubella was 100% and at least 95.8% for varicella
Page 3 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
4
14 Nov 2014
across the three vaccine groups. Non-inferiority of MMRV/MMRV and MMR/MMRV to
MMR/MMR+V was achieved for all antigens, 43-days post-dose-2. The three vaccination
regimens were generally well-tolerated in terms of solicited local and general symptoms.
Conclusion: The immune responses elicited by the MMRV/MMRV and MMR/MMRV vaccination
regimens were non-inferior to those elicited by the MMR/MMR+V regimen for all antigens. The
three vaccination schedules also exhibited an acceptable safety profile in Indian children.
Abstract word count: 295/300
Trial registration: (NCT00969436)
Page 4 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
5
14 Nov 2014
Article Summary
• Measles, mumps, rubella (MMR) and varicella are highly infectious vaccine-preventable
childhood diseases with high mortality rates in India.
• A combined MMR-varicella vaccine may potentially facilitate the control of all four
diseases which is as immunogenic as separate MMR and varicella vaccinations.
Strengths and limitations of this study
This Indian study provides first time data on:
• A combined MMRV vaccine in a highly endemic measles setting.
• MMRV administered to children at 9 months of age which aligns with the expanded
programme of immunization schedule of measles vaccine administered at this age.
• Prevaccination serostatus that offers epidemiological indicators on the early disease
burden for measles, mumps, rubella and varicella
This study had no limitations.
Page 5 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
6
14 Nov 2014
Introduction
Measles, mumps, rubella and varicella are highly infectious vaccine-preventable childhood
diseases that continue to pose a significant public health problem in India and beyond.1-4
In
2010, global measles mortality was estimated at 139,000 (71,200–447,800) deaths, 47% of
which was estimated to have occurred in India.5 In 2011, large measles outbreaks were
reported in India (29,339 cases), Pakistan (4,386 cases), Nigeria (18,843 cases) and other
countries.6 Although measles elimination was declared in the United States in 2000, the
importation of the disease led to the highest number of cases in 2011 (220 cases) since 1996
while 159 cases were reported in 2013 by 16 states.7 In the European Union, the Dutch
authorites reported 1540 measles cases since May 2013 and in Germany, the reported number
of cases is nearly 10 times higher than the total cases in 2012.8 During the 2012–2013 outbreak,
there were over 2000 confirmed cases of measles in England and Wales.9 10
Thus, even
developed settings may be prone to epidemics if coverage wanes.
A dramatic decrease in the worldwide mumps disease burden has been observed since the
implementation of large-scale immunization in 1967.2 However, the true incidence in India is
difficult to ascertain due to limited baseline epidemiological data.11
Data from 2006 revealed that 82.2% children aged between 1 and 5 years, and 13.5% aged
between 10 and 15 years are susceptible to rubella in the Indian sub-continent.12
Although
congenital rubella syndrome (CRS) has been reported in most parts of India, no measures have
been undertaken to control this crippling disease and presently, reliable data on CRS in India is
limited.13
Page 6 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
7
14 Nov 2014
Epidemiological data on varicella-zoster virus (VZV) are also scarce in India as chickenpox was
not a notifiable disease in India until 200514
and due to the locally-perceived self-limiting and
relatively less severe nature, the disease is under-reported.
Globally, routine and effective vaccination has been identified as a critical approach towards
achieving high and sustained vaccination coverage rates and to strategically deal with the
burden of these four diseases.15
Consequently, the Indian Academy of Pediatrics (IAP) has
recommended the inclusion of a combined measles-mumps-rubella vaccine (MMR) in the
national immunization schedule to provide protection against CRS and also to reduce the
disease burden of measles and mumps.16
In countries with ongoing measles transmission, the
World Health Organization (WHO) recommends a first dose of measles vaccine at 9 months of
age to afford early protection and second dose at 15–18 months with a minimum interval of
one month between the two doses.1 In India, the observed high morbidity and mortality due to
measles has necessitated the administration of the measles vaccine at 9 months of age (by
which time most children will have lost their maternal antibodies to measles)17
followed by
MMR at 15 months of age.18
The IAP also recommends two doses of a varicella vaccine, with
the first dose administered at 15 months of age.18
The second dose may be administered three
months after the first, but is usually given at 4–6 years.18
There is increasing global evidence in
many settings that the high economic burden of varicella would be beneficially alleviated with
the inclusion of varicella vaccine.19-21
GSK’s MMR and varicella vaccines are available in over 100 countries22
and 80 countries,23
respectively. These vaccines are currently not included in the Indian national (government-
provided) immunization program; however, they are available via private practitioners. Based
Page 7 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
8
14 Nov 2014
on commercially available formulations, a combined MMR-varicella vaccine (MMRV) has been
developed to not only realize the benefits of vaccination against measles, mumps and rubella,
but also to facilitate the potential inclusion of varicella into national immunization programs.24-
27 The new vaccine is as immunogenic as separate MMR and varicella vaccinations.
28-30
This study evaluated the non-inferiority of two different vaccination regimens of the new
MMRV vaccine to the control regimen of separate injections when the vaccines were
administered at 9 and 15 months of age to healthy Indian children.
Page 8 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
9
14 Nov 2014
Methods
Study design and subjects
This phase IIIb, open, randomized, controlled study (NCT00969436) was conducted at six
tertiary care centers (Supplementary table) in India between November 2009 and February
2011. Healthy subjects aged 9–10 months were randomized (2:2:1) to receive either two doses
of the MMRV vaccine (MMRV/MMRV group) or MMR followed by MMRV (MMR/MMRV group),
or MMR followed by MMR+V (MMR/MMR+V group; control) at 9 and 15 months of age. The
control regimen largely reflects the optimum standard of care available in India under the IAP
recommendations.18
Among the six centers, the center in Bangalore did not enroll subjects according to the
randomization scheme and enrollment ceased at a small number of subjects because the
investigator was transferred (Supplementary table). Subjects were excluded from the study if
they had received any investigational drug/vaccine 30 days before the study vaccine or
immunosuppressants/immune-modifying drugs/blood products six months before the study.
Subjects previously vaccinated against/exposed to measles, mumps, rubella and varicella or
with a history of these diseases could not participate. A history of allergy likely to be aggravated
by any of the vaccine components, neurological disease/seizures, chronic illness or family
history of immunodeficiency, or symptoms of acute illness at the time of enrollment were other
reasons for exclusion. Vaccination was postponed for subjects with a rectal temperature
≥38.0°C/an axillary temperature ≥37.5°C. Subjects were also excluded if they lived in a
household with newborn infants or pregnant women who have not contracted chickenpox
previously or immunocompromised individuals.
Page 9 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
10
14 Nov 2014
The study adhered to Good Clinical Practice, the Declaration of Helsinki, and all applicable
regulations. The participating centers’ Institutional Ethics Committees/Institutional Review
Boards31
reviewed and approved the protocol. Parents/guardians provided written informed
consent before performing any study-related procedures.
Study Vaccines
All study vaccines: MMR (Priorix™), varicella (Varilrix™) and MMRV (Vammrix™ [same as Priorix-
Tetra™]) were manufactured by GSK, Belgium. The minimum expected potencies for measles,
rubella and varicella were identical between the MMR+V and MMRV vaccines.30
The minimum
expected potency for the mumps content was higher in the MMRV vaccine (≥104.4
median cell
culture infective dose [CCID50]) than in the MMR vaccine (≥103.7
CCID50). The vaccines supplied
in monodose vials contained a freeze-dried pellet which was reconstituted with the diluent
(provided in a pre-filled syringe) before subcutaneous injection into the anterolateral thigh.
Immunogenicity assessment
Blood samples were collected at pre-vaccination and 43 days after doses one and two. Antibody
titers were measured using a commercial enzyme-linked immunosorbent assay (ELISA;
Enzygnost™, Dade Behring, Marburg, Germany) with cut-off values of 150 mIU/mL (measles),
231 U/mL (mumps), and 4 IU/mL (rubella). For varicella, antibody titers were measured using
an immunofluorescence assay (Virgo™, Hemagen Diagnostics, Columbia, MD, USA) (assay cut-
off value of 4 dilution-1
).
Safety/Reactogenicity assessment
Parents/guardians used diary cards to record the occurrence of solicited local symptoms (pain,
redness and swelling at the injection site) for 4 days after each dose and solicited general
Page 10 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
11
14 Nov 2014
symptoms (fever [axillary temperature ≥37.5°C/rectal temperature ≥38°C], rash/exanthema,
parotid/salivary gland swelling and any suspected signs of meningeal irritation, including febrile
convulsions) for 43 days after each dose. Body temperature was measured daily via the
rectal/axillary route for 15 days after each vaccination. Between days 15 and 42, the presence
of fever was monitored using a temperature-sensitive pad,32
and if fever was suspected,
temperature was accurately measured with a thermometer. There were two follow-up visits
with the investigator at each study center, one vist 42–56 days following each vaccine
administration. During these visits, diary cards were returned to the investigator for
assessment.
Unsolicited symptoms were recorded for 43 days after each dose and the occurrence of serious
adverse events (SAEs) was recorded throughout the study. Intensity of symptoms was graded
on a scale of 0–3. Grade 3 solicited symptoms were defined as: pain: child cried when limb was
moved or a spontaneously painful limb; redness and swelling: injection site surface diameter
>20 mm; fever: axillary temperature >39°C/rectal temperature >39.5°C. Unsolicited symptoms
(including SAEs) were defined as grade 3 when they prevented normal daily activity.
Statistical Analyses
All statistical analyses were performed using SAS version 9.2, and 95% confidence intervals (CI)
were calculated using Proc StatXact 8.1. The sample size was estimated taking into
consideration the co-primary objectives of non-inferiority. Non-inferiority was achieved if the
lower limit of the two-sided standardized asymptotic 95% CI for the difference in
seroconversion rates between the two treatment groups and control group (MMRV/MMRV
minus MMR/MMR+V; MMR/MMRV minus MMR/MMR+V) was ≥-10% for each vaccine antigen,
Page 11 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
12
14 Nov 2014
43 days post-dose-2. Similarly, the secondary non-inferiority objective was achieved if the lower
limit of the two-sided standardized asymptotic 95% CI for the difference in seroconversion rates
between the MMRV/MMRV group and pooled MMR results from the MMR/MMRV and
MMR/MMR+V groups, 43 days post-dose-1 was ≥-10% for measles, mumps and rubella. A
sample size of 130 evaluable subjects in each treatment group and 65 evaluable subjects in the
control group was planned, which gave a power of at least 93.91% to meet the co-primary
objectives. A central randomization system using a minimization algorithm provided each child
with a unique treatment number. A randomization (2:2:1) blocking scheme ensured that the
balance between treatments was maintained by providing a unique treatment number that
identified the vaccine dose to be administered to the subjects. Furthermore, given different
physical characteristics of the study vaccines and the number of injections between study
groups, the study was conducted in an open manner where in the treatment allocation of
subjects was known to the investigators and the parents/guardians.
Immunogenicity analysis was performed on the according-to-protocol (ATP) cohort which
included all subjects for whom pre- and post-vaccination serology results were available and
who complied with study procedures. Seroconversion rates (defined as the appearance of
antibodies [i.e. antibody concentration/titer ≥cut-off value] in the serum of subjects who were
seronegative before vaccination) and geometric mean titers (GMTs) were calculated with exact
95% CIs for antibodies against each vaccine antigen after each dose. The 95% CIs for the GMTs
were obtained by exponential transformation of the 95% CI for the mean of log-transformed
titer.
Page 12 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
13
14 Nov 2014
Safety analysis was performed on the total vaccinated cohort (TVC) which included all
vaccinated subjects. Solicited and unsolicited symptoms reported for the subjects during the
respective post-vaccination periods were calculated with exact 95% CIs. All SAEs reported
during the entire conduct of the study were described.
Page 13 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
14
14 Nov 2014
Results
Demographics
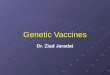
All 450 subjects enrolled in the study were vaccinated and included in the TVC: MMRV/MMRV
(n=180); MMR/MMRV (n=180) and MMR/MMR+V (n=90). Of these, 382 subjects were included
in the ATP cohort for immunogenicity: MMRV/MMRV (n=151); MMR/MMRV (n=156) and
MMR/MMR+V (n=75) (Figure 1). The median age of subjects in the ATP was 9 months (range:
9–10 months); 51.7% were male and all subjects were Indian. No demographic variations were
observed between the study groups (Supplementary table).
Immunogenicity
The proportion of initially seropositive subjects for measles, mumps and rubella was <2.7% in
all three groups. For varicella, 7.4% subjects in the MMRV/MMRV group, 8.3% in the
MMR/MMRV group and 2.7% in the MMR/MMR+V group were initially seropositive. After
dose-1, the seroconversion rates ranged from 87.5%–93.2% for measles, 83.3%–86.1% for
mumps and 98.7%–100% for rubella (Table 1). Post-dose-2 seroconversion rates were 100% for
measles, mumps and rubella and were at least 95.8% for varicella. Across the three vaccination
groups, the observed GMTs to measles, mumps and rubella increased between doses one and
two (Table 1). The co-primary objectives of non-inferiority with respect to seroconversion rates
43 days after dose-2 were achieved for all vaccine antigens, i.e. the lower bounds of the 95% CIs
for the difference in seroconversion rates between groups (MMRV/MMRV vs MMR/MMR+V;
MMR/MMRV vs MMR/MMR+V) was ≥-10%.
Page 14 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
15
14 Nov 2014
Table 1 Seroconversion rates and Antibody GMTs of the MMRV/MMRV, MMR/MMRV and MMR/MMR+V groups 43 days post-
vaccination (ATP cohort)
Antigen MMRV/MMRV group (N=151) MMR/MMRV group (N=156) MMR/MMR+V group (N=75)
Dose Na
SCb (%)
c (95% CI) GMT
d (95% CI) N
a SC
b (%)
c (95% CI) GMT
d (95% CI) N
a SC
b (%)
c (95% CI) GMT
d (95% CI)
Measles Pre-dose 2 1.3 - 3 1.9 - 2 2.7 -
Post-dose-
1
148 93.2 (87.9; 96.7) 2013.6 (1662.2; 2439.3) 153 88.2 (82.0; 92.9) 1180.4 (963.0; 1446.7) 72 87.5 (77.6; 94.1) 1200.0 (887.9; 1621.8)
Post-dose-
2
149 100 (97.6; 100) 4471.3 (3975.3; 5029.2) 153 100 (97.6; 100) 3358.7 (3017.5; 3738.4) 72 100 (95.0; 100) 2495.0 (2064.5; 3015.2)
Mumps Pre-dose 2 1.3 - 3 1.9 - 2 2.7 -
Post-dose-
1
144 86.1 (79.4; 91.3) 991.9 (819.7; 1200.3) 152 84.2 (77.4; 89.6) 746.6 (628.0; 887.6) 72 83.3 (72.7; 91.9) 775.1 (600.9; 999.7)
Page 15 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
16
14 Nov 2014
Post-dose-
2
149 100 (97.6; 100) 6428.0 (5774.9; 7154.9) 152 100 (97.6; 100) 10108.5 (9223.9; 11078.0) 72 100 (95.0; 100) 4925.3 (4200.9; 5774.7)
Rubella Pre-dose 1 0.7 - 4 2.6 - 2 1.7 -
Post-dose-
1
149 98.7 (95.2; 99.8) 45.4 (38.3; 53.7) 152 99.3 (96.4; 100) 63.8 (55.9; 72.8) 73 100 (95.1; 100) 62.0 (51.3; 74.9)
Post-dose-
2
150 100 (97.6; 100) 148.4 (136.1; 161.8) 152 100 (97.6; 100) 164.8 (152.1; 178.6) 73 100 (95.1; 100) 173.0 (153.0; 195.6)
Varicella Pre-dose 11 7.4 - 13 8.3 - 2 2.7 -
Post-dose-
1
138 94.2 (88.9; 97.5) 120.5 (90.8; 160.0) 142 2.8 (0.8; 7.1) 2.2 (2.0; 2.4) 72 1.4 (0.0; 7.5) 2.2 (1.8; 2.6)
Post-dose-
2
138 100 (97.4; 100) 5318.5 (4318.7; 6549.8) 143 98.6 (95.0; 99.8) 198.0 (158.2; 247.7) 72 95.8 (88.3; 99.1) 128.0 (91.7; 178.7)
a Number of children initially seronegative with available results
b Seroconversion
Page 16 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
17
14 Nov 2014
c Percentage of children that seroconverted for each antigen
d Geometric mean titers
The secondary objective of non-inferiority of the MMRV/MMRV group and pooled MMR results from the MMR/MMRV and
MMR/MMR+V groups in terms of seroconversion rates 43-days post-dose-1 for measles, mumps and rubella was also achieved (Table
2).
Table 2 Post-dose-1 seroconversion rates between the MMRV/MMRV group and pooled MMR/MMRV + MMR/MMR+V groups (ATP
cohort)
MMRV MMR
Antibody (MMRV/MMRV group) (Pooled
[MMR/MMRV] +
[MMR/MMR+V]
groups)
Difference in percentage (MMRV
minus MMR)
Na
%b
Na
%b
%c (95% CI)
Page 17 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
18
14 Nov 2014
MMRV MMR
Antibody (MMRV/MMRV group) (Pooled
[MMR/MMRV] +
[MMR/MMR+V]
groups)
Difference in percentage (MMRV
minus MMR)
Na
%b
Na
%b
%c (95% CI)
Measles 148 93.2 225 88.0 5.24 (-1.06; 11.13)
Mumps 144 86.1 224 83.9 2.18 (-5.66; 9.42)
Rubella 149 98.7 225 99.6 -0.90 (-4.36; 1.29)
Varicella 138 94.2 - - -
a Number of children initially seronegative with available results
b Percentage of children that seroconverted for each antigen
Page 18 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
19
14 Nov 2014
c Difference in percentage of children that seroconverted for each antigen between the MMMR/MMRV group and the pooled MMR results from the (MMR/MMRV
+ MMR/MMR+V) groups
Safety and Reactogenicity
During the 43-day post-vaccination period, the occurrence of solicited and unsolicited symptoms ranged between 51.1%–56.1% after
dose-1 and 36.2%–37.3% after dose-2 across the three vaccine groups. During the 4-day post-dose-1 follow-up period, injection site
pain was the most commonly reported solicited local symptom: MMRV/MMRV (11.5%), MMR/MMRV (7%) and MMR/MMR+V (10.7%).
Post-dose-2, injection site symptoms were reported by fewer than 6.5% of subjects (Table 3). Redness was the grade 3 local symptom
reported by 3 subjects (1.9%) in the MMRV/MMRV group, post-dose-2.
Fever was the most commonly reported solicited general symptom in all three vaccine groups during the 43-day post-vaccination
follow-up period after each dose (Table 3). The observed incidence of fever across all vaccine groups decreased between doses one and
two during the 15-day and 43-day post-vaccination follow-up periods (Table 3).
Page 19 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
20
14 Nov 2014
Table 3 Incidence of solicited local symptoms (during the 4-day) and fever (during the 15-day and 43-day) post-vaccination period
(Total vaccinated cohort)
MMRV/MMRV group MMR/MMRV group MMR/MMR+V group
Dose-1 Na=174;
Dose-2 Na=155
Dose-1 Na=172;
Dose-2 Na=159
Dose-1 Na=84;
Dose-2 Na=79
%b
(95% CI) %b
(95% CI) %b
(95% CI)
Pain Post-dose-1 11.5 (7.2; 17.2) 7.0 (3.7; 11.9) 10.7 (5.0; 19.4)
Post-dose-2 5.8 (2.7; 10.7) 6.3 (3.1; 11.3) 3.8 (0.8; 10.7)
Redness Post-dose-1 8.6 (4.9; 13.8) 4.7 (2.0; 9.0) 3.6 (0.7; 10.1)
Post-dose-2 6.5 (3.1; 11.5) 3.8 (1.4; 8.0) 0.0 (0.0; 4.6)
Swelling Post-dose-1 4.6 (2.0; 8.9) 2.9 (1.0; 6.7) 3.6 (0.7; 10.1)
Post-dose-2 5.8 (2.7; 10.7) 3.8 (1.4; 8.0) 0.0 (0.0; 4.6)
Page 20 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
21
14 Nov 2014
Fever (15 days
post-dose-1)
Any 32.2 (25.3;39.7) 28.5 (21.9; 35.9) 21.7 (13.4; 32.1)
Grade 3
(>39.5°C)
3.4 (1.3; 7.4) 1.7 (0.4; 5.0) 1.2 (0.0; 6.5)
Related 28.2 (21.6; 35.5) 24.4 (18.2; 31.5) 16.9 (9.5; 26.7)
Medical Advice 6.3 (3.2; 11.0) 7.6 (4.1; 12.6) 2.4 (0.3; 8.4)
Fever (15 days
post-dose-2)
Any 17.4 (11.8;24.3) 13.2 (8.4; 19.5) 15.2 (8.1; 25.0)
Grade
3(>39.5°C)
1.3 (0.2; 4.6) 1.3 (0.2; 4.5) 0.0 (0.0; 4.6)
Related 13.5 (8.6; 20.0) 11.9 (7.4; 18.0) 12.7 (6.2; 22.0)
Medical Advice 3.9 (1.4; 8.2) 1.3 (0.2; 4.5) 1.3 (0.0; 6.9)
Any 43.7 (36.2; 51.4) 40.7 (33.3; 48.4) 32.5 (22.6; 43.7)
Grade 6.3 (3.2; 11.0) 2.9 (1.0; 6.7) 1.2 (0.0; 6.5)
Page 21 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
22
14 Nov 2014
Fever (43 days
post-dose-1)
3(>39.5°C)
Related 30.5 (23.7; 37.9) 27.9 (21.3; 35.2) 18.1 (10.5; 28.0)
Medical Advice 13.8 (9.0; 19.8) 16.9 (11.6; 23.3) 4.8 (1.3; 11.9)
Fever (43 days
post-dose-2)
Any 26.5 (19.7; 34.1) 23.3 (16.9; 30.6) 27.8 (18.3; 39.1)
Grade
3(>39.5°C)
1.3 (0.2; 4.6) 3.8 (1.4; 8.0) 2.5 (0.3; 8.8)
Related 14.2 (9.1; 20.7) 13.2 (8.4; 19.5) 12.7 (6.2; 22.0)
Medical Advice 4.5 (1.8; 9.1) 5.6 (2.6; 10.5) 7.6 (2.8; 15.8)
a Number of children with at least one documented dose
b Percentage of children reporting the symptom at least once
Page 22 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
23
14 Nov 2014
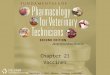
An absence of a clear peak in the prevalence of fever during the 43-day period after dose-1 for
all three vaccine groups is depicted in Figure 2(a). Post-dose-2 fever is depicted in Figure 2(b).
Rash occurred in one subject after the first dose of MMRV in the MMRV/MMRV group as
compared to three subjects after the first MMR dose (MMR/MMRV [n=2]; MMR/MMR+V [n=1])
groups). Only one subject developed rash after dose-2 in the MMR/MMRV group. There were
no reports of meningeal irritation, febrile convulsions or parotid gland swelling during the 43-
day period after each vaccine dose.
At least one unsolicited symptom was reported in 20.6% subjects after the first dose of MMRV
in the MMRV/MMRV group and in 21.7% and 20.0% subjects after the first dose of MMR in the
MMR/MMRVand MMR/MMR+V groups, respectively. The most commonly reported symptoms
in each group were: upper respiratory tract infection in the MMRV/MMRV group (n=10; 5.6%);
cough in the MMR/MMRV group (n=10; 5.6%) and nasopharyngitis, rhinitis and cough in the
MMR/MMR+V group (n=6; 6.7% for each symptom). Similarly, at least one unsolicited symptom
was reported in 10.6% subjects after the second dose of MMRV in the MMRV/MMRV group, in
10.0% subjects who received their first dose of MMRV in the MMR/MMRV groups and in 12.2%
subjects following dose-2 of MMR+V in the MMR/MMR+V group. The most commonly reported
symptoms in each group were: rhinitis and cough in the MMRV/MMRV group (n=6; 3.3% for
each symptom) and rhinitis in the MMR/MMRV (n=7; 3.9%) and MMR/MMR+V groups (n=5;
5.6%).
Overall, 18 SAEs occurred in the study. At least one SAE occurred in 13 subjects (MMRV/MMRV
[n=7]; MMR/MMRV [n=6]; MMR/MMR+V [n=0] groups). The most commonly reported SAEs
were lower respiratory tract infection (in two subjects) in the MMRV/MMRV group, and
Page 23 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
24
14 Nov 2014
gastroenteritis (in three subjects) in the MMR/MMRV group. Other SAEs reported were
gastroenteritis, pneumonitis, wheezing, viral infection, pneumonia, febrile convulsion, upper
respiratory tract inflammation, dehydration and bronchiolitis. All SAEs resolved without
sequelae and were considered unrelated to vaccination.
Page 24 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
25
14 Nov 2014
Discussion
This non-inferiority study evaluated the immunogenicity and safety of two vaccination regimens
(1) two-dose MMRV/MMRV (2) MMR followed by MMRV compared to a control group (MMR
followed by MMR+V) when administered to healthy Indian children at 9 and 15 months of age.
The co-primary non-inferiority criterion ruling out a 10% difference in seroconversion rates
post-dose-2 of MMRV/MMRV and MMR/MMRV compared to MMR/MMR+V was achieved for
all antigens, indicating that the immune responses elicited by the two vaccination regimens
were non-inferior to those elicited by the control regimen. Although the two-dose
MMRV/MMRV schedule is not included in several immunization programs, this regimen has
been established to be non-inferior to the two-dose MMR+V schedule in separate studies in
Germany and Singapore.30 33
Additionally, on comparing the post-dose-1 responses, one dose of
MMRV in the MMRV/MMRV group elicited non-inferior immune responses against measles,
mumps and rubella compared to pooled results of one dose of MMR in the MMR/MMRV and
MMR/MMR+V groups.
In the three vaccine groups, we observed low baseline seropositivity rates (<2.7%) for measles,
mumps and rubella in subjects at 9 months of age. This finding suggests a possible decline in
circulating maternal antibodies and measles infection by this age which would support 9
months as a suitable age for initial vaccination. However, it should be noted that this finding is
inconsistent with a notable Indian study conducted approximately a decade ago that suggested
the persistence of high circulating maternal antibodies at 9 months of age.11
Additionally, while
lowering the measles vaccination age in low income countries is supported by many,
vaccinating at 9 months or earlier may mean that the immune system has not reached
Page 25 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
26
14 Nov 2014
optimum maturity to mount an effective response and provide effective long-term protection
against measles or the other diseases with just a single vaccine dose.34 35
The seroconversion
rates for all antigens in the MMRV/MMRV group were consistent with previous observations in
Singaporean children at 9 months of age by Goh et al.33
However, with a first dose of MMR, the
observed post-dose-1 seroconversion rates to measles (MMR/MMRV=88.2%;
MMR/MMR+V=87.5%) and mumps (MMR/MMRV=84.2%; MMR/MMR+V=83.3%) in this study
were somewhat lower than those reported by Schuster et al, following administration of a first
dose of MMR to children aged 11–21 months in Germany (measles: 93.4%; mumps: 93.6%).30
A
contrast in immune responses between the current and German study may be attributed to the
age at vaccination, maturity of the immune system and circulating maternal antibodies. Also,
the higher GMTs oberved to measles in the MMRV/MMRV group compared to the
MMR/MMRV and MMR/MMR+V groups could translate to more effective protection in a highly
endemic measles environment where coverage from a second dose of a measles-containing
vaccine remains variable throughout the country.6 Lower seroconversion rates with other live-
attenuated vaccines (such as the oral polio vaccine and the rotavirus vaccine) have also been
observed in India and South Asia compared to more industrialized settings.36-38
Nevertheless, we observed high seroconversion rates for all vaccine antigens following
administration of second vaccination at 15 months of age, indicating that an early two-dose
immunization strategy when the first dose is administered as early as 9 months elicits a
satisfactory immune response. An interesting observation was the markedly high GMT against
mumps post-dose-2 in the MMR/MMRV (10108.5) group compared to the MMR/MMR+V
(4925.3) and MMRV/MMRV (6428.0) groups. This observation has not been reported previously
Page 26 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
27
14 Nov 2014
despite the higher mumps antigen content in the MMRV vaccine when compared to the MMR
vaccine. Studies to further evaluate this finding may be needed in the future.
Early administrations of all three vaccination regimens were well-tolerated when administered
to young children at 9 and 15 months of age. Similar differences in solicited general symptoms
have been observed in studies conducted in the Indian subcontinent with other live attenuated
viral vaccines (such as Rotarix™) compared with other countries.37 39
Notably, unlike previous
studies conducted in other countries,28-30 33
this study did not demonstrate any difference in
fever rates between MMRV and MMR when used as a first dose of measles-containing vaccine.
Although this may be related to the epidemiological context in India, which differs from
developed countries, the reason is unclear. In general, the reporting rate of fever was also
lower than that seen in other studies.28-30 33
Again, this may be due to the younger age of
children enrolled, or the presence of maternal antibodies, which may have limited measles
virus replication post-dose-1, resulting in the blunting of immune response and fever response
rates; or cross-cultural/geographical differences in the reporting of symptoms. Further data
may be needed to determine if there is in fact a difference in the reactogenicity profile between
developed and developing countries.
It is possible to eliminate measles from a specific region by sustaining high immunization
coverage as is evident from Latin America, Finland and the United States40-42
; countries such as
Finland have also successfully eliminated mumps and rubella using the MMR vaccine.41
In view
of the ongoing transmission and high mortality risk of measles in India, immunization coverage
of ≥95% for the first and second dose would be required to ensure prevention of measles virus
transmission.43
Currently, the Indian national immunization schedule’s 9 months single dose
Page 27 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
28
14 Nov 2014
immunization coverage is 74%44
; however, as this represents the average, coverage rates in
some parts of the country may be even lower. Several European countries, where the first
MMR dose is administered to children in the second year of life (12–24 months), continue to
face a relatively low immunization coverage rates resulting in measles and mumps outbreaks,24
as was recently observed even in South Wales.10
An earlier vaccination schedule was
implemented in Germany as a result of such outbreaks, whereby the first dose is now
administered at 11–14 months followed by the second dose at 15–23 months of age.24
This
revised strategy achieved well-documented successful immunization coverage rates,24
and
highlights the importance of early vaccination with increased compliance and subsequently
higher coverage rates.
Conclusion
This study demonstrates that in an Indian setting, the two-dose vaccination regimens of
MMRV/MMRV and MMR/MMRV are non-inferior to the control MMR/MMR+V regimen (i.e.
the local standard of care recommended by the IAP)17
in terms of immunological response.
Both vaccination schedules demonstrated an acceptable safety profile when administered to
healthy Indian children at 9 and 15 months of age. Introduction of the MMRV vaccine may
achieve higher coverage rates in India by increasing compliance for two-dose MMR and
varicella vaccines, and thereby improving the limited success of the MMR vaccination program.
This will not only facilitate effective population protection against measles, but against three
other common childhood viral infectious diseases: mumps, rubella and varicella.
Page 28 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
29
14 Nov 2014
Trademarks
Vammrix, Priorix-Tetra, Priorix, Varilrix and Rotarix are registered trademarks of
GlaxoSmithKline group of companies.
Virgo is a registered trademark of Hemagen Diagnostics, Columbia, MD, USA.
Enzygnost is a registered trademark of Dade Behring, Marburg, Germany.
Contributors: SL, SB, SC and AB were involved in the recruitment of subjects. SL critically
reviewed the protocol and study report and also provided scientific and medical inputs during
the development of the study report. SB was involved in providing scientific and medical inputs
to the protocol and critically reviewing the protocol. SC coordinated and supervised data
collection at one site and carried out the initial analyses. AB provided critical inputs to the study
report and reviewed the content of the study report. SM and SD conceptualized and designed
the study. SM also supervised data collection at all sites. MP was involved in data analysis and
interpretation. SD and ON provided input to the interpretation of clinical data.
All authors critically reviewed and revised the manuscript during the development and
approved the final version of the manuscript. All authors are guarantors and accept full
responsibility for the work and/or conduct of the study, had access to the data, and controlled
the decision to publish.
Funding: This study was sponsored and funded by GlaxoSmithKline Biologicals SA.
GlaxoSmithKline Biologicals SA was involved in all stages of the study conduct and analysis; and
also took charge of all costs associated with the development and the publishing of the
manuscript.
Page 29 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
30
14 Nov 2014
Competing interests: All authors have completed the ICMJE uniform disclosure form at
www.icmje.org/coi_disclosure.pdf. SL declares to have received institutional grant (for BVDU
Medical college, Dept. of Pediatrics) and travel support for the meeting from GlaxoSmithKline
group of companies. He also declares to have received fees for lecture at Pedicon 2011. SB
declares that The childs trust medical research foundation received grant from GlaxoSmithKline
group of companies. AB declares to have received institutional grant for conducting this trial
and has pending institutional grants from GlaxoSmithKline group of companies for other
vaccine trials. He also declares to have received support for travel/accomodation while
participating in investigator meetings and renumeration for participating in a meeting on
adjuvants from GlaxoSmithKline group of companies. SM, SD, MP and ON are employees of
GlaxoSmithKline group of companies; SD and ON declare to have stock options. MP declares
that he received payment/fees for review of statistical analysis and reviewing this manuscript
from GlaxoSmithKline group of companies. SC has no conflict of interest. The authors have no
financial relationships relevant to this article to disclose.
Data sharing: Upon authorization or termination of development of this medicine, anonymized
patient-level data underlying this study will be made available to independent researchers,
subject to review by an independent panel, at www.clinicalstudydatarequest.com. Consent for
data sharing was not obtained from the participants, but the presented data are anonymized
and risk of identification is low.
Acknowledgements
The authors thank the study nurses and staff members involved, and the parents and children
who participated in the study. The authors acknowledge Dr. Sonali Palkar for her support in
Page 30 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
31
14 Nov 2014
conducting the clinical trial and Dipti Phatarpekar for coodinating and supervising data
collection at two study sites. The authors also thank Ashmita Ravishankar for medical writing
and publication coordination (GlaxoSmithKline Vaccines), Jarno Jansen (Keyrus Biopharma for
GlaxoSmithKline Vaccines), Geetha Subramanyam (GlaxoSmithKline Vaccines) and Shruti MP
(GlaxoSmithKline Vaccines) for editorial assistance and publication coordination.
Trial registration: (NCT00969436)
Page 31 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
32
14 Nov 2014
References:
1 World Health Organization. Measles vaccines. Wkly Epidemiol Rec 2009;84:349–60.
2 World Health Organization. Mumps virus vaccines. Wkly Epidemiol Rec 2007;82:49–60.
3 World Health Organization. Rubella vaccines. Wkly Epidemiol Rec 2011;86:301–16.
4 CDC. Prevention of varicella: Recommendations of the Advisory Committee on
Immunization Practices (ACIP). MMWR 2007;56(RR04):1–40.
5 Simons E, Ferrari M, Fricks J, et al. Assessment of the 2010 global measles mortality
reduction goal: results from a model of surveillance data. Lancet 2012;379:2173–8.
6 World Health Organization Media Centre. WHO: Measles deaths decline, but elimination
progress stalls in some regions. 2013. Avaiblat at:
http://www.who.int/mediacentre/news/notes/2013/measles_20130117/en/. Accessed 25
November, 2013.
7 Centers for Disease Control and Prevention (CDC). Measles – United States, January 1-
August 24, 2013. MMWR Morb Mortal Wkly Rep 2013;62:741–3.
8 European Centre for Disease Prevention and Control. Monitoring current health threats,
week 39/2013: measles and possible polio re-emergence in focus. Available at:
http://ecdc.europa.eu/en/press/news/_layouts/forms/News_DispForm.aspx?List=8db7286
c%2Dfe2d%2D476c%2D9133%2D18ff4cb1b568&ID=872&RootFolder=%2Fen%2Fpress%2Fn
ews%2FLists%2FNews&Web=86661a14%2Dfb61%2D43e0%2D9663%2D0d514841605d&pr
eview=yes&pdf=yes. Accessed 26 February, 2014.
9 Health Protection Report. Confirmed measles cases (England) to end-September. Updated 8
November 2013; Volume 7, No. 45. Available at:
Page 32 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
33
14 Nov 2014
http://www.hpa.org.uk/hpr/archives/2013/news4513.htm#msls1309. Accessed 25
November 2013.
10 Jacqui Wise. Largest group of children affected by measles outbreak in Wales is 10-18 year
olds. BMJ 2013;346:f2545.
11 Yadav S, Thukral R, Chakarvarti A. Comparative evaluation of measles, mumps & rubella
vaccine at 9 & 15 months of age. Indian J Med Res 2003;118:183–6.
12 Ramamurty N, Murugan S, Raja D, et al. Serosurvey of rubella in five blocks of Tamil Nadu.
Indian J Med Res 2006;123:51–4.
13 Verma R, Khanna P, Chawla S. Rubella vaccine: New horizon in prevention of congenital
rubella syndrome in India. Hum Vaccin Immunother 2012;8:1-3.
14 Verma R, Bairwa M, Chawla S, et al. Should the chickenpox vaccine be included in the
national immunization schedule in India? Hum Vaccin 2011;7:874–7.
15 World Health Organization. Wkly Epidemiol Rec 2011;86:437–44.
16 Singhal T, Amdekar YK, Thacker N. IAP Committee on Immunization. Indian Pediatrics
2007;44:390–2.
17 Verma R, Khanna P, Bairwa M, et al. Introduction of a second dose of measles in national
immunization program in India: A major step towards eradication. Hum Vaccin
2011;7:1109–11.
18 Indian Academy of Pediatrics Committee on Immunization (IAPCOI). Consensus
recommendations on immunization and IAP immunization timetable 2012. Indian Pediatrics
2012;49:549–64.
Page 33 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
34
14 Nov 2014
19 Ozdemir H, Candir MO, Karbuz A, et al. Chickenpox complications, incidence and financial
burden in previously healthy children and those with an underlying disease in Ankara in the
pre-vaccination period. Turk J Pediatr 2011;53:614–25.
20 Bilcke J, Ogunjimi B, Marais C, et al. The health and economic burden of chickenpox and
herpes zoster in Belgium. Epidemiol Infect 2012;140:2096–109.
21 Da YP, Luo LY, Song LZ. [Economic burden of inpatient of varicella in Shandong, Gansu and
Hunan provinces, 2007]. Zhongguo Yi Miao He Mian Yi 2009;15:438–42.
22 Department of Health. Childhood immunizations guidance. Available at:
http://www.gov.im/lib/docs/health/Public_Health/Immunisation/imm010112immunisation
bookletlress.pdf. Accessed 8 November, 2012.
23 Chiu SS, Lau Y-L. Review of the Varilrix™ varicella vaccine. Expert Rev Vaccines 2005;4:629–
43.
24 Vesikari T, Sadzot-Delvaux C, et al. Increasing coverage and efficiency of measles, mumps,
and rubella vaccine and introducing universal varicella vaccination in Europe. A role for the
combined vaccine. Pediatr Infect Dis J 2007;26:632–8.
25 Rentier B, Gershon AA. European Working Group on Varicella. Consensus: varicella
vaccination of healthy children – a challenge for Europe. Pediatr Infect Dis J 2004;23:379–
89.
26 Czajka H, Schuster V, Zepp F, et al. A combined measles, mumps, rubella and varicella
vaccine (Priorix-Tetra™): Immunogenicity and safety profile. Vaccine 2009;27:6504–11.
27 Knuf M, Faber J, Barth I, et al. A combination vaccine against measles, mumps, rubella and
varicella. Drugs Today 2008;44:279–92.
Page 34 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
35
14 Nov 2014
28 Nolan T, McIntyre P, Roberton D, et al. Reactogenicity and immunogenicity of a live and
attenuated tetravalent measles-mumps-rubella-varicella (MMRV) vaccine. Vaccine
2002;21:281–9.
29 Knuf M, Habermehl P, Zepp F, et al. Immunogenicity and safety of two doses of tetravalent
measles-mumps-rubella-varicella vaccine in healthy children. Pediatr Infect Dis J
2006;25:12–8.
30 Schuster V, Otto W, Maurer L, et al. Immunogenicity and safety assessments after one and
two doses of a refrigerator-stable tetravalent measles-mumps-rubella-varicella vaccine in
healthy children during the second year of life. Pediatr Infect Dis J 2008;27;724–30.
31 Indian clinical trial registry. Available at:
http://ctri.nic.in/Clinicaltrials/showallp.php?mid1=930&EncHid=&userName=CTRI/2009/09
1/000750. Accessed 3 May, 2013.
32 Martyn KK, Urbano MT, Hayes JS, et al. Comparison of axillary, rectal and skin-based
temperature assessment in preschoolers. Nurse Pract 1988;13:31–6.
33 Goh P, Lim FS, Han HH, Willems P. Safety and Immunogenicity of early vaccination with two
doses of tetravalent measles-mumps-rubella-varicella (MMRV) vaccine in healthy children
from 9 months of age. Infection 2007;35:326–33.
34 Aaby P, Martins CL, Garly ML, et al. The optimal age of measles immunisation in low-income
countries: a secondary analysis of the assumptions underlying the current policy. BMJ Open
2012;12:e000761.
35 Gomber S, Arora SK, Das S, et al. Immune response to second dose of MMR vaccine in
Indian children. Indian J Med Res 2011;134:302–6.
Page 35 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
36
14 Nov 2014
36 Patriarca PA, Wright PF, John TJ. Factors affecting the immunogenicity of oral poliovirus
vaccine in developing countries: review. Rev Infect Dis 1991;13:926–39.
37 Narang A, Bose A, Pandit AN, et al. Immunogenicity, reactogenicity and safety of human
rotavirus vaccine (RIX4414) in Indian infants. Hum Vaccin 2009;5:414–9.
38 Zaman K, Sack DA, Yunus M, et al. Successful co-administration of a human rotavirus and
oral poliovirus vaccines in Bangladesh infants in a 2-dose schedule at 12 and 16 weeks of
age. Vaccine 2009;27:1333–9.
39 Vesikari T, Karvonen A, Puustinen L, et al. Efficacy of RIX4414 live attenuated human
rotavirus vaccine in Finnish infants. Pediatr Infect Dis J 2004;23:937–43.
40 Andrus JK, de Quadros CA, Solorzano CC, et al. Measles and rubella eradication in the
Americas. Vaccine 2011;29S:D91–6.
41 Davidkin I, Kontio M, Paunio M, et al. MMR vaccination and disease elimination: the Finnish
experience. Expert Rev Vaccines 2010;9:1045–53.
42 Mulholland EK. Measles in the United States, 2006. N Engl J Med 2006;355:440–3.
43 World Health Organization. Field guidelines for measles elimination, 2004. Available at:
http://www.measlesrubellainitiative.org/mi-
files/Tools/Guidelines/WPRO/Field_guidelines_measles_elimination.pdf. Accessed 26
September, 2012.
44 World Health Organization. Immunization profile – India. Available at:
http://apps.who.int/immunization_monitoring/en/globalsummary/countryprofileresult.cfm
?C=ind. Accessed 13 November, 2012.
Page 36 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
37
14 Nov 2014
Figure legends
Figure 1 Subject disposition
Figure 2a Prevalence of fever during the 43-day post-vaccination period after Dose 1
(Total vaccinated cohort)
Figure 2b Prevalence of fever during the 43-day post-vaccination period after Dose 2
(Total vaccinated cohort)
Page 37 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
292x179mm (300 x 300 DPI)
Page 38 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
149x118mm (300 x 300 DPI)
Page 39 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
148x117mm (300 x 300 DPI)
Page 40 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
1
14 Nov 2014
Supplementary table
Number of children recruited by study center and demographic characteristics
Name and location of study center in
India
MMRV/MMRV MMR/MMRV
MMR/MMR+V Total
na
%a
Center 1, Pune 37 37 18 92 20.4
Center 2, Pune 53 53 26 132 29.3
Center 3, Bangalore 2 2 2 6 1.3
Center 4, Chennai 24 24 12 60 13.3
Center 5, Kolkata 34 34 17 85 18.9
Center 6, Goa 30 30 15 75 16.7
All 180 180 90 450 100
Demographic characteristics MMRV/MMRV MMR/MMRV MMR/MMR+V Total
Age (months) Mean (standard
deviation)
9 (0.0) 9 (0.11) 9 (0.0) 9 (0.07)
Median (range) 9 (9–9) 9 (8–10) 9 (9–9) 9 (8–10)
Page 41 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
2
14 Nov 2014
n
% n % n % n %
Gender Female 79 44.4 89 49.2 49 54.4 216 48.3
Male 99 55.6 91 50.8 41 45.6 231 51.7
a number (percentage) of children in a given category
Page 42 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
3
14 Nov 2014
Page 43 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
CONSORT 2010 checklist Page 1
CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title 1
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 3-4
Introduction
Background and
objectives
2a Scientific background and explanation of rationale 6-8
2b Specific objectives or hypotheses 7-8
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 9
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons 9
Participants 4a Eligibility criteria for participants 9
4b Settings and locations where the data were collected 9 and Supp.
table
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered
9-10
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed
10-11
6b Any changes to trial outcomes after the trial commenced, with reasons Not applicable
Sample size 7a How sample size was determined 12
7b When applicable, explanation of any interim analyses and stopping guidelines Not applicable
Randomisation:
Sequence
generation
8a Method used to generate the random allocation sequence 12
8b Type of randomisation; details of any restriction (such as blocking and block size) 12
Allocation
concealment
mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers),
describing any steps taken to conceal the sequence until interventions were assigned
12
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to
interventions
9, 11
Page 44 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 2
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those
assessing outcomes) and how
Not applicable
11b If relevant, description of the similarity of interventions Not applicable
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 11-13
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses Not applicable
Results
Participant flow (a
diagram is strongly
recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome
14/Figure 1
13b For each group, losses and exclusions after randomisation, together with reasons Figure 1
Recruitment 14a Dates defining the periods of recruitment and follow-up Not applicable
14b Why the trial ended or was stopped Not applicable
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group Supp. Table
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was
by original assigned groups
14
Outcomes and
estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its
precision (such as 95% confidence interval)
14, 15/Tables
1-3/Figures
2(a) & (b)
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended Not applicable
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory
Not applicable
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 15,16
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses Not applicable
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 17-20
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 17-20
Other information
Registration 23 Registration number and name of trial registry 24
Protocol 24 Where the full trial protocol can be accessed, if available Not applicable
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders 21
Page 45 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 3
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic trials.
Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
Page 46 of 46
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
Immunogenicity and safety of early vaccination with two doses of a combined measles-mumps-rubella-varicella
vaccine in healthy Indian children from 9 months of age: a phase III, randomized, non-inferiority trial.
Journal: BMJ Open
Manuscript ID: bmjopen-2014-007202.R1
Article Type: Research
Date Submitted by the Author: 21-May-2015
Complete List of Authors: Lalwani, Sanjay; Bharati Vidyapeeth Medical College, Pediatrics Chatterjee, Sukanta; Medical College Kolkata, Department of Pediatrics Balasubramanian, Sundaram; Kanchi Kamakoti Childs Trust Hospital, Bavdekar, Ashish; KEM Hospital, Mehta, Shailesh; GSK Pharmaceuticals, Datta, Sanjoy; GSK Vaccines, Povey, Michael; GSK Vaccines, Henry, Ouzama; GSK Vaccines,
<b>Primary Subject Heading</b>:
Paediatrics
Secondary Subject Heading: Paediatrics
Keywords: immunogenicity, India, measles-mumps-rubella-varicella vaccine, safety, vaccination schedule
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on January 4, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-007202 on 11 S
eptember 2015. D
ownloaded from

For peer review only
1
\
Title page 1
Title: Immunogenicity and safety of early vaccination with two doses of a combined measles-2
mumps-rubella-varicella vaccine in healthy Indian children from 9 months of age: a phase III, 3
randomized, non-inferiority trial. 4
Authors: Sanjay Lalwani, Vice Principal, Professor and Head of Departmenta, Sukanta 5
Chatterjee, Professor of Pediatricsb, Sundaram Balasubramanian, Senior Pediatric Consultant
c, 6
Ashish Bavdekar, Associate Professor and Consultant Pediatric Gastroenterologistd, Shailesh 7
Mehta, Area Medical Leader (South Asia)e, Sanjoy Datta, VP, Clinical R&D and Medical Affairs
f, 8
Michael Povey, Biostatisticianf, Ouzama Henry, Clinical Research Development Lead
g 9
Affiliations: aDepartment of Pediatrics, Bharati Vidyapeeth Deemed University, Pune 411043, 10
India 11
bDepartment of Pediatrics, Medical College Kolkata, 88 College street, Kolkata 700073, India 12
cKanchi Kamakoti Childs Trust Hospital, 12-A, Nageswara Road, Nungambakkam, Chennai 13
600034, India 14
dDepartment of Pediatrics, KEM Hospital, 489 Rasta Peth, Sardar Moodliar Road, Pune 411011, 15
India 16
eGSK Pharmaceuticals Ltd., Dr. Annie Besant Road, Worli, Mumbai 400030, India 17
fGSK Vaccines, Avenue Fleming 20, B-1300 Wavre, Belgium 18
gGSK Vaccines, 2301 Renaissance Boulevard, RN 0220, P.O. Box 61540, King of Prussia, PA 19
19406-2772, USA 20
Correspondence to: Sanjay Lalwani 21
Page 1 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
2
\
Contact Details: +91 9822051716 22
Fax: +91 20 24364308 23
Email: [email protected] 24
Short title: Combined MMRV vaccine in Indian children 25
Abbreviations 26
ATP–according-to-protocol; CCID50–median cell culture infective dose; CI–confidence interval; 27
CRS–congenital rubella syndrome; ELISA–enzyme-linked immunosorbent assay; GMT–28
geometric mean titer; IAP–Indian Academy of Pediatrics; mIU/mL–milli international unit per 29
milliliter; MMR–combined measles-mumps-rubella vaccine; MMR+V–coadministration of MMR 30
and V; MMRV–combined measles-mumps-rubella-varicella vaccine; pfu–plaque forming units; 31
SAE–serious adverse event; TVC–total vaccinated cohort; V–varicella; VZV–varicella zoster-32
virus; WHO–World Health Organization 33
Keywords: immunogenicity, India, measles-mumps-rubella-varicella vaccine, safety, vaccination 34
schedule 35
Word count: 3521 36
Page 2 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
3
\
Abstract 37
Objective: This study (NCT00969436) compared the immunogenicity and safety of measles-38
mumps-rubella (MMR) followed by MMR+varicella (V) vaccines to (1) two doses of combined 39
MMRV and (2) MMR followed by MMRV, in Indian children. 40
Design: Phase III, open, randomized, non-inferiority study. 41
Setting: Six tertiary care hospitals located in India. 42
Participants: Healthy subjects aged 9–10 months not previously vaccinated against/exposed to 43
measles, mumps, rubella and varicella or without a history of these diseases. 44
Interventions: Subjects were randomized (2:2:1) to receive two doses of either MMRV 45
(MMRV/MMRV group) or MMR followed by MMRV (MMR/MMRV group) or MMR followed by 46
MMR+V (MMR/MMR+V, control group) at 9 and 15 months of age. Antibody titers against 47
measles, mumps and rubella were measured using ELISA and against varicella using an 48
immunofluorescence assay. 49
Main outcome measures: To demonstrate non-inferiority of the two vaccination regimens vs. 50
the control in terms of seroconversion rates, defined as a group difference with a lower bound 51
of the 95% confidence interval >-10% for each antigen, 43-days post-dose-2. Parents/guardians 52
recorded solicited local and general symptoms for a 4-day and 43-day period after each vaccine 53
dose, respectively. 54
Results: The seroconversion rates post-dose-1 ranged from 87.5%–93.2% for measles, 83.3%–55
86.1% for mumps and 98.7%–100% for rubella across the three vaccine groups. Seroconversion 56
rates post-dose-2 for measles, mumps and rubella was 100% and at least 95.8% for varicella 57
Page 3 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
4
\
across the three vaccine groups. Non-inferiority of MMRV/MMRV and MMR/MMRV to 58
MMR/MMR+V was achieved for all antigens, 43-days post-dose-2. The three vaccination 59
regimens were generally well-tolerated in terms of solicited local and general symptoms. 60
Conclusion: The immune responses elicited by the MMRV/MMRV and MMR/MMRV vaccination 61
regimens were non-inferior to those elicited by the MMR/MMR+V regimen for all antigens. The 62
three vaccination schedules also exhibited an acceptable safety profile in Indian children. 63
Abstract word count: 295/300 64
Trial registration: (NCT00969436)65
Page 4 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
5
\
Article Summary 66
• Measles, mumps, rubella (MMR) and varicella are highly infectious vaccine-preventable 67
childhood diseases with high mortality rates in India. 68
• A combined MMR-varicella vaccine may potentially facilitate the control of all four 69
diseases which is as immunogenic as separate MMR and varicella vaccinations. 70
Strengths and limitations of this study 71
• This Indian study provides data for the first time on: 72
• A combined MMRV vaccine in a highly endemic measles setting. 73
• MMRV administered to children at 9 months of age which aligns with the 74
expanded programme of immunization schedule of measles vaccine administered 75
at this age. 76
• Prevaccination serostatus that offers epidemiological indicators on the early 77
disease burden for measles, mumps, rubella and varicella 78
• Limitations of study: The six tertiary care centres where the study was conducted are 79
not representative of the entire Indian population, investigator-bias while reporting AEs 80
due to the the open design of the study, and there were no adjustments made for 81
confounding factors (eg: centers) in the analysis. 82
83
Page 5 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
6
\
Introduction 84
Measles, mumps, rubella and varicella are highly infectious vaccine-preventable childhood 85
diseases that continue to pose a significant public health problem in India and beyond.1-4
In 86
2010, global measles mortality was estimated at 139,000 (71,200–447,800) deaths, 47% of 87
which was estimated to have occurred in India.5 In 2011, large measles outbreaks were 88
reported in India (29,339 cases), Pakistan (4,386 cases), Nigeria (18,843 cases) and other 89
countries.6 Although measles elimination was declared in the United States in 2000, the 90
importation of the disease led to the highest number of cases in 2011 (220 cases) since 1996 91
while 159 cases were reported in 2013 by 16 states.7 In the European Union, the Dutch 92
authorites reported 1540 measles cases since May 2013 and in Germany, the reported number 93
of cases is nearly 10 times higher than the total cases in 2012.8 A large number of confirmed 94
cases of measles was also reported in England and Wales between 2012 and 2013, 95
respectively.9 10
Thus, even developed settings may be prone to epidemics if coverage wanes.7-
96
10 97
A dramatic decrease in the worldwide mumps disease burden has been observed since the 98
implementation of large-scale immunization in 1967.2 However, the true incidence in India is 99
difficult to ascertain due to limited baseline epidemiological data.11
100
A study conducted in 2006 revealed that 82.2% children aged between 1 and 5 years, and 101
13.5% aged between 10 and 15 years are susceptible to rubella in the state of Tamil Nadu in 102
southern India.12
Although congenital rubella syndrome (CRS) has been reported in most parts 103
of India, no measures have been undertaken to control this crippling disease and presently, 104
reliable data on CRS in India is limited.13
105
Page 6 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
7
\
Epidemiological data on varicella-zoster virus (VZV) are also scarce in India as chickenpox was 106
not a notifiable disease in India until 200514
and due to the locally-perceived self-limiting and 107
relatively less severe nature, the disease is under-reported.
108
Globally, routine and effective vaccination has been identified as a critical approach towards 109
achieving high and sustained vaccination coverage rates and to strategically deal with the 110
burden of these four diseases.15
Consequently, the Indian Academy of Pediatrics (IAP) has 111
recommended the inclusion of a combined measles-mumps-rubella vaccine (MMR) in the 112
national immunization schedule to provide protection against CRS and also to reduce the 113
disease burden of measles and mumps.16
In countries with ongoing measles transmission, the 114
World Health Organization (WHO) recommends a first dose of measles vaccine at 9 months of 115
age to afford early protection and second dose at 15–18 months with a minimum interval of 116
one month between the two doses.1 In India, the observed high morbidity and mortality due to 117
measles has necessitated the administration of the measles vaccine at 9 months of age (by 118
which time most children will have lost their maternal antibodies to measles)17
followed by 119
MMR at 15 months of age.18
The IAP also recommends two doses of a varicella vaccine, with 120
the first dose administered at 15 months of age.18
The second dose may be administered three 121
months after the first, but is usually given at 4–6 years.18
There is increasing global evidence in 122
many settings that the high economic burden of varicella would be beneficially alleviated with 123
the inclusion of varicella vaccine.19-21
124
GSK’s MMR and varicella vaccines are available in over 100 countries22
and 80 countries,23
125
respectively. These vaccines are currently not included in the Indian national (government-126
provided) immunization program; however, they are available via private practitioners. Based 127
Page 7 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
8
\
on commercially available formulations, a combined MMR-varicella vaccine (MMRV) has been 128
developed to not only realize the benefits of vaccination against measles, mumps and rubella, 129
but also to facilitate the potential inclusion of varicella into national immunization programs.24-
130
27 The new vaccine is as immunogenic as separate MMR and varicella vaccinations.
28-30 131
This study evaluated the non-inferiority of two different vaccination regimens of the new 132
MMRV vaccine to the control regimen of separate injections when the vaccines were 133
administered at 9 and 15 months of age to healthy Indian children. 134
135
Page 8 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
9
\
Methods 136
Study design and subjects 137
This phase IIIb, open, randomized, controlled study (NCT00969436) was conducted at six 138
tertiary care centers (Supplementary table) in India between November 2009 and February 139
2011. The open nature of the study implied that both the investigators and the 140
parents/guardians were aware of the treatment, however the lab personnel generally were 141
unaware of the treatment allocation. Healthy subjects aged 9–10 months were randomized 142
(2:2:1) to receive either two doses of the MMRV vaccine (MMRV/MMRV group) or MMR 143
followed by MMRV (MMR/MMRV group), or MMR followed by MMR+V (MMR/MMR+V group; 144
control) at 9 and 15 months of age. The control regimen largely reflects the optimum standard 145
of care available in India under the IAP recommendations.18
146
Among the six centers, the center in Bangalore did not enroll subjects according to the 147
randomization scheme and enrollment ceased at a small number of subjects because the 148
investigator was transferred (Supplementary table). Subjects were excluded from the study if 149
they had received any investigational drug/vaccine 30 days before the study vaccine or 150
immunosuppressants/immune-modifying drugs/blood products six months before the study. 151
Subjects previously vaccinated against/exposed to measles, mumps, rubella and varicella or 152
with a history of these diseases could not participate. A history of allergy likely to be aggravated 153
by any of the vaccine components, neurological disease/seizures, chronic illness or family 154
history of immunodeficiency, or symptoms of acute illness at the time of enrollment were other 155
reasons for exclusion. Vaccination was postponed for subjects with a rectal temperature 156
≥38.0°C/an axillary temperature ≥37.5°C. Subjects were also excluded if they lived in a 157
Page 9 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
10
\
household with newborn infants or pregnant women who have not contracted chickenpox 158
previously or immunocompromised individuals. 159
The study adhered to Good Clinical Practice, the Declaration of Helsinki, and all applicable 160
regulations. The participating centers’ Institutional Ethics Committees/Institutional Review 161
Boards31
reviewed and approved the protocol. Parents/guardians provided written informed 162
consent before performing any study-related procedures. 163
Study Vaccines 164
All study vaccines: MMR (Priorix™), varicella (Varilrix™) and MMRV (Vammrix™ [same as Priorix-165
Tetra™]) were manufactured by GSK, Belgium. The minimum expected potencies for measles, 166
rubella and varicella were identical between the MMR+V and MMRV vaccines.30
The minimum 167
expected potency for the mumps content was higher in the MMRV vaccine (≥104.4
median cell 168
culture infective dose [CCID50]) than in the MMR vaccine (≥103.7
CCID50). The vaccines supplied 169
in monodose vials contained a freeze-dried pellet which was reconstituted with the diluent 170
(provided in a pre-filled syringe) before subcutaneous injection into the anterolateral thigh. 171
Immunogenicity assessment 172
Blood samples were collected at pre-vaccination and 43 days after doses one and two. Antibody 173
titers were measured using a commercial enzyme-linked immunosorbent assay (ELISA; 174
Enzygnost™, Dade Behring, Marburg, Germany) with cut-off values of 150 mIU/mL (measles), 175
231 U/mL (mumps), and 4 IU/mL (rubella). For varicella, antibody titers were measured using 176
an immunofluorescence assay (Virgo™, Hemagen Diagnostics, Columbia, MD, USA) (assay cut-177
off value of 4 dilution-1
). 178
Page 10 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
11
\
Safety/Reactogenicity assessment 179
Parents/guardians used diary cards to record the occurrence of solicited local symptoms (pain, 180
redness and swelling at the injection site) for 4 days after each dose and solicited general 181
symptoms (fever [axillary temperature ≥37.5°C/rectal temperature ≥38°C], rash/exanthema, 182
parotid/salivary gland swelling and any suspected signs of meningeal irritation, including febrile 183
convulsions) for 43 days after each dose. Body temperature was measured daily via the 184
rectal/axillary route for 15 days after each vaccination. Between days 15 and 42, the presence 185
of fever was monitored using a temperature-sensitive pad,32
and if fever was suspected, 186
temperature was accurately measured with a thermometer. There were two follow-up visits 187
with the investigator at each study center, one vist 42–56 days following each vaccine 188
administration. During these visits, diary cards were returned to the investigator for 189
assessment. 190
Unsolicited symptoms were recorded for 43 days after each dose and the occurrence of serious 191
adverse events (SAEs) was recorded throughout the study. Intensity of symptoms was graded 192
on a scale of 0–3. Grade 3 solicited symptoms were defined as: pain: child cried when limb was 193
moved or a spontaneously painful limb; redness and swelling: injection site surface diameter 194
>20 mm; fever: axillary temperature >39°C/rectal temperature >39.5°C. Unsolicited symptoms 195
(including SAEs) were defined as grade 3 when they prevented normal daily activity. 196
Statistical Analyses 197
All statistical analyses were performed using SAS version 9.2, and 95% confidence intervals (CI) 198
were calculated using Proc StatXact 8.1. The sample size was estimated taking into 199
consideration the co-primary objectives of non-inferiority. Non-inferiority was achieved if the 200
Page 11 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
12
\
lower limit of the two-sided standardized asymptotic 95% CI for the difference in 201
seroconversion rates between the two treatment groups and control group (MMRV/MMRV 202
minus MMR/MMR+V; MMR/MMRV minus MMR/MMR+V) was ≥-10% for each vaccine antigen, 203
43 days post-dose-2. Similarly, the secondary non-inferiority objective was achieved if the lower 204
limit of the two-sided standardized asymptotic 95% CI for the difference in seroconversion rates 205
between the MMRV/MMRV group and pooled MMR results from the MMR/MMRV and 206
MMR/MMR+V groups, 43 days post-dose-1 was ≥-10% for measles, mumps and rubella. 207
Considering that up to 25% of the subjects enrolled could be non-evaluable, a total of 450 208
subjects (180 subjects in each of the treatment groups and 90 subjects in the control group) 209
were to be enrolled in the study. A sample size of 130 evaluable subjects in each treatment 210
group and 65 evaluable subjects in the control group was planned, which gave a power of at 211
least 93.91% with a non-inferiority margin of 10% for all antigens to meet the co-primary 212
objectives. A central randomization system using a minimization algorithm provided each child 213
with a unique treatment number. A randomization (2:2:1) blocking scheme ensured that the 214
balance between treatments was maintained by providing a unique treatment number that 215
identified the vaccine dose to be administered to the subjects. Furthermore, given different 216
physical characteristics of the study vaccines and the number of injections between study 217
groups, the study was conducted in an open manner where in the treatment allocation of 218
subjects was known to the investigators and the parents/guardians. 219
Immunogenicity analysis was performed on the according-to-protocol (ATP) cohort which 220
included all subjects for whom pre- and post-vaccination serology results were available and 221
who complied with study procedures. Seroconversion rates (defined as the appearance of 222
Page 12 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
13
\
antibodies [i.e. antibody concentration/titer ≥cut-off value] in the serum of subjects who were 223
seronegative before vaccination) and geometric mean titers (GMTs) were calculated with exact 224
95% CIs for antibodies against each vaccine antigen after each dose. The 95% CIs for the GMTs 225
were obtained by exponential transformation of the 95% CI for the mean of log-transformed 226
titer. 227
Safety analysis was performed on the total vaccinated cohort (TVC) which included all 228
vaccinated subjects. Solicited and unsolicited symptoms reported for the subjects during the 229
respective post-vaccination periods were calculated with exact 95% CIs. All SAEs reported 230
during the entire conduct of the study were described. 231
232
Page 13 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
14
\
Results 233
Demographics 234
All 450 subjects enrolled in the study were vaccinated and included in the TVC: MMRV/MMRV 235
(n=180); MMR/MMRV (n=180) and MMR/MMR+V (n=90). Of these, 382 subjects were included 236
in the ATP cohort for immunogenicity: MMRV/MMRV (n=151); MMR/MMRV (n=156) and 237
MMR/MMR+V (n=75) (Figure 1). The median age of subjects in the ATP was 9 months (range: 238
9–10 months); 51.7% were male and all subjects were Indian. No demographic variations were 239
observed between the study groups (Supplementary table). 240
Immunogenicity 241
The proportion of initially seropositive subjects for measles, mumps and rubella was <2.7% in 242
all three groups. For varicella, 7.4% subjects in the MMRV/MMRV group, 8.3% in the 243
MMR/MMRV group and 2.7% in the MMR/MMR+V group were initially seropositive. After 244
dose-1, the seroconversion rates ranged from 87.5%–93.2% for measles, 83.3%–86.1% for 245
mumps and 98.7%–100% for rubella (Table 1). Post-dose-2 seroconversion rates were 100% for 246
measles, mumps and rubella and were at least 95.8% for varicella. Across the three vaccination 247
groups, the observed GMTs to measles, mumps and rubella increased between doses one and 248
two (Table 1). The co-primary objectives of non-inferiority with respect to seroconversion rates 249
43 days after dose-2 were achieved for all vaccine antigens, i.e. the lower bounds of the 95% CIs 250
for the difference in seroconversion rates between groups (MMRV/MMRV vs MMR/MMR+V; 251
MMR/MMRV vs MMR/MMR+V) was ≥-10%. 252
253
Page 14 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
15
\
Table 1 Seroconversion rates and Antibody GMTs of the MMRV/MMRV, MMR/MMRV and MMR/MMR+V groups 43 days post-254
vaccination (ATP cohort) 255
Antigen MMRV/MMRV group (N=151) MMR/MMRV group (N=156) MMR/MMR+V group (N=75)
Dose Na
SCb (%)
c (95% CI) GMT
d (95% CI) N
a SC
b (%)
c (95% CI) GMT
d (95% CI) N
a SC
b (%)
c (95% CI) GMT
d (95% CI)
Measles Pre-dose* 2 1.3 - 3 1.9 - 2 2.7 -
Post-dose-
1
148 93.2 (87.9; 96.7) 2013.6 (1662.2; 2439.3) 153 88.2 (82.0; 92.9) 1180.4 (963.0; 1446.7) 72 87.5 (77.6; 94.1) 1200.0 (887.9; 1621.8)
Post-dose-
2
149 100 (97.6; 100) 4471.3 (3975.3; 5029.2) 153 100 (97.6; 100) 3358.7 (3017.5; 3738.4) 72 100 (95.0; 100) 2495.0 (2064.5; 3015.2)
Mumps Pre-dose* 2 1.3 - 3 1.9 - 2 2.7 -
Post-dose-
1
144 86.1 (79.4; 91.3) 991.9 (819.7; 1200.3) 152 84.2 (77.4; 89.6) 746.6 (628.0; 887.6) 72 83.3 (72.7; 91.9) 775.1 (600.9; 999.7)
Page 15 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
16
\
Post-dose-
2
149 100 (97.6; 100) 6428.0 (5774.9; 7154.9) 152 100 (97.6; 100) 10108.5 (9223.9; 11078.0) 72 100 (95.0; 100) 4925.3 (4200.9; 5774.7)
Rubella Pre-dose* 1 0.7 - 4 2.6 - 2 1.7 -
Post-dose-
1
149 98.7 (95.2; 99.8) 45.4 (38.3; 53.7) 152 99.3 (96.4; 100) 63.8 (55.9; 72.8) 73 100 (95.1; 100) 62.0 (51.3; 74.9)
Post-dose-
2
150 100 (97.6; 100) 148.4 (136.1; 161.8) 152 100 (97.6; 100) 164.8 (152.1; 178.6) 73 100 (95.1; 100) 173.0 (153.0; 195.6)
Varicella Pre-dose* 11 7.4 - 13 8.3 - 2 2.7 -
Post-dose-
1
138 94.2 (88.9; 97.5) 120.5 (90.8; 160.0) 142 2.8 (0.8; 7.1) 2.2 (2.0; 2.4) 72 1.4 (0.0; 7.5) 2.2 (1.8; 2.6)
Post-dose-
2
138 100 (97.4; 100) 5318.5 (4318.7; 6549.8) 143 98.6 (95.0; 99.8) 198.0 (158.2; 247.7) 72 95.8 (88.3; 99.1) 128.0 (91.7; 178.7)
*Pre-dose values refer to baseline seropositivity rates before vaccination 256
a Number of children initially seronegative with available results 257
Page 16 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
17
\
b Seroconversion 258
c Percentage of children that seroconverted for each antigen 259
d Geometric mean titers 260
The secondary objective of non-inferiority of the MMRV/MMRV group and pooled MMR results from the MMR/MMRV and 261
MMR/MMR+V groups in terms of seroconversion rates 43-days post-dose-1 for measles, mumps and rubella was also achieved (Table 262
2). 263
Table 2 Post-dose-1 seroconversion rates between the MMRV/MMRV group and pooled MMR/MMRV + MMR/MMR+V groups (ATP 264
cohort) 265
MMRV MMR
Antibody (MMRV/MMRV group) (Pooled
[MMR/MMRV] +
[MMR/MMR+V]
groups)
Difference in percentage (MMRV
minus MMR)
Na
%b
Na
%b
%c (95% CI)
Page 17 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
18
\
MMRV MMR
Antibody (MMRV/MMRV group) (Pooled
[MMR/MMRV] +
[MMR/MMR+V]
groups)
Difference in percentage (MMRV
minus MMR)
Na
%b
Na
%b
%c (95% CI)
Measles 148 93.2 225 88.0 5.24 (-1.06; 11.13)
Mumps 144 86.1 224 83.9 2.18 (-5.66; 9.42)
Rubella 149 98.7 225 99.6 -0.90 (-4.36; 1.29)
Varicella 138 94.2 - - -
a Number of children initially seronegative with available results 266
b Percentage of children that seroconverted for each antigen 267
Page 18 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
19
\
c Difference in percentage of children that seroconverted for each antigen between the MMMR/MMRV group and the pooled MMR results from the (MMR/MMRV 268
+ MMR/MMR+V) groups 269
Safety and Reactogenicity 270
During the 43-day post-vaccination period, the occurrence of solicited and unsolicited symptoms ranged between 51.1%–56.1% after 271
dose-1 and 36.2%–37.3% after dose-2 across the three vaccine groups. During the 4-day post-dose-1 follow-up period, injection site 272
pain was the most commonly reported solicited local symptom: MMRV/MMRV (11.5%), MMR/MMRV (7%) and MMR/MMR+V (10.7%). 273
Post-dose-2, injection site symptoms were reported by fewer than 6.5% of subjects (Table 3). Redness was the grade 3 local symptom 274
reported by 3 subjects (1.9%) in the MMRV/MMRV group, post-dose-2. 275
Fever was the most commonly reported solicited general symptom in all three vaccine groups during the 43-day post-vaccination 276
follow-up period after each dose (Table 3). The observed incidence of fever across all vaccine groups decreased between doses one and 277
two during the 15-day and 43-day post-vaccination follow-up periods (Table 3). 278
279
280
281
282
Page 19 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
20
\
Table 3 Incidence of solicited local symptoms (during the 4-day) and fever (during the 15-day and 43-day) post-vaccination period 283
(Total vaccinated cohort) 284
MMRV/MMRV group MMR/MMRV group MMR/MMR+V group
Dose-1 Na=174;
Dose-2 Na=155
Dose-1 Na=172;
Dose-2 Na=159
Dose-1 Na=84;
Dose-2 Na=79
%b
(95% CI) %b
(95% CI) %b
(95% CI)
Pain Post-dose-1 11.5 (7.2; 17.2) 7.0 (3.7; 11.9) 10.7 (5.0; 19.4)
Post-dose-2 5.8 (2.7; 10.7) 6.3 (3.1; 11.3) 3.8 (0.8; 10.7)
Redness Post-dose-1 8.6 (4.9; 13.8) 4.7 (2.0; 9.0) 3.6 (0.7; 10.1)
Post-dose-2 6.5 (3.1; 11.5) 3.8 (1.4; 8.0) 0.0 (0.0; 4.6)
Swelling Post-dose-1 4.6 (2.0; 8.9) 2.9 (1.0; 6.7) 3.6 (0.7; 10.1)
Post-dose-2 5.8 (2.7; 10.7) 3.8 (1.4; 8.0) 0.0 (0.0; 4.6)
Page 20 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
21
\
Fever (15 days
post-dose-1)
Any 32.2 (25.3;39.7) 28.5 (21.9; 35.9) 21.7 (13.4; 32.1)
Grade 3
(>39.5°C)
3.4 (1.3; 7.4) 1.7 (0.4; 5.0) 1.2 (0.0; 6.5)
Related 28.2 (21.6; 35.5) 24.4 (18.2; 31.5) 16.9 (9.5; 26.7)
Medical Advice 6.3 (3.2; 11.0) 7.6 (4.1; 12.6) 2.4 (0.3; 8.4)
Fever (15 days
post-dose-2)
Any 17.4 (11.8;24.3) 13.2 (8.4; 19.5) 15.2 (8.1; 25.0)
Grade
3(>39.5°C)
1.3 (0.2; 4.6) 1.3 (0.2; 4.5) 0.0 (0.0; 4.6)
Related 13.5 (8.6; 20.0) 11.9 (7.4; 18.0) 12.7 (6.2; 22.0)
Medical Advice 3.9 (1.4; 8.2) 1.3 (0.2; 4.5) 1.3 (0.0; 6.9)
Any 43.7 (36.2; 51.4) 40.7 (33.3; 48.4) 32.5 (22.6; 43.7)
Grade 6.3 (3.2; 11.0) 2.9 (1.0; 6.7) 1.2 (0.0; 6.5)
Page 21 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
22
\
Fever (43 days
post-dose-1)
3(>39.5°C)
Related 30.5 (23.7; 37.9) 27.9 (21.3; 35.2) 18.1 (10.5; 28.0)
Medical Advice 13.8 (9.0; 19.8) 16.9 (11.6; 23.3) 4.8 (1.3; 11.9)
Fever (43 days
post-dose-2)
Any 26.5 (19.7; 34.1) 23.3 (16.9; 30.6) 27.8 (18.3; 39.1)
Grade
3(>39.5°C)
1.3 (0.2; 4.6) 3.8 (1.4; 8.0) 2.5 (0.3; 8.8)
Related 14.2 (9.1; 20.7) 13.2 (8.4; 19.5) 12.7 (6.2; 22.0)
Medical Advice 4.5 (1.8; 9.1) 5.6 (2.6; 10.5) 7.6 (2.8; 15.8)
a Number of children with at least one documented dose 285
b Percentage of children reporting the symptom at least once 286
Page 22 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
23
An absence of a clear peak in the prevalence of fever during the 43-day period after dose-1 for 287
all three vaccine groups is depicted in Figure 2(a). Post-dose-2 fever is depicted in Figure 2(b). 288
Rash occurred in one subject after the first dose of MMRV in the MMRV/MMRV group as 289
compared to three subjects after the first MMR dose (MMR/MMRV [n=2]; MMR/MMR+V [n=1]) 290
groups). Only one subject developed rash after dose-2 in the MMR/MMRV group. There were 291
no reports of meningeal irritation, febrile convulsions or parotid gland swelling during the 43-292
day period after each vaccine dose. 293
At least one unsolicited symptom was reported in 20.6% subjects after the first dose of MMRV 294
in the MMRV/MMRV group and in 21.7% and 20.0% subjects after the first dose of MMR in the 295
MMR/MMRVand MMR/MMR+V groups, respectively. The most commonly reported symptoms 296
in each group were: upper respiratory tract infection in the MMRV/MMRV group (n=10; 5.6%); 297
cough in the MMR/MMRV group (n=10; 5.6%) and nasopharyngitis, rhinitis and cough in the 298
MMR/MMR+V group (n=6; 6.7% for each symptom). Similarly, at least one unsolicited symptom 299
was reported in 10.6% subjects after the second dose of MMRV in the MMRV/MMRV group, in 300
10.0% subjects who received their first dose of MMRV in the MMR/MMRV groups and in 12.2% 301
subjects following dose-2 of MMR+V in the MMR/MMR+V group. The most commonly reported 302
symptoms in each group were: rhinitis and cough in the MMRV/MMRV group (n=6; 3.3% for 303
each symptom) and rhinitis in the MMR/MMRV (n=7; 3.9%) and MMR/MMR+V groups (n=5; 304
5.6%). 305
Overall, 18 SAEs occurred in the study. At least one SAE occurred in 13 subjects (MMRV/MMRV 306
[n=7]; MMR/MMRV [n=6]; MMR/MMR+V [n=0] groups). The most commonly reported SAEs 307
were lower respiratory tract infection (in two subjects) in the MMRV/MMRV group, and 308
Page 23 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
24
gastroenteritis (in three subjects) in the MMR/MMRV group. Other SAEs reported were 309
gastroenteritis, pneumonitis, wheezing, viral infection, pneumonia, febrile convulsion, upper 310
respiratory tract inflammation, dehydration and bronchiolitis. All SAEs resolved without 311
sequelae and were considered unrelated to vaccination. 312
313
Page 24 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
25
Discussion 314
This non-inferiority study evaluated the immunogenicity and safety of two vaccination regimens 315
(1) two-dose MMRV/MMRV (2) MMR followed by MMRV compared to a control group (MMR 316
followed by MMR+V) when administered to healthy Indian children at 9 and 15 months of age. 317
The co-primary non-inferiority criterion ruling out a 10% difference in seroconversion rates 318
post-dose-2 of MMRV/MMRV and MMR/MMRV compared to MMR/MMR+V was achieved for 319
all antigens, indicating that the immune responses elicited by the two vaccination regimens 320
were non-inferior to those elicited by the control regimen. Although the two-dose 321
MMRV/MMRV schedule is not included in several immunization programs, this regimen has 322
been established to be non-inferior to the two-dose MMR+V schedule in separate studies in 323
Germany and Singapore.30 33
Additionally, on comparing the post-dose-1 responses, one dose of 324
MMRV in the MMRV/MMRV group elicited non-inferior immune responses against measles, 325
mumps and rubella compared to pooled results of one dose of MMR in the MMR/MMRV and 326
MMR/MMR+V groups. 327
In the three vaccine groups, we observed low baseline seropositivity rates (<2.7%) for measles, 328
mumps and rubella in subjects at 9 months of age. This finding suggests a possible decline in 329
circulating maternal antibodies and measles infection by this age which would support 9 330
months as a suitable age for initial vaccination. However, it should be noted that this finding is 331
inconsistent with a notable Indian study conducted approximately a decade ago that suggested 332
the persistence of high circulating maternal antibodies at 9 months of age with baseline 333
seropositivity rates of 15% for measles and 20% each for mumps and rubella.11
Additionally, 334
while lowering the measles vaccination age in low income countries is supported by many, 335
Page 25 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
26
vaccinating at 9 months or earlier may mean that the immune system has not reached 336
optimum maturity to mount an effective response and provide effective long-term protection 337
against measles or the other diseases with just a single vaccine dose.34 35
The seroconversion 338
rates for all antigens in the MMRV/MMRV group were consistent with previous observations in 339
Singaporean children at 9 months of age by Goh et al.33
However, with a first dose of MMR, the 340
observed post-dose-1 seroconversion rates to measles (MMR/MMRV=88.2%; 341
MMR/MMR+V=87.5%) and mumps (MMR/MMRV=84.2%; MMR/MMR+V=83.3%) in this study 342
were somewhat lower than those reported by Schuster et al, following administration of a first 343
dose of MMR to children aged 11–21 months in Germany (measles: 93.4%; mumps: 93.6%).30
A 344
contrast in immune responses between the current and German study may be attributed to the 345
age at vaccination, maturity of the immune system and circulating maternal antibodies. Also, 346
the higher GMTs oberved to measles in the MMRV/MMRV group compared to the 347
MMR/MMRV and MMR/MMR+V groups could translate to more effective protection in a highly 348
endemic measles environment where coverage from a second dose of a measles-containing 349
vaccine remains variable throughout the country.6 Lower seroconversion rates with other live-350
attenuated vaccines (such as the oral polio vaccine and the rotavirus vaccine) have also been 351
observed in India and South Asia compared to more industrialized settings.36-38
352
Nevertheless, we observed high seroconversion rates for all vaccine antigens following 353
administration of second vaccination at 15 months of age, indicating that an early two-dose 354
immunization strategy when the first dose is administered as early as 9 months elicits a 355
satisfactory immune response. An interesting observation was the markedly high GMT against 356
mumps post-dose-2 in the MMR/MMRV (10108.5) group compared to the MMR/MMR+V 357
Page 26 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
27
(4925.3) and MMRV/MMRV (6428.0) groups. This observation has not been reported previously 358
despite the higher mumps antigen content in the MMRV vaccine when compared to the MMR 359
vaccine and studies that evaluate this finding may be needed in the future. 360
Early administrations of all three vaccination regimens were well-tolerated when administered 361
to young children at 9 and 15 months of age. Similar differences in solicited general symptoms 362
have been observed in studies conducted in the Indian subcontinent with other live attenuated 363
viral vaccines (such as Rotarix™) compared with other countries.37 39
Notably, unlike previous 364
studies conducted in other countries,28-30 33
this study did not demonstrate any difference in 365
fever rates between MMRV and MMR when used as a first dose of measles-containing vaccine. 366
Although this may be related to the epidemiological context in India, which differs from 367
developed countries, the reason is unclear. In general, the reporting rate of fever was also 368
lower than that seen in other studies.28-30 33
Again, this may be due to the younger age of 369
children enrolled, or the presence of maternal antibodies, which may have limited measles 370
virus replication post-dose-1, resulting in the blunting of immune response and fever response 371
rates; or cross-cultural/geographical differences in the reporting of symptoms. Further data 372
may be needed to determine if there is in fact a difference in the reactogenicity profile between 373
developed and developing countries. 374
It is possible to eliminate measles from a specific region by sustaining high immunization 375
coverage as is evident from Latin America, Finland and the United States40-42
; countries such as 376
Finland have also successfully eliminated mumps and rubella using the MMR vaccine.41
In view 377
of the ongoing transmission and high mortality risk of measles in India, immunization coverage 378
of ≥95% for the first and second dose would be required to ensure prevention of measles virus 379
Page 27 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
28
transmission.43
Currently, the Indian national immunization schedule’s 9 months single dose 380
immunization coverage is 74%44
; however, as this represents the average, coverage rates in 381
some parts of the country may be even lower. Several European countries, where the first 382
MMR dose is administered to children in the second year of life (12–24 months), continue to 383
face a relatively low immunization coverage rates resulting in measles and mumps outbreaks,24
384
as was recently observed even in South Wales.10
An earlier vaccination schedule was 385
implemented in Germany as a result of such outbreaks, whereby the first dose is now 386
administered at 11–14 months followed by the second dose at 15–23 months of age.24
This 387
revised strategy achieved well-documented successful immunization coverage rates,24
and 388
highlights the importance of early vaccination with increased compliance and subsequently 389
higher coverage rates. 390
A few limitations of the study that should be considered: (1) the six tertiary care centers where 391
the study was conducted are not representative of the entire Indian population, (2) 392
investigator-bias while reporting AEs due to the the open design of the study, and (3) there 393
were no adjustments made for confounding factors (eg: centers) in the analysis.
394
Conclusion 395
This study demonstrates that in an Indian setting, the two-dose vaccination regimens of 396
MMRV/MMRV and MMR/MMRV are non-inferior to the control MMR/MMR+V regimen (i.e. 397
the local standard of care recommended by the IAP)17
in terms of immunological response. 398
Both vaccination schedules demonstrated an acceptable safety profile when administered to 399
healthy Indian children at 9 and 15 months of age. Introduction of the MMRV vaccine may not 400
Page 28 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
29
only facilitate effective population protection against measles, but against three other common 401
childhood viral infectious diseases: mumps, rubella and varicella.
402
403
Page 29 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
30
Trademarks 404
Vammrix, Priorix-Tetra, Priorix, Varilrix and Rotarix are registered trademarks of 405
GlaxoSmithKline group of companies. 406
Virgo is a registered trademark of Hemagen Diagnostics, Columbia, MD, USA. 407
Enzygnost is a registered trademark of Dade Behring, Marburg, Germany. 408
Contributors: SL, SB, SC and AB were involved in the recruitment of subjects. SL critically 409
reviewed the protocol and study report and also provided scientific and medical inputs during 410
the development of the study report. SB was involved in providing scientific and medical inputs 411
to the protocol and critically reviewing the protocol. SC coordinated and supervised data 412
collection at one site and carried out the initial analyses. AB provided critical inputs to the study 413
report and reviewed the content of the study report. SM and SD conceptualized and designed 414
the study. SM also supervised data collection at all sites. MP was involved in data analysis and 415
interpretation. SD and OH provided input to the interpretation of clinical data. 416
All authors critically reviewed and revised the manuscript during the development and 417
approved the final version of the manuscript. All authors are guarantors and accept full 418
responsibility for the work and/or conduct of the study, had access to the data, and controlled 419
the decision to publish. 420
Funding: This study was sponsored and funded by GlaxoSmithKline Biologicals SA. 421
GlaxoSmithKline Biologicals SA was involved in all stages of the study conduct and analysis; and 422
also took charge of all costs associated with the development and the publishing of the 423
manuscript. 424
Page 30 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
31
Competing interests: All authors have completed the ICMJE uniform disclosure form at 425
www.icmje.org/coi_disclosure.pdf. SL declares to have received institutional grant (for BVDU 426
Medical college, Dept. of Pediatrics) and travel support for the meeting from GlaxoSmithKline 427
group of companies. He also declares to have received fees for lecture at Pedicon 2011. SB 428
declares that The childs trust medical research foundation received grant from GlaxoSmithKline 429
group of companies. AB declares to have received institutional grant for conducting this trial 430
and has pending institutional grants from GlaxoSmithKline group of companies for other 431
vaccine trials. He also declares to have received support for travel/accomodation while 432
participating in investigator meetings and renumeration for participating in a meeting on 433
adjuvants from GlaxoSmithKline group of companies. SM, SD, MP and OH are employees of 434
GlaxoSmithKline group of companies; SD and OH declare to have stock options. MP declares 435
that he received payment/fees for review of statistical analysis and reviewing this manuscript 436
from GlaxoSmithKline group of companies. SC has no conflict of interest. The authors have no 437
financial relationships relevant to this article to disclose. 438
Data sharing: Upon authorization or termination of development of this medicine, anonymized 439
patient-level data underlying this study will be made available to independent researchers, 440
subject to review by an independent panel, at www.clinicalstudydatarequest.com. Consent for 441
data sharing was not obtained from the participants, but the presented data are anonymized 442
and risk of identification is low. 443
Acknowledgements 444
The authors thank the study nurses and staff members involved, and the parents and children 445
who participated in the study. The authors acknowledge Dr. Sonali Palkar for her support in 446
Page 31 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
32
conducting the clinical trial and Dipti Phatarpekar for coodinating and supervising data 447
collection at two study sites. The authors also thank Ashmita Ravishankar for medical writing 448
and publication coordination (GlaxoSmithKline Vaccines), Jarno Jansen (Keyrus Biopharma for 449
GlaxoSmithKline Vaccines), Geetha Subramanyam (GlaxoSmithKline Vaccines) and Shruti MP 450
(GlaxoSmithKline Vaccines) for editorial assistance and publication coordination. 451
Trial registration: (NCT00969436) 452
453
Page 32 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
33
References: 454
1 World Health Organization. Measles vaccines. Wkly Epidemiol Rec 2009;84:349–60. 455
2 World Health Organization. Mumps virus vaccines. Wkly Epidemiol Rec 2007;82:49–60. 456
3 World Health Organization. Rubella vaccines. Wkly Epidemiol Rec 2011;86:301–16. 457
4 CDC. Prevention of varicella: Recommendations of the Advisory Committee on 458
Immunization Practices (ACIP). MMWR 2007;56(RR04):1–40. 459
5 Simons E, Ferrari M, Fricks J, et al. Assessment of the 2010 global measles mortality 460
reduction goal: results from a model of surveillance data. Lancet 2012;379:2173–8. 461
6 World Health Organization Media Centre. WHO: Measles deaths decline, but elimination 462
progress stalls in some regions. 2013. Avaiblat at: 463
http://www.who.int/mediacentre/news/notes/2013/measles_20130117/en/. Accessed 25 464
November, 2013. 465
7 Centers for Disease Control and Prevention (CDC). Measles – United States, January 1-466
August 24, 2013. MMWR Morb Mortal Wkly Rep 2013;62:741–3. 467
8 European Centre for Disease Prevention and Control. Monitoring current health threats, 468
week 39/2013: measles and possible polio re-emergence in focus. Available at: 469
http://ecdc.europa.eu/en/press/news/_layouts/forms/News_DispForm.aspx?List=8db7286470
c%2Dfe2d%2D476c%2D9133%2D18ff4cb1b568&ID=872&RootFolder=%2Fen%2Fpress%2Fn471
ews%2FLists%2FNews&Web=86661a14%2Dfb61%2D43e0%2D9663%2D0d514841605d. 472
Accessed 20 April, 2015. 473
9 Jacqui Wise. Measles outbreak hits northeast England. BMJ 2013;346:f662. 474
Page 33 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
34
10 Jacqui Wise. Largest group of children affected by measles outbreak in Wales is 10-18 year 475
olds. BMJ 2013;346:f2545. 476
11 Yadav S, Thukral R, Chakarvarti A. Comparative evaluation of measles, mumps & rubella 477
vaccine at 9 & 15 months of age. Indian J Med Res 2003;118:183–6. 478
12 Ramamurty N, Murugan S, Raja D, et al. Serosurvey of rubella in five blocks of Tamil Nadu. 479
Indian J Med Res 2006;123:51–4. 480
13 Verma R, Khanna P, Chawla S. Rubella vaccine: New horizon in prevention of congenital 481
rubella syndrome in India. Hum Vaccin Immunother 2012;8:1-3. 482
14 Verma R, Bairwa M, Chawla S, et al. Should the chickenpox vaccine be included in the 483
national immunization schedule in India? Hum Vaccin 2011;7:874–7. 484
15 World Health Organization. Wkly Epidemiol Rec 2011;86:437–44. 485
16 Singhal T, Amdekar YK, Thacker N. IAP Committee on Immunization. Indian Pediatrics 486
2007;44:390–2. 487
17 Verma R, Khanna P, Bairwa M, et al. Introduction of a second dose of measles in national 488
immunization program in India: A major step towards eradication. Hum Vaccin 489
2011;7:1109–11. 490
18 Indian Academy of Pediatrics Committee on Immunization (IAPCOI). Consensus 491
recommendations on immunization and IAP immunization timetable 2012. Indian Pediatrics 492
2012;49:549–64. 493
19 Ozdemir H, Candir MO, Karbuz A, et al. Chickenpox complications, incidence and financial 494
burden in previously healthy children and those with an underlying disease in Ankara in the 495
pre-vaccination period. Turk J Pediatr 2011;53:614–25. 496
Page 34 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
35
20 Bilcke J, Ogunjimi B, Marais C, et al. The health and economic burden of chickenpox and 497
herpes zoster in Belgium. Epidemiol Infect 2012;140:2096–109. 498
21 Da YP, Luo LY, Song LZ. [Economic burden of inpatient of varicella in Shandong, Gansu and 499
Hunan provinces, 2007]. Zhongguo Yi Miao He Mian Yi 2009;15:438–42. 500
22 Department of Health. Childhood immunizations guidance. Available at: 501
http://www.gov.im/lib/docs/health/Public_Health/Immunisation/imm010112immunisation502
bookletlress.pdf. Accessed 8 November, 2012. 503
23 Chiu SS, Lau Y-L. Review of the Varilrix™ varicella vaccine. Expert Rev Vaccines 2005;4:629–504
43. 505
24 Vesikari T, Sadzot-Delvaux C, et al. Increasing coverage and efficiency of measles, mumps, 506
and rubella vaccine and introducing universal varicella vaccination in Europe. A role for the 507
combined vaccine. Pediatr Infect Dis J 2007;26:632–8. 508
25 Rentier B, Gershon AA. European Working Group on Varicella. Consensus: varicella 509
vaccination of healthy children – a challenge for Europe. Pediatr Infect Dis J 2004;23:379–510
89. 511
26 Czajka H, Schuster V, Zepp F, et al. A combined measles, mumps, rubella and varicella 512
vaccine (Priorix-Tetra™): Immunogenicity and safety profile. Vaccine 2009;27:6504–11. 513
27 Knuf M, Faber J, Barth I, et al. A combination vaccine against measles, mumps, rubella and 514
varicella. Drugs Today 2008;44:279–92. 515
28 Nolan T, McIntyre P, Roberton D, et al. Reactogenicity and immunogenicity of a live and 516
attenuated tetravalent measles-mumps-rubella-varicella (MMRV) vaccine. Vaccine 517
2002;21:281–9. 518
Page 35 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
36
29 Knuf M, Habermehl P, Zepp F, et al. Immunogenicity and safety of two doses of tetravalent 519
measles-mumps-rubella-varicella vaccine in healthy children. Pediatr Infect Dis J 520
2006;25:12–8. 521
30 Schuster V, Otto W, Maurer L, et al. Immunogenicity and safety assessments after one and 522
two doses of a refrigerator-stable tetravalent measles-mumps-rubella-varicella vaccine in 523
healthy children during the second year of life. Pediatr Infect Dis J 2008;27;724–30. 524
31 Indian clinical trial registry. Available at: 525
http://ctri.nic.in/Clinicaltrials/showallp.php?mid1=930&EncHid=&userName=CTRI/2009/09526
1/000750. Accessed 3 May, 2013. 527
32 Martyn KK, Urbano MT, Hayes JS, et al. Comparison of axillary, rectal and skin-based 528
temperature assessment in preschoolers. Nurse Pract 1988;13:31–6. 529
33 Goh P, Lim FS, Han HH, Willems P. Safety and Immunogenicity of early vaccination with two 530
doses of tetravalent measles-mumps-rubella-varicella (MMRV) vaccine in healthy children 531
from 9 months of age. Infection 2007;35:326–33. 532
34 Aaby P, Martins CL, Garly ML, et al. The optimal age of measles immunisation in low-income 533
countries: a secondary analysis of the assumptions underlying the current policy. BMJ Open 534
2012;12:e000761. 535
35 Gomber S, Arora SK, Das S, et al. Immune response to second dose of MMR vaccine in 536
Indian children. Indian J Med Res 2011;134:302–6. 537
36 Patriarca PA, Wright PF, John TJ. Factors affecting the immunogenicity of oral poliovirus 538
vaccine in developing countries: review. Rev Infect Dis 1991;13:926–39. 539
Page 36 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
37
37 Narang A, Bose A, Pandit AN, et al. Immunogenicity, reactogenicity and safety of human 540
rotavirus vaccine (RIX4414) in Indian infants. Hum Vaccin 2009;5:414–9. 541
38 Zaman K, Sack DA, Yunus M, et al. Successful co-administration of a human rotavirus and 542
oral poliovirus vaccines in Bangladesh infants in a 2-dose schedule at 12 and 16 weeks of 543
age. Vaccine 2009;27:1333–9. 544
39 Vesikari T, Karvonen A, Puustinen L, et al. Efficacy of RIX4414 live attenuated human 545
rotavirus vaccine in Finnish infants. Pediatr Infect Dis J 2004;23:937–43. 546
40 Andrus JK, de Quadros CA, Solorzano CC, et al. Measles and rubella eradication in the 547
Americas. Vaccine 2011;29S:D91–6. 548
41 Davidkin I, Kontio M, Paunio M, et al. MMR vaccination and disease elimination: the Finnish 549
experience. Expert Rev Vaccines 2010;9:1045–53. 550
42 Mulholland EK. Measles in the United States, 2006. N Engl J Med 2006;355:440–3. 551
43 World Health Organization. Field guidelines for measles elimination, 2004. Available at: 552
http://www.measlesrubellainitiative.org/mi-553
files/Tools/Guidelines/WPRO/Field_guidelines_measles_elimination.pdf. Accessed 26 554
September, 2012. 555
44 World Health Organization. Immunization profile – India. Available at: 556
http://apps.who.int/immunization_monitoring/en/globalsummary/countryprofileresult.cfm557
?C=ind. Accessed 13 November, 2012. 558
559
Page 37 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
38
Figure legends 560
Figure 1 Subject disposition 561
Figure 2a Prevalence of fever during the 43-day post-vaccination period after Dose 1 562
(Total vaccinated cohort) 563
Figure 2b Prevalence of fever during the 43-day post-vaccination period after Dose 2 564
(Total vaccinated cohort) 565
Page 38 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
Subject disposition
292x179mm (300 x 300 DPI)
Page 39 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
Prevalence of fever during the 43-day post-vaccination period after Dose 1 (Total vaccinated cohort) 149x118mm (300 x 300 DPI)
Page 40 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
Prevalence of fever during the 43-day post-vaccination period after Dose 2 (Total vaccinated cohort) 148x117mm (300 x 300 DPI)
Page 41 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
1
14 Nov 2014
Supplementary table
Number of children recruited by study center and demographic characteristics
Name and location of study center in
India
MMRV/MMRV MMR/MMRV
MMR/MMR+V Total
na
%a
Center 1, Pune 37 37 18 92 20.4
Center 2, Pune 53 53 26 132 29.3
Center 3, Bangalore 2 2 2 6 1.3
Center 4, Chennai 24 24 12 60 13.3
Center 5, Kolkata 34 34 17 85 18.9
Center 6, Goa 30 30 15 75 16.7
All 180 180 90 450 100
Demographic characteristics MMRV/MMRV MMR/MMRV MMR/MMR+V Total
Age (months) Mean (standard
deviation)
9 (0.0) 9 (0.11) 9 (0.0) 9 (0.07)
Median (range) 9 (9–9) 9 (8–10) 9 (9–9) 9 (8–10)
Page 42 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
2
14 Nov 2014
n
% n % n % n %
Gender Female 79 44.4 89 49.2 49 54.4 216 48.3
Male 99 55.6 91 50.8 41 45.6 231 51.7
a number (percentage) of children in a given category
Page 43 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
3
14 Nov 2014
Page 44 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-007202 on 11 Septem
ber 2015. Dow
nloaded from

For peer review only
CONSORT 2010 checklist Page 1
CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title 1
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 3-4
Introduction
Background and
objectives
2a Scientific background and explanation of rationale 6-8
2b Specific objectives or hypotheses 7-8
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 9
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons 9
Participants 4a Eligibility criteria for participants 9
4b Settings and locations where the data were collected 9 and Supp.
table
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered
9-10
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed
10-11
6b Any changes to trial outcomes after the trial commenced, with reasons Not applicable
Sample size 7a How sample size was determined 12
7b When applicable, explanation of any interim analyses and stopping guidelines Not applicable
Randomisation:
Sequence
generation
8a Method used to generate the random allocation sequence 12
8b Type of randomisation; details of any restriction (such as blocking and block size) 12
Allocation
concealment
mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers),
describing any steps taken to conceal the sequence until interventions were assigned
12
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to
interventions
9, 11
Page 45 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 2
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those
assessing outcomes) and how
Not applicable
11b If relevant, description of the similarity of interventions Not applicable
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 11-13
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses Not applicable
Results
Participant flow (a
diagram is strongly
recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome
14/Figure 1
13b For each group, losses and exclusions after randomisation, together with reasons Figure 1
Recruitment 14a Dates defining the periods of recruitment and follow-up Not applicable
14b Why the trial ended or was stopped Not applicable
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group Supp. Table
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was
by original assigned groups
14
Outcomes and
estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its
precision (such as 95% confidence interval)
14-23/Tables
1-3/Figures
2(a) & (b)
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended Not applicable
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory
Not applicable
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 23
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses Not applicable
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 25-29
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 25-29
Other information
Registration 23 Registration number and name of trial registry 32
Protocol 24 Where the full trial protocol can be accessed, if available Not applicable
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders 30
Page 46 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 3
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic trials.
Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
Page 47 of 47
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on January 4, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-007202 on 11 September 2015. Downloaded from



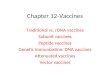








![Types of vaccines 1 - First generation vaccines are whole-organism vaccines - either live and weakened, or killed forms. [1] Live, attenuated vaccines,](https://img.pdfslide.net/doc/110x75/56649e155503460f94afff0b/types-of-vaccines-1-first-generation-vaccines-are-whole-organism-vaccines.jpg)