Embed Size (px)
Citation preview

For peer review only
Vaccination Coverage and Frequency of Out-of-Sequence Vaccinations in Rural Guinea-Bissau
Journal: BMJ Open
Manuscript ID: bmjopen-2012-001509
Article Type: Research
Date Submitted by the Author: 18-May-2012
Complete List of Authors: Hornshøj, Linda; Bandim Health Project, INDEPTH NETWORK, Fisker, Ane; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut, ; Bandim Health Project Fernandes, Manuel; Bandim Health Project, INDEPTH NETWORK, Rodrigues, Amabelia; Bandim Health Project, INDEPTH NETWORK, Benn, Christine; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut, ; Bandim Health Project, INDEPTH NETWORK,
Aaby, Peter; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut, ; Bandim Health Project, INDEPTH NETWORK,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Global health, Infectious diseases, Epidemiology, Health services research
Keywords:
Public health < INFECTIOUS DISEASES, International health services < HEALTH SERVICES ADMINISTRATION & MANAGEMENT, Epidemiology < INFECTIOUS DISEASES, Paediatric infectious disease & immunisation < PAEDIATRICS
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 2 F
ebruary 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2012-001509 on 19 Novem
ber 2012. Dow
nloaded from
For peer review only
Vaccination Coverage and Frequency of Out-of-Sequence Vaccinations in Rural
Guinea-Bissau
Linda Hornshøja, Ane Bærent Fisker
a,b, Manuel Fernandes
a, Amabelia Rodrigues
a,
Christine Stabell Benna,b, Peter Aaby
a,b
a) Bandim Health Project, INDEPTH Network, Apartado 861, Bissau, Guinea-Bissau
b) Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project,
Statens Serum Institut, 2300 Copenhagen S, Denmark
Corresponding author:
Linda Hornshøj, Research Center for Vitamins and Vaccines (CVIVA), Bandim
Health Project, Statens Serum Institut, 2300 Copenhagen S, Denmark. E-mail:
[email protected]. Telephone: +45 32683162.
Keywords:
EPI, vaccination, coverage, out-of-sequence, vaccines
Word count:
Abstract 284, text 2552
Page 1 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
2
ABSTRACT
Objective
The WHO aims for 90% coverage of the Expanded Program on Immunization (EPI),
which in Guinea-Bissau includes bacillus Calmette-Guérin vaccine (BCG) at birth, 3
doses of diphtheria-tetanus-pertussis vaccine (DTP) and oral polio vaccine (OPV) at
6, 10 and 14 weeks and measles vaccine (MV) at 9 months. The WHO assesses
coverage by 12 months of age. The sequence of vaccines may have an effect on child
mortality, but is not considered in official statistics or assessments of programme
performance. We assessed vaccination coverage and frequency of out-of-sequence
vaccinations by 12 and 24 months of age.
Design
Observational cohort study.
Setting and participants
The Bandim Health Project’s rural Health and Demographic Surveillance System in
rural Guinea-Bissau was used, it covers 258 randomly selected villages. Villages are
visited biannually and vaccination cards inspected to ascertain vaccination status.
Between 2003 and 2009 vaccination status by 12 months of age was assessed for 5806
children aged 12-23 months and by 24 months of age for 3792 children aged 24-35
months.
Outcome measures
Coverage of EPI vaccinations and frequency of out-of-sequence vaccinations.
Results
Half of 12-month-old children and 65% of 24-month-old children had completed all
EPI vaccinations. Many children received vaccines out-of-sequence: 54% of BCG
vaccinated children received DTP with or before BCG and 28% of measles vaccinated
children received DTP with or after MV by 12 months of age, by 24 months of age
58% and 35%, respectively.
Conclusions
In rural Guinea-Bissau vaccination coverage by 12 months of age was low, but
continued to increase beyond 12 month of age. The current practice of limiting
vaccinations to children below 12 months of age will lower overall coverage
considerably. More than half of all children received vaccinations out-of-sequence.
Page 2 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
3
ARTICLE SUMMARY
Article focus
- The World Health Organization (WHO) aims for a 90% coverage of the
Expanded Program on Immunization (EPI) by 12 months of age.
- The third dose of diphtheria-tetanus-pertussis vaccine (DTP) is used as a
proxy for vaccination coverage and performance.
- Several studies indicate that the sequence of vaccinations affects child
mortality, but current polices do not take out-of-sequence vaccinations into
account.
Key messages
- Only half of all children were fully vaccinated by 12 months of age, but the
coverage continued to increase beyond 12 months of age.
- Limiting vaccinations to children below 12 months of age will lower overall
vaccination coverage considerably.
- More than half of the children received vaccinations out-of sequence.
Strengths and limitations of this study
- The study population was sizeable and the continued demographic
surveillance has many advantages compared with other household surveys.
- The study was limited to rural Guinea-Bissau and may not necessarily be
representative of other low-income settings.
Page 3 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
4
INTRODUCTION
In 1974 the World Health Organization (WHO) launched the Expanded Program on
Immunization (EPI), to provide routine vaccinations against tuberculosis, polio,
diphtheria, tetanus, pertussis and measles to all children. At the time less than 5% of
children worldwide were vaccinated against these diseases.[1] In most low-income
countries the standard schedule for EPI vaccines includes bacillus Calmette-Guérin
vaccine (BCG) and oral polio vaccine (OPV) at birth, diphtheria- tetanus-pertussis
vaccine (DTP) and OPV at 6, 10 and 14 weeks and measles vaccine (MV) at 9 months
of age.[2]
The Global Immunization Vision and Strategy 2006-2015 (GIVS) developed by the
WHO/UNICEF focused on ensuring equity in access to vaccination and aimed for a
90% national vaccination coverage and a 80% vaccination coverage in every district
by 2010.[3]
WHO and UNICEF estimates of vaccination coverage are based on reports of
vaccinations performed by service providers (administrative data) and surveys of
vaccination history (coverage surveys). The estimates refer to vaccinations given
during routine immunisation services to children below 12 months of age, not
including supplemental activities such as OPV and MV campaigns. The
administrative data are based on the number of vaccine doses administered to the
estimated target population, most commonly the estimated number of children
surviving their first year of life.[4] The WHO EPI cluster methodology is commonly
used for coverage surveys. Survey results typically report on annual cohorts of
children so that all children included have had 12 months to receive all vaccinations
(being between 12–23 months of age at the time of the survey as shown in figure
1).[4,5]
Studies from low-income countries suggest that the routine vaccinations have effects
on mortality beyond that of protecting against the target disease. These effects are
referred to as non-specific effects (NSE). BCG and MV have beneficial effects in
lowering overall child morbidity and mortality,[6-10] whereas DTP may be associated
with increased morbidity and mortality.[6,9-17] The NSEs depend on the most recent
vaccine and giving vaccines out-of-sequence may therefore affect child mortality.
Page 4 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
5
Worryingly several studies have shown that DTP given together with MV or after MV
is associated with increased child morbidity and mortality.[12,18-21]
The purpose of this study was to determine the overall vaccination coverage of EPI
routine vaccinations and to determine the prevalence of out-of-sequence vaccinations
in rural Guinea-Bissau. Both outcomes were determined among 12-month-old and 24-
month-old children.
METHODS
Setting
In 1978, the Bandim Health Project (BHP) was established as a Health and
Demographic Surveillance System (HDSS) in Guinea-Bissau. Outside the capital,
Guinea-Bissau is divided into ten health regions. Since 1990, five of these regions
have been visited biannually by mobile teams from BHP. At each visit the teams
collect information about health, socio-economic and vaccination status. In 2006, the
remaining regions were included in the surveillance and the mobile teams now cover
258 villages in all ten regions. The study population in the HDSS is based on 182
randomly selected clusters of 100 women of fertile age and their children below five
years of age. In the cluster areas all new households are registered and in all
households new women and children taking up residence are added. The HDSS
cohort is therefore continuously growing.
Study population
The study population for the present study was extracted from the HDSS cohort. The
population base for the 12-month-old children was children born from the 1st January
2004 until 31st of December 2006, registered before 12 months of age and resident in
the study area when completing 12 months of age. For the 24-month-old children,
children born from the 1st January 2004 until 31st of December 2005, registered before
24 months of age and resident in the study area when completing 24 months of age
were included.
Vaccinations
Guinea-Bissau follows the standard EPI and children in the present study were to be
vaccinated in accordance with the EPI schedule shown in figure 1.
Page 5 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
6
A child in Guinea-Bissau can be vaccinated at hospitals, most health centres and
during outreach visits to the villages. All national vaccines are provided through
UNICEF and are free of charge for the parents. However, in order for a child to
receive its vaccinations it must have a vaccination card. The card is used to register
the child’s personal information, vaccinations and the weight of the child. Although
the card should also be free of charge, it is most often sold by the health workers for
the equivalent of $ 1(unpublished data). Since September 2007, the BHP teams have
been accompanied by nurses who vaccinate children missing doses of OPV, DTP or
MV and children receive a vaccination card free of charge. In selection of the two
cohorts for this study, children were only included if they had reached 12 or 24
months of age before the BHP nurses began administering vaccines.
Assessment of vaccination coverage
To emulate the EPI survey methodology used by WHO, we determined the
vaccination coverage by 12 months of age in children aged 12-23 months at home
visits. Vaccination status was determined based on the first visit among children aged
12-23 months in 2005-2009, at which vaccination status could be assessed by
inspecting the vaccination card. If the child did not have a vaccination card at the time
of our visits, it was defined as unvaccinated if the mother confirmed that the child had
never received any vaccines. If we were not able to verify a child’s vaccinations at
any visit in the interval of 12-23 months of age either by 1) by seeing the vaccination
card or 2) ascertaining that the child had never received vaccinations, the child was
not included in the analysis. The vaccination status by 24 months of age was
determined using the same method for children visited at 24-35 months of age.
Definitions
We defined fully vaccinated as completion of the EPI vaccinations not including OPV
at birth (OPV0), because very few children received OPV0 in the rural areas.
Out-of-sequence vaccinations were 1) BCG administered together with any dose of
DTP, 2) any dose of DTP with or before BCG, 3) MV with any dose of DTP and 4)
any dose of DTP with or after MV.
Statistical analysis
Page 6 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
7
Relative risks and 95% confidence intervals (CI) were calculated using Poisson
regression with robust variance estimates.[22] Coverage for different regions was
compared using chi-2-tests. Data was analysed using STATA 11.0.
RESULTS
We determined vaccination status for 5806 children by 12 months of age and for 3792
children by 24 months of age (figure 2). A larger proportion of children were assessed
by 12 months of age (68%) than by 24 months of age (59%), RR=1.15 (95% CI=1.12-
1.18).
Vaccination coverage
By 12 months of age only 50% of children were fully vaccinated if whether or not a
child had received OPV0 was disregarded. If OPV0 was included in the definition of
“fully vaccinated” only 9% of 12-month-old children were fully vaccinated. There
were large regional differences: only 26% of children were fully vaccinated in
Tombali compared with 65% in Gabu and Bafata, the regions with highest coverage
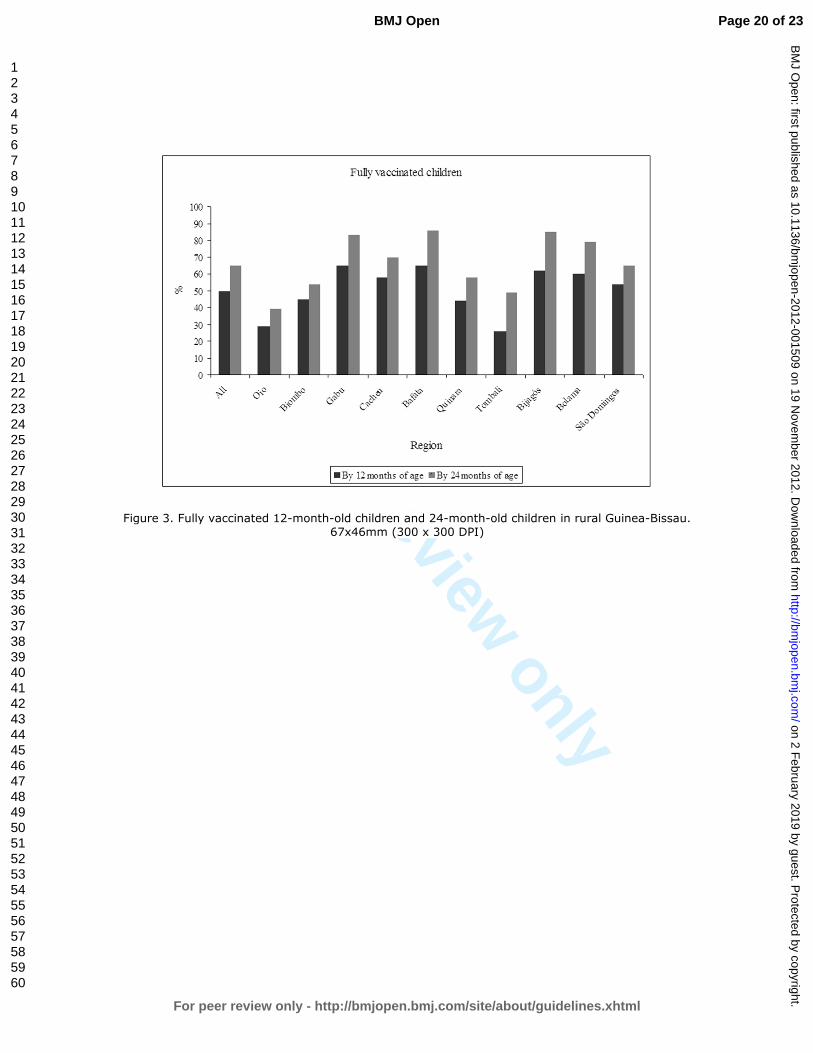
(table 1). By 24 months of age the percentage of fully vaccinated children was 65%, a
29% (95%CI=25-34%) increase. The increase ranged from 20% to 87% in the
different regions (table 1, figure 3).
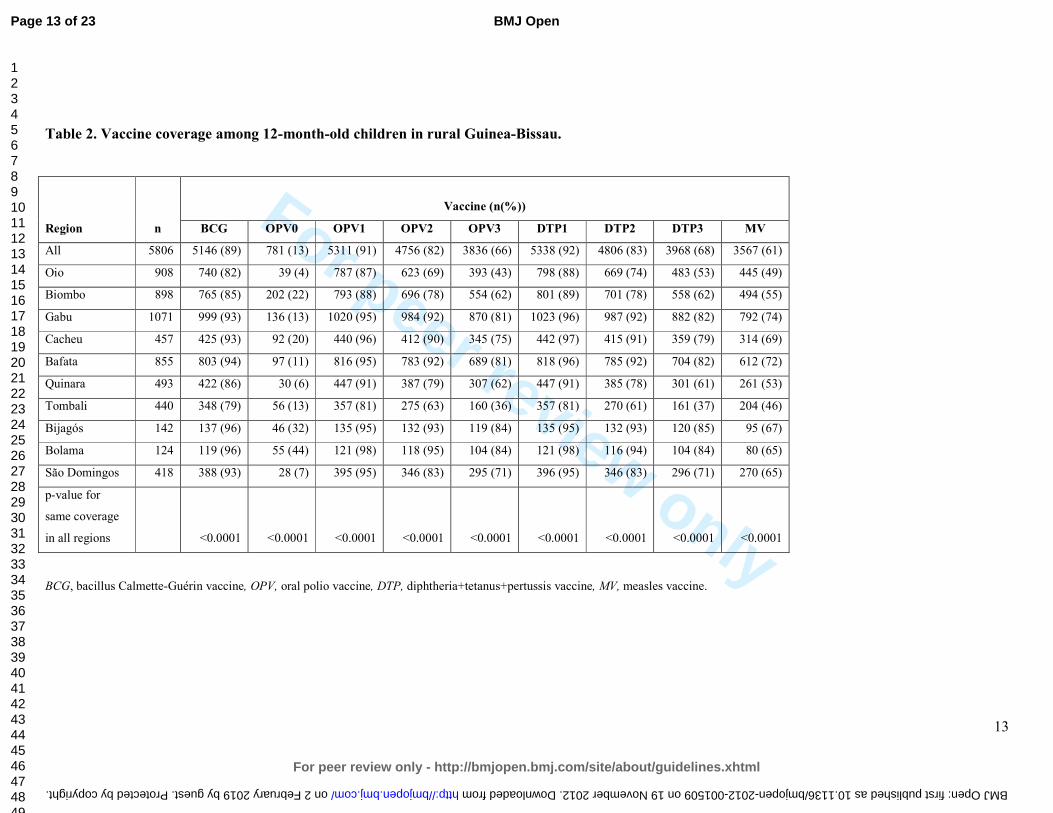
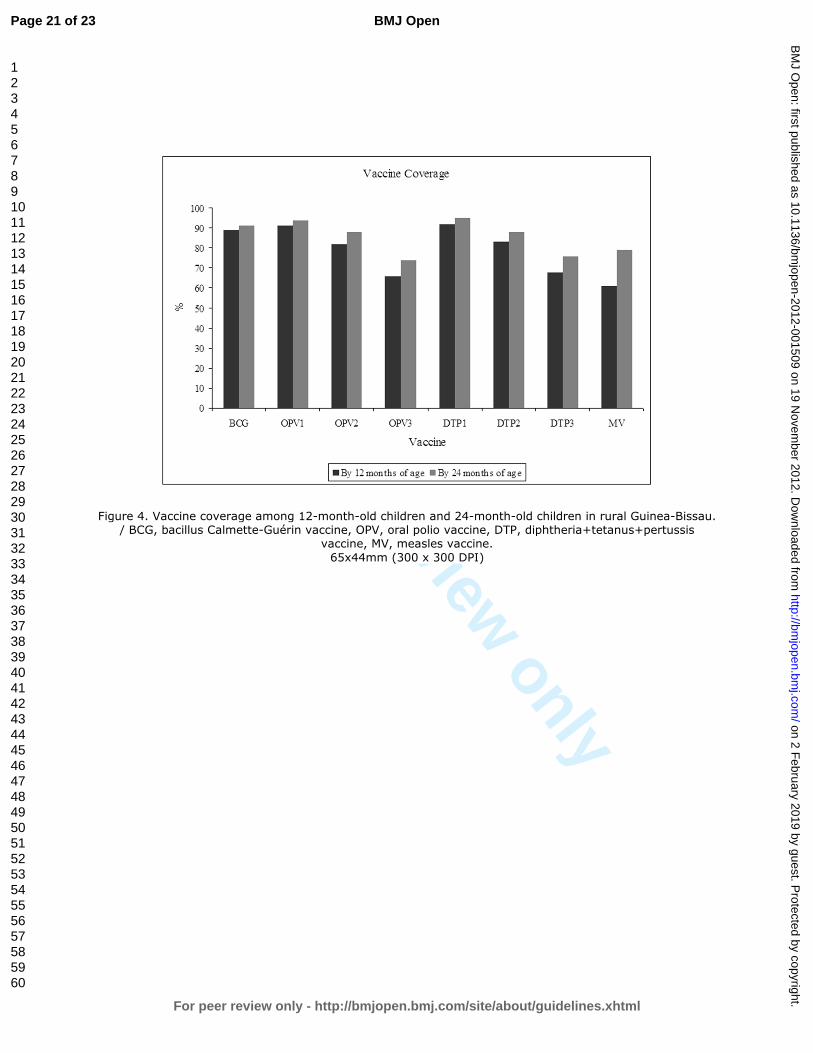
Vaccine-specific coverages by 12 months of age were: BCG 89%, OPV0 13%, OPV1
91%, OPV2 82%, OPV3 66%, DTP1 92%, DTP2 83%, DTP3 68% and MV 61%,
with large regional differences (table 2). There was only a slight increase in the
vaccines the children receive early in life when comparing vaccine coverage at 12 and
24 months of age, but the increase for vaccines given later in life was much higher.
BCG, OPV1 and DTP1 increased by 3%, whereas OPV3 increased by 12%, DTP3 by
11% and MV increased by 28% (figure 4). The DTP3 coverage was higher than the
MV coverage by 12 months of age in all regions, except for Tombali. By 24 months
of age the overall MV coverage was higher than DTP3, but in four out of ten regions
(Cacheu, Quinara, Bijagós and Bolama) the MV coverage was still lower than the
DTP3 coverage (data not shown).
Out-of-sequence vaccinations
Page 7 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
8
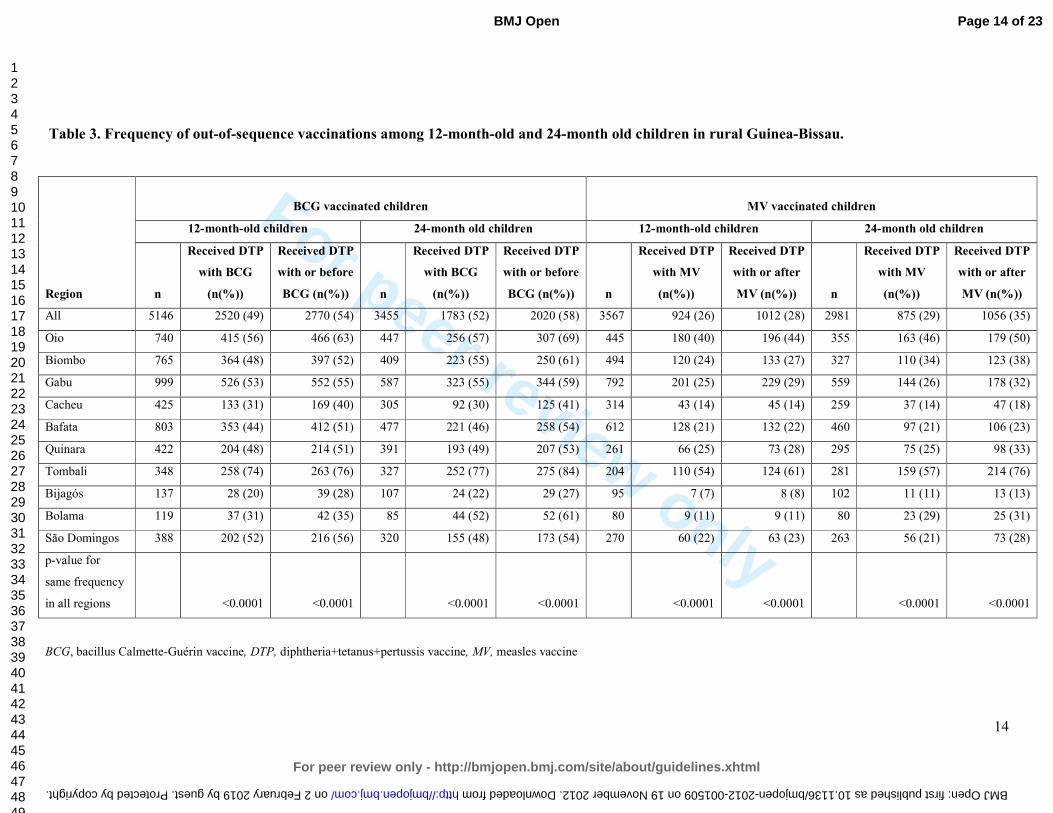
Among children who had received BCG by 12 months of age, 49% received BCG
together with a dose of DTP and 54% DTP with or before BCG. By 24 months of age
these proportions were 52% and 58% (table 3). The region of Bijagós managed to stay
well below 30%. In comparison in Tombali more than 75% of children in both age
groups received DTP with or before BCG (table 3).
Among children who had received MV by 12 months of age, 26% received it together
with a dose of DTP; this figure was 29% by 24 months of age. Among the children
who had received MV, 28% had received DTP with or after MV by 12 months of age,
and this increased to 35% by 24 months of age, a 25% (95%CI=16-34%) increase
(table 3). Again there were large regional differences (table 3).
DISCUSSION
Main results
Vaccinations are important in lowering overall child mortality. In our study, only half
of all children were fully vaccinated by 12 months of age and 65% by 24 months of
age (table 1, figure 2). Only estimating vaccination coverage among 12-month-old
children therefore underestimates final coverage considerably. Many children had
initiated the vaccination program, but not received all the EPI vaccines by 12 months
of age. This was reflected in high coverage of vaccines scheduled early in life, with
little increased from 12 to 24 months of age, whereas the increase in vaccines
scheduled later was much higher: MV increased by 28% (25-31%) (figure 4).
Regional differences in vaccination coverage and frequency of out-of-sequence
vaccinations were large (tables 1,3).
A substantial number of children received out-of-sequence vaccinations. More than
half of all BCG vaccinated children received DTP with or before BCG and a third of
MV vaccinated children received DTP with or after MV (table 3). As vaccination
coverage increased among 24-month-old children, so did the frequency of out-of-
sequence vaccinations (tables 1,3).
Strengths and weaknesses
The HDSS clusters are randomly selected and the sample size substantial. The
villages have been visited biannually for years, thus offering the opportunity to verify
Page 8 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
9
and correct ambiguous data. We believe that the continued surveillance contributes to
more reliable data than other types of surveys. For example, in this study, children
with previously registered vaccinations could not be misclassified as unvaccinated at
a later visit if the vaccinations card had been lost. A study from Malawi showed a
BCG scar rate of 70% among children without documents, making it clear how
vaccination coverage can be underestimated if children without vaccination cards are
simply classified as unvaccinated.[23] We also registered pregnancies and births and
could thereby determine date of birth fairly precisely if there was no written record.
Comparison to other studies
We found that estimating vaccination coverage among 12-month-old children
underestimated final coverage. Similarly, Clark and Sanderson found that DTP3
coverage increased from 67% to 74% and MV from 59% to 77%, when comparing
the coverage at 12 months of age to the coverage at 36 months of age in survey data
from 45 low- and middle-income countries.[24]
In our study we emulated the methodology used by the WHO to make the results
comparable. A WHO EPI cluster survey was conducted in the capital Bissau in 2005
using vaccination cards or history to confirm vaccination status. It found vaccine
coverage to be: BCG 87%, OPV3 60%, DTP3 59% and MV 71%.[25] When we
compared their results to ours BCG coverage did not differ, WHO OPV3 and DTP3
coverage was 10-13% (5-18%) lower and WHO MV coverage was 16% (11-21%)
higher than our estimates (table 2,[25]). The higher MV coverage may in part be
explained by our study not including data from the urban Bissau. In Bissau the
coverage is higher as vaccinations are more accessible. However, surprisingly higher
coverage of all antigens was not found in the WHO survey. If the WHO survey
underestimated the true coverage it could in part be due to the use of history, i.e.
maternal recall, to confirm vaccination status. The validity of recall is correlated to
the number of doses received and the age of the child. Mothers tend to recall
vaccinations more accurately for younger children with fewer doses and the use of
recall seems to underestimate vaccination coverage.[26,27] In the WHO survey, visits
are made to randomly selected houses according to the survey method.[5] Unlike in
our study, there are no follow-up visits to households in which the vaccination status
for a child can not be determined at the time of the visit. The WHO EPI survey
Page 9 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
10
methodology has previously been criticised for lacking methodological rigour and for
introducing bias.[28,29]
Implications
At present vaccination coverage estimates used by WHO and United Nations
Children’s Fund (UNICEF) emphasises the coverage of DTP3 by 12 months of age,
not taking into account the timing of the vaccines received or vaccines received at a
later age.[30,31] This has two consequences, which may have large implications.
First, the emphasis on DTP3 leads to more focus on DTP3 and less focus on measles
vaccine. It is often used by funding agencies such as the Global Alliance for Vaccines
and Immunizations (GAVI) to evaluate programme performance[32] and
improvement of vaccination coverage is often linked to additional funding.[33] As a
result many African countries now have a lower coverage of MV than DTP3.[2] This
is unfortunate. Several studies show that MV lowers overall child morbidity and
mortality[6-10,13-15] and several studies suggest that DTP is associated with
increased female morbidity and mortality.[6,9-15]
Second, our data was from before 2007, and it showed that MV coverage increased by
28% during the second year of life. However, the current donor focus on vaccination
status by 12 months of age leads to many countries, including Guinea-Bissau, have
now stopped vaccinating children above 12 months of age, because they do not count
in the statistics. The current policy not to vaccinate children above 12 months of age
gives children only a 3-month-time-window to be measles vaccinated. This will
undoubtedly lead to a lower MV coverage and an increasing number of children being
susceptible to measles infection.
CONCLUSION
Our study showed that the vaccination coverage in Guinea-Bissau is far from the
WHO goal of 90%. Only half of all 12-month-old children were fully vaccinated, with
great regional differences in vaccination coverage. Coverage based on vaccinations
received during the first 12 months of life significantly underestimated the final
coverage. We found that a considerable number of children received out-of-sequence
vaccinations. As several studies suggest that out-of-sequence vaccinations have an
impact on overall survival[18-21] such deviations from the schedule need to be taken
Page 10 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
11
into account and should be reported as performance indicators for vaccination
programmes in likening with specific antigen coverage.
The current drive to limit vaccinations to children below 12 months of age[34] will
prevent many children from completing their vaccination schedule and this negative
effect will be strongest for measles vaccination. This will lower heard immunity to
measles infections and increase the risk of epidemics. Since all studies show that
measles vaccination administered as the most recent vaccine has a beneficial effect on
child survival[6-8,10,14] it will have unfortunate consequences that an increasing
proportion of children will have DTP as their most recent vaccination.
[10,12,15,17,35]
Funding
This study was supported by the Danish Medical Research Council, the Aase and
Ejnar Danielsen's Foundation and DANIDA. The Bandim Health Project received
support from DANIDA to conduct their rural HDSS. CVIVA receives support from
the Danish National Research Foundation. CSB is funded by the European Research
Council (ERC-2009-StG, grant agreement no. 243149). PA holds a research
professorship grant from the Novo Nordic Foundation. Funding agencies had no hand
in study design, execution, data analysis, data interpretation or the writing of this
paper.
Competing interests
None declared.
Contributors
LH, ABF, CSB and PA designed and planned the study. LH, ABF, MF and AR
supervised data collection and data entry. LH carried out the statistical analysis with
help from ABF, CSB and PA. LH wrote the first draft of the paper and holds the
primary responsibility for its final content. All authors contributed to and approved
the final manuscript.
Data sharing statement
No additional data available.
Page 11 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
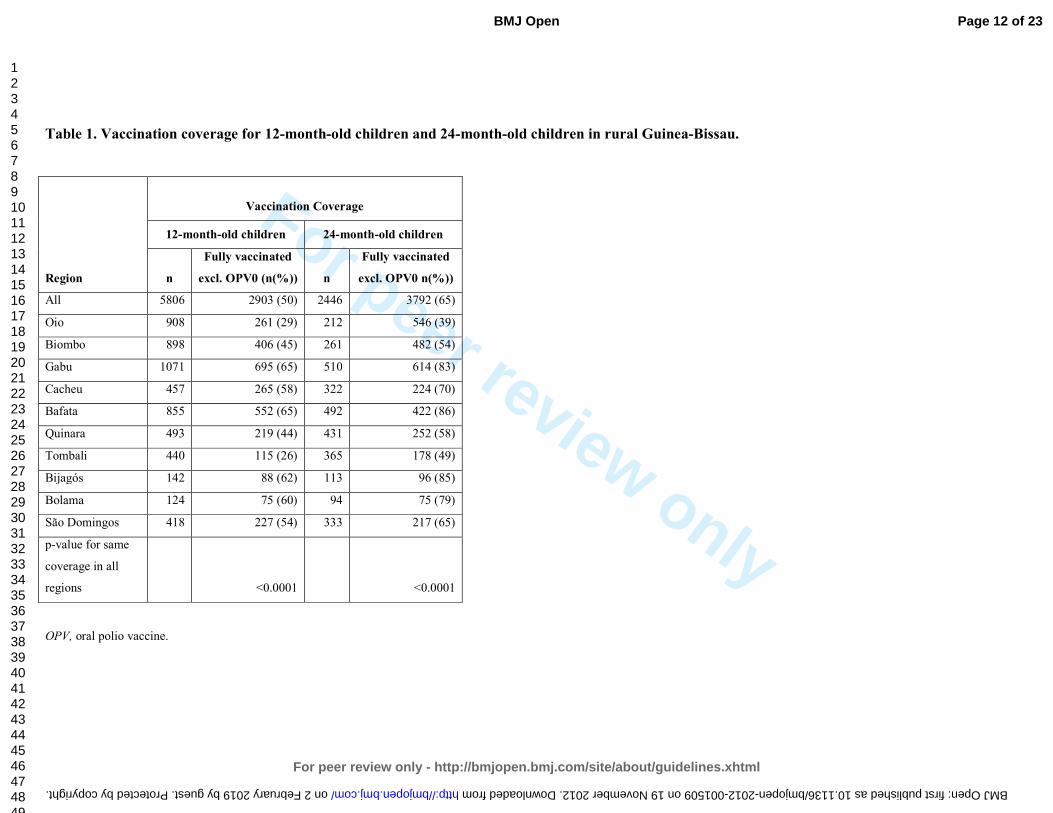
Table 1. Vaccination coverage for 12-month-old children and 24-month-old children in rural Guinea-Bissau.
Region
Vaccination Coverage
12-month-old children 24-month-old children
n
Fully vaccinated
excl. OPV0 (n(%))
n
Fully vaccinated
excl. OPV0 n(%))
All 5806 2903 (50) 2446 3792 (65)
Oio 908 261 (29) 212 546 (39)
Biombo 898 406 (45) 261 482 (54)
Gabu 1071 695 (65) 510 614 (83)
Cacheu 457 265 (58) 322 224 (70)
Bafata 855 552 (65) 492 422 (86)
Quinara 493 219 (44) 431 252 (58)
Tombali 440 115 (26) 365 178 (49)
Bijagós 142 88 (62) 113 96 (85)
Bolama 124 75 (60) 94 75 (79)
São Domingos 418 227 (54) 333 217 (65)
p-value for same
coverage in all
regions <0.0001 <0.0001
OPV, oral polio vaccine.
Page 12 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
13
Table 2. Vaccine coverage among 12-month-old children in rural Guinea-Bissau.
Region n
Vaccine (n(%))
BCG OPV0 OPV1 OPV2 OPV3 DTP1 DTP2 DTP3 MV
All 5806 5146 (89) 781 (13) 5311 (91) 4756 (82) 3836 (66) 5338 (92) 4806 (83) 3968 (68) 3567 (61)
Oio 908 740 (82) 39 (4) 787 (87) 623 (69) 393 (43) 798 (88) 669 (74) 483 (53) 445 (49)
Biombo 898 765 (85) 202 (22) 793 (88) 696 (78) 554 (62) 801 (89) 701 (78) 558 (62) 494 (55)
Gabu 1071 999 (93) 136 (13) 1020 (95) 984 (92) 870 (81) 1023 (96) 987 (92) 882 (82) 792 (74)
Cacheu 457 425 (93) 92 (20) 440 (96) 412 (90) 345 (75) 442 (97) 415 (91) 359 (79) 314 (69)
Bafata 855 803 (94) 97 (11) 816 (95) 783 (92) 689 (81) 818 (96) 785 (92) 704 (82) 612 (72)
Quinara 493 422 (86) 30 (6) 447 (91) 387 (79) 307 (62) 447 (91) 385 (78) 301 (61) 261 (53)
Tombali 440 348 (79) 56 (13) 357 (81) 275 (63) 160 (36) 357 (81) 270 (61) 161 (37) 204 (46)
Bijagós 142 137 (96) 46 (32) 135 (95) 132 (93) 119 (84) 135 (95) 132 (93) 120 (85) 95 (67)
Bolama 124 119 (96) 55 (44) 121 (98) 118 (95) 104 (84) 121 (98) 116 (94) 104 (84) 80 (65)
São Domingos 418 388 (93) 28 (7) 395 (95) 346 (83) 295 (71) 396 (95) 346 (83) 296 (71) 270 (65)
p-value for
same coverage
in all regions
<0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine.
Page 13 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
14
Table 3. Frequency of out-of-sequence vaccinations among 12-month-old and 24-month old children in rural Guinea-Bissau.
Region
BCG vaccinated children MV vaccinated children
12-month-old children 24-month old children 12-month-old children 24-month old children
n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%))
All 5146 2520 (49) 2770 (54) 3455 1783 (52) 2020 (58) 3567 924 (26) 1012 (28) 2981 875 (29) 1056 (35)
Oio 740 415 (56) 466 (63) 447 256 (57) 307 (69) 445 180 (40) 196 (44) 355 163 (46) 179 (50)
Biombo 765 364 (48) 397 (52) 409 223 (55) 250 (61) 494 120 (24) 133 (27) 327 110 (34) 123 (38)
Gabu 999 526 (53) 552 (55) 587 323 (55) 344 (59) 792 201 (25) 229 (29) 559 144 (26) 178 (32)
Cacheu 425 133 (31) 169 (40) 305 92 (30) 125 (41) 314 43 (14) 45 (14) 259 37 (14) 47 (18)
Bafata 803 353 (44) 412 (51) 477 221 (46) 258 (54) 612 128 (21) 132 (22) 460 97 (21) 106 (23)
Quinara 422 204 (48) 214 (51) 391 193 (49) 207 (53) 261 66 (25) 73 (28) 295 75 (25) 98 (33)
Tombali 348 258 (74) 263 (76) 327 252 (77) 275 (84) 204 110 (54) 124 (61) 281 159 (57) 214 (76)
Bijagós 137 28 (20) 39 (28) 107 24 (22) 29 (27) 95 7 (7) 8 (8) 102 11 (11) 13 (13)
Bolama 119 37 (31) 42 (35) 85 44 (52) 52 (61) 80 9 (11) 9 (11) 80 23 (29) 25 (31)
São Domingos 388 202 (52) 216 (56) 320 155 (48) 173 (54) 270 60 (22) 63 (23) 263 56 (21) 73 (28)
p-value for
same frequency
in all regions <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine
Page 14 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
REFERENCES
(1) UNICEF. Expanding Immunization Coverage. 2011. Available from: http://www.unicef.org/immunization/index_coverage.html.
(2) UNICEF, WHO. Immunization summary - A statistical reference containing data through 2010. UNICEF, WHO 2012.
(3) WHO. GIVS : global immunization vision and strategy : 2006-2015. WHO 2005.
(4) WHO. WHO vaccine-preventable diseases : monitoring system : 2010 global summary. WHO 2010.
(5) WHO. Immunization coverage cluster survey: Reference manual. WHO 2005.
(6) Veirum JE, Sodemann M, Biai S, et al. Routine vaccinations associated with divergent effects on female and male mortality at the paediatric ward in Bissau, Guinea-Bissau. Vaccine 2005;23:1197-1204.
(7) Aaby P, Samb B, Simondon F, et al. Non-specific beneficial effect of measles immunisation: analysis of mortality studies from developing countries. BMJ 1995;311:481-485.
(8) Kabir Z, Long J, Reddaiah VP, et al. Non-specific effect of measles vaccination on overall child mortality in an area of rural India with high vaccination coverage: a population-based case-control study. Bull World Health Organ 2003;81:244-250.
(9) Aaby P, Martins C, Bale C, et al. Sex differences in the effect of vaccines on the risk of hospitalization due to measles in Guinea-bissau. Pediatr Infect Dis J 2010;29:324-328.
(10) Kristensen I, Aaby P, Jensen H. Routine vaccinations and child survival: follow up study in Guinea-Bissau, West Africa. BMJ 2000;321:1435-1438.
(11) Aaby P, Jensen H, Gomes J, et al. The introduction of diphtheria-tetanus-pertussis vaccine and child mortality in rural Guinea-Bissau: an observational study. Int J Epidemiol 2004;33:374-380.
(12) Agergaard J, Nante E, Poulstrup G, et al. Diphtheria-tetanus-pertussis vaccine administered simultaneously with measles vaccine is associated with increased morbidity and poor growth in girls. A randomised trial from Guinea-Bissau. Vaccine 2011;29:487-500.
(13) Aaby P, Jensen H, Rodrigues A, et al. Divergent female-male mortality ratios associated with different routine vaccinations among female-male twin pairs. Int J Epidemiol 2004;33:367-373.
(14) Aaby P, Vessari H, Nielsen J, et al. Sex differential effects of routine immunizations and childhood survival in rural Malawi. Pediatr Infect Dis J 2006;25:721-727.
(15) Aaby P, Jensen H, Walraven G. Age-specific changes in the female-male mortality ratio related to the pattern of vaccinations: an observational study from rural Gambia. Vaccine 2006;24:4701-4708.
(16) Aaby P, Benn CS, Nielsen J, et al. Testing the hypothesis that diphtheria-tetanus-pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012. In press.
Page 15 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
16
(17) Aaby P, Ravn H, Roth A, et al. Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial. Arch Dis Child 2012. In press.
(18) Aaby P, Jensen H, Samb B, et al. Differences in female-male mortality after high-titre measles vaccine and association with subsequent vaccination with diphtheria-tetanus-pertussis and inactivated poliovirus: reanalysis of West African studies. Lancet 2003;361:2183-2188.
(19) Biai S, Rodrigues A, Nielsen J, et al. Vaccination status and sequence of vaccinations as risk factors for hospitalisation among outpatients in a high mortality country. Vaccine 2011;29:3662-3669.
(20) Aaby P, Ibrahim SA, Libman MD, et al. The sequence of vaccinations and increased female mortality after high-titre measles vaccine: trials from rural Sudan and Kinshasa. Vaccine 2006;24:2764-2771.
(21) Aaby P, Biai S, Veirum JE, et al. DTP with or after measles vaccination is associated with increased in-hospital mortality in Guinea-Bissau. Vaccine 2007;25:1265-1269.
(22) Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 2003;3:21.
(23) Jahn A, Floyd S, Mwinuka V, et al. Ascertainment of childhood vaccination histories in northern Malawi. Trop Med Int Health 2008;13:129-138.
(24) Clark A, Sanderson C. Timing of children's vaccinations in 45 low-income and middle-income countries: an analysis of survey data. Lancet 2009;373:1543-1549.
(25) WHO, UNICEF. Review of national immunization coverage 1980-2008 - Guinea-Bissau. WHO 2009.
(26) Suarez L, Simpson DM, Smith DR. Errors and correlates in parental recall of child immunizations: effects on vaccination coverage estimates. Pediatrics 1997;99:E3.
(27) Valadez JJ, Weld LH. Maternal recall error of child vaccination status in a developing nation. Am J Public Health 1992;82:120-122.
(28) Luman ET, Worku A, Berhane Y, et al. Comparison of two survey methodologies to assess vaccination coverage. Int J Epidemiol 2007;36:633-641.
(29) Burton A, Monasch R, Lautenbach B, et al. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull World Health Organ 2009;87:535-541.
(30) WHO, UNICEF, and World Bank. State of the world's vaccines and immunization. 3rd ed. WHO 2009.
(31) WHO. World Health Statistics 2011 - Indicator compendium. WHO 2011.
(32) GAVI alliance. Guidelines on country proposals - For support for: New and Underused Vaccines. GAVI alliance 2011.
(33) Arevshatian L, Clements C, Lwanga S, et al. An evaluation of infant immunization in Africa: is a transformation in progress? Bull World Health Organ 2007;85:449-457.
Page 16 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
17
(34) Fisker A, Hornshøj L, Balde I, et al. Vaccination coverage before and after the introduction of pentavalent and yellow fever vaccines in Guinea-Bissau: Decline in the coverage for measles vaccine. Submitted.
(35) Aaby P, Benn CS, Nielsen J, et al. Testing the hypothesis that diphtheria-tetanus-pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012.
Page 17 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
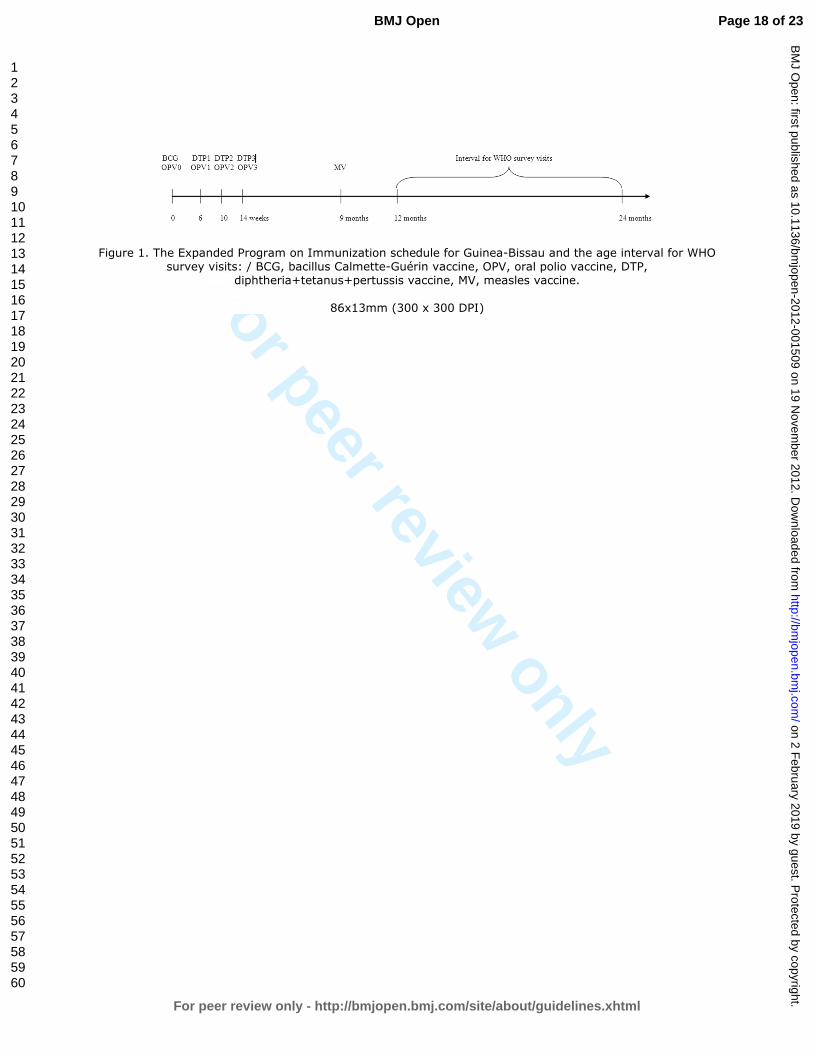
Figure 1. The Expanded Program on Immunization schedule for Guinea-Bissau and the age interval for WHO survey visits: / BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP,
diphtheria+tetanus+pertussis vaccine, MV, measles vaccine.
86x13mm (300 x 300 DPI)
Page 18 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
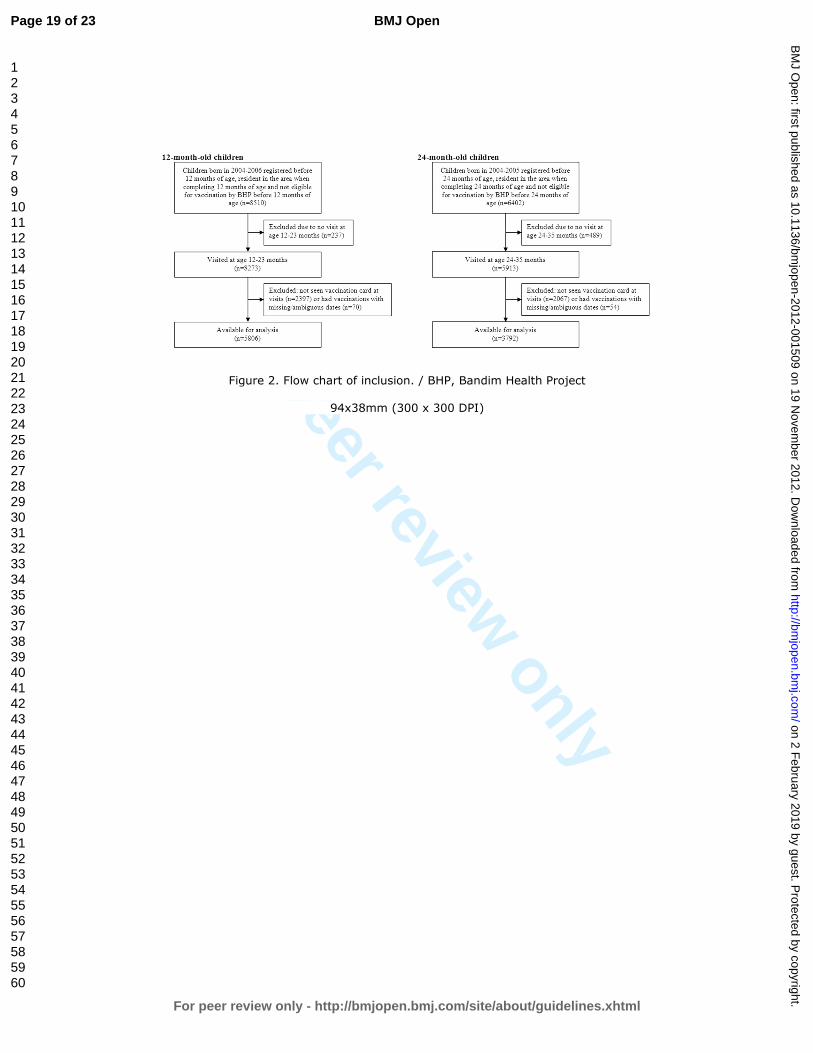
Figure 2. Flow chart of inclusion. / BHP, Bandim Health Project
94x38mm (300 x 300 DPI)
Page 19 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
Figure 3. Fully vaccinated 12-month-old children and 24-month-old children in rural Guinea-Bissau.
67x46mm (300 x 300 DPI)
Page 20 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
Figure 4. Vaccine coverage among 12-month-old children and 24-month-old children in rural Guinea-Bissau. / BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP, diphtheria+tetanus+pertussis
vaccine, MV, measles vaccine. 65x44mm (300 x 300 DPI)
Page 21 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
STROBE 2007 (v4) checklist of items to be included in reports of observational studies in epidemiology*
Checklist for cohort, case-control, and cross-sectional studies (combined)
Section/Topic Item # Recommendation Reported on page #
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 2
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 2
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4-5
Objectives 3 State specific objectives, including any pre-specified hypotheses 5
Methods
Study design 4 Present key elements of study design early in the paper 5
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection 5
Participants 6 (a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe
methods of follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control
selection. Give the rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
5-6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case N/A
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic
criteria, if applicable 6
Data sources/ measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group 6
Bias 9 Describe any efforts to address potential sources of bias 6,9
Study size 10 Explain how the study size was arrived at 7, fig 2
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen
and why 6-7
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding 7
(b) Describe any methods used to examine subgroups and interactions N/A
(c) Explain how missing data were addressed 6, fig2
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed N/A
Page 22 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
(e) Describe any sensitivity analyses N/A
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed 7, fig 1-2
(b) Give reasons for non-participation at each stage 6, fig2
(c) Consider use of a flow diagram Fig2
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and
potential confounders 5-6
(b) Indicate number of participants with missing data for each variable of interest Fig2
(c) Cohort study—Summarise follow-up time (eg, average and total amount) N/A
Outcome data 15* Cohort study—Report numbers of outcome events or summary measures over time N/A
Case-control study—Report numbers in each exposure category, or summary measures of exposure -
Cross-sectional study—Report numbers of outcome events or summary measures -
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95%
confidence interval). Make clear which confounders were adjusted for and why they were included 7-8, tables 1-3
(b) Report category boundaries when continuous variables were categorized N/A
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period N/A
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses N/A
Discussion
Key results 18 Summarise key results with reference to study objectives 8
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction
and magnitude of any potential bias 8-9
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results
from similar studies, and other relevant evidence 9-10
Generalisability 21 Discuss the generalisability (external validity) of the study results 10
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based 11
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE
checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at
http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 23 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
Vaccination Coverage and Out-of-Sequence Vaccinations in Rural Guinea-Bissau: An Observational Cohort Study
Journal: BMJ Open
Manuscript ID: bmjopen-2012-001509.R1
Article Type: Research
Date Submitted by the Author: 03-Sep-2012
Complete List of Authors: Hornshøj, Linda; Bandim Health Project, INDEPTH NETWORK, Benn, Christine; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut, ; Bandim Health Project, INDEPTH NETWORK, Fernandes, Manuel; Bandim Health Project, INDEPTH NETWORK, Rodrigues, Amabelia; Bandim Health Project, INDEPTH NETWORK, Aaby, Peter; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut, ; Bandim Health Project, INDEPTH
NETWORK, Fisker, Ane; Bandim Health Project; Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project, Statens Serum Institut,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Global health, Infectious diseases, Epidemiology, Health services research
Keywords:
Public health < INFECTIOUS DISEASES, International health services < HEALTH SERVICES ADMINISTRATION & MANAGEMENT, Epidemiology < INFECTIOUS DISEASES, Paediatric infectious disease & immunisation < PAEDIATRICS
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 2 F
ebruary 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2012-001509 on 19 Novem
ber 2012. Dow
nloaded from
For peer review only
Vaccination Coverage and Out-of-Sequence Vaccinations in Rural Guinea-
Bissau: An Observational Cohort Study
Linda Hornshøja, Christine Stabell Benn
a,b, Manuel Fernandes
a, Amabelia Rodrigues
a,
Peter Aabya,b, Ane Bærent Fisker
a,b
a) Bandim Health Project, INDEPTH Network, Apartado 861, Bissau, Guinea-Bissau
b) Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project,
Statens Serum Institut, 2300 Copenhagen S, Denmark
Corresponding author:
Linda Hornshøj, Research Center for Vitamins and Vaccines (CVIVA), Bandim
Health Project, Statens Serum Institut, 2300 Copenhagen S, Denmark. E-mail:
[email protected]. Telephone: +45 32683162.
Keywords:
EPI, vaccination, coverage, out-of-sequence, vaccines
Word count:
Abstract 293, text 2746
Page 1 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
2
ABSTRACT
Objective
The WHO aims for 90% coverage of the Expanded Program on Immunization (EPI),
which in Guinea-Bissau included bacillus Calmette-Guérin vaccine (BCG) at birth, 3
doses of diphtheria-tetanus-pertussis vaccine (DTP) and oral polio vaccine (OPV) at
6, 10 and 14 weeks and measles vaccine (MV) at 9 months when this study was
conducted. The WHO assesses coverage by 12 months of age. The sequence of
vaccines may have an effect on child mortality, but is not considered in official
statistics or assessments of programme performance. We assessed vaccination
coverage and frequency of out-of-sequence vaccinations by 12 and 24 months of age.
Design
Observational cohort study.
Setting and participants
The Bandim Health Project’s rural Health and Demographic Surveillance site covers
258 randomly selected villages in all regions of Guinea-Bissau. Villages are visited
biannually and vaccination cards inspected to ascertain vaccination status. Between
2003 and 2009 vaccination status by 12 months of age was assessed for 5806 children
aged 12-23 months; vaccination status by 24 months of age was assessed for 3792
children aged 24-35 months.
Outcome measures
Coverage of EPI vaccinations and frequency of out-of-sequence vaccinations.
Results
Half of 12-month-old children and 65% of 24-month-old children had completed all
EPI vaccinations. Many children received vaccines out-of-sequence: by 12 months of
age 54% of BCG vaccinated children had received DTP with or before BCG and 28%
of measles vaccinated children had received DTP with or after MV. By 24 months of
age the proportion of out-of-sequence vaccinations was 58% and 35%, respectively,
for BCG and MV.
Conclusions
In rural Guinea-Bissau vaccination coverage by 12 months of age was low, but
continued to increase beyond 12 month of age. More than half of all children received
vaccinations out-of-sequence. This highlights the need to improve vaccination
services.
Page 2 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
3
ARTICLE SUMMARY
Article focus
- The World Health Organization (WHO) aims for a 90% coverage of the
Expanded Program on Immunization (EPI) by 12 months of age.
- The third dose of diphtheria-tetanus-pertussis vaccine (DTP3) is used as a
proxy for vaccination coverage and performance.
- Several studies indicate that the sequence of vaccinations affects child
mortality, but current polices do not take out-of-sequence vaccinations into
consideration.
Key messages
- Only half of all children were fully vaccinated by 12 months of age, but the
coverage continued to increase beyond 12 months of age.
- Limiting vaccination services to children less than 12 months of age will lower
the effective vaccination coverage considerably.
- More than half of the children received vaccinations out-of sequence.
Strengths and limitations of this study
- The study population was sizeable and the continued demographic
surveillance has many advantages compared with EPI household surveys.
- Though the study was representative for rural Guinea-Bissau, it may not
necessarily be representative of other low-income settings.
Page 3 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
4
INTRODUCTION
In 1974 the World Health Organization (WHO) launched the Expanded Program on
Immunization (EPI), to provide routine vaccinations against tuberculosis, polio,
diphtheria, tetanus, pertussis and measles to all children. At the time less than 5% of
children worldwide were vaccinated against these diseases.[1] In most low-income
countries the core vaccines in the EPI vaccines are bacillus Calmette-Guérin vaccine
(BCG) and oral polio vaccine (OPV) at birth, diphtheria- tetanus-pertussis vaccine
(DTP) and OPV at 6, 10 and 14 weeks and measles vaccine (MV) at 9 months of age
though new vaccines are now being added in many places.[2]
The Global Immunization Vision and Strategy 2006-2015 (GIVS) developed by the
WHO/UNICEF focused on ensuring equity in access to vaccination and aimed for a
90% national vaccination coverage and a 80% vaccination coverage in every district
by 2010.[3]
WHO and UNICEF estimates of vaccination coverage are based on reports of
vaccinations performed by service providers (administrative data) and surveys of
vaccination history (coverage surveys). The estimates refer to vaccinations given
during routine immunisation services to children below 12 months of age, not
including supplemental activities such as campaigns with OPV and MV. The
administrative data are based on the number of vaccine doses administered to the
estimated target population, most commonly the estimated number of children
surviving their first year of life.[4] The WHO EPI cluster methodology is commonly
used for coverage surveys. Survey results typically report on annual cohorts of
children so that all children included have had 12 months to receive all vaccinations,
i.e. being between 12–23 months of age at the time of the survey as shown in figure
1.[4,5]
Studies from Guinea-Bissau and other low-income countries suggest that the routine
vaccinations have effects on mortality beyond that of protecting against the target
disease. These effects are referred to as non-specific effects (NSE). BCG and MV
have beneficial effects in lowering overall child morbidity and mortality,[6-18]
whereas DTP may be associated with increased morbidity and mortality.[7-
9,11,12,17-21] The NSEs depend on the most recent vaccine and giving vaccines out-
Page 4 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
5
of-sequence may therefore affect child mortality. Worryingly several studies have
shown that DTP given together with MV or after MV is associated with increased
child morbidity and mortality.[9-13,19,21-23]
The purpose of this study was to determine the overall vaccination coverage of EPI
routine vaccinations and to determine the prevalence of out-of-sequence vaccinations
in rural Guinea-Bissau. Both outcomes were determined among 12-month-old and 24-
month-old children.
METHODS
Setting
In 1978, the Bandim Health Project (BHP) was established as a Health and
Demographic Surveillance System (HDSS) in Guinea-Bissau. Outside the capital,
Guinea-Bissau is divided into ten health regions. Since 1990, five of these regions
have been visited biannually by mobile teams from BHP. At each visit the teams
collect information about health, socio-economic and vaccination status. In 2006, the
remaining regions were included in the surveillance and the mobile teams now cover
all ten regions. The study population in the HDSS is based on 182 randomly selected
clusters of 100 women of fertile age and their children below five years of age living
in a total of 258 villages. In the cluster areas all new households are registered and in
all households new women and children taking up residence are added. The HDSS
cohort is therefore continuously growing.
Study population
The study population for the present study was extracted from the HDSS cohort. The
population base for the 12-month-old children was children born from the 1st January
2004 until 31st of December 2006, registered before 12 months of age and resident in
the study area when completing 12 months of age. For the 24-month-old children,
children born from the 1st January 2004 until 31st of December 2005, registered before
24 months of age and resident in the study area when completing 24 months of age
were included.
Vaccinations
Page 5 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
6
Guinea-Bissau follows the standard EPI. Children in the present study were to be
vaccinated in accordance with the EPI schedule shown in figure 1, which at the time
included only BCG, OPV0-3, DTP1-3 and MV. The booster MV (MV2) is not part of
the routine vaccination schedule as the MV coverage in Guinea-Bissau is far from the
80% criterion for implementation of MV2.[24] MV campaigns have been conducted
in 2006 and 2009.
A child in Guinea-Bissau can be vaccinated at hospitals, most health centres and
during outreach visits to the villages. All national vaccines are provided through
UNICEF and are free of charge for the parents. However, in order for a child to
receive its vaccinations it must have a vaccination card. The card is used to register
the child’s personal information, vaccinations and the weight of the child. Although
the card should also be free of charge, it is most often sold by the health workers for
the equivalent of $ 1(unpublished data). Since September 2007, the BHP teams have
been accompanied by nurses who vaccinate children missing doses of OPV, DTP or
MV and children receive a vaccination card free of charge. Children were only
included in the two cohorts for this study if they had reached 12 or 24 months of age
before the BHP nurses began administering vaccines.
Assessment of vaccination coverage
To emulate the EPI survey methodology used by WHO, we determined the
vaccination coverage by 12 months of age in children aged 12-23 months at the time
of a home visit. Vaccination status was determined based on the first visit among
children aged 12-23 months in 2005-2009 at which vaccination status could be
assessed by inspecting the vaccination card. If the child did not have a vaccination
card at the time of our visits, it was defined as unvaccinated if the mother confirmed
that the child had never received any vaccines. If we were not able to verify a child’s
vaccinations at any visit in the interval of 12-23 months of age either by 1) seeing the
vaccination card or 2) ascertaining that the child had never received vaccinations, the
child was not included in the analysis. The vaccination status by 24 months of age
was determined using the same method for children visited at 24-35 months of age.
Definitions
Page 6 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
7
We defined fully vaccinated as completion of the EPI vaccinations not including OPV
at birth (OPV0), because very few children receive OPV0 in the rural areas. Out-of-
sequence vaccinations were 1) BCG administered together with any dose of DTP, 2)
any dose of DTP before BCG, 3) MV with any dose of DTP and 4) any dose of DTP
after MV.
Statistical analysis
Relative risks and 95% confidence intervals (CI) were calculated using Poisson
regression with robust variance estimates.[25] Regional coverages were compared
using chi-2-tests. Data was analysed using STATA 11.0.
RESULTS
We determined vaccination status for 5806 children by 12 months of age and for 3792
children by 24 months of age (figure 2). A larger proportion of children were assessed
by 12 months of age (68%) than by 24 months of age (59%), RR=1.15 (95% CI 1.12-
1.18).
Vaccination coverage
By 12 months of age only 50% of children were fully vaccinated if reception of OPV0
was disregarded. If OPV0 was included in the definition of “fully vaccinated” only
9% of 12-month-old children were fully vaccinated. There were large regional
differences: only 26% of children were fully vaccinated in the region of Tombali
compared with 65% in Gabu and Bafata, the regions with highest coverage (table 1).
By 24 months of age the percentage of fully vaccinated children was 65%, a 29%
(95%CI =25-34%) increase. The increase ranged from 20% to 87% in the different
regions (table 1).
Vaccine-specific coverages by 12 months of age were: BCG 89%, OPV0 13%, OPV1
91%, OPV2 82%, OPV3 66%, DTP1 92%, DTP2 83%, DTP3 68% and MV 61%,
with large regional differences (table 2). The drop-out rate between DTP1 and DTP3
was 24% and the dropout rate between BCG and MV was 31%. There was only a
slight increase in the vaccines the children receive early in life when comparing
vaccine coverage at 12 and 24 months of age, but the increase for vaccines given later
in life was much higher. BCG, OPV1 and DTP1 increased by 3%, whereas OPV3
Page 7 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
8
increased by 12%, DTP3 by 11% and MV increased by 28% (figure 3). By 24 months
of age, the drop-out rate between DTP1 and DTP3 was 20% and 13% between BCG
and MV. The DTP3 coverage was higher than the MV coverage by 12 months of age
in all regions, except for Tombali. By 24 months of age the overall MV coverage was
higher than DTP3, but in four out of ten regions (Cacheu, Quinara, Bijagós and
Bolama) the MV coverage was still lower than the DTP3 coverage (data not shown).
Out-of-sequence vaccinations
Among children who had received BCG by 12 months of age, 49% received BCG
together with a dose of DTP and 54% DTP with or before BCG. By 24 months of age
these proportions were 52% and 58% (table 3). The region of Bijagós managed to stay
well below 30%. In comparison in Tombali more than 75% of children in both age
groups received DTP with or before BCG (table 3).
Among children who had received MV by 12 months of age, 26% received it together
with a dose of DTP; this figure was 29% by 24 months of age. Among the children
who had received MV, 28% had received DTP with or after MV by 12 months of age,
and this increased to 35% by 24 months of age, a 25% (95%CI=16-34%) increase
(table 3). Again there were large regional differences (table 3).
DISCUSSION
Main results
There were two main observations. First, only half of all children were fully
vaccinated by 12 months of age and 65% by 24 months of age (table 1, figure 2).
Estimating vaccination coverage only by 12 months of age therefore underestimates
the final coverage considerably. Many children had initiated the vaccination program,
but not received all the EPI vaccines by 12 months of age. This was reflected in high
coverage of vaccines scheduled early in life, with little increased from 12 to 24
months of age, whereas the increase in vaccines scheduled later in infancy was much
higher: MV increased by 28% (25-31%) (figure 3).
Second, a substantial number of children received out-of-sequence vaccinations. More
than half of all BCG vaccinated children received DTP with or before BCG and a
third of MV vaccinated children received DTP with or after MV (table 3). As
Page 8 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
9
vaccination coverage increased among 24-month-old children, so did the frequency of
out-of-sequence vaccinations (tables 1,3).
Strengths and weaknesses
The HDSS clusters are randomly selected in all regions. The sample size is substantial
and the data obtained is therefore representative of the population in Guinea-Bissau
excluding the urban area of Bissau. The villages have been visited biannually for
years, thus offering the opportunity to verify and correct ambiguous data. We believe
that the continued surveillance contributes to more reliable data than other types of
surveys. For example, in this study, children with previously registered vaccinations
could not be misclassified as unvaccinated at a later visit if the vaccinations card had
been lost. A study from Malawi showed a BCG scar rate of 70% among children
without documents, making it clear how vaccination coverage can be underestimated
if children without vaccination cards are classified as unvaccinated.[26] We also
registered pregnancies and births and could thereby determine date of birth fairly
precisely if there was no written record.
Comparison to other studies
We found that estimating vaccination coverage among 12-month-old children
underestimated final coverage. Similarly, Clark and Sanderson found that DTP3
coverage increased from 67% to 74% and MV from 59% to 77%, when comparing
the coverage at 12 months of age to the coverage at 36 months of age in survey data
from 45 low- and middle-income countries.[27]
In our study we emulated the methodology used by the WHO to make the results
comparable. A WHO EPI cluster survey was conducted in the capital Bissau in 2005
using vaccination cards or history to confirm vaccination status. It found vaccine
coverage to be: BCG 87%, OPV3 60%, DTP3 59% and MV 71%, with a 26%
DTP1/DTP3 dropout rate.[28] When we compared their results to ours, BCG
coverage did not differ, but the WHO OPV3 and DTP3 coverage was 10-13% (5-
18%) lower and the WHO MV coverage was 16% (11-21%) higher than our estimates
(table 2,[28]). The higher MV coverage may in part be explained by our study not
including data from the urban Bissau. In Bissau the coverage is higher as vaccinations
are more accessible. However, surprisingly higher coverage of all antigens was not
Page 9 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
10
found in the WHO survey. If the WHO survey underestimated the true coverage it
could in part be due to the use of history, i.e. maternal recall, to confirm vaccination
status. The validity of recall is correlated to the number of doses received and the age
of the child. Mothers tend to recall vaccinations more accurately for younger children
with fewer doses and the use of recall seems to underestimate vaccination
coverage.[29,30] In the WHO survey, visits are made to randomly selected houses
according to the survey method.[5] Unlike in our study, there are no follow-up visits
to households in which the vaccination status for a child can not be determined at the
time of the visit. The WHO EPI survey methodology has previously been criticised
for lacking methodological rigour and for introducing bias.[31,32]
Implications
The vaccination coverage estimates used by WHO and United Nations Children’s
Fund (UNICEF) emphasises the coverage by 12 months of age, not taking into
account the timing of the vaccines received or vaccines received after 12 months of
age.[33,34] Also, DTP3 is used by funding agencies to evaluate programme
performance[35] and improvements in DTP3 coverage is often linked to additional
funding.[36] This emphasis on vaccinations given during the first year of life and on
DTP3 rather than MV may have unwarranted consequences. First, there is less focus
on MV[37,38] and many African countries now have a lower coverage of MV than
DTP3.[2] Second, the current donor focus on vaccination status by 12 months of age
may lead to vaccination providers limiting vaccinations only to children less 12
months of age. This has happened in Guinea-Bissau recently, after the completion of
this study.[38] Our data showed that MV coverage increased by 28% during the
second year of life. Not vaccinating children after 12 months of age provides only a 3-
month-window for children to receive routine MV and based on our data it will lead
to a considerably lower MV coverage. Added together the emphasis on early
vaccinations and on DTP3 rather on MV is likely to lead to more children with DTP
as their last vaccination and an increasing number of children not receiving MV. This
may be particularly unfortunate as several studies show that MV lowers overall child
morbidity and mortality[6,8-14,16-18] whereas DTP is associated with increased
morbidity and mortality, especially for girls.[7-9,11,12,17-21]
Page 10 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
11
Currently the evaluation of the vaccination program does not take the frequency of
out-of-sequence vaccinations into account. Several studies have indicated that out-of-
sequence MV and DTP vaccinations have a negative effect on both child morbidity
and mortality[9-13,19,21-23]. The frequency of out-of-sequence vaccinations should
therefore be included as an indicator of the performance of routine vaccination
programmes.
CONCLUSION
Our study showed that the vaccination coverage in Guinea-Bissau is far from the
WHO goal of 90%. Only half of all 12-month-old children were fully vaccinated, with
great regional differences in vaccination coverage. Coverage based on vaccinations
received during the first 12 months of life significantly underestimated the final
coverage. We found that a considerable number of children received out-of-sequence
vaccinations. We suggest that vaccination coverage should also be reported by 24
months of age to encourage vaccination of older children and that the proportion of
children receiving DTP with or after MV should be the central performance indicator.
The focus on vaccinations to children less than 12 months of age[38] may lead to a
stop of vaccination of older children as experienced recently in Guinea-Bissau. This
will obviously restrain many children from completing their vaccination schedule and
this negative effect will be strongest for MV. This will lower herd immunity to
measles infections and increase the risk of epidemics. Since all studies show that MV
administered as the most recent vaccine has a beneficial effect on child survival[6,8-
14,16-18] it may also have unfortunate consequences that an increasing proportion of
children will have DTP as their most recent vaccination.[7-9,11,12,17-21]
Funding
This study was supported by the Danish Medical Research Council, the Aase and
Ejnar Danielsen's Foundation and DANIDA. The Bandim Health Project received
support from DANIDA to conduct their rural HDSS. CVIVA receives support from
the Danish National Research Foundation. CSB is funded by the European Research
Council (ERC-2009-StG, grant agreement no. 243149). PA holds a research
professorship grant from the Novo Nordic Foundation. Funding agencies had no hand
Page 11 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
12
in study design, execution, data analysis, data interpretation or the writing of this
paper.
Competing interests
None declared.
Contributors
LH, ABF, CSB and PA designed and planned the study. LH, ABF, MF and AR
supervised data collection and data entry. LH carried out the statistical analysis with
help from ABF, CSB and PA. LH wrote the first draft of the paper and holds the
primary responsibility for its final content. All authors contributed to and approved
the final manuscript.
Ethical approval
No ethical approval has been sought for this study as its data is observational and
derived from the Bandim Health Project’s HDSS which has been in place in Guinea-
Bissau since 1978 and is conducted by request from the Guinean Ministry of Health.
Data sharing statement
No additional data available.
Page 12 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
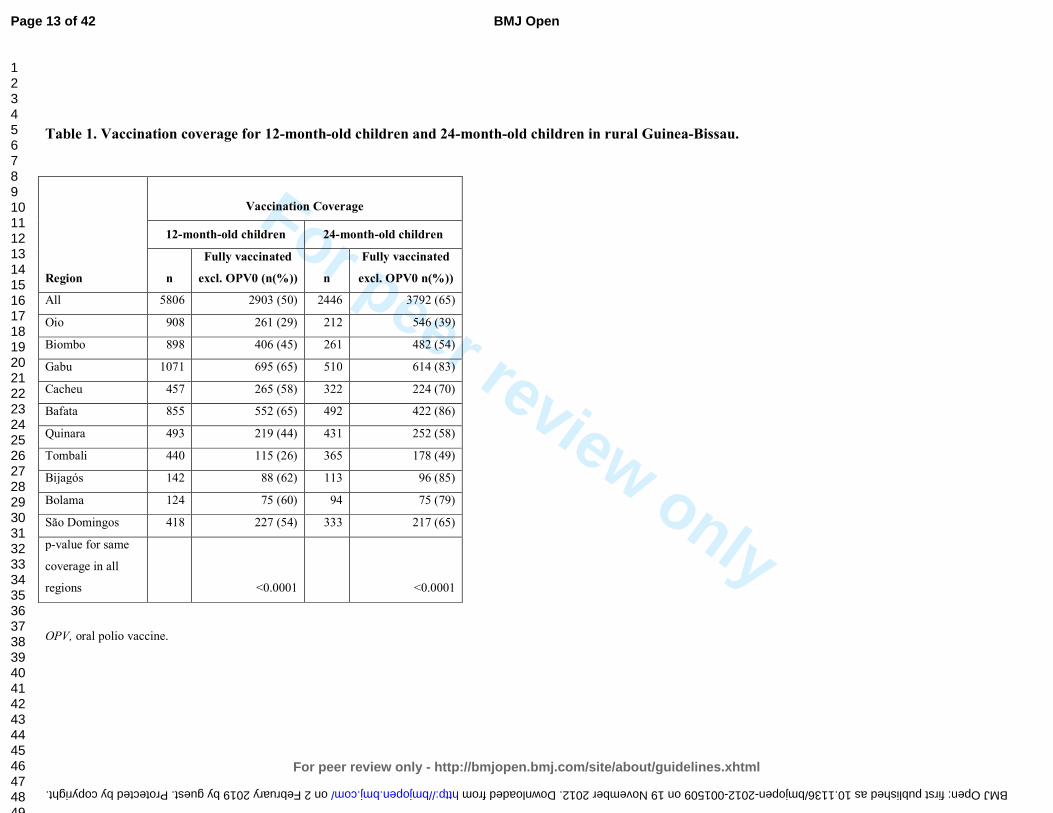
For peer review only
Table 1. Vaccination coverage for 12-month-old children and 24-month-old children in rural Guinea-Bissau.
Region
Vaccination Coverage
12-month-old children 24-month-old children
n
Fully vaccinated
excl. OPV0 (n(%))
n
Fully vaccinated
excl. OPV0 n(%))
All 5806 2903 (50) 2446 3792 (65)
Oio 908 261 (29) 212 546 (39)
Biombo 898 406 (45) 261 482 (54)
Gabu 1071 695 (65) 510 614 (83)
Cacheu 457 265 (58) 322 224 (70)
Bafata 855 552 (65) 492 422 (86)
Quinara 493 219 (44) 431 252 (58)
Tombali 440 115 (26) 365 178 (49)
Bijagós 142 88 (62) 113 96 (85)
Bolama 124 75 (60) 94 75 (79)
São Domingos 418 227 (54) 333 217 (65)
p-value for same
coverage in all
regions <0.0001 <0.0001
OPV, oral polio vaccine.
Page 13 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
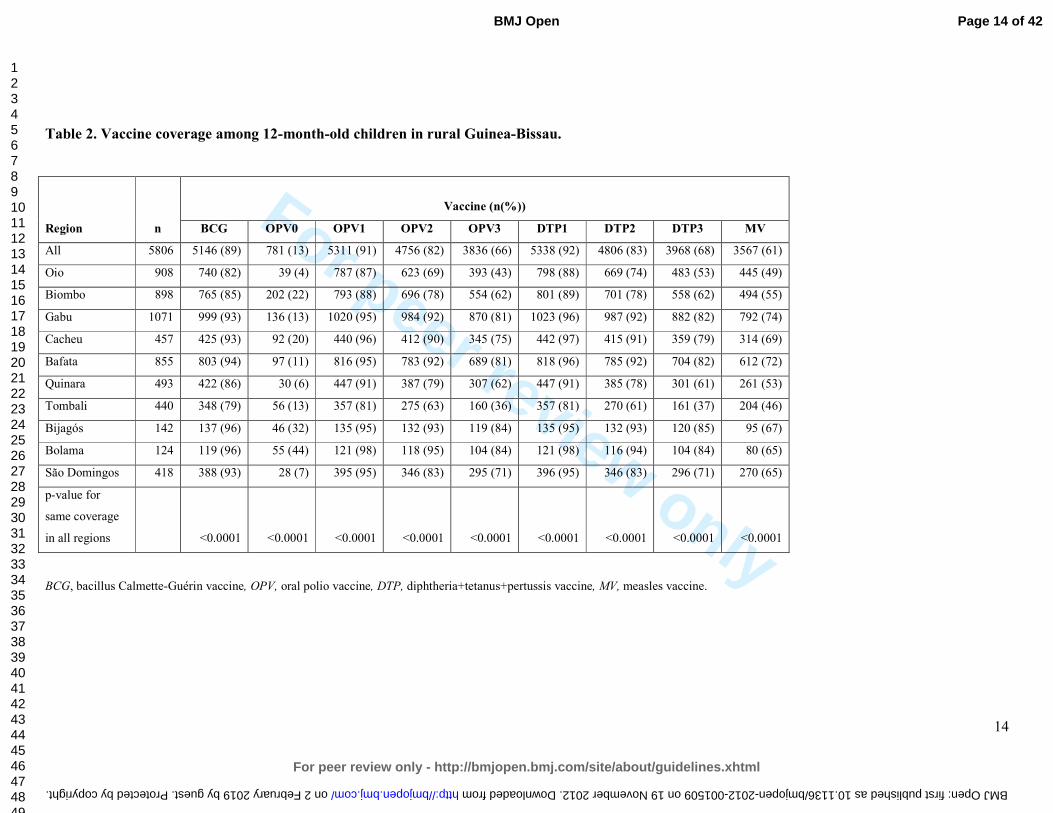
For peer review only
14
Table 2. Vaccine coverage among 12-month-old children in rural Guinea-Bissau.
Region n
Vaccine (n(%))
BCG OPV0 OPV1 OPV2 OPV3 DTP1 DTP2 DTP3 MV
All 5806 5146 (89) 781 (13) 5311 (91) 4756 (82) 3836 (66) 5338 (92) 4806 (83) 3968 (68) 3567 (61)
Oio 908 740 (82) 39 (4) 787 (87) 623 (69) 393 (43) 798 (88) 669 (74) 483 (53) 445 (49)
Biombo 898 765 (85) 202 (22) 793 (88) 696 (78) 554 (62) 801 (89) 701 (78) 558 (62) 494 (55)
Gabu 1071 999 (93) 136 (13) 1020 (95) 984 (92) 870 (81) 1023 (96) 987 (92) 882 (82) 792 (74)
Cacheu 457 425 (93) 92 (20) 440 (96) 412 (90) 345 (75) 442 (97) 415 (91) 359 (79) 314 (69)
Bafata 855 803 (94) 97 (11) 816 (95) 783 (92) 689 (81) 818 (96) 785 (92) 704 (82) 612 (72)
Quinara 493 422 (86) 30 (6) 447 (91) 387 (79) 307 (62) 447 (91) 385 (78) 301 (61) 261 (53)
Tombali 440 348 (79) 56 (13) 357 (81) 275 (63) 160 (36) 357 (81) 270 (61) 161 (37) 204 (46)
Bijagós 142 137 (96) 46 (32) 135 (95) 132 (93) 119 (84) 135 (95) 132 (93) 120 (85) 95 (67)
Bolama 124 119 (96) 55 (44) 121 (98) 118 (95) 104 (84) 121 (98) 116 (94) 104 (84) 80 (65)
São Domingos 418 388 (93) 28 (7) 395 (95) 346 (83) 295 (71) 396 (95) 346 (83) 296 (71) 270 (65)
p-value for
same coverage
in all regions
<0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine.
Page 14 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
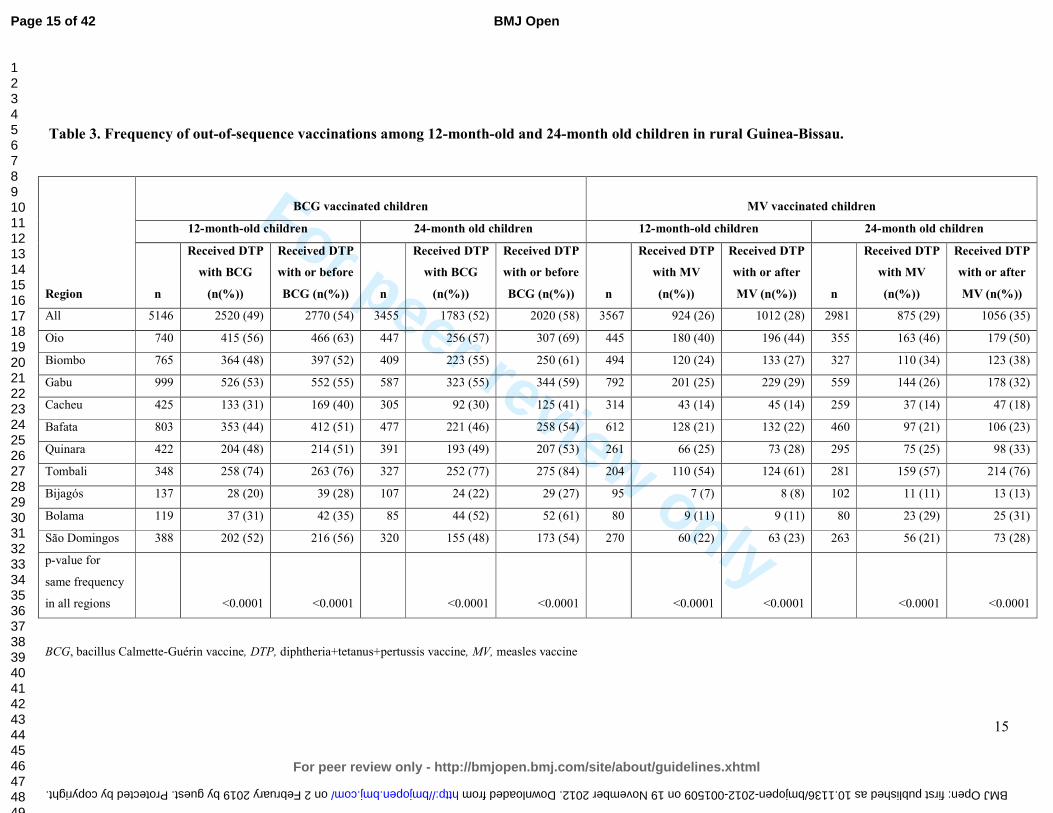
For peer review only
15
Table 3. Frequency of out-of-sequence vaccinations among 12-month-old and 24-month old children in rural Guinea-Bissau.
Region
BCG vaccinated children MV vaccinated children
12-month-old children 24-month old children 12-month-old children 24-month old children
n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%))
All 5146 2520 (49) 2770 (54) 3455 1783 (52) 2020 (58) 3567 924 (26) 1012 (28) 2981 875 (29) 1056 (35)
Oio 740 415 (56) 466 (63) 447 256 (57) 307 (69) 445 180 (40) 196 (44) 355 163 (46) 179 (50)
Biombo 765 364 (48) 397 (52) 409 223 (55) 250 (61) 494 120 (24) 133 (27) 327 110 (34) 123 (38)
Gabu 999 526 (53) 552 (55) 587 323 (55) 344 (59) 792 201 (25) 229 (29) 559 144 (26) 178 (32)
Cacheu 425 133 (31) 169 (40) 305 92 (30) 125 (41) 314 43 (14) 45 (14) 259 37 (14) 47 (18)
Bafata 803 353 (44) 412 (51) 477 221 (46) 258 (54) 612 128 (21) 132 (22) 460 97 (21) 106 (23)
Quinara 422 204 (48) 214 (51) 391 193 (49) 207 (53) 261 66 (25) 73 (28) 295 75 (25) 98 (33)
Tombali 348 258 (74) 263 (76) 327 252 (77) 275 (84) 204 110 (54) 124 (61) 281 159 (57) 214 (76)
Bijagós 137 28 (20) 39 (28) 107 24 (22) 29 (27) 95 7 (7) 8 (8) 102 11 (11) 13 (13)
Bolama 119 37 (31) 42 (35) 85 44 (52) 52 (61) 80 9 (11) 9 (11) 80 23 (29) 25 (31)
São Domingos 388 202 (52) 216 (56) 320 155 (48) 173 (54) 270 60 (22) 63 (23) 263 56 (21) 73 (28)
p-value for
same frequency
in all regions <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine
Page 15 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
REFERENCES
(1) UNICEF. Expanding Immunization Coverage. 2011. Available from: http://www.unicef.org/immunization/index_coverage.html.
(2) UNICEF, WHO. Immunization summary - A statistical reference containing data through 2010. WHO 2012.
(3) WHO. GIVS : global immunization vision and strategy : 2006-2015. WHO 2005.
(4) WHO. WHO vaccine-preventable diseases : monitoring system : 2010 global summary. WHO 2010.
(5) WHO. Immunization coverage cluster survey: Reference manual. WHO 2005.
(6) Aaby P, Samb B, Simondon F, et al. Non-specific beneficial effect of measles immunisation: analysis of mortality studies from developing countries. BMJ 1995;311:481-485.
(7) Aaby P, Jensen H, Gomes J, et al. The introduction of diphtheria-tetanus-pertussis vaccine and child mortality in rural Guinea-Bissau: an observational study. Int J Epidemiol 2004;33:374-380.
(8) Aaby P, Jensen H, Rodrigues A, et al. Divergent female-male mortality ratios associated with different routine vaccinations among female-male twin pairs. Int J Epidemiol 2004;33:367-373.
(9) Aaby P, Vessari H, Nielsen J, et al. Sex differential effects of routine immunizations and childhood survival in rural Malawi. Pediatr Infect Dis J 2006;25:721-727.
(10) Aaby P, Ibrahim SA, Libman MD, et al. The sequence of vaccinations and increased female mortality after high-titre measles vaccine: trials from rural Sudan and Kinshasa. Vaccine 2006;24:2764-2771.
(11) Aaby P, Jensen H, Walraven G. Age-specific changes in the female-male mortality ratio related to the pattern of vaccinations: an observational study from rural Gambia. Vaccine 2006;24:4701-4708.
(12) Aaby P, Martins C, Bale C, et al. Sex differences in the effect of vaccines on the risk of hospitalization due to measles in Guinea-bissau. Pediatr Infect Dis J 2010;29:324-328.
(13) Biai S, Rodrigues A, Nielsen J, et al. Vaccination status and sequence of vaccinations as risk factors for hospitalisation among outpatients in a high mortality country. Vaccine 2011;29:3662-3669.
(14) Breiman RF, Streatfield PK, Phelan M, et al. Effect of infant immunisation on childhood mortality in rural Bangladesh: analysis of health and demographic surveillance data. Lancet 2004;364:2204-2211.
(15) El-Zein M, Parent ME, Benedetti A, et al. Does BCG vaccination protect against the development of childhood asthma? A systematic review and meta-analysis of epidemiological studies. Int J Epidemiol 2010;39:469-486.
Page 16 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
17
(16) Kabir Z, Long J, Reddaiah VP, et al. Non-specific effect of measles vaccination on overall child mortality in an area of rural India with high vaccination coverage: a population-based case-control study. Bull World Health Organ 2003;81:244-250.
(17) Kristensen I, Aaby P, Jensen H. Routine vaccinations and child survival: follow up study in Guinea-Bissau, West Africa. BMJ 2000;321:1435-1438.
(18) Veirum JE, Sodemann M, Biai S, et al. Routine vaccinations associated with divergent effects on female and male mortality at the paediatric ward in Bissau, Guinea-Bissau. Vaccine 2005;23:1197-1204.
(19) Aaby P, Benn C, Nielsen J, et al. Testing the hypothesis that diphtheria-tetanus-pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012;2:e000707.
(20) Aaby P, Ravn H, Roth A, et al. Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial. Arch Dis Child 2012;97:685-691.
(21) Agergaard J, Nante E, Poulstrup G, et al. Diphtheria-tetanus-pertussis vaccine administered simultaneously with measles vaccine is associated with increased morbidity and poor growth in girls. A randomised trial from Guinea-Bissau. Vaccine 2011;29:487-500.
(22) Aaby P, Jensen H, Samb B, et al. Differences in female-male mortality after high-titre measles vaccine and association with subsequent vaccination with diphtheria-tetanus-pertussis and inactivated poliovirus: reanalysis of West African studies. Lancet 2003;361:2183-2188.
(23) Aaby P, Biai S, Veirum JE, et al. DTP with or after measles vaccination is associated with increased in-hospital mortality in Guinea-Bissau. Vaccine 2007;25:1265-1269.
(24) WHO. Weekly epidemiological record. 2009;35:349-360.
(25) Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 2003;3:21.
(26) Jahn A, Floyd S, Mwinuka V, et al. Ascertainment of childhood vaccination histories in northern Malawi. Trop Med Int Health 2008;13:129-138.
(27) Clark A, Sanderson C. Timing of children's vaccinations in 45 low-income and middle-income countries: an analysis of survey data. Lancet 2009;373:1543-1549.
(28) WHO, UNICEF. Review of national immunization coverage 1980-2008 - Guinea-Bissau. WHO 2009.
(29) Suarez L, Simpson DM, Smith DR. Errors and correlates in parental recall of child immunizations: effects on vaccination coverage estimates. Pediatrics 1997;99:E3.
(30) Valadez JJ, Weld LH. Maternal recall error of child vaccination status in a developing nation. Am J Public Health 1992;82:120-122.
(31) Luman ET, Worku A, Berhane Y, et al. Comparison of two survey methodologies to assess vaccination coverage. Int J Epidemiol 2007;36:633-641.
Page 17 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
18
(32) Burton A, Monasch R, Lautenbach B, et al. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull World Health Organ 2009;87:535-541.
(33) WHO, UNICEF, and World Bank. State of the world's vaccines and immunization. 3rd ed. WHO 2009.
(34) WHO. World Health Statistics 2011 - Indicator compendium. WHO 2011.
(35) GAVI alliance. Guidelines on country proposals - For support for: New and Underused Vaccines. GAVI alliance 2011.
(36) Arevshatian L, Clements C, Lwanga S, et al. An evaluation of infant immunization in Africa: is a transformation in progress? Bull World Health Organ 2007;85:449-457.
(37) Aaby P, Benn CS. Assessment of childhood immunisation coverage. Lancet 2009;373:1428.
(38) Fisker A, Hornshøj L, Rodrigues A, et al. The new decade of vaccines: Improving DTP-3 coverage and reducing coverage for measles vaccine. An observational study of the introduction of new vaccines in Guinea-Bissau. Submitted 2012.
Page 18 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from

For peer review only
Vaccination Coverage and Frequency of Out-of-Sequence Vaccinations in Rural
Guinea-Bissau: An Observational Cohort Study
Linda Hornshøja, Christine Stabell Benna,b Ane Bærent Fiskera,b, Manuel Fernandesa,
Amabelia Rodriguesa, Christine Stabell Benn
a,b, Peter Aaby
a,b, Ane Bærent Fisker
a,b
a) Bandim Health Project, INDEPTH Network, Apartado 861, Bissau, Guinea-Bissau
b) Research Center for Vitamins and Vaccines (CVIVA), Bandim Health Project,
Statens Serum Institut, 2300 Copenhagen S, Denmark
Corresponding author:
Linda Hornshøj, Research Center for Vitamins and Vaccines (CVIVA), Bandim
Health Project, Statens Serum Institut, 2300 Copenhagen S, Denmark. E-mail:
[email protected]. Telephone: +45 32683162.
Keywords:
EPI, vaccination, coverage, out-of-sequence, vaccines
Word count:
Abstract 29384, text 2746552
Page 19 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
2
ABSTRACT
Objective
The WHO aims for 90% coverage of the Expanded Program on Immunization (EPI),
which in Guinea-Bissau includeds bacillus Calmette-Guérin vaccine (BCG) at birth, 3
doses of diphtheria-tetanus-pertussis vaccine (DTP) and oral polio vaccine (OPV) at
6, 10 and 14 weeks and measles vaccine (MV) at 9 months when this study was
conducted. The WHO assesses coverage by 12 months of age. The sequence of
vaccines may have an effect on child mortality, but is not considered in official
statistics or assessments of programme performance. We assessed vaccination
coverage and frequency of out-of-sequence vaccinations by 12 and 24 months of age.
Design
Observational cohort study.
Setting and participants
The Bandim Health Project’s rural Health and Demographic Surveillance site System
in rural Guinea-Bissau was used, it covers 258 randomly selected villages in all
regions of Guinea-Bissau. Villages are visited biannually and vaccination cards
inspected to ascertain vaccination status. Between 2003 and 2009 vaccination status
by 12 months of age was assessed for 5806 children aged 12-23 months; vaccination
status and by 24 months of age was assessed for 3792 children aged 24-35 months.
Outcome measures
Coverage of EPI vaccinations and frequency of out-of-sequence vaccinations.
Results
Half of 12-month-old children and 65% of 24-month-old children had completed all
EPI vaccinations. Many children received vaccines out-of-sequence: by 12 months of
age 54% of BCG vaccinated children had received DTP with or before BCG and 28%
of measles vaccinated children had received DTP with or after MV. by 12 months of
age, bBy 24 months of age the proportion of out-of-sequence vaccinations was 58%
and 35%, respectively, for BCG and MV.
Conclusions
In rural Guinea-Bissau vaccination coverage by 12 months of age was low, but
continued to increase beyond 12 month of age. The current practice of limiting
vaccinations to children below 12 months of age will lower overall coverage
considerably. More than half of all children received vaccinations out-of-sequence.
This highlights the need to improve vaccination services.
Page 20 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
3
ARTICLE SUMMARY
Article focus
- The World Health Organization (WHO) aims for a 90% coverage of the
Expanded Program on Immunization (EPI) by 12 months of age.
- The third dose of diphtheria-tetanus-pertussis vaccine (DTP3) is used as a
proxy for vaccination coverage and performance.
- Several studies indicate that the sequence of vaccinations affects child
mortality, but current polices do not take out-of-sequence vaccinations into
considerationaccount.
Key messages
- Only half of all children were fully vaccinated by 12 months of age, but the
coverage continued to increase beyond 12 months of age.
- Limiting vaccination servicess to children less thanbelow 12 months of age
will lower the effectiveoverall vaccination coverage considerably.
- More than half of the children received vaccinations out-of sequence.
Strengths and limitations of this study
- The study population was sizeable and the continued demographic
surveillance has many advantages compared with EPIother household surveys.
- Though the study was representative for limited to rural Guinea-Bissau, it and
may not necessarily be representative of other low-income settings.
Page 21 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
4
INTRODUCTION
In 1974 the World Health Organization (WHO) launched the Expanded Program on
Immunization (EPI), to provide routine vaccinations against tuberculosis, polio,
diphtheria, tetanus, pertussis and measles to all children. At the time less than 5% of
children worldwide were vaccinated against these diseases.[1] In most low-income
countries the core vaccines in the standard schedule for EPI vaccines are includes
bacillus Calmette-Guérin vaccine (BCG) and oral polio vaccine (OPV) at birth,
diphtheria- tetanus-pertussis vaccine (DTP) and OPV at 6, 10 and 14 weeks and
measles vaccine (MV) at 9 months of age though new vaccines are now being added
in many places.[2]
The Global Immunization Vision and Strategy 2006-2015 (GIVS) developed by the
WHO/UNICEF focused on ensuring equity in access to vaccination and aimed for a
90% national vaccination coverage and a 80% vaccination coverage in every district
by 2010.[3]
WHO and UNICEF estimates of vaccination coverage are based on reports of
vaccinations performed by service providers (administrative data) and surveys of
vaccination history (coverage surveys). The estimates refer to vaccinations given
during routine immunisation services to children below 12 months of age, not
including supplemental activities such as OPV and MV campaigns with OPV and
MV. The administrative data are based on the number of vaccine doses administered
to the estimated target population, most commonly the estimated number of children
surviving their first year of life.[4] The WHO EPI cluster methodology is commonly
used for coverage surveys. Survey results typically report on annual cohorts of
children so that all children included have had 12 months to receive all vaccinations,
(i.e. being between 12–23 months of age at the time of the survey as shown in figure
1).[4,5]
Studies from Guinea-Bissau and other low-income countries suggest that the routine
vaccinations have effects on mortality beyond that of protecting against the target
disease. These effects are referred to as non-specific effects (NSE). BCG and MV
have beneficial effects in lowering overall child morbidity and mortality,[6-18][6-10]
whereas DTP may be associated with increased morbidity and mortality.[7-
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Page 22 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
5
9,11,12,17-21][6,9-17] The NSEs depend on the most recent vaccine and giving
vaccines out-of-sequence may therefore affect child mortality. Worryingly several
studies have shown that DTP given together with MV or after MV is associated with
increased child morbidity and mortality.[9-13,19,21-23][12,18-21]
The purpose of this study was to determine the overall vaccination coverage of EPI
routine vaccinations and to determine the prevalence of out-of-sequence vaccinations
in rural Guinea-Bissau. Both outcomes were determined among 12-month-old and 24-
month-old children.
METHODS
Setting
In 1978, the Bandim Health Project (BHP) was established as a Health and
Demographic Surveillance System (HDSS) in Guinea-Bissau. Outside the capital,
Guinea-Bissau is divided into ten health regions. Since 1990, five of these regions
have been visited biannually by mobile teams from BHP. At each visit the teams
collect information about health, socio-economic and vaccination status. In 2006, the
remaining regions were included in the surveillance and the mobile teams now cover
258 villages in all ten regions. The study population in the HDSS is based on 182
randomly selected clusters of 100 women of fertile age and their children below five
years of age living in a total of 258 villages. In the cluster areas all new households
are registered and in all households new women and children taking up residence are
added. The HDSS cohort is therefore continuously growing.
Study population
The study population for the present study was extracted from the HDSS cohort. The
population base for the 12-month-old children was children born from the 1st January
2004 until 31st of December 2006, registered before 12 months of age and resident in
the study area when completing 12 months of age. For the 24-month-old children,
children born from the 1st January 2004 until 31
st of December 2005, registered before
24 months of age and resident in the study area when completing 24 months of age
were included.
Vaccinations
Page 23 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
6
Guinea-Bissau follows the standard EPI. and cChildren in the present study were to be
vaccinated in accordance with the EPI schedule shown in figure 1, which at the time
included only BCG, OPV0-3, DTP1-3 and MV. The booster MV (MV2) is not part of
the routine vaccination schedule as the MV coverage in Guinea-Bissau is far from the
80% criterion for implementation of MV2.[24] MV campaigns have been conducted
in 2006 and 2009.
A child in Guinea-Bissau can be vaccinated at hospitals, most health centres and
during outreach visits to the villages. All national vaccines are provided through
UNICEF and are free of charge for the parents. However, in order for a child to
receive its vaccinations it must have a vaccination card. The card is used to register
the child’s personal information, vaccinations and the weight of the child. Although
the card should also be free of charge, it is most often sold by the health workers for
the equivalent of $ 1(unpublished data). Since September 2007, the BHP teams have
been accompanied by nurses who vaccinate children missing doses of OPV, DTP or
MV and children receive a vaccination card free of charge. CIn selection of the two
cohorts for this study, children were only included in the two cohorts for this study if
they had reached 12 or 24 months of age before the BHP nurses began administering
vaccines.
Assessment of vaccination coverage
To emulate the EPI survey methodology used by WHO, we determined the
vaccination coverage by 12 months of age in children aged 12-23 months at the time
of a home visits. Vaccination status was determined based on the first visit among
children aged 12-23 months in 2005-2009, at which vaccination status could be
assessed by inspecting the vaccination card. If the child did not have a vaccination
card at the time of our visits, it was defined as unvaccinated if the mother confirmed
that the child had never received any vaccines. If we were not able to verify a child’s
vaccinations at any visit in the interval of 12-23 months of age either by 1) by seeing
the vaccination card or 2) ascertaining that the child had never received vaccinations,
the child was not included in the analysis. The vaccination status by 24 months of age
was determined using the same method for children visited at 24-35 months of age.
Definitions
Page 24 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
7
We defined fully vaccinated as completion of the EPI vaccinations not including OPV
at birth (OPV0), because very few children receive d OPV0 in the rural areas.
Out-of-sequence vaccinations were 1) BCG administered together with any dose of
DTP, 2) any dose of DTP with or before BCG, 3) MV with any dose of DTP and 4)
any dose of DTP with or after MV.
Statistical analysis
Relative risks and 95% confidence intervals (CI) were calculated using Poisson
regression with robust variance estimates.[25][22] Regional Ccoverages werefor
different regions was compared using chi-2-tests. Data was analysed using STATA
11.0.
RESULTS
We determined vaccination status for 5806 children by 12 months of age and for 3792
children by 24 months of age (figure 2). A larger proportion of children were assessed
by 12 months of age (68%) than by 24 months of age (59%), RR=1.15 (95% CI
=1.12-1.18).
Vaccination coverage
By 12 months of age only 50% of children were fully vaccinated if reception whether
or not a child had received of OPV0 was disregarded. If OPV0 was included in the
definition of “fully vaccinated” only 9% of 12-month-old children were fully
vaccinated. There were large regional differences: only 26% of children were fully
vaccinated in the region of Tombali compared with 65% in Gabu and Bafata, the
regions with highest coverage (table 1). By 24 months of age the percentage of fully
vaccinated children was 65%, a 29% (95%CI =25-34%) increase. The increase ranged
from 20% to 87% in the different regions (table 1, figure 3).
Vaccine-specific coverages by 12 months of age were: BCG 89%, OPV0 13%, OPV1
91%, OPV2 82%, OPV3 66%, DTP1 92%, DTP2 83%, DTP3 68% and MV 61%,
with large regional differences (table 2). The drop-out rate between DTP1 and DTP3
was 24% and the dropout rate between BCG and MV was 31%. There was only a
slight increase in the vaccines the children receive early in life when comparing
vaccine coverage at 12 and 24 months of age, but the increase for vaccines given later
Page 25 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
8
in life was much higher. BCG, OPV1 and DTP1 increased by 3%, whereas OPV3
increased by 12%, DTP3 by 11% and MV increased by 28% (figure 34). By 24
months of age, the drop-out rate between DTP1 and DTP3 was 20% and 13%
between BCG and MV. The DTP3 coverage was higher than the MV coverage by 12
months of age in all regions, except for Tombali. By 24 months of age the overall MV
coverage was higher than DTP3, but in four out of ten regions (Cacheu, Quinara,
Bijagós and Bolama) the MV coverage was still lower than the DTP3 coverage (data
not shown).
Out-of-sequence vaccinations
Among children who had received BCG by 12 months of age, 49% received BCG
together with a dose of DTP and 54% DTP with or before BCG. By 24 months of age
these proportions were 52% and 58% (table 3). The region of Bijagós managed to stay
well below 30%. In comparison in Tombali more than 75% of children in both age
groups received DTP with or before BCG (table 3).
Among children who had received MV by 12 months of age, 26% received it together
with a dose of DTP; this figure was 29% by 24 months of age. Among the children
who had received MV, 28% had received DTP with or after MV by 12 months of age,
and this increased to 35% by 24 months of age, a 25% (95%CI=16-34%) increase
(table 3). Again there were large regional differences (table 3).
DISCUSSION
Main results
There were two main observations. FirstVaccinations are important in lowering
overall child mortality. In our study, only half of all children were fully vaccinated by
12 months of age and 65% by 24 months of age (table 1, figure 2). Only eEstimating
vaccination coverage only amongby 12- months of age-old children therefore
underestimates the final coverage considerably. Many children had initiated the
vaccination program, but not received all the EPI vaccines by 12 months of age. This
was reflected in high coverage of vaccines scheduled early in life, with little increased
from 12 to 24 months of age, whereas the increase in vaccines scheduled later in
infancy was much higher: MV increased by 28% (25-31%) (figure 34). Regional
Page 26 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
9
differences in vaccination coverage and frequency of out-of-sequence vaccinations
were large (tables 1,3).
Second, Aa substantial number of children received out-of-sequence vaccinations.
More than half of all BCG vaccinated children received DTP with or before BCG and
a third of MV vaccinated children received DTP with or after MV (table 3). As
vaccination coverage increased among 24-month-old children, so did the frequency of
out-of-sequence vaccinations (tables 1,3).
Strengths and weaknesses
The HDSS clusters are randomly selected in all regions. Tand the sample size is
substantial and the data obtained is therefore representative of the population in
Guinea-Bissau excluding the urban area of Bissau. The villages have been visited
biannually for years, thus offering the opportunity to verify and correct ambiguous
data. We believe that the continued surveillance contributes to more reliable data than
other types of surveys. For example, in this study, children with previously registered
vaccinations could not be misclassified as unvaccinated at a later visit if the
vaccinations card had been lost. A study from Malawi showed a BCG scar rate of
70% among children without documents, making it clear how vaccination coverage
can be underestimated if children without vaccination cards are simply classified as
unvaccinated.[26][23] We also registered pregnancies and births and could thereby
determine date of birth fairly precisely if there was no written record.
Comparison to other studies
We found that estimating vaccination coverage among 12-month-old children
underestimated final coverage. Similarly, Clark and Sanderson found that DTP3
coverage increased from 67% to 74% and MV from 59% to 77%, when comparing
the coverage at 12 months of age to the coverage at 36 months of age in survey data
from 45 low- and middle-income countries.[27][24]
In our study we emulated the methodology used by the WHO to make the results
comparable. A WHO EPI cluster survey was conducted in the capital Bissau in 2005
using vaccination cards or history to confirm vaccination status. It found vaccine
Field Code Changed
Field Code Changed
Page 27 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
10
coverage to be: BCG 87%, OPV3 60%, DTP3 59% and MV 71%, with a 26%
DTP1/DTP3 dropout rate.[28][25] When we compared their results to ours, BCG
coverage did not differ, but the WHO OPV3 and DTP3 coverage was 10-13% (5-
18%) lower and the WHO MV coverage was 16% (11-21%) higher than our estimates
(table 2,[28][25]). The higher MV coverage may in part be explained by our study not
including data from the urban Bissau. In Bissau the coverage is higher as vaccinations
are more accessible. However, surprisingly higher coverage of all antigens was not
found in the WHO survey. If the WHO survey underestimated the true coverage it
could in part be due to the use of history, i.e. maternal recall, to confirm vaccination
status. The validity of recall is correlated to the number of doses received and the age
of the child. Mothers tend to recall vaccinations more accurately for younger children
with fewer doses and the use of recall seems to underestimate vaccination
coverage.[29,30][26,27] In the WHO survey, visits are made to randomly selected
houses according to the survey method.[5] Unlike in our study, there are no follow-up
visits to households in which the vaccination status for a child can not be determined
at the time of the visit. The WHO EPI survey methodology has previously been
criticised for lacking methodological rigour and for introducing bias.[31,32][28,29]
Implications
At presentThe vaccination coverage estimates used by WHO and United Nations
Children’s Fund (UNICEF) emphasises the coverage of DTP3 by 12 months of age,
not taking into account the timing of the vaccines received or vaccines received at a
later ageafter 12 months of age.[33,34][30,31] This has two consequences, which
may have large implications. First, the emphasis on DTP3 leads to more focus on
Also, DTP3 and less focus on measles vaccine. It is often used by funding agencies
such as the Global Alliance for Vaccines and Immunizations (GAVI) to evaluate
programme performance[35][32] and improvements in DTP3 coverage of vaccination
coverage is often linked to additional funding.[36][33] This emphasis on vaccinations
given during the first year of life and on DTP3 rather than MV may have unwarranted
consequences. First, there is less focus on MV[37,38] andAs a result many African
countries now have a lower coverage of MV than DTP3.[2] Second, the current donor
focus on vaccination status by 12 months of age may lead to vaccination providers
limiting vaccinations only to children less 12 months of age. This has happened in
Guinea-Bissau recently, after the completion of this study.[38] This is unfortunate.
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Field Code Changed
Page 28 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
11
Several studies show that MV lowers overall child morbidity and mortality[6-10,13-
15] and several studies suggest that DTP is associated with increased female
morbidity and mortality.[6,9-15]
Second, oOur data was from before 2007, and it showed that MV coverage increased
by 28% during the second year of life. However, the current donor focus on
vaccination status by 12 months of age leads to many countries, including Guinea-
Bissau, have now stopped vaccinating children above 12 months of age, because they
do not count in the statistics. The current policy not to vaccinate children above 12
months of age gives children only a 3-month-time-window to be measles vaccinated.
This will undoubtedly lead to a lower MV coverage and an increasing number of
children being susceptible to measles infectionNot vaccinating children after 12
months of age provides only a 3-month-window for children to receive routine MV
and based on our data it will lead to a considerably lower MV coverage. Added
together the emphasis on early vaccinations and on DTP3 rather on MV is likely to
lead to more children with DTP as their last vaccination and an increasing number of
children not receiving MV. This may be particularly unfortunate as several studies
show that MV lowers overall child morbidity and mortality[6,8-14,16-18] whereas
DTP is associated with increased morbidity and mortality, especially for girls.[7-
9,11,12,17-21]
Currently the evaluation of the vaccination program does not take the frequency of
out-of-sequence vaccinations into account. Several studies have indicated that out-of-
sequence MV and DTP vaccinations have a negative effect on both child morbidity
and mortality[9-13,19,21-23]. The frequency of out-of-sequence vaccinations should
therefore be included as an indicator of the performance of routine vaccination
programmes.
.
CONCLUSION
Our study showed that the vaccination coverage in Guinea-Bissau is far from the
WHO goal of 90%. Only half of all 12-month-old children were fully vaccinated, with
great regional differences in vaccination coverage. Coverage based on vaccinations
received during the first 12 months of life significantly underestimated the final
coverage. We found that a considerable number of children received out-of-sequence
Page 29 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
12
vaccinations. As several studies suggest that out-of-sequence vaccinations have an
impact on overall survival[18-21] such deviations from the schedule need to be taken
into account and should be reported as performance indicators for vaccination
programmes in likening with specific antigen coverage.
We suggest that vaccination coverage should also be reported by 24 months of age to
encourage vaccination of older children and that the proportion of children receiving
DTP with or after MV should be the central performance indicator.
The focus current drive to limit on vaccinations to children less thanbelow 12 months
of age[38][34] may lead to a stop of vaccination of older children as experienced
recently in Guinea-Bissau. This will obviously restrainprevent many children from
completing their vaccination schedule and this negative effect will be strongest for
MVmeasles vaccination. This will lower heard immunity to measles infections and
increase the risk of epidemics. Since all studies show that MVmeasles vaccination
administered as the most recent vaccine has a beneficial effect on child survival[6,8-
14,16-18][6-8,10,14] it may also will have unfortunate consequences that an
increasing proportion of children will have DTP as their most recent vaccination.[7-
9,11,12,17-21] [10,12,15,17,35]
Funding
This study was supported by the Danish Medical Research Council, the Aase and
Ejnar Danielsen's Foundation and DANIDA. The Bandim Health Project received
support from DANIDA to conduct their rural HDSS. CVIVA receives support from
the Danish National Research Foundation. CSB is funded by the European Research
Council (ERC-2009-StG, grant agreement no. 243149). PA holds a research
professorship grant from the Novo Nordic Foundation. Funding agencies had no hand
in study design, execution, data analysis, data interpretation or the writing of this
paper.
Competing interests
None declared.
Contributors
Page 30 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from

For peer review only
13
LH, ABF, CSB and PA designed and planned the study. LH, ABF, MF and AR
supervised data collection and data entry. LH carried out the statistical analysis with
help from ABF, CSB and PA. LH wrote the first draft of the paper and holds the
primary responsibility for its final content. All authors contributed to and approved
the final manuscript.
Ethical approval
No ethical approval has been sought for this study as its data is observational and
derived from the Bandim Health Project’s HDSS which has been in place in Guinea-
Bissau since 1978 and is conducted by request from the Guinean Ministry of Health.
Data sharing statement
No additional data available.
Page 31 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
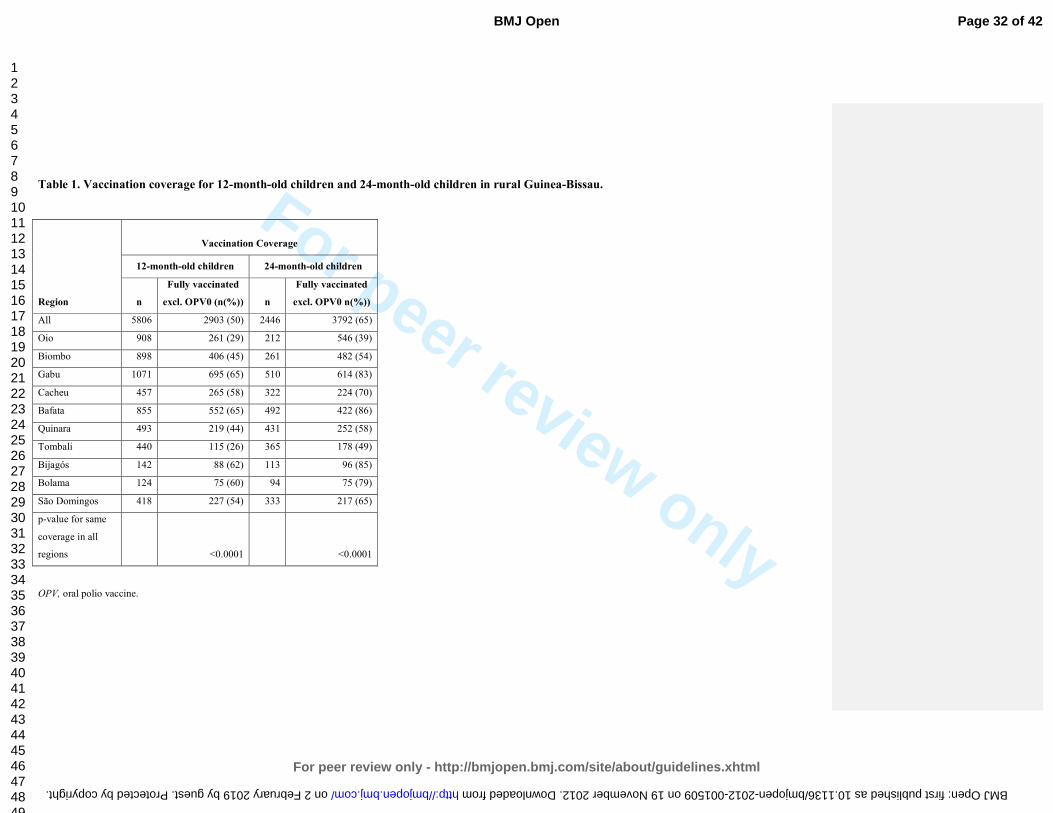
For peer review only
Table 1. Vaccination coverage for 12-month-old children and 24-month-old children in rural Guinea-Bissau.
Region
Vaccination Coverage
12-month-old children 24-month-old children
n
Fully vaccinated
excl. OPV0 (n(%))
n
Fully vaccinated
excl. OPV0 n(%))
All 5806 2903 (50) 2446 3792 (65)
Oio 908 261 (29) 212 546 (39)
Biombo 898 406 (45) 261 482 (54)
Gabu 1071 695 (65) 510 614 (83)
Cacheu 457 265 (58) 322 224 (70)
Bafata 855 552 (65) 492 422 (86)
Quinara 493 219 (44) 431 252 (58)
Tombali 440 115 (26) 365 178 (49)
Bijagós 142 88 (62) 113 96 (85)
Bolama 124 75 (60) 94 75 (79)
São Domingos 418 227 (54) 333 217 (65)
p-value for same
coverage in all
regions <0.0001 <0.0001
OPV, oral polio vaccine.
Page 32 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
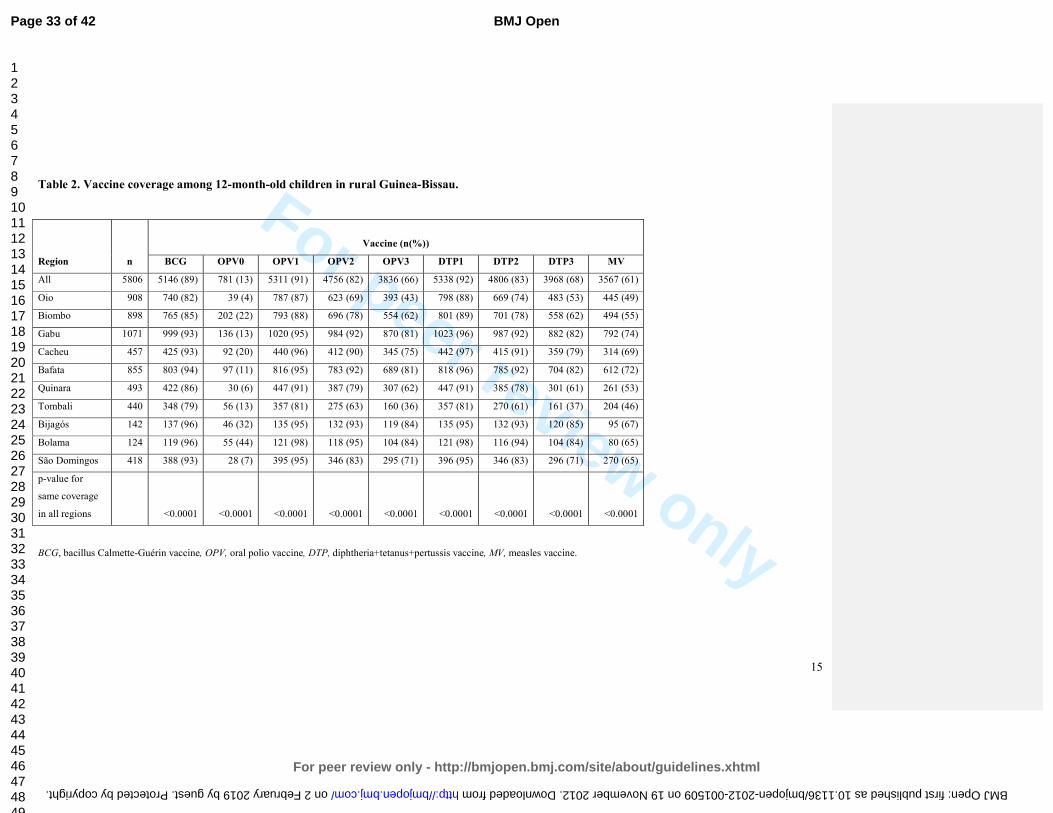
For peer review only
15
Table 2. Vaccine coverage among 12-month-old children in rural Guinea-Bissau.
Region n
Vaccine (n(%))
BCG OPV0 OPV1 OPV2 OPV3 DTP1 DTP2 DTP3 MV
All 5806 5146 (89) 781 (13) 5311 (91) 4756 (82) 3836 (66) 5338 (92) 4806 (83) 3968 (68) 3567 (61)
Oio 908 740 (82) 39 (4) 787 (87) 623 (69) 393 (43) 798 (88) 669 (74) 483 (53) 445 (49)
Biombo 898 765 (85) 202 (22) 793 (88) 696 (78) 554 (62) 801 (89) 701 (78) 558 (62) 494 (55)
Gabu 1071 999 (93) 136 (13) 1020 (95) 984 (92) 870 (81) 1023 (96) 987 (92) 882 (82) 792 (74)
Cacheu 457 425 (93) 92 (20) 440 (96) 412 (90) 345 (75) 442 (97) 415 (91) 359 (79) 314 (69)
Bafata 855 803 (94) 97 (11) 816 (95) 783 (92) 689 (81) 818 (96) 785 (92) 704 (82) 612 (72)
Quinara 493 422 (86) 30 (6) 447 (91) 387 (79) 307 (62) 447 (91) 385 (78) 301 (61) 261 (53)
Tombali 440 348 (79) 56 (13) 357 (81) 275 (63) 160 (36) 357 (81) 270 (61) 161 (37) 204 (46)
Bijagós 142 137 (96) 46 (32) 135 (95) 132 (93) 119 (84) 135 (95) 132 (93) 120 (85) 95 (67)
Bolama 124 119 (96) 55 (44) 121 (98) 118 (95) 104 (84) 121 (98) 116 (94) 104 (84) 80 (65)
São Domingos 418 388 (93) 28 (7) 395 (95) 346 (83) 295 (71) 396 (95) 346 (83) 296 (71) 270 (65)
p-value for
same coverage
in all regions
<0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine.
Page 33 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
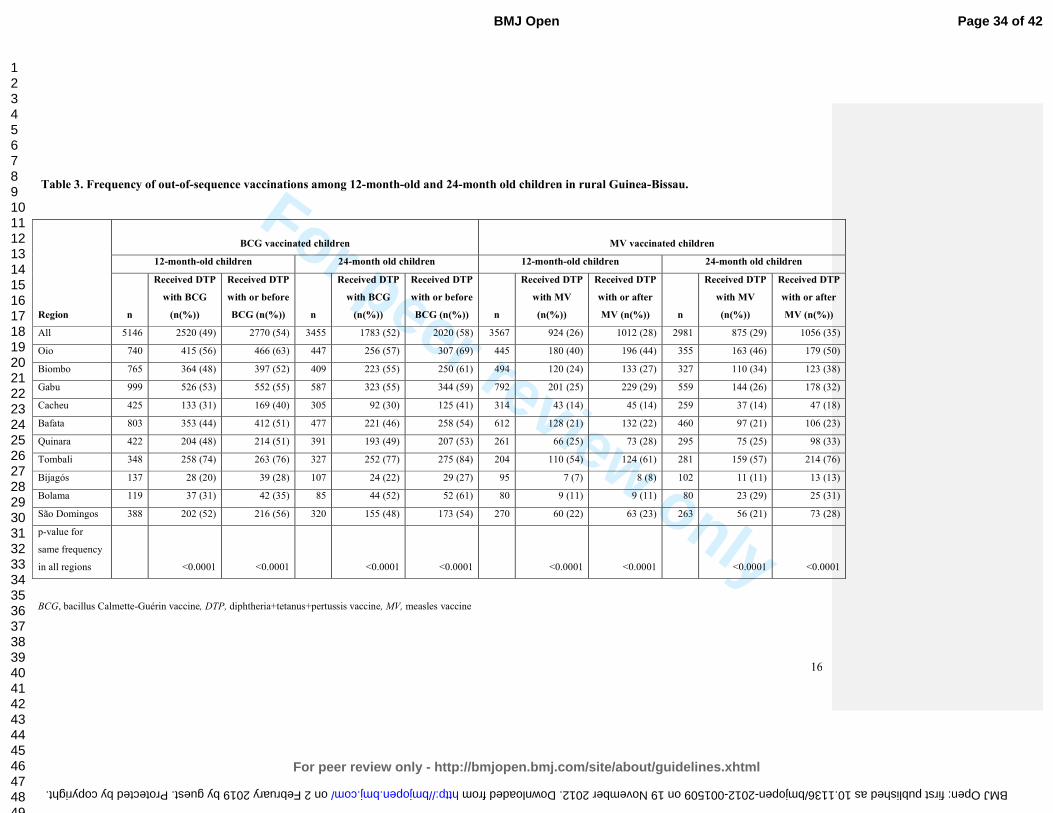
For peer review only
16
Table 3. Frequency of out-of-sequence vaccinations among 12-month-old and 24-month old children in rural Guinea-Bissau.
Region
BCG vaccinated children MV vaccinated children
12-month-old children 24-month old children 12-month-old children 24-month old children
n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with BCG
(n(%))
Received DTP
with or before
BCG (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%)) n
Received DTP
with MV
(n(%))
Received DTP
with or after
MV (n(%))
All 5146 2520 (49) 2770 (54) 3455 1783 (52) 2020 (58) 3567 924 (26) 1012 (28) 2981 875 (29) 1056 (35)
Oio 740 415 (56) 466 (63) 447 256 (57) 307 (69) 445 180 (40) 196 (44) 355 163 (46) 179 (50)
Biombo 765 364 (48) 397 (52) 409 223 (55) 250 (61) 494 120 (24) 133 (27) 327 110 (34) 123 (38)
Gabu 999 526 (53) 552 (55) 587 323 (55) 344 (59) 792 201 (25) 229 (29) 559 144 (26) 178 (32)
Cacheu 425 133 (31) 169 (40) 305 92 (30) 125 (41) 314 43 (14) 45 (14) 259 37 (14) 47 (18)
Bafata 803 353 (44) 412 (51) 477 221 (46) 258 (54) 612 128 (21) 132 (22) 460 97 (21) 106 (23)
Quinara 422 204 (48) 214 (51) 391 193 (49) 207 (53) 261 66 (25) 73 (28) 295 75 (25) 98 (33)
Tombali 348 258 (74) 263 (76) 327 252 (77) 275 (84) 204 110 (54) 124 (61) 281 159 (57) 214 (76)
Bijagós 137 28 (20) 39 (28) 107 24 (22) 29 (27) 95 7 (7) 8 (8) 102 11 (11) 13 (13)
Bolama 119 37 (31) 42 (35) 85 44 (52) 52 (61) 80 9 (11) 9 (11) 80 23 (29) 25 (31)
São Domingos 388 202 (52) 216 (56) 320 155 (48) 173 (54) 270 60 (22) 63 (23) 263 56 (21) 73 (28)
p-value for
same frequency
in all regions <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
BCG, bacillus Calmette-Guérin vaccine, DTP, diphtheria+tetanus+pertussis vaccine, MV, measles vaccine
Page 34 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
For peer review only
REFERENCES
(1) UNICEF. Expanding Immunization Coverage. 2011. Available from: http://www.unicef.org/immunization/index_coverage.html.
(2) UNICEF, WHO. Immunization summary - A statistical reference containing data through 2010. WHO 2012.
(3) WHO. GIVS : global immunization vision and strategy : 2006-2015. WHO 2005.
(4) WHO. WHO vaccine-preventable diseases : monitoring system : 2010 global summary. WHO 2010.
(5) WHO. Immunization coverage cluster survey: Reference manual. WHO 2005.
(6) Aaby P, Samb B, Simondon F, et al. Non-specific beneficial effect of measles immunisation: analysis of mortality studies from developing countries. BMJ 1995;311:481-485.
(7) Aaby P, Jensen H, Gomes J, et al. The introduction of diphtheria-tetanus-pertussis vaccine and child mortality in rural Guinea-Bissau: an observational study. Int J Epidemiol 2004;33:374-380.
(8) Aaby P, Jensen H, Rodrigues A, et al. Divergent female-male mortality ratios associated with different routine vaccinations among female-male twin pairs. Int J Epidemiol 2004;33:367-373.
(9) Aaby P, Vessari H, Nielsen J, et al. Sex differential effects of routine immunizations and childhood survival in rural Malawi. Pediatr Infect Dis J 2006;25:721-727.
(10) Aaby P, Ibrahim SA, Libman MD, et al. The sequence of vaccinations and increased female mortality after high-titre measles vaccine: trials from rural Sudan and Kinshasa. Vaccine 2006;24:2764-2771.
(11) Aaby P, Jensen H, Walraven G. Age-specific changes in the female-male mortality ratio related to the pattern of vaccinations: an observational study from rural Gambia. Vaccine 2006;24:4701-4708.
(12) Aaby P, Martins C, Bale C, et al. Sex differences in the effect of vaccines on the risk of hospitalization due to measles in Guinea-bissau. Pediatr Infect Dis J 2010;29:324-328.
(13) Biai S, Rodrigues A, Nielsen J, et al. Vaccination status and sequence of vaccinations as risk factors for hospitalisation among outpatients in a high mortality country. Vaccine 2011;29:3662-3669.
(14) Breiman RF, Streatfield PK, Phelan M, et al. Effect of infant immunisation on childhood mortality in rural Bangladesh: analysis of health and demographic surveillance data. Lancet 2004;364:2204-2211.
(15) El-Zein M, Parent ME, Benedetti A, et al. Does BCG vaccination protect against the development of childhood asthma? A systematic review and meta-analysis of epidemiological studies. Int J Epidemiol 2010;39:469-486.
Formatted: Space After: 12 pt
Page 35 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from

For peer review only
18
(16) Kabir Z, Long J, Reddaiah VP, et al. Non-specific effect of measles vaccination on overall child mortality in an area of rural India with high vaccination coverage: a population-based case-control study. Bull World Health Organ 2003;81:244-250.
(17) Kristensen I, Aaby P, Jensen H. Routine vaccinations and child survival: follow up study in Guinea-Bissau, West Africa. BMJ 2000;321:1435-1438.
(18) Veirum JE, Sodemann M, Biai S, et al. Routine vaccinations associated with divergent effects on female and male mortality at the paediatric ward in Bissau, Guinea-Bissau. Vaccine 2005;23:1197-1204.
(19) Aaby P, Benn C, Nielsen J, et al. Testing the hypothesis that diphtheria-tetanus-pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012;2:e000707.
(20) Aaby P, Ravn H, Roth A, et al. Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial. Arch Dis Child 2012;97:685-691.
(21) Agergaard J, Nante E, Poulstrup G, et al. Diphtheria-tetanus-pertussis vaccine administered simultaneously with measles vaccine is associated with increased morbidity and poor growth in girls. A randomised trial from Guinea-Bissau. Vaccine 2011;29:487-500.
(22) Aaby P, Jensen H, Samb B, et al. Differences in female-male mortality after high-titre measles vaccine and association with subsequent vaccination with diphtheria-tetanus-pertussis and inactivated poliovirus: reanalysis of West African studies. Lancet 2003;361:2183-2188.
(23) Aaby P, Biai S, Veirum JE, et al. DTP with or after measles vaccination is associated with increased in-hospital mortality in Guinea-Bissau. Vaccine 2007;25:1265-1269.
(24) WHO. Weekly epidemiological record. 2009;35:349-360.
(25) Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 2003;3:21.
(26) Jahn A, Floyd S, Mwinuka V, et al. Ascertainment of childhood vaccination histories in northern Malawi. Trop Med Int Health 2008;13:129-138.
(27) Clark A, Sanderson C. Timing of children's vaccinations in 45 low-income and middle-income countries: an analysis of survey data. Lancet 2009;373:1543-1549.
(28) WHO, UNICEF. Review of national immunization coverage 1980-2008 - Guinea-Bissau. WHO 2009.
(29) Suarez L, Simpson DM, Smith DR. Errors and correlates in parental recall of child immunizations: effects on vaccination coverage estimates. Pediatrics 1997;99:E3.
(30) Valadez JJ, Weld LH. Maternal recall error of child vaccination status in a developing nation. Am J Public Health 1992;82:120-122.
(31) Luman ET, Worku A, Berhane Y, et al. Comparison of two survey methodologies to assess vaccination coverage. Int J Epidemiol 2007;36:633-641.
Page 36 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
For peer review only
19
(32) Burton A, Monasch R, Lautenbach B, et al. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull World Health Organ 2009;87:535-541.
(33) WHO, UNICEF, and World Bank. State of the world's vaccines and immunization. 3rd ed.
WHO 2009.
(34) WHO. World Health Statistics 2011 - Indicator compendium. WHO 2011.
(35) GAVI alliance. Guidelines on country proposals - For support for: New and Underused Vaccines. GAVI alliance 2011.
(36) Arevshatian L, Clements C, Lwanga S, et al. An evaluation of infant immunization in Africa: is a transformation in progress? Bull World Health Organ 2007;85:449-457.
(37) Aaby P, Benn CS. Assessment of childhood immunisation coverage. Lancet 2009;373:1428.
(38) Fisker A, Hornshøj L, Rodrigues A, et al. The new decade of vaccines: Improving DTP-3 coverage and reducing coverage for measles vaccine. An observational study of the introduction of new vaccines in Guinea-Bissau. Submitted 2012.
Formatted: Tab stops: 0.5", Right + 0.63",
Left + Not at 0.38"
Page 37 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
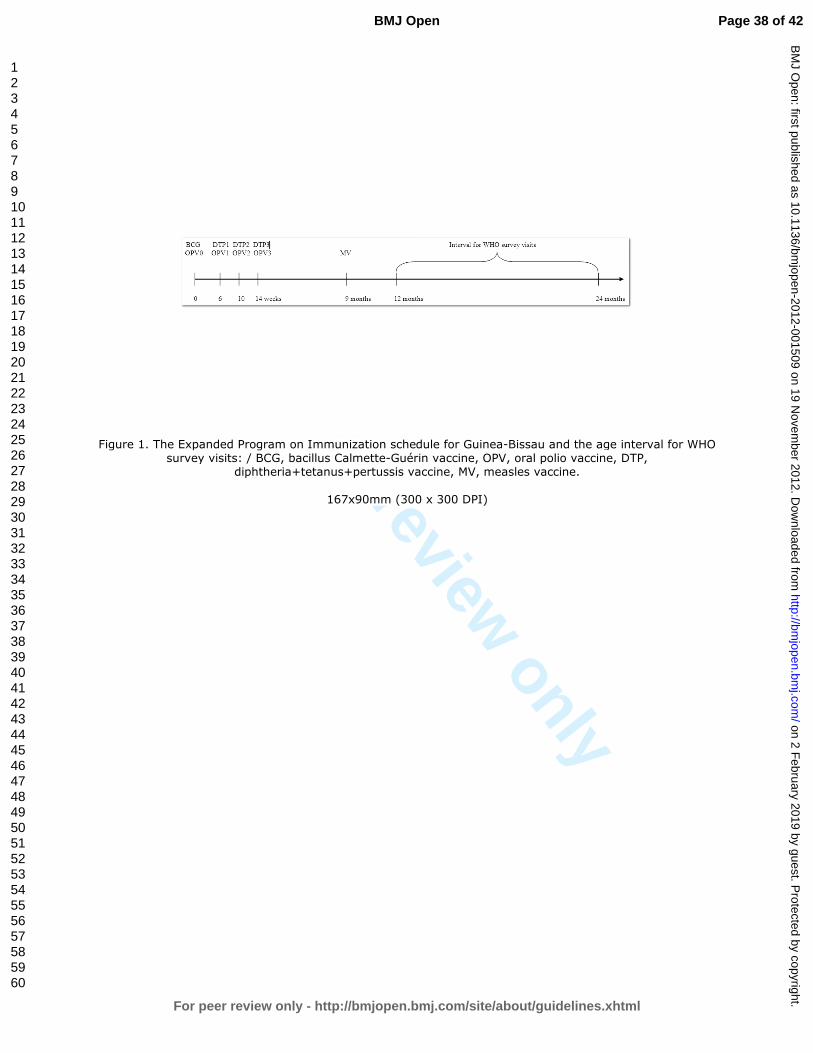
For peer review only
Figure 1. The Expanded Program on Immunization schedule for Guinea-Bissau and the age interval for WHO survey visits: / BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP,
diphtheria+tetanus+pertussis vaccine, MV, measles vaccine.
167x90mm (300 x 300 DPI)
Page 38 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
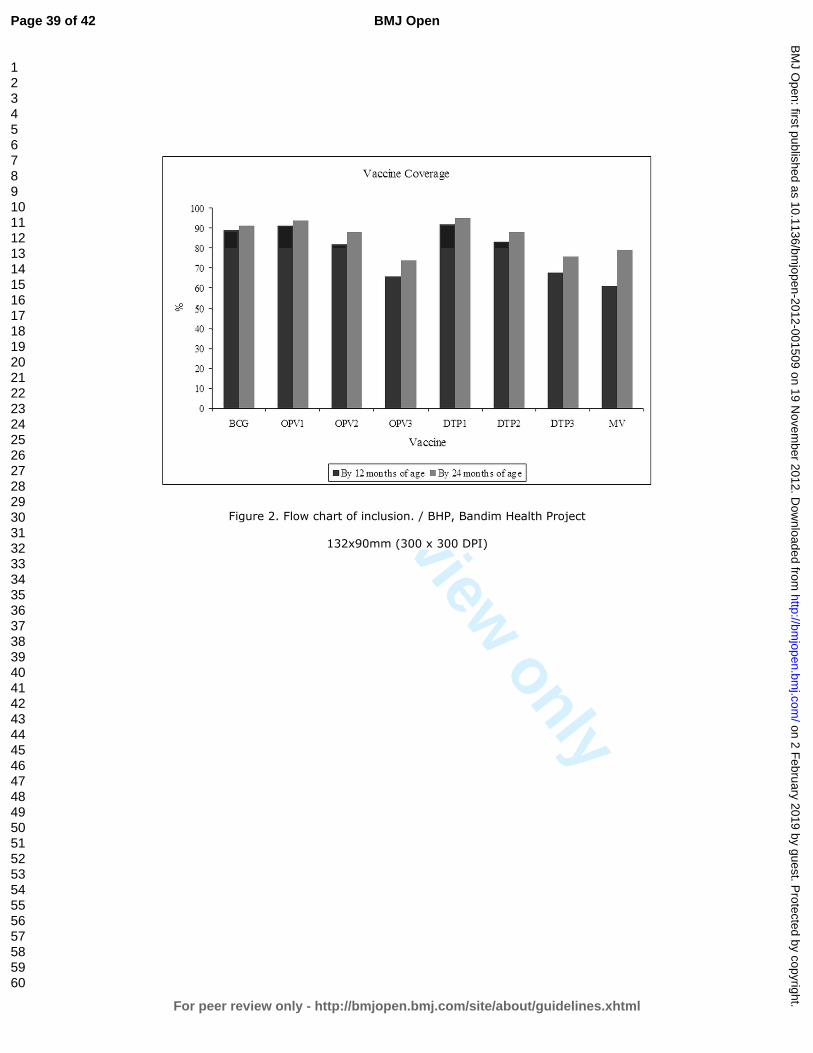
For peer review only
Figure 2. Flow chart of inclusion. / BHP, Bandim Health Project
132x90mm (300 x 300 DPI)
Page 39 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
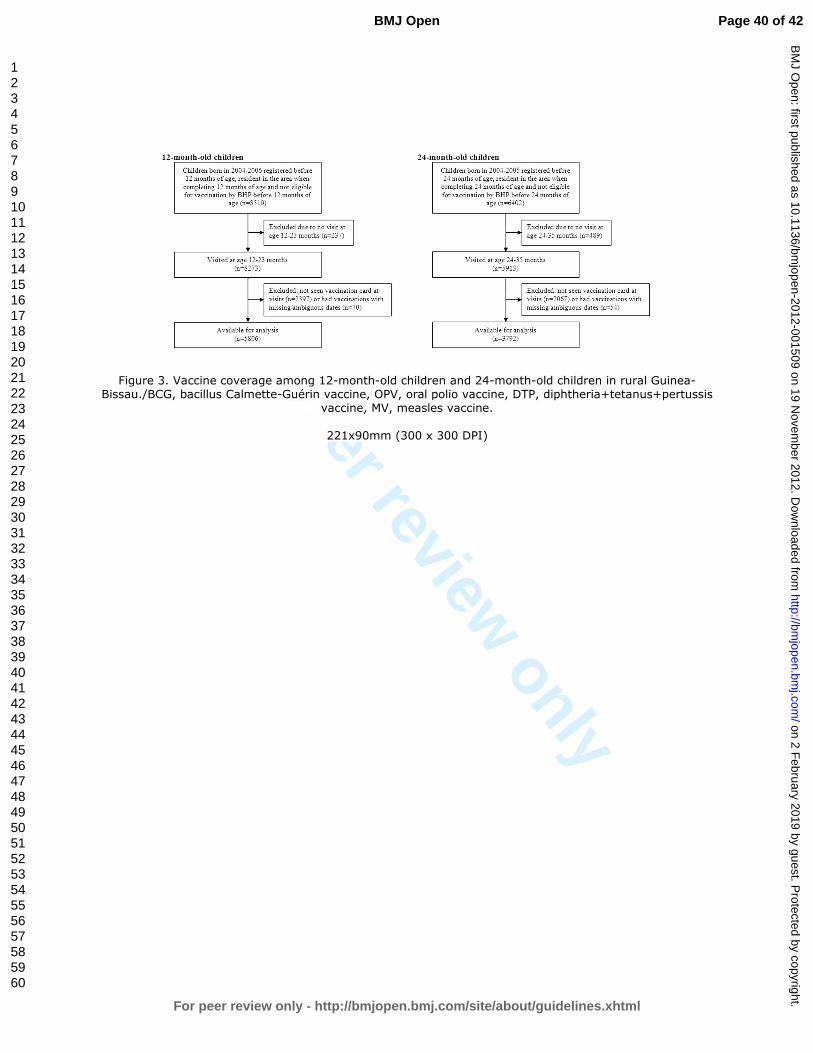
For peer review only
Figure 3. Vaccine coverage among 12-month-old children and 24-month-old children in rural Guinea-Bissau./BCG, bacillus Calmette-Guérin vaccine, OPV, oral polio vaccine, DTP, diphtheria+tetanus+pertussis
vaccine, MV, measles vaccine.
221x90mm (300 x 300 DPI)
Page 40 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2012-001509 on 19 N
ovember 2012. D
ownloaded from
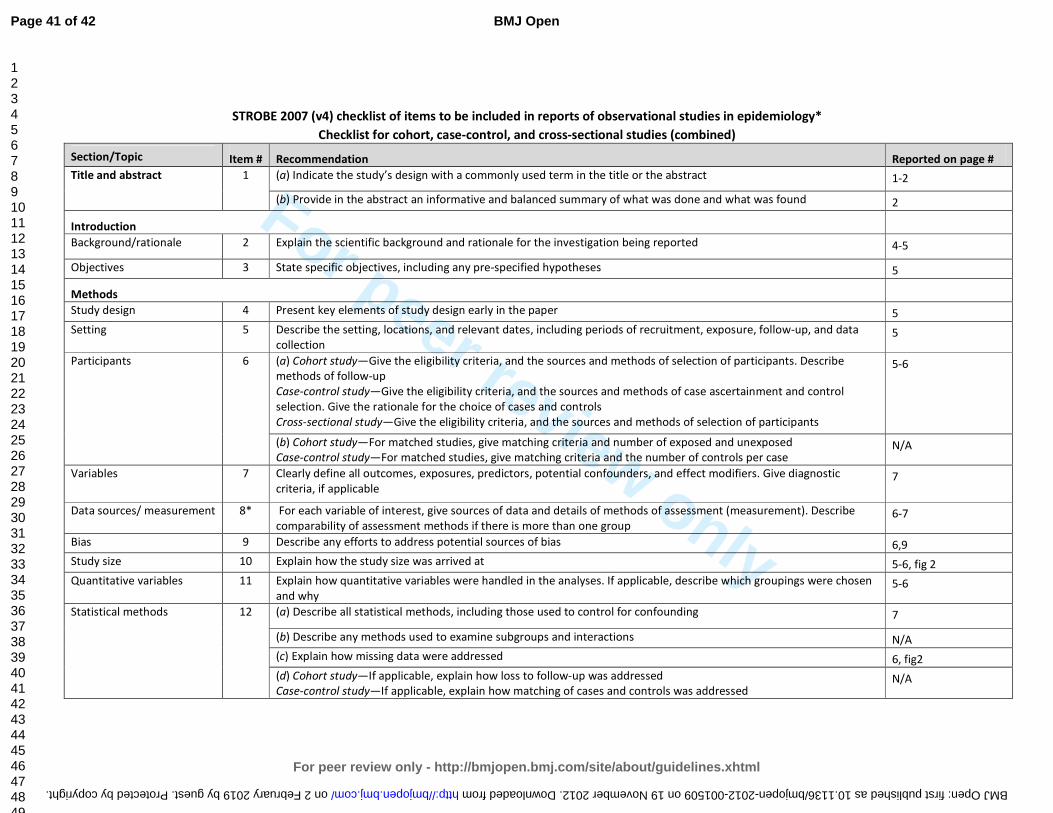
For peer review only
STROBE 2007 (v4) checklist of items to be included in reports of observational studies in epidemiology*
Checklist for cohort, case-control, and cross-sectional studies (combined)
Section/Topic Item # Recommendation Reported on page #
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 1-2
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 2
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4-5
Objectives 3 State specific objectives, including any pre-specified hypotheses 5
Methods
Study design 4 Present key elements of study design early in the paper 5
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection 5
Participants 6 (a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe
methods of follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control
selection. Give the rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
5-6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case N/A
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic
criteria, if applicable 7
Data sources/ measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group 6-7
Bias 9 Describe any efforts to address potential sources of bias 6,9
Study size 10 Explain how the study size was arrived at 5-6, fig 2
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen
and why 5-6
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding 7
(b) Describe any methods used to examine subgroups and interactions N/A
(c) Explain how missing data were addressed 6, fig2
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed N/A
Page 41 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from
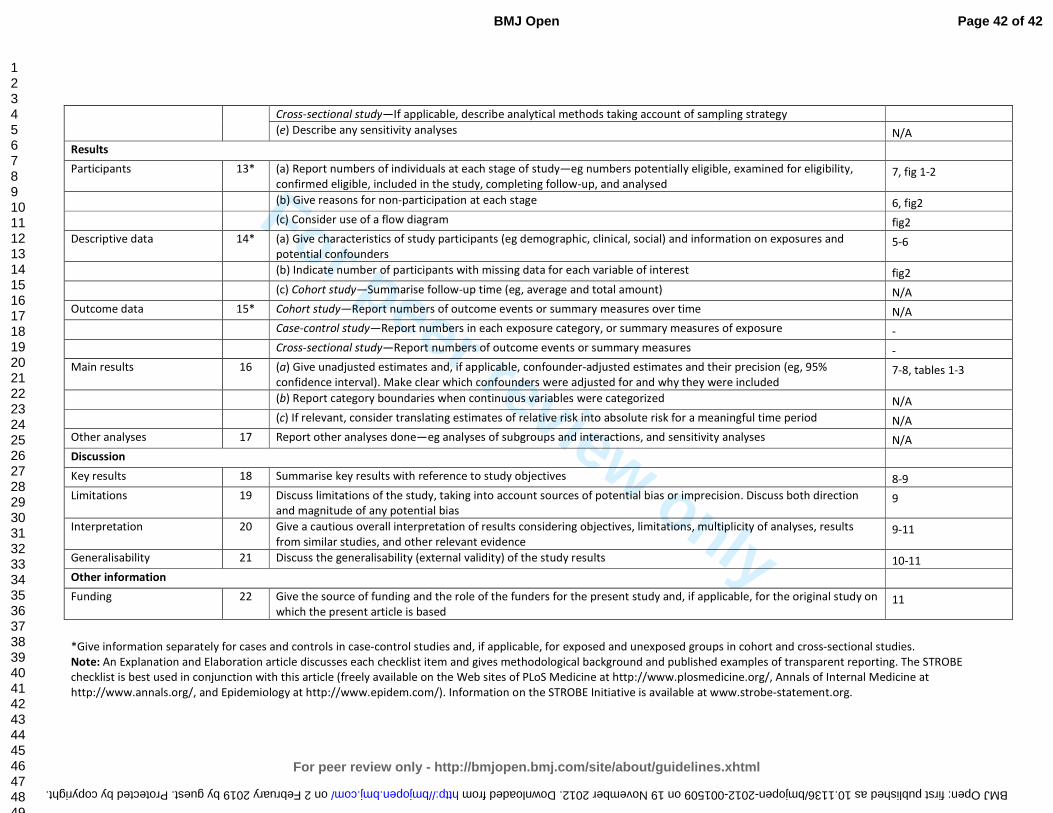
For peer review only
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
(e) Describe any sensitivity analyses N/A
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed 7, fig 1-2
(b) Give reasons for non-participation at each stage 6, fig2
(c) Consider use of a flow diagram fig2
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and
potential confounders 5-6
(b) Indicate number of participants with missing data for each variable of interest fig2
(c) Cohort study—Summarise follow-up time (eg, average and total amount) N/A
Outcome data 15* Cohort study—Report numbers of outcome events or summary measures over time N/A
Case-control study—Report numbers in each exposure category, or summary measures of exposure -
Cross-sectional study—Report numbers of outcome events or summary measures -
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95%
confidence interval). Make clear which confounders were adjusted for and why they were included 7-8, tables 1-3
(b) Report category boundaries when continuous variables were categorized N/A
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period N/A
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses N/A
Discussion
Key results 18 Summarise key results with reference to study objectives 8-9
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction
and magnitude of any potential bias 9
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results
from similar studies, and other relevant evidence 9-11
Generalisability 21 Discuss the generalisability (external validity) of the study results 10-11
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based 11
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE
checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at
http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 42 of 42
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 2 February 2019 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2012-001509 on 19 November 2012. Downloaded from












