Embed Size (px)
Citation preview

BNP: What’s in it for you or BNP: What’s in it for you or is it “another D-dimer”?is it “another D-dimer”?
October 7, 2004October 7, 2004Chris HallChris Hall
- with the help of Debra Isaac, Bryan Young, a - with the help of Debra Isaac, Bryan Young, a bunch of cardiology fellows and Adam Osterbunch of cardiology fellows and Adam Oster

CHF: the condition of interest, how CHF: the condition of interest, how common is it?common is it?
USA prevalence 4.6 x 10USA prevalence 4.6 x 1066 cases casesUSA incidence: 550,000 new cases/yearUSA incidence: 550,000 new cases/yearThat translates into Canadian numbers of:That translates into Canadian numbers of: 55,000 new cases/year55,000 new cases/year 5500 cases/year/province roughly5500 cases/year/province roughly 2000 cases per year in Calgary…or about 7 per day2000 cases per year in Calgary…or about 7 per day
Cost:Cost: $56 billion/year in USA$56 billion/year in USA $39 billion of that re: hospitalization$39 billion of that re: hospitalization

Admission ratesAdmission rates
75-90% of patients with suspected CHF are 75-90% of patients with suspected CHF are admittedadmitted Graff et al PROVIDE study, Ann Emerg Med 1999Graff et al PROVIDE study, Ann Emerg Med 1999
77% of admissions originate in the ED77% of admissions originate in the ED
Absent clinical criteriaAbsent clinical criteria
Absent lab criteriaAbsent lab criteria
BUT…if you are a good clinician, you know who BUT…if you are a good clinician, you know who is in CHF and who isn’t…don’t you?is in CHF and who isn’t…don’t you?

The problem with signs and symptomsThe problem with signs and symptoms
Poor relationship between symptoms and severity Poor relationship between symptoms and severity (more about that later)(more about that later)BNP levels correlate with both severity and outcomeBNP levels correlate with both severity and outcome Harrison et al Harrison et al Ann Emerg Med 2002Ann Emerg Med 2002: : BNP predicts future BNP predicts future
events in ED ptsevents in ED pts Cheng et al Cheng et al JACC 2001JACC 2001: : BNP predicts outcome in admitted BNP predicts outcome in admitted
patientspatients Bettencourt et al Bettencourt et al Am J Med 2002Am J Med 2002: : BNP predicts outcome BNP predicts outcome
after dischargeafter discharge Maeda et al Maeda et al JACC 1999JACC 1999: : Increased BNP is an independent Increased BNP is an independent
predictor of mortality.predictor of mortality.

So….So….
BNP should assist with appropriate treatment BNP should assist with appropriate treatment and disposition of CHF patients in the EDand disposition of CHF patients in the ED
What the heck is BNP again?????What the heck is BNP again?????

Natriuretic Peptides: Origin and Natriuretic Peptides: Origin and Stimulus of ReleaseStimulus of Release
Adapted from Burnett JC, J Hypertens 2000;17(Suppl 1):S37-S43
ANP = Atrial Natriuretic PeptideBNP = B-type Natriuretic PeptideCNP = C-type Natriuretic Peptide
Peptide Primary Origin Stimulus of Release
ANP Cardiac atria Atrial distension
BNP Ventricular myocardium Ventricular overloadCNP Endothelium Endothelial stress

Relationship between BNP Relationship between BNP Concentration and Pulmonary Artery Concentration and Pulmonary Artery
Wedge PressureWedge Pressure
R= 0.729P< .05
PAW
0
2
4
6
0 1 2 3 4 5 6 7
BN
P
Maisel, A., Kazenegra, R. et al. J Cardiac Failure, Vol. 7, No. 1, 2001
Change per hour
PAW (mm Hg)
BNP (pg/ml)
0.00.20.40.60.81.0
010203040
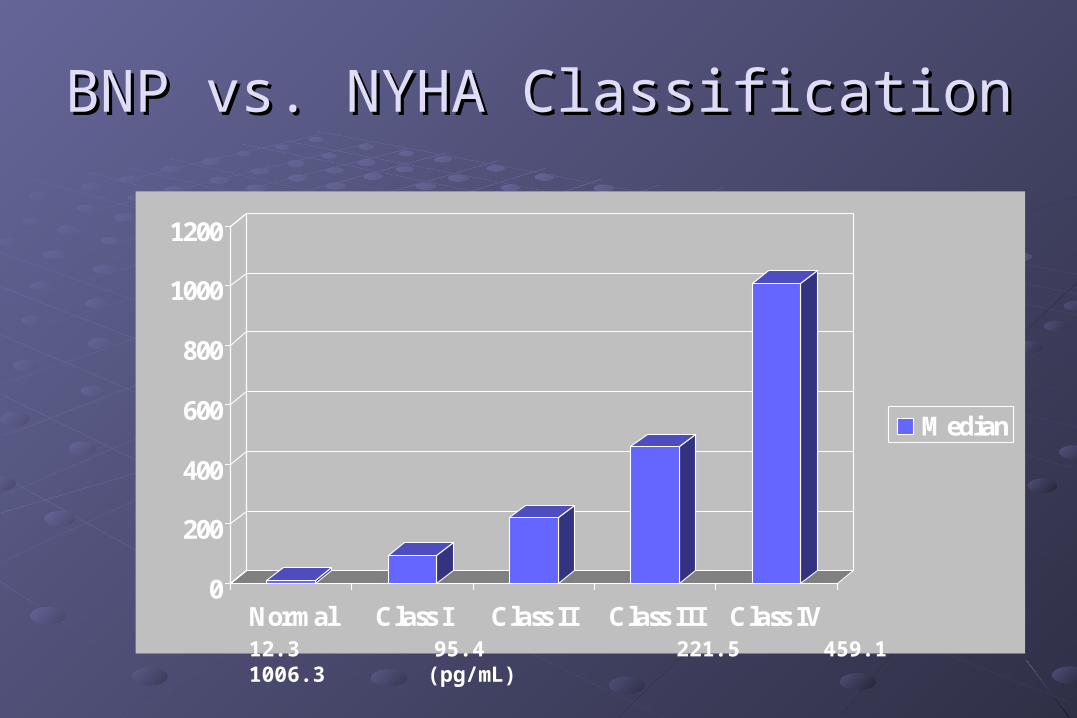
BNP vs. NYHA ClassificationBNP vs. NYHA Classification
0
200
400
600
800
1000
1200
Normal Class I Class II Class III Class IV
Median
12.3 95.4 221.5 459.1 1006.3 (pg/mL)

Cumulative Survival Rates in CHF Patients With Left Ventricular Dysfunction Stratified on Median Plasma BNP Concentration
Tsutamoto T. et al. Circulation 1997;96:509-516
0
20
40
60
80
100
0 10 20 30 40 50
BNP < 73 pg/ml
BNP > 73 pg/ml
Months
Cu
mu
lativ
e S
urvi
val (
%)
p < 0.0001

But is it specific?But is it specific?

Is it specific? BNP Levels in Patients Is it specific? BNP Levels in Patients With Dyspnea Secondary to CHF or With Dyspnea Secondary to CHF or
COPDCOPD
86 +/- 39
1076 +/- 138
0
200
400
600
800
1000
1200
BN
P p
g/m
L
COPD CHF
Cause of DyspneaN=56 N=94
Dao, Q., Maisel, A. et al. J. American College of Cardiology, Vol 37, No. 2, 2001
So, what’s the ED literature say?So, what’s the ED literature say?
The REDHOT trial:The REDHOT trial:
Ann Emerg Med October 2004Ann Emerg Med October 2004

1. To establish whether BNP levels are 1. To establish whether BNP levels are associated with outcomes independent of ED associated with outcomes independent of ED physician assessment (Is there a “disconnect” physician assessment (Is there a “disconnect” between perceived severity of illness and BNP between perceived severity of illness and BNP levels?)levels?) 2. 2. To identify BNP levels that might help decide To identify BNP levels that might help decide admission or dischargeadmission or discharge

R.E.D.H.O.T. Study DesignR.E.D.H.O.T. Study Design
10 USA Hospitals10 USA HospitalsBNP Levels Taken SeriallyBNP Levels Taken SeriallyPhysicians blinded to BNP Concentrations unless Physicians blinded to BNP Concentrations unless <100<100Key Outcomes Determined at Both 30 & 90 DaysKey Outcomes Determined at Both 30 & 90 Days MortalityMortality Hospital ReadmissionHospital Readmission

Inclusion Criteria:Inclusion Criteria: 18 Years of Age or Older18 Years of Age or Older CHF Diagnosed by CHF Diagnosed by
Either Cardiologist or Either Cardiologist or E.D. PhysicianE.D. Physician
Patient Requires Patient Requires Treatment for CHFTreatment for CHF
Exclusion CriteriaExclusion Criteria BNP Levels Equal to or BNP Levels Equal to or
Less Than 100 pg/mlLess Than 100 pg/ml Patients with Current Patients with Current
M.I. Or ACS with ST M.I. Or ACS with ST Elevation of 1mm or Elevation of 1mm or greatergreater
Patients with Renal Patients with Renal Failure Requiring Failure Requiring HemodialysisHemodialysis
R.E.D.H.O.T. Study Design R.E.D.H.O.T. Study Design (Continued)(Continued)

Patient Characteristics
AgeMaleFemaleCaucasianAfrican American
Hx CHFHx COPD
63.4%53.9%46.1%32.5%
63.4%
76.5%21.7%
N=464
PNDJVPRalesS3PeripheralEdema
59.0%42.6%74.8%19.6%
75.0%

AdmitAdmit DischargeDischarge
InitialInitial
IntentIntent68.3%68.3% 31.7%31.7%
AdmitAdmit DischargeDischarge
FinalFinal
DispositionDisposition90.3%90.3% 9.7%9.7%
Decision for admissionDecision for admission

And of the patients who got And of the patients who got discharged…discharged…
If 90% were admitted, everyone sick must have If 90% were admitted, everyone sick must have been admitted…been admitted…
Not so fastNot so fast

Perceived NYHA Class in patientsUltimately discharged home from the ED
Discharge Discharge HomeHome
II IIII IIIIII IVIV TotalTotal
BNP<400BNP<400
pg/mlpg/ml 22 66 22 -- 1010
BNPBNP400400
pg/mlpg/ml 11 1212 2121 11 3535
78% of discharged patients have BNP 400 pg/ml

20%
63%
0%10%20%30%40%50%60%70%
D<400pg/ ml D≥400pg/ ml
NYH
A I
II,
IV
%
0%0%0%
20%
40%
60%
80%
100%
D<400pg/ ml D≥400pg/ ml
NYH
A I
II,
IV %
30 day follow-up
9.0%
0%0%
2%
4%
6%
8%
10%
D<400pg/ ml D≥400pg/ ml
NYH
A I
II,
IV %
90 day follow-up
Discharged patients: NYHA class andSubsequent mortality

So, does that mean everyone needs So, does that mean everyone needs admission?admission?

Perceived NYHA Class in patientsUltimately admitted from the ED
II IIII IIIIII IVIV TotalTotal
BNP<200BNP<200
pg/mlpg/ml 11 1414 1818 1111 4444
BNPBNP200200
pg/mlpg/ml 1010 103103 168168 9393 374374
11% of all patients admitted with BNP<200 pg/ml
66% of patients admitted with BNP<200pg/mlperceived NYHA III,IV

66%
70%
64%
66%
68%
70%
72%
A<200pg/ ml A≥200pg/ ml
NY
HA
III, IV
%
4%
0%0%
2%
4%
6%
A<200pg/ ml A≥200pg/ ml
NYH
A I
II, IV
%
2.0%
9.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
A<200pg/ ml A≥200pg/ ml
NYH
A I
II, IV
%
30 day follow-up
90 day follow-up
Admitted patients: NYHA class andSubsequent mortality

REDHOT BNP Values REDHOT BNP Values & Patient Disposition& Patient Disposition
976
767
0100200300400500600700800900
1000
Discharged Admitted
Previous Data Link High BNP to Previous Data Link High BNP to Morbidity & Mortality Morbidity & Mortality
Actual BNP Values Blinded to Actual BNP Values Blinded to E.D. PhysicianE.D. Physician
BNP Median Values ~22% BNP Median Values ~22% Higher in Patients Discharged Higher in Patients Discharged Home from E.D.Home from E.D.
CONCLUSIONS:CONCLUSIONS:
In patients presenting with shortness of breath to In patients presenting with shortness of breath to the ED, there is a large “disconnect” between the ED, there is a large “disconnect” between perceived severity of CHF and the BNP level.perceived severity of CHF and the BNP level.
Even in the setting where CHF severity is perceived Even in the setting where CHF severity is perceived as severe, a low BNP level portends a favorable as severe, a low BNP level portends a favorable short and long term prognosisshort and long term prognosis

The Calgary ImplementationThe Calgary Implementation
Organized plan of implementation to reduce the Organized plan of implementation to reduce the D dimer, troponin, “all things ordered at D dimer, troponin, “all things ordered at presentation” effectpresentation” effect
Protocol driven approachProtocol driven approach
Also contribute to the literature in organized Also contribute to the literature in organized study formatstudy format
Protocol implementation arranged by billing Protocol implementation arranged by billing group to simplify education of MD’sgroup to simplify education of MD’s

Protocol #1: RGH; multicenter trial Protocol #1: RGH; multicenter trial sponsored by Rochesponsored by Roche
Patients suspected to have CHFPatients suspected to have CHF
Consented for trial (blood draw and chart review)Consented for trial (blood draw and chart review)
BNP drawn in EDBNP drawn in ED
Randomized to know results or notRandomized to know results or not
Compare admission rates, test utilization and outcome Compare admission rates, test utilization and outcome in the two groupsin the two groups
Determine the effect of BNP measurement on local Determine the effect of BNP measurement on local resource utilization and patient outcomeresource utilization and patient outcome
Are USA studies generalizable?Are USA studies generalizable?
Protocol #2: FMC and PLCProtocol #2: FMC and PLC
Patients with SOB suspected to be CHFPatients with SOB suspected to be CHFConsented for involvement in study by EDConsented for involvement in study by EDInvolvement consists of BNP drawn and some patients Involvement consists of BNP drawn and some patients with phone follow-upwith phone follow-upBNP drawn in EDBNP drawn in EDBNP values not known to MDsBNP values not known to MDsUsual treatment and disposition of all patientsUsual treatment and disposition of all patientsPhone follow-up only for 300 patients with BNP<100Phone follow-up only for 300 patients with BNP<100Determine M&M in 30 and 90 days to determine Determine M&M in 30 and 90 days to determine “safety” of the 100 cutoff locally“safety” of the 100 cutoff locally

Research-speakResearch-speak
EP considers diagnosis of CHF who demonstrate a BNP level of EP considers diagnosis of CHF who demonstrate a BNP level of <100 pg/ml. <100 pg/ml. followed for the rates of pre-specified CHF events and CHF followed for the rates of pre-specified CHF events and CHF investigative procedures over the 30-day period following their investigative procedures over the 30-day period following their ED visit. ED visit. Endpoints: Endpoints:
Cardiac endpoints (or Cardiac endpoints (or SafetySafety endpoints) endpoints) investigational or diagnostic procedures endpoints (investigational or diagnostic procedures endpoints (Resource)Resource)
A 30-day follow-up period re: related to index ED visit. A 30-day follow-up period re: related to index ED visit. The incidence of The incidence of ResourceResource endpoints will form the basis for endpoints will form the basis for further study into optimal resource utilization for patients who are further study into optimal resource utilization for patients who are at low risk of adverse CHF events. at low risk of adverse CHF events.

Questions?Questions?

““BNP Guided” E.D. Discharge @ 200pg/ml: BNP Guided” E.D. Discharge @ 200pg/ml: Annual Economic Impact Potential:Annual Economic Impact Potential:
DRG 127 DRG 127 680,106 Admissions in ‘01680,106 Admissions in ‘01 5.27 Day L.O.S.5.27 Day L.O.S. $5,414.68 Cost per Patient$5,414.68 Cost per Patient Medicare = 80% Total CostsMedicare = 80% Total Costs
$4,600
$4,094
Standard Care Rapid BNP
$4,600,000,000.00 Total$4,600,000,000.00 Total
U.S. Inpatient CostU.S. Inpatient Cost
11% Reduction$506mm Reduction

BNP Levels in Patients With Dyspnea BNP Levels in Patients With Dyspnea Secondary to CHF or COPDSecondary to CHF or COPD
86 +/- 39
1076 +/- 138
0
200
400
600
800
1000
1200
BN
P p
g/m
L
COPD CHF
Cause of DyspneaN=56 N=94
Dao, Q., Maisel, A. et al. J. American College of Cardiology, Vol 37, No. 2, 2001

BNP Levels in Patients With Edema BNP Levels in Patients With Edema Diagnosed With CHF or Without CHFDiagnosed With CHF or Without CHF
63 +/- 16
1038 +/- 163
0
200
400
600
800
1000
1200
BN
P p
g/m
L
No CHF CHF
Cause of EdemaN=44 N=44
Dao, Q., Maisel, A. et al. J. American College of Cardiology, Vol 37, No. 2, 2001

ConclusionsConclusions
BNP levels accurately reflect the cause of BNP levels accurately reflect the cause of dyspnea and/or edemadyspnea and/or edema
BNP levels add additional information to that BNP levels add additional information to that gathered by the physician, allowing the correct gathered by the physician, allowing the correct diagnosis of congestive heart failure diagnosis of congestive heart failure

clinical and economic value of BNP clinical and economic value of BNP measurement measurement
ERER
time and volume issues at play! time and volume issues at play! higher percentage of diagnostic dilemmashigher percentage of diagnostic dilemmas limited access to immediate specialist input limited access to immediate specialist input probably highest potential for economic / resource use probably highest potential for economic / resource use benefit benefit - reduce cost of “fishing expeditions”reduce cost of “fishing expeditions”
- reduce waiting time for unnecessary consultsreduce waiting time for unnecessary consults- speed up diagnosis; reduced time in ER until speed up diagnosis; reduced time in ER until disposition determineddisposition determined- speed up initiation of appropriate rxspeed up initiation of appropriate rx





























