-
7/30/2019 Boa Lower Limb 2009
1/24
OPEN FRACTURESOF THE LOWER LIMB
Standards or the management o
BritishOrthopaedicAssociation
A SHORT GUIDE
-
7/30/2019 Boa Lower Limb 2009
2/24
who should
read this guide?
Standards for the management of open fractures of the lower limb
details the optimaltreatment or patients with these challenging
injuries. Drawing on an extensivereview o the published evidence
and their personal experience, the authors set outeach stage o the
management pathway, including what to do i complications arise.
O relevance to pre-hospital, emergency room and hospital
clinicians, each chaptercontains key recommendations or the
standards o care that should be deliveredand practical advice.
Containing important new guidance or getting the best outcomes,
the Standardsare an essential reerence text or orthopaedic, plastic
surgery, emergencymedicine, and rehabilitation specialists who
treat these injuries as well or thosewho plan and commission trauma
care.
Endorsed by the Councils o the British Association o Plastic,
Reconstructive andAesthetic Surgeons and the British Orthopaedic
Association, the Standards for themanagement of open fractures of
the lower limb replace previous guidelines in theUK and will have
worldwide relevance.
This short guide contains only the key recommendations rom the
Standards.Readers wishing to review the evidence-base behind them
should reer to theull Standards publication. Details o how to
obtain a copy may be ound on ourwebsites:www.bapras.org.uk and
www.boa.ac.uk
-
7/30/2019 Boa Lower Limb 2009
3/24
01
contents
1. Foreword
2. Introduction
3. The working group
4. Principal recommendations
Specialistcentres
Emergencymanagement
Antibioticprophylaxis
Timingofwounddebridement
Softtissuedebridement
Bonedebridement
Deglovinginjuries
Classication Temporarywounddressings
Techniquesofskeletalstabilisation
Timingofsofttissuereconstruction
Typeofsofttissuereconstruction
Compartmentsyndrome
Vascularinjuries
Footandankle
Whenthingsgowrongwithsofttissues Whenthingsgowrongwithbone
Guidelinesforamputation
Outcomemeasures
Managementofsevereopenfracturesinchildren
Acknowledgements
02
05
06
07
Back cover
-
7/30/2019 Boa Lower Limb 2009
4/24
02
1
foreword
Lord Darzi
The British Association o Plastic,Reconstructive and Aesthetic
Surgeons(BAPRAS) and the British OrthopaedicAssociation (BOA) have
been workingto promote the joint care o patientswith severe open
ractures o thelower limb by plastic and orthopaedic
surgeons to minimise complicationsand optimise outcomes.
These Standards for the managementof open fractures of the lower
limb gobeyond this to provide an evidence-basedapproach to improve
the managementoftheseuncommon,difcultinjuries.The authors have
built on the previousguidelinestodenethestandardsof
treatment and provide clear guidance ohow these patients should
be managed.They have addressed all aspects o thecare o the patient,
rom initial assessmentthrough to reconstruction and
theindicationsforamputation.Wherethereare no clear data, a balanced
view o theavailable evidence is presented, withrecommendations
based on principlesand experience. Importantly, they have
also detailed how outcomes can beassessed. I am delighted to
note that theintention is or the specialist centres toaudit their
outcomes using the evidence-based standards. Oten neglected are
ways to deal with problems when thingsgo wrong, and again the
authors haveaddressed this important area.
The recommendation or the patientsto be transerred directly to
specialistcentres refects my proposals in the NHS
Next Stage Review or the treatment omajor trauma in specialist
centres.
This publication is aimed at improving
thequalityoftreatmentthrougheducation.BAPRAS and BOA are to be
commendedor making the entire publication availableonline via their
websites and ree to
downloadinPDFformat,aswellasproducingthisabridged version o the
principal guidelines.
The BOAST poster should enable theStandards to be widely
publicised.
Our NHS has been at the oreront onumerous innovations and it is
hearteningto see that the authors have drawn on awealth o
international knowledge to setthe highest standards or patient
care.
Proessor, the Lord Darzi o Denham KBE,
HonFREng, FmedSci
-
7/30/2019 Boa Lower Limb 2009
5/24
03
1
foreword
Simon Kay
Plastic surgery is by its nature oneo the most collaborative
specialties,orming part o many dierent careteams. No cooperation
has been sostrong or productive as that alliancewith orthopaedic
and trauma surgery,and this was underlined in the revolution
in the care o the mangled limb, andespecially the open tibial
racture.
Whenin1986MarcoGodinademonstratedhow to manage these injuries
with the ullbenetoftheemergingeldofmicrovasculartransplantation, he
presaged a new era insalvaging limbs. This would not have
beenpossible without the advances in
racturexation,northeskillsandknowledgein
sot tissue debridement and repair. Butit has been the synergy
between thesedisciplines and the remarkable cooperationbetween
teams all over the world that haswrought this change most
emphatically.
TherstUKguidanceonthejointmanagement o lower limb trauma camerom
the BOA and the (then) BAPS in1993andthispresentguidancefollows
in the same tradition. However now, ina contemporary manner, the
guidanceismorespecic,morecomprehensive, and evidence-based. These
standards
will prove invaluable to teams aroundthe world and the joint
working partyis owed a debt o gratitude rom allmanaging trauma and
rom all thosepatientswhowillsurelybenetinyearsto come.
Proessor Simon KayPresident, BAPRAS
-
7/30/2019 Boa Lower Limb 2009
6/24
04
1
foreword
Clare Marx
I am delighted to see the publicationo Standards for the
managementof open fractures of the lower limb.This is an excellent
example ohow the two Specialist Associations,BAPRAS and BOA, can
work togetherto set standards and give practical
guidance to surgeons dealing withthese complex injuries.
I would encourage all orthopaedicsurgeons involved in trauma
care toensure that the BOAST and the jointbooklet are seen by as
wide an audienceas possible to ensure that standards ocare are
improved and assured or theuture. The BOA also recommends those
wishing to have more detailed inormationto purchase the
excellent book to bepublishedbytheJointWorkingParty.
Clare MarxPresident, BOA
-
7/30/2019 Boa Lower Limb 2009
7/24
05
The frst meeting between the British Orthopaedic Association
(BOA) and the BritishAssociation o Plastic, Reconstructive and
Aesthetic Surgeons (BAPRAS) was convenedin 1991 to oster closer
working between the specialties or the management o patientswith
open tibial ractures.
Therewasaclearconsensusthattheyshouldbemanagedjointlyandin1993andagainin1997,representativesfrombothassociationspublishedguidelinesforthemanagementofopentibial
ractures. The main aims were to promote cooperation between
orthopaedic and plasticsurgeons, improve the understanding o these
uncommon but complex injuries and encourage
their treatment in specialist centres. However, the publication
went beyond these, providingan algorithmic approach to the
management o the injuries and guidance on how to do
it.Atasubsequentmeetingofthetwoassociationsin2003,itwasclearthereweredifcultiesin
ollowing the guidelines owing to geographical constraints, lack o
resources and remainingareas o clinical controversy.
In2007,theBOAandtheBAPRASnominatedrepresentativestoupdatetheguidelines.Anincreasing
awareness o the complexity o these injuries and an appreciation o
limitationsofpreviousclassicationstopredictoutcomepromptedtheworkinggrouptoexaminethepublished
literature in all areas pertaining to the management o open
ractures o the lower
limb with a particular ocus on injuries below the knee. As in
other areas o surgery, there wereew randomised trials and an
approach based purely on levels o evidence would not havebeen
possible. However, we have been able to draw on a wealth o
excellent publications
andendeavouredtoputtheavailableevidenceincontext.Wherethereisnoclearconsensus,wehave
drawn on data rom associated areas and on our experience. I no
clear choice betweenavailable alternatives or management was
present, we have tried to provide a balanced viewthrough
highlighting the relative merits and drawbacks o each. The
evidence-base upon
whichwehavedrawnispublicationsinEnglish.WearedelightedthattheBritishInfectionSocietyandtheAssociationofMedicalMicrobiologistshavereviewedtheguidelinesforantibioticprophylaxis.The
ormat is designed to give the reader easy access to the principal
recommendations. Details
on how they were derived and a bibliography o the relevant
literature can be ound in the ullStandards publication.
Finally,thispublicationreectsthecurrentevidence-baseforourrecommendationsandwe
are unanimous in the view that these are the standards o care every
patient with
theseinjuriesshouldreceive.TheserecommendationsshouldndapplicationbeyondtheUK.
05
2
introduction
-
7/30/2019 Boa Lower Limb 2009
8/24
06
BAPRAS and BOA established a working group with experienced
clinicians to defne thestandards or the management o open ractures
o the lower limb. The authors are allpracticing specialists in the
UK with a particular interest in the evidence-based managemento
open ractures o the lower limb, rom an orthopaedic, plastic surgery
and inectioncontrol viewpoint.
Authors:
Jagdeep Nanchahal
Proessor o Hand, Plastic & Reconstructive Surgery,
London
Selvadurai NayagamConsultant Orthopaedic Surgeon, LiverpoolUmraz
KhanConsultant Plastic Surgeon, Bristol
Christopher MoranProessor o Trauma & Orthopaedic Surgery,
Nottingham
Stephen BarrettConsultantinMedicalMicrobiology,Southend
Frances SandersonConsultant in Inectious Diseases, London
Ian PallisterReader in Trauma & Orthopaedic surgery,
Swansea
Managing editor:
Hamish LaingConsultant Plastic Surgeon, Swansea
3
the working group
-
7/30/2019 Boa Lower Limb 2009
9/24
07
The recommendations that ollow are a summary o the main
standards publication Standardsfor the management of open fractures
of the lower limb. Each section heading below correspondsto a
chapter within the ull standards publication.
1. Specialist centres
Principal recommendations
Amultidisciplinaryteam,includingorthopaedicandplasticsurgeonswithappropriateexperience,isrequiredforthetreatmentofcomplexopenfractures.
Hospitalswhichlackateamwithrequisiteexpertisetotreatcomplexopenfractureshavearrangements
or immediate reerral to the nearest specialist centre.
Theprimarysurgicaltreatment(wounddebridement/excisionandskeletalstabilisation)o
these complex injuries takes place at the specialist centre
whenever possible.
Specialistcentresforthemanagementofsevereopenfracturesareorganisedon
a regional basis as part o a regional trauma system. Usually these
centres also providethe regional service or major trauma.
The characteristics o open injuries that should prompt reerral
to a specialist centre are
based on:
1. Fracture patterns:
(a)Transverseorshortobliquetibialfractureswithbularfracturesatasimilarlevel
(b)Tibialfractureswithcomminution/butteryfragmentswithbularfracturesatasimilarlevel
(c) Segmental tibial ractures
(d)Fractureswithboneloss,eitherfromextrusionatthetimeofinjuryorafterdebridement.
2. Sot tissue injury patterns:
(a) Skin loss such that direct tension-ree closure is not
possible ollowing wound excision
(b) Degloving
(c)Injurytothemuscleswhichrequiresexcisionofdevitalisedmuscleviawoundextensions
(d) Injury to one or more o the major arteries o the leg.
The specialist centre will need to:
Includeorthopaedictraumasurgery,withspecialexpertiseincomplextibialfracturesand
bone reconstruction.
Includeplasticandmicrovascularsurgery,withexpertiseinvascularreconstruction.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
10/24
08
Providefacilitiesforsimultaneousdebridementbyorthopaedicandplasticsurgicalteams.
Ensureorthopaedicandplasticsurgicalplanningofmanagementstrategytoavoidmultipleepisodesoftreatment,therebyensuringefcientandoptimalpatientcare.
Providededicatedtheatresessionsforthecombinedorthoplasticmanagementofthepatientsduring
the normal working day.
Includemicrobiologyandinfectiousdiseaseconsultantswithexpertiseinmusculoskeletalinection.
Includefacilitiesforemergencymusculoskeletalimaging,withangiographyandinterventional
radiology.
Provideaservicefor,orhaveaccessto,articiallimbttingandrehabilitationor
amputees.
Haveaccesstophysicalandpsychosocialrehabilitationservices.
Includeauditofoutcomeaspartofthecarepathway.
Aimtoreachathroughputof30suchcasesperannumtomaintainappropriateskillandexperience
levels.
Providecombinedorthoplasticclinicsandmultidisciplinarywardrounds.
Possessintensivecareandothertraumafacilitiesforthemultiplyinjuredpatient.
2. Primary management in the emergency department
Principal recommendations
Initialassessmentandtreatmentofthepatientoccurssimultaneouslyandinaccordance
with Advanced Trauma Lie Support (ATLS) principles.
Assessmentoftheopentibialinjuryissystematic,carefulandrepeatedinordertoidentifyestablished
or evolving limb-threatening conditions and to document limb status
prior tomanipulation or surgery.
Haemorrhagecontrolisthroughdirectpressureor,asalastresort,applicationofatourniquet.
Woundsarehandledonlyto
a. Remove gross contaminants
b. Photograph or record
c. Seal rom the environment.
Woundsarenotprovisionallycleanedeitherby:
a. exploration
b. irrigation.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
11/24
09
LimbsplintageisthemostappropriatemeansofimmobilisationavailableintheEmergencyDepartment.Provisionalexternalxatorsarenotapplied.
Antibioticandanti-tetanusprophylaxisisgiven.
Inadditiontotwoorthogonalviewsofthetibia,radiographicassessmentincludesthekneeand
ankle joints.
3. Antibiotic prophylaxis
Principal recommendations
Antibioticsshouldbeadministeredassoonaspossibleaftertheinjury,andcertainlywithin
three hours.
Theantibioticofchoiceisco-amoxiclav(1.2g8hourly),oracephalosporin(egcefuroxime1.5g8hourly),andthisshouldbecontinueduntilrstdebridement(excision).
Atthetimeofrstdebridement,co-amoxiclav(1.2g)oracephalosporin(suchascefuroxime1.5g)andgentamicin(1.5mg/kg)shouldbeadministeredandco-amoxiclav/cephalosporincontinueduntilsofttissueclosureorforamaximumof72hours,whicheverissooner.
Gentamicin1.5mg/kgandeithervancomycin1gorteicoplanin800mgshouldbeadministered
oninductionofanaesthesiaatthetimeofskeletalstabilisationanddenitivesofttissueclosure.
These should not be continued post-operatively. The vancomycin
inusion shouldbestartedatleast90minutespriortosurgery.
Patientswithanaphylaxistopenicillinshouldreceiveclindamycin(600mgivpre-op/qds)inplaceofco-amoxiclav/cephalosporin.Forthosewithlesserallergicreactionsacephalosporinis
considered to be sae and is the agent o choice.
4. Timing o wound excision in open ractures
Principal recommendations
Broadspectrumantibioticsareadministeredassoonaftertheinjuryaspossible.
Theonlyreasonsforimmediatesurgicalexplorationarethepresenceof:
a.Grosscontaminationofthewound
b. Compartment syndrome
c. A devascularised limb
d. A multiply injured patient.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
12/24
10
Intheabsenceofthesecriteria,thewound,softtissueandboneexcision(debridement)is
perormed by senior plastic and orthopaedic surgeons working
together on
scheduledtraumaoperatinglistswithinnormalworkinghoursandwithin24hoursoftheinjuryunlessthereismarine,agriculturalorsewagecontamination.The6hourruledoesnotapplyforsolitary
open ractures.
5. Guidelines or wound debridement (excision)
Principal recommendations
Early,accuratedebridementofthetraumaticwoundisthemostimportantsurgicalprocedurein
the management o open tibial ractures.
Debridementmeansexcisionofalldevitalisedtissue(exceptneurovascularbundles).
Traumaticwoundsareexcisedcomprehensivelyandsystematicallyandthefollowingsequenceisfollowedinallcases:
Initially,thelimbiswashedwithasoapysolutionandatourniquetisapplied
The limb is then prepped with an alcoholic chlorhexidine
solution, avoiding contact o
theantisepticwiththeopenwoundandpoolingunderthetourniquet
Softtissuedebridement/excisionissafelyperformedundertourniquetcontrol,especiallyincasesofextensivedegloving.Thisallowsidenticationofkeystructuressuchasneurovascular
bundles, which may be displaced, and permits accurate examinationo
tissues by avoiding blood-staining
Visualisationofthedeeperstructuresisfacilitatedbywoundextensionsalongthefasciotomylines,describedinsection13,page17
Thetissuesareassessedsystematicallyinturn,fromsupercialtodeep(skin,fat,muscle,bone)
and rom the periphery to the centre o the wound. Non-viable skin,
at, muscle andbone is excised
Atthisstagetheinjurycanbeclassiedanddenitivereconstructionplannedjointlybythesenior
members o the orthopaedic and plastic surgical team
Ifdenitiveskeletalandsofttissuereconstructionisnottobeundertakeninasinglestage,thenavacuumfoamdressing(orantibioticbeadpouchifsignicantsegmentalbonehasbeenlost)isapplieduntildenitivesurgeryisperformed.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
13/24
11
6. Bone exposure, decontamination and preservation:
debridement
Principal recommendations
Extensionofthetraumaticwoundisalongthenearestfasciotomyincision(seesection13,page17).
Whilstabloodlesseldduringsofttissuedebridementmaybehelpful,deatingthetourniquetbeforebonedebridementallowssatisfactoryconrmationofacapacityoftheboneendstobleed.
This is probably the most useul determinant o bone viability.
Carefulsurgicaldeliveryofboneendsthroughthewoundextensionaidscircumferentialassessment.
Particulateforeignmatterisremovedwithperiodicirrigationtokeepclearvisibilityofthesurgicaleld.
Loosefragmentsofbonewhichfailthetugtestareremoved.
Fractureendsandlargerfragmentswhichfailtodemonstratesignsofviabilityareremoved.
Majorarticularfragmentsarepreservedaslongastheycanbereducedandxedwithabsolute
stability.
Lavagefollows,onceacleanwoundisobtainedbyameticulouszone-by-zonedebridement.
Highpressurepulsatilelavageisnotrecommended.
7. Degloving
Principal recommendations
Deglovingofthelimboccursintheplanesupercialtothedeepfasciaandtheextentofinjuryis
oten underestimated.
Thrombosisofthesubcutaneousveinsusuallyindicatestheneedtoexcisetheoverlyingskin.
Circumferentialdeglovingoftenindicatesthattheinvolvedskinisnotviable.
Insevereinjuries,multi-planardeglovingcanoccurwithvariableinvolvementofindividualmuscles,
and these may be stripped rom the bone. Under these circumstances,
a second
lookmaybenecessarytoensurethatallthenon-viabletissueshavebeenexcisedpriortodenitivereconstruction
within seven days.
8. Classifcation o open ractures
Principal recommendations
Accurate,simpleandreproduciblesystemsforclassicationoflowerlimbinjuriesfacilitate
communication between health care proessionals, assist transer o
appropriate cases tospecialist centres and should lead to a
treatment plan.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
14/24
12
Theyprovideaplatformforconductingdetailedauditofcaretoensureoptimalmanagemento
these patients.
TheGustiloandAndersongradingiswidelyusedandisrelativelysimple,buthaspoorinter-observer
reliability and is best applied ater wound excision.
Others,suchastheAOsystem,arecomprehensivesystemsbestusedforauditanddatacollection
o outcomes.
9. Temporary wound dressings
Principal recommendations
Negativepressuredressingsmayreducebacterialingressandtissuedesiccationaswellas
avoid pooling o serous fuid.
Negativepressuredressingsarenotusedasasubstituteformeticuloussurgicalwoundexcision.
Negativepressuredressingsarenotasubstituteforcoverageofexposedfractureswithvascularised
faps.
Antibioticimpregnatedbonecementbeadsunderasemi-permeablemembraneare
associated with reduced inection rates.
Thesebeadsaremostapplicableinpatientswithsegmentalboneloss,grosscontamination
or established inection, perhaps in combination with negative
pressure dressings.
10. Techniques or skeletal stabilisation in open tibial
ractures
Principal recommendations
Spanningexternalxationisrecommendedwhendenitivefracturestabilisationandimmediate
wound cover is not carried out at the time o primary
debridement.
Fracturepatternsandbonelossdeterminethemostappropriateformofdenitiveskeletal
stabilisation.
Exchangefromspanningexternalxationtointernalxationisdoneasearlyaspossible.
Internalxationissafeifthereisminimalcontaminationandsofttissuecoverageisachievedat
the same time as insertion o the implant.
Modernmultiplanarandcircularxatorsareusedifthereissignicantcontamination,bone
loss and multilevel ractures o the tibia.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
15/24
13
4
Principalrecommendations
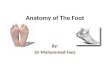
Segment 1
Segment 2
Segment 3
Safe corridors for pin
placement in the tibia
The tibia can be conveniently dividedinto three segments in
which the saecorridors are relatively constant.
Figure 1In segment one, the posterior tibial
neurovascular bundle lies close tothe midline and directly
behind theposteriorcortex.Obliquely-directedscrews avoid accidental
injury.
In segment two, a buer o the deepposterior compartment muscles
liesbetween the posterior cortex o the tibiaand the posterior
tibial neurovascularbundle. Although anteromedial
placement is popular, anterior toposterior screws are sae as
long ascare is taken to avoid over-penetration.These sagittal plane
screws are useulas they give good access or plasticsurgical
procedures on either sideo the sagittal plane o the limb.
In segment three, the anterior toposterior screw is inserted
through
a small incision and the plane betweenthe lateral edge o
tibialis anteriorand extensor hallucis longus ound.An anteromedial
screw is also useulbut attention needs to be paid toavoid tethering
the medial skin in theevent a distally-based asciocutaneousfap is
needed or racture cover.
Figure 1
-
7/30/2019 Boa Lower Limb 2009
16/24
14
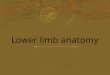
Figure 2aPinsinsertedabout1cmmedialtothetibial crest and
directed posteriorly allowasimplesagittalplanespanningxatortobe
constructed. This provides good accessor most plastic surgical
procedures.
Figure 2bThe tibial pins are inserted in the sagittal
planeapproximately1cmmedialtothecrest.Two coronal plane pins are
inserted in the oscalcis and neck o talus on the medial side.This
arrangement provides good control o thedistal tibia by eliminating
hindoot movement.Alternative pin placement includes the
baseoftherstandfthmetatarsalsbutsmallerdiameter pins should be used
in these areas.
Figure 2c
Access to the medial aspect o the distal tibiaor plastic
surgical procedures is acilitated
byalteringthepositionoftheobliqueposteriorconnecting rod as shown.
The rod is returnedto its original position ater the procedure
orthespanningxatorreplacedbydenitivestabilisation.
Figure 2dControl o knee movement (which occurs in
the sagittal plane) and access to the ront
andrearoftheproximaltibiaaretworequisitesofthespanningxatorinopenproximaltibialfractures.Therstisachievedbyusingsagittal
plane pins in both tibia and emur;an additional anterolateral pin
in the distalfemursignicantlyimprovesthestabilityofthe construct.
The second is met by keepingthe tibial pins distal to the junction
o proximaland middle tibia, thereby permitting easy
access or potential sot tissue reconstructionusing either local
or ree vascularised tissue.
4
Principalrecommendations
Figure 2a
Figure 2b
Figure 2c
Figure 2d
-
7/30/2019 Boa Lower Limb 2009
17/24
15
11. Timing o sot tissue reconstruction
Principal recommendations
Localapsaresafelyperformedatthesametimeasskeletalxation.Internalxationis
only undertaken i sot tissue coverage can be perormed at the same
time.
Freeapreconstructionisbestperformedonscheduledtraumalistsbyexperienced,dedicatedseniorsurgicalteamsfollowingadequatepreparationofthepatient,includingimaging
such as angiography or CT scanning o comminuted ractures. This
should beundertaken in a specialist centre.
Thereislittleevidencefortheve-dayrule.Microsurgeryisbestperformedbeforethe
vesselsbecomefriableorbrosedandthisbecomesincreasinglylikelyaftertherstweek.Werecommendthatdenitivesofttissuereconstructionbeundertakenwithintherstsevendays
ater injury.
12. Type o sot tissue reconstruction
Principal recommendations
Allopenfracturesarecoveredwithvascularisedsofttissue.
Dressingssuchasthoseusingfoamwithnegativepressurecantemporisefollowingwoundexcision,butarenottobeusedasasubstitutefordenitiveapcoverage.
Relativelylowenergytibialfracturesarecoveredbylocalfasciocutaneousapssolongasthevascularityhasnotbeencompromisedbythezoneofinjuryanddegloving.
Strongclinicalevidencetosupporttheuseofoneformofsofttissuecoveroveranotherinopen
tibial shat ractures is absent. However, available experimental
data would suggest thatdiaphyseal tibial ractures with periosteal
stripping are best covered by muscle faps insteado asciocutaneous
faps.
Metaphysealfractures,especiallythosearoundtheankle,arebestcoveredbyfasciocutaneous
faps, including ree faps.
13. Compartment syndrome
Principal recommendations
Compartmentsyndromeisasurgicalemergencyandmustbediagnosedpromptlyandtreated.
Theearlysignsareparaesthesiainthedistributionofthesensorynervespassingthroughthe
aected compartment and disproportionate pain, especially on passive
stretch o theaected muscles.
Theseimportantsignsmaybeaffectedbythepreviousadministrationofperipheralnerveblocks
and regional anaesthesia, as well as by the presence o nerve
injury.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
18/24
16
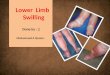
Posteromedial
incision
Anterial tibialartery and
vein and deepperoneal nerve
Peronealartery and veins
Anterolateral incision
Posterior tibialartery and veinand tibial nerve
Subcutaneoustibial border
4
Principalrecommendations
Figure 3
Compartmentsyndromedoesnotusuallyresultinthelossofperipheralpulses.Absentpulses
should alert the surgeon to the possibility o vascular injury.
Intra-compartmentpressuremeasurementisperformedmostreliablyusingdevicesdesignedspecicallyforthispurpose.Adifferenceof30mmHgorlessbetweenthemeasuredpressureand
the diastolic blood pressure is a reasonable threshold or
decompression.
Everyeffortismadetoachieveanaccuratediagnosisbecauseinappropriatefasciotomycanbeassociatedwithsignicantmorbidity.
Thetwoincisiontechniqueprovidesoptimalaccessforfourcompartmentdecompression.
The medial incision does not compromise the availability o
available local asciocutaneousfaps. It can also be used to extend
pre-existing traumatic lacerations to achieve access ordebridement
as well as provide an approach to the posterior tibial vessels as
recipientvessels or ree faps.
Allnon-viablemuscleisexcisedandfasciotomywoundseitherclosedwithsplitskingraftsor
directly, i possible, once the swelling has reduced.
Alatediagnosisofcompartmentsyndromeisamanagementdilemma.Oncethemuscleis
no longer viable, compartment release will predispose to inection,
and may result incompartmentectomy or amputation o the limb.
Figure 3 Recommended approach to the our compartments o the
leg
Anterior compartment
Peroneal compartment
Deep posterior compartment
Supercialposteriorcompartment
-
7/30/2019 Boa Lower Limb 2009
19/24
17
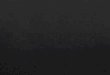
Figure 4 Landmarks, major vessels and their perorators to be
preserved
Recommended incisions for fasciotomy and wound
extensions.(a)Marginsofsubcutaneousborder o tibia marked in green,
asciotomy incisions in blue and the perorators on the medialside
arising rom the posterior tibial vessels in red. (b) line drawing
depicting the location o
theperforators.(c)montageofanarteriogram.The10cmperforatoronthemedialsideisusuallythe
largest and most reliable or distally-based asciocutaneous faps. In
this patient, theanterior tibial artery had been disrupted ollowing
an open dislocation o the ankle; hence
thepoorowevidentinthisvesselinthedistal1/3oftheleg.Thedistancesoftheperforatorsfrom
the tip o the medial malleolus are approximate and vary between
patients. It is essential topreserve the perorators and avoid
incisions crossing the line between them.
14. Vascular injuries
Principal recommendations
Devascularisedlimbsareasurgicalemergency.Theyarerecognisedimmediatelyandrequireurgent
surgical exploration. The aim is to restore circulation within
three to our hours o theinjury, ater which muscle death begins. The
maximum acceptable delay is six hours o warmischaemia time.
Capillaryrellinthetoescanbemisleadingand,ifthecirculationisnotnormalcomparedto
the contralateral limb, there is a low threshold or
exploration.
4
Principalrecommendations
5cm 5cm5cm
10cm
15cm
10cm 10cm 10cm
Peronealartery
Anteriortibial artery
Peronealartery
Anteriortibial artery
Posterior
tibial artery
Posterior
tibial artery
Figure 4a Figure 4b Figure 4c
-
7/30/2019 Boa Lower Limb 2009
20/24
18
Absentperipheralpulsesarenotattributedtovascularspasmorcompartmentsyndrome.A
major vascular injury is always considered and senior surgical
opinion is sought.
Preoperativeangiographyinthedevascularisedlimbwastesvaluabletime.Itispossibletodenethelevelofinjuryfromthefracturecongurationandanysiteofdislocation.
Shuntingsignicantlyreducesthemorbidityassociatedwiththeseinjuriesbyreducingtheischaemictime.Musclesuffersirreversibleischaemicdamagewithinthreetofourhourso
complete ischaemia. Nerves are also susceptible to ischaemic
injury.
Oncethecirculationisrestored,thelimbisreassessedwithregardtothepotentialforsalvage.
Theskeletonisthenstabilisedbeforereplacingtheshuntswithreversedveingrafts.
Proximaltothelevelofthetrifurcation,anydeepvenousinjuryisalsoreconstructed.
Accessincisionsforvascularrepairtakeintoaccountthenecessityforapcoverandthepresence
o adjacent ractures.
Fasciotomyisperformedifindicatedbythepresenceofraisedintra-compartmentalpressurescompared
to the diastolic blood pressure. However, it is important that
these measurementsare perormed repeatedly, as muscle swelling may
not develop until several hours
aterrevascularisation(seesection13).
Thepresenceofasinglepatentarterytothefootisnotacontraindicationtofreeapreconstruction
using end-to-side anastomoses. In this situation, reconstruction o
theinjured vessels is considered, especially the posterior tibial
artery.
15. Open ractures o the oot and ankle
Principal recommendations
Theseareparticularlychallenginginjuriesowingtothelimitedlocalsofttissueapoptions,likelihood
o injury to the neurovascular bundles, intra-articular ractures
predisposing
topoorlongtermfunction,anddifcultyinstabilisingthefractures.
Amputationisconsideredwhenthenalfunctionaloutcomefollowingreconstructionislikelyto
be inerior to a trans-tibial amputation. This is especially likely
to be the case or a foatingankle injury or crush injuries with an
open mid- and oreoot.
Initialskeletalstabilisationisachievedwithaspanningexternalxator,avoidingbularplating.Thereareinherentdifcultiesinstabilisingthesefracturesastheanchorpointsformostspanningexternalxatorsrelyonanintactoscalcis/talus/metatarsals.
Denitiveskeletalxationisperformedatthetimeofsofttissuecoverage.Theexactcongurationwilldependonthefracturepattern,withintra-articularfracturesusuallybestmanagedbyinternalxation.Internalxationisnotrecommendedintheabsenceof
adequatesofttissuecover,asthismaybeassociatedwithanincreasedriskofdeepsepsis.
Deglovedplantarskin:
a. I supraascial, is deatted and replaced as ull-thickness
grat
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
21/24
19
b. I subascial and proximally based, is sutured back without
tensionc. I subascial and distally based, is considered or
revascularisation.
Plantarsofttissuelossisbestmanagedusingfasciocutaneousaps,andreinnervationmayconer
some protection against the development o neuropathic ulceration.
Dorsal skin losscan be managed by split skin grats or thin, ree
asciocutaneous faps.
Openpilonfracturesarestabilisedwithaspanningexternalxator.Iftheplanneddenitivetreatmentisinternalxationofthetibialplafond,andprovidedthesofttissuespermit,openreductionandinternalxationofthebulaatprimarysurgerymayhelptoassistmaintainthe
limb out to length. Sot-tissue cover should be by way o thin,
pliable asciocutaneous faps.
Injuriestotheposteriortibialnerveareaccuratelyassessedandconsiderationisgivento
reconstruction o segmental deects o the posterior tibial artery
with autologous vasculargrat. End-to-end anastomoses to avulsed
vessels are perormed with care as it can
bedifculttoassesstheextentofintimaldamage.
Openhind-footinjuriesaremanagedasforadiaphysealinjurywhenonlyonearticularsurfaceisinvolved.Whenthereisgreaterdisruptionofthehind-foot,atrans-tibialamputationisconsidered.
Isolatedopenmid-footinjuriesareoftencausedbyheavyobjectsfallingonthefoot.These
resultinsignicantpost-operativestiffnessandpainduetoligamentousdisruptionandagain,amputation
is considered.
Openforefootinjuriesinvolvingtherstmetatarsalaretreatedasaggressivelyasopendiaphysealinjuries.Whentheothermetatarsalsareinjuredinisolation,arayamputationresults
in a reasonable return to ambulation.
16. When things go wrong with sot tissues
Principal recommendations
Necrosisofalocalapoverthefracturesiteismanagedbyearlyreturntotheatreand
revision surgery to achieve healthy sot tissue coverage.
Limitedtipcongestionmayrespondtoleechtherapy.
Somelocalfasciocutaneousapsmaybemorepronetodevelopcomplicationsinpatientswith
co-morbidities.
Freeapcomplicationsarereducedbypatientpreparation,carefulplanningandperformingtheanastomosesoutsidethezoneofinjury,ideallyproximally.
Thereisalowthresholdforimmediatere-explorationofafreeapwithsuspectedcirculatorycompromise.
Deepinfectionrequiresareturntofracturesiteexploration,debridement,deadspacemanagementandantibiotictherapy.Fracturexationmayneedrevision.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
22/24
20
17. When things go wrong with bone
Principal recommendations
Earlycomplicationswithboneoccurasaconsequenceoftheoriginalinjuryorfromsurgery.
Problemsthatpresentare:
a. wound leakage
b. sepsis
c. loss o alignment.
Commoncausesincludeinadequatedebridement,haematomaformation,inappropriateordelayedsofttissuecoverandunstablexation.Eachcauseissoughtandremediedpromptly.
Anexpectantapproachisseldomfruitfuland,ifadopted,shouldbeforalimitedperiodonly.
Adecisiontointerveneistakenifthereisfailuretoimprove.
Earlyproblemscanexertanundueinuenceonthenaloutcomeunlessweighedfortheirsignicanceandacteduponappropriatelyandpromptly.
Discussionofthecasewiththenearestspecialistcentreisencouragedandgivestheopportunity
to correct the problem at the earliest opportunity.
18. Guidelines or primary amputation
Principal recommendations
Aprimaryamputationisperformedasadamagecontrolprocedureifthereisuncontrollablehaemorrhagefromtheopentibialinjury(usuallyfrommultiplelevelsofarterial/venousdamage
in blast injuries), or or crush injuries exceeding a warm ischaemic
period o six hours.
Primaryamputationisalsoneededforincompletetraumaticamputationswherethedistalremnantissignicantlyinjured.
Aprimaryamputationisconsideredanoptionwheninjurycharacteristicsincludeoneorseveral
o the ollowing:
avascular limbs exceeding a our to six hour threshold o warm
ischaemia
segmental muscle loss aecting more than two compartments
segmental bone loss greater than one third the length o the
tibia.
Absentorreducedplantarsensationatinitialpresentationisnotanindicationforamputation.
Amputationlevelsarepreferablytrans-tibialortrans-femoral(ifsalvageofthekneeisnotpossible).
Through-the-knee amputations are not recommended or adults.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
23/24
21
Thedecisiontoamputateprimarilyshouldbetakenbytwoconsultantsurgeonswith,i
possible, patient and amily involvement.
Discussionwiththenearestspecialistcentreisadvisedwhenthereisuncertaintyordisagreementbetweensurgeonrecommendationsandpatient/familywishes.
19. Outcome measures
Principal recommendations
PatienthealthstatusquestionnairessuchasSicknessImpactProleandMedicalOutcomes
StudyShortForm-36(SF-36)provideavaluableoverallassessmentofthepatient.
Uniontimeofdiaphysealfracturescanbedifculttoassessbutisanacceptedoutcomemeasure.
Ratesofsignicantcomplicationssuchasdeepinfection,apfailureandsecondaryamputation
are recorded.
LimbfunctionscoressuchastheEnnekingScore,whichisexpressedasapercentageo
the contralateral uninjured limb, are recommended.
Peri-articularinjuriesideallyshouldincludemeasuresoftheaffectedjoints.
20. Management o severe open ractures in children
Principal recommendations
Thewoundforopenchildrensfracturesisdebrided(excised)asrecommendedforadults.There
is no evidence to suggest that tissues with compromised viability
are more likely torecover in children compared to adults.
Skeletalxationisdeterminedbythefractureconguration.Theuseofintramedullarydevicesmay
be limited by the presence o growth plates.
Theavailableevidencesuggeststhatchildrenundertheageoftwelveyears(prepubertal)
are likely to have shorter union times.
Softtissuereconstructionforopenfracturesinchildrenofallagesreliesonvascularisedfaps,
as it does or adults.
4
Principalrecommendations
-
7/30/2019 Boa Lower Limb 2009
24/24
BAPRAS
BAPRAS, the British Association o Plastic, Reconstructive
andAesthetic Surgeons, is the voice o plastic surgery in the UK. It
aimsto increase the understanding o the proessional specialty
andscope o plastic surgery, promoting innovation in teaching,
learningandresearch.Foundedin1946(originallyastheBritishAssociationofPlasticSurgeons),todayBAPRAShasover800membersandis
the proessional representative body or reconstructive and
aestheticplastic surgeons providing services to patients on the NHS
andprivately in the UK.
The British Association o Plastic, Reconstructiveand Aesthetic
Surgeons
(BAPRAS)35-43LincolnsInnFields,LondonWC2A3PE,Telephone:02078315161,Fax:02078314041
www.bapras.org.uk
BOAThe BOA is the proessional association or trauma and
orthopaedicsurgeons in the UK and those abroad who have had
orthopaedictraining in the UK or who show a continuing interest in
the aairs o
theAssociation.Foundedin1918,ourmissionistobringrelieftopeoplesuering
rom injury or musculoskeletal disorder by advancing thescience, art
and practice o orthopaedic surgery. The BOA
currentlyhasabout4000membersintheUKandoverseas,themajorityofthese
are UK consultant and trainee orthopaedic surgeons.
The British Orthopaedic Association (BOA)
35-43LincolnsInnFields,LondonWC2A3PE,Telephone:02074056507,Fax:02078312676
www.boa.ac.uk
BritishOrthopaedicAssociation
ACKNOWLEDGEMENTS
Wearegratefulthatthepublicationofthesestandardshasbeensupportedwitheducationalgrantsfrom:DePuy,Orthox,Smith&
Nephew and Synthes.