Embed Size (px)
Citation preview

1
Board Assurance Framework
Document information
Version Version 3.0
Reported to To be reported to Newham CCG Board meeting – 09.09.2013
Next review October 2013
Author Luke Moore – Governance and Risk Manager
Chair: Dr Zuhair Zarifa Accountable Officer: Steve Gilvin

2
Contents
2. Purpose and Scope ........................................................................................................... 3
2.1 Board Assurance Framework ...................................................................................... 3
2.2 Risk Management Governance ................................................................................... 3
2.3 Risk Areas ................................................................................................................... 4
2.4 Risk Identifiers ............................................................................................................. 4
3. Board Assurance Framework ............................................................................................ 5
3.1 Risk profile ................................................................................................................... 5
3.2 Risk Area 1- To reduce health inequalities, improve access and reduce variation ........... 6
3.3 Risk Area 2 - To develop Integrated Care, in particular to support improved management
of long term conditions ........................................................................................................ 12
3.4 Risk Area 3 - To ensure robust patient and public engagement is embedded in the
operations of Newham CCG and at all stages of the commissioning cycle .......................... 13
3.5 Risk Area 4 -To ensure that Newham CCG achieves robust financial stability and
balance to supporting effective working and implementation of our plans ........................... 14
3.6 Risk Area 5 - To support quality improvements in primary care services to ensure they
are fit for purpose and able to support the shift in care out of hospital ................................. 18
3.7 Risk Area 6 - To ensure that Newham CCG has transparent and effective corporate and
clinical governance arrangements in place to comply with relevant legislation and mitigate
the risk of non-delivery of strategic objectives ..................................................................... 23
4. How to interpret the Newham CCG BAF ......................................................................... 26
4.1 Risk profile ................................................................................................................. 26
4.2 Full BAF risk entries ...................................................................................................... 27
5. Newham CCG Risk Grading Matrix ................................................................................. 28

3
2. Purpose and Scope
2.1 Board Assurance Framework
The primary purpose of the Newham CCG Board Assurance Framework (BAF) is to:
1) Act as a mechanism for alerting and appraising the Board of the main risks to
achieving to the CCG in terms of achieving strategic objectives as set out in
the Operating Plan
2) List, evaluate and provide assurance to the Board regarding the mitigations in
place to the reduce the likelihood or impact of the risk
3) Summarise to the Board the remedial or proposed actions that further
mitigate the likelihood or impact of the risk
The BAF is also an important document for providing external assurance (to NHS England,
Internal Audit and patients and public) that the CCG is sighted on its risks and has a robust
system of internal control.
A guide to interpreting individual BAF entries is shown at 4. How to interpret the Newham
CCG BAF
The risk scoring matrix to establish initial risk ratings is shown at 5. Newham CCG Risk
Grading Matrix
2.2 Risk Management Governance
Risk Management is embedded in Newham CCG’s Governance Structure:-
The Audit Committee is responsible for scrutinising the group’s Risk Management policies
and procedures. Accountable to the group’s Board, the Committee provides the Board with
an independent and objective view of the group’s financial systems, financial information and
compliance with laws, regulations and directions governing the group in so far as they relate
to finance.
The Executive Committee is responsible for approving internal control arrangements, risk
sharing and pooling agreements.
The Chief Officer is responsible for approving the group’s arrangements for business
continuity and emergency planning.
The Chief Finance Officer is responsible for approving the group’s Counter Fraud, Security
Management and Risk Management arrangements.
The Governing Board is responsible for approving and monitoring the Board Assurance
Framework.

4
2.3 Risk Areas
BAF risks have been categorised into six main risk areas. Five of these risks areas link to
the core strategic objectives of Newham CCG, as outlined in the Newham CCG Operating
Plan. These are:
1. To reduce health inequalities, improve access and reduce quality variation
2. To develop Integrated Care, in particular to support improved management of long
term conditions
3. To ensure robust patient and public engagement is embedded in the operations of
Newham CCG and at all stages of the commissioning cycle
4. To ensure that Newham CCG achieves robust financial stability and balance to
supporting effective working and implementation of our plans
5. To support quality improvements in primary care services to ensure they are fit for
purpose and able to support the shift in care out of hospital
The Board has taken the view to include a sixth risk area to highlight the importance of
establishing and maintaining good governance practices to enable the CCG to effectively
deliver against its core strategic objectives:
6. To ensure that Newham CCG has transparent and effective corporate and clinical
governance arrangements in place to comply with relevant legislation and mitigate
the risk of non-delivery of strategic objectives
It is recognised that a number of BAF risks will be linked to one or more of the above risk
areas. This will be noted where applicable on the risk profile template (section 3.1).
2.4 Risk Identifiers
Each BAF risk will be assigned a unique risk identifier (number). This will be based upon the
primary area of risk identified from the five designed risk areas and subsequently the order in
which the risk is added to the BAF. For example, the first risk added to the BAF with a
primary risk area of category 1 (to reduce health inequalities… etc.) would be assigned a risk
identifier of 1.1.

5
3. Board Assurance Framework
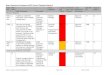
3.1 Risk profile
Risk
Identifier
Linked to
Risk AreasRisk Summary Risk Owner
Initial Risk
rating (April
2013)
October
2013
forecast
Trend
End of
Year
Target
Difference
between
target and
forecast
1.1 1,2,4,5 Failure to deliver QIPP Plans within target Scott Hamilton 15 12 8 4
1.2 1,2,4,5Failure to develop future QIPP plans appropriate to the evolving needs of the CCG
in a timely and robust mannerScott Hamilton 12 12 8 4
1.3 1,2 CSU ability to deliver on contracted services due to capability / capacity. Scott Hamilton 20 10 5 5
1.4 1 Quality of Commissioned Services at Barts Health Chetan Vyas 15 15 5 10
1.5 1,2Failure to establish and/or maintain effective enagement and collaborative working
arrangements with the Local AuthoritySatbinder Sanghera 9 9 3 6
1.6 1,2,4,5,6 Failure to recruit develop and retain key staff Steve Gilvin 20 9 6 3
2.1 1,2Failing to develop models of integrated care and robust cost and savings
assumptions to support the shift to care out of hospitalScott Hamilton 15 15 10 5
3.1 1,2,3Failing to embed meaningful patient and public engagement at all levels of the
CCGSatbinder Sanghera 10 10 10 0
4.1 4Monitoring and planning for the possible impact to CCG from Barts Health financial
performanceChad Whitton 20 15 10 5
4.2 4 Failure to monitor performance and activity at Barts Health Chad Whitton 15 15 10 5
4.3 4 Financial management of the CCG Chad Whitton 16 8 4 4
4.4 4Transfer of a proportion of the specialised commissioning budget from NCCG to
NHS EnglandScott Hamilton 20 15 10 5
5.1 5 Failing to build appropriate capacity and support for Primary Care Jane Lindo 12 12 4 8
5.2 5,6 Staff skills and competencies within the CCG Chetan Vyas 16 12 4 8
5.3 5,6 Board skills and competencies within NCCG Chetan Vyas 12 12 8 4
5.4 4,5Failure to develop practices as the "power house" of commissioning through
development of Clusters as CommissionersMargaret Chirgwin 12 12 8 4
5.5 5Failing to develop new and functional Extended Primary Care Providers/Shared
Services ProvidersMargaret Chirgwin 12 12 8 4
6.1 6 CCG has outstanding conditions for authorisation Satbinder Sanghera 12 1 1 0
6.2 6 NCCG is underpreared for its role in emergency planning procedures Satbinder Sanghera 12 8 2 6
6.3 6 Information Governance arrangements for NCCG are in an undeveloped state. Satbinder Sanghera 15 9 3 6
Risks last reviewed: September to October 2013 (for October 2013 update to Newham CCG Board)

6
3.2 Risk Area 1- To reduce health inequalities, improve access and reduce variation
Internal External Control Assurance
Actions completed
since last review
(Date)
- Revise QIPP plans to
ensure they contain
high level strategic
intentions and delivery
plans until 2014/15
- CCG Governance
revised to enable
broader oversight of
QIPP initiatives - *
Review completed and
revised CCG Governance
structure in place from
August 2013
- NHS England
sign-off of
CCG QIPP
initiatives by
March 2013
- QIPP tracker
regularly
reviewed by
SMT
- Prepare and submit
detailed QIPP plans with
a focus on low level
implementation for
2013/14/15/16.
- Revise QIPP plans to
ensure they contain
high level strategic
intentions and delivery
plans until 2014-15
- Focus on stakeholder
and PPE strategy to
ensure patients and
public are effectively
engaged in the detail of
QIPP initiatives
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
Failure to deliver QIPP
plans could result in:
- A reduced ability to
deliver local service
improvements for
patients (this year and
beyond)
- An increase in the
likelihood of
performance
management
measures from NHS
England
- Adverse media
coverage
- Failure to meet
national QIPP financial
targets and a
deterioration in the
CCG financial position
which impact the
CCG's ability to
implement service re-
design and invest to
save initiatives to
support
improvements in
commissioned care
and the shift in care
out of hospital
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
Programme Boards
(*Commissioning
Committees from Aug
2013) have responsibility
for managing/monitoring
QIPP schemes with
oversight from Quality
and Delivery PG and
Executive Committee
- QIPP trackers
developed for each
initiative to monitor
progress against
objective - led by Carl
Edmonds for CSU and
Scott Hamilton for CCG
- QIPP trackers are
reported to NCCG Quality
Committee and fed back
to CCG Board as part of
Activity and Finance
report
- QIPP trackers also
scrutinised at NCCG
Executive with input
from QIPP leads to report
on mitigations to keep
trackers on target
- Senior management
meeting between CCG
and CSU relating to
finance activity and
performance
- Terms of
reference,
agendas,
minutes of
Commissioning
Committee
meetings, Q&D
PB and CCG
Executive
Committee (for
oversight)
demonstrate
CCG focus on
delivery
- Service level
agreement
between NCCG
and NEL CSU
demonstrates
CSU support in
development
and monitoring
of QIPP
initiatives
- management
leads are in post
working with
CSU teams (e.g.
Borough Team
and Health
Intelligence) to
ensure delivery
within financial
envelope.
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- McKinsey
Consulting were
commissioned
by NHS England
to undertake a
review and
report on the
robustness of
NCCG QIPP Plans
and identify
scope for further
initiatives and
savings.
Risk Description
Risk 1.1. Failure to deliver QIPP Plans within target
Risk Lead
1.1 1,2,4,5
Proposed Actions
Target
Risk
Rating
Assurances GapsRisk
Ref
Linked
to Risk
Areas
Initial
Risk
Rating
Controls
Current
Risk
Rating
Director of
Delivery
(Scott
Hamilton)
No formal
process (i.e.
threshold) in
place for
exception
reporting to
Board as
trackers are
reviewed in
the context of
individuals
schemes (it is
expected that
this would be
picked up
through
Quality /
Executive
Committees
and reported
to Board via
special
discussion
paper as and
when
required)

7
Internal External Control Assurance
Risk 1.2 Failure to develop future QIPP plans appropriate to the evolving needs of the CCG in a timely and robust manner
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
Target
Risk
Rating
1.2 1,2,4,5 Director of
Delivery
(Scott
Hamilton)
Failing to develop
future QIPP plans in a
timely and/or robust
manner could result
in:
- Failure to reach
savings targets due to
inaccuracies in
underlying savings
assumptions
- Reputational damage
to CCG
- The possibility of
performance
measures
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
- 13/14 QIPP process fully
mapped with QIPP
identified, Lead Senior
Officers appointed, risk
assessed plans and KPIs,
and summarised in
trackers.
- Trackers updated and
reviewed monthly at
H6Executive Committee.
- Outcomes and QIPP
progress reported
monthly to Board.
- Quarterly QIPP review
meetings with input form
CCG QIPP leads, finance
and CSU to look in-depth
at in-year delivery of
QIPP to date, forward
assessment for 2014/15
with assessment of need
to carry over QIPP plans +
gap identification for
additional savings
requirements (Outputs
form QIPP review
meetings to be cascaded
through CCG Practice
Member Council and
clusters in parallel with
14/15 commissioning
round
Monthly update
and review of
trackers inc
financial and KPI
delivery.
Monthly review
by Executive
Committee.
Monthly update
in A&F report to
Board. Remedial
process
available to
ensure targets
are met. On-
going review to
identify further
QIPP. 14/15
target and early
development
programme core
to CSP.
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
QIPP identified
at scheme level
and risk rated in
Operation Plan
financial
template.
Monthly report
to NHSE.
McKinsey
assessment
provided to CCG
and NHSE and
NHSE assurance
provided
through a deep
dive assessment
in July 2013.
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
Detailed
remedial
process to be
identified.
N/A Internal audit review of
QIPP - results to be
reviewed and process
adjusted to reflect
recommendations.
Development of
remedial process to be
agreed by Quality
Committee and
Executive Committee.
Development of source
and apps financial
model to determine
2014/15 and 2015/16
QIPP requirements.
Development of
detailed plan for QIPP
identification, scheme
development and risk
rating as integral part of
CSP planning.

8
Internal External Control Assurance
Risk 1.3 NEL CSU ability to deliver on contracted services due to capability or capacity
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
1.3 1,2 Director of
Delivery
(Scott
Hamilton)
NEL CSU failing in
capability/capacity to
deliver on contracted
services could result
in:
- the increased
likelihood of failure to
deliver CCG strategic
objectives, including:
- Delivering QIPP plans
on time and on target
- Monitoring and
resolution of quality
issues with service
providers
Seve
re (
5)
x Li
kely
(4
) =
Hig
h R
isk
(20
)
- Documented
process for
escalation and
contract levers
to manage
performance
- Market test exercise to
be undertaken
- Service line price list
from CSU
Seve
re (
5)
x R
are
(1
) =
Low
Ris
k (5
)
- Monthly SLA review
meetings between
Senior CCG and CSU
teams
- Quarterly review
meeting with CSU Chief
Executive
- Annual review to test
services provided under
SLA are fit for purpose
with marketing testing
- SLA between
NCCG and NEL
CSU sets out
agreed service
areas and
performance
requirements
covered under
the contract
- CSU KPI's and
meeting
schedules
WELC POD
meeting every
two weeks to
review
performance
- Monthly CSU
Executive
Meeting for
escalation
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
- Finalise KPIs
for CSU
including local
Newham KPIs
- Establish a
CCG network
for
performance
management
of CSU
- Develop
contingency
plans for
alternative
commissionin
g support
arrangements
- Embed CSU
into the CCG
governance
structure
- Quarterly SLA review
conducted with CSU
- Restructure agreed of
the CSU team internal
process
- CCG Governance
restructure
- Developed KPIs and
performance
management process
for CSU
- Established an
escalation process for
the resolution of issues

9
Internal External Control Assurance
• Barts Health CQRM and
SPR meetings which
include trend analysis
and assurance reports
across key quality
indicators
• WELC POD Quality
Leads meetings to
commence in July 13
• Quality Leads of WELC
CCGs routinely share
information and
intelligence regarding
Barts Health
• CSU Quality and
Contracting Team
working with DD of
Quality
• Refreshed Amber Alerts
mechanism rolled out
across Member Practices
July 2013
• CCG Quality and
Delivery Programme
Board (*Quality
Committee from August
2013) where quality of
services at Barts Health is
discussed
- ToRs in place
for routine
meetings
- Agenda and
papers for 1st
Quality Leads
meeting
- Amber Alerts
received and
responded to by
Barts Health
- Quality reports
that indicate the
quality of
services at Barts
Health
- Minutes from
Quality and
Delivery
Programme
Board (*Quality
Committee from
August 2013)
Seve
re (
5)
x R
are
(1
) =
Low
Ris
k (5
)
- SLA with CSU to
support contract
and
performance
monitoring
arrangements
- Agendas and
minutes of Barts
health CQRM
and SPR
meetings
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
- Embedded
quality
monitoring of
Barts Health
- Robust
recovery
action plans
from provider
to remedy
quality
concerns
- CCG capacity
to fully
understand
the quality of
services across
Barts Health
upon
commenceme
nt of Lead
Commissioner
Role
- None
identified at
present
• Review quality
management processes
with CSU
• Agree ways of working
with WELC CCG Quality
Leads
• Review Amber Alerts
process after one
quarter and provide a
report to the Quality
and Delivery
Programme Board and
CCG Board
- NCCG Board
Development session
on 25/07 with specific
focus on Barts quality,
performance and
finance
- Barts Health Summit
meeting scheduled for
02/08 to involve key
stakeholders: TDA,
WELC CCGs, NHSE and
NELCSU
• Explore the possibility
of securing extra
resources to support the
quality management of
Barts Health upon
commencement of Lead
Commissioner role
- NCCG Governance
review completed and
revised governance
structure (inc. remit of
Quality Committee)
agreed and in place
from August 2013
1.4 1,2 Deputy
Director of
Quality
(Chetan
Vyas)
Failure to manage and
effectively monitor
the quality of
commissioned care
providers could result
in:
- Failure to meet
contractual targets
which will negatively
impact upon the
healthcare of the local
population, CCG
finances and
reputation.
- Poor value for money
for the CCG and the
taxpayer
- Potential risk in
falling to adequately
identify, monitor and
manage quality
performance issues
which could result in
unacceptable
standards of care and
the possibility of
serious incidents
occurring
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
Risk 1.4 Quality of Commissioned Services at Barts Health
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
Target
Risk
Rating

10
Internal External Control Assurance
Risk 1.5 Failure to establish and/or maintain effective engagement and collaborative working arrangements with the local authority
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
1.5 1,2 Head of
Governance
and
Engagement
(Satbinder
Sanghera)
Failure to establish
effective engagement
and collaborative
working with the Local
Authority could result
in:
- Reputational damage
and/or increased
complaints/ adverse
media coverage
- Duplication of effort
e.g. around jointly
commissioned care
areas
- Services which fail to
meet population
needs
- Poor value for money
through missed
opportunities
Mo
de
rate
(5
) x
Po
ssib
le (
3)
= M
ed
ium
Ris
k (9
)
- None
identified at
present
- Development of a
communications and
engagement strategy to
highlight the range of
communication
mediums used to
engage and collaborate
with stakeholders.
- Further clarification on
the role of LBN
representation on CCG
Board and the working
partnership on the
Health and Wellbeing
Board.
- Identify CCG
representation on other
LBN Partnership Boards
such as Children's Trust
Mo
de
rate
(3
) x
Rar
e (
1)
= Lo
w R
isk
(3)
- Joint Commissioning
Programme Board
(*Partnership
Commissioning
Committee from August
2013) meets monthly
with LA input with a focus
on jointly commissioned
areas of care.
- Monthly joint ops
meeting with LA to
discuss areas of
commonality to ensure
VFM and to identify
further joint working
opportunities
-Section 75/256 contracts
agreed with LBN
- Health and Well Being
Board
- Integrated Care
Transformation
Programme
- Work plan and
membership of
Partnership
Commissioning
Committee
established with
LBN Senior Team
and CCG GP
Chair.
- S75/256
agreements and
MOUs in place
for joint working
and joint
services to
continue.
- H&W strategy
and
implementation
plan that both
organisations
have agreed and
are jointly
implementing
- Clarity on
governance
arrangements
for the
Integrated Care
Transformation
Board
- Joint agenda
and work
programme
agreed for
Partnerships
Committee,
Health and
Wellbeing and
Integrated Care
Mo
de
rate
(3
) x
Po
ssib
le (
3)
= M
ed
ium
Ris
k (9
)
- Awaiting
NHS England
monitoring /
performance
management
process for
novated
services such
as Health
Visiting,
School
Nursing etc.
- NCCG Governance
review completed and
revised governance
structure (inc. remit of
Partnerships
Commissioning
Committee) agreed and
in place from August
2013

11
Internal External Control Assurance
Risk 1.6 Failure to recruit develop and retain key staff
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
1.6 1,2,4,5,6 Chief
Executive
Officer
(Steve Gilvin)
Failure to recruit and
or retain key staff
across the
organisation could
result in:
- loss of organisation
memory
- Increased difficulty
in monitoring and
meeting QIPP targets
and strategic
objectives
- Negative financial
implications as a result
of increased
recruitment costs
Seve
re (
5)
x Li
kely
(4
) =
Hig
h R
isk
(20
)
- All staff to undertake
an appraisal process
with PDPs to support
career and skills
development
- Initial appraisals and
agreed 2013/14 PDPs for
all staff to be finalised
and signed-off by end
September 2013
Min
or
(2)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(6)
- Nearly all permanent
posts now recruited to
- External recruitment
being undertaken if no
suitable candidates in
internal redeployment
pool
- Temporary staff
recruited if business
need is agreed
- Training and
skills
development
programme in
place for all staff
to support
succession
planning and the
development of
future
organisational
leaders.
- NEL CSU
support for
temporary/short
term
recruitment and
substantive
recruitment
processes
Mo
de
rate
(3
) x
Po
ssib
le (
3)
= M
ed
ium
Ris
k (9
)
- One
substantive
post in CCG
structure
currently
vacant
(Performance
Manager)
- CCG Head of
Informatics post
appointed as at 21/07/13

12
3.3 Risk Area 2 - To develop Integrated Care, in particular to support improved management of long term
conditions
Internal External Control Assurance
2x Project management
support roles appointed
to support the overall
delivery of the
Integrated Care
programme
Proposed Actions
Target
Risk
Rating
2.1 1,2 Bob Arora,
Integrated
Care Project
Lead
- Increased activity
levels in acute and
increased cost under
PBR arrangements
- Fragmentation of
care pathways and a
lack of joined up
services
- Lack of clarity around
national IG guidelines
for risk stratification
and integrated care
could impede linking
of patient data across
providers
- Failure to work
collaboratively with
providers to ensure
flows of money
effectively follow the
patient journey could
lead to cost
duplication, i.e. an
increase in costs for
community provision
without subsequent
reduction in acute
capacity
Seve
re (
5)
x Li
kely
(4
) =
Hig
h R
isk
(20
)
3 dedicated integrated
care work streams
established: -
1. Rapid Response
2. Discharge support -
including Mental Health
liaison and discharge
support (RAID model)
3. Coordination
- CCG and local authority
leads for IC appointed to
lead development of IC
in Newham
- IC Programme
Board (* IC
Transformation
Board from
August 2013) and
delivery work
streams (ToR,
Minutes)
- WELC
Integrated Care
Board to look at
elements of IC
that can be
effectively
developed and
delivered across
WELC
- NCCG IC
Programme
Board receives
regular reports
and integrates
with WELC IC
Board. _
Monthly reports
from NCCG IC
Transformation
Board to NCCG
Board to track
and monitor
progress of the
development of
Integrated Care
UC streamer
model supports
appropriate A&E
admissions
avoidance
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
- IC
Management
lead post to
be re-
advertised
- One
Integrated
Care project
management
support post
remains
vacant
awaiting
recruitment
LBN
advertising for
a Band 7 IC
Transformatio
n Manager to
support the
delivery of
Integrated
Care
Work closely with
providers to develop
appropriate
reimbursements models
aimed at ensuring the
money follows the
patients and where
appropriate releasing
capacity savings in acute
(recognition that savings
may not be only
financial but also
possibility in freeing up
Consultant time to
provide step down
support to Community
and Primary Care).
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
Risk 2.1. Failing to develop models of integrated care and robust cost and savings assumptions to support the shift of care out of hospital
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
Gaps Actions completed
since last review
(Date)

13
3.4 Risk Area 3 - To ensure robust patient and public engagement is embedded in the operations of Newham
CCG and at all stages of the commissioning cycle
Internal External Control Assurance
Proposed Actions
Target
Risk
Rating
Current
Risk
Rating
Gaps
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
-
Development
of a CCG
Comms. and
Engagement
Strategy
- More detail
required
around
processes in
place to
monitor the
effectiveness
of patient
engagement
activities
- PPE Manager
leading on
engagement
strategy with
support from
CSU on
comms.
element
Development of a
communications and
engagement strategy
and action plan to build
on existing engagement
platforms and develop
new platforms to
increase borough wide
participation and
strengthen inclusion of
hard to reach groups
- Conduct a scoping
exercise to potentially
further develop the role
of PPGs at cluster level
- Develop a forward plan
to track and coordinate
PPE needs across the
CCG and ensure the CCG
is delivering on its duty
to involve
- Increase promotion of
how to get people
involved through
community outreach
and CCG communication
channels
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
Actions completed
since last review
(Date)
- Appointment
of Board Lay-
Member
responsible for
PPE
- Head of
Governance and
Engagement and
PPE Manager
posts in place
- PPE Strategy
and action plan-
Complaints
monitoring
process adds
additional level
of assurance
around capturing
patient feedback
- PPE Manager to
build capacity of
CCG staff to
deliver effective
PPE and embed
across all levels
of the CCG
- CCG website
- PPE support
commissioned
through Forum
for Health and
Wellbeing
- Patient forums
and PPGs act as
mediums to
capture
feedback
Risk 3.1 Failing to embed meaningful and measurable patient engagement at all levels of the CCG structure and throughout the commissioning cycle
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances
3.1 1,2,3 Head of
Governance
and
Engagement
(Satbinder
Sanghera)
Failure to implement
meaningful PPE
strategies could result
in:
1. CCG unable to
deliver on Section 242
of the NHS Act 2006,
which mandates NHS
organisations to
involve patients in the
planning,
development of
proposals and
commissioning of
healthcare services.
2. Reputational
damage and / or
increased complaints /
adverse media
coverage
3. Services which fail
to meet population
needs (and
consequently offer
poor value)
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
Established PPE
platforms:
- Newham Patient Forum,
Community Reference
Group, Health and Social
Care Network and PPGs

14
3.5 Risk Area 4 -To ensure that Newham CCG achieves robust financial stability and balance to supporting
effective working and implementation of our plans
Internal External Control Assurance
Risk 4.1 Monitoring and planning for the possible impact to NCCG arising from the financial performance of Barts Health
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
4.1 4 Chief Finance
Officer
(Chad Whitton)
Failure to monitor and
plan for the impact on
the CCG arising from
the financial
performance at Barts
Health could result in:
- Reduced ability to
plan for/shift care out
of hospital
- reduction in local
acute services
Requirements for
allocation of
contingency funding
to support Barts
Health which could
reduce CCGs
bargaining power in
other provider
contract negotiations
Seve
re (
5)
x :L
ikel
y (4
) =
Hig
h R
isk
(20
)
- Co-ordination
of monitoring
and control -
triangulation
with Specialised
commissioning
activity
- Clarification of
commitment to
WELC CCGs
through risk
share on impact
of turnaround
- Input and
agreement
required with
Commissioning
Lead to Barts
Health
Turnaround Plan
- Board development
session to focus on
mitigation strategies for
Barts financial risk.
Development of BH
Productivity
Improvement Plan - CSU
dedicated team to
monitor contract
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
- WELC Mgt and
Collaborative
Commissioning
Governance Structure
overseeing
implementation of
contract including in-
depth analytics, claim
management.
- CCG Acute
Commissioning
Committee overseeing
CCG specific analysis.
- Dedicated CCG/CSU
capacity to ensure
effective monitoring and
contract control
- Updates on Barts
financial performance
picked up through
discussions with
collaborative leads
through the WELC Clinical
Strategy Groups
- Barts Health provide an
update on the CIP
programme to the WELC
Clinical Strategy group
attended by COs, Chair's,
and CFOs of all WELC
CCGs - pertinent updates
will be fed back via
reporting to NCCG Board
CCG Acute
Commissioning
Committee
WELC Mgt and
Collaborative
review, Monthly
contract
meetings,
monitoring
against
projected
activity including
agreed BH
Productivity
Improvement
Plan
- CCG review of
Barts CIP plan to
sign-off that CCG
are happy there
are no material
quality
implications as a
result of
proposed
savings
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
- In depth
analysis of Barts
Health Cost
Improvement
Programme (CIP)
- Formal access
and input to
Barts Health
Turnaround and
other associated
plans
- Timely access
to Barts Health
financial
reporting

15
Internal External Control Assurance
Risk 4.2 Failure to monitor performance and activity levels at Barts Health
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
4.2 4 Chief Finance
Officer
(Chad
Whitton)
Failure to monitor
performance and
activity at Barts Health
could result in:
- Increased risk of over
performance due to
loss of 5% cap and
collar arrangement
and move to PBR
contract for 2013/14
with associate risk of
uplift in contract
value.
- Reduced bargaining
position in contract
negotiations with
other providers
- Reduction in the
CCG's budget to
support the shift in
care out of hospital
and integrated care
work streams
- Disaggregation of
specialised
commissioned
services could lead to
duplication of charge
Seve
re (
5)
x Li
kely
(4
) =
Hig
h R
isk
(20
)
- Strong well
established
collaborative
working
arrangements
with other
significant
commissioners
(WELC)
- Robust
alignment with
specialised
commissioning
- Development of
demand management
targets at cluster level
- Triangulation with
specialised
commissioning contract
and monitoring teams
- Continuation of regular
update via weekly
CFO/WELC Collaborative
Telcons with Lead
Commisioner CFO
- Triangulation with
TDA/NHSE on
turnaround to ensure
limited liability
- Recruitment of
informatics/analytics
capacity to work with
CSU to enhance
effectiveness of
monitoring
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
- Focus on demand
management initiatives
at cluster level
- Contractual levers
including KPIs and
CQUINS
- Monthly CQRM and SPR
meetings to review
quality and performance
issues at the Trust
- Urgent Care re-
procurement and service
re-design to support the
management of patients
in non acute setting and
appropriate streaming of
patients to non-urgent
community care settings
- Development of virtual
ward to reduce
admissions and LOS
- Clinical engagement in
Barts Health productivity
agreement
- Regular update via
weekly CFO/WELC
Collaborative Telcons
with Lead Commisioner
CFO
- Minutes of
cluster meetings
to demonstrate
work around
demand
management
- Clinical
engagement
into CQRM and
SPR processes
- Monthly high
level service
review meetings
between NCCG
and Barts Health
SLA with CSU for
contract and
finance activity
monitoring
arrangements
- NHS England
performance
management
processes would
ensure that a
development
plan is initiated
upon major
slippages
- Tripartite
formal
agreement
between NHS
London, DH and
Barts Health (on
Merger FBC and
Barts CIP)
Seve
re (
5)
x P
oss
ible
(3
) =
Hig
h R
isk
(15
)
- NCCG
Informatics /
information
analyst post
remains
vacant
- Emerging
national IG
regulations
may prohibit
CCGs from
accessing PID
data around
financial
activity which
could prevent
clinical
challenge
- CCG Head of
Informatics post
appointed as at 21/07/13

16
Internal External Control Assurance
Risk 4.3 Financial management of Newham CCG
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
4.3 4 Chief Finance
Officer
(Chad
Whitton)
Failure to plan for a
sustainable financial
future could result in:
- Major impact on the
CCG's ability to deliver
its strategic objectives
and QIPP targets
- Severe impact on
CCG finances and the
likelihood of a
deterioration in the
budget position with
the possibility of a
deficit budget at year
end
- Severe damage to
CCG reputation
- The possibility of
performance
management
measures being
imposed by NHS
England Maj
or
(4)
x Li
kely
(4
) =
Hig
h R
isk
(16
)
- Final
financial plan
- Scheme of
delegation
- Review of core
governance policies
including prime
financial policies in
Sept/Oct 2013 agreed
with NCCG Audit
Committee
- Internal audit review
agreed for the following
areas: Continuing Care;
Clinical Governance &
Quality;
Governance Framework -
Phase One & Two;
Budgetary Control,
Financial Reporting &
QIPP;
Commissioning &
Contract Management ;
Contract Monitoring –
Commissioning Support
Unit ;
Payroll & Financial
Feeders;
Risk Management /
Board Assurance Part
Two;
Remuneration of
Members.
Maj
or
(4)
x R
are
(1
) =
Low
Ris
k (4
)
- Finance plan for 2013/14
has a 1% surplus target
and will provide 2% non-
recurrent headroom and
1% contingency, 50% of
which is to cover acute
contracting risk. There
will be a risk reserve of
£2.3 million and plans to
commit the balance of
£3.8m brought forward
12/13 surplus on non-
recurrent pump-priming
initiatives.
- Detailed monthly
reporting to NCCG Board
and Q&D Programme
Board
- Monthly FIMS return to
NHS England
- Substantive
CFO in post
- Documented
NCCG Board
approval of
Financial Plan
- Audit
Committee TOR,
agenda and
minutes
- CCG Board and
Q&D PG minutes
- Financial
reports process
to Board
provides
indicative
position at
ledger close
- NHS England
approval of
financial plan as
part of the
authorisation
process
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
- Review of
standing
financial
instructions
and scheme of
delegation

17
Internal External Control Assurance
Risk 4.4 Transfer of a proportion of the specialised commissioning budget from NCCG to NHS England
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
4.4 4 Director of
Delivery
(Scott
Hamilton)
There is a risk that the
CCG will not be able to
fully recover funding
transferred pro-rata to
NHS England to enable
the Londonwide costs
of specialised
commissioning to be
met. As a result:
- This could impact the
CCG's ability to reach
acceptable Heads of
Terms with providers
(* though outline HoT
have been agreed
with major Acute and
Community providers
for 2013/14)
Seve
re (
5)
x Li
kely
(4
) =
Hig
h R
isk
(20
)
- Detailed work to be
undertaken by
NCL/NELC CCG in
conjunction with the
CSU contracting team to
monitor and challenge
the contract value of
specialist
commissioning services
transferred to NHS
England
- Capturing and coding
of CCG specialist
commissioning activity
to be established with
activity flows linked to
established pathways
and protocols
- CCG to define and
referral activity and
guidelines for
specialised
commissioning
Seve
re (
5)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(10
)
- The NCCG Board holds
overall responsibility for
commissioning services
within budget
- Programme Boards
(*Commissioning
Committees from August
2013) hold devolved
budgets for their defined
areas of commissioning
- CCG providers are
engaged through
Programme Boards and
contract negotiation
meetings.
Director of
Delivery holds
overall
responsibility
for acute
commissioning
- A technical
group led by the
London area DoF
and including
CCG
representatives
is working with
the SCG to
ensure CCGs
contributions
are matched to
commitments
throughout the
year with
appropriate
repatriation of
excess funding
Seve
re (
5)
x M
od
era
te (
3)
= H
igh
Ris
k (1
5)
Deep dive into
the detail of
the main areas
of specialist
commissionin
g to be
undertaken
jointly
between CCG
Informatics
Lead and
NELCSU team.
- CGG Head of
Informatics post
appointed as at 21/07/13

18
3.6 Risk Area 5 - To support quality improvements in primary care services to ensure they are fit for
purpose and able to support the shift in care out of hospital
Internal External Control Assurance
Risk 5.1 Failing to build appropriate capacity and support for the development of Primary Care
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
5.1 5 Deputy
Director of
Delivery
(Jane Lindo)
Failure to build
appropriate skills,
capacity and support
for primary care
providers could result
in:
- Adverse
media/reputational
risk
- An under-resourced
workforce
- Primary Care
Facilities not fit for
purpose
- Lack of capacity to
manage expected
increase in demand
for Primary Care
services as a result in
the planned shift in
care out of hospital
-Unnecessary
unscheduled
admissions
- Failure to meet
outcome framework
indicators
Maj
or
(4)
x Li
kely
(4
) =
Hig
h R
isk
(16
)
- Monthly
cluster reports
Development of a
primary care strategy
that incorporates a
workforce skills and
education mapping
exercise to be
undertaken to identify
gaps and plan
contingencies
Development of a
Performance framework
to monitor cluster plans
Strongly performance
manage CSU data
reporting function. At
present NELIE and other
reports not meeting
basic requirements.
Development of
integrated care
programme including
extended Primary Care
Team to support
practices to keep
patients out of hospital -
extended district nurse
pilot covering 6
practices will become
fully operational end of
September
Maj
or
(4)
x R
are
(2
) =
Low
Ris
k (4
)
- Development of Primary
Care Strategy to include
development of Performance
Management Support to
clusters and practices and
development of future
models of primary care
providers e.g. federated
models/networks.
Development of Cluster
plans to support primary
care targets and demand
management initiatives.
- Prescribing team
supporting practices
- Monthly cluster meeting to
review activity and quality
data and other reports,
discuss ideas, share
concerns and share best
practice between practices
and other clusters
- Monthly cluster leads
meeting to coordinate ideas,
share concerns and share
best practice between
clusters to feed up through
the CCG structure
- educational curriculum
with monthly GP educational
meetings reflecting key
priorities
- Introduction of EMIS web
and training to support use
-Monthly MDTs in place for
Diabetes.
- Each NCCG
cluster has
dedicated
Practice
Facilitator
support
- Project Director
for Primary Care
Strategy
appointed to
lead the
development of
a primary care
strategy for
Newham
- Agendas and
papers from
cluster and
cluster leads
meetings
- Cluster Plans
- Extended hours
schemes help to
support
improved access
- Working
collaboratively
with NHS
England to
identify and
mitigate against
risks in primary
care skills and
capacity gaps
- Working
collaboratively
NBC to ensure
the primary care
role in
prevention is
not reduced or
lost
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- Statistically
valid analytics
to support
clusters and
practices to
understand
where there is
true quality
variation with
national and
other useful
benchmarks
Development
of the CHN
services
focussed on
supporting
practices and
patients to
avoid
emergency
admissions
(Virtual Ward,
Rapid
Response,
Extended
Primary Care
Team)

19
Internal External Control Assurance
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
5.2 5,6 Deputy
Director of
Quality
(Chetan
Vyas)
Failure to bridge skills
and competency gaps
throughout the
organisation could
lead to:
- Errors or significant
incidents resulting in
financial and/or
reputational loss
- Difficulty with
succession planning
-Failure to deliver
objectives on time and
on-targetM
ajo
r (4
) x
Like
ly (
4)
= H
igh
Ris
k (1
6)
Analysis of
Gaps to be
undertaken
subsequent to
the
completion of
the Training
Needs
Analysis
- Training Needs
Assessment (TNA) of
CCG staff to understand
their requirements
- Continue Staff
Development sessions
- Roll-out of Personal
Development Review
process to ensure all
staff have objectives
and PDPs
- Initial appraisals and
2013/14 PDPs for all staff
to be finalised and
signed-off by end Sept
2013
- Roll-out of Learning
and Development policy
to access CCG funds
- Understand what
learning and
development
opportunities CCG staff
can access via the CSU
- Staff Development
Sessions have
commenced
- Staff meetings are being
re-shaped to encourage
collective development
in meetings
- SMT development day
held to develop the SMT
SMT Devt Day
agenda
None identified
at present
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)

20
Internal External Control Assurance
Risk 5.3 Board skills and competencies within NCCG
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
Target
Risk
Rating
5.3 5,6 Deputy
Director of
Quality
(Chetan
Vyas)
Failure to bridge skills
and competency gaps
in the Board of NCCG
could lead to:
- Errors or significant
incidents resulting in
financial and/or
reputational loss
- Significant
reputational damage
and/or adverse media
interest
- Difficulty with
succession planning
-Failure to deliver
objectives on time and
on-target
- Potential for
enforced performance
management
conditions from NHSE
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- Board Development
Plan in place signed off
via the authorisation
process
- Board Development
schedule in place
- Board
Development
Plan
- Board
Development
Meetings
- Agendas of
Board
Development
Meetings
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
Review of the
effectiveness
of the Board
Development
Plan to
understand
progress made
by the Board
development
• Board Code of Conduct
to be drafted
• Board Conflicts of
Policy to be reviewed
and amended
• Review of how the
Board has collectively
performed

21
Internal External Control Assurance
5.4 Failure to develop practices as the "power house" of GP commissioning through development of Clusters as Commissioners
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
Target
Risk
Rating
5.4 4,5 Project
Director for
Primary Care
Strategy
(Margaret
Chirgwin)
Failure to build
appropriate skills,
capacity and support
for clusters as
commissioners could
result in:
- CCG failure to live
within budget
- Lack of provision for
expected increase in
demand for PC
services as a result in
the planned shift in
care out of hospital
- Increased activity
and therefore cost
under Barts PBR
- Failure to meet
outcome framework
indicators
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- Development of
Primary Care Strategy to
include development of
Commissioning role of
clusters
- Monthly cluster
meeting to discuss ideas,
share concerns and share
best practice between
practices and other
clusters
- Monthly cluster leads
meeting to coordinate
ideas, share concerns and
share best practice
between clusters to feed
up through the CCG
structure
- CCG engagement LES
requiring attendance at
cluster and CCG wide
events
- Monthly Practice
Member Council
Meetings
- Each NCCG
locality
(covering 2
clusters)has
dedicated
Practice
Facilitator
support
- Programme
Director for
Primary Care
Strategy
appointed to
lead the
development of
a primary care
strategy for
Newham
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- CCG
constitution
clearly defines
the Clusters as
Committees of
the Board and
their
commissioning
roles and
responsibil ities
- Agreement on
budget
allocation
methodology to
practices and
clusters
- Agreement on
risk sharing
between
practices and
clusters
- Agreement on
management of
cluster under
and overspends
at the end of
year
- Financial
reporting at
cluster and
practice level
- Financial and
commissioning
support to
clusters
-Board papers
- Changes to
constitution
- Review relevant
sections of the
constitution
-Take paper to the Board
on budget allocation
formula to practices and
clusters for 2013/14 for
shadow budget and
process for 14/15 budget
allocations
-Take paper to the Board
on risk sharing proposals
within and between
clusters
- Take paper to the
Board on how propose
to manage cluster under
and over spends at end
of 2013/14
- Agree CCG
Management and
finance support
required to develop
clusters as
commissioners
(recommend an 8D
supporting 2 clusters +
finance to attend cluster
meetings)

22
Internal External Control Assurance
Risk 5.5 Failing to develop new and functional Extended Primary Care Providers/Shared Services Providers
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
Target
Risk
Rating
5.5 5 Project
Director for
Primary Care
Strategy
(Margaret
Chirgwin)
Failing to develop new
Extended Primary Care
Providers/Shared
Services Providers
could result in:
- Adverse
media/reputational
risk
- An under-resourced
workforce
- Lack of provision for
expected increase in
demand for PC
services as a result in
the planned shift in
care out of hospital
- Increased activity
under Barts PBR
- Unnecessary
unscheduled
admissions
- Failure to meet
outcome framework
indicators
- Widening gap in life
expectancy between
best and worst off
decile of the Newham
population and
between Newham and
England average
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- Development of
Primary Care Strategy to
include development of
Extended Primary Care
Providers including how
this market should be
developed and how the
CCG will commission
these kinds of services
and service
developments
- Engagement with
Member Practices in the
development of the
strategy
- Primary Care
Strategy Draft
Outline
document
- Agendas for
practice Council,
Cluster meetings
etc. include
discussion of
what kind of
providers the
CCG should
develop
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
- The present
Newham CCG
procurement
strategy is out
of date and
not reflective
of the current
NHS position
with respect
to
procurement
New CCG
procurement
strategy
- NELCSU in discussion
with NCCG to develop a
new draft procurement
strategy for discussion
and approval by NCCG
Board

23
3.7 Risk Area 6 - To ensure that Newham CCG has transparent and effective corporate and clinical
governance arrangements in place to comply with relevant legislation and mitigate the risk of non-delivery
of strategic objectives
Internal External Control Assurance
None
identified at
present
Insi
gnif
ican
t (1
) x
Rar
e (
1)
= Lo
w R
isk
(1)
- Evidence to support the
removal of the remaining
conditions was submitted
to NHS England in the
June evidence window
- Working with NHS
England to clarify
expecttaions on the
WELC conditions,
particularly risk share
Mitigation plan
developed and
regularly
submitted to
NHS England for
review
Authorisation
feedback and
feedback on
evidence
submissions
from NHS
England to
identify areas
where further
detail is
required
Insi
gnif
ican
t (1
) x
Rar
e (
1)
= Lo
w R
isk
(1)
- Awaiting
guidance on
how end of
year 1
assessment
will be
undertaken
Confirmation received
from NHSE on 23/07 that
all 8 outstanding
conditions have been
removed.
6.1 6 Head of
Governance
and
Engagement
(Satbinder
Sanghera)
NCCG has been
authorised by NHS
England (With 8
remaining conditions
as at the June 2013
evidence window).
In order to fully
discharge its
commissioning duties
the CCG must remove
the remaining
conditions as soon as
possible.
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
Risk 6.1 NCCG has outstanding authorisation conditions
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)

24
Internal External Control Assurance
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Actions completed
since last review
(Date)
6.2 6 Head of
Governance
and
Engagement
(Satbinder
Sanghera)
Uncertainty over
emergency planning
and NCCG's role
Maj
or
(4)
x P
oss
ible
(3
) =
Me
diu
m R
isk
(12
)
None
identified at
present
Business Continuity and
Emergency planning
arrangements require
sign-off from Executive
Committee
NCCG is working with
colleagues at NHS
England, CSU, other CCGs
and LBN to ensure that
robust emergency
planning remains in place
throughout the transition
period and into the
future.
- Desktop emergency
planning exercise
facilitated by NHS
England planned for CCG
and key Health
Organisation EPRR
leaders in July 2013
- Attending EPPR/BCP
London quarterly
meetings hosted by NHS
England (London office)
to share common
concerns and best
practice
NCCG Business
Continuity Plan
developed
outlining local
business
continuity
arrangements to
feed into wider
emergency
planning
arrangements
- On call rota
established for
EPRR between
senior NCCG
Directors as part
of WELC Pod on-
call
arrangements
CSU specialist
support for EPRR
and surge
management
Maj
or
(4)
x U
nlik
ely
(2
) =
Me
diu
m R
isk
(8)
None
identified at
present

25
Internal External Control Assurance
Risk 6.3 Information Governance arrangements for Newham CCG are in an underdeveloped state
Risk
Ref
Linked
to Risk
Areas
Risk Lead Risk Description
Initial
Risk
Rating
ControlsAssurances Current
Risk
Rating
GapsProposed Actions
Target
Risk
Rating
Actions completed
since last review
(Date)
6.3 6 Head of
Governance
and
Engagement
(Satbinder
Sanghera)
Information
Governance
arrangements for
Newham CCG are
under developed
Mo
de
rate
(3
) x
Ce
rtai
n (
5)
= H
igh
Ris
k (1
5)
Shared folder
resource
between CCG
and CSU IG
support team
developed
with template
policies for
Information
Governance
Work in progress on
completion of IG Toolkit
in conjunction with
specialist support from
CSU IG team.
Mo
de
rate
(3
) x
Rar
e (
1)
= Lo
w R
isk
(3)
- IG Toolkit to be
completed to ensure
compliance with relevant
IG legislation
- IG development plan
established to monitor
progress against IG
Toolkit completion and
development of
associated IG policies and
procedures
- Procedures are in place
to ensure all NCCG staff
complete mandatory IG
training on an annual
basis
- Corporate incident
reporting procedures
developed to identify
monitor and follow up
risks or incidents which
impact on IG
NCCG has
appointed a
Caldicott
Guardian, Senior
Information Risk
Owner (SIRO)
and Information
Governance
Lead to ensure
the CCG remains
compliant with
relevant IG
legislation and
to promote best
practice IG
arrangements
throughout the
CCG
NCCG has
commissioned
expert
information
governance
support from the
CSU which
includes support
around
completion of
the IG Toolkit
Mo
de
rate
(3
) x
Like
ly (
4)
= M
ed
ium
Ris
k (1
2)
Development
of NCCG
specific IG
policies
- Appointments of CG,
SIRO and IG leads for
NCCG recognised by
Audit Committee
- All NCCG staff
registered on IG online
training tool for 2013/14

26
4. How to interpret the Newham CCG BAF
4.1 Risk profile

27
4.2 Full BAF risk entries

28
5. Newham CCG Risk Grading Matrix

29