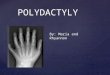
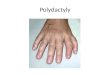
Major: functional significance Polydactyly, colobomas,
meningomyelocele, cleft lip Incidence 1% Minor: cosmetic
significance Epicanthal folds, single transverse palmar crease,
supernumerary nipples Incidence 14% Both more common in premature
babies
Slide 3
Pierre Robin is best described as a A.Deformation B.Disruption
C.Dysplasia D.Sequence E.Association
Slide 4
Broad term An abnormality of embryonic morphogenesis Usually
results from genetic, chromosomal, or teratogenic influences May be
multifactorial Constitutes single primary defect OR, component of
multiple malformation syndrome Often require surgical
intervention
Slide 5
Alteration (often molding) of intrinsically normal tissue due
to exposure of unusual extrinsic forces. Uterine constraint from
crowding Potter facies Most respond to medical therapy and have
good prognosis
Slide 6
Breakdown of normally formed tissue Vascular accidents Amniotic
bands Earlier in embryogenesis: More severe
Slide 7
Abnormal organization of cells within tissue Genetic basis
Achondroplasia Most frequent cause of skeletal dysplasia
Slide 8
Malformation: Embryonic morphogenesis Deformation: Alteration
of intrinsically normal tissue by external force Disruption:
Breakdown of normally formed tissue Dysplasia: Abnormal
organization of cells within tissue
Slide 9
Single problem in morphogenesis Cascade resulting in series of
structural alterations Recognizable pattern of multiple anomalies
Pierre Robin Microretrognathia (single, primary malformation)
Glossoptosis: posterior placement of tongue U-shaped cleft
palate
Slide 10
Pattern of malformations that occurs together too frequently to
be due to random chance. No specific etiology is known.
Slide 11
Slide 12
Nonspecific
Slide 13
Congenital heart disease (45%) AV Canal Defects GI anomalies
(5%) Duodenal atresia Hirschsprung Thyroid disorders ! Regular
Screening ! Leukemia 15 to 20 times more common Neonates may have
transient leukemoid reaction
Slide 14
Cognitive impairment IQ 20-80 Mild to Moderate Developmental
Delay Early intervention, education, and sporting activities
demonstrate improved outcomes. Atlanto-axial instability
Slide 15
Slide 16
A parent of a child with Down Syndrome is found to have a 21/21
translocation. What are the chances that her next child will have
Down Syndrome? A.2% B.15% C.33% D.50% E.100%
Slide 17
If either parent has 21/21 translocation All children will have
Down Syndrome If parent has 21/centric translocation 2% of fathers
children 15% of mothers children
Slide 18
Maternal AgePrevalence 251/1350 351/355 451/23 Remember!!!!
Most children with Down Syndrome are NOT born to older
parents!!!!
Slide 19
13 (Patau) and 18 (Edwards) May overlapping features! Focus on
characteristic features.
Slide 20
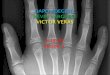
P = Patau = Pits = Polydactyly 3 is a clefted 8 13= Midline
defects
Slide 21
8 8
Slide 22
A 15-year-old girl comes to your office because she never has
had a menstrual period. She has no chronic illnesses and is active
playing softball once a week. Her mother and sister both had
menarche at age 13 years. On physical examination, she is at the
15th percentile for height and weight and has no hirsutism or acne,
no breast development, and Sexual Maturity Rating 3 pubic hair
development. The MOST appropriate lab test is: A.Karyotype B.
Progesterone and 17-hydroxyprogesterone C.Microarray D.FISH
E.Testosterone
Slide 23
Slide 24
1/2000 liveborn females Characteristics: Primary amenorrhea
Sterility Sparse pubic hair Underdeveloped breasts Short stature
Webbing of neck Cubitus valgus Low hairline Shield chest with wide
spaced nipples lymphedema
Slide 25
Other organ systems Renal anomalies Congenital heart disease
Bicuspid aortic valve (30%) Aortic coarctation (10%) Mental
development usually normal Findings may be subtle and missed until
adolescence Get karyotype on adolescent female with delayed
puberty, especially if short stature
Slide 26
Karyotype 45X Recurrence risk for parents is 1-2% unless a
parent has abnormal X 15% are Mosaics If mosaic has an XY cell
line, gonads should be removed
Slide 27
Does the risk of having a child with Turner Syndrome or
Klinefelter Syndrome increase with advanced maternal age? A. Yes
for both B. No for Turner, Yes for Klinefelter C. Yes for Turner,
No for Klinefelter D. No for both
Slide 28
1/500 newborn boys Physical stigmata may not be obvious until
puberty Testosterone levels usually low (variable) IQ is normal (or
mildly decreased) Behavioral problems may be more common
Slide 29
Karyotype XXY 80% XY/XXY in 20% IF additional X present (XXXY)
More cognitive and skeletal abnormalities Congenital Heart Disease
may be seen PDA most common Parents recurrence risk 1-2% Risk
increases with maternal age
Slide 30
Klinefelter
Slide 31
A new 13 year old male patient has a long, narrow face and
enlarged, protruding ears, and joint laxity. He is very active, has
difficulty making eye contact, and engages in some hand flapping.
His most recent testing showed an IQ of 45. Family history reveals
that the maternal uncle has intellectual disability. The MOST
appropriate test to confirm the diagnosis is A.Karyotype B.Skin
biopsy for staining C. Molecular DNA analysis D.MRI of Brain E.
Clinical Diagnosis Only
Slide 32
Slide 33
There is an excess of males in the mentally retarded population
This is largely due to Fragile-X
Slide 34
Most common chromosomal cause of MR May be expressed (less
severe) in females Expression may be amplified over generations
(anticipation) Physical Long face Long, protruding ears MR
Prominent jaw Macroorchidism May have hyper-extensible joints
Slide 35
Trinucleotide repeat disorder Inheritance X-linked Dominant
Variable expressivity Expression amplified over generations Look
for Hx of affected male family members (uncles) Choose molecular
DNA analysis Methylation study Otherwise PCR or Southern Blot
Slide 36
Angelman Prader-Willi
Slide 37
Function of certain genes is dependent on their parental origin
Maternal vs Paternal Particularly for 15q11-13 Prader-Willi
Deletion of paternally derived Chromosome 15 Angelman Deletion of
maternally derived Chromosome 15 Diagnosis: Methylation,
High-resolution cytogenetics, or FISH
Slide 38
Markedly Hypotonic baby May have decreased DTR May be SGA Poor
feeding and FTT Developmental Delay Hypotonia resolves Insatiable
appetite Obesity Extreme tantrums
Slide 39
Diabetes Mellitus Slipped Capital Femoral Epiphysis Limited
life expectancy Cardiorespiratory complications Pickwickian
syndrome AKA (Obesity hypoventilation) Skin picking
Slide 40
Slide 41
Severe cognitive deficits Speech impaired or absent
Inappropriate paroxysms of laughter May have ataxia and
seizures
Slide 42
You evaluate a 16-year-old varsity volleyball player. The
girl's height is 71 inches, weight is 125 lb, and blood pressure is
115/74 mm Hg. You note scoliosis and a 3/6 holosystolic murmur
heard at the cardiac apex with radiation to the left axilla Choose
the MOST likely diagnosis A.Ehlers-Danlos B.Infective endocarditis
C.Marfan syndrome D.Rheumatic heart disease E.Williams
syndrome
Slide 43
Slide 44
Avoid contact sports Connective tissue (joint) injury Marfan:
Also avoid any strenuous exercise Aortic dissection
Slide 45
AD- Fibrillin Gene Normal intelligence = upward lens Findings
more obvious with aging
Slide 46
Mostly AD Defect of collagen Fragil velvety skin Cigar Paper
Scar formation Impaired wound healing Use glue or tape
Slide 47
Beals Syndrome Abnormal fibrillin 2 Tall, arachnodactyly Broad
forehead and hypertelorism are distinct features
Slide 48
Homocystinuria Error of methionine metabolism Tall, thin
habitus, scoliosis, pectus Distinctive features: Inferiorly
displaced lens Hypercoaguability Mental retardation Treatment May
respond to B6 (pyridoxine)
Slide 49
Slide 50
Altered or abnormal gene that codes for the production of an
abnormal product Enzyme or cofactor needed for metabolic process
Cannot make end-product Abnormal structure and function Increased
precursors
Slide 51
AR 1/20,000 Abnormal cholesterol biosynthesis Block in the
final step Toxic precursors 7-dehydrocholesterol
Slide 52
Clinical features Pregancy SGA Decreased fetal movement Breech
Abnormal CNS development Microcephaly Prominent occiput Narrow
bifrontal diameter Seizures Hypotonia then hypertonia Irritable
behavior Shrill screaming MR
Slide 53
Facial stigmata Eyelid ptosis Epicanthal folds Strabismus
Low-set or posteriorly rotated ears Broad nasal tip with upturned
nares Micrognathia
Slide 54
Clinical Features Simian crease Syndactyly of 2 nd and 3 rd
toes Hypospadias with cryptorchidism Ambiguous genitalia Less
common Clenched hands Digital abnormalities Cataracts Cleft palate
Bifid uvula
Slide 55
Other Systems Feeding problems Failure to thrive Heart GI
Kidneys Treatment Oral cholesterol Some improvement
Slide 56
A 14 month old female presented with developmental delay to
your clinic. The patient has been pulling to stand but lost this
ability and seems to be regressing in overall development. Late in
infancy, the parents noticed gradual changes in craniofacial
features including prominence of forehead. On exam, you notice
frontal bossing, cloudy cornea, HSM and stiff elbows. The patient
most likely has a disorder within which category of inborn error of
metabolism? A. Lysosomal Storage Disease B. Glycogen Storage
Disease C. Organic Acidemia D. Non Ketotic Hyperglycinemia E.
Galactosemia
Normal ammonia Clinical Differences Galactosemia Cataracts
Hyperbilirubinemia Reducing substances Hypoglycemia Gram negative
sepsis Dx: GALT in RBCs Non Ketotic Hyperglycinemia Encephalopathy
Burst suppression on EEG Difficult to control seizures
Slide 62
Mutation in gene coding for production of lysosomal enzymes
Accumulation of substrate Impairment of cell function >40
different LSD Start in late infancy or early childhood with slowly
progressive symptoms
Mucopolysaccharidoses Cannot break down glycosaminoglycans
Clinical effects Coarsening of facial features Skeletal
abnormailities Dysostosis multiplex Joint structure and function
Organomegaly +/- Cognitive abilities +/- Corneal clouding
Treatment: enzyme replacement or BMT
Slide 65
DiseaseDescriptionInheritance Hurlers (MPS I)+ corneal clouding
+ developmental regression AR Hunters (MPS II)no corneal clouding +
developmental regression X-linked Sanfilippo (MPS III)no corneal
clouding + developmental regression AR Morquiro (MPS IV)+ corneal
clouding * Normal intelligence AR
Slide 66
Sphingolipidoses Developmental regression Organomegaly Cherry
red macula Bone pain Short
Slide 67
DiseaseDescription GaucherHSM, bone pain, easy bruisibility
FabryOrange-colored skin lesions, opacities of the eye, vascular
disease (heart, brain, kidney) KrabbeDemyelination and progressive
neuro deterioration Tay SachsNo HSM, cherry red spot, neuro
deterioration Niemann-PickHSM, cherry red spot
Slide 68
Von Gierke Disease (GSD I) Liver cant produce glucose Features
Hypoglycemia with prolonged fasting Organomegaly Cherubic face Poor
growth Elevated TG and cholesterol Lab findings Elevated lactic and
uric acid Treatment Frequent snacks and meals
Slide 69
Pompe Disease (GSD II) Cannot use muscle glycogen Features
Muscle weakness Muscles are hard Rhabdomyolysis FTT Macroglossia
Cardiomegaly Treatment Enzyme replacement
Slide 70
Slide 71
You suspect that a newborn may have VATER association. You can
tell the parents that all of these findings are common EXCEPT:
A.Vertebral Anomalies B.Anal Atresia C.TE fistula D.Mental
retardation E.Renal Anomalies
Slide 72
CColoboma of retina (or iris) HHeart abnormalities AAtresia of
the choanae RRetarded growth and mental development GGenital
hypoplasia in males EEar anomalies (hearing loss)
Slide 73
Facial Features Wide-spaced, slightly down- slanting palpebral
fissures, anteverted nares, a short philtrum, small dysmorphic ears
Diagnosis 4 of 6 criteria One must be coloboma or choanal atresia
Inheritance - heterogeneous May have clefts and/or renal
abnormalities May have agenesis or aplasia of thymus or
parathyroids Dont confuse with DiGeorge!
Etiology Unknown Normal intelligence Must get a karyotype to
rule out chromosomal disorders Townes-Brocks Similar to VATER
Autosomal Dominant Ear, thumb and anal abnormalities No vertebral
anomalies or TE fistula
Slide 77
Slide 78
Features IUGR FTT Moderate to severe cognitive impairment
Microcephaly Flat occiput Low posterior hairline Facial Features
Long eyelashes, synophrys, small upturned nose with anteverted
nostrils, long philtrum, downturned upper lip with cupids bow shape
and micrognathia Small hands and feet
Slide 79
Features cont... Proximally placed thumbs Flexion contractures
of elbows Hypoplastic limbs Phocomelia Hirsutism Cutis marmorata
Males Hypospadias and cryptorchidism Females Bicornate uterus
Autosomal dominant Most cases are new mutations
Slide 80
What is the most common heart defect seen in patients with
Noonan Syndrome? A. Supravalvular aortic stenosis B. Coarctation of
the aorta C. Pulmonary valvular stenosis D. VSD E. AV canal
Slide 81
Autosomal Dominant Similar to Turner Chromosomal studies may be
beneficial 1/1000 to 1/2500 Males = Females
Slide 82
Features Webbing of neck Sternal abnormalities - pectus
Pulmonic stenosis, hypertrophic cardiomyopathy Coagulation
abnormalities Males Cryptorchidisn
Slide 83
Features Facial features Widely spaced eyes with down-slanting
palpebral fissures, ptosis, retrognathia, low set, posteriorly
rotated ears, coarse, curly hair with low hairline Delayed puberty
Short-stature Normal intelligence
Slide 84
Slide 85
A child exposed to alcohol during pregnancy is most likely to
exhibit which of the following: A. Neural Tube Defect B. Tricuspid
Atresia C. Micropthalmia D. Developmental Delay E. Stippled
epiphyses on x-ray of long bones
Slide 86
No amount of alcohol is safe in pregnancy! Features
Microcephaly Pre and post natal growth deficiency Short palpebral
fissures Long, smooth philtrum Thin upper lip Short nose Hypoplasia
of nails and distal phalanges
Slide 87
Newborns SGA Poor catch up growth Hyper or hypotonia Irritable
or tremulous Older children Thin Hyperactive >80% developmental
delay Fine motor
Slide 88
Phenytoin, phenobarbital, carbamazepine Features Microcephaly
IUGR Facial Features Broad nasal bridge, small anteverted nostrils,
long upper lip Fingernail hypoplasia Heart defects Hypospadias with
cryptorchidism Clubfoot Valproic Acid NTD
















![Computed Tomography of Ocular Colobomas - AJNR · of the absence of overlying uveal tract and retina [1]. We report three cases of ocular colobomas and demonstrate the computed tomographic](https://img.pdfslide.net/doc/110x75/5eadbc3f2d29ab297a0f4307/computed-tomography-of-ocular-colobomas-of-the-absence-of-overlying-uveal-tract.jpg)