Embed Size (px)
Citation preview
EU Fallsfest Bologna February 2016
Professor Finbarr Martin Geriatrician, Guys and St Thomas’ NHS Trust
and King’s College London, UK
Developing a comprehensive national approach for falls and fragility fractures reduction: obstacles, alliances and opportunities
Declarations
I am speaking in personal capacity, but am also • Clinical lead for the England national falls and
fragility fracture audit programme • Non-executive director of NICE (both funded by the England Dept of Health) • No commercial conflicts of interest
Summary
• this is a story of events the facts are true but the explanations are just opinions the are many actors
Policy and guidance
National Service Framework for Older People (Dept Health 2001)
Standard 6 (of 8) “By 2005, all local health systems should have established an integrated service for the prevention of falls and fractures” “ The aim of this standard is to reduce the number of falls resulting in serious injury and ensure effective treatment and rehabilitation for those who have fallen”
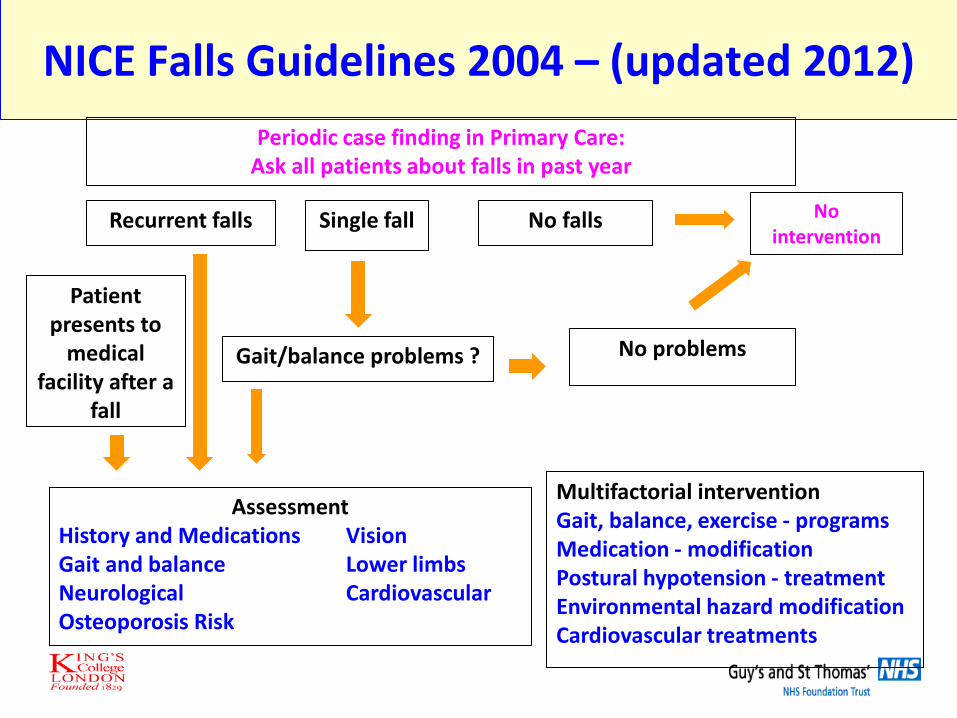
NICE Falls Guidelines 2004 – (updated 2012)
Recurrent falls Single fall No intervention
No falls
Periodic case finding in Primary Care: Ask all patients about falls in past year
Gait/balance problems ? No problems
Patient presents to
medical facility after a
fall
Assessment History and Medications Vision Gait and balance Lower limbs Neurological Cardiovascular Osteoporosis Risk
Multifactorial intervention Gait, balance, exercise - programs Medication - modification Postural hypotension - treatment Environmental hazard modification Cardiovascular treatments
Audit
RCP National Audit 2007
• Organisational audit of policies etc • Individual patient level data on 8826 cases • Patients attending Emergency Departments from 91%
of acute hospitals and local primary care • Non-hip fractures (40 per hospital) of radius, ulna,
humerus, pelvis or vertebra • Hip fractures (20 per hospital) • Followed patients from A&E / MIU • Reviewed falls and bone health secondary prevention
in hospital and community up to 16 weeks
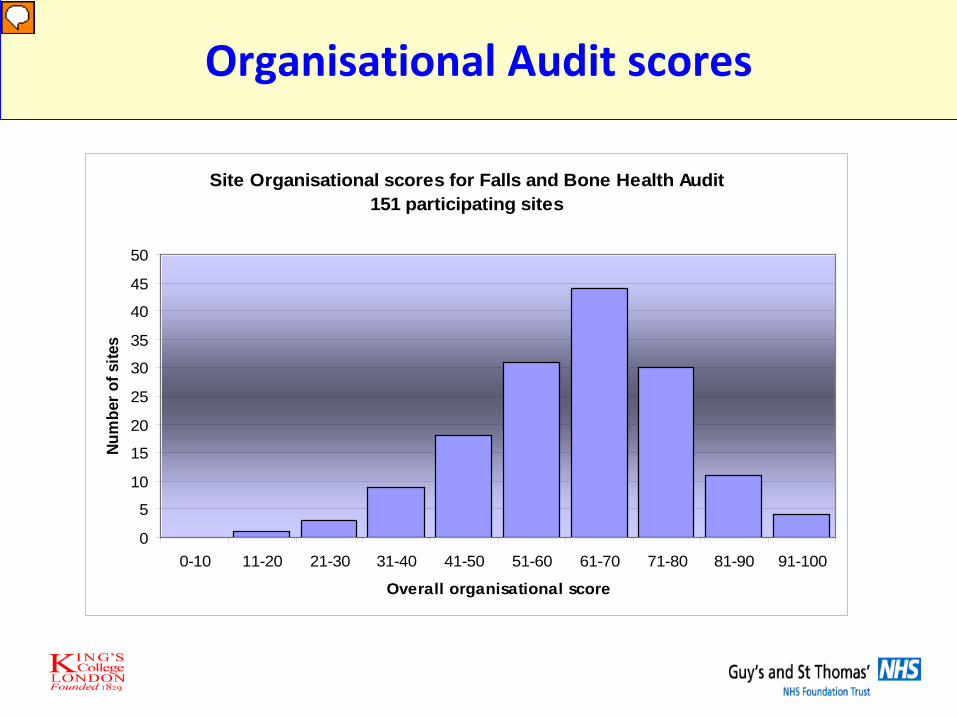
Organisational Audit scores
Site Organisational scores for Falls and Bone Health Audit151 participating sites
0
5
10
15
20
25
30
35
40
45
50
0-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 91-100
Overall organisational score
Num
ber o
f site
s
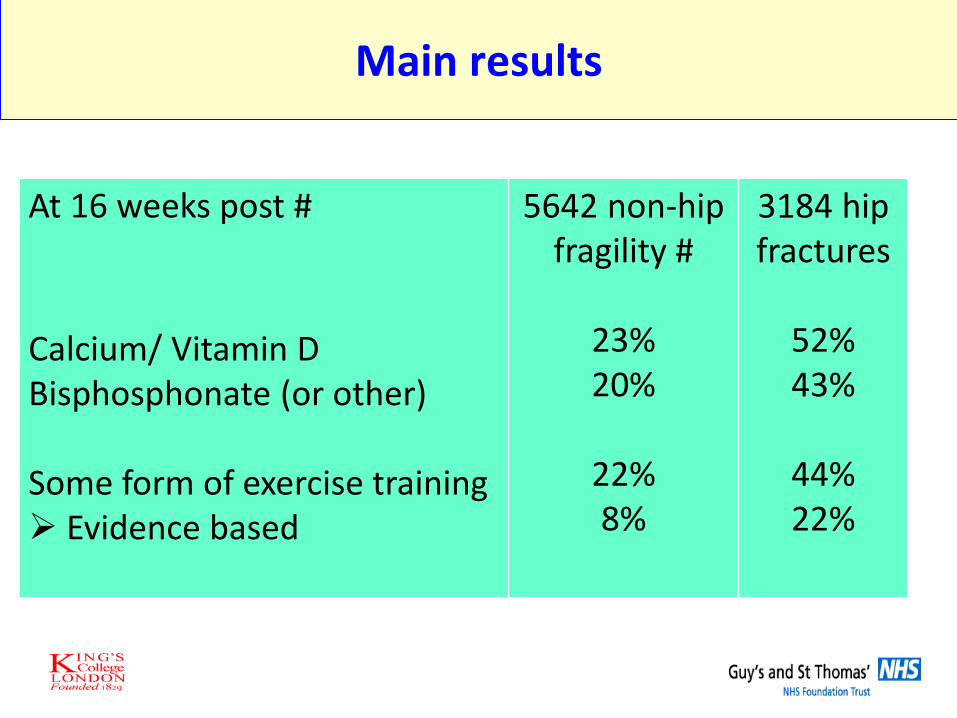
Main results
At 16 weeks post # Calcium/ Vitamin D Bisphosphonate (or other) Some form of exercise training Evidence based
5642 non-hip fragility #
23% 20%
22% 8%
3184 hip fractures
52% 43%
44% 22%
Responses
• Professional • Stakeholders • National policy
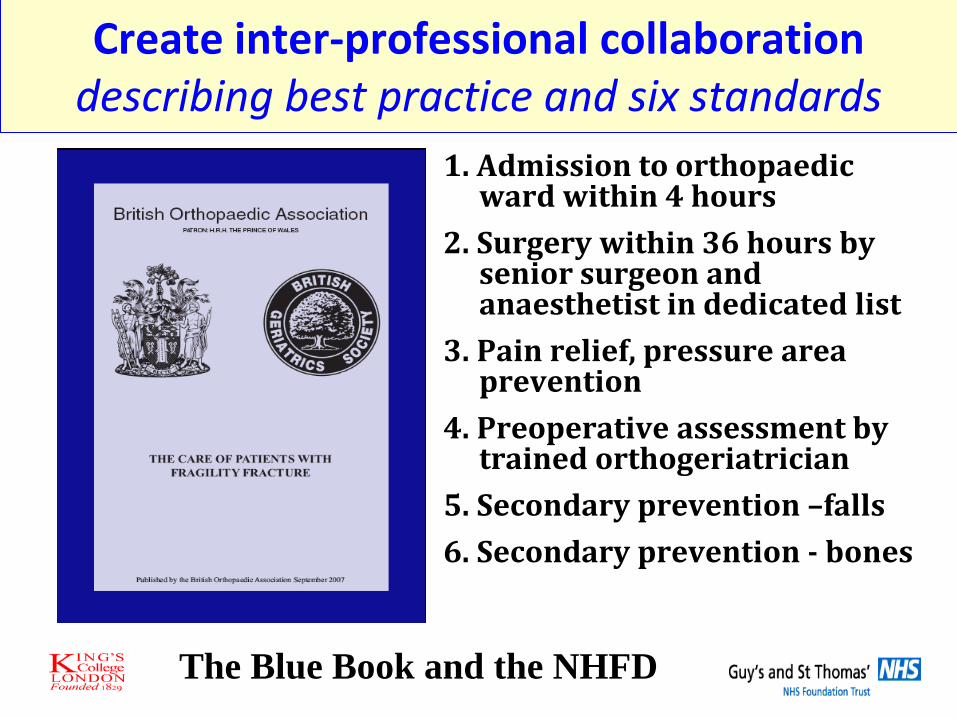
Create inter-professional collaboration describing best practice and six standards
The Blue Book and the NHFD
1. Admission to orthopaedic ward within 4 hours
2. Surgery within 36 hours by senior surgeon and anaesthetist in dedicated list
3. Pain relief, pressure area prevention
4. Preoperative assessment by trained orthogeriatrician
5. Secondary prevention –falls 6. Secondary prevention - bones
Professional peer pressure based on reliable data
Standards to be measured for database
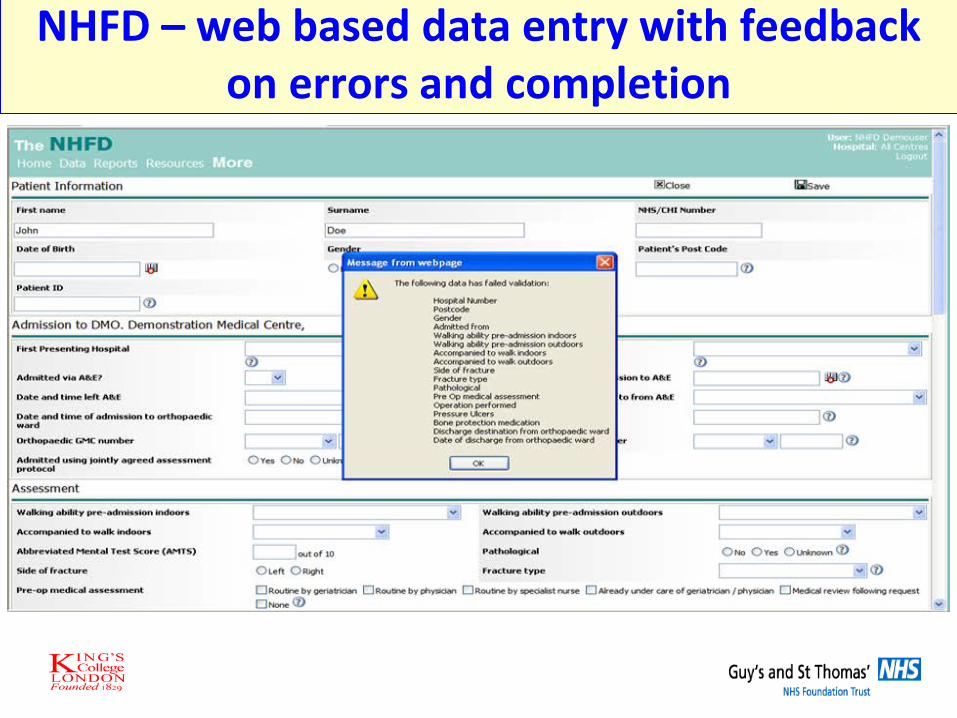
NHFD – web based data entry with feedback on errors and completion
Draft records
Ground-level assets for establishing the NHFD
• Lead clinicians in orthopaedics knew the service needed to improve and wanted to do it
• They believed that managers would respond only to hard data
• Geriatrics involvement in post-op rehabilitation was already established
• A few specialist nurses already existed
Ground-level threats for establishing the NHFD
• Surgeons were wary of a surveillance system that might judge them, leave them open to litigation or create unfair ‘league tables
therefore individual surgeons were not named • Geriatricians were wary of extending their role to
the peri-operative phase without adequate resources
Business case with resource needs on website
NHFD Reports: 2008-2010
Individual reports for 26 hospitals
Analysis on 12,983 records from 64
hospitals
Analysis on 36,556 records from 129
hospitals
2015 – all hospitals and 60,000 cases; total >400,000
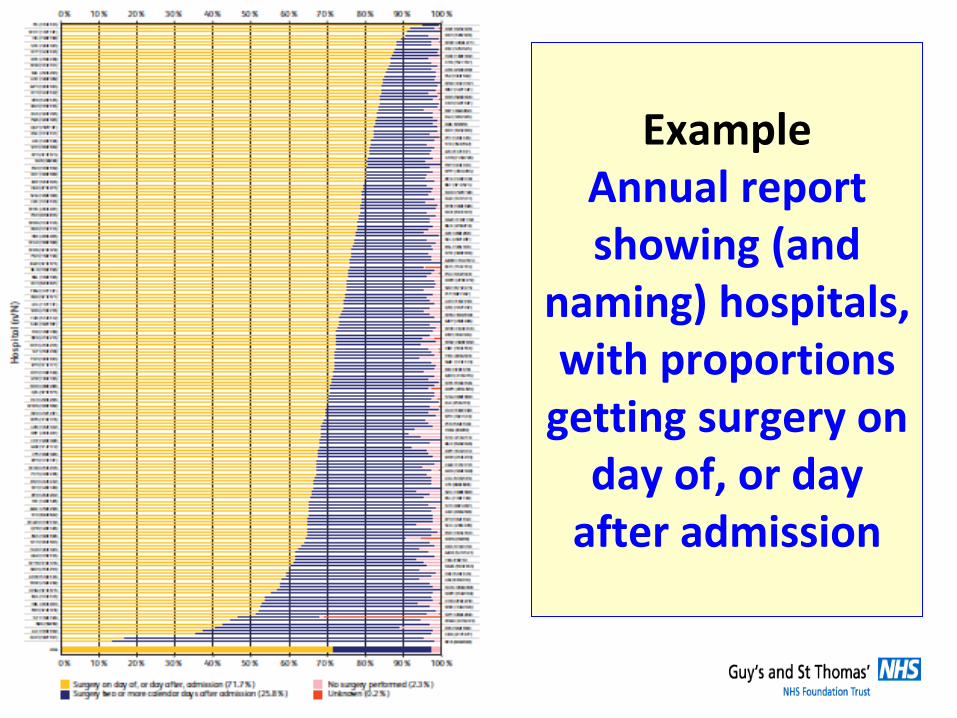
Example Annual report showing (and
naming) hospitals, with proportions
getting surgery on day of, or day
after admission
alliances
plus-..............Advocacy from charities etc
Policy into practice
Simplify and focus
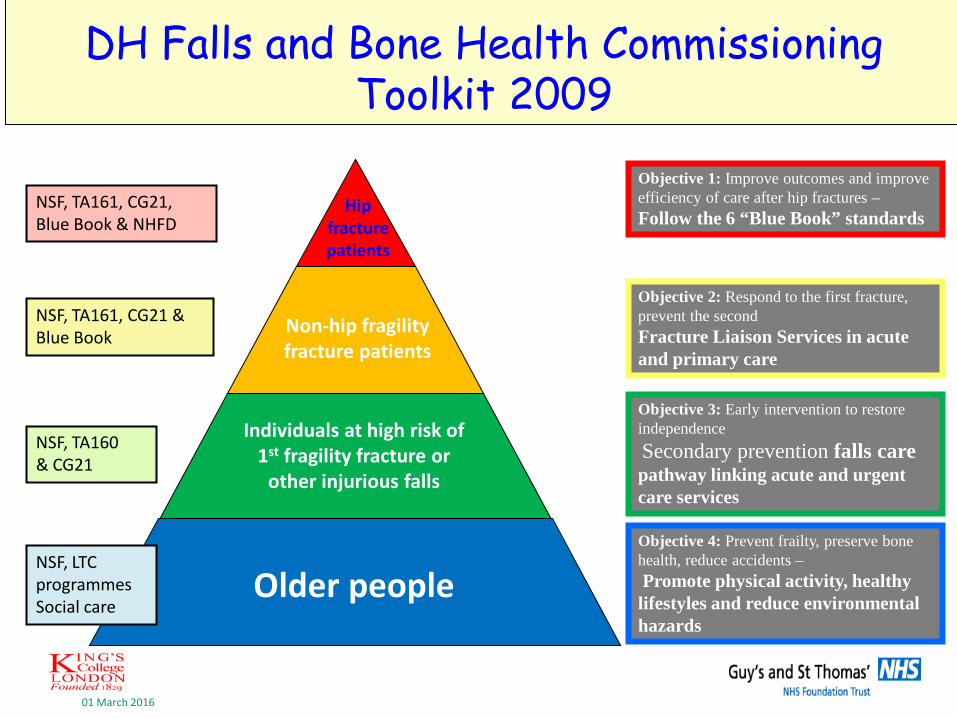
DH Falls and Bone Health Commissioning Toolkit 2009
01 March 2016
Objective 1: Improve outcomes and improve efficiency of care after hip fractures – Follow the 6 “Blue Book” standards Hip
fracture patients
Objective 2: Respond to the first fracture, prevent the second Fracture Liaison Services in acute and primary care
Non-hip fragility fracture patients
Objective 3: Early intervention to restore independence Secondary prevention falls care pathway linking acute and urgent care services
Individuals at high risk of 1st fragility fracture or
other injurious falls
Objective 4: Prevent frailty, preserve bone health, reduce accidents – Promote physical activity, healthy lifestyles and reduce environmental hazards
Older people
NSF, TA161, CG21, Blue Book & NHFD
NSF, TA161, CG21 & Blue Book
NSF, TA160
& CG21
NSF, LTC programmes Social care
Dept Health falls and bone health commissioning toolkit 2009
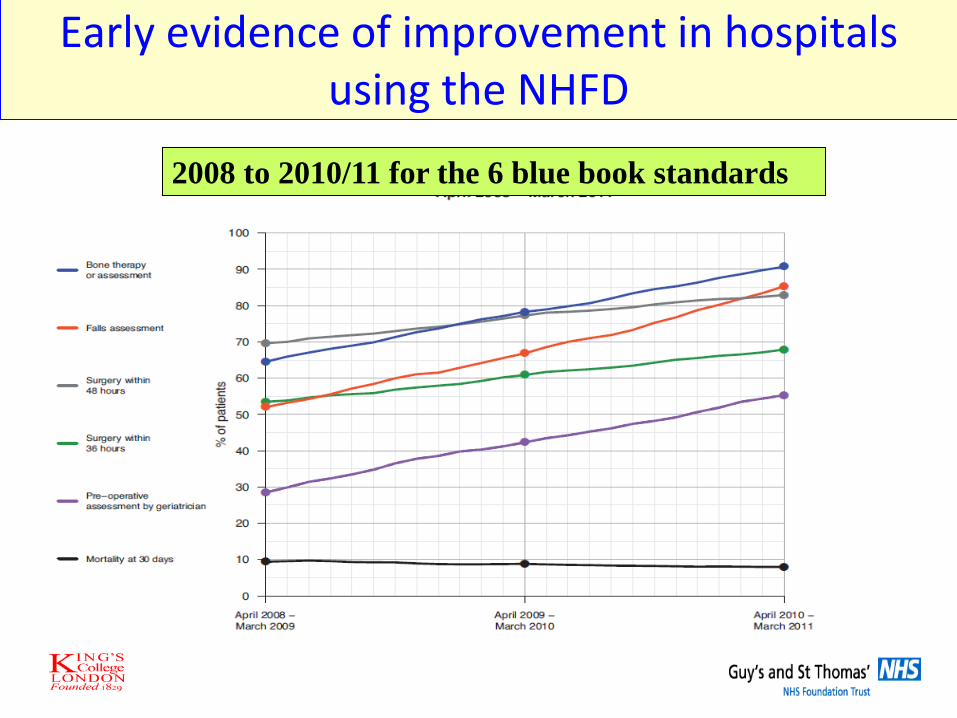
Early evidence of improvement in hospitals using the NHFD
2008 to 2010/11 for the 6 blue book standards

Incentives to spread participation
Best Practice Tariff of standards with reliable data about relevant issues
• Time to surgery (<36 hours)
• Involvement of geriatrician and anaesthetists
• Fracture prevention (falls and bones)
• Cognitive assessment at admission and discharge
28
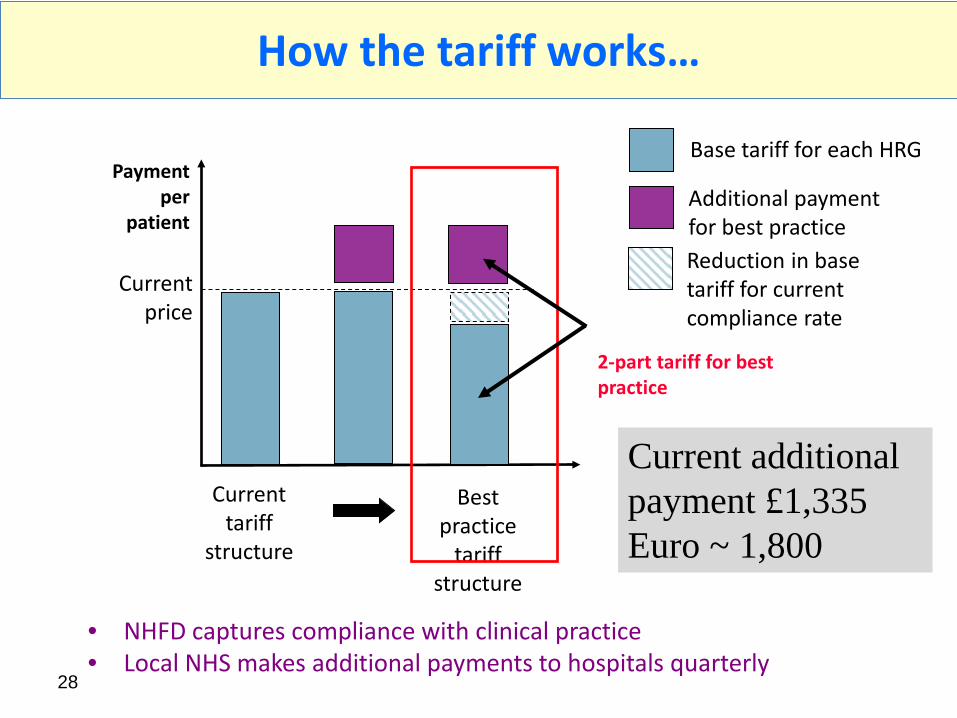
How the tariff works…
• NHFD captures compliance with clinical practice • Local NHS makes additional payments to hospitals quarterly
Base tariff for each HRG
Additional payment for best practice Reduction in base tariff for current compliance rate
Payment per
patient
Current tariff
structure
Best practice
tariff structure
2-part tariff for best practice
Current price
Current additional payment £1,335 Euro ~ 1,800
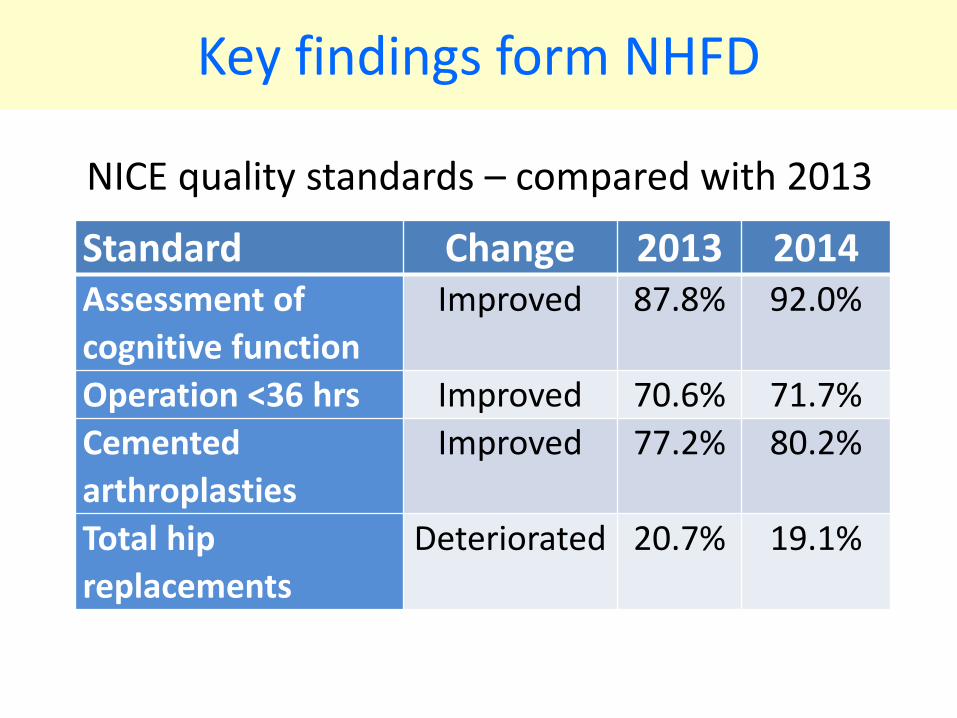
Key findings form NHFD
NICE quality standards – compared with 2013 Standard Change 2013 2014
Assessment of cognitive function
Improved 87.8% 92.0%
Operation <36 hrs Improved 70.6% 71.7% Cemented arthroplasties
Improved 77.2% 80.2%
Total hip replacements
Deteriorated 20.7% 19.1%
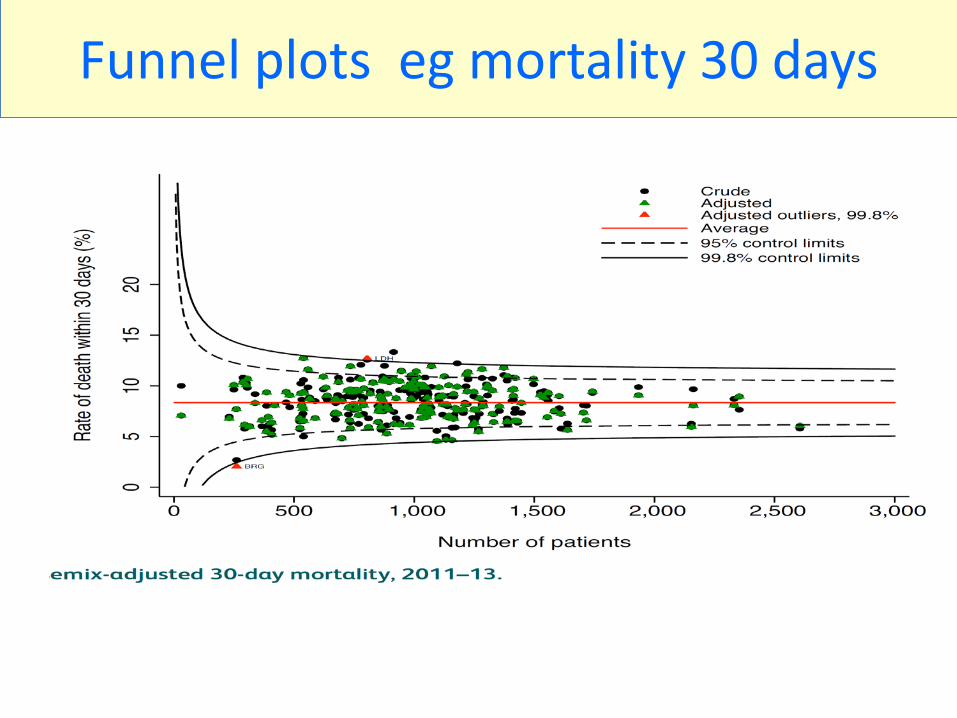
Funnel plots eg mortality 30 days
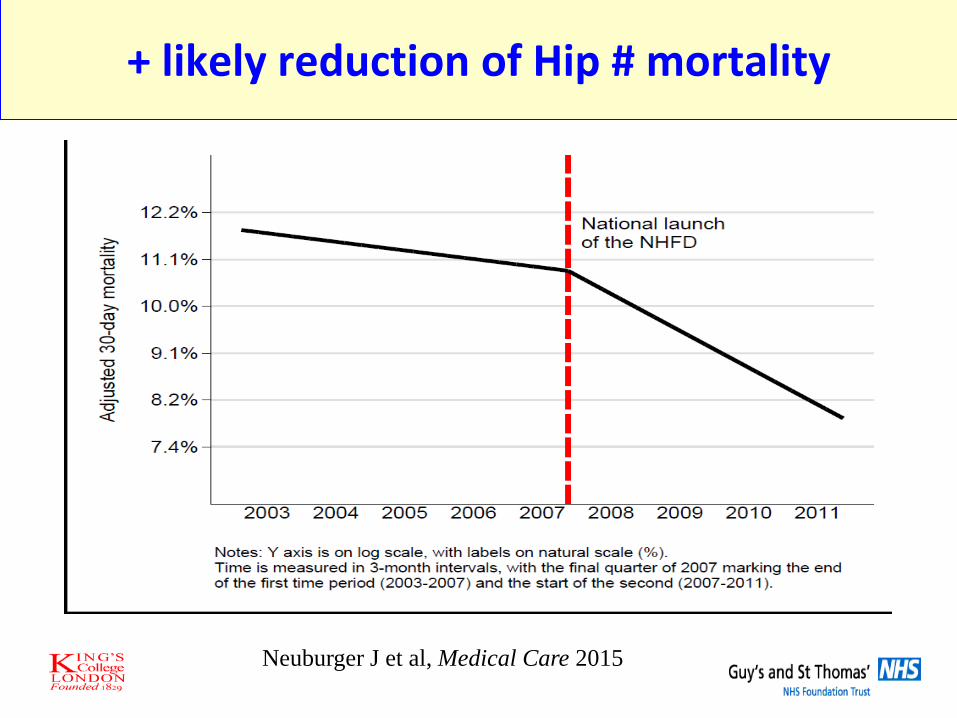
+ likely reduction of Hip # mortality
Neuburger J et al, Medical Care 2015
Direct feedback for patients
2014 audit data arranged around key questions that focus groups have identified
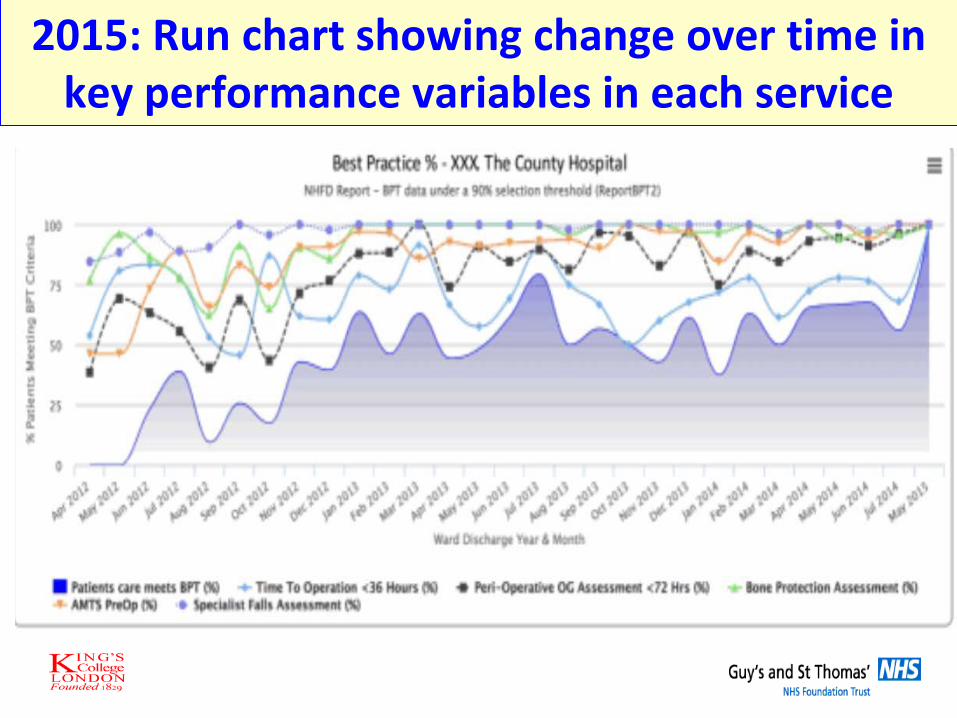
2015: Run chart showing change over time in key performance variables in each service
What about secondary falls and fractures prevention?
IN CONTRAST Incentive in GP Contract 2012
• All patients with fragility fracture on a register • All over 75 with fragility fracture on secondary
prevention treatment and Calcium/Vit D unless justifiable exemption
• Under 75s with previous fracture or at risk of osteoporosis to have investigation and assessment of bone fragility
• With appropriate treatment commenced if osteoporosis proven
ineffective
RCP Falls and Bone Health Audit 2011 (compared to 2008)
2014 – fracture liaison services database
• ~ 35% hospitals participated • large variation in staffing and scope • indicators of what works • funding to continue till 2018
2015 data

Supported by a Falls and Fractures Alliance and Implementation Champions
What about community falls work?
• We have no reliable data on process or outcomes • We have 4000 postural stability instructors trained • We have large variation in service approaches
Why so difficult?
•The NICE guidance is not easy to operationalise in a quantitative way • Ownership is diffuse • Regard for evidence is variable
Possible ways forward
• Focus on community frailty interventions • Promote all types of physical activity and exercise programmes – (don’t mention falls!)
In hospital falls
•2015 National audit programme: 100% participation • Now built into regulator assessments of acute hospitals (CQC) MD falls group 85% Discuss falls rates/1000 OBDs 79% Vision assessment within 3days 43% Ax for Orthostatic hypotension 16% Delirium assessment 36% Mobility aids nearby 68%
But what should be done to improve things?
• RCT evidence for inpatient falls reduction is mixed, despite some definite successes • Implementation is contextual • Quality improvement approaches incorporating falls and other issues may be more effective than refining a universal package
What has helped promote change?
• Evidence helps • Policy and top down pressure alone cannot do it • Inter-specialty collaboration and peer pressure • Reliable clinical performance data • Stakeholder pressure and assistance • Financial incentives don’t work alone
Acknowledgements
• Rikshoft – the original Sweden hip audit • BGS and BOA as partners • Dave Marsh as founder leader of NHFD • Blue Book Authorship Group • NOS and AgeUK –stakeholder partners • DH – for policy • FFFAP programme Board and advisory groups • Royal College of Physicians of London – for managing
the audits • AHPs and patients for partnerships




























