Embed Size (px)
Citation preview

Bone case scenarios
Rasha Odeh

Serum Ca:
45% is present in physiologically active ionized Calcium (Ca++)
40% is bound to albumin (ca : albumin 0.8:1)15% circulates as complexes with other molecules
(such as citrate and sulphate)
Serum Calcium concentration is influenced by:
• Intestinal Ca ++ absorption
• Ca deposition in bone & mobilization of Ca following bone
resorption
• Renal tubular Ca reabsorption

• Parathyroid hormone (PTH) – increases reabsorption of calcium and excretion of phosphorus from
distal tubules
– During hypocalcemia, mobilizes calcium from bone through stimulating osteoclast activity
– Enhances 1hydroxylase activity and calcitriol production in proximal tubules
– Bicarb and aminoacid excretion.
• 1,25(OH)2D (vitamin D) – accelerates calcium absorption from the intestine and stimulates bone
resorption
• Calcitonin– inhibits osteoclastic bone resorption stimulated by PTH
Which hormones regulate calcium homeostasis?

Primary function of PTH prevent hypocalcemia
Within minutes changes in PTH
increasing Ca abs & P exc.
Osteoclastic bone resorption
Over a period of 1-2 days,by stimulating synthesis of
1,25(OH)2D3
increase intestinal Ca abs

CaSR
PTHR1
Gs,
PTH
Serum Ca++
Par
ath
yro
id
glan
d
Target organs•Kidney
•Bone
Hypocalcemia Hypercalcemia
Autosomal dominant hypocalcemia (CaSR activating mutation)
Famil benign Hypocalciu/ hypercalcemia
(CaSR inactivating mutation)
Hypoparathyroidism(XLR,AR)•Di George Syndrome•SYNDROMES(Sanjad Sakati)•APECED Syndrome / mitochondrial•Infiltrative disease (thalasemia)•Parathyroid surgery
Hyperparathyroidism
•MEN-1, MEN 2a
•Sporadic parathyroid adenomas
•Tertiary hyperparathyroidism
Blomstrand’s chondrodysplasia(inactivating mutation)
Jansen disease
Pseudohypoparathyroidism•Type Ia•Type Ib•Type Ic•Type II
McCune–Albright syndrome
Chronic renal failure Hypophosphatasia
Modified from Allgrove J. In: Brook CGD, Clinical Pediatric Endocrinology, 5th edn. Oxford:
AR, AD familial isolated hypopa Sporadic parathyroid tumors

Stage Ca P Alk P PTH Events
Stage 1 N to
Low
N N to
high
N to
high
Poor Ca absorption from
gut
Stage 2 N Low High High Secondary hyperPTH, bone
loss
Stage 3 Low Very
low
Very
high
Very
high
Ca stores depleted, severe
hypocalcemia, seizures
Biochemical Stages of Nutritional Rickets

Case 1
• Ca 6.8 mg/dL
• P 7.6 mg/dL
• Mg 3.7 mg/dl
• ALP 333 U/L
• PTH 4 pg/mL (low)
• Albumin 3.7 mg/dl
• 25 (OH)D 55 ng/ml

How to approach
• Low calcium
• High phosphate
• ?? MG and albumin
• KFT
• Vit D
• PTH level
• Cause

Answer
• Primary hypoparathyroidism due to SanjadSakati Syndrome

3 year old with delayed walking and bowing of lower limbs
• Ca 6.5 mg/dL
• P 2.3 mg/dL
• Mg 2.5 mg/dl
• ALP 720 U/L
• PTH 500 pg/mL.high
• Albumin 3.7 mg/dl
• 25 (OH)D 3 ng/ml

Answer
• (nutritional) rickets

• Ca 6.5 mg/dL
• P 7 mg/dL
• Mg 2.5 mg/dl
• ALP 220 U/L
• PTH 500 pg/mL (high)
• Albumin 3.7 mg/dl
• 25 (OH)D 38 ng/ml

AHO Phenotypic features
• Syndromes are associated with specific dysmorphic features
• Round face• Short neck• Short stature
• Shortened fourth metacarpal & metatarsal

Answer
• Pseudohypoparathyroidism, type 1a or 1c

Case presentation:
8month old female baby presented with:
• poor appetite
• decreased activity
• Preference of water over milk
• Polyurea and polydipsia
• symptoms increased in severity in the last 2months
• Incidental finding of hypercalcemia
• (ca=16.5 mg/dl)

• Vaccination up to age
• Day care attendance
• not on medication nor supplemental vitamins
• Feeding regular formula
• Bowel motion once daily
• First alive baby In the family(first trimester abortion and 2ed baby was IUFD)
• parents are cousins
• Mother had celiac and protein c deficiency

P/E:
• V/S :
HR 126 RR 35 BP90\50
• Growth parameter
HT 65 10th centile WT 6.8 kg 10th centile
• Sunken eyes, dry lips
• GAEB with normal heart sounds
• Soft lax abdomen
• No organomegally

Routine Labs:platlymphneutwbcrdwmcvhtchb
27770.720.79.1115.283.733.611.3
Alka.pho
rbsmgcaclphosBUNcrkna
82921.6819.51085.643.60.434.7141
LDHastAltalbumT.prot
402.831144.16.4

problem list:
1.Hypercalcemia
2.Dehydration

Management
1.correct dehydration with 7%
2.treat hypercalcemia with hydration and furosamide
3.strict urin output u.o=5-8ml\kg\hr
4.look for causes
5.complications of hypercalcemia
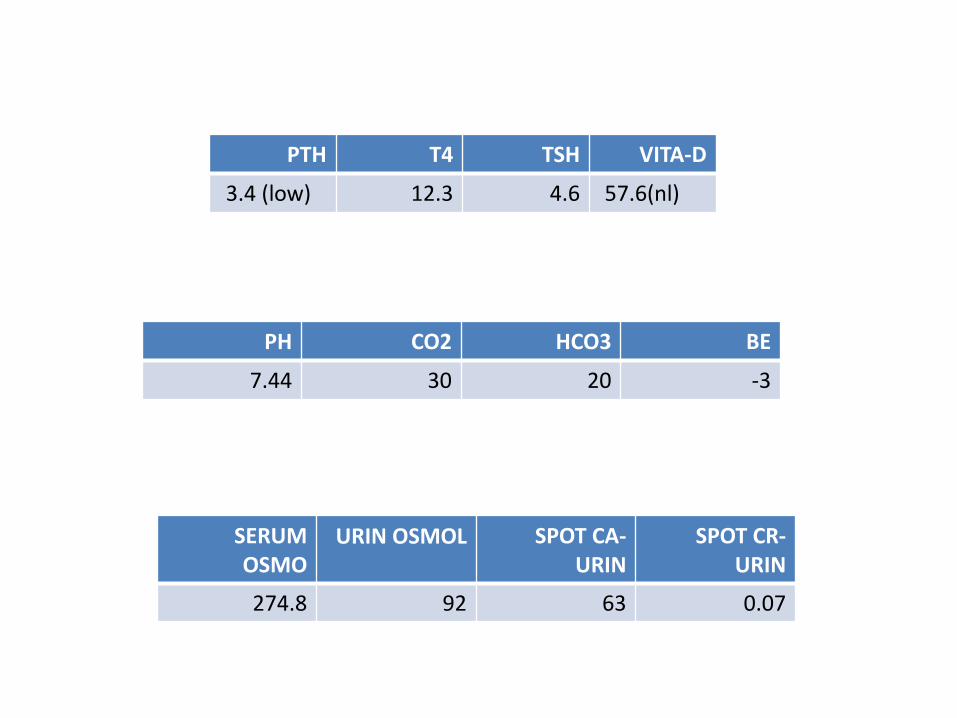
VITA-DTSHT4PTH
57.6(nl)4.612.33.4 (low)
SPOT CR-URIN
SPOT CA-URIN
URIN OSMOLSERUM OSMO
0.076392274.8
BEHCO3CO2PH
-320307.44

• Hypercalcemia NOT due to vit D intoxication or hyperparathyroidism
• No evidence for granulomatous disease
• No evidence of malignancy


• The hypercalcemia was due to the fact that the patient has Williams syndrome
• Hypercalcemia can occur in these patients and it usually is transient and mild, but can also be severe as in this patient.

Thank you