Embed Size (px)
Citation preview
Prof M A Khan FCPS, FRCP.
Professor of BMT
BMT unit, Dept of Hematology
DMCH
Bone Marrow Transplantation in Bangladesh: our experience
CONFLICT OF INTEREST
I have no conflict of interest to declare.
29-Aug-2019
2

TOP STORIES
• Importance of bone marrow transplant
• Background history of BMT at DMCH
• Stem cell Transplant activity of Bangladesh
• Overall status of ASCT
• Complications of Autologous stem cell transplant
• Future goal
• Achievement
3
29-Aug-2019
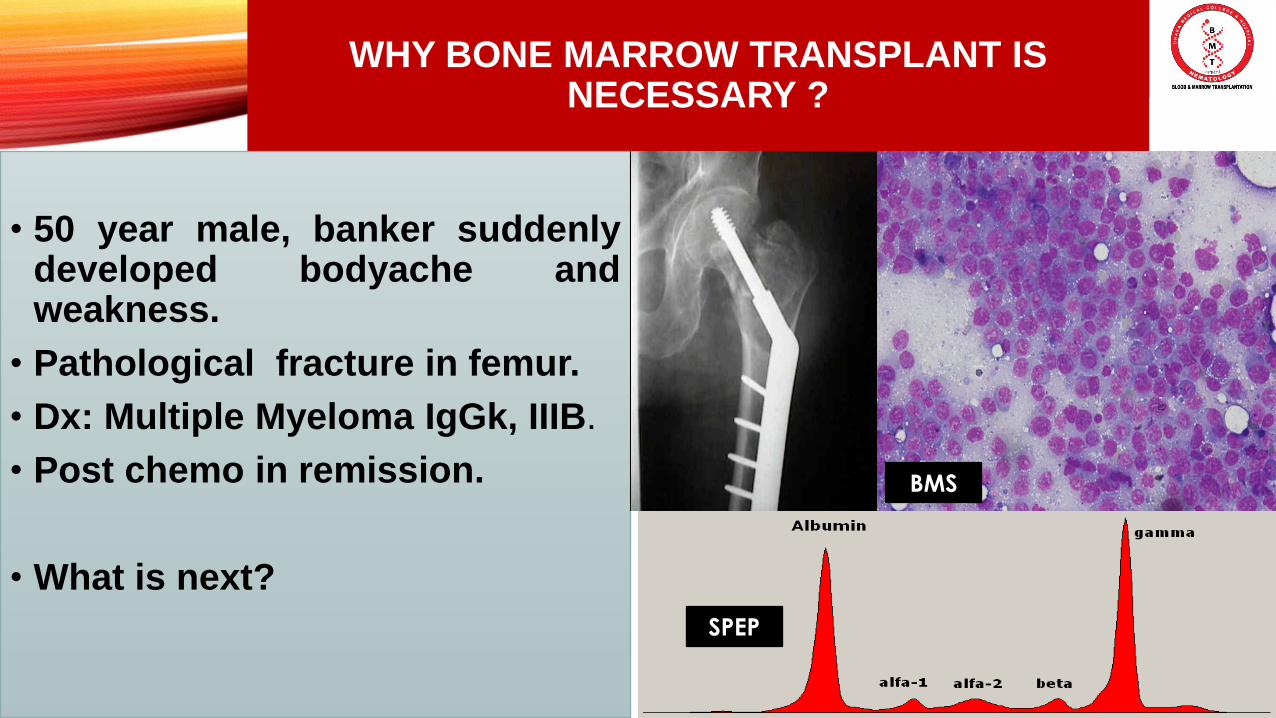
WHY BONE MARROW TRANSPLANT IS NECESSARY ?
• 50 year male, banker suddenlydeveloped bodyache andweakness.
• Pathological fracture in femur.
• Dx: Multiple Myeloma IgGk, IIIB.
• Post chemo in remission.
• What is next?
29-Aug-2019
4
BMS
SPEP
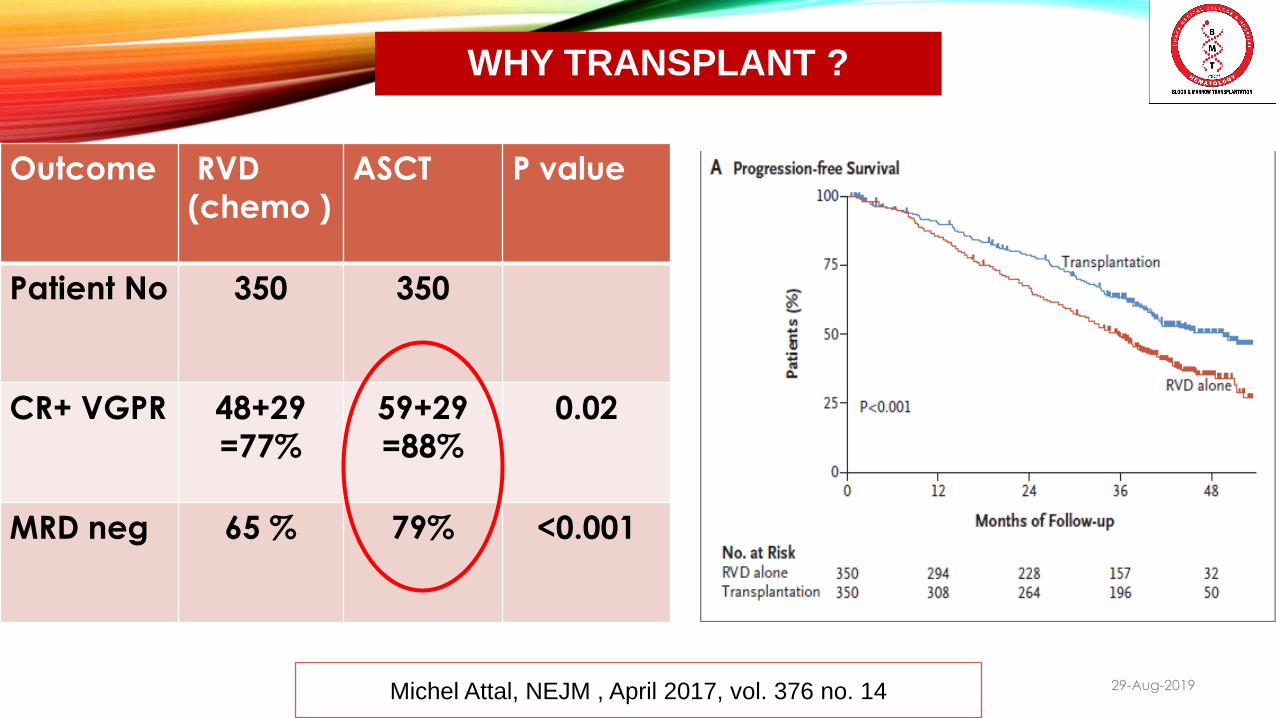
WHY TRANSPLANT ?
29-Aug-2019
5
Michel Attal, NEJM , April 2017, vol. 376 no. 14
Outcome RVD
(chemo )
ASCT P value
Patient No 350 350
CR+ VGPR 48+29
=77%
59+29
=88%
0.02
MRD neg 65 % 79% <0.001
CASE HISTORY
• 18 Y boy, DLBCL, IIIB> CHOPx6 >relapsed after 1 yr.
• 28 Y male of HodgkinsLymphoma, IIIB, Rx : ABVD x6> end of therapy PET scanwas still positive for significantactive disease> Refractory HL.
29-Aug-2019
6
What should be next approach?
TRANSPLANT VS CHEMO IN RELAPSED LYMPHOMA
29-Aug-2019
7
5 Y EFS 46% in Transplanted
Vs
12 % in chemo alone.
Autologous Stem cell transplant is the standard ofcare in relapsed chemosensitive NHL as well as rHD.
29-Aug-2019
8
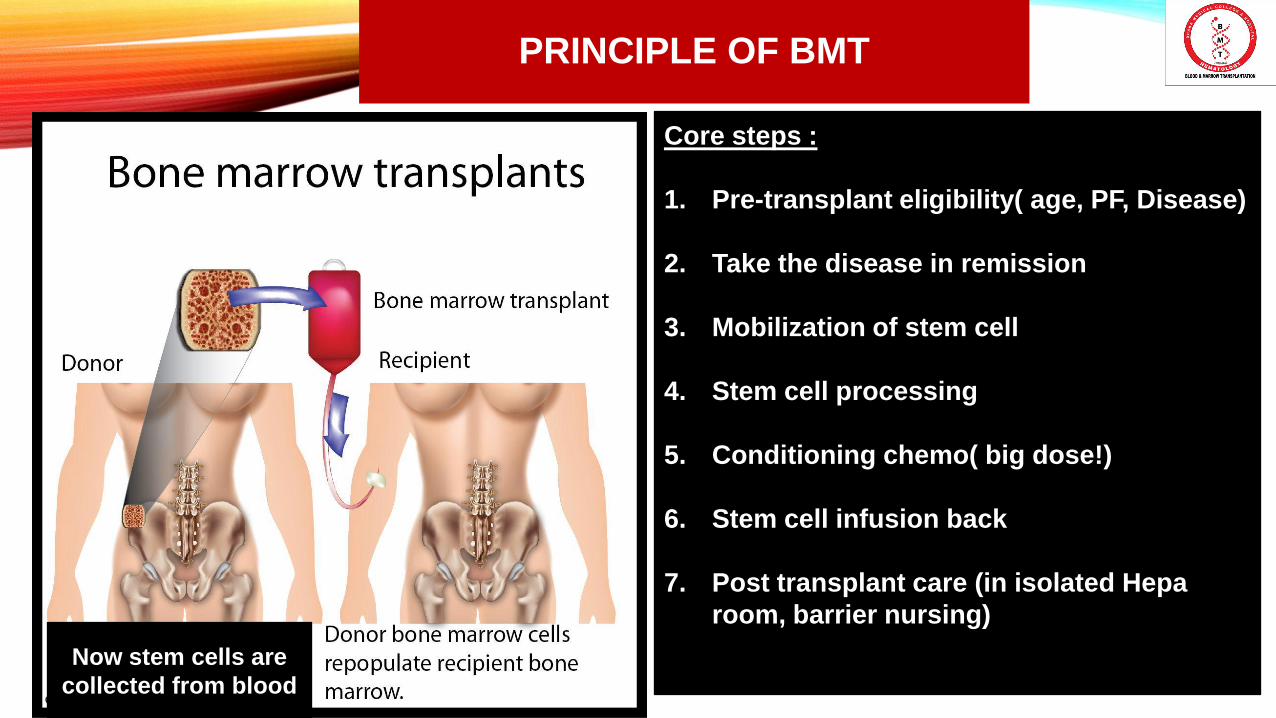
PRINCIPLE OF BMT
29-Aug-2019
9
Core steps :
1. Pre-transplant eligibility( age, PF, Disease)
2. Take the disease in remission
3. Mobilization of stem cell
4. Stem cell processing
5. Conditioning chemo( big dose!)
6. Stem cell infusion back
7. Post transplant care (in isolated Hepa
room, barrier nursing)
Now stem cells are
collected from blood
29-Aug-2019
10FATHER OF BONE MARROW TRANSPLANT
(Left )Edward Donnall Thomas (1920-2012) , the noble laureate in 1990 for
Stem cell transplantation.
29-Aug-2019
11ANCIENT BONE MARROW TRANSPLANT
First BMT Team of Dr Thomas
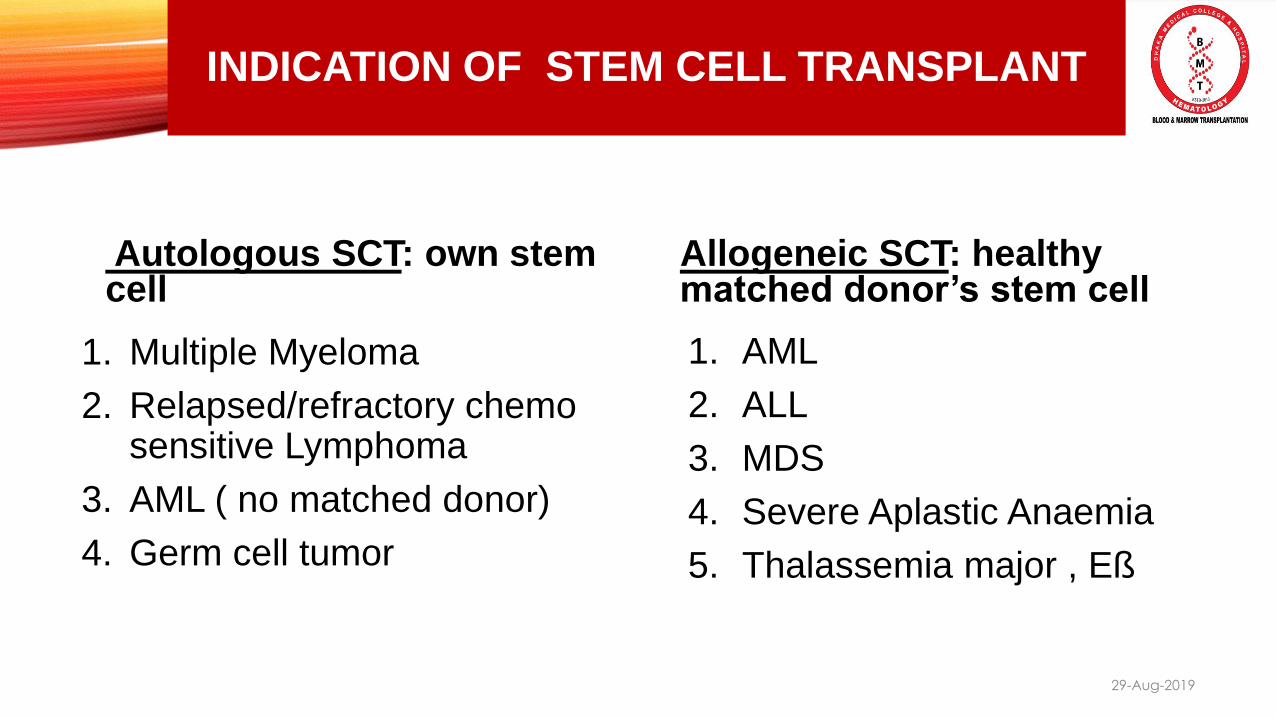
INDICATION OF STEM CELL TRANSPLANT
Autologous SCT: own stem cell
Allogeneic SCT: healthy matched donor’s stem cell
29-Aug-2019
12
1. Multiple Myeloma
2. Relapsed/refractory chemo sensitive Lymphoma
3. AML ( no matched donor)
4. Germ cell tumor
1. AML
2. ALL
3. MDS
4. Severe Aplastic Anaemia
5. Thalassemia major , Eß

DREAM OF BMT STARTED ON 2007 WITH MAKING INTERNATIONAL COLLABORATION
29-Aug-2019
13
2007 Saudi Team visited DMCH Prof Mamen Chandy, Prof Najmul
Ahsan, Prof Khan, Prof Deen Md. 2010: Prof Taher Pakistan
•2011 : Prof Khan to Vietnam
As a speaker on ‘BMT in emerging
countries ‘
•Project proposal rejected many
times.
29-Aug-2019
14
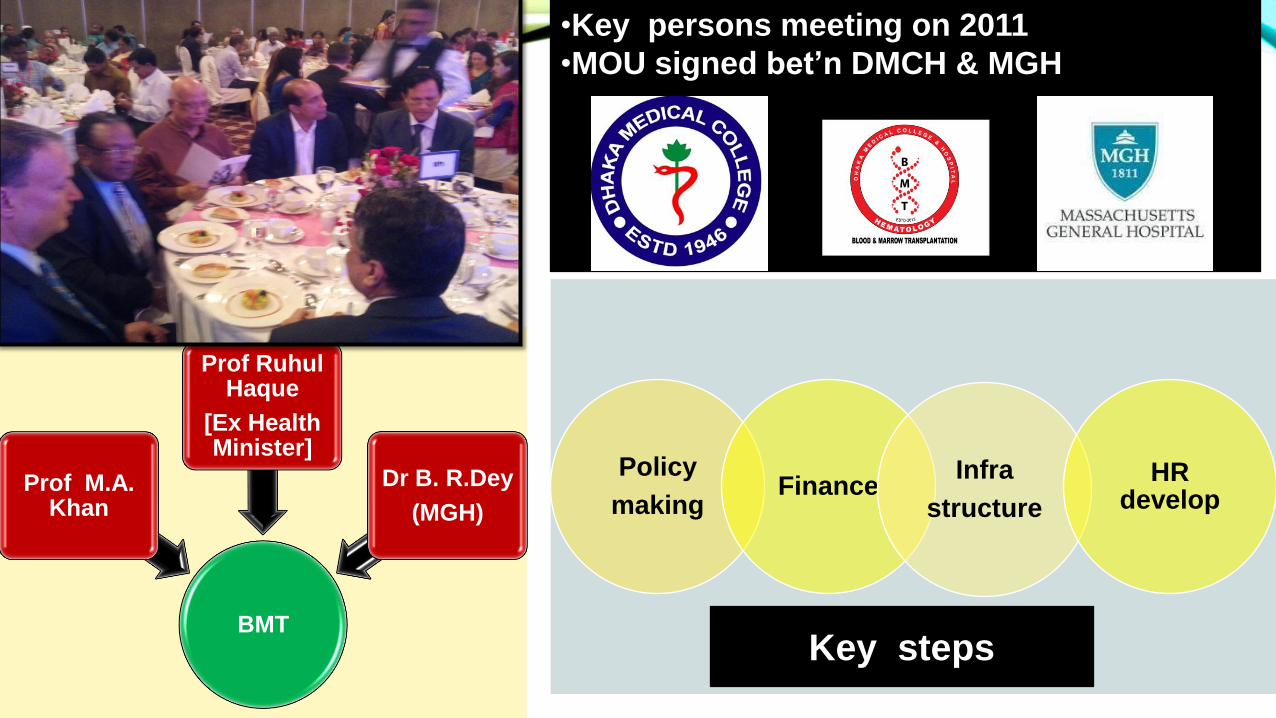
BMT
Prof M.A. Khan
Prof RuhulHaque
[Ex Health Minister]
Dr B. R.Dey
(MGH)
Policy
makingFinance
Infra
structure
HR develop
•Key persons meeting on 2011
•MOU signed bet’n DMCH & MGH
Key steps

INFRASTRUCTURE DEVELOPMENT
2012: site visit by MGH team 2012: work monitoring
29-Aug-2019
15
DMCH – 2 building BMT Unit at top floor
29-Aug-2019
16

Nurses Training Lab training
29-Aug-2019
17

Prof Ruhul Haq’s Visit
Decoration time
29-Aug-2019
18
Inauguration on 2013
WHAT’S MISSING?
Stem cell lab
29-Aug-2019
19
Third Party Inspection

HISTORY BEGINS HERE !
First ASCT on 10th March 2014 Press meeting
29-Aug-2019
20
36 ASCT by BMT Team >80 Stem cell apheresis
21
29-Aug-2019
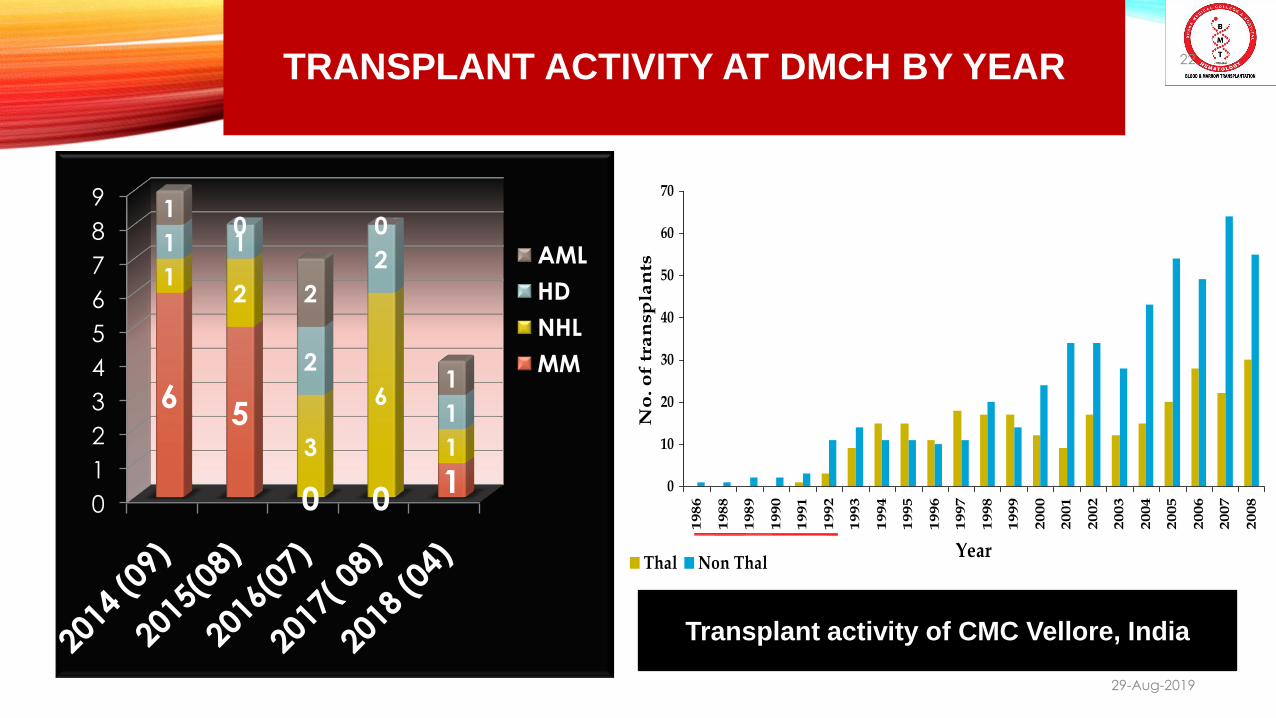
TRANSPLANT ACTIVITY AT DMCH BY YEAR
0
1
2
3
4
5
6
7
8
9
65
0 01
12
3
6
1
1 1
2
2
1
10
2
0
1
AML
HD
NHL
MM
22
29-Aug-2019
0
10
20
30
40
50
60
70
1986
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Year
No
. o
f tr
an
sp
lan
ts
Thal Non Thal
Transplant activity of CMC Vellore, India
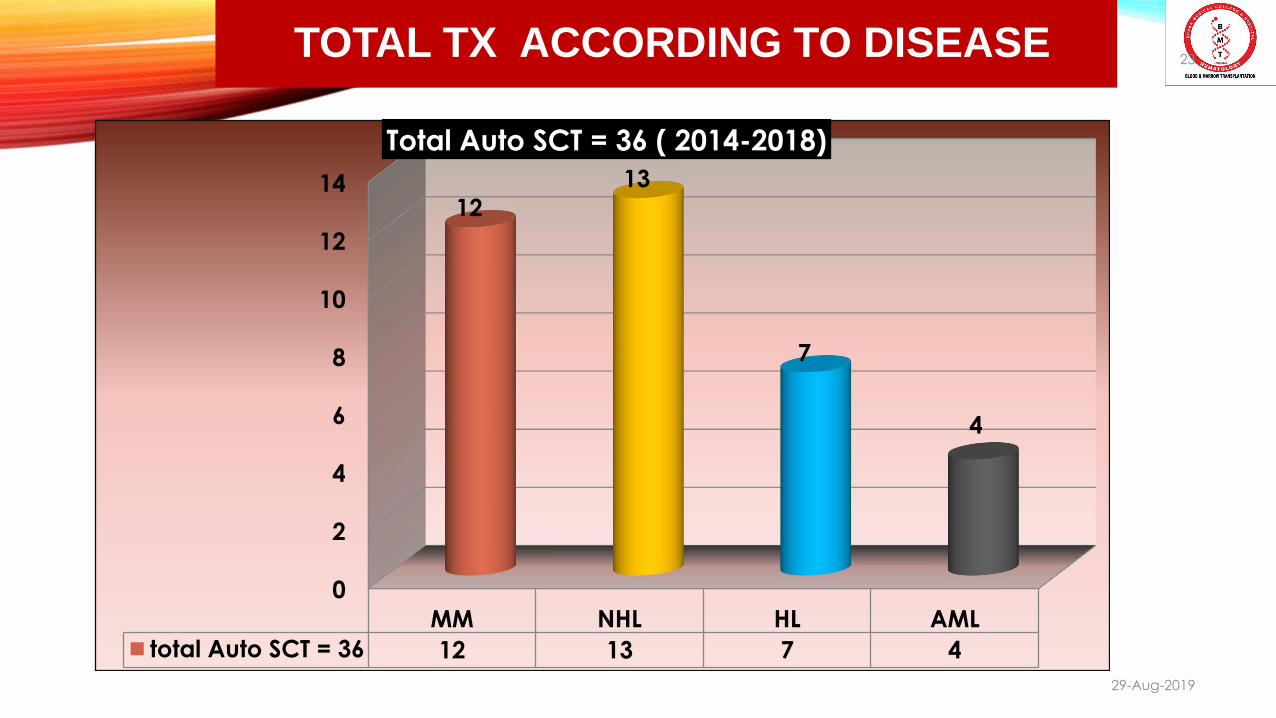
TOTAL TX ACCORDING TO DISEASE
0
2
4
6
8
10
12
14
MM NHL HL AML
total Auto SCT = 36 12 13 7 4
12
13
7
4
Total Auto SCT = 36 ( 2014-2018)
23
29-Aug-2019
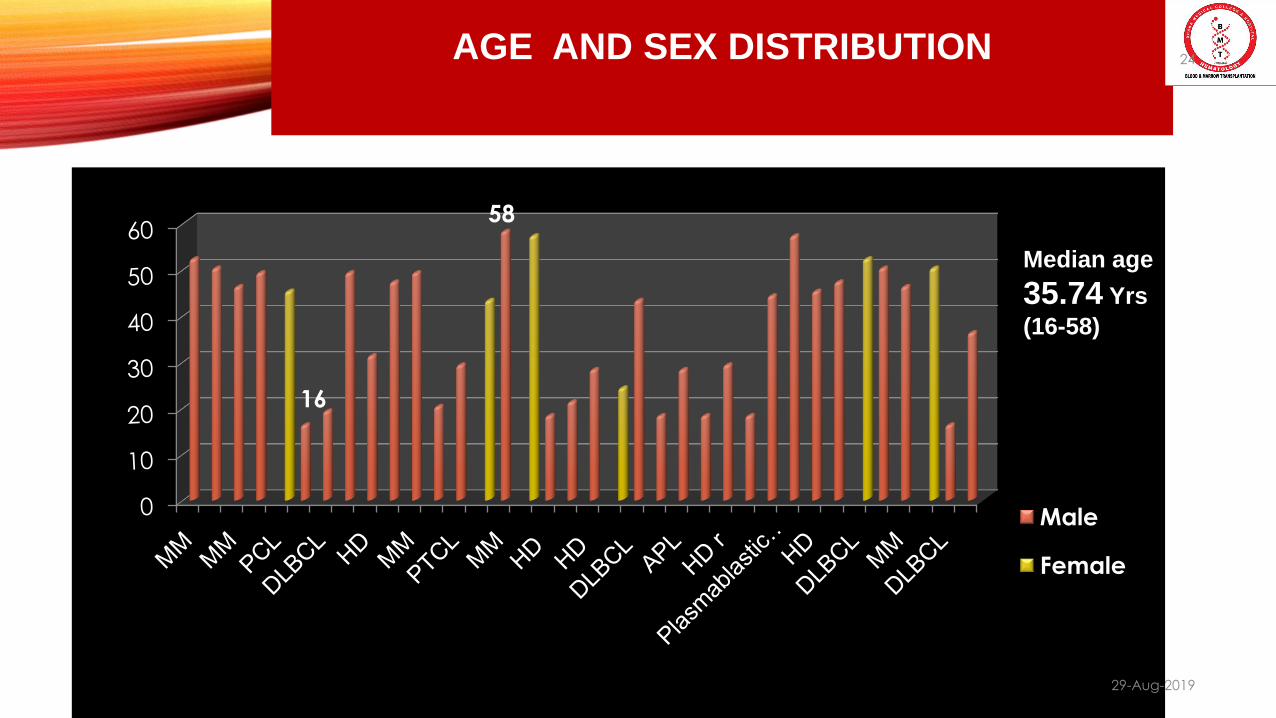
AGE AND SEX DISTRIBUTION
16
58
Male
Female
Median age
35.74 Yrs
(16-58)
24
29-Aug-2019
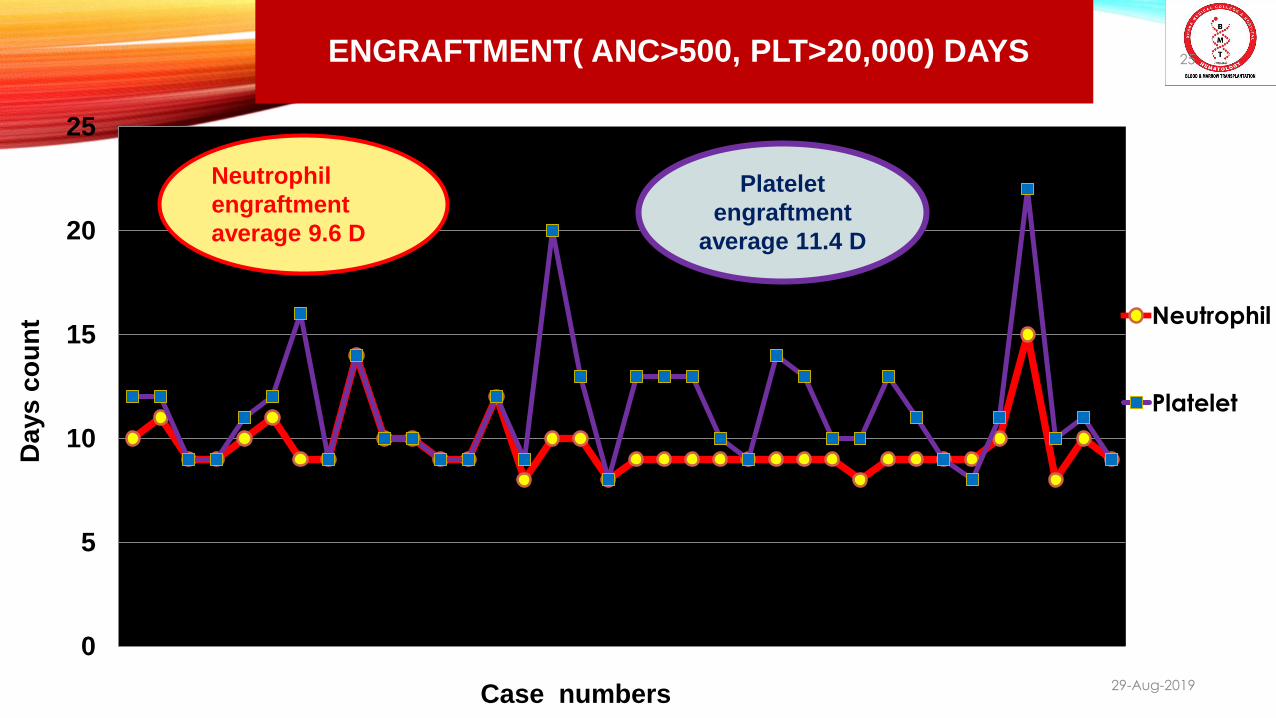
ENGRAFTMENT( ANC>500, PLT>20,000) DAYS
0
5
10
15
20
25
Da
ys
co
un
t Neutrophil
Platelet
Case numbers
Neutrophil
engraftment
average 9.6 D
Platelet
engraftment
average 11.4 D
25
29-Aug-2019
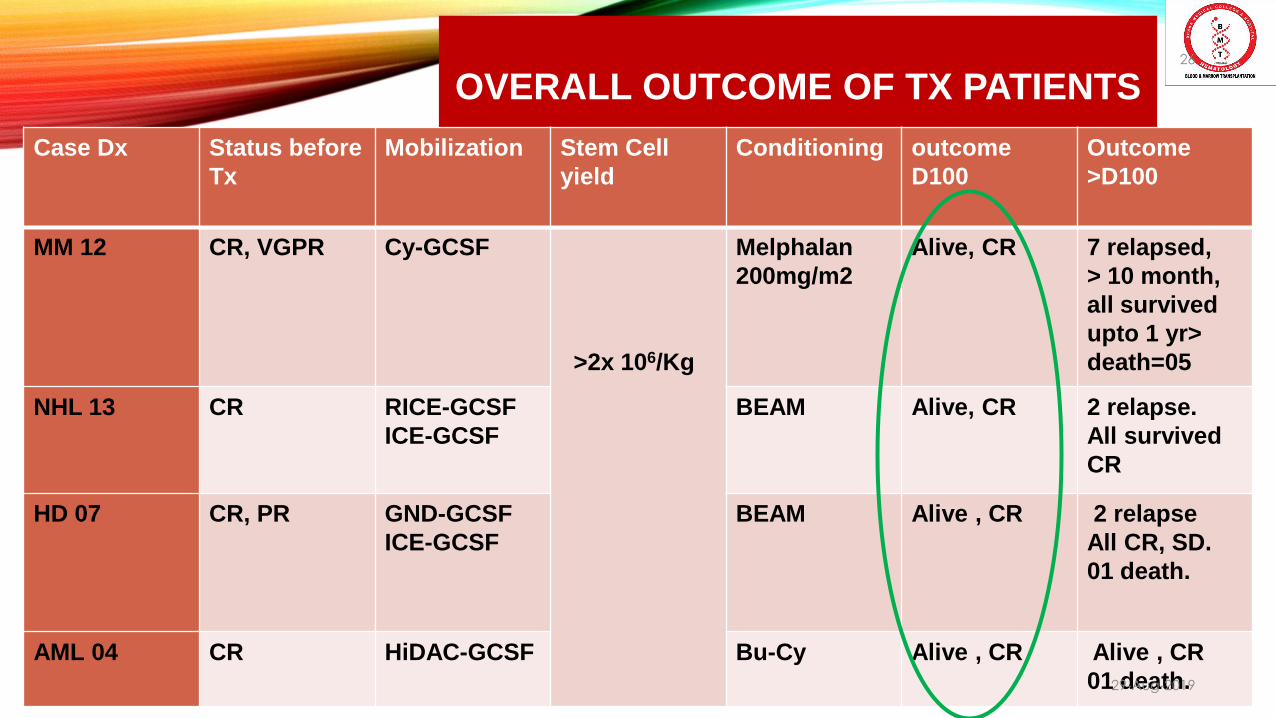
OVERALL OUTCOME OF TX PATIENTS
Case Dx Status before
Tx
Mobilization Stem Cell
yield
Conditioning outcome
D100
Outcome
>D100
MM 12 CR, VGPR Cy-GCSF
>2x 106/Kg
Melphalan
200mg/m2
Alive, CR 7 relapsed,
> 10 month,
all survived
upto 1 yr>
death=05
NHL 13 CR RICE-GCSF
ICE-GCSF
BEAM Alive, CR 2 relapse.
All survived
CR
HD 07 CR, PR GND-GCSF
ICE-GCSF
BEAM Alive , CR 2 relapse
All CR, SD.
01 death.
AML 04 CR HiDAC-GCSF Bu-Cy Alive , CR Alive , CR
01 death.
26
29-Aug-2019
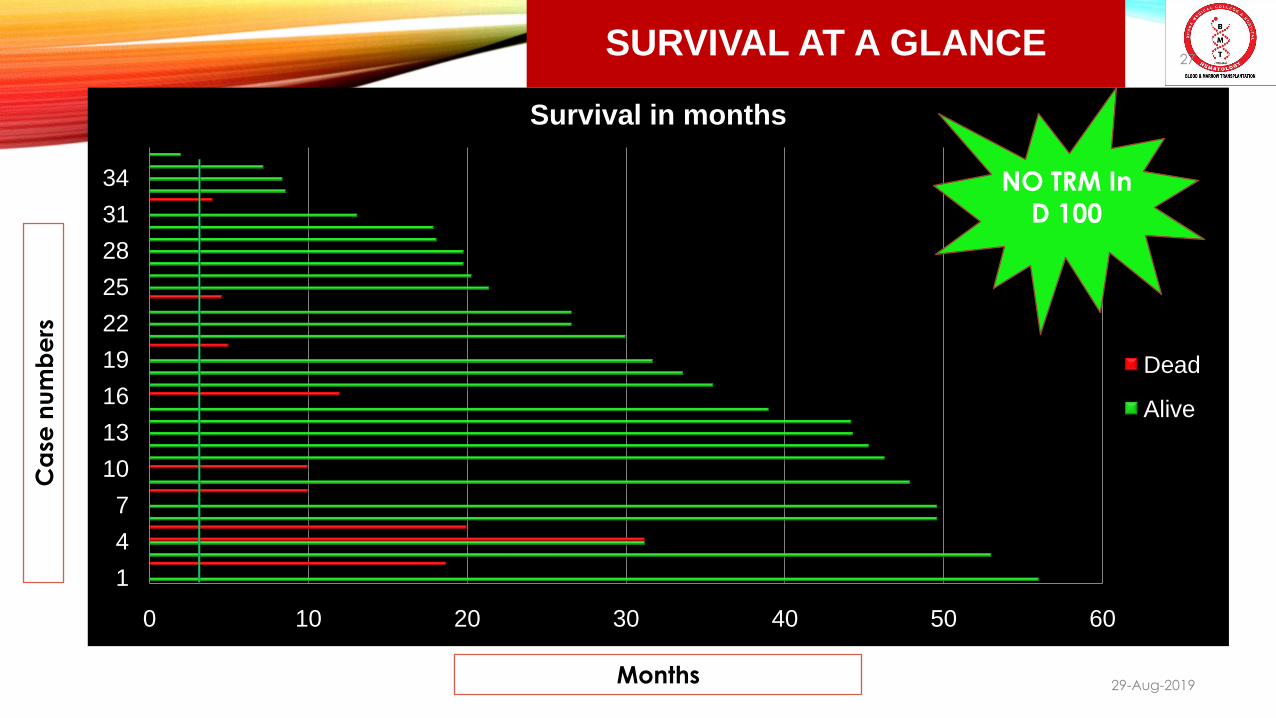
SURVIVAL AT A GLANCE
0 10 20 30 40 50 60
1
4
7
10
13
16
19
22
25
28
31
34
Survival in months
Dead
Alive
NO TRM In
D 100
Months
Ca
se n
um
be
rs27
29-Aug-2019
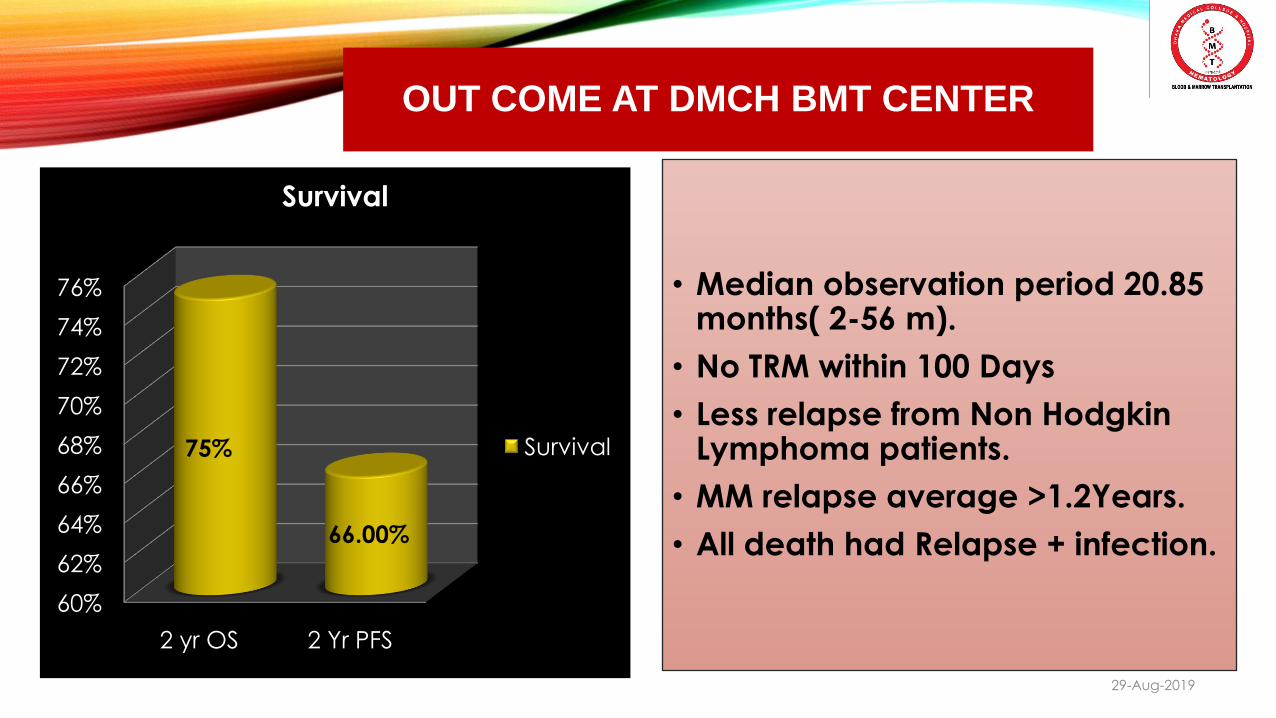
OUT COME AT DMCH BMT CENTER
60%
62%
64%
66%
68%
70%
72%
74%
76%
2 yr OS 2 Yr PFS
75%
66.00%
Survival
Survival
• Median observation period 20.85 months( 2-56 m).
• No TRM within 100 Days
• Less relapse from Non Hodgkin Lymphoma patients.
• MM relapse average >1.2Years.
• All death had Relapse + infection.
28
29-Aug-2019
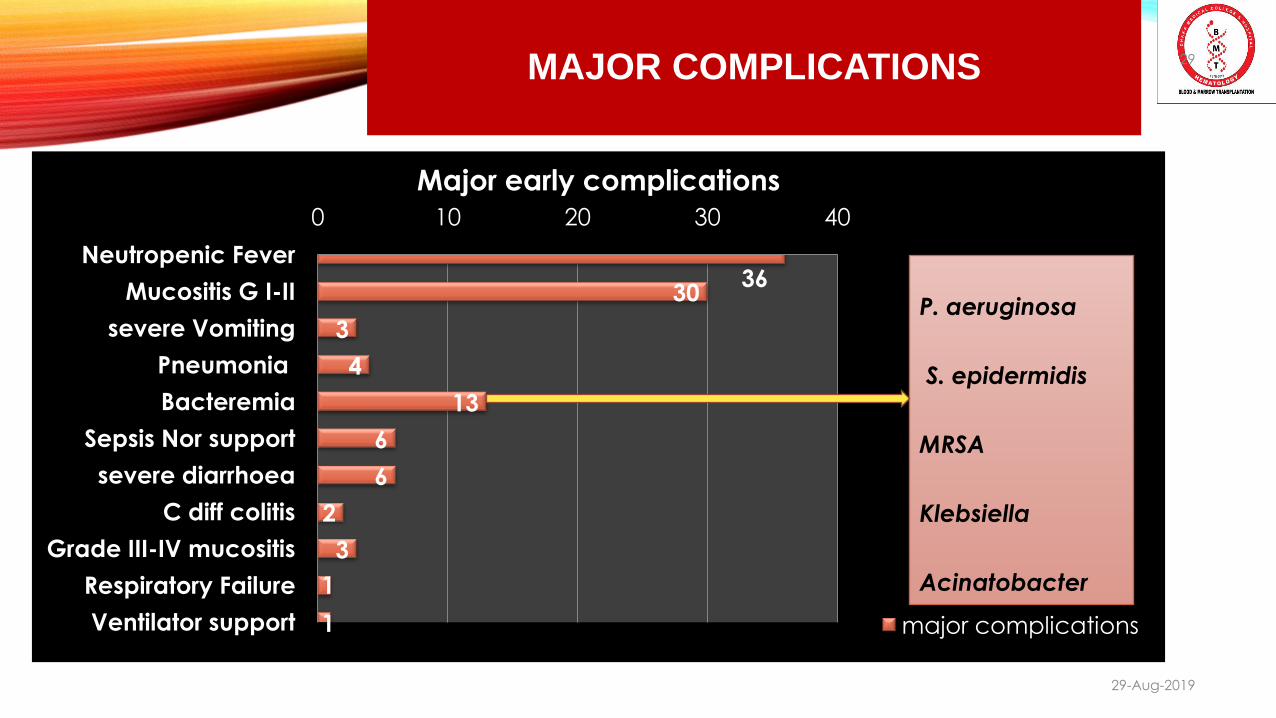
MAJOR COMPLICATIONS
3630
3
4
13
6
6
2
3
1
1
0 10 20 30 40
Neutropenic Fever
Mucositis G I-II
severe Vomiting
Pneumonia
Bacteremia
Sepsis Nor support
severe diarrhoea
C diff colitis
Grade III-IV mucositis
Respiratory Failure
Ventilator support
Major early complications
major complications
P. aeruginosa
S. epidermidis
MRSA
Klebsiella
Acinatobacter
29
29-Aug-2019
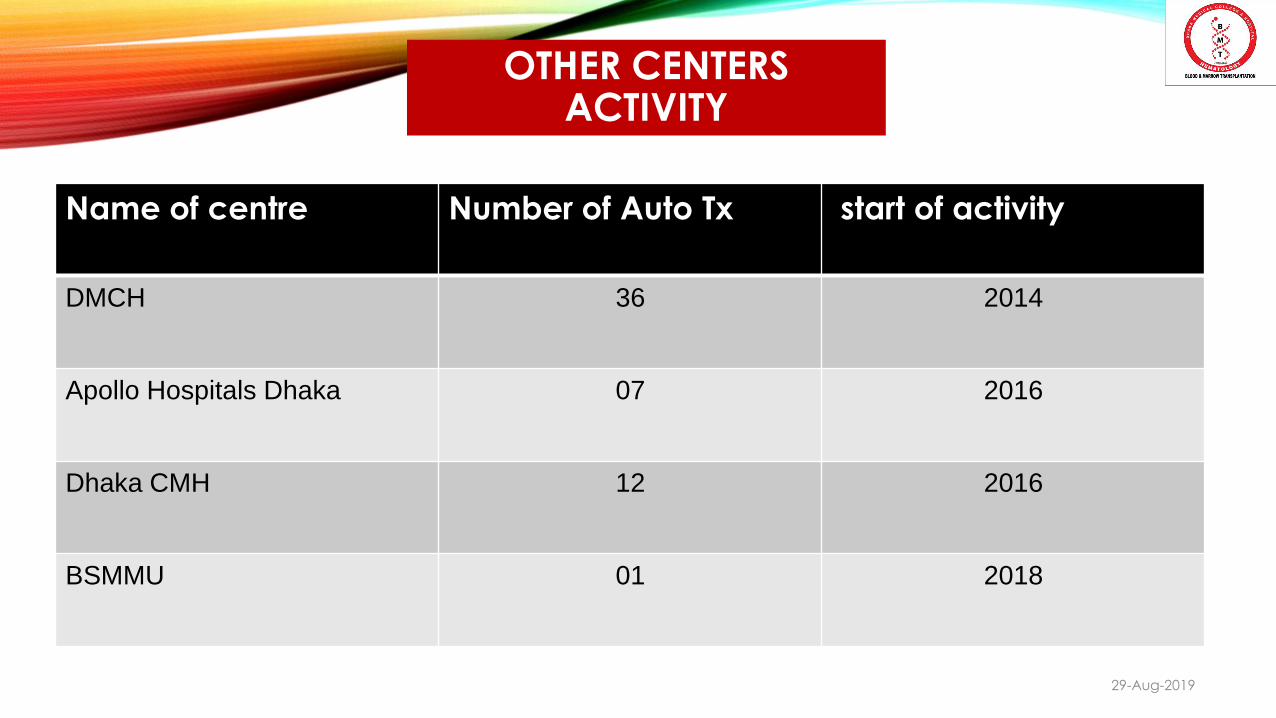
OTHER CENTERS ACTIVITY
30
29-Aug-2019
Name of centre Number of Auto Tx start of activity
DMCH 36 2014
Apollo Hospitals Dhaka 07 2016
Dhaka CMH 12 2016
BSMMU 01 2018

GOAL & VISION
Improved Cancer Care
Laboratory facilities , molecular testing
HLA lab & National Donor registry
Allogeneictransplant Center
31
29-Aug-2019
2015 national
donor registration
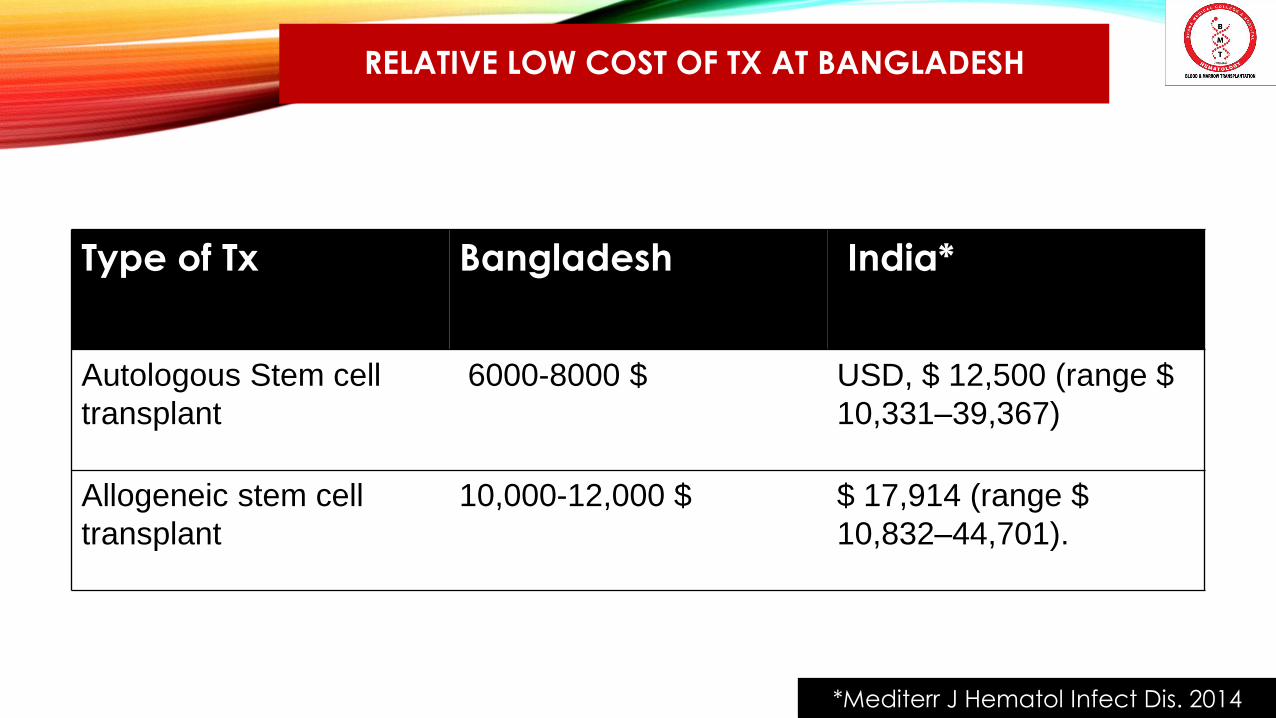
RELATIVE LOW COST OF TX AT BANGLADESH 32
29-Aug-2019
Type of Tx Bangladesh India*
Autologous Stem cell
transplant
6000-8000 $ USD, $ 12,500 (range $
10,331–39,367)
Allogeneic stem cell
transplant
10,000-12,000 $ $ 17,914 (range $
10,832–44,701).
*Mediterr J Hematol Infect Dis. 2014

29-Aug-2019
33
•2017 ASH : Digital poster award
and publication in ‘Blood
Advances’.
• 2 more articles in ‘Journal of
Global Oncology’ .
•ASH VTP award on BMT
Achievements!
TAKE HOME MESSAGES
Extreme dedication and strong TEAM work is the key to run BMT unit.
36 ASCT have been done at DMCH BMT unit.
No TRM in 100D so far.
2 year OS is 75%.
Challenges in every steps of running BMT. [ *Financial constrain is a major challenge].
Extensive and continuous government support is necessary for running this program.
34
29-Aug-2019
ACKNOWLEDGEMENT 35
29-Aug-2019
All the departments are involved directly or indirectly.
• Department of Anesthesiology
• Department of Nephrology
• Department of Radiology
• Department of Microbiology
• Department of Medicine and all allied subject

THANK YOU
FURTHER READING 1. Moskowitz CH, Bertino JR, Glassman JR, Hedrick EE, Hunte S, Coady-Lions N, et al. Ifosfamide, carboplatin and etoposide: A
highly effective cyto-reduction and peripheral blood progenitor cell mobilization regimen for transplant-eligible patients with non-Hodgkins lymphoma. J Clin Oncol. 1999;17:3776–85. [PubMed]
2. Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy sensitive non-Hodgkin lymphoma. N Engl J Med. 1995;333:1540–5. [PubMed]
3. Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, et al. Salvage regimens with autologoustransplantation for relapsed large B-Cell lymphoma in the Rituximab Era. J Clin Oncol. 2010;28:4184–90. [PMC free article] [PubMed]
4. Sehn LH, Donaldson J, Chhanabhai M, et al. Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J Clin Oncol.2005;23(22):5027-5033.
5. Friedberg JW. Rituximab for early-stage diffuse large-B-cell lymphoma.LancetOncol.2006;7(5):357-359.
6. Salvage Regimens With Autologous Transplantation for Relapsed Large B-Cell Lymphoma in the Rituximab Era J Clin Oncol28:4184-4190. © 2010 by American Society of Clinical Oncology/ Guglielmi C, Gomez F, Philip T, et al: Time to relapse has prognostic value in patients with agressive lymphoma enrolled onto the Parma trial. J Clin Oncol 16:3264-3269, 1998
7. Blay J, Gomez F, Sebban C, et al: The International Prognostic Index correlates to survival in patients with aggressive lymphoma in relapse: Analysis of the PARMA trial. Parma Group. Blood 92: 3562-3568, 1998
37
29-Aug-2019





























