Embed Size (px)
Citation preview

BONE METABOLISM IN PATIENTS BONE METABOLISM IN PATIENTS AFFECTED BY GLYCOGEN STORAGE AFFECTED BY GLYCOGEN STORAGE
DISEASE TYPE IDISEASE TYPE I
Ilaria Giulini NeriDepartment of Pediatrics
San Paolo Hospital University of Milan
International meeting glycogen storage diseases associations
2-3 October, Milan

Glycogen storage disease type I (GSD I)Glycogen storage disease type I (GSD I)
• Disorder of glucose homeostasis Disorder of glucose homeostasis (glycogenolysis/gluconeogenesis)(glycogenolysis/gluconeogenesis)
• Incidence: 1/100Incidence: 1/100..000000
• Autosomal recessive transmissionAutosomal recessive transmission
• Type Ia Type Ia glucose-6-phosphatase deficiency glucose-6-phosphatase deficiency • Type Ib Type Ib glucose-6-phosphatase translocase glucose-6-phosphatase translocase

Clinical and biochemical features of GSD IClinical and biochemical features of GSD I
Metabolic derangements: fasting hypoglycaemia, lactic acidosis, hyperuricaemia, hyperlipidaemia
Several long term complications: short stature, liver adenoma, renal damage, osteoporosis, polycistic ovaries.
Type Ib: neutropenia and neutrophil dysfunction
Accumulation of glycogen in liver, kidney, and intestine

Bone matrix loss in GSD/literature dataBone matrix loss in GSD/literature data
• Histopathological study: osteoporosis, no osteomalacia (Soejima et al., Pediatr Pathol, 1985)
• Radiographic study: osteopenia, retarded bone maturation, fractures, nonspecific skeletal abnormalities (Miller et al., AM J Roentgenol, 1979)
• BMC in prepubertal patients (Lee et al., Eur J Pediatr 1995)
• Association with reduced muscle force and metabolic control (Schwan et al., J Pediatr 2002)
• BMD in adolescence/adult patients: diminished bone MD in adolescence/adult patients: diminished bone mass accretion during childhood or historical differences in mass accretion during childhood or historical differences in treatment? (Rake et al., J Inherit Met Dis, 2003)treatment? (Rake et al., J Inherit Met Dis, 2003)
• NNo correlation between BMD and markers of bone turnover (Cabrera-Abreu et al., J Inherit Met Dis, 2004)J Inherit Met Dis, 2004)

Bone matrix loss in GSD/pathophysiologyBone matrix loss in GSD/pathophysiology
Restrictive diet (dairy products, other sources of sucrose, fructose, galactose need to be avoided)
Hypoglycaemia and low insulin values lead to a low non-enzymatic glycosilation of bone matrix proteins impaired bone resistance
Chronic lactic acidosis:1. increase of mobilization and release of bone alkaline salts
(calcium phosphate and carbonate) in response to a acid load to mantain acid-base balance
2. loss of calcium and phosphate with urine hypercalciuria and reduced tubular reabsorption of phosphate
3. high activity of osteoclasts, reduced of osteoblasts

Bone matrix loss in GSD/pathophysiologyBone matrix loss in GSD/pathophysiology
Endogenous glucocorticoid excess, altered levels of GH and IGF-1 seems to reduce collagen content in bone and matrix synthesis
Abnormal pubertal growth spurt with sex hormone secretory dysfunction (important role in bone formation and adequate peack bone mass, especially during puberty)
Decreased calcium absorption

Bone matrix loss in GSD/pathophysiologyBone matrix loss in GSD/pathophysiology
Hypotrophic muscles and decreased muscle function (result of reduced whole-body protein synthesis and of increased proteinolysis due to increased gluconeogenesis, especially in poor metabolic control)
Decreased physical activity (chronic disease) ?

AIM OF THE STUDYAIM OF THE STUDY
To study prevalence of To study prevalence of osteopenia osteopenia and and osteoporosisosteoporosis
To determine To determine plasmatic levels of 25(OH)D plasmatic levels of 25(OH)D and to research a and to research a correlation with bone mineral density (BMD)correlation with bone mineral density (BMD)
To evaluate correlation between metabolic balance and To evaluate correlation between metabolic balance and bone bone markersmarkers
BONE METABOLISM AND VITAMIN D ROLE BONE METABOLISM AND VITAMIN D ROLE IN PATIENTS WITH GSD IIN PATIENTS WITH GSD I

Why vitamin D?Why vitamin D?
Important role in calcium homeostasis and bone metabolism
Vitamin D insufficiency osteoporosis (not rickets or osteomalacia) as a result of calcium malabsorption
Vitamin D deficiency proximal muscle weakness (receptor for vitamin D (VDR) is expressed in human muscle tissue, and VDR activation may promote de novo protein synthesis in muscle)
BACKGROUNDBACKGROUND

Why vitamin D?Why vitamin D?
Serum 25(OH)D is the correct functional indicator of vitamin D status; reference values according to Holick, M. F. Vitamin D deficiency. N Engl J Med (2007).
The increment in serum 25(OH)D produced by an oral dose of vitamin D is greater at low basal levels than at higher values.Safe upper limit: 2000UI(=50 ug)/day (Food and Nutrition Board)
BACKGROUNDBACKGROUND

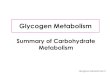
Sun exposure could be sufficient to cover requests (UVB exposure for 10-15 min generates 10000-20000 UI vit D3/24 h).
Problems: winter months, sunscreen, sun-protective clothing, low outdoor activities, northern latitudes, dark skin pigmentation, reduced skin synthesis in older people.
Vitamin D/skin productionVitamin D/skin production

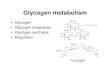
Vitamin D/food contentVitamin D/food content
Modified by Zittermann, Vitamin D in preventive medicine: are we ignoring the evidence?British Journal of Nutrition (2003)
1UI = 0,025 µg/die

American Academy of Pediatrics (2008): 400 IU per day to prevent ricket and vitamin D deficiency in children and adolescents
Institute of Medicine (1997):-200 IU per day for adults up to 50 years of age-400 IU per day for adults between age 51 and 70-600 IU per day for those aged 70 years and over.
In absence of adequate sun exposure: 800-1000 UI/day (20-25μg/day).
Vitamin D/recommended adequate intakeVitamin D/recommended adequate intake

Daily recommended amount of calcium and Daily recommended amount of calcium and vitamin D (L.A.R.N.)vitamin D (L.A.R.N.)
Age
(y
ears
)
Wei
ght
(K
g)
Cal
cium
(m
g)
Vit
.D
(mg)
Infancy 0,5-1 7-10 600 10-25
Childhood 1-3 9-16 800 10
4-6 16-22 800 0-10
7-10 23-33 1000 0-10
Male 11-14 35-53 1200 0-15
15-17 55-66 1200 0-15
18-29 65 1000 0-10
30-59 65 800 0-10
60+ 65 1000 10
Female 11-14 35-51 1200 0-15
15-17 52-55 1200 0-15
18-29 56 1000 0-10
30-49 56 800 0-10
50+ 56 1200-1500(5)* 10

Serum concentrations of 25(OH)D levels are low in patients with inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease (Jahnsen et al. 2002).
Moreover, supplementation with vitamin D or calcitriol significantly ameliorated symptoms (Cantorna et al. 2000).
Vitamin D/inflammatory bowel diseaseVitamin D/inflammatory bowel disease

In GSD type I:In GSD type I:
Dietary restrictionsDietary restrictions
Metabolic derangementsMetabolic derangements
Intestinal malabsorptionIntestinal malabsorption
The current guidelines for GSD I do not recommend The current guidelines for GSD I do not recommend evaluation of vitamin D as part of routine follow upevaluation of vitamin D as part of routine follow up
Banugaria et al., Mol Genet Met, 2009: “Banugaria et al., Mol Genet Met, 2009: “Hypovitaminosis D Hypovitaminosis D in glycogen storage disease type I”in glycogen storage disease type I”

PATIENTS and PATIENTS and METHODSMETHODS
PATIENTS:PATIENTS:
• n n = 13= 13
• Ia/Ib = 6/7Ia/Ib = 6/7
• M/F = 8/5M/F = 8/5
• Median age: 22 y, 7 moMedian age: 22 y, 7 mo
• Range = 8 – 30 yRange = 8 – 30 y
METHODS:METHODS:
Every 4 – 6 monthsEvery 4 – 6 months::
1.1. ClinicalClinical evaluationevaluation
2.2. Nutritional evaluationNutritional evaluation
3.3. Laboratory analysis Laboratory analysis
4.4. DXA scansDXA scans

RESULTS and DISCUSSIONRESULTS and DISCUSSION
Bone mineral density (BMD)Bone mineral density (BMD)
Reduced BMD in 69% of patients

BMD in GSD Ia/IbBMD in GSD Ia/Ib
RESULTS and DISCUSSIONRESULTS and DISCUSSION

BMD and markers of bone turnoverBMD and markers of bone turnover
RESULTS and DISCUSSIONRESULTS and DISCUSSION

BMD and metabolic controlBMD and metabolic control
RESULTS and DISCUSSIONRESULTS and DISCUSSION

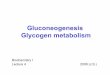
Vitamin D statusVitamin D status
RESULTS and DISCUSSIONRESULTS and DISCUSSION
Low 25(OH)D in 69% of patients

Vitamin D and BMDVitamin D and BMD
RESULTS and DISCUSSIONRESULTS and DISCUSSION
pz^ : taking supplements

Correlation between bone disease and metabolic control
High prevalence of low 25(OH)D levels
Low 25(OH)D levels despite supplementation
CONCLUSIONSCONCLUSIONS

Correction of low 25(OH)D concentration - 1Correction of low 25(OH)D concentration - 1
Some or all of the following: Some or all of the following:
1.1. encouragement of safe, moderate exposure of skin to encouragement of safe, moderate exposure of skin to ultraviolet lightultraviolet light
2.2. appropriate increases in food fortification with appropriate increases in food fortification with vitamin Dvitamin D
3.3. provision of higher doses of vitamin D in provision of higher doses of vitamin D in supplementssupplements
Banugaria et al., HBanugaria et al., Hypovitaminosis D in glycogen storage ypovitaminosis D in glycogen storage disease type I.disease type I. Mol Genet Met, 2009 Mol Genet Met, 2009

Correction of low 25(OH)D concentration - 2Correction of low 25(OH)D concentration - 2
- 50,000 IU for adult patients (4,000 IU daily for 50,000 IU for adult patients (4,000 IU daily for children) of vitamin Dchildren) of vitamin D22 once weekly for 8 weeks. once weekly for 8 weeks.
- Maintenance dose = 1000 IU vitamin D daily or, Maintenance dose = 1000 IU vitamin D daily or,
alternatively, 50,000 IU vitamin D every other weekalternatively, 50,000 IU vitamin D every other week
Holick et al., Vitamin D deficiency. N Engl J Med 357, 266-Holick et al., Vitamin D deficiency. N Engl J Med 357, 266-281 (2007).281 (2007).


Thanks for your attention!Thanks for your attention!