Embed Size (px)
Citation preview

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 1/80
BONE TUMORS

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 2/80
Bone Tumors & Tumor-Like Lesions

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 3/80
Bone Tumors & Tumor-Like Lesions

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 4/80
• Osteoma
•Osteoid Osteoma and Osteoblastoma
• Osteosarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 5/80
Osteoma
• Bosselated, round-to-
oval sessile tumors
• Subperiosteal surface of
cortex
• On or inside skull and
facial bones
• Usually solitary• Middle age

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 6/80
Osteoid Osteoma and Osteoblastoma
Osteoid osteoma – <2cm, teens and 20s,
M>F 2:1
–
Appendicular skeleton,posterior elements ofspine
– Cortex>medullary cavity
– Symptoms• Nocturnal pain
• Relieved by aspirin
Osteoblastoma
– >2cm
– Spine
– Symptoms• Dull, achy
• Unresponsive tosalicylates

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 7/80
Osteoid Osteoma and Osteoblastoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 8/80
Osteosarcoma
• Most common primary
malignant tumor (20%)
• Mesenchymal tumor
• Bimodal age distribution
• M>F (1.6:1)
• Metaphyseal region of long
bones

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 9/80
Osteosarcoma
Genetic abnormality
• RB
•
P53• INK4a (p16)
Characteristics
• Metaphysis of long
bones• Primary
• Solitary
• Intramedullary• Poorly differentiated

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 10/80
Osteosarcoma
Gross
• Big, bulky tumors
• Gritty, gray-white
• Areas of hemorrhage &cystic degeneration

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 11/80
Osteosarcoma
Microscopic
• Large hyperchromatic
nuclei
• Bizarre tumor giant cells
• Mitosis
• Formation of bone
• Coarse, lace likearchitecture

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 12/80
Osteosarcoma
Clinical Course
• Painful
• Progressively enlarging
mass• Reactive periosteal
formation
• Hematogenous spread
• (+) metastases: lungs,
bones, brain

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 13/80
• Osteochondroma
• Chondroma
•
Chondroblastoma• Chondromyxoid Fibroma
• Chondrosarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 14/80
Osteochondroma
• Exostosis
• Benign
• Attached to skeleton by
a bony stalk
• Most common benignbone tumor
•
Solitary• Autosomal dominant:
EXT1, EXT2
• Late adolescencce, earlyadulthood
• M>F (3:1)
• Endochondral origin
• Metaphysis, near growth
plate of long tubularbones (knee)

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 15/80
Osteochondroma
• Sessile
• Mushroom shaped
• 1-20cm
• Cap: benign hyalinecartilage covered byperichondrium
• Cortex of stalk mergewith host bone
• Slow-growing mass
• Can be painful
• Incidental finding
• Stop growing at timeof growth plateclosure
• Can give rise tochondrosarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 16/80
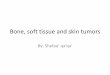
Osteochondroma
• FIGURE 26-25 Osteochondroma. A, X-ray of an osteochondroma arising off the posteriorsurface of the tibia. B, Axial CT scan shows continuity of the cortex of the bone and the
center of the osteochondroma. The fibula is adjacent to the mass. C, Gross specimen of
sessile osteochondroma composed of a cap of hyaline cartilage undergoing enchondral
ossification. D, The cartilage cap has the histologic appearance of disorganized growth
plate-like cartilage.

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 17/80
Chondroma and Enchondroma
• Benign
• Hyaline cartilage
• Bones of endochondral
origin
• Medullary cavity:
enchondromas
•
Surface of bone:subperiosteal /
juxtacortical chondromas
• 20-40’s
• Solitary
• Metaphyseal lesion of
tubular bones (shorttubular bones of hands
and feet)
•
Ollier disease(enchondromatosis)
• Maffucci Syndrome

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 18/80
Chondroma
• <3cm
• Gray-blue, translucent
• Well-circumscribed
nodules

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 19/80
Chondroma
•
Asymptomatic• Cause pathologic fracture
• Numerous, large tumors
•
C or O ring sign

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 20/80
Chondroblastoma
• Rare, benign tumor• Teens, M>F 2:1
• Knee
•Epiphyses and apophyses
• Sheets of chondroblasts
• Well-defined cytoplasmic
borders
• Moderate pink cytoplasm
• Hyperlobulated nuclei
• Chicken-wire mineralization
Scattered through the lesion are non-neoplastic
osteoclast-type giant cells.
Occasionally the tumors undergo prominent
hemorrhagic cystic degeneration.

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 21/80
Chondromyxoid firboma
• Rarest• Teens, 20’s
• M>F
• Metaphysis of longtubular bones
• 3-8cm
•
Well-circumscribed• Solid
• Glistening tan-gray

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 22/80
Chondrosarcoma
• Neoplastic cartilage
• Central (intramedullary)
vs peripheral
(juxtacortical andsurface)
• Conventional (hyaline
and/or myxoid), clear
cell, dedifferentiated,mesenchymal variants
•
Second most commonmalignant matrix-
producing tumor
• >40’s
• M>F 2:1
• Malignant hyaline and
myxoid cartilage
• Nodules of gray-whitetranslucent glistening
tissue

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 23/80
Chondrosarcoma
• Predominantly myxoid
– Viscous, gelatinous
tumors – Spotty calcifications
present
– Central necrosis
cystic spaces
• Grading

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 24/80
Chondrosarcoma
• Central portions of
skeleton
• Rarely involves distal
extremities• Painful, enlarging mass
• Imaging: endosteal
scalloping
Prognostic
• As grade progresses,
chance of metastases
increases (lungs,skeleton)
• >10cm – aggressive
Treatment• Wide surgical incision
• Chemotherapy

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 25/80
Fibrous Cortical Defect and Non-Ossifying Fibroma
• FCD common (30-50%, >2y/o)
• Metaphysis of distal femur and proximal tibia
• Bilateral, multiple
• 0.5cm – 5 or 6cm (non-ossifying fibroma)

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 26/80
Fibrous Cortical Defect and Non-
Ossifying Fibroma
Morphology
• Elongated, sharply
demarcated
radiolucencies• Surrounded by thin rim
of sclerosis

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 27/80
Fibrous Cortical Defect and Non-
Ossifying Fibroma
• Gray-yellow brown cellular
lesions with fibroblast and
macrophage
• Storiform (pinwheel)pattern
• Histiocytes are
multinucleated giant cells
or clusters of foamy
macrophages

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 28/80
Fibrous Dysplasia
• Benign tumor
• Does not differentiate to
mature structures
•
Mutation in GNAS gene
Patterns:1. Invovlement of single
bone (monostotic)
2. Invovlement of multiplebones (polyostotic)
3. Polyostotic disease, with
café-au-lait skin
pigmentation and
endrocrine abnormalities

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 29/80
Monostotic fibrous dysplasia
• 70% of cases
• M=F, early adolescence
• Stops enlarging at time
of growth plate closure
•Femur, tibia, ribs,
jawbones, calvaria,
humerus
• Asymptomatic
• Cause pain, fracture,
discrepancy in limb
length
Polyostotic fibrous dysplasia
w/o endocrine dysfunction
• 27% of cases• Early age
• Craniofacial involvement
•Crippling deformities
• Recurrent fractures

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 30/80
Polyostotic Fibrous Dysplasia
assoc. w/ café-au-lait
pigmentation andendocrinopathies
• McCune-Albright syndrome
•
3% of cases• Precocious sexual
development (F>M)
• Pigmentation: neck, chest,
back, shoulder, pelvic region
Polyostotic Fibrous Dysplasia assoc

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 31/80
Polyostotic Fibrous Dysplasia assoc.
w/ café-au-lait pigmentation and
endocrinopathiesMorphology
• Well-circumscribed
• Intramedullary
• Tan-white and gritty• Curvilinear trabeculae of
woven bone
•
Moderately cellularfibroblastic proliferation
• Trabeculae mimic
Chinese letters

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 32/80
Fibrosarcoma variants
• Collagen-producing with
fibroblastic phenotype
• Middle-aged, elderly
• M=F
Morphology
• Gross
• Large, hemorrhagic
• Tan-white mass• Destroy bone and extend
to soft tissues
Microscopic
• Malignant fibroblast
• Herringbone storiform
pattern
• Malignant fibrous
histiocytoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 33/80
Ewing sarcoma and Primitive
Neuroectodermal tumor (PNET)
• primary malignant small round cell tumors of
bone and soft tissue
• Identical chromosome translocation, differing
only in their degree of neural differentiation
– neural differentiation – PNETs
– undifferentiated - Ewing sarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 34/80
Ewing sarcoma and Primitive
Neuroectodermal tumor (PNET)
• 2nd most common group of bone sarcomas in
children
• 10 to 15 years old (~ 80% are < 20 years)
• Translocation: EWS gene on chromosome 22
and most commonly involved ETS gene is
FLI1, as part of a (11;22) (q24;q12)
translocation
– abnormal cell proliferation and survival

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 35/80
Sheets of small round cells with small amounts of clearcytoplasm
arises from the medullary cavity, invading the cortex, periosteum, and soft tissue.
tumor is soft, tan-white, and frequently contains areas of hemorrhage and necrosis
composed of sheets of uniform small, round cells that are slightly larger than lymphocytes with scant clear cytoplasm
Homer-Wright rosettes (tumor cells arranged in a circle about a central fibrillary space) is indicative of neural differentiation

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 36/80
Ewing sarcoma and Primitive
Neuroectodermal tumor (PNET)
• Diaphysis of long tubular bones (femur andflat bones of the pelvis)
• Systemic findings: fever,↑ sedimentationrate, anemia, and leukocytosis,
• Plain radiograms - destructive lytic tumor
– periosteal reaction produces layers ofreactive bone deposited in an onion-skin
fashion• Treatment: chemotherapy and surgical
excision with or without irradiation

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 37/80
Giant-cell Tumor
• Mixture of mononuclear cells and
multinucleated osteoclast-type giant cells
(osteoclastoma)
• Uncommon benign-locally aggressive
neoplasm
• RANK/RANKL signaling pathway

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 38/80
Abundance of multinucleated giant cells with background mononuclear
stromal cells
large, red-brown tumors that frequently undergo cystic degeneration
composed of uniform oval mononuclear cells that constitute the proliferating component of the tumor
osteoclast-type giant cells having 100 or more nuclei that resemble those of the mononuclear cells
necrosis, hemorrhage, hemosiderin deposition, and reactive bone formation are common secondaryfeatures
Giant Cell Tumor

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 39/80
Giant Cell Tumor
• Adults - epiphyses and the metaphyses
• Adolescents -limited to the metaphysis
• Majority arise around the knee
• Most are solitary
• Erode into the subchondral bone plate and
destroy the overlying cortex

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 40/80
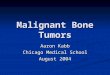
Giant Cell Tumor
Magnetic resonance image
of a giant-cell tumor that
replaces most of the femoralcondyle and extends to the
subchondral
bone plate

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 41/80
Aneurysmal Bone Cyst
• Benign tumor
• Multiloculated blood-filled cystic spaces
• 17p13 translocations that result in up-
regulation of USP6, a deubiquitinating
enzyme

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 42/80
multiple blood-filled cystic spaces separated by thin, tan-white septa
walls are composed of plump uniform fibroblasts (which may be mitotically active),
multinucleated osteoclast-like giant cells, and reactive woven bone
bone is lined by osteoblasts that follow the contours of the fibrous septa
Aneurysmal Bone Cyst

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 43/80
Aneurysmal Bone Cyst
• Generally occurs during the first 2 decades of
life
• Metaphyses of long bones and the posterior
elements of vertebral bodies
• Radiograph- eccentric, expansile lesion with
well-defined margins
• Most lesions are completely lytic and often
with thin shell of reactive bone

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 44/80
Aneurysmal Bone Cyst
Soft-tissue component is delineated by a
thin rim of reactive subperiosteal boneCharacteristic fluid-fluid levels

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 45/80
Metastatic Disease
• most common form of skeletal malignancy
Pathways
(1) direct extension
(2) lymphatic or hematogenous dissemination
(3) intraspinal seeding (via the Batson plexus of
veins)

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 46/80
Metastatic Disease
• adults: > 75% from cancers of the prostate,
breast, kidney, and lung
• children: neuroblastoma, Wilms tumor,
osteosarcoma, Ewing sarcoma, and
rhabdomyosarcoma
• most involve the axial skeleton > proximal
femur > humerus

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 47/80
REACTIVE TUMOR-LIKE LESIONS OFJOINTS

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 48/80
Ganglion Cyst
• ganglion cyst is a small (1 to 1.5 cm) cyst that
is almost always located near a joint capsule
or tendon sheath
• firm, fluctuant, pea-sized translucent nodule
• Usually around wrist joints
• Fluid-filled but non communicating
• Myxoid degeneration and softening of
connective tissue

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 49/80
Ganglion Cyst

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 50/80
Synovial Cyst
• Herniation of synovium through a joint
capsule or massive enlargement of a bursa
may produce a synovial cyst
• Baker cyst (RA setting)
• Synovial lining may be hyperplastic and
contain inflammatory cells and fibrin but is
otherwise unremarkable

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 51/80
Synovial Cyst
Vill d l S iti d Gi t C ll

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 52/80
Villonodular Synovitis and Giant Cell
Tumor of Tendon Sheath
• Group of benign neoplasms that develop in
the synovial lining of joints, tendon sheaths,
and bursae
• Consistent chromosomal aberrations
(neoplastic nature)
• Presents as a monoarticular arthritis that
affects the knee in 80% of cases

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 53/80
PVNS GCT

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 54/80
SOFT TISSUE TUMORS

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 55/80
Sources
• Fat
• Fibrous tissue and Fibrohistiocytic
• Skeletal muscle
• Smooth muscle
• Vascular
•
Peripheral nerve• Uncertain: synovial sarcoma, alveolar soft part sarcoma,
epitheliod sarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 56/80
Soft tissue tumors
• Causes of most are unknown
• Documented associations with radiation orprevious tissue injury
• Genetic syndromes – neurofibromatosis type 1 (neurofibroma,
malignant schwannoma)
– Gardner syndrome (fibromatosis)
– Li-Fraumeni syndrome (soft tissue sarcoma)
– Osler-Weber-Rendu syndrome (telangiectasia)

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 57/80
Soft tissue tumors
• 40% occur in the lower extremities, especiallythe thigh
• Fifteen per cent arise in children(4th most
common malignancy)• Grading (I to III) is based on degree of
differentation, mitoses, pleomorphism,necrosis
• Clinical staging involves the extent and size ofthe tumor

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 58/80
Soft tissue tumors

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 59/80
Soft tissue tumors

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 60/80
FAT
•lipoma
• liposarcoma
Normal fatLipoma,
encapsulated Liposarcoma, oftenretroperitoneal

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 61/80
Lipoma
• More common in women
• Benign soft tissue tumor composed of
differentiated fat cells
• Subcutaneous, mostly occur on the upper half
of the body (trunk, neck)
• Can occur in deep tissues (intramuscular,
intermuscular)
• 5th to 6th decade of life

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 62/80
Liposarcoma
• One of the most common sarcomas of adulthood
• 40s to 60s
• Arise in the deep soft tissues of the proximal
extremities and retroperitoneum
• Can be Well differentiated
• Myxoid
• Round cell type
• Pleiomorphic type

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 63/80
Fibrous tissue
• Nodular fasciitis(pseudosarcomatous)
• Fibromatoses
(plantar, palmar, penile)• Fibrosarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 64/80
Nodular fascitiis
• infiltrative or pseudosarcomatous fasciitis
• most common of the reactive pseudosarcomas
• often occurs in adults on the volar aspect of the
forearm
• arise in the deep dermis, subcutis, or muscle
• several-week history of a solitary, rapidly
growing, and sometimes painful mass
• Sometimes associated with preceding trauma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 65/80
Nodular Fascitiis
Nodular fasciitis is richly cellular and consists of plump, immature-appearing fibroblasts
arranged randomly (simulating cells growing in tissue culture) or in short intersecting fascicles,
The cells vary in size and shape (spindle to stellate) and have conspicuous nucleoli and
abundant mitotic figures

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 66/80
Myositis Ossificans
• presence of metaplastic bone
• usually develops in athletic adolescents and
young adults
• follows an episode of trauma >50% of cases
• Early phase: swelling and pain
• Later stage: well circumscribed, firm mass
• Final stage: painless, hard, well-demarcated mass
• Progress in as little time as 3 weeks

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 67/80
Myositis Ossificans
MYOSITOS OSSIFICANS can be thought of as being a METAPLASTIC process, often following inflammationi.e.:
Usual scenario:InflammationFibrosis
Myositis Ossificans:InflammationFibrosisOssification

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 68/80
Superficial Fibromatoses
• Palmar (Dupuytren contracture) – irregular or nodular thickening of the palmar fascia
– progressive flexion contracture develops
– fourth and fifth fingers of the hand
• Plantar
– Similar to plantar fibromatoses, except contracturesand bilaterality are uncommon
• Penile (Peyronie disease) – palpable induration or mass appears usually on the
dorsolateral aspect of the penis
Deep seated Fibromatoses

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 69/80
Deep seated Fibromatoses
(Desmoid tumors)
• Borderland behavior
• Large, infiltrative masses recur afterincomplete excision
Extra-abdominal ( shoulder, chest wall, back, andthigh)
Abdominal ( Abdominal musculoaponeurotic inwomen)
Intra-abdominal ( Intra-abdominal; associated withFAP)

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 70/80
Fibrosarcoma
• Rare, malignant, collagen-forming non
pleomorphic, fibroblastic cell tumor, mainly of
adulthood, occasionally congenital
• Unencapsulated, well circumscribed, softmasses
• recurring in more than 50% of the cases and
metastasizing in more than 25%

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 71/80
Fibrosarcoma
Note the malignant spindle cells arranged in
a herringbone pattern

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 72/80
Skeletal Muscle
RhabdomyosarcomaRhabdomyoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 73/80
Rhabdomyosarcoma
• most common soft tissue sarcoma of childhoodand adolescence
• <20 years old
•
most occur in the head and neck orgenitourinary tract
• With embryonic, alveolar, and pleomorphicvariants
• Involve t(2;13)(q35;14) translocations
• Rhabdomyoblast - diagnostic cell

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 74/80
Rhabdomyosarcoma
Alveolar rhabdomyosarcoma
with numerous spaces lined by
tumor cells
Rhabdomyosarcoma composed of malignant
small round cells. The rhabdomyoblasts are
large and round and have abundant
eosinophilic cytoplasm.

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 75/80
Smooth Muscle
Leiomyoma
Leiomyomasarcoma

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 76/80
Leiomyoma
• Benign
• Most often arising from the uterus, but also
from erector pili muscles found in the skin,
nipples, scrotum, and labia
• tendency to develop multiple lesions is
thought to be hereditary

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 77/80
Leiomyosarcoma
• 10% to 20% of soft tissue sarcomas
• Skin and deep soft tissues of the extremities
and retroperitoneum
• Painless firm masses
• malignant spindle cells that have cigar-shaped
nuclei arranged in interweaving fascicles

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 78/80
Synovial Sarcoma
• Cell of origin is still unclear
• 20s to 40s
• deep soft tissue extremities
• 60% to 70% involve the lower extremities
• chromosomal translocation t(x;18) producing
SYT-SSX1 or -SSX2 fusion genes
• Commonly metastasizes to the lung, skeleton
k l

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 79/80
Unknown- Synovial Sarcoma
-dual line of differentiation of the tumor cells (i.e., epithelial-like and spindle cells); The
epithelial cells are cuboidal to columnar and form glands or grow in solid cords or aggregates,
The spindle cells are arranged in densely cellular fascicles that surround the epithelial cells

7/24/2019 Bone Soft Tumors
http://slidepdf.com/reader/full/bone-soft-tumors 80/80
END