-
Perspective Ramez ShehadiAli HashemiWalid TohmeJad Bitar
Getting a Handle on Chronic DiseaseHealth Management Services in
the GCC Region
-
Booz & Company
Contact Information
BeirutRamez
[email protected]
Walid [email protected]
Jad BitarSenior [email protected]
DubaiAli [email protected]
-
Booz & Company 1
EXECUTIVE SUMMARY
HMS programs address critical gaps in the care of chronically
ill patients by helping them understand the implications of their
disease and underlying lifestyle factors, amend their harmful
behavior, adhere to treatment regimens, and navigate the healthcare
system. HMS programs have been proven to be successful at improving
individuals health and generating significant savings for
healthcare payors when all stakehold-erspatients, physicians,
hospitals, insurers, and governmentbuy into their development. A
number of best
practicesincluding effective use of incentives, physician
involvement, and personalizationcan help HMS pro-grams achieve
their goals. But before GCC governments and healthcare
organizations can implement HMS programs, they will need to answer
strategic questions about the segments of society that should be
targeted, the programs that will be most relevant, the incentives
that would encourage involvement, the funding mechanism that will
support HMS, the objec-tives of the program, and the roles of
public and private entities.
The growing prevalence of chronic diseases in Gulf Cooperation
Council (GCC)1 nations has socioeconomic implications that are
quickly adding up. Chronic diseases generate higher healthcare
costs, which are borne by govern-ments, insurers, and patients.
They also lower productivity among workers, clog healthcare service
channels, and bring about declines in a populations health status.
As GCC nations continue to invest in their healthcare systems, the
regions leaders should take their cue from certain developed
nations in adopting health management services (HMS) to help
address the specter of a chronic disease epidemic.
-
Booz & Company
Around the world, unhealthy lifestyles and aging populations are
leading to a higher prevalence of chronic disease, thus driving up
healthcare costs and keeping economies from perform-ing at their
true potential. Chronic diseases strain healthcare providers and
the overall healthcare system with patients frequent and costly
trips to the emergency room (ER) and longer average stays. Long and
resource-intensive treatment periods make patients with chronic
disease heavy users of healthcare services, leading them to consume
a dispropor-tionate amount of the total available services. This
has a severe impact on the distribution of those services and clogs
providers ER and other delivery channels.
Chronic diseases not only negatively affect a populations
general health status, but they also levy serious
hidden costs on society, such as lower worker productivity.
Recent research shows that on-the-job productivity losses account
for up to 60 percent2 of the total healthcare costs associated with
chronic diseases.
To counter these trends, care provid-ers in North America are
increasingly turning to health management services (HMS). These
services primarily work in two ways: They help mitigate the spread
of chronic diseases by estab-lishing wellness programs and other
preventive strategies, and they reduce the costs of treating
chronic diseases once they are diagnosed through ongoing monitoring
and frequent interaction with patients.
HMS will be a critical element of GCC countries overall
healthcare strategies in the future, as chronic diseases exact a
toll in terms of costs, strain on providers, and healthcare status:
In the coming years, chronic diseases are expected to account for a
significant portion of healthcare expenses. As governments,
healthcare organizations, and private insurers in the region look
to develop a compre-hensive health management strategy that
addresses this mounting problem, HMS programs are a key tool.
2
THE RUNAWAY COSTS OF CHRONIC DISEASES
KEY HIGHLIGHTS
HMSprogramsareakeytoolinthe effort to halt the rise of chronic
diseases in GCC countries and keephealthcarecostsincheck.
NumerousstudieshavedemonstratedthebenefitsofHMSonindividualshealthand
on overall healthcare cost management.
HMSprogramsblendwellnessservices that provide healthy
individuals with information and
encouragementtobettermanagetheirhealthriskswithdiseasemanagementthatincreaseschronicallyillpatientscompliancewith
prescribed treatments.
EffectiveHMSprogramsarecharacterized by three common themes:
incentives to ensure
patientparticipation,strategiestoinvolvephysiciansaskeyprogramfacilitators,
and communications and incentives that are tailored to individual
preferences.
-
Booz & Company 3
The rapid economic expansion of the GCC region has brought its
member nations the benefits of advanced developed countrieshigher
stan-dards of living, lower unemployment, and increased purchasing
power. But along with such advantages also come new and pressing
challenges, particularly in the realm of health-care. In recent
years, GCC nations effectively combated typical third world health
challenges such as tuberculosis and malaria. However, due to the
rapid growth and develop-ment of the region and the resultant
change in lifestyles, GCC leaders are now turning their attention
to
an increasing prevalence of chronic diseases among their
citizenry.
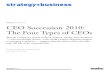
In the typical GCC country today, chronic diseases are a leading
cause of mortality; in 2007, the region was home to four of the top
five nations in the world for diabetes cases among adults (see
Exhibit 1). Based on data available from several GCC geog-raphies,
chronic diseases currently account for approximately 35 percent or
more of the deaths in those regionsfast approaching levels in
developed countries such as the U.S., where chronic diseases
account for an estimated 70 percent of mortalities.
A PRESSING PROBLEM FOR GCC NATIONS
Exhibit 1 Prevalence of Chronic Diseases in the GCC Region
Source:HAADstatistics;WorldHealthOrganization
32%
6%
7%14%
23%
18%
LEADING CAUSES OF DEATH IN ABU DHABI2007
Nauru UAE
16.7%
SaudiArabia
Bahrain Kuwait Oman Egypt USA
PERCENTAGE OF ADULT POPULATION WITH DIABETES BY RANKING2007
7.8%
11.0%13.1%
14.4%15.2%
19.5%
30.7%
Accidents/Injury
Cardiovascular
Cancer
Diabetes
Congenital
Other
-
Booz & Company4
Lifestyle factors in the GCC region have contributed mightily to
this scourge, setting the stage for the creation of a chronic
disease epi-demic. Increasing affluence in GCC countries has caused
a once highly active population to become largely sedentary,
resulting in reduced levels of physical activity, increased smoking
rates, and other unhealthy lifestyle changes. These changes are
triggering heightened obesity rates and inci-dences of
hypertension, key factors that contribute to chronic disease.
Because many of these factors are not addressed before they
mature into chronic diseases, GCC governments are being forced to
dedicate more of their budgets to treat a growing wave of patients.
In the UAE, where one in every five adults is afflicted with
dia-betes, treatment of that illness alone takes up approximately
40 percent of the nations overall healthcare expen-ditures.3 The
burden posed by chronic diseases weighs more heavily on GCC
governments because they shoulder a greater share of healthcare
expen-
ditures than governments in other parts of the world. Public
spending on healthcare averaged 74 percent in GCC countries in
2006, nearly 20 percentage points higher than the global average of
57 percent4 (see Exhibit 2). But the issue also looms large for the
private insurance compa-nies that are entering GCC markets, which
need to keep their costs down to remain competitive.
Exhibit 2 GCC Governments Contribute Significantly More to
Healthcare Costs Than the Global Average
*HDI=HumanDevelopmentIndex;WorldAverageisbasedon177countries;Top30excludesHongKong,forwhichfigureswerenotavailable.
Source: WHO Statistical Information System, 2006 data
Publ
ic E
xpen
ditu
re a
s a
% o
f Tot
al H
ealth
care
Exp
endi
ture
Top 30 HDI* Average = 71%
World Average* = 57%
GCC Average = 74%
SHARE OF PUBLIC EXPENDITURE IN HEALTHCARE 2006
30%
40%
50%
60%
70%
80%
90%
UnitedKingdom
Japan Sweden France Germany Canada Australia Switzerland
Republicof Korea
UnitedStates ofAmerica
China Oman Kuwait SaudiArabia
Qatar UnitedArab
Emirates
Bahrain
-
Booz & Company 5
Needless to say, the rising socioeco-nomic costs of chronic
diseases have caught the attention of GCC govern-ments. Some have
set up government bodies and programs to develop preventative
healthcare strategies and address the low level of health
aware-ness in the region. In many cases involving chronic diseases,
consumers have little knowledge about preven-tion and management of
their condi-tions. For instance, a study about osteoporosis among
educated women in the UAE found that 44 percent of women with at
least a secondary school education had minimal or zero knowledge of
the disease.5
To date, however, such government programs have not been able to
fully address the escalating needs of the GCC regions large and
grow-ing population of chronic disease sufferers. Post-diagnosis,
chronic disease patients have a broad array of clinical and
non-clinical needs associ-ated with managing their condition.
Diabetics, for example, need to continually manage their disease,
on top of identifying and changing the lifestyle factors that
caused it. Their responsibilities include measuring blood glucose
levels, taking insulin shots, and getting regular screenings and
tests.
Typically, chronically ill patients need assistance in four
major elements of their disease management: under-standing the
implications of their dis-ease, such as treatment options, risk
factors, and potential complications; navigating the healthcare
system and communicating with the various care providers,
especially for patients with multiple chronic diseases who must
make multiple visits; gathering information about the various
actions they need to undertake, including self-care, dietary
changes, and exer-cise; and complying with their care regimen, such
as planning multiple provider visits and taking prescribed
medicines.6
Currently, though, such needs are filled only during formal
physician visits or informally by other sources such as family and
friends. These interactions only partially address a chronically
ill patients continuous need for care advice, monitoring, and
compliance. As such, critical gaps in care provision exist before,
between, and after provider visits, particularly when it comes to
identifying high-risk behavior, adhering to a treatment regimen,
patient monitoring, and other elements of care coordination.
ADDRESSING GAPS IN PATIENT CARE
-
Booz & Company6
To close these gaps and improve the overall care of chronically
ill patients, healthcare leaders in some developed economies are
employing HMS, which bundle a prescribed set of healthcare services
into condition-specific programs that are based on scientific
evidence and data analysis. The healthcare services address the
patients needs identified above: risk identification, awareness and
education, adherence to treatment regimen, monitoring health
indicators, and care coordination. The HMS program encourages
individual members to improve their health by creating a support
system that helps them manage their condition, increasing their
awareness, providing critical guidance, and employing incentives to
encourage healthy behavior. HMS also strengthen relationships
between hospitals and their patients and physicians, by creating a
continuous, longitudinal view of patient care that competitors
cannot match.
THE CASE FOR HMS
FACTS AND FIGURES
Obesity:GCCnationsarehometosomeofthehighestobesityratesintheworld.
Thirty percent or more of the adult populations in Saudi Arabia,
the
UAE,Kuwait,andBahrainhaveabodymassindex(BMI)of30ormore,theclinicaldefinitionofobese.InAbuDhabi,theaverageBMIis29amongadults.i
Smoking:GCCcountrieshavearelativelymoderatenumberofsmokers36percentversusaglobalaverageof33percent.Butonapercapitabasis,theirannualintakeofcigarettesismuchhigher,fueledbyhigherconsumptionamongyoungmales.Forexample,theaverageKuwaitismokerconsumesmorethan2,500cigarettesayear,comparedwithaworldwideaverageof900.
Physical Inactivity: At least 40 percent of the GCC population
fails to achieve the minimum daily recommendation of 30 minutes of
moderate-intensity
physicalactivity.Thisrateismorethandoubletheglobalestimateof17percent.ii
Hypertension:
ModernizationhasbeendirectlylinkedtohigherstresslevelsinGCCnations.Roughly34percentiii
of the adult population in Abu Dhabi
hashighbloodpressure,comparedwithjust18percentintheU.S.Statisticsalsorevealahighcorrelationbetweenhypertensionandtheoccurrenceofdiabetes.
-
7Booz & Company 7Booz & Company
As an example, diabetics enrolled in an HMS program designed to
help manage their condition can expect the following services:
Comprehensive diabetes plan including diet, medication,
exercise, and screening
Diabetes articles and the latest research on diabetes
Coordination with provider
Remote consultation and setting of appointments
Diabetic community tools
Glycemic index counter and low glycemic food guide
Medication and screening test alerts
Coaching and intervention-related services are at the core of
HMS programs and they are typically conducted by a call center
staffed by nurses. The call centers contact patients to provide
them with vari-ous services based on the program in which the
patient is enrolled (e.g., information on care regimen, reminders
for screening, coordinat-ing physician visits). Through these
coaching and intervention services, HMS provide consumers with the
information and guidance required while coordinating care in order
to help consumers manage their health and directly address the gaps
in care provision.
By supporting individuals in main-taining their health and
helping chronic patients with their condi-tions, HMS programs have
a direct impact on healthcare costs. Although
such savings are often difficult to quantify, numerous studies
have demonstrated the benefits of HMS on individuals health, as
well as on overall healthcare costs. For instance, a study
published in Health Affairs in 2004 showed an 8.1 percent drop in
hospitalization costs of diabetes patients after they were enrolled
in an HMS program to help manage their treatment.7 A separate
finding published in 2005 in the European Journal of Public Health
found that HMS smoking cessation programs resulted in a 15 percent
to 35 percent quit rate, saving employers (here collectively
referred to as payors) an average of US$11,880 per smoker over
their lifetimes.8
By supporting individuals in maintaining their health and
helping chronic patients with their conditions, HMS programs have a
direct impact on healthcare costs.
-
Booz & Company8
Such success stories have led health insurance companies and
payors to increasingly adopt these services as a way of controlling
their soaring healthcare costs. The HMS industry has been growing
significantly in early adopter markets such as the U.S., where it
has enjoyed a com-pound annual growth rate of more than 25 percent
over the past decade and now enjoys a penetration rate of 5 percent
to 10 percent of total insured lives.9 In recent years, pilot HMS
programs have begun to crop up in Latin America, Europe, and Asia.
Payors especially have found these programs to be beneficial, due
to their positive impact on employee productivity and satisfaction.
Additionally, HMS programs are one of the few options available to
payors that believe that prevention needs to be a key element of
their healthcare cost containment strategy. A recent evolution in
the HMS delivery model has been the integration of Internet-based
platforms, while face-to-face coaching continues to be used to
deliver interventions (see Health Management Goes Online).
HEALTH MANAGEMENT GOES ONLINE
HMSprovidersareincreasinglyleveragingtechnologytoconductdataanalytics,integrateremotemonitoringdevices,andleveragealternativeaccesschannels.Still,itwasntuntilrecentlythatHMSbeganmigratingtoInternet-basedplatforms.Traditionally,healthmanagementprogramsweredeliveredsolelythroughanurseoracoachanexpensivemediumforparlayingservices.Intheinterestofreducingcosts,providershavebeguneffectivelyincorporatingWeb-basedprogramsinconjunctionwithcoachesandnurse-staffedcallcenters.AnotheradvantagetoonlineHMSisitprovidesmoreleewaytopersonalizeprogramelements,whichevidenceshowsincreasespatientsparticipationinandcompliancewithHMSprograms.
Citingtheseadvantages,leadingHMSprovidersaremakingacquisitionsandotherkeyinvestmentstoincorporateInternet-basedmodelsasakeyvehiclefordeliveringHMSprograms.Infact,certainleading-edgeprovidershaveintroducedprogramsthataredeliveredexclusivelyovertheInternet.LeadingHMScompanies,includingHealthwaysInc.andMatriaHealthcare,havemadenotableforaysintoonlineprogramdelivery.Healthwayshasmadesignificant,targetedinvestmentsinthisarea,mainlyfocusedonbuildinganinternaltechnologyteamthatcouldhelpitdeliveranonlineplatformforitsprograms,whileMatria,nowpartofAlereMedical,acquiredonlineHMSproviderWinningHabits.com.Conversely,leadinghealthcareportalssuchasWebMDandRevolutionHealthhavepurchasedcompaniestoaddHMSprogramstotheiralready
popular Web services.
HMS programs are one of the few options available to payors that
believe that prevention needs to be a key element of their
cost-containment strategy.
-
9Booz & Company
screenings and immunizations (e.g., flu shots), and share
information to foster self-care practices. Follow-up support is
provided by on-site, telephone-based, or online coaching assistance
through condition-specific programs such as weight manage-ment,
smoking cessation, and stress management.
Disease-management programs offer a prospective,
disease-specific approach to coordinating the care of high-cost and
high-risk populations with chronic conditions, including dia-betes,
asthma, and congestive heart failure. They typically involve a
coor-dinated set of healthcare interven-tions and communications
designed to support the patientphysician relationship by ensuring
the patients compliance with the prescribed care plan. These
programs focus on keeping conditions from being exacerbated,
through co-morbidities or other complications, by using
evidence-based practice guidelines and strategies to empower
patients.
Both types of HMS program are typically designed around four
major components:
Adoption focuses on understand-ing members or employees needs,
evaluating patients risk profiles through health-risk appraisals,
selecting the appropriate program and pricing strategy, and
encourag-ing adoption through marketing efforts and enrollment
incentives.
Program delivery centers on core intervention elements that are
designed to help the consumer manage his or her condition and
reduce risk factors through a per-sonalized delivery strategy.
Monitoring sets clear performance metrics, measures against
them, and verifies desired outcomes.
Improvement involves modifying the program elements to enhance
the effectiveness of the program.
HMS programs are broadly classified as either wellness programs
or disease management programs. Whereas the latter deals with
patients already afflicted with chronic diseases, the former aims
to reduce risk fac-tors that cause the onset of chronic diseases in
the first place through the pursuit of mental and physical
well-being.
Typical wellness programs provide healthy individuals with
information, support, guidance, and encourage-ment to better manage
their lifestyle-related health risks. First, health-risk
assessments help assign consumers to various risk groups. Then
providers institute preventive measures such as
KEY COMPONENTS OF HMS PROGRAMS
-
Booz & Company10
To be sure, health management is not an exact science, given
that the success of these programs depends to a large extent on
their ability to change behavior. The HMS industry is constantly
innovating to develop new techniques to improve programs ability to
ensure compliance, reduce risk factors, and carry out preventive
screenings and thus deliver on their promised benefits. There are
three key ingredients in successfully deployed HMS programs, all of
which can be leveraged in GCC markets:
Incentives: Well-designed HMS programs provide consumers with a
variety of incentives to ensure partici-pation, such as reduced
premiums, cash incentives, and redeemable reward points akin to
points given by various reward programs. HMS programs are also
using negative incentives such as higher premiums or co-pays for
non-participants. Increasingly, programs are adopt-ing a
combination of bothnegative incentives to ensure enrollment and
positive incentives to effect behavioral change.
Physician Involvement: Coordinating program interventions and
other elements with the patients physi-cian is another critical
facilitator in assuring program efficacy. In a case where drug
adherence is identified as a problem, for instance, involving the
physician isnt just about relat-ing critical information; it
creates an opportunity for the physician to inter-vene and
reinforce the importance of sticking to the drug regimen. Given the
low level of health literacy and
awareness of health issues in GCC countries, there is greater
reliance on physicians by patients, making physician involvement
all the more critical. HMS programs in the region will need to
engage relevant physi-cian groups to obtain their buy-in and ensure
their participation and involvement.
Personalization: Tailoring com-munications and incentives to the
individuals tastes and preferences is a new and evolving trend
credited with increasing patient compliance with HMS programs.
Participants receive personalized letters, educa-tional brochures,
and booklets to increase awareness. Incentives and other aspects of
the plans design are customized to adjust to the individual
participants ability to change. HMS providers are building large
databases of consumer information to document the success of
interventions, incen-tives, and communications, and to leverage
these large data warehouses to personalize their interactions with
other members.
The ways in which these building blocks are used will be
determined by healthcare payors overall HMS strategy, which will
require analysis, judgment, detailed design, and pilot-ing of
alternative concepts, as well as allocation of significant
resources for implementation. Payors will also likely require the
involvement of lead-ing disease management and wellness companies
from mature HMS mar-ketsprimarily the U.S.to ensure that the plan
imperatives highlighted above are incorporated.
PUTTING HMS INTO PRACTICE
-
11Booz & Company
To help jump-start the process and lay a sound foundation for
successful implementation, GCC governments and healthcare
organizations must assess their current overall healthcare strategy
to address a number of stra-tegic questions:
How should HMS programs be integrated into their current
health-care strategic framework?
Which segments of the population will be targeted? How will the
pro-gram design be modified to address the cultural characteristics
of the population?
Which HMS programs would be most relevant for GCC
populations?
What incentives will be required to ensure significant program
adop-tion among targeted segments?
How will health management ser-vices be funded? How will the
costs (and risks) be distributed among the various
stakeholders?
What would be the financial and health status objectives of HMS
programs? Should GCC govern-ments support these programs if the
financial return on investment is not clear but there is a positive
impact on the health status of the population? What will be the
role of healthcare providers and health insurance companies?
Through which entity will the programs be offered? Will it be a
publicprivate partnership between a GCC government and an
interna-tional disease management/wellness company, or will it be
an entirely private undertaking?
What policy initiatives will be required to support HMS
rollout?
How will GCC governments ensure that other healthcare
stakeholders, primarily providers, support the rollout of the HMS
programs?
What will be the role of e-health in delivering HMS to the
population?
CONCLUSION
-
Booz & Company12
How will the execution of HMS programs be managed across various
governmental authorities? What are the critical factors for the
successful execution and rollout of HMS programs?
Chronic disease management is an issue that GCC nations can ill
afford to ignore. Countries that fail to address this pressing
concern run a real risk of being engulfed in a chronic disease
epidemic, resulting in reduced health status, crippling healthcare
costs, lower workforce
productivity, and immense strain on the healthcare system.
Well-crafted HMS programs are a valuable tool that can help GCC
nations stem the rising tide of chronic diseases by helping to
identify unhealthy and risky behaviors, raise awareness of
underlying lifestyle fac-tors, improve adherence to treatment
regimens, and strengthen the bonds between patients and physicians.
Now is an opportune time for GCC nations to adopt HMS programs as
most GCC nations are undertak-
ing significant investments in their healthcare systems. Indeed,
rapid implementation of such programs is within grasp for smaller
markets in the region.
As GCC nations prime for a robust economic recovery, their
leaders will need to put a premium on smart growth strategies. When
it comes to managing the populations most serious and costly
illnesses, there is no smarter healthcare strategy than HMS.
-
13Booz & Company
About the Authors
Ramez Shehadi is a partner with Booz & Company in Beirut. He
leads the
informa-tiontechnologypracticeintheMiddleEast.Hespecializesine-government,e-business,andtechnology-enabledtransfor-mation,helpingbothprivatecorporationsandgovern-mentorganizationsleveragetechnology,achieveoperationalefficiencies,andimprovegovernance.
Ali Hashemi is a principal with Booz & Company in Dubai and
a leader in the healthcare practiceintheMiddleEast.He specializes
in business strategyforplayersthroughoutthe healthcare value chain,
as
wellasadvisinggovernmententitiesondefiningtheiroverallhealthcareagendas.
Walid Tohme is a principal with Booz & Company in Beirut and
a leader in the information
tech-nologypracticewithafocusonhealthcare. He specializes in
themanagementandstrategicuseoftechnologytoenablethetransformation
of healthcare organizations,services,andinfrastructure.
Jad Bitar is a senior associate with Booz & Company in
Beirut and a leader in the informa-tiontechnologypracticewitha
focus on healthcare. He specializes in healthcare and
businesstechnology,par-ticularlystrategy,organization,operations,
and innovation.
Endnotes
1 The Gulf
CooperationCouncilconsistsofBahrain,Kuwait,Oman,Qatar,SaudiArabia,andtheUnitedArabEmirates.2WHOMortalityFactSheetforSaudiArabia(2006)andQatarMinistryofHealthstatistics.3TreatmentofDiabetesaBigDrainonNationalHealthcareBud-get,Gulf
News,November11,2007.4 WHO Statistical Information System, 2006
data.5HaiderM.AlAttia,AmalA.AbuMerhi,andMahaM.AlFarhan,HowMuchDotheArabFemalesKnowaboutOsteoporosis?TheScopeandtheSourcesofKnowledge,Clinical
Rheumatology, vol. 27, no. 9, September 2008, 11671170.
6Apresumablysimpleelementofthecomplianceregimen,adherencetoprescribeddrugregimen,suffersfromalargenoncompliance
rate.
7 Victor
G.VillagraandTamimAhmed,EffectivenessofaDiseaseManagementProgramforPatientswithDiabetes,Health
Affairs, vol. 23, no. 4, 2004,
255266.8SusanneR.Rasmussen,EvaPrescott,ThorkildI.A.Srensen,andJesSgaard,TheTotalLifetimeHealthCostSavingsofSmokingCessationtoSociety,European
Journal of Public Health, vol. 15, no. 6, December 2005.9 Booz
& Company
estimates.iHealthAuthorityAbuDhabi(HAAD)statistics.iiWorldHealthOrganizationandOxfordHealthAlliance;theratesforphysicalinactivityinUAEwereforthetopandbottomquintilesof
income class.iii HAAD statistics.
-
2009 Booz & Company Inc.
Booz & Company is a leading global management consulting
firm, helping the worlds top businesses, governments, and
organizations. Our founder, Edwin Booz, defined the profession when
he established the first management consulting firm in 1914.
Today, with more than 3,300 people in 59 offices around the
world, we bring foresight and knowledge, deep functional expertise,
and a practical approach to building capabilities and delivering
real impact. We work closely with our clients to create and deliver
essential advantage.
For our management magazine strategy+business, visit
www.strategy-business.com. Visit www.booz.com to learn more about
Booz & Company.
The most recent list of ourofficeaddressesandtelephone numbers
can be found on our website, www.booz.com
Worldwide Offices
AsiaBeijing DelhiHongKongMumbaiSeoulShanghaiTaipeiTokyo
Australia, New Zealand & Southeast
AsiaAdelaideAucklandBangkokBrisbaneCanberraJakartaKualaLumpurMelbourneSydney
EuropeAmsterdamBerlinCopenhagen
DublinDsseldorfFrankfurtHelsinkiLondonMadridMilanMoscowMunichOsloParisRomeStockholmStuttgartViennaWarsawZurich
Middle EastAbu DhabiBeirutCairoDubaiRiyadh
North
AmericaAtlantaChicagoClevelandDallasDetroitFlorhamParkHoustonLosAngelesMcLean
MexicoCityNewYorkCityParsippanySanFrancisco
South AmericaBuenos AiresRio de JaneiroSantiagoSo Paulo