Embed Size (px)
Citation preview

Department of Thoracic and Cardiovascular Surgery, Stanford University School of Medicine, Stanford, CA.
Department of Cardiovascular Physiology and Biophysics, Palo Alto Medical Foundation Research Institute, Palo Alto, CA.
Department of Biomedical Engineering, Texas A&M University, College Station, TX.
Alterations in Transmural Borderzone Strains during
Acute Mid-Circumflex OcclusionFiliberto Rodriguez, Frank Langer,
Katherine B. Harrington, Allen Cheng, George T. Daughters, John C. Criscione,
Neil B. Ingels Jr., D. Craig Miller

Non-ischemic infarct borderzone expansion may be important in the progression of ischemic cardiomyopathy.
Alterations in myocyte strain patterns:– Trigger production of reactive oxygen species– Stimulate myocyte apoptosis – Activate matrix metalloproteinases (MMPs)
Introduction

Characterize the abrupt alterations in transmural systolic strains during
acute ischemia that underlie LV borderzone remodeling, with emphasis
on fiber-sheet mechanics.
Purpose

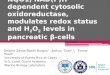
How does the LV wall thicken > 40%,when fibers shorten only 15% and thicken
only 8%?
Understanding Wall Thickening

Streeter DD et al, Circ Res 1969; 24:339-47
Epi Endo
Transmural Fiber HelicesEpicardial Counter-Spiral Fiber
Circumferential Midwall Fiber
Endocardial Spiral Fiber

Spotnitz HM et al, J Mol Cell Cardiol 1973;6:317-31
Transmural Fiber Rearrangement

< 0
Sheet shear, thickening, and extension allow systolic wall thickening of > 40%
Costa KD et al, Am J Physiol 1999;276:H595-H607
Radial Wall-Thickening
Xn Xs
XnXs
Sheet shear(Esn < 0)
Sheet extension(Ess > 0)
Sheet thickening(Enn > 0)
Transmural Sheet Model

Fiber and sheet strains are altered in the borderzone between acutely ischemic
and non-ischemic myocardium.
Hypothesis

9 SheepLeft ThoracotomyCPBGlobal LV Marker Array

circumferential
longitudinal
radial
endocardium
epicardium

Video Recording
3-D reconstruction
LAO View RAO View
LVP
dP/dtECG
RAOLAO

Acute Mid-Circumflex Occlusion

Quantitative Microstructural Measurements

Cardiac coordinate system
longitudinal (X2)
circumferential (X1)
radial (X3)
Quantitative Microstructural Measurements

Cardiac coordinate system
Fiber-sheet coordinate system
fiber (Xf)
sheet (Xs)
normal (Xn)
-
- fiber angle sheet angle
longitudinal (X2)
circumferential (X1)
radial (X3)
Quantitative Microstructural Measurements

3-D Model of Wall Thickening Mechanics

Results
Baseline Ischemia p HR (b/min) 101 ± 15 101 ± 16 0.37
dP/dtmax (mmHg/s) 2310 ± 691 1600 ± 541 0.0005 EDV (mL) 213 ± 50 229 ± 46 0.02 ESV (mL) 156 ± 51 181 ± 49 0.0006
EDP (mmHg) 20 ± 4 24 ± 6 0.05 ESP (mmHg) 72 ± 7 56 ± 8 0.00003
LVPmax (mmHg) 104 ± 10 86 ± 13 0.0001
Hemodynamics

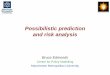
Defining the functional borderzone
Systolic Fractional Area Shortening
Annular
Basal
Equatorial
Apical
Antero-septal
Antero-lateral
Postero-lateral
Postero-septal

Antero-septal
Antero-lateral
Postero-lateral
Postero-septal
14 ± 3p=0.10
13 ± 5*p=0.02
28 ± 4p=0.14
20 ± 7*p=0.05
11 ± 4*p<0.01
14 ± 6*p<0.01
22 ± 6p=0.32
23 ± 4*p=0.03
18 ± 8p=0.24
13 ± 5p=0.20
IschemiaAntero-septal
Antero-lateral
Postero-lateral
Postero-septal
15 ± 5 17 ± 2
27 ± 7 23 ± 7 20 ± 5 21 ± 7
27 ± 8 23 ± 7 20 ± 5 23 ± 4
21 ± 5 20 ± 6 16 ± 7 20 ± 3
Baseline
17 ± 5†p=0.06
17 ± 7*p<0.01
30 ± 6*p<0.01
12 ± 4*p<0.01
Annular
Basal
Equatorial
Apical
Systolic Fractional Area Shortening

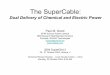
Altered Borderzone Cardiac Strains
circumferential
Increased circumferential-radial shear:Subepicardium 0.04±0.04 vs. 0.11±0.05, p=0.002Midwall 0.03±0.04 vs. 0.07±0.04, p=0.0004
ED
ES
radial
endo epi endo epi
circumferential
radial
IschemiaBaseline

Altered Borderzone Fiber-Sheet Strains
fiber
sheet
fiber
sheet
ED
ES
Decreased subendocardial fiber shortening: -0.06±0.06 vs. 0.00±0.07, p=0.02Increased subendocardial fiber-sheet shear: 0.07±0.01 vs. 0.11±0.04, p=0.04
IschemiaBaseline

Summary
Increased subepicardial and midwall circumferential-radial shear.
Acute ischemia altered transmural borderzone:
Cardiac Strains
Reduced end-systolic subendocardial fiber shortening.Increased subendocardial fiber-sheet shear.
Fiber-Sheet Strains

Implications
the perturbations we observed in the non-ischemic borderzone may be responsible for progression of ischemic cardiomyopathy.
Are remodeling processes triggered by these fiber and sheet strain alterations?
Assuming cardiac microstructure is optimally designed for normal strain patterns,