Embed Size (px)
Citation preview

Bowel Preparation RegimensDanielle Goodrich, MSIVUniversity of Maryland School of Medicine

Overview
•Colorectal Cancer•Bowel Preparation Regimens•Survey
2

Colorectal Cancer
•Third most common cancer•Second leading cause of cancer-related
deaths•Screening colonoscopy has been shown to
reduce mortality▫U.S Preventive Services Task Force
recommends Colorectal Cancer Screening for those aged 50 years and above with average risk
USPSTF 2009
3

Adequacy of Colonoscopy Depends on Prep
4

Adequacy of Colonoscopy
•Up to 25% of patients undergoing colonoscopy have poor bowel preparation▫Lowers the detection of small polyps
(<9mm)▫Increased risk of procedural complications▫Decreased completion rates▫Increases the time the endoscopist takes to
try to suction and clean the colon
Van Dongen 2011
5
Liquid coming from the bowel before colonoscopy should look like….
6

Different Dosing Regimens
Split-Dose
Traditional
Same Day
Time of day
7
Split-Dose
•Superior to full-dose PEG with respect to▫Colon Cleansing▫Patient compliance▫Patient’s willingness to repeat the same
bowel preparation ▫Nausea
Kilgore et al 2011
8
Survey of Local CRF Programs in Maryland•13 questions aimed to identify practice
habits of endoscopists involved in the program
•Program managers in each county of Maryland who work directly with endoscopists through the statewide Cigarette Restitution Fund Colorectal Cancer Screening Program
9

Survey Results: Client Education
10
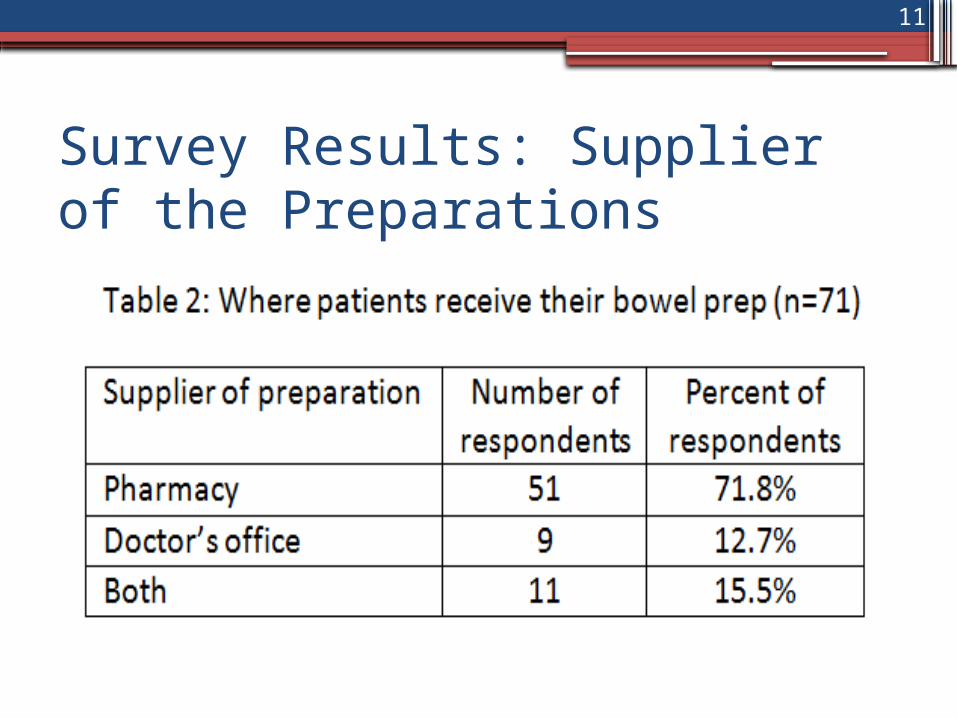
Survey Results: Supplier of the Preparations
11
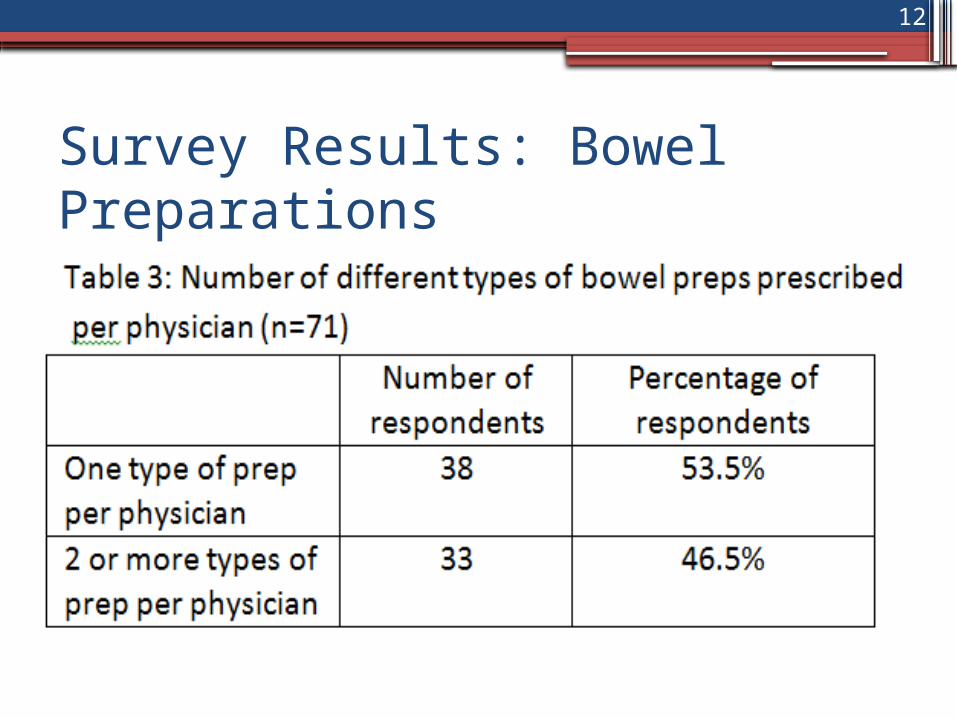
Survey Results: Bowel Preparations
12
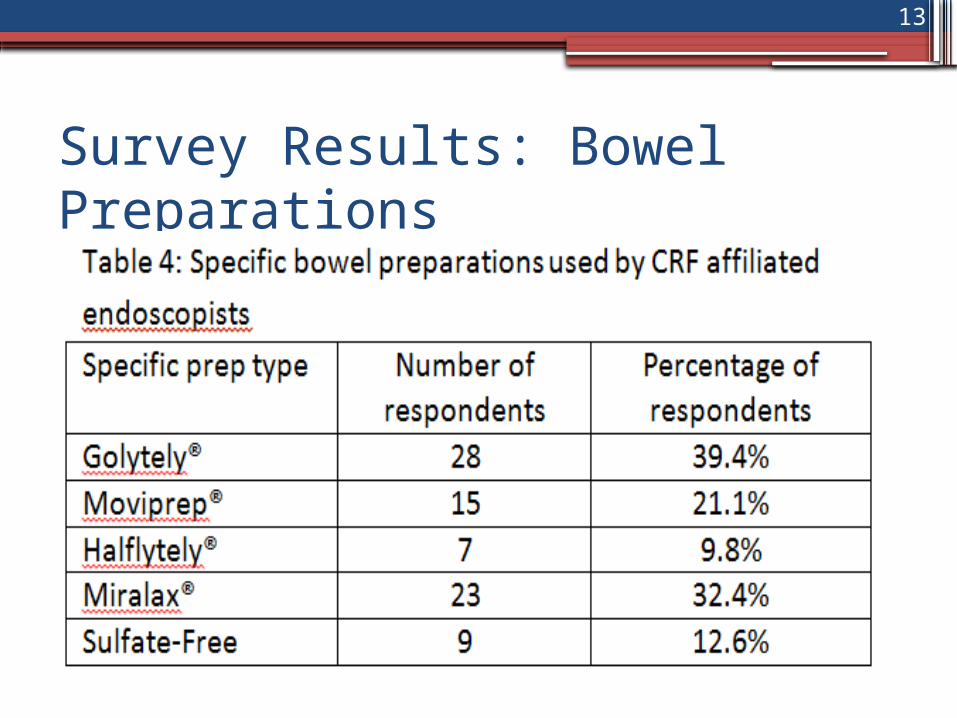
Survey Results: Bowel Preparations
13
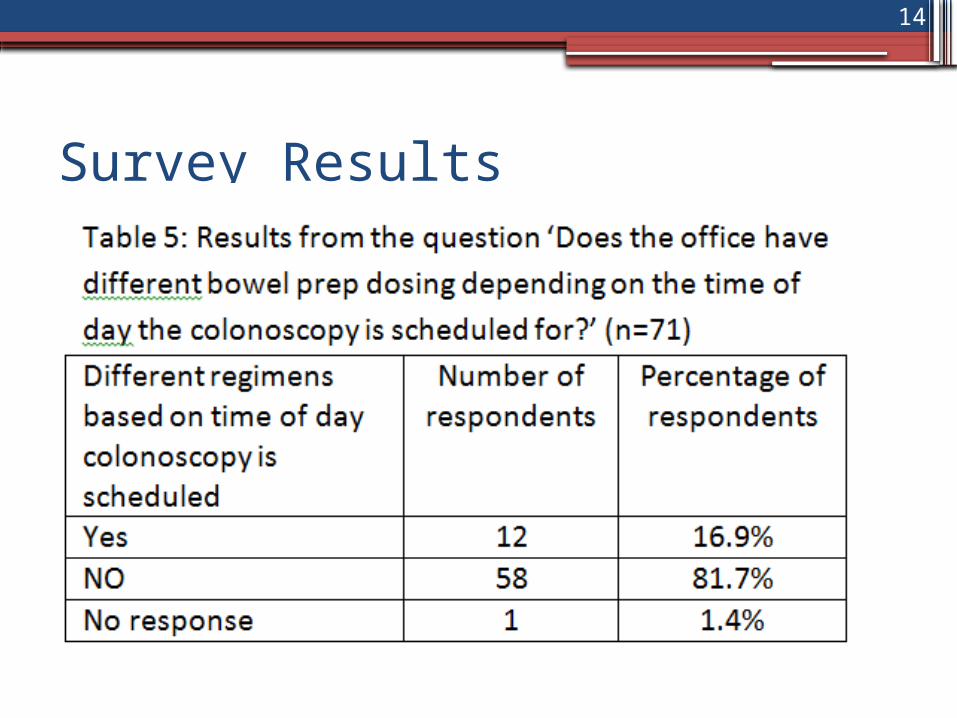
Survey Results
14
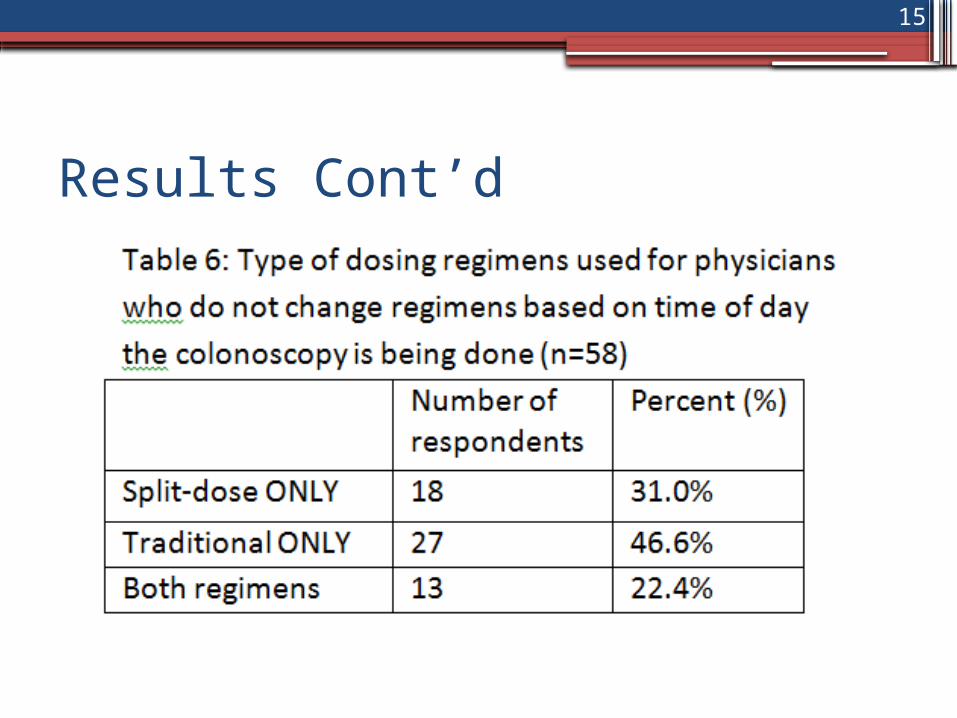
Results Cont’d
15

Conclusions
•Physicians are implementing split dose regimens into their practice.
•Physicians are using different bowel preps for different patients, suggesting they are taking into account the patients past medical history and ability to complete the various regimens.
16
Conclusion
•The literature suggests that split-dose regimens:▫Improve quality of the study▫Reduce cost and complications▫Are more favorable to the patient
17

Information for the screening programs:•Please encourage your providers to use
split-dosing regimens if not using split dose currently
•Please disseminate our “Information to the Provider” handout to the endoscopists in your program
18

Acknowledgements
•Many thanks to the program managers in the Cigarette Restitution Fund colorectal cancer screening program at the local health departments in Maryland who collected and submitted the data for this survey
•Maryland DHMH Center for Cancer Prevention and Control
19

References • Monica Van Dongen. Enhancing Bowel Preparation for Colonoscopy.
Gastroenterology Nursing (2012) 35;36-44.• Dwyer DM et al. Experience of a public health colorectal cancer
testing program in Maryland. Public Health Reports (2012)127:330-339.
• Unger RZ et al. Willingness to Undergo Split-Dose Bowel Preparation for Colonoscopy and Compliance with Split-Dose Instructions. Dig Dis Sci (2010) 55:2030-2034.
• Di Palma J and Rex D. Advances in Bowel Preparations. Gastroenterology Nursing (2011) 55:S2-S8
• Kilgore et al. Bowel Preparation with split-dose polyethylene glycol before colonoscopy: a meta-analysis of randomized controlled trials. Gastrointestinal Endoscopy (2011) 73:1240-1245.
• Longcroft-Wheaton G and Bhandari P. Same-Day Bowel Cleansing Regimen is Superior to a Split-Dose Regimen over Two Days for Afternoon Colonoscopy. J Clin Gastroenterol (2012)46:57-61
20