Embed Size (px)
Citation preview

BPIP Best Practice
Intervention PackageCross Setting I
This material was prepared by Quality Insights, the Medicare Quality Innovation Network-Quality Improvement Organization supporting the Home Health Quality Improvement National Campaign, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department
of Health and Human Services. The views presented do not necessarily reflect CMS policy. Publication number 11SOW-WV-HH-MMD-010517BPIPI
Best Practice Intervention Package
Cross Setting
This material was prepared by Quality Insights, the Medicare Quality Innovation Network-Quality Improvement Organization supporting the Home Health Quality Improvement National Campaign, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department
of Health and Human Services. The views presented do not necessarily reflect CMS policy. Publication number 11SOW-WV-HH-MMD-010517
Cross Setting I

Acknowledgements The Home Health Quality Improvement Campaign would like to thank everyone who contributed to the Cross Setting I Best Practice Intervention Package (BPIP), including the following individuals and organizations for their contributions as our Technical Expert Panel.
Donna Anderson, Ph.D., RN, CCP-C, Care Transitions Project Coordinator, Quality Insights of PA Patrick Archambeault, RN, MS, CRNI, Director of Clinical Specialties, Eddy Visiting Nurse Association Mara Benner, Vice President, Government Affairs – Gentiva Health Services Cindy Bigbee, RN, MSN, Care Transitions Quality Improvement Consultant, TMF Health Quality Institute Deborah Chisholm, RN, BSN, CPHQ, COS-C, Senior Associate Consultant, OASIS Answers, Inc Margaretta Dorey, RN, BSN, Patient Safety Project Lead, Quality Insights of Delaware Sherry Dukes, RN, COS-C, HCS-D, National Director Quality & Outcomes Education, Quality Management & Analytics, Amedisys Jettie Eddleman, BSN, RN, Team Member, Director of Clinical Quality Outcomes Cher Edmonds, MS, CHES, SSW, Project Coordinator - HealthInsight Dennee Frey, PharmD, Project Consultant, Medication Management Information System (MMIS), Partners In Care Foundation Barbara Goodman, RN, BSN, MSN, CHCE, COS-C, HCS-D, Vice President of Quality LHC Group Melinda Huffman, BSN, MSN, CCNS, CHC, Principal, Miller & Huffman Outcome Architects, LLC Misty Kevech, RN, BS Ed, MS, COS-C, Director of Nursing Education and Program Development - Celtic Home Care Linda Krulish, PT, MHS, COS-C, OASIS Answers, Inc. Margherita Labson, RN, MSHSA, CCM, CPHQ, CGB, Executive Director, Home Care Program, The Joint Commission Judith L. Miller, MS, RN, Quality Improvement Specialist, Healthcare Quality Strategies, Inc. Mary Naylor, PhD, RN, FAAN, Director of the New Courtland Center for Transitions and Health at the University of Pennsylvania, School of Nursing Teresa Northcutt, RN, BSN, COS-C HCS-D, Program Manager, Primaris Deborah Perian, RN MHA, Manager of Clinical Leadership, Skilled Visit Services, Bayada Nurses Mary Perloe, RN, MS, GNP-BC, Manager CMS Care Transitions Initiative, Georgia Medical Care Foundation Laura E. Peterson, BSN, SM, Health Care Consultant Mary St. Pierre, RN, BSN, MGA, Vice President for Regulatory Affairs, National Association for Home Care and Hospice Laurie Reische, BS, CHAMP Program Manager, Visiting Nurse Service of New York Colleen M. Rose, PT, COS-C, Quality Manager VNA of RI Carol Siebert, MS, OTR/L, FAOTA, The Home Remedy Monica Smith, Deputy Director - Home Care Association of Florida Paula Suter, RN, MA, Director, Center of Excellence for Chronic Care Management, Baptist Home Health Network/ 2020 Health Solutions Thomedi Ventura, MS, MSPH, Health Data Analyst, Evaluator, Colorado Foundation for Medical Care
A special thanks to additional reviewers of the Cross Setting I BPIP. Cynthia Pamon, RN, BSN, MS, CCM, HHQI National Campaign Government Task Leader, Office of Clinical Standards and Quality, Centers for Medicare & Medicaid Services Robin Dowell, RN, BSN, Nurse Consultant - Quality Measurement and Health Assessment Group, Office of Clinical Standards and Quality, Centers for Medicare & Medicaid Services
- 2

Debora A. Terkay, RN, MS, Nurse Consultant - Home Health and Hospice, Survey and Certification Group, Division of Continuing Care Providers, Centers for Medicare & Medicaid Services, State Operations (CMSO)
Physician Advisory Panel Justin V. Bartos III, MD – American Academy of Family Physicians Delegate, Congress of Delegates and Commission on Practice Enhancement, Private Practice Family Physician and Administrative Physician
Eric Coleman, MD, MPH- Professor of Medicine, Divisions of Health Care Policy and Research and Geriatric Medicine at the University of Colorado, Denver. Director of the Care Transitions Program
Andrew Cole Eisenberg, MD, MHA – American Academy of Family Physicians
Jay Gold, MD, JD, MPH – Metastar – (Wisconsin QIO) , Senior Vice President and Medicare Chief Medical Officer
E. Rodney Hornbake, MD, FACP – Private Practice of Internal Medicine and Geriatrics, Chief Medical Officer (consulting role) for Gentiva Health Services
Steve Landers, MD, MPH - Medical Director, Center for Home Care and Community Rehabilitation, Cleveland Clinic Foundation
James E. Lett II, MD, CMD –Chairman, AMDA CPG Workgroup for Care Transitions in the Long-Term Care Continuum, Chief Medical Officer for Long-Term Care California Prison Health Care Services, Sacramento, CA
Cathy Newhouse – Senior Vice President of Sales and Clinical Programs – Almost Family – Alliance for Home Health Quality and Innovation
Joseph G. Ouslander, MD - Professor of Clinical Biomedical Science, Associate Dean for Geriatric Programs, Charles E. Schmidt College of Biomedical Science, Executive Editor of Journal of the American Geriatrics Society
Mark V. Williams, MD, FACP, FHM - Professor & Chief, Division of Hospital Medicine, Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST®, Society of Hospital Medicine
Steven L. Yount, DO, Solo Family Practitioner, Clinical Assistant Professor, Adjunct, Department of Family Medicine, University of North Texas Health Science Center, Texas College of Osteopathic Medicine
HHQI Team
Shanen Wright, HHQI Campaign Director Cynthia Pamon, RN, BSN, MS, CCM, Government Task Leader, CMS
Eve Esslinger, RN, BSN, MS, COS-C, Lead Project Coordinator Cindy Sun, MSN, APRN, Project Coordinator David Wenner, DO, FAAFP, Medical Director Bethany Knowles, Communications Specialist
- 3

Table of Contents
ACKNOWLEDGEMENTS 2
TABLE OF CONTENTS 4
QUICK START GUIDE 5
LEADERSHIP 9
FOCUS ON CARE TRANSITIONS AND COACHING 12
SKILLED NURSING TRACK: FOCUS ON CARE TRANSITIONS 74
THERAPY TRACK: FOCUS ON CARE TRANSITIONS 75
MEDICAL SOCIAL WORKER TRACK : FOCUS ON CARE TRANSITIONS 76
HOME HEALTH AIDE TRACK: FOCUS ON CARE TRANSITIONS 77
REFERENCE AND RESOURCE LIST 78
- 4

Quick Start Guide QUICK START GUIDE: A brief guide and introduction to the Best Practice Intervention Package (BPIP) contents.
INTRODUCTION: A brief introduction to the topic of the Cross Setting I BPIP*-- Care Transitions and aligning/working with other health care providers.
LEADERSHIP TRACK (PAGE 9): Designed for agency leadership and the quality or implementation team. Although this section is designed for leadership and the implementation team, it is divided in sections so that it can be printed and shared with other staff.
Contents include: • Care Transitions Information for Leadership • Suggested Timeline for BPIP • Focus on Care Transitions and Coaching • Checklist for Agency Leadership (Select interventions) • Tools and Resources • Links to Success Stories • Organizational Culture • Physician Perspective
DISCIPLINE TRACKS: These 1-page guides are designed for the following disciplines: • Skilled nurse (also on page 74) • Therapist (also on page 75) • Medical social worker (also on page 76) • Home health aide (also on page 77)
The content is very similar between the discipline tracks since they are designed to be interdisciplinary. Each will include discipline specific best practice(s) and checklist. We suggest printing front/back for ease of distribution or sending electronically to staff.
My HHQI offers a collection of resources you can use to connect with campaign organizers, experts, other participants and supporters. Take advantage of these Social Networking opportunities. For Quick Tips and Fun Facts to share with your staff, see the HHQI blog.
ASSOCIATED RESOURCES includes supportive resources for the topic of this BPIP. In addition to the resources in this package, links to a number of important additional resources are provided on the Cross Setting I BPIP webpage. For a complete listing of tools see pages 45-48. This toolbox logo indicates tools and resources.
*There will be three Cross Setting BPIPs. Each will address pertinent topics about transitions and more efficiently managing patients in all provider settings.
- 5

Hospitals
Home Health
Agencies
PhysicianOffices
NursingHomes
Stakeholders (local, state
and national)
Home Health
Agencies
CommunityBased
Services
INTRODUCTION The goals of the Cross Setting I Best Practice Intervention Package (BPIP) are to: • Provide home care leaders with guidance for
selecting best practices for improving care transitions and aligning with other health care providers to work together to decrease avoidable hospitalizations and improving quality of care.
• Provide clinicians with best practice tools and resources to assist them with improving care transitions for their patients.
The Cross Setting I (October 2010), Cross Setting II (January 2011) and Cross Setting III (April 2011) BPIPs focus on improving care across provider settings and more efficiently managing patients in all provider settings.
DID YOU KNOW? • Almost one-fifth of the Medicare beneficiaries who had been discharged
from an acute care facility were rehospitalized within 30 days, and 34.0% were rehospitalized within 90 days (Jencks, Williams, and Coleman, 2009).
• “Nearly 90% of readmissions are unplanned and potentially preventable, which translates into $17 billion or nearly 20% of Medicare’s hospital payments” (Hernandez et al., 2010).
• Heart failure is the most common diagnosis associated with 30-day readmission among Medicare beneficiaries (Hernandez et al., 2010).
• There have been increases in 30-day readmission rates for patients admitted with Heart Failure during the past 14 years. This is accompanied with reduction in length of stay and in-hospital mortality, with less marked reductions in 30-day mortality (Bueno et al., 2010).
• The costs for hospital care and rehospitalizations increases with the number of different chronic conditions (Friedman, Jiang, and Elixhauser, 2008).
• The National Quality Forum (NQF) has endorsed 10 performance measures and 25 preferred practices for care coordination. The endorsement is a step toward achieving the goals of the care coordination priority area set out by the National Priorities Partnership to transform healthcare.
CCOONNSSIIDDEERR the unmet needs of patients/caregivers, medication errors and other patient safety issues that
- 6
“By meeting regularly we have a better understanding of each other roles and challenges.”
Susan Ambrosy, Quality Manager Seton Health Home Care Troy, NY

occur during transitions (often as a result of lack/poor communication between health care providers), and the impact of a hospitalization on a patient and their family. Furthermore think about the patient/caregiver frustration if the hospitalization, the medication error, and/or the patient discomfort could have been prevented.
CARE TRANSITONS
National and local efforts to improve care delivery at transitions between settings are being developed and implemented. Improving care transitions is a significant part of decreasing avoidable hospitalizations. The time of transitions between care settings is targeted because of the potentially harmful situation to the patient, the frequent breakdown in communications between health care providers, and the need for clear communication between the health care professional and patient/caregiver. Studies have shown that targeted interventions at transitions can reduce readmissions (Naylor, 2004 and Coleman, 2009).
As a result of these studies, several readmission intervention models have emerged. Some have gained more attention that others and include the following:
• Transitional Care Model: The Transitional Care Model (TCM) provides comprehensive in-hospital planning and home follow-up for chronically ill high-risk older adults hospitalized for common medical and surgical conditions. The use of advanced practice nurse-centered discharge planning and home care intervention for at-risk hospitalized elders reduced readmissions, lengthened the time between discharge and readmission, and decreased the costs of providing health care (Naylor et al., 1999). References for TCM can be found at the end of this BPIP: (References) and on the TCM website: Transitional Care Model
• Project RED: The Project RED model implemented a nurse discharge advocate during the hospital stay to arrange follow-up appointments, confirm medication reconciliation, and conduct patient education with an individualized discharge booklet that was sent to the primary care provider. Additionally, a follow-up telephone call to the patient was made by a clinical pharmacist 2 to 4 days after discharge. Project RED was shown to reduce hospital utilization within 30 days of discharge (Jack et al., 2009). Project RED
• Care Transitions Intervention: The Care Transitions Program SM
is under the leadership of Dr. Eric Coleman. During a four-week program, patients with complex care needs and their family caregivers receive specific tools and work with a “Transitions Coach” to learn self-management skills that will ensure their needs are met during the transition from hospital to home. Patients who received this program were
- 7

significantly less likely to be readmitted to the hospital, and the benefits were sustained for five months after the end of the one-month intervention. Thus, rather than simply managing post-hospital care in a reactive manner, imparting self management skills pays dividends long after the program ends. The Care Transitions Program
In addition to the care transition improvement models identified above, many tools and resources have been developed to assist in these efforts. While the primary audience of the BPIPs is home health agencies, the resources and guidance can be used by all healthcare providers. For example, the Discharge/Transfer Nursing Summary Note is a multi-provider tool. This tool is ideally used during patient transitions of care. Additionally, SBAR, a communication-briefing tool, is a featured tool and appropriate for clinicians in all provider settings (see page 45-48 for a listing and a description of all tools).
- 8

Leadership The Cross Setting I BPIP will support you with either initiating or enhancing care transition improvement in your community. This BPIP provides insights and success stories from home health agencies that have implemented coaching, and includes excerpts and guidance from many leaders involved with the improvement in care transitions and the reduction of 30-day avoidable readmission rates. This BPIP also highlights the work of the Care Transitions Quality Improvement Organization (QIO) Project which includes 14 QIOs. The Care Transitions QIO Project focuses on improving coordination across the continuum of care. In particular, QIOs promote seamless transitions from the hospital to skilled nursing care, home health care, or home. Additionally, QIOs work to reduce unnecessary readmissions to hospitals that may increase risk or harm to patients and cost to Medicare.
This BPIP will review best practices associated with care transitions. Features of the BPIP include a Focus on Care Transitions which includes excerpts from leaders at National Transitions of Care Coalition (NTOCC), Health Sciences Institute (HSI), the Transitional Care Model (TCM), the Care Transitions QIO Project, and many others. The four success stories focus on agencies: • Improving communication with physician groups • Meeting regularly with community providers • Implementing a coaching model • Using a personal health record to improve patient adherence.
Insights are also provided throughout the BPIP from agencies that are part of the Care Transitions QIO Project. Everyone is encouraged to use the lessons learned from the Insights and Success Stories.
WHY IS THE IMPROVEMENT OF CARE TRANSITIONS IMPORTANT TO HOME CARE?
First, the importance of reducing avoidable hospitalizations has been a quality concern for several years for home care agencies and other providers. In fact, for Medicare beneficiaries, nearly 18% of hospitalizations resulted in a readmission within 30 days. The national home health acute care hospitalization (ACH) rate has hovered around 28-29% for several years. An improvement in this rate by a few percentage points would make a big impact on health care quality and expenditures. Secondly, included in the financing health care reform are bundled payments for hospitalization and certain post-acute care into one payment. Bundled payment is defined as making a “single payment for all services related to a treatment or condition, possibly spanning multiple providers in multiple settings” (Rand Compare). Hospitals with high patient readmission rates within 30 days of discharge will be paid less.
- 9

This is a time that home care agencies need to step forward and demonstrate what we do. Home care agencies need to communicate with other providers that we coordinate care from the patient’s home, are accountable to ensure a safe transition for the patient, and provide quality care in the patient’s home. We must seize this opportunity to show the value of home health services.
How does an agency know if they are improving in care transitions? • Continue to work on and monitor agency acute care hospitalization rate • Be proactive and evaluate the ‘near misses’—those that didn’t result in
hospitalization but could have • Evaluate staff with low and high patient hospitalization rates—not to be
punitive but to learn from each other • Set goals and focus on improving or sustaining your targeted rate • Understand the impact of comorbidities while working to decreasing
rehospitalizations and improving care coordination • Recognize that the attention of better transitional care processes during an
acute episode of care can interrupt the illness trajectory and result in longer-term, positive outcomes—
“Patients see us as one organization— beyond 30 days the more knowledgeable you are about their hospital stay means more to the CARE TRANSITIONS:TERMS patients.”
The National Transitions of Care Coalition Susan Ambrosy, Quality Manager (NTOCC) has identified communication Seton Health Home Care as the main driver for improving Troy, NY transitions of care. NTOCC identifies six key elements to an effective transition of care. • Sender: The health care professional who is accountable for the
sending of key information necessary to ensure continuity of care.
• Receiver: The health care professional who is accountable for receiving the key information (usually at the next care setting) shared by the sender about the patient undergoing transition.
• Key Information: Critical information (such as most up to date medical history, medical diagnosis, medication list, time of most recent pain medication or antibiotic, discharge instructions, results from tests/procedures) available in a clear, complete, and timely manner.
• Action: Obligations and tasks the Receiver of the key information must execute in a timely manner to maintain continuity of care and services for the patient.
- 10

• Verification: A necessary action by the Sender to ensure the key information sent has been appropriately received and acknowledged by the intended health care professional.
• Clarification: A necessary action by the Receiver to ensure the transition information is clear and if concerns are present enables the Receiver to pose questions to the Sender, in order to proceed with appropriate patient-centered care (Tahan, 2009).
The following are additional terms associated with Transitional Care.
• Transitional care: The term that encompasses transitional care is “defined as a set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location. Representative locations include (but are not limited to) hospitals, subacute and postacute nursing facilities, patients’ homes, primary and specialty care offices, and longterm care facilities. Ideally, transitional care is based on a comprehensive plan of care and the availability of healthcare practitioners who are well trained in the care of complex acute and chronic illness and have current information about the patient’s goals, preferences, and clinical status. It includes logistical arrangements, education of the patient and family, and coordination among the health professionals involved in the transition. Transitional care, which encompasses the sending and the receiving aspects of the transfer, is essential for persons with complex care needs and their caregivers.” Position Statement of The American Geriatrics Society Health Care Systems Committee (Coleman & Boult, 2003).
Health coaching • Care Transitions: The actual experience of the encompasses five principal
roles: care recipients. 1) Providing self-management support
• Personal Health Record: Either a written or 2) Bridging the gap between electronic record the patient owns and updates which clinician and patient contains medications, diagnoses, hospitalizations, and 3) Helping patients navigate
the health care system other appropriate medical information. 4) Offering emotional support
• Health Coach/Navigator: Clinician acts as a health 5) Serving as a continuity coach through active listening, working for the figure
Bennett, Coleman, Parry, patient’s agenda, and identifying patient beliefs and Bodenheimer, & values to activate a patient’s own motivation for Chen, 2010.
change and adherence to treatment (Huffman, 2007).
- 11

A COMMUNITY RELATIONSHIP
The concept of community has a critical part of the Care Transitions QIO project. A community relationship is between senders and receivers. This can be just a few senders and receivers (hospital, HHA, physician). It can be between one to two providers or several, depending on your location. For home health agencies this means to communicate fully with the providers from whom you receive referrals. If you don’t receive the information necessary to effectively manage the patient, you must request until it is received. This communication does not end with the receipt of the patient; you must communicate fully with those to whom you transition patients such as acute care, skilled nursing facilities as well as community support service providers. Those who collaborate together at a community level can examine root causes for readmissions and collectively plan appropriate interventions while problem solving to overcome the identified root cause (cfmc.org).
The leadership section for the Cross Setting I BPIP provides home health agency leaders with perspectives from experts on cross setting topics. This information covers a variety of topics: including coaching, motivational interviewing, a care transition model, and updates on national and state care transitions projects. These begin on the following page: Focus on Care Transitions and Coaching.
- 12

If'who you are and where you live' determines your care1, and 'all health care is local'2 then it makes intuitive sense that change for improvement must occur at the local community level. What is less intuitive, at least within the confines of the traditional health care quality improvement project, is exactly how to go about leveraging local infrastructure and culture to meet the needs of a local population.
The Care Transitions Theme is a Centers for Medicare & Medicaid Services (CMS)-funded initiative to reduce unwanted hospital readmissions for a geographically defined population of fee-for-service (FFS) Medicare beneficiaries. Community is the unit of intervention for the Theme, and 14 communities scattered across the US are successfully changing the trend in readmission rates for their FFS populations. Providers in the Theme communities are using evidence based interventions, designed by others and well described in the peer-reviewed literature,3 but what is emerging from the overall project is a collection of insights about the importance of cooperative implementation activity, and the power of collective action to improve the health care experience of a population. As new options become available to providers for delivering transitional care services through The Affordable Care Act4, both through direct payment for transitional care services (section 3026) and through financial incentives (sections 3022,3025) cooperative activity will become increasingly important. If not, we risk creating new but still disconnected services, adding to the confusion typical of what frail elderly patients now experience, and increasing costs without benefit.
What Causes Hospital Readmissions?Quality Improvement Organizations (QIOs) facilitating Care Transitions Theme communities typically began their projects using medical record reviews of care given during hospitalizations resulting in early readmissions, and root cause analyses of provider processes involved in hospital discharge, transfer, or receiving patient care responsibility following hospital discharge. In general terms, patients returned to the hospital because of unmanaged worsening of their conditions, the use of suboptimal medication regimens, and returning to emergency departments instead of accessing a different type of medical service. The root causes of these problems could be attributed to 3 basic system gaps:
1) Lack of engagement or activation of patients and families into effective post-acute self management,
2) Lack of standard and known processes among providers for transferring patients and medical responsibility, and
Care Transitions Quality Improvement Organization Support Center
Best Practice: Community-based efforts to reduce hospital readmissions
1 Baicker K, Chandra A, Skinner JS, Wennberg JE. Who you are and where you live: how race and geography affect the
treatment of Medicare beneficiaries. Health Aff (Millwood). 2004;Suppl Web Exclusives:VAR33-44. 2 Hodification of “!ll politics are local” attributed to Tip O’Eeill, former Speaker of the US House of Representatives, frequently
heard by this author in various local and national conversations. 3
http://www.communitysolutions.com/assets/2012_Institute_Presentations/caretransitioninterventions051812.pdf 4
http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?dbname=111_cong_bills&docid=f:h3590enr.txt.pdf
- 13 -
Focus on care transitions and coaching

3) Ineffective or unreliable sharing of relevant clinical information
It is again intuitive that each of these system gaps cannot be solved by a given provider in isolation: effective patient activation needs to be supported by every provider involved in the chain of medical care, transfer of care responsibility involves both a sender and receiver, and clinical information isolated within a single provider setting, even if perfectly accurate, is not safe medical management. But what has not been widely appreciated, even if still somewhat intuitive, is the degree to which closing the gaps in care relies on intentionally designing local working arrangements or community vision.Drivers of Hospital Readmission:
Poor Provider-Patient interfaceI—| insufficient medication management, ineffective
support for patient self-management, unreliable f/u other than return to the ED
Unreliable system supportLack of standard and known processes Unreliable information transfer Unsupported patient activation during transfers
No Community infrastructure for achieving common goals
Evidence-Based Interventions to Improve Transitional CareMost evidence-based interventions to improve transitional care and/or to reduce unwanted hospital readmissions target one or more of the system-level drivers defined through the CT Theme participants' work. For example, The Care Transitions Intervention (CTI™) is a patient activation intervention delivered through transitions coaches that engages patients and families in effective self-care practices, one of which is carrying important information about their medical needs in their own personal health records5. Project BOOST is a comprehensive set of resources, tools and data collection strategies developed by the Society for Hospital Medicine to support continuous improvement of discharge practices by hospitalists and other hospital staff aiming for high-quality, high-reliability transitional care. Elements of BOOST include strategies for timely transfers of clinical information, and appropriate referral to transitions coaches6. The Transitional Care Nursing model trains nurses to lead multidisciplinary teams in delivering comprehensive care across settings, including within the setting of patient homes, to support fragile patients during transitions7.
A key feature of many of the evidence-based models is a set of services to be delivered in patients' homes, as opposed to traditional medical settings, and therefore offer many opportunities for home health agencies (HHAs). Over the 14 communities participating in the Care Transitions (CT) Theme, readmission rates are declining, and can be partially attributed
5 http://www.caretransitions.org/
6 http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/CT_Home.cfm
7 http://www.transitionalcare.info/
- 14 -

to changes in the use in home health services. In 2007 care patterns in the communities were characterized by 17.9% of all hospital discharges to HHAs, and the readmission rate for HHAs was 22.7%. By 2009,18.4% of all hospital discharges were to HHAs and the HHA readmission rate had decreased to 22.2%, indicating that the communities are using more home health services, and those services are resulting in fewer readmissions. However the CT Theme approach has shown that HHAs can make the most difference for a population when they target improvement in home based services generally as a collaborative group of home service experts aiming to deliver high value services to that population. For example, in one community 28 agencies worked together to identify common barriers to home health, then developed local intervention packages designed to promote more reliable appropriate referral and to standardize expectations of services to be provided. In that community, readmissions resulting from home health agencies have declined by more than 2% (absolute change) while referrals have increased by about 1 %.8 In another community, 8 home health agencies working together to standardize services and quality measures for heart failure patients have reduced acute care hospitalization (ACH) rates by about 0.5%, compared to background community rates of ACH increasing by 2.5%. A large hospital in the community which refers about 80% of their home health cases to one or more of these agencies has experienced a 4.5% reduction in readmissions of heart failure patients9.
It Takes A Village: A Conceptual Basis for Community ActionIt is tempting to view the layering on of additional services directed specifically at a patient- level driver of readmission as the easiest solution, because there is clear need for services different from what has been traditionally provided to patients. But the history of medical care expansion in the US has demonstrated that often more care is unassociated with better outcomes, or in fact may be associated with worse outcomes through increasing care complexity10. Certainly if'value' is a relationship between cost and quality it would be better if regions could design rational approaches to enhancing service arrays collectively rather than merely adding more services, even if those services in and of themselves should add value.
The Institute for Healthcare Improvement notes that regional reform makes sense for the following reasons:11
• All the components needed to construct a health system are within a region• Common values are more likely to emerge• Solutions to problems depend upon context, and context is known most accurately
locally• Platforms for dialogue exist or can be created• Other health determinants are attributes of a region
8 Results being prepared for publication 9 Results being prepared for publication 10 http://www.dartmouthatlas.org/downloads/reports/Spending_Brief_022709.pdf 11 Nolan TW. US Health Care Reform by Region. Cambridge, Massachusetts: Institute for Healthcare Improvement; February 2010.
- 15 -

Home-based services are likely to be an important component of any value proposition for serving a community; therefore home health agencies are well positioned to be leaders in designing and delivering better service arrays.
What a motivated HHA could do• Become familiar with evidence-based models for transitional care improvement• Assess your strengths and consider what you could add to community-based
strategies for better population careo Transitions coaches o Transitional care nurses o Others
• Review sections 3022,3025 and 3026 of The Affordable Care Act to construct value- based strategies
• Become a community of practice by building relationships with other HHAso Agree on best practiceso Develop a unified message for what home health services can do o Agree to compete on execution
• Develop relationships with your referral streamo Where do your patients come from and where do they go next? o Develop standard referral, communication and transfer processes o Develop mechanisms for accountability to those processes o Explore web-based sharing instruments to drive improvement
• Review a(some) readmission case(s) with those partnerso Create individualized solutions o Expand individual solutions into better processes
The Medicare program will need to expand dramatically in response to the graying of the population, and we have only a few years to become adept at efficient population management to accommodate them. Without embracing collaboration and efficiency, the mechanism for accommodating growth will likely be continued capital investment in growth, production of more competitors in every local market, and continued rising national costs.
Jane Brock, M.D.Chief Medical Officer for the Colorado Foundation for Medical Care (CFMC)Chief Medical Officer, Care Transitions Theme Quality Improvement Organization Support Center Clinical Lead of the NW Denver Care Transitions Community Clinical Adviser to the Geographic Variations Project
o o o
o o o
o o o o
o o
- 16 -

Care Transitions New York QIO: IPRO
New York Care Transitions Experience
The IPRO Care Transitions Initiative target community is based in the Upper Capital Region of New York State in a five contiguous county region that encompasses metropolitan, urban, rural and suburban communities. The provider community within this region consists of five acute care hospitals, six home health agencies, 28 nursing homes, five dialysis centers, five hospice organizations, several physician health networks and primary care practices, three major payors and two Regional Health Information Organizations (RHIOs).Our project team works collaboratively onsite with our provider community, facilitating review of current systems and processes to identify gaps in cross-setting communication and care coordination that result in avoidable readmissions.
Our initial strategy, which has continued to date, was to facilitate meetings to bring all of the providers within the community together at the table to encourage cross-setting sharing of issues and concerns as well as have them become aware of the circumstances that influenced and impacted patient care within each health provider setting. The common theme incorporated into these meetings was focus on the patient/care giver experience during transitions of care and the overall impact on health outcomes. We found that many providers never had the opportunity to discuss what is working well with the system or to work in partnership with other health care organizations to resolve important care issues and staff workarounds that have complicated information transfer, cross-setting communication and care coordination. Our experience has shown that the resulting partnering and open communication to resolve issues and improve the systems across settings to be one of the most important components of success in this initiative.
Our New York target community's primary cross setting interventions involved concurrent monitoring of readmissions, review of medication discrepancies, incorporation of 7 day follow-up primary care physician visits into discharge instructions post acute care and short term rehab discharge and use of Teach Back to support improved patient/caregiver activation and self-management. Our project team also conducted onsite outreach to physician practices to gain a better understanding ofhow they interfaced with the health care community and then shared their identified issues with the providers to begin to address opportunities to improve communication and care management.
One of the most valuable learning experiences has come from the Medicare beneficiary outreach sessions our team has conducted within our target community. These sessions are
Best Practice: Partnering and open communication to resolve issues and improve the systems across settings is one of the most important components of success in the Care Transitions initiative.
Two of the featured success stories are home health agencies that worked with IPRO for the QIO Care Transitions Project. Review the success stories from Eddy Visiting Nursing Association and Seton Home Health.
- 17 -

held at senior centers, housing units and locations where seniors gather for community activities. The sessions are interactive to learn about the senior's perspectives on health care and their personal experiences with transitions of care. Our team also provides educational information during the session on medication management, use of Personal Health Records and proactive planning for hospitalizations, discharge planning and physician follow-up. In addition, we partnered in each county with agency programs, volunteer and senior organizations that are working to identify gaps and enhance services in the community to learn about the concerns and issues that are impacting the health care of seniors in that region.
Our IPRO project team has truly learned that it does "take a village" to address all of the multiple issues and drivers involved in preventing avoidable readmissions and improving transitions across the health care continuum. We are very proud of the efforts and successes that our target community providers have been able to demonstrate as the "pioneers" in our New York care transitions initiative journey!
Sara Butterfield, RN, BS, CPHQ, CCMSenior Director, Health Care Quality Improvement Project Leader, Care Transitions Initiative, IPRO
INSIGHTS
See the Seton Health Home Care Success Story (p.67) for more on their program.
To improve care transitions our focus has been monthly meetings of all providers.
What we have learned: Include expertise of all health care disciplines and community organizations— palliative care representative, hospitalist, faith-based community representative, and pharmacist have all been essential members of the team. Use the electronic health record to improve communication at transfers. Employ essential interventions:
PCP appointment is scheduled within 7 days of discharge Pharmacist reviews medication list before hospital discharge for accuracy Patients at high- risk for falls is communicated between settings
Remember that the patient is really central with improving care between transitions. Teach the patient to bring his/her medication list to each dr. appt. Encourage the use of Teach Back.
Susan Ambrosy, Quality Manager, Seton Health Home Care, Troy, NY
- 18 -

National Transitions of Care Coalition [NTOCCjMedication reconciliation, National Patient Safety Goal 8 of The Joint Commission's Hospital Accreditation Program, is currently under review and reassessment. This safety goal has the potential to positively affect patient safety and hospital readmissions if properly implemented. The Patient Protection and Affordable Care Act provide various provisions addressing the reduction of hospital readmissions and improving transitions of care. Poor medication reconciliation can contribute to unplanned readmissions.
The National Transitions of Care Coalition (NTOCC) supports a more concise and quality process around medication reconciliation at transition to ensure patient safety, transition quality, reduction in readmissions, and improve provider and patient satisfaction.’
1) Quality Medication Re conciliation at Transition includes:a) Identification of all medications in use: prescription, non-prescription (over the
counter drugs, supplements, vitamins, etc), and medications obtained from other sources;
b) Determination that all medications are currently necessary, appropriate for the patient, and free of discrepancies;
c) Instruction for the patients and family caregivers on reasons for taking and how to take their medications, possible side effects, and what to do with discontinued medications; and,
d) Assessment of the patient and family caregiver's health literacy regarding ability to properly follow medication instructions when moving to the next site of care.
2) Quality Medication Reconciliation at Transition must occur at each care transition encountered by the patient, both by the sending and the receiving care entity (i.e., hospital, office practice, skilled nursing facility, community clinic, retail clinic, etc).
3) Quality Medication Reconciliation at Transition engages patients and family caregivers in the medication decision-making process, and assesses the ability of the patient to afford, obtain, and safely take medications.
4) Quality Medication Reconciliation at Transition requires that an accurate, reconciled medication list be provided to all care givers, including the patient and family and documented in the patients plan of care.
5) Align performance measures and payment incentives to support "best practices" in the Quality Medication Reconciliation at Transition exchange points as noted above.
A reconciled medication list is not all that is needed to ensure patient safety and adherence to taking medication as prescribed. To improve the quality of medication reconciliation practitioners must expand their informational intake as indicated above to be more inclusive than a list of prescribed medications. Other concerns that should be assessed during the reconciliation are patient health literacy, knowledge level and self motivation.
1)
2)
3)
4)
5)
- 19 -

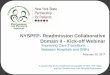
The Case Management Society of America (CMSA) recommends an adherence assessment addressing the patient's health literacy, knowledge, functional social support system and motivation. It is well known that an individual's knowledge, motivation and attitudes toward drug therapy can significantly influence medication adherence.2
The World Health Organization (WHO) published a foundational model for medication adherence that is based on patient information, motivation and behavior skill (WHO, 2002). CMSA developed the Case Management Adherence Guidelines (CMAG) from the concepts developed by WHO to aid in the assessment, planning, facilitation and advocacy of patient adherence. As such the guidelines provide an interaction and management algorithm (figure 4) to assess and improve patient knowledge and motivation to take medications as they are prescribed. The guidelines, including disease specific interventions, can be downloaded from www.cmsa.org at no cost. (Or go to http://www.cmsa.orq/portalsZ0/pdf/CMAG2.pdf -direct link to the guidelines.) Ensuring that medication reconciliation incorporates assessing medication adherence enhances the quality of patient information and provides the ability of providers to improve patient/provider communication, minimize or remove barriers, and enhance patient safety.3
KEY
KIMI - Knowledge low, Motivation low KIMh - Knowledge low; Motivation high KhlYll - Knowledge high, Motivation low KhMh - Knowledge high* Motivation high
AI - Adherence Intention
Figure 4, CMAG adherence management algorithm.
Practitioners should ensure that medication reconciliation is incorporated in the patient's plan of care and patients and their family caregivers receive a copy. Patients and caregivers need the opportunity to review the information contained in the care plan, discuss the options with their practitioner and confirm that they feel confident they can manage not only their medication list but the care plan addressing their individual medical, behavioral, psychosocial, and health care complexity needs.
- 20 -

The National Quality Forum (NQF) endorsed a preferred practice for healthcare providers and entities to have structured and effective systems, policies, procedures, and practices to create, document, execute, and update a plan of care with every patient (Preferred Practice6). Providing a written plan of care developed by a multidisciplinary provider team of all appropriate clinical staff should be a primary driver of appropriate transitions between treating physicians, patients and settings of care. Part of the written care plan should be medication reconciliation and adherence management. NQF has endorsed a performance measure for medication reconciliation - a reconciled medication list received by discharged patients (inpatient discharges to home/self care or any other site of care).4
Quality medication reconciliation and developing a written plan of care at transition will require appropriate alignment of performance measures and pay incentives. Regulators need to explore payment reforms that incentivize the use of a written care plan which includes quality medication reconciliation.
Cheri Lattimer, RN, BSNExecutive Director, Case Management Society of America Coalition Director National Transitions of Care Coalition
References:1) Medication Reconciliation at Transition, National Transitions of Care Coalition, NTOCC 20102) CM AG Case Management Adherence Guidelines, Version 2,2006 June3) Case Management Adherence Guidelines, Version 2, Copyright©, 20044) National Quality Forum, Preferred Practices and Performance Measures for Measuring and Reporting Care
Coordination, October 2010
1)
2) 3) 4)
- 21 -

To paraphrase a now well worn book title, it takes a community to provide health care. If we didn't think so previously, recent legislation and policy actions are now requiring 'a community effort' to ensure appropriate, medically necessary care to obtain good patient outcomes.
In my nearly twenty-seven years in home care, there certainly have been significant changes in the level of sophistication of care, the increased use of technology and in the structure and processes necessary for delivering home health care. Interestingly over the years, home care has usually taken pride in the fact that we serve as coordinators of care that enable individuals to live at home despite often intense care needs. The links with other community providers have been important to provide the social and environmental support to our clients. What home care awards program doesn't include citations of extraordinary efforts to link all the pieces necessary to keep that difficult or complicated patient at home?
However, one could argue that we haven't always done as good a job at actively coordinating other medical components of care. Perhaps it just has been easier to complain about the discharge planners and their unrealistic or uninformed expectations, late Friday afternoon discharges--and of course the physicians who won't call back or sign documents. Certainly not many of us have met with hospital administrators to more fully understand their expectations and limitations or to explain ours. At times, we probably have been guilty of an "us versus them" mentality when planning our procedures and implementing care plans. Those days are over or should be. There are a new set of the 3 R's to being successful in this new environment of a community delivering care.
• The first is Rethinking every facet of what we do and how we interact with all our customers.
• The second is to Restructure or realign those functions, our expectations and how we define what we deliver.
• The third is Relationships. Relationships are built on more than leaving a nice brochure in the doctor's office or delivering the periodic pizza to the staff.
During a conference session we conducted in the spring of 2010, we structured a panel discussion that included a home health agency clinical administrator, a discharge planner for a regional medical center and a physician. Dr. David Bensema who is Executive Director of Central Baptist Physicians in Lexington Kentucky has been in private practice in internal medicine. He has been a hospitalistand now manages activities of a large physician group of
State Association Perspective of Care Transitions
Best Practice: Rethink, Restructure, and Relationships
- 22 -

various specialties. As he discussed the interactions of physicians and home health he emphasized the necessity of developing a relationship with each physician. As a busy practitioner, he pointed out that calls received while he is seeing patients from a home health nurse he doesn't know was never high on his list. He pointed out the necessity of understanding the physician's point of view and of developing realistic and practical ways to build trust, develop protocols and create communication channels that work for everyone. Creating a functional community where we have been in the habit of functioning in separate silos that over interact sporadically is no small task. This BPIP provides information, suggestions and tools to help you to do.
Karen P. Hinkle, MSWExecutive DirectorKentucky Home Health Association
- 23 -

HealthSciences InstituteAddressing the Core Causes of Avoidable Health Care Costs
Today chronic diseases—not acute or episodic conditions—are the biggest threats to health, independence and quality of life. Chronic conditions also drive most health care spending. According to the Centers for Medicare and Medicaid (CMS) over 75% of total US health care costs can be attributed to the care of chronic conditions. An estimated three out often patients are alone responsible for 70% of all US health care spending. Poor medication adherence costs an estimated $290 billion annually. Fortunately many chronic disease- related costs are avoidable. The World Health Organization estimates that 80% of heart disease, stroke and type 2 diabetes—and 40% of cancer—could be avoided through healthy diet, regular physical activity and avoidance of tobacco use. Many hospitalizations would also be unnecessary if patients adhered with recommended treatments, effectively self-managed their conditions, responded appropriately to complication warning signs, made lifestyle changes, and were more active partners in their care. How many of your patients are ready, willing and able to partner with you in making these changes? What are you doing to prepare and support them?
Is Health Coaching a Trend?
Yes. Health coaching has emerged as a highly popular approach for addressing the behavioral causes of chronic disease and chronic disease-related costs. Today, many corporate life coaches, fitness trainers, nutritional supplement salespeople—as well as nurse or behavioral health professionals—now refer to themselves as "health coaches" or "wellness coaches." Yet, many self-described health coaches have had no formal training or preparation in formal and effective health coaching approaches. Further, experts cite that most popular health coaching training programs are based on unvalidated life coaching methods adapted from corporate settings—often without critical review by medical or behavioral science experts. While these approaches may be appealing and perhaps helpful in nonclinical settings, nurses and health care providers are held to a higher standard of practice—patients and purchasers expect that health care
Best Practice: Evidence-Based Health Coaching: A Lever for Better Home Health Outcomes.
One of the fastest growing fields in health care Targets the primary causes of poor health, disability and avoidable health care spending A patient-centered and effective practice Founded on validated approaches such as motivational interviewing (Ml) An effective and efficient approach for strategically addressing adherence, selfcare and lifestyle management barriers Superior to usual patient education or goal-setting
Highly effective or patients labeled as "resistant" A competency set that is not "innate" and can be difficult to master-but one that can be developed.
Evidence-Based Health Coaching
approaches
- 24 -

services be evidence-based. If evidence determines the choice of medications and treatments, shouldn't it also guide how patients are supported in adherence and self-care, particularly when patient-level behavioral factors are often the most powerful predictors of clinical and cost outcomes?
What's Different About Evidence-Based Health Coaching?
In most health care settings, the practice of health coaching remains poorly defined. Some nurses consider any patient education encounter to be health coaching, while others believe that identifying and discussing patient goals is health coaching. Some even believe that reminding, nagging or cajoling patients about their health is health coaching! While all of these approaches may work some of the time with some patients, to be effective most of the time, health coaching must be a strategic and formal approach—based on principles and validated techniques—which can be applied briefly and routinely in usual health care encounters. Without focus and without a formal approach, health coaching encounters may result in aimless, unfocused or "feel good" conversations—perhaps pleasant, but often unproductive. Evidence-based health coaching incorporates validated and formal approaches for helping patients succeed, together with targeted steps to support disease self-care, medication adherence, or lifestyle changes including weight loss, diet or physical activity. While there are a number of approaches from the fields of behavioral medicine, health psychology and nursing that have proven effective in health coaching encounters, motivational interviewing (Ml) is the only approach that has been validated in numerous clinical studies to positively impact health-related outcomes for patients at risk of, or affected by chronic conditions.
How Can Motivational Interviewing Help?
Motivational interviewing is a patient-centered approach for building patient motivation and helping patients resolve ambivalence about change. Ml was developed by psychologists Drs. William Miller and Stephen Rollnick and is currently used widely in the US and abroad. While it is not the only evidence-based health coaching approach, it is an approach that has been widely recognized as core to evidence-based health coaching practice. Ml has been particularly effective in building patient engagement, readiness and motivation to change. Unlike common advice-giving and teaching approaches to health coaching, Ml works best with patients who often labeled as "noncompliant" or "resistant." Ml is more than just a collection of techniques, but an overall orientation and approach to working with patients. Ml relies on open-ended questions, reflections, and various guiding strategies that support patients in making their own arguments and plans for change. While Ml may seem like an intuitive, easy approach—it is not simple. Experts note that Ml often represents a significant change in how nurses and other clinicians have been trained to work with patients on health- related behavior change.
- 25 -

How Can Ml be Used with Patients Who Are Nonadherent?
Research finds that most patients who do not take their medications or follow other self-care recommendations do so consciously. This is not to say that forgetfulness is not a factor— particularly among the aged—but a secondary factor. While patient education, medication set-up and instruction, or reminding can help improve adherence, poor adherence is usually not an information or organization problem, but a motivation problem. Effective health coaches use approaches like Ml to routinely check adherence using open-ended questions that do not imply judgment and evoke joint problem-solving, e.g., "has anything been getting in the way of you taking your medications?" Or, "You sure have lots of pills to take; how do you manage?" These questions are much more likely to encourage discussion about adherence, thoughts and feelings about their self-care, or concerns about side effects or other barriers. They are also more likely to defuse patient defensiveness and bypass a recitation of excuses for not taking medications.
How is Health Coaching Different from Patient Education or Teaching?
As the Institute of Medicine, the World Health Organizations and leading experts have cited, health care professional and continuing education training has been acute care-oriented, rather than chronic care oriented. Along with this acute focus has come an overemphasis on disease-focused patient education. However, most self-care, adherence or lifestyle management problems are often not due to lack of disease-related information or self-care steps. Most patients with longstanding chronic conditions have been lectured repeatedly about what they should do. For individuals who have been educated, reminded or nagged about health-related behaviors, additional patient education can evoke resistance. In fact, researchers have found that overused or poorly timed patient education or advice can actually reduce the likelihood patients will make a health-related change and can damage rapport. This is not to say that patient education, teaching or advice are not helpful— clinicians are obligated to provide instruction and advice—patients expect it. However, instruction and advice need to be delivered judiciously. Ml experts recommend avoiding unsolicited advice—always ask for permission from the patient before providing any information or advice. For example, "You mentioned your frustration with weight loss, would that be something you would like to learn more about?"
How Can Health Coaching Be Used with "Resistant Patients?"
From an Ml perspective, resistance is not a patient problem but a relationship problem. When clinicians use approaches such as Ml, they avoid the "resistance trap" and instead put the choice and responsibility for change back in the hands of patients. Most people have a natural tendency to resist being told what to do—even if the advice is well-intentioned. People often respond to such advice with direct or indirect resistance. Examples of direct resistance include avoiding health care providers, changing the subject, or making excuses. Indirect resistance is often harder to detect. When patients appear too compliant or overly agreeable, suspect passive resistance. To avoid creating resistance, Ml experts advise clinicians to avoid what
- 26 -

they refer to as the "righting reflex" or the natural tendency to try to stop patients from doing things that are unhealthy or to get them to engage in healthy behaviors. Not only are these approaches usually ineffective, they are exhausting and frustrating for the patient and the clinician! From an Ml perspective, patient autonomy is always reinforced.
Can Health Coaching Be Briefly Applied in Usual Patient Encounters?
Today, clinicians are busier than ever and must work efficiently and effectively. The benefit of evidence-based health coaching approaches such as Ml, is that they are surprisingly effective in limited doses or brief health care encounters. Evidence-based health coaching provides a structured format for quickly targeting what is most important to the patient and addressing the key barriers to healthier behavior. Traditional disease-focused patient education approaches to health coaching often fail to address what matters most to the patient—which is typically not the disease, but the problems that the disease causes in their daily life or the threats that the disease poses to their quality of life or personal priorities. On the other hand, informal or popular health coaching approaches—while usually patient centered—may take much more time than is available and may be unproductive. By working strategically and systematically, clinicians can make the most of the limited time they have with patients.
How is Proficiency in Evidence-Based Health Coaching Developed?
Experienced clinicians may be pleased to learn that they are already using many of the evidence-based health coaching techniques. For these individuals, formal training and preparation in formal, evidence-based health coaching can help them apply familiar approaches more strategically and routinely. For others who are more comfortable teaching, directing or advising patients, the transition to more patient-centered approaches like Ml can be difficult. It is also important to note that health care and behavioral science experts emphasize that health coaching skills are not simply "soft skills" that are innate to nurses or other clinicians. On the contrary, evidence-based health coaching requires advanced communication skills. While the concepts and foundations of approaches such as Ml seem to be "common sense," applying these practical approaches skillfully within the time constraints of routine health care encounters takes preparation and practice.Developing proficiency in health coaching, like most clinical skills, requires competency- based learning and objective assessment of the knowledge and skills.
Where Do We Learn More About Evidence-Based Health Coaching?
Infocus: Evidence-Based Health Coaching. HealthSciences Institute offers a free electronic publication with video resources for organizations and clinicians who would like to learn more about evidence-based health coaching practices and skill development.Population Health Improvement Learning Collaborative. HealthSciences Institute and Partners in Improvement host an interdisciplinary community of clinicians from various health care settings working in health coaching, disease management and chronic care. Each month a free webinar is offered and an online networking community is available.
- 27 -

• Motivational Interviewing Network of Trainers (MINT). MINT is a national group of Ml professionals from the behavioral sciences and other fields who specialize in the application of Ml in behavioral health, substance abuse, health care and many other setting. The MINT website provides a wealth of general Ml information and resources.
• The 2008 book Motivational Interviewing in Health Care: Helping Patients Change Behavior (Applications of Motivational Interviewing) by Drs. Stephen Rollnick, William Miller, and Christopher Butler is an excellent resource for clinicians interested in the application of Ml in health care.
Blake T. Andersen, Ph.D.CEO, HealthSciences Institute
-------------------------------------- -d
For additional information on Motivational Interviewing, see the Principles ofMotivational
Interviewing handout.
The Chronic Care Professional (CCP) Program is a nationally-recognized disease management and health coaching training and certification program. CCP is based on the recommendations of the Institute of Medicine and the World Health Organization for a 21st Century health care workforce. CCP is offered in jointly with the health management industry group (DMAA: The Care Continuum Alliance) and other partners including the Case Management Society of America. CCP includes a variety of evidence-based health coaching materials and Ml resources, including the six-hour Miller and Rollnick Motivational Interviewing Video Training Series and new Evidence-Based Health Coaching & Ml Video Skill-Building Series. A state home care association partnership program was launched in 2010, currently providing partial CCP tuition support to home health care agencies in Pennsylvania and Massachusetts.
- 28 -

facility.
Focus of coaching: to make patients and their caregivers more comfortable and competent in participating in their own care.
INSIGHTS
Our Coaching Program for AMI patients: Two in-home visits by nurse within first 14 days of hospital discharge from inpatient
Two follow-up phone calls spaced during next two weeks. st visit:
Medication reconciliation/checking to see if new prescriptions are filled
Review education book - signs and symptoms on when to seek care Encourage patients to make follow up appointments with PCP and cardiologist Discuss support system
Medication reconciliation, if needed Ensure physician appointments are scheduled Reinforce signs and symptoms of when to call physician Answer questions Discuss benefits of Cardiac nutrition class Discuss benefits of Cardiac Rehab program
nd visit:
Two follow up phone calls: Answer questions that might have arisen Ensure follow up appointments were kept Reinforce benefits of Cardiac nutrition class/rehab program
Referrals come from: Case management team and physicians
Powell, Administrative Director Sparrow Home Care Lansing, Ml
Review any equipment needs and discuss how to obtain
1
2
- 29 -
facility.

Miller & Huffman Outcome Architects, LLC and National Society ofHealth CoachesTelephonic Coaching: Is it Effective?
According to Dr. John Piette, Associate Professor of Internal Medicine at the University of Michigan, "Individuals often remember little of what they are told during outpatient encounters." Many people are not well prepared to manage their conditions without intermittent help and guidance along the way. Managed care organizations have had plenty of experience in using the telephone as a primary means of communication with members, but other healthcare providers have been slow to adopt telephony as a frequent means to guide care. With health coaching emerging as a unique and different way of improving outcomes and communicating with individuals, it only seems reasonable that we pay proper respects to phone communication as a means to implement this fresh, new coaching approach.
There are several reasons to consider the telephone as an effective means by which a healthcare provider can communicate with individuals who making the transition from one care setting to another, and those seeking support, guidance and information about their health risks, condition(s), or illness:
Ninety-eight percent of American households have phone communication Enhanced timeliness of appointments Affords more frequent contactCellular communication affords mobility for the users; no specific locale needed for a meeting placeImproved adherence to medication and treatment plans
A study conducted by Thomson Reuters and American Specialty Health concluded that a program of telephone-based health coaching for weight management can change employees' behavior and reduce their health risk factors. At the end of one year, the study of 890 employees demonstrated significant decreases in risk prevalence for poor eating habits (21.3% reduction) and poor physical activity (15.1% reduction). All of the biometric measures related to overweight and obesity also decreased, including percent overweight or obese (5.8% reduction), weight (4.5 pounds reduction), and body mass index (0.9 reduction).
Pinnock, Bawden, Proctor, Wolfe, Scullion, and Price found that assessments conducted via phone increased the proportion of those with asthma who received appropriate monitoring versus those receiving face-to-face encounters in the clinic setting. While there was no
Best Practice: Telephonic coaching is as an effective means by which a healthcare provider can communicate with individuals who are making the transition from one care setting to another, and those seeking support, guidance and information about their health risks, condition(s), or illness.
- 30 -

difference in "quality of life" in both groups, patients' access was increased and outcomes were comparable with telephone communication.
Simon, Ludman, Tutty, Operskalski, and Von Korff found that using the telephone to engage the depressed patient in cognitive behavioral therapy was substantially effective. After six months, those who received counseling over the phone were more likely to have improved depressive symptoms and were more satisfied with treatment.
There are Six Telephone Coaching Tips that will make your experience more successful for both the coach and the patient.
1. Schedule the call. Set the time, date and who will initiate the call. This places importance on the call and generally results in better compliance.
2. Work from an agreed upon agenda. Remember, to be successful you must work from the patient's agenda, not your own! This means setting the agenda together or asking the patient's permission to include certain items on the agenda for the next call. For example, while we may want to discuss medications and side effects on this first call, the patient may be interested only in what the hospital discharge nurse said about what to do to keep his incision from becoming infected. Work from the patient's interest first, and then integrate specific health teaching along the way!
3. Use active listening skills to enhance call effectiveness. Active listening is a skill that must be practiced. The human being can hear approximately 500 words a minute, but can speak only at a rate of approximately 175 words per minute. So it is not uncommon for our minds to wander during a conversation. Add this factor to a conversation that does not have a visual component and staying focused during a discussion becomes even more difficult. Listen for what the patient is not saying and any distracting noises in the background. Without being able to "see" the patient's body language, it's critical that your listening be keen and uninterrupted.
4. Location, Location, Location. The location for both the coach and the patient is critical. The patient is not the only one who can be distracted during this call. You must take every precaution not to be in a place of high traffic or noise during this call. The patient must perceive that you are sitting next to them in the room. Your attention to the patient at this point will make or break this time together. When scheduling the time and date, set up the patient's physical location for the telephone call as well. Just like face-to- face coaching, make every effort to eliminate or minimize distractions.
5. Call, just because... Call your patient occasionally at unscheduled times. This call is to see how their day is going and remind them of their next scheduled coaching call.
- 31 -

Focus on Care Transitions and Coaching6. Avoid using a speaker phone during a coaching call. People are often hesitant to
engage in conversation if they have been placed on a speaker phone. When a caller uses a speaker phone, this is often perceived as a lack of interest and frequently indicates that the caller is multi-tasking. In this instance, the patient may not be as candid in their conversation.
As you consider implementing or improving coaching interventions via the phone, Piette listed several factors that should be considered:
1. Content should be clearly structured2. Don't try and accomplish too much in one setting3. Target those individuals who are likely to benefit most in your population4. Most effective programs are linked to outpatient clinical follow-up5. Incorporate outcome measures to validate program's impact
Telephone outcomes that can be considered for measurement include, but aren't limited to:1. Confidence level of the individual to reach goal(s)2. Number of phone appointments kept3. Satisfaction (from coach and patient) with phone encounters4. Improvement in symptoms, weight, exercise, diet, smoking cessation and/or stress
To improve health outcomes in the population you serve, consider a wider use of the telephone as an adjunct to the individual's treatment plan or if you already use the telephone to provide interventions, make sure that your active listening skills are sharp, that distractions are minimal to none, that you have an appointment for the call, and that you have an agreed upon agenda!
Melinda Huffman, BSN, MSN, CCNS, CHC Co-Founder, National Society of Health Coaches Principal, Miller & Huffman Outcome Architects, LLC
ReferencesPiette, J.D. (2005, June). Using telephone support to manage chronic disease. Prepared for the California Healthcare
Foundation. Retrieved August 8,2010 from www.chcf.org/- /media/Files/PDF/U/Usingtelephonesupporttomanagechronicdisease.pdf
Pinnock, H., Bawden, R., Proctor, S., Wolfe, S., Scullion, J., Price, et al. (2003). Accessibility, acceptability and effectiveness in primary care of routine telephone review of asthma: A pragmatic, randomized controlled trial. British Medical Journal, 326: pp. 477-479.
Simon, G.E., Ludman, E.J., Tutty, S., Operskalski, B., Von Korff, M. ((2004). Telephone psychotherapy and telephone care management for primary care patients starting antidepressant treatment. JAMA, 292(8), pp.935-42.
©2010 Melinda Huffman
Important Note: The National Society of Health Coaches (NSHC) provides health coaching certification, education and training developed by clinicians for clinicians! Visit the Society at www.nshcoa.com for program detail, content, lead coaches, organizations using the program,
and testimonials. Contact [email protected] or call 931.967.0894 for further detail.
- 32 -

Amedisys Home Health has launched a home-based Care Transitions program. The launch of the program began in April of 2010 and is an offering for patients at all 600 Amedisys Care Centers across the country as of September 1,2010. The initiative is an effort to reduce acute care hospitalizations, create a stronger continuum of care and ultimately create self-managing patients who are empowered over their condition.
Amedisys has developed a program that involves all agency staff in providing self-management education and support to all home health patients that use our services. This process is incorporated into the clinician visits that are already being provided to our patients so it is scalable, sustainable and cost effective.
The Amedisys Care Transitions program begins in the hospital prior to the patient being discharged to home.Our Care Transitions Coordinator visits the patient and introduces them to our services and the idea of selfmanagement. They collect clinical information while discussing with the patient their reason for current hospitalization. Patients need to have a clear idea of what caused their current hospitalization so focus can be provided in this area to prevent future hospitalizations.
Patients are provided with a copy of the Bridge to Healthy Living, a Personal Health Planner. The discharge checklist is reviewed with the patient. This area assures the patient has necessary information prior to their discharge from the facility. This information contains areas such as, what medications are they to take once home, if equipment has been ordered and if the patient needs to pick it up or if it will be delivered, etc. Simple things, but many patients do not have this information when they leave the hospital. Patients are encouraged and coached to obtain a current medication list prior to discharge. Again simple, but many patients do not know if they continue previous medications and include the new ones, or if they discontinue all previous medications and just take the new ones.
Amedisys: Bridge To HealthyLiving
Core Elements of Our Care Transitions Program
Working with patients on effective communication with their physicians and other health care providers Getting the patient connected in the community so they will have on-going support after home health care giver leaves Using the Bridge To Healthy Living as a communication tool How to do a self assessment and track health data, which will lead them to determine what actions they need to take Identifying symptoms and how to respond Setting goals, building action plans to work toward goals and to use this to make changes in their life/health Working with the patient to find a medication system that works within the patient's environment, mental and physical limitations Guiding patients to do medication reconciliations anytime there is a change/adjustment in their medications Making physician appointments
- 33 -

The last area that is covered in the hospital is the follow up physician appointment. Every effort is made to get the patient to schedule a follow up physician appointment within two- weeks of discharge from hospital. Patients are also provided with contact numbers for the home health agency to call if they have questions. If the hospital will not allow Care Transitions Coordinators in, the process begins on the first visit in the patient's home.
Once the patient is home, clinicians in the home assist the patient to do a medication reconciliation contacting the physician to clarify any issues found. Clinicians also ensure the patient has the follow up physician appointment scheduled and have transportation to the appointment arranged. The Bridge to Health Living booklet is used on every visit to keep the patient focused and provide a place for them to record pertinent information that they will need when communicating with health care providers. Patients are coached on how to identify areas of their life that need to be changed based on their health data and self assessment.
Practical skills such as how to change a behavior in a sustainable fashion are taught to the patient, which involves goal setting and building actions plans. This ensures the patient can continue to learn from their own health data after home health services are discontinued and the patient will be able to continue to make necessary changes to reach their health status goals. Coaching the patient in effective communication with health care providers is a major focus of the process. Symptom assessment with early identification and a plan of action to follow if noted assist in patients being treated earlier in the home as opposed to being hospitalized.
Providing care with our Care Transitions model is proving its effectiveness and is a benefit for our patients.
Sherry DukesAmedisys National Director Quality & Outcomes Education
A HHQI national teleconference is scheduled for November 12,2010 at 12 ET featuring one of the Amedisys Home Health Agencies -Amedysis Georgia, who has implemented coaching. Register now for this teleconference on the HHQI home page.
One of the featured success stories is a North Carolina Amedisys Home Health agency with a home care nurse discussing the impact of the Bridge to Healthy Living program.
- 34 -

The Community^Based Transitions Model of Carez—A Model for the Field ofHOMECARE
The time during patient care transitions from one care setting to another, or from one level of care to another, has been identified as burdensome for patients with chronic diseases. These patients are expected to take an active role in their care, often with little support or understanding of their care plan, resulting in a high rate of hospital admissions or readmissions.
Models have been developed to support patients during care transitions, particularly from hospital to home. Homecare is an ideal provider of transitions support for many reasons. OASIS data is in place to evaluate both process and outcome measures in a risk-adjusted standardized manner. Numerous variables can be evaluated, such as re-hospitalization rates, emergent care rates, and appropriate oral medication management. These variables can be utilized to drive care improvement initiatives across providers and across settings. Homecare can be poised to help patients become as independent as possible in disease self management, with minimal re-tooling of staff in health coaching techniques and the ability to facilitate behavior change.
The Community-Based Transitions Model ™ (CBTM™) was developed by homecare providers to address gaps in all care transitions. One time period for interventions is during the time of hospital discharge but a focus remains at periods all along the entire disease trajectory, and across time. The CBTM™ builds on previous transition models yet adds four new areas of concentration. These new areas include: a) medication adherence and persistence, b) understanding on-going treatment changes by supporting health literacy, and c) on-going monitoring for change in symptoms or status, such as depression screening, nutrition risk, and caregiver support, and d) theory-based remote patient monitoring, with the implementation of associated interventions. As an example, the CBTM™ addresses on-going transitions when a patient returns home from a physician office visit, when symptom management becomes an issue, or when the patient approaches the end-of-life (See Figure 13).
The CBTM™ is a patient-centered model. The CBTM™ clinician utilizes motivational interviewing and the principles of Albert Bandura's Self-Efficacy Theory (Bandura, 1977) to guide their interactions and care planning. As many patient challenges are intimate in nature, clinicians must have the ability to connect with patients in a way that facilitates trust. Trustbuilding permits important dialogues needed to understand the patients' personal goals and future aspirations. The CBTM™ clinician has the responsibility to ensure that the patient understands the connection between their aspirations for their future, and how condition management behaviors can help them realize these aspirations. The CBTM™ places emphasis on the patients' short term and long term goals, and pairs those with evidence-based care.
Best Practice: Homecare is an ideal provider of transitions support.
- 35 -

Chronic conditions cannot be cured; therefore care delivery must address changing patient needs over time. Care complexity may increase as patients develop new co-morbid conditions, experience role changes or face new financial challenges due to changed prescriptions or treatments.
The CBTM™ case manager leads a multidisciplinary team, such as registered nurses, physical, occupational and speech therapists, nutritionists and social workers who meet the holistic needs of the patient. The CBTM™ case manager-patient relationship remains intact over time so that interventions can be adapted to meet changing needs. With this additional on-going support, patients may be able to remain relatively independent in the least restrictive setting, their home.
The Patient Protection and Affordable Care Act (PPACT) includes a provision for Community- Based Transition Programs (Sec. 3026 of HR 3590) specified to improve transition services for high risk Medicare beneficiaries. In addition, there is a provision for home health agencies to demonstrate value in long-term chronic care management (Sec. 3021 of HR 3590). This provision will enable home health providers to freely and ethically partner with other providers such as physician practices or hospitals for the acquisition of positive health outcomes, past the typical acute episode of care.
The adoption of the Community-Based Transitions Model™ provides a new vision for chronic care delivery, with homecare playing a key role in patient transitions. If homecare professionals can be held to a consistently high standard of chronic care delivery via training and chronic care certification programs, and by the use of a standardized patient-centered model of care, untold positive outcomes may be realized.
To download a free white paper on our care coordination model in homecare go to http://www.pentahealth.com. For more information on the Chronic Care Specialist Train the Trainer program which includes health coaching, motivational interviewing, care transitions, and evidence-based care for diabetes, heart failure, COPD and depression, go to www.pentahealth.com.
Paula Suter, RN, MADirector, Center of Excellence for Chronic Care Management Baptist Home Health Network/ 2020 Health Solutions Little Rock, Arkansas
- 36 -

Figure 1.
Figure 2.© 2010- Penta Health (All Rights Reserved)
HOSPITAL
Add text title
Add text title
Add text title
HOMEHEALTH
PALLIATIVECARE HOSPICE
CBTM™: Effective Transitions toPalliative CareCBTM™: Effective Transitions toPalliative Care
© 2010- Penta Health (All Rights Reserved)
MDSPECIALISTS
WOUNDCLINIC
PCP PHARMACY
CBTM™:Across Post Acute SettingsCBTM™:Across Post Acute Settings
- 37 -

References:
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84,191-215.
H.R. 3590, Patient Protection and Affordable Care Act, § 3021 (2009) (establishment of Center for Medicare and Medicaid Innovation with CMS, p. 227)
H.R. 3590, Patient Protection and Affordable Care Act, § 3026 (2009) (establishment of Community- Based Transition Programs with CMS, p. 247)
Figure 3.
© 2010- Penta Health (All Rights Reserved)
ApptScheduledwithin a wk
ANDable to get
there
ComprehendS&S that require
attention AND
whom to contact
Is patientfamiliar&
competentAND
have access
MedicationManagement
EarlyFollow-up
SymptomManagement
Adherence &persistence
Support health literacy for
changes in Rx or Tx
Monitoring to identify change
in Rx or Tx
Community-BasedTransitions Model™ (CBTM)Community-BasedTransitions Model™ (CBTM)
- 38 -

CHECKLIST FOR AGENCY LEADERSHIP How to use:
1. Review this checklist and select a few interventions that are appropriate for your agency after targeting areas for improvement. Remember, these activities are designed for agencies with varied degrees of best practice implementation. These activities are best practices and are included to guide and direct you with improving quality of care.
o Cross setting chart reviews and staff input can help identify areas that need improvement (for example, the focus area may be improving patient education, medication reconciliation and/or resources for staff)
o The improvement team should make intervention selection with staff
o Select 1-4 interventions to begin
o Depending on the size of your agency, plan small tests of change with new tools and processes, evaluate effectiveness (what works and what doesn’t) and then move to total agency implementation
o Add additional interventions as team/staff sees other areas for improvement
o Identify who will champion the process from senior leadership? Who will steward resource allocation?
2. Utilize the ‘assigned to’ and ‘notes’ if needed.
3. Refer to the BPIP timeline (pg. 71) to plan implementation of the selected interventions.
4. Revisit this list after a few weeks and consider additional interventions.
The checklist begins on the following page; the checklist can be printed independent of the additional leadership information.
- 39

CHECKLIST FOR AGENCY LEADERSHIP SUGGESTED ACTIVITIES:
ASSIGNED
TO:
NOTES DATE
COMPLETE:
� Select 2 or 3 tools from this BPIP, Associated Resources and other Web link tools (pages 4548). Adapt tools so they work with internal processes. For example—use SBAR with internal processes as well as nurse to physician communication.
� Begin with a brainstorming effort of all staff to identify perceived and actual barriers to improving care transitions.
o Move towards staff suggestions to improving care transitions.
o Make lists of their suggestions and prioritize the proposed interventions.
o Begin with a very quick look at internal processes that should be improved?
o Discuss communication technique (look at the SBAR communication/briefing model on page 56)
o Identify areas where staff may need more education: pharmacology, wound care, communication
� Evaluate staff education—it should include:
o What is Care Transitions? o What is Health Coaching? Share the
Eddy VNA Success Story about coaching o Staff’s role in improving care transitions o Staff need to understand that transitional
care isn’t a ‘one size fits all’. The individual needs and risks of a patient must be considered. For example, the complex patient, those with multiple health needs will require much more that coaching.
o Sections of the BPIP can be used for staff education: Discipline tracks, all or some of the Focus on Care Transitions Section for explanations of Coaching and Care Transitions (Page 13-38)
� Be creative with the education: distribute memos, use bulletin boards, wallet cards, hold contests
- 40

CHECKLIST FOR AGENCY LEADERSHIP SUGGESTED ACTIVITIES:
ASSIGNED
TO:
NOTES DATE
COMPLETE:
� Measure your patients’ rehospitalization rate. This will take some extra data collection but will help you have a better understanding of readmissions. Track patients who have been in the hospital (ROC or SOC) and then record when/if a rehospitalization occurs, reason for hospitalization, and number of days since hospital discharge.
� Measure improvement through baseline and ongoing evaluations (e.g., measures of patient and family caregiver’s experience)
� Identify one or two core improvement areas such as improving information transfers
� Review the care of any recently hospitalized patient and determine if all interventions were appropriate. Examine and discuss any delays in care and communication breakdowns.
� Track if patient contacted agency before going back to hospital
� Track if patient was identified as ‘high-risk’ at SOC/ROC
� Focus audit activities on charts of clinicians who have high rehospitalization rates vs. those with low rehospitalization rates to identify causal factors. (Important: Make this a collaborative, learning investigation---not a punitive one!)
� Call all patients (or caregivers) who have experienced a recent rehospitalization or readmission and determine if anything could be changed to prevent future hospitalizations from the patient perspective.
� Send patient’s primary care physician/provider (PCP) a typed list of all current patient medications within 24 hours of admission to home care. Make this a standard of care!
� Ensure all hospital discharged patients are seen by the PCP and other physicians as appropriate within 7 days of discharge. Consult with MSW if transportation to appointments is a problem for the patient.
- 41

CHECKLIST FOR AGENCY LEADERSHIP SUGGESTED ACTIVITIES:
ASSIGNED
TO:
NOTES DATE
COMPLETE:
� Case conference your high risk patients. Make sure internal ‘transitions’ between disciplines are smooth and complete.
� See Case Conference form � Where does patient keep living will and other
important papers? Suggest a 9 x 12 manila envelope (with copies) in an easily accessed area. Stress need to take these paper to ED, etc.
� Begin brainstorming with staff from across care settings if possible.
� Review the National Quality Forum, Care Coordination Practice & Measures. Evaluate your agency for gaps with regard to new performance measures. Determine where to start efforts.
� Work on a communication tool that can be used by all settings to communicate patient needs and plan of care during transitions.
� Develop/adopt a Personal Health Record to provide to patients to ensure consistency of care form provider to provider.
� Does your agency have a ‘niche’—wound care or diabetic care or heart failure expertise? Share this and promote it with other providers.
� Reach out to other providers and begin discussions on improving care transitions in your community.
� Share your hospitalization and rehospitalization rates. Share what has been learned in the QIO Care Transition pilots—a meeting of all interested providers in the community is the initial step.
� Make sure to involve hospital departments of pharmacy and community resource groups such as aging services, parish nurse services, and palliative care. See Seton Home Health Success Story.
� Work with other provider groups to align protocols and processes. See the Gentiva Success Story about working with orthopedic physician groups.
- 42

CHECKLIST FOR AGENCY LEADERSHIP SUGGESTED ACTIVITIES:
ASSIGNED
TO:
NOTES DATE
COMPLETE:
� Review the insights and success stories in this BPIP and investigate how these agencies have implemented coaching. Discuss this with community providers and begin steps to implement coaching. Two well-known care transition models with extensive evidence to support a coaching model are the The Care Transitions Model (http://caretransitions.org) and Transitional Care Model (http://www.transitionalcare.info). The Transitional Care Model is one of the featured BPIP tools --page 64.
� Paula Suter (page 35) shares the new Community-Based Transitions Model ™ This model is designed for home care providers that addresses gaps in care transitions and has four areas of focus 1) Medication adherence and persistence, 2) Understanding of on-going treatment changes, 3) On-going monitoring for change in health status 4)Theory-based remote patient monitoring. http://www.suttercenterforintegratedcare.org/
� Refer to the Care Transitions: Barriers and Strategies document on page 54-55. This is valuable input, guidance, and resources from the QIO Care Transitions Project. Read the Focus on Care Transitions’ and Coaching Section excerpts—borrow and learn from those with experience!
� Focus on your medication reconciliation process (See April BPIP—Improvement in Management of Oral Medications) See also CHAMP tools: Review of the 3-Step Medication Reconciliation Process and Medication Management
- 43

� When and if possible share strategies/resources across all settings. Strategies/resources to consider are:
o Teach-back drug cards o Personal Health Record (Spanish
version) o Nursing Transfer/Discharge Summary
(pages 52-53) o Consistent Messaging (see Barrier and
Strategy document page 54-55) � Share your successes with your community of
providers. Share specific patient successes— those that show care coordination is working. Market this as appropriate. See the Success Story that Amedisys shares about their Bridge to Healthy Living and successful impact on a patient.
� Track your progress—both objective (rehospitalization rate and ACH rate improvement) and subjective (patient successes, provider collaboration).
“Postdischarge PCP involvement is particularly essential with shorter hospital stays, as patients will predictably have complex postdischarge needs as they complete their recuperation at home.” (Balaban and Williams, 2010)
- 44

SELECTED TOOLS AND RESOURCES The tools in this package are: • Contributed by home health agencies featured in the INSIGHTS and
Success Stories, transitional care leaders, quality improvement organizations, and/or recommended from other organizations concerned with care transitions
• Available in the BPIP or on the HHQI BPIP webpage (must be logged in to access)
• Available through links to other organization websites
Additionally, look for links to the numerous tools and resources throughout the package. Due to the number of tools and resources, it is easy to select too many resources. It is suggested that you choose carefully which tools you would like to use and select a few that are best suited for your prioritized interventions. So please examine the tools in this BPIP, the tools available through Web links, or tools under Associated Resources on the Cross Settings I BPIP Web page--then pick and choose what you would like to use!
WVMI & Quality Insights does not recommend any one particular tool. We simply provide tools associated with a best practice that are in the public domain or given to us to share by other organizations or home health agencies.
The tools included as part of this package (pages 52-66) are: Tool Designed for: Discharge and Transfer Nursing Summary This tool is used by Pennsylvania providers in the Note QIO Care Transitions Project to improve
communication about patient status at transfer between provider settings.
Improving Care Transitions: Barriers and Strategies
This document was developed with the help of the 14 Care Transitions QIOs. It lists barriers that have been encountered by the home health agencies and other providers in the Care Transitions Project and strategies that can be employed to overcome them.
SBAR worksheet and Review of the SBAR Technique
A briefing tool that will improve communication between health care providers. SBAR will help your clinicians communicate with physicians and other health care providers. Many hospitals, home health agencies and nursing homes have already adopted SBAR as a communication tool.
Transitional Care Model See page 16 in the Focus on Care Transitions and Coaching Section for an update on the TCM. The following link will take you to the CHAMP website and features a video on Dr. Mary D. Naylor describing the Transitional Care Model and how it can serve as a platform for home care clinicians that are building plans of care for frail older adults that are making the transition from hospital to home.
http://www.champ-program.org/blog/?p=786
- 45

Tools available through web links Website: Designed for: Better Outcomes for Older adults through Safe Transitions (BOOST®) Project BOOST® provides resources to optimize
the hospital discharge process. By improving discharge processes, Project BOOST® aims to reduce 30 day readmission rates for general medicine patients (with particular focus on older adults), improve facility patient satisfaction scores, improve the institution’s H-CAHPS scores related to discharge, improve flow of information between hospital and outpatient physicians, ensure high-risk patients are identified and specific interventions are offered to mitigate their risk, and improve patient and family education practices to encourage use of the teach-back process around risk specific issues.
Look under The BOOST® Intervention for tools. Care Transitions SM
This is the web site for the Care Transitions Intervention. Resources include:
• Care Transitions MeasureTM
• Medication Discrepancy Tool • Patient Activation Assessment • Discharge Preparation Checklist
CHAMP A national initiative to improve the quality of home care for older persons.
Enter “care transitions” in the Text Search box for a number of downloadable tools for care transitions. The SBAR tools that are featured in this BPIP are also from CHAMP Other helpful CHAMP tools are Review of the 3Step Medication Reconciliation Process and Medication Management Some links to additional CHAMP tools are on page 72.
- 46

HealthSciences Institute The HealthSciences Institute is a multidisciplinary collaborative and health care certification, development, and resource organization founded in 2003. HealthSciences prepares health care organizations and professionals for a new health care environment in which chronic, not episodic, conditions are the biggest threats to health. HealthSciences developed the Chronic Care Professional Certification Program—review their Web site for current chronic care information.
In Home Palliative Care Kaiser Permanente developed a home-based model of palliative care that uses an interdisciplinary team of providers to manage symptoms and pain, provide emotional and spiritual support, and educate patients and family members on an ongoing basis about changes in the patient’s condition. One randomized controlled trial and one comparison-group study showed that the program increases patient satisfaction, increases the portion of patients dying at home rather than in the hospital, and reduces emergency department visits, inpatient admissions, and costs.
Information can be found in these articles: http://www.ncbi.nlm.nih.gov/pubmed/14622451 http://www.ncbi.nlm.nih.gov/pubmed/17608870
The Institute for Healthcare The IHI How-To Guide: Creating an Ideal Improvement (IHI)-- How-To Guide: Transition Home is a comprehensive Creating an Ideal Transition Home document that includes action and progress
documentation resources. This is part of the Transforming Care at the Bedside Series. You will need to register on the IHI Web site to retrieve this free resource.
Additional IHI initiatives: • STate Action on Avoidable
Rehospitalizations (STAAR) Initiative
• The STARR initiative aims to reduce rehospitalizations by working across organizational boundaries in three states, initially — Massachusetts, Michigan, and Washington — and by engaging payers, state and national stakeholders, patients and families, and caregivers at multiple care sites and clinical interfaces.
- 47

• Hospital to Home (H2H) • H2H is led by the American College of Cardiology and the Institute for Healthcare Improvement (IHI), is a national rallying point to reduce cardiovascular-related hospital readmissions and improve the transition from inpatient to outpatient status for individuals hospitalized with cardiovascular disease.
National Transitions of Care Coalition (NTOCC)
The National Transitions of Care Coalition (NTOCC) was formed in 2006 bringing together thought leaders, patient advocates, and health care providers from various care settings dedicated to improving the quality of care coordination and communication when patients are transferred from one level of care to another. This site includes many free tools and resources for consumers (in English, Spanish and French) and for providers. Some of the provider tools including a Module: Hospital to Home and Emergency Department to Home . Review the entire site for current information and tools on care transitions.
Project Re-Engineered Discharge (Project RED)
Project Re-Engineered Discharge is a research group at Boston University Medical Center that develops and tests strategies to improve the hospital discharge process in a way that promotes patient safety and reduces re-hospitalization rates. Here is a link of a printable version of the Components of the Re-Engineered Discharge.
Transitional Care Model The Transitional Care Model (TCM) provides comprehensive in-hospital planning and home follow-up for chronically ill high-risk older adults hospitalized for common medical and surgical conditions. The heart of the model is the Transitional Care Nurse (TCN), who follows patients from the hospital into their homes and provides services designed to streamline plans of care, interrupt patterns of frequent acute hospital and emergency department use, and prevent health status decline.
- 48

INSIGHTS
• We utilize the Hospitalization Risk Assessment* (HRA) tool in our weekly team conferences to update the plan of care
• We involve the home health aide in our weekly conferences to get a timely report on the patients’ current status and any changes in ADLs.
• We instruct the patient/caregiver to always take the emergency folder anytime going to the hospital including the emergency department.
• The emergency folder includes the following information: • The client’s updated medication record • The patient’s personal health record • The name and phone number of the PCP • The name and phone number of our agency
With this basic information the transfer is more efficient, the receiving hospital or agency has current medical documentation and phone numbers to get more information as it is needed. *HRA in the January 2010 BPIP
Nancy Wade, RN, BSN, MHM Nursing South Corporation Miami, Florida
- 49

Tools included on the BPIP webpage Tool: Designed for: Case Studies Clinician Education Coaching forms from Eddy VNA Also included with the success story—
read the success story. Discharge Criteria* IPRO (New York QIO)
Worksheet 1 Worksheet 2
Navigational Tool to share with hospital case managers, discharge planners, and physicians to help determine appropriate care at discharge.
I-SBAR-R This document is from Girling Health Care
Clinician education and guide for SBAR
Phone Monitoring Assessment Guides Includes guides for HF, COPD, Diabetes, Cancer and Medication Management
Guides for phone assessments.
Phone Monitoring Patient Encounter Form
Documentation tools for phone assessments.
Options for Next Level of Care* Qualis Health (Washington QIO)
Navigational Tool to share with hospital case managers, discharge planners, and physicians to help determine appropriate care at discharge. Options for Next Level of Care is available in a poster and brochure.
Principles of Motivational Interviewing An Excerpt from MassPro’s PLANNED CARE: SELF-MANAGEMENT SUPPORT IN HOME HEALTHCARE
Some tips and suggestions that can easily be shared with staff on motivational interviewing.
SBAR High-Risk ACH Physician’s Notification of High-Risk Patient for Acute Care Hospitalization
Teach Back Nurse Practice Exercise TMF Health Quality Institute For more information on Teach Back visit http://www.healthliteracy.com/
This is a practice exercise in Teach Back for nurses.
Teach Back Medication Cards A number of Teach Back Cards that have been utilized by providers in the Care Transitions Project. Teach Back is a technique providers ask patients to state in their own words (i.e. teach back) key concepts, decisions, or instructions just discussed.
*All tools include specific community and state specific criteria and resources and may need to be modified for your agency use.
- 50

“The only way to know for sure whether patients understand is by asking. One technique to do just that is the “teach-back,” in which providers ask patients to state in their own words (i.e. teach back) key concepts, decisions, or instructions just discussed.” Helen Osborne, M.Ed., OTR/L President of Health Literacy Consulting
INSIGHTS ON DISCHARGE/TRANSFER NURSING SUMMARY NOTE*
Use of this note has:
1. Standardized the hand-off of information across the care continuum. 2. Provided excellent communication tool for how care is to be rendered in
the Home environment. 3. Made available baseline of information of 'where the patient is at'
regarding care needs at the time of transition from the previous level of care, (snapshot of the patient).
4. Captured what is presently happening with the patient to hand-off to the next level of care when Home Care is completing the Transfer/Discharge form.
In Summary, the use of the form has focused care around the patient thus improving patient outcomes.
*This form is utilized by some of the hospital, home care, and nursing homes providers in the Pennsylvania QIO Care Transitions Project. It is on the following page of this BPIP.
Sue Kezmarsky, BSN - COS-C, Education and Quality Manager Becky King, BSN, Case Manager Excela Health Home Care and Hospice
- 51

■
■
■
DISCHARGE / TRANSFER NURSING SUMMARY NOTE:1. Complete on all patients. NOTE: This is not a physician order sheet2. Provide copy of code status or advance directive, demographic sheet,
PMH, medication list and nursing summary note to receivingfacility if patient not discharged to home.
3. Reason for transfer:_____________________________________________Date:_____________ Primary Contact/POA:_____________________________Relationship:________________________ Notified : □ Telephone #_________________________ Cell #__________________________
VITAL SIGNS: Temp: P R BP HEIGHT: WEIGHT:CODE STATUS: ALLERGIES:DIAGNOSIS / CHIEF COMPLAINT:IMMUNIZATION/Date: Flu Pneumovax PPD Tetanus PATIENT ID BRACELETSURGICAL PROCEDURE: INCISION SITE / APPEARANCE:PAIN: N/A Chronic Acute Location Last Pain Med Time / TypeCARDIOVASCULAR: PACEMAKER SiteISOLATION / SOURCE: □ NONE IV THERAPY □ NONE
□ Change from Baseline □ C DIFF □ PERIPHERAL □ TPN□ MRSA □ ESBL □ PICC LINE □ IV FLUID□ VRE □ other □ PORT □ IV Antibiotics
□ CULTURE(S) PENDING SITE DATE INSERTED □ OTHER
DIET: APPETITE: Good. Fair Poor MENTAL STATUS: □ Change from Baseline□ NPO □ FEEDS SELF □ ALERT/ORIENTED X 3 □ RESTRAINED
□ □DIET NEEDS ASSIST □ CONFUSED/DISORIENTED
□ □SWALLOWING PRECAUTIONS NGT □ Temporary NG/OG FT □ person □ PLACE □ TIME
□ □LIQ CONSISTENCY: GT □ JT □ COOPERATIVE □ COMBATIVE □ WANDERS
□ BLOOD SUGAR MONITORING □ ENTERAL FEEDING □ OTHER □ ELOPEMENT RISK
Frequency: Type:
SENSORY DEFICIT : □ NONE MOBILITY: □ Change from Baseline□ VISION □ GLASSES AMBULATION: □ SELF □assistance needed
□ HEARING □ HEARING AID □ BED-RIDDEN □ FALL RISK
□ SPEECH □ EXPRESSIVE □ RECEPTIVE □ LOW BED □ BED ALARM
□ EXTREMITY □ WEIGHT BEARING RESTRICTIONS
□ LANGUAGE □ other
□other
ELIMINATION: □ NORMAL RESPIRATORY/OXYGEN MODE/AMOUNT: □ none
□ CONTINENT □ BLADDER □ BOWEL □ PULSE OX % on □ NEBS
□ INCONTINENT □ BLADDER □ BOWEL □ CONTINUOUS L/M via □ HS via
□ COLOSTOMY □ LAST BM □ PRN L/M via □ other□ ILEOSTOMY □ ILEOCONDUIT Last Changed □ VENT □ TRACH SIZE LAST CHANGED
□ FOLEY INSERTION DATE Size □ BI-PAP □ C-PAP Patient Owned? Settings Confirmed?□ DIALYSIS X WEEK ACCESS: □ Respiratory Status CHANGED From Baseline
Days scheduled (circle): M T W Th Fr Sa □ Patient counseled to QUIT if they smoke or use tobacco products
SPECIAL EQUIPMENT: □ none □ walker □ cane
________________________________________________ □ CPM □ SPLINT □ BRACE
SKIN INTEGRITY / TREATMENT □ Normal □
□ Rash _________________________________________________________________________________
□ skin Tear ________________________________________________________________________________
□ Wound/Tx_______________________________________________________________________________
□ Decubiti / #____________ Stage______________________ #____________________ Stage___________
#__________Stage______________________ #__________________Stage___________
(ENTER LOCATION NUMBER OF EACH ULCER ON DIAGRAM)
□ Wound Vac □ OTHER:___________________________________________________
□ QUAD CANE □ W/C
□ other
Braden Score
Patient Discharged/Transferred To:
Nurse Signature:White Copy - Original (Chart)
________________________________ via_________________________________ at_______________________________AM / PM
________________________________ Date / Time__________________________ Unit_____________Phone Number_____________*** CALL WITH ANY QUESTIONS*** Canary Copy - Transfer Facility exc 9600-018 (Rev. 9/09)
FRONT
BACK
BED .
DO NOT WRITE
IN THIS SPACE
EXCELA HEALTH DISCHARGE/TRANSFER NURSING SUMMARY NOTE
Frick HospitalLatrobe HospitalWestmoreland Hospital
YES NO TEMPORARY
YES NO YES NO +1 +2 +3 +4
Patient Owned?
Number EXC 9600-018 (Rev. 9/09) Canary Copy - Transfer Facility White Copy - Original (Chart)
Yes No
EDEMA

_____________________________________ _______________________________
IV Therapy: □ N/A□ Designated Caregiver:□ Willing and able to learn IV administration? Yes No□ Home infusion vendor noted on discharge instructions
OstomySupplies:
□ N/ABrand SizesSpecial Needs
*DressingSupplies:
□ N/A□ Dressing/Wound instructions noted on discharge instructionsType* Patient should have at least 24 hours of supplies sent home at discharge
Labs/Testing: □ N/ALast PT/INR ResultsNext PT/INR Due Results toOther labs ordered DueSpecial instructions□ Other diagnostic testing after discharge noted on discharge instructions
PhysicianInformation:
• Ordering (Referring) Physician(First and Last Name)
• Attending (PCP) Physician(First and Last Name)
VisitAddress:
□ Patient’s Home Address□ Other:
Visit Location Contact Info:
If different than Demographic Sheet Information (Patient’s Home Address)Phone Number:
FOR USE WITH HOME HEALTH REFERRALS ONLY
Additional information needed at discharge for patients who are ordered and will receive home health/home infusion services at discharge:
DO NOT WRITE
IN THIS SPACE
PhysicianInformation:
If different than Demographic Sheet Information (Patient’s Home Address)Phone Number:___________________________________
Signature of Health Care Provider Date/Time

Care Transitions: Barriers and Strategies
BARRIER STRATEGY Hospital patients not Use navigational resources to educate potential referral referred to home health source of appropriate home health referrals (See
Associated Resources: Options for Next Level of Care - poster and pocket card, Discharge Criteria -links patient risk to appropriate hospital discharge care setting and Medicare Beneficiary Discharge Reference List- guide on referral to home health under the Medicare benefit)
Strategize with hospitals concerning patients who initially refuse home care. Does the hospital make a follow-up call with the patient after they are home to check on the patient? Patient may be willing to accept home care after hospital discharge
Lack of engagement of physicians
Share specific success stories with the physician -demonstrate how your agency is able to coordinate and provide care to a patient allowing him / her to remain in their home and avoid a rehospitalization
Aim marketing to physician on what the agency has to offer—agency “niche” (HF, Wounds, etc), nursing skills, and experience
Pair nurses with physician practices - both parties will become familiar with each other’s practices which will increase communications
Actively practice care coordination – ensure all hospital discharged patients are seen by the primary care provider within 7 days of discharge*
Home health staff not Confirm that staff understands appropriateness in acknowledging the requesting a referral for other disciplines. importance of improving Ask intake staff to evaluate “PT only patients” who are patient care as they on multiple medications for possible SN referral. transition from one care Make sure nurses understand medication reconciliation setting to another is just one part of medication management. Medication
Management includes assessment, reconciliation,
simplification, and ongoing medication assessment
and review throughout the episode
Commit your goals and interventions to an Action
Plan (The Institute for Healthcare Improvement --
How-To Guide: Creating an Ideal Transition Home is a
comprehensive document that includes action and
progress documentation resources. This is part of the
Transforming Care at the Bedside Series. You will need
to register to retrieve this free resource)
- 54 -

Care Transitions: Barriers and Strategies
BARRIER STRATEGY
Know what resources have worked with the CT QIO project home health agencies: o Patient Emergency Plan (see January 2010 BPIP) o Coaching (Found in the “Focus on Care Transitions”, “Insights” and “Success Stories” in this BPIP)
o “Personal Health Record” (Example in April 2010 BPIP)
o Zone Tools (Examples in January 2010 BPIP) Healthcare providers Use consistent messaging (List three things the (facilities, physicians, patient must know to maintain their disease process other HHAs) in your outside of the hospital - this can be shared and community are not reinforced across all provider settings) working together Use teach-back (Several types of teach-back resources
are available under Associated Resources)
Become knowledgeable of the 30-day readmission criteria for hospitals
Staff opposition/frustration
Dialogue with staff to determine points of frustration regarding care transition improvement while uncovering system issues that may be contributing to the problem
Include staff in the development and implementation of a consistent and effective approach to reconciliation
Ensure a process for interdisciplinary communication exists and use an interdisciplinary care plan between staff and other settings if possible (e.g. see Discharge/Transfer Nursing Summary Note in Cross Setting I BPIP or utilize an agency care plan that is succinct but communicates vital information)
* Primary care provider follow-up within 7 days post-hospitalization is important. Hernandez, Greiner, Fonarow, Hammill, Heidenreich, Yancy, Peterson and Curtis found for heart failure, physician follow-up within 1 week of discharge was low and varied across hospitals. Rates of 30-day hospital readmission were lower for patients with higher rates of early follow-up.
The Care Transitions: Barrier and Strategy resource was developed with the assistance of the Quality Improvement Organizations in the Care Transitions Project and the Care Transitions Quality Improvement Organization Support Center.
- 55 -

SBAR Worksheet
Communicating with a physician about a patient issue or complication
S Situation Identify yourself and the patient. Briefly state the problem, what it is, when it happened or started and how severe it is or appears to be.
This is <your name> from <your agency> calling about your patient <name>
The problem I am calling about is _________________
B Background: Provide pertinent background information related to the Situation. This may include diagnoses, current medications, most recent pain intensity score, most recent lab results, and the patient’s code status.
A Assessment: Say what you think is the problem. State specifically why you are calling and what the issue is today.
I think the problem is ______________ The problem seems to be ______________________
I am not sure what the problem is but I’m concerned because _______________________
R Recommendation: State your recommendation or what you want, or
ask the physician what they would like to do if you do not know.
I suggest or request that you <say what you would like to see done>
*Adapted with permission from material of Kaiser Foundation Health Plan, Inc., California Regions

collaboration for home care advances in management and practice
champ-program.org
Review of the SBAR Technique
CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation

The SBAR Technique
The SBAR Technique promotes systematic and efficient communication between health care professionals about a particular patent condition orissue.
SBAR stands for: Situation
Background
Assessment
Recommendation
SBAR provides a script that can be used to organizeinformation for communicating collaboratively with a physician about a patient. It is effective both verbally and in writing.
2

The SBAR Technique: Situation
Identify yourself and the patient. Briefly state the problem, what it is, when it happened or started, how severe it is or appears to be.
“Dr Austin? This is Jane Williams from Lakewood County Home Care. I’m calling because our mutual patient, Adele Sorensen, is experiencing dizziness, fatigue, and reports losing her balance 3 times a week.”
3

The SBAR Technique: Background
Provide pertinent background information related to the Situation. This may include diagnoses, current medications, most recent vital signs, most recent lab results (and results of previous tests for comparison if relevant), or code status.
“Ms. Sorensen, has just been discharged following hospitalization for a hip fracture and is currently undergoing physical therapy to restore ambulation. She has a history of chronic anxiety disorder and has been taking Valium 10mg bid. The only other medication she is taking is Motrin 400mg prn for occasional hip pain. Her vital signs are all normal. She reports being fearful of falling while doing her exercises or ambulating.”
The biggest challenge at this step is in not giving more information than is necessary. Be prepared to offer other information if asked, but consider “What information will the physician find useful to address this particular issue?”
4

The SBAR Technique: Assessment
Say what you think is the problem or state specifically why you are calling and what the issue is today.
“I suspect Ms. Sorensen’s dizziness and loss of balance are related to her Valium, which has a long half life in elderly patients. I fear that continued use of this medication will result in her falling and possibly another fracture.”
5

The SBAR Technique: Recommendation
State your recommendation or what you want, or ask the physician what they would do if you do not know.
“Can you prescribe a different anxiolytic for Ms. Sorensen? Or would you prefer to see her in your office first?”
At the conclusion of the communication, document the patient’s condition, the physician notification, and any change in the plan or orders. If the physician has no orders, document their response.
6

SBAR Worksheet*
Communicating with a physician about a patient issue or complication
S Situation Identify yourself and the patient. Briefly state the problem, what it is, when it happened or started and how severe it is or appears to be. This is <your name> from <your agency> calling about your patient <name>
The problem I am calling about is _________________
B Background: Provide pertinent background information related to the Situation. This may include diagnoses, current medications, most recent pain intensity score, most recent lab results, and the patient’s code status.
A Assessment: Say what you think is the problem. State specifically why you are calling and what the issue is today.
I think the problem is ______________
The problem seems to be ______________________
I am not sure what the problem is but I’m concerned because _______________________
R Recommendation: State your recommendation or what you
want, or ask the physician what they would like to do if you do
not know.
I suggest or request that you <say what you would like to see
done>
*Adapted with permission from material of Kaiser Foundation Health Plan, Inc., California Regions 7

Transitional Care Model
Ten Core Elements
1. In-hospital assessment, preparation, and development of an evidence-based plan of care.
2. Consistency of provider across entire episode with a transitional care nurse as the primary coordinator of care.
3. Regular home visits with telephone support for an average of two months.
4. Transitional care nurse accompanying patients to first follow-up visit.
5. Comprehensive, holistic medicine practices focus on patient’s needs, including primary and coexisting events.
6. Active engagement of patients, families and caregivers including education and support.
7. Education regarding early identification and response to health care risks and symptoms and avoidance of adverse and untoward events.
8. Multidisciplinary approach to care that includes patient, family and caregivers as a team.
9. Physician-nurse collaboration.
10. Communicate to, between, and among the patient and family, informal caregivers and health care providers and professionals.
The Transitional Care Model (TCM) provides comprehensive in-hospital planning and home follow-up for chronically ill high-risk older adults hospitalized for common medical and surgical conditions. More information on the Transitional Care Model can be found on the TCM website: http://www.transitionalcare.info
The following link will take you to the CHAMP website and features a video on Dr. Mary D. Naylor describing the Transitional Care Model and how it can serve as a platform for home care clinicians that are building plans of care for frail older adults that are making the transition from hospital to home. http://www.champ-program.org/blog/?p=786
The National Association for Home Care & Hospice has a recorded webinar available on the Transitional Care Model. This webinar features Dr. Mary Naylor and was recorded October 12, 2010. Information available at http://www.nahc.org
- 64

TRANSLATING RESEARCH INTO PRACTICE Despite the evidence establishing the linkage between TCM and enhanced value, a number of organizational, regulatory, financial and cultural barriers have prevented the model’s adoption.
In response to these challenges and with the support of a number of foundations,4 the Penn team formed partnerships with leaders of the Aetna Corporation (Aetna) and Kaiser Permanente Health Plan (KP) to translate and integrate the TCM for use in everyday practice and promote widespread adoption of the model by demonstrating its effectiveness among at risk, chronically ill older adults. The findings of this translational research effort have resulted in TCM being identified as a “high value” proposition by Aetna leaders. The project with KP is ongoing. Based on the improvements in health outcomes, member and physician satisfaction and the reductions in rehospitalizations and total health care costs observed in the Aetna project, the University of Pennsylvania Health System (UPHS) has adopted TCM as a service and local insurers are expected to reimburse UPHS for delivery of TCM to their members in 2009.
CONTINUING TO ADVANCE THE SCIENCE The Penn team is currently testing the effects of TCM among hospitalized cognitively impaired older adults in the Enhancing Care Coordination project.5 Medicare costs for cognitively impaired patients are three times higher than for other older adults. Another ongoing study, Health Related Quality of Life (HRQoL): Elders in Long Term Care,6 is helping to making the case to expand the application of TCM among elders receiving long-term care. Frail older adults receiving both acute and long-term care services are arguably the most vulnerable of patient groups.
1. Naylor MD, Brooten D, Jones R, Lavizzo-Mourey R, Mezey M, & Pauly M. Comprehensive discharge planning for the hospitalized elderly. Ann Intern Med. 1994;120:999-1006. 2. Naylor MD, Brooten D, Campbell R, Jacobsen BS, Mezey MD, Pauly MV, & Schwartz JS. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-620. 3. Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, & Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc. 2004;52:675-684. 4. The Commonwealth Fund; Jacob & Valeria Langeloth Foundation; The John A. Hartford Foundation, Inc.; Gordon and Betty Moore Foundation; California HealthCare Foundation. 5. PI: Naylor, MD. Hospital to Home: Cognitively Impaired Elders and Their Caregivers. Sponsored by: National Institute on Aging, R01-AG023116-04, and the Marian S. Ware Alzheimer’s Program (2005-1010). 6. PI: Naylor, MD. Health Related Quality of Life: Elders in Long-Term Care. Sponsored by: National Institute on Aging, the National Institute of Nursing Research, R01-AG025524-03, and the Marian S. Ware Alzheimer’s Program, 2006-2011. www.transitionalcare.info
TTRRAANNSSIITTIIOONNAALL CCAARREE
MMOODDEELL

OOvveerrvviieeww ooff tthhee TTrraannssii tt iioonnaall CCaarree MMooddeell ((TTCCMM)) Given the expected growth of older adults coping with complex chronic conditions, rapidly rising health care costs and a projected shortfall in the Medicare Trust Fund, there is an urgent need to promote older adults’ access to high quality, cost-effective and efficient services such as those provided via the TCM.
For the millions of older Americans who suffer from multiple chronic conditions, the TCM emphasizes identification of patients’ health goals, coordination and continuity of care throughout acute episodes of illness, development of a rationale, streamlined plan of care to prevent future hospitalizations, and preparation of the patient and family caregivers to implement this care plan—all accomplished with the active engagement of patients and their family caregivers and in collaboration with the patient’s physicians and other health team members.
1100 EEsssseenntt iiaall EElleemmeennttss ooff TTCCMM TCM targets older adults with two or more risk factors, including a history of recent hospitalizations, multiple chronic conditions and poor self-health ratings.
1. The transitional care nurse (TCN), a master’s prepared nurse with advanced knowledge and skills in the care of this population, as the primary coordinator of care to assure continuity throughout acute episodes of care;
2. In-hospital assessment, collaboration with team members to reduce adverse events and prevent functional decline, and preparation and development of a streamlined, evidenced-based plan of care;
3. Regular home visits by the TCN with available, ongoing telephone support (seven days per week) through an average of two months post-discharge;
4. Continuity of medical care between hospital and primary care providers facilitated by the TCN accompanying patients to first follow-up visit(s);
5. Comprehensive, holistic focus on each patient’s goals and needs including the reason for the primary hospitalization as well as other complicating or coexisting health problems and risks;
6. Active engagement of patients and family caregivers with focus on meeting their goals;
7. Emphasis on patients’ early identification and response to health care risks and symptoms to achieve longer term positive outcomes and avoid adverse and untoward events that lead to readmissions;
8. Multidisciplinary approach that includes the patient, family caregivers and health care providers as members of a team;
9. Physician-nurse collaboration across episodes of acute care; and
10. Communication to, between, and among the patient, family caregivers, and health care providers.
wwwwww..ttrraannssiittiioonnaallccaarree..iinnffoo
EEffffeeccttss oonn QQuuaall ii ttyy,, CCoosstt ,, aanndd VVaalluuee The TCM has been tested and refined for more than 20 years by a multidisciplinary team of clinical scholars and health service researchers from the University of Pennsylvania. Across three National Institute of Nursing Research (NINR)-funded RCTs completed to date,1-3 TCM has demonstrated improved quality and cost outcomes for high risk, cognitively intact older adults when compared to standard care:
9 Reductions in preventable hospital readmissions for both primary and co-existing healthconditions. Additionally, among those patients who are rehospitalized, the time between their index hospital discharge and readmission was increased and the number of inpatient days decreased.
TCM's Impact on Readmission Rates After Index Hospitalization
70% 60% 50%
% of 40% Patients 30%
20% 10%
0%
10%
28%
48%
23%
56% 61%
at 6 at 26 at 52
weeks1 weeks2 weeks3
Readmission After Hospital Discharge
TCM Group
Control Group
9 Improvements in health outcomes. In the most recently reported RCT,3 short term improvements in physical health, functional status, and quality of life were reported by patients who received TCM.
9 Enhancement in patient satisfaction. Overall patient satisfaction has increased among patients receiving TCM.
9 Reductions in total health care costs. Both total and average reimbursements per patient have been reduced in TCM focused RCTs.2-3
* Total costs were calculated using average Medicare reimbursements for hospital readmissions, ED visits, physician visits, and care provided by visiting nurses and other healthcare personnel. Costs for TCM care is included in the intervention group total. ** Naylor et al., JAMA, 1999; *** Naylor et al., JAGS, 2004
$6,661
$12,481
$3,630
$7,636
at 2
6w
eeks
**
at 5
2w
eeks
***
Dollars (US)
TCM's Impact on Total Health Care Costs*
TCM Group
Control Group
‡ ▲
‡
▲
‡
‡
‡ ‡
‡ ▲
▲▲
▲
▲
▲

SUCCESS STORIES
There are four success stories featured in the Cross Setting I BPIP. The success stories will give your agency and staff some tangible ideas for improving care transitions. The featured agencies are:
1. Seton Home Health 2. Amedisys Home Health
Services 3. Eddy Visiting Nurse
Association/Northeast Health (includes tools this agency uses for coaching)
4. Gentiva of Nashville
INSIGHTS
Improving communication with physicians has improved our hospitalization rate: • We preplan care with orthopedic surgeons. We have worked with
these physician groups to know their protocol ahead of time so we can streamline processes.
• Our outcomes include relevant practical information: degrees of ROM for knees, the TUG score or gait score for a frequent faller
• Nurses use SBAR—it is effective
Practical tips to decrease hospitalizations: • Patient offered a plastic container for meds with agency name/phone
number at top and we tell them to take to physician appointment • Our standard is for any patient with more than one discipline involved to
case conference to improve collaboration • We case conference every Wednesday/Thursday morning and ask: Who
can we intervene on before this weekend? Could we do some intervention that prevents a hospitalization?
Pam Perez, PT, Safe Strides® Specialty Director, Gentiva® Nashville, TN
- 67

PHYSICIAN ADVISORY GROUP The following are ideas and information gathered from a meeting of the HHQI campaign physician advisory panel (see page 3 of this BPIP for a list of the physicians on the panel).
Tips from the physican group to improving communication between providers: • Use and update systems
to include notifications to other providers of patient admissions/discharges
• Each provider must be accountable to make the call/send the fax to the PCP or other provider
Use and share navigational
"It is critical to update the patient's PCP. Include the PCP phone number and fax number on the patient record when the patient is going to the ED or hospital. Ask hospital providers to notify the PCP when patient is admitted and discharged and provide a copy of the discharge summary within 24 hours of discharge, or ideally at the time of discharge to the patient. Successful hospital discharges/transitions programs set a goal of including the PCP 100% of the time."
Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST®
Society of Hospital Medicine
resources with physician offices and Family Practice Management (September/October hospitals. 2010) has an article describing coaching: Health (See Associated Resources: Options Coaching for Patients With Chronic Illness.for Next Level of Care - poster and This is primarily written for primary care providers. pocket card, Discharge Criteria (Authors: Bennett, Coleman, Parry, Bodenheimer & Chen) links patient risk to appropriate hospital
discharge care setting and Medicare Beneficiary Discharge Reference List- guide on referral to home health under the Medicare benefit.)
Physicians tell us that they appreciate SBAR! • SBAR is organized in a way to facilitate
how physicians are trained to communicate
• SBAR is an effective way to communicate important information.
“Home care is well positioned to be the care coordinator for patients that are in transition between provider settings.”
Steven L. Yount, DO, Solo Family Practitioner, Clinical Assistant Professor, Adjunct, Department of Family Medicine, University of North Texas Health Science Center, Texas College of Osteopathic
“Physicians that are concerned about their reputational risk and possible financial impact of reported readmission rates will be interested in better care coordination models. The Cleveland Clinic has helped develop a multicomponent model that includes pre-discharge preparation, structured home health, telehealth monitoring, telephonic health coaching and care coordination-some of the components are for patients irrespective of home health eligibility---I believe this will be an important function in home health.” Steve Landers, MD, MPH - Medical Director, Center for Home Care and Community Rehabilitation, Cleveland Clinic Foundation
- 68

INSIGHTS
Our coaching model: • Use a modified The Care Transitions ProgramSM model • Target specific diagnosis groups. We target HF, COPD, Diabetes,
CAD (request from payer), ESRD, and Pneumonia. • Coach has 2 visit encounters and does follow-up phone calls
• Hospital encounter is to begin early care transitions planning: Can patient afford medications? Does he/she have transportation to the doctor’s office? Schedule PCP appointment within 7 days of hospital
discharge. • In-home assessment made 1-2 days after hospital discharge
to: Evaluate patient’s literacy level Complete Personal Health Record Coach about disease—red flags (similar to ZONE tools) Take patient toolkit (scale, spirometer, medication box,
and low-salt cookbook if appropriate) Make sure patient has a PCP appointment within 7
days of hospital discharge Complete medication reconciliation Fax reconciled medication list to the primary care
physician so he/she has it before the patient arrives for the follow-up appointment
• Caregiver is included in visit and phone encounters • Phone coaching continues weekly for 4 weeks
• Sustain the coaching program: • Track your outcomes
Total number of patients coached: 273 Total number of patients rehospitalized: 13.5%
• Recognize that some patients need both home care and coaching
• Send patient vignettes (successes) to payers and other providers weekly
Michelle Mazzacco, Director, Eddy Visiting Nursing Association Patrick Archambeault, Director of Clinical Specialties, Eddy Visiting Nursing Association Troy, NY
See the Eddy Visiting Nurse Association Success Story (pg.67) for more on their program.
- 69

TRACKING DATA AND MEASURING PROGRESS
HHQI Data Reports The data is available for all HHQI registered agencies.
What are they? • Your agency’s reports for ACH and Oral Medications based on OASIS-C
data. • A unique look into the potential causative factors focusing on M2020
from OASIS-C for the Oral Medication report and M2410 for the ACH report (for the September 2010 reports)
• Remember all the data—agency, state and national rates are not adjusted!
How do I access the HHQI Data Reports? • Step 1: Go to the HHQI Web site, www.homehealthquality.org • Step 2: Click on the Data tab,
https://secure.homehealthquality.org/default.aspx
• Step 3: Log in with your Data Access username and password. If you do not have a Data Access username and password yet, please register.
o For more detailed instruction on registering for the data site watch the Data Access Tutorial webinar for the registration process.
o Also read the FAQ’s: Data Access Reports
Contact HHQInfo at [email protected] for further assistance.
- 70

BEST PRACTICE INTERVENTION PACKAGE TIMELINE
Release Date begin on 10/28/2010
Within 3-4 weeks __/__/2010
Within 4-6 weeks __/__/2010
Within 6-8 weeks __/__/2010
Within 8-12 weeks __/__ 2010
Download BPIP Package
Schedule team to review package
Continue Staff Education
Implemention of new tools/process changes
Begin evaluation of process changes
Begin some preliminary staff education on care Team decides on transition a plan and Conduct small
HHHH
AA BB
PP IIPP
II mmpp ll
ee mmee nn
tt aatt ii oo
nn TT
ii mmee ll
ii nnee concepts and
why agency needs to get involved
selects tools/resources based on audit and staff input
tests of change (e.g., Plan/Do/Study/ Act)
Revise Process as necessary
Schedule a brainstorming session or seek staff input in other ways--through email or other means
Plan and initiate efforts to reach other community providers with need to improve care transitions
Begin meeting with other community providers
Identify ways your agency may need to improve internal processes and structure--communication, staff educational needs.
Start tracking rehospitalization rates
Follow up on all patients who experience a readmission--review their record for missed opportunities and talk with the patient/caregiv er to get his/her perspective
- 71
HH
A B
PIP
Impl
emen
tatio
n Ti
mel
ine
HH
A B
PIP
Impl
emen
tatio
n Ti
mel
ine

ORGANIZATIONAL CULTURE
The Cross Setting I BPIP discusses care transitions and aligning/communicating with other care providers. An examination of internal communication within the agency is also appropriate. Leaders need to ensure that communication is ongoing between staff and management as well as between disciplines. One aspect of communication is fostering a blame-free culture that supports and learns from employee oversights or mistakes and focuses on improving patient care and outcomes. Obviously, staff must be held accountable for behavior that recklessly disregards agency standards and protocols, but fostering a transparent environment so staff are prone to report misjudgments,
“We must continue to change our expectations of oversights, or errors is each other. Our focus must be less about human
essential to being able to error, and more about behavioral choices. Less improve. For example, about blame, and more about learning”. learning how to reduce hospitalizations by examining David Marx (Whack.A.Mole, p. 127) patient hospitalizations or rehospitalizations is a step toward improvement. There may be some apparent or not-so-obvious ‘lessons learned’ that help your staff prevent future hospitalizations.
This type of environment is called Just Culture—“a just culture recognizes that competent professionals make mistakes and acknowledges that even competent professionals will develop unhealthy norms (shortcuts, “routine rule violations”), but has zero tolerance for reckless behavior.” [Agency for Healthcare Research and Quality (AHRQ)] Thus learning from “For those who run or regulate organizations, the errors (or potential errors) is a incentive to have a just culture is very simple. culture your agency wants Without it, you won’t know what’s going on”. to cultivate.
Sidney Dekker (Just Culture: Balancing Safety and Effective managers look for Accountability, p. 26) ways to educate clinicians, and this fosters a proactive and learning environment. The following are links to helpful CHAMP resources. The first looks at coaching clinicians. The second provides additional opportunities for clinicians (For example--learn how to improve communications with physicians). • Clinical Coaching --An overview of a strategy to help front line managers
move evidence more quickly into practice among home care clinicians. • See CHAMP’s other Programs & Learning, including Improving
Communication with Physicians
- 72

INSIGHTS We use a system-wide nurse liaison position which improves care coordination by: • Enhanced Communication – Physicians and hospital staff know who to call
for home care referrals. They are recognized on the floors and answer questions as needed. Our liaisons not only complete our referrals but offer freedom of choice to all patients and communicate this information to each home health agency. They assist with DME supplies for patients going home and also IV therapy/tube feedings.
• UP-To-Date medical information - With the use of laptops and accessibility to the hospital system, Home Health Agencies receive the latest hospital information, labs, discharge instructions and test results.
• Patient Satisfaction – Patients are more comfortable with a face-to-face encounter with a home health representative that can explain home care, the disciplines involved and what to expect, verify demographics, emergency contacts and discuss the layout of the home for DME accessibility.
• Staff Satisfaction – With all of the updated hospital information going out to home health staff on their laptops, they are more prepared to complete a thorough admission visit. They are able to see the hospital diagnoses, tests and the results, medication profile, past medical and surgical histories, immunizations and all physicians involved in the patient’s care.
• More accurate SOC date –With the implementation of OASIS-C there is a greater need for a more accurate SOC date. The liaison’s provide updates as to delays in discharges, setting changes from home to SNF’s etc.
• More accurate medication lists – Liaisons and home health staff are able to see an up to date medication listing while patients are hospitalized and are able to reconcile with the medications at home on the first visit to the patient.
Patricia Fletcher RN, BSN, Senior Manager of Outcomes, UPMC/Jefferson Regional Home Health
- 73

i
Skilled Nursing Track: Focus on Care Transitions SN CHECKLIST: Do you:
� Know your agency ACH rate? Understand how many of the hospitalizations are rehospitalizations?
� Know when/which patients are most at-risk for rehospitalizations?
� Know your patient’s risk factors for ACH and interventions [e.g., fall risk (therapy), Heart Failure (telehealth), Wound needs (WOCN).] Intervene early and refer to other disciplines as appropriate to help prevent rehospitalizations.
� Send patient’s PCP (and other physicians as appropriate) a typed list of all current patient medications within 24 hours of admission to home care?
� Ensure that all hospital discharged patients are seen by the primary care provider (and other physicians as appropriate) within 7 days of hospital discharge? Consult with MSW if transportation is a problem for the
Hospitals
Health Agencies
Phys cianOffices
NursingHomes
Stakeholders (local, state
and national)
Home Health
Agencies
CommunityBased
Services
patient? � Understand your role in improving
transitional care at your agency? Some of the terms used in care transitions are in the blue boxes on this page.
“Among hospitals with higher rates of early (physician) follow-up, the risk of 30-day readmission was lower (for heart failure)” Hernandez et al. (2010).
� Communicate with other providers either at a transfer (e.g. ED) or at a discharge (e.g. nursing home)? We are both a Sender and Receiver for care transitions.
� Use SBAR? This is a briefing model that has been adopted by many hospital, home care, and nursing home clinicians. SBAR resources are available in this BPIP. Ask your QI director or manager for a copy of SBAR.
� Think about communication within your agency as an opportunity to improve care transitions? SN to therapist, etc.
• Sender: The health care professional who is accountable for the sending of key information necessary to ensure continuity of care.
• Receiver: The health care professional who is accountable for receiving the key information (usually at the next care setting) shared by the sender about the patient undergoing transition.
• Transitional care encompasses the sending and the receiving aspects of the transfer and is essential for persons with complex needs and their caregivers.
• Care Transitions is the actual experience of the care recipients.
Discussion question: • As a Receiver, what do you need to
know to safely care for your patient? • As a Sender, what information do you
send to other care providers?
- 74

i i
Therapy Track: Focus on Care Transitions THERAPY CHECKLIST: Do you:
� Know your agency ACH rate? Understand how many of the hospitalizations are rehospitalizations?
� Know when/which patients are most at-risk for rehospitalizations?
� Know your patient’s risk factors for ACH and interventions [e.g., medication management issues (SN), Heart Failure (SN, Telehealth), Wound need (WOCN).] Intervene early and refer to other disciplines as appropriate to help prevent rehospitalizations.
� Understand your role in improving transitional care at your agency? � Ensure that all hospital discharged patients are seen by the primary care
provider (and other physicians as appropriate) within 7 days of hospital discharge? Consult with MSW if transportation is a problem for the patient?
� Understand your role in improving transitional care at your agency? Some
Hospitals
Health Agencies
Phys c anOffices
NursingHomes
Stakeholders (local, state
and national)
Home Health
Agencies
CommunityBased
Services
of the terms used in care transitions are in the blue boxes on this page.
� Communicate with other providers either at a transfer (e.g. ED) or at a discharge (e.g. nursing home)? We are both a Sender and Receiver for
“Among hospitals with higher rates of early (physician) follow-up, the risk of 30-day readmission was lower (for heart failure)” Hernandez et al. (2010).
care transitions. � Use SBAR? This is a briefing model that has been adopted by many
hospital, home care, and nursing home clinicians. SBAR resources are available in this BPIP. Ask your QI director or manager for a copy of SBAR.
� Think about communication within your agency as an opportunity to improve care transitions? Therapist to SN, etc.
• Sender: The health care professional who is accountable for the sending of key information necessary to ensure continuity of care.
• Receiver: The health care professional who is accountable for receiving the key information (usually at the next care setting) shared by the sender about the patient undergoing transition.
• Transitional care encompasses the sending and the receiving aspects of the transfer and is essential for persons with complex needs and their caregivers.
• Care Transitions is the actual experience of the care recipients.
Think about the following: • As a Receiver, what do you need to
know to safely care for your patient? • As a Sender, what information do you
send to other care providers?
- 75

i
Medical Social Worker Track : Focus on Care Transitions MEDICAL SOCIAL WORKER CHECKLIST: Do you:
� Know your agency ACH rate? Understand how many of the hospitalizations are rehospitalizations?
� Know when/which patients are most at-risk for rehospitalizations?
� Receive referrals for caregiver issues that may put patient at risk for a rehospitalization?
� Help ensure that all hospital discharged patients are seen by the primary care provider (and other physicians as appropriate)
Hospitals
Health Agencies
Phys cianOffices
NursingHomes
Stakeholders (local, state
and national)
Home Health
Agencies
CommunityBased
Services
within 7 days of hospital discharge? SN and Therapy should be requesting MSW help when patient needs transportation assistance.
� Use SBAR? This is a briefing model that has been adopted by many hospital, home care, and nursing home clinicians. SBAR resources are available in this BPIP. Ask your QI director or manager for a copy of SBAR.
� Understand your role in improving transitional care at your agency? Some of the terms used in care transitions are in the blue boxes on this page.
� Think about communication within your agency as an opportunity to improve care transitions? MSW to therapist, etc.
• Transitional care encompasses the sending and the receiving aspects of the transfer and is essential for persons with complex needs and their caregivers.
• Care Transitions is the actual experience of the care recipients.
“Patients see us as one organization— the more knowledgeable you are about their hospital stay means more to the patients.”
Susan Ambrosy, Quality Manager Seton Health Home Care Troy, NY
Think about the following: • As a Receiver, what do you need to
know to safely care for your patient? • As a Sender, what information do
you send to other care providers?
• Sender: The health care professional who is accountable for the sending of key information necessary to ensure continuity of care.
• Receiver: The health care professional who is accountable for receiving the key information (usually at the next care setting) shared by the sender about the patient undergoing transition.
- 76

i i
Home Health Aide Track: Focus on Care Transitions HOME HEALTH AIDE CHECKLIST: Do you:
� Know your agency ACH rate? � Know when/which patients are most at-risk for
rehospitalizations? � Use SBAR? This is a briefing model that has been
adopted by many hospital, home care, and nursing home staff. SBAR resources are available in this BPIP. Ask your QI director or manager for a copy of SBAR. You can use this in reporting patient information to a nurse or therapist.
� Understand your role in improving transitional care at your agency? Some of the terms
Hospitals
Health Agencies
Phys c anOffices
NursingHomes
Stakeholders (local, state
and national)
Home Health
Agencies
CommunityBased
Services
used in care transitions are in the blue boxes on this page.
� Think about communication within your agency as an opportunity to improve care transitions? HHA to nurse or therapist, etc.
• Transitional care encompasses the sending and the receiving aspects of the transfer and is essential for persons with complex needs and their caregivers.
• Care Transitions is the actual experience of the care recipients.
“Patients see us as one organization— the more knowledgeable you are about their hospital stay means more to the patients.”
Susan Ambrosy, Quality Manager Seton Health Home Care Troy, NY
Think about the following: • As a Receiver, what do you need to
know to safely care for your patient? • As a Sender, what information do
you send to other care providers?
• Sender: The health care professional who is accountable for the sending of key information necessary of ensuring continuity of care.
• Receiver: The health care professional who is accountable for receiving the key information (usually at the next care setting) shared by the sender about the patient undergoing transition.
- 77

Reference List
Agency for Healthcare Research and Quality (AHRQ) http://www.psnet.ahrq.gov/glossary.aspx
Balaban, R.B. & Willliams, M.V. (2010). Improving Care Transitions: Hospitalists Partnering with Primary Care. Journal of Hospital Medicine, 5 (7), 375377. DOI 10.1002/jhm.824
Bennett, H.D., Coleman, E.A., Parry, C., Bodenheimer, T., & Chen, E.H. Health Coaching for Patients with Chronic Illness. Family Practice Management, 17, (5), 24-29.
Bueno, H., Ross, J.S., Wang, Y., Chen, J., Vidan, M.T., Normand, S.L.T., Curtis, J.P., Drye, E.E., Lichtman, J.H., Keenan, P.S., Kosiborod, M., & Krumholz, H.M. (2010). Trends in Length of Stay and Short-term Outcomes Among Medicare Patients Hospitalized for Heart Failure, 1993-2006. The Journal of the American Medical Association, 303 (21), 2141-2147.
Coleman, E.A., Parry, C., Chalmers, S., & Min, S.J. (2006). The Care Transitions Intervention: Results of a Randomized Controlled Trial. Archives of Internal Medicine, 166 (17), 1822-1828.
Coleman, E.A., Smith, J.D., Frank, J.C., Min, S., Parry, C., & Kramer, A.M. (2004). Preparing Patients and Caregivers to Participate in Care Delivered Across Settings: The Care Transitions Intervention. Journal of the American Geriatrics Society. 52 (11), 1817-1825.
Coleman, E.A. (2003). Falling Through the Cracks: Challenges and Opportunities for Improving Transitional Care for Persons with Continuous Complex Care Needs. Journal of the American Geriatrics Society, 52 (4), 549-555.
Coleman, E.A., & Boult, C. (2003). Improving the Quality of Transitional Care for Persons with Complex Care Needs. Position Statement of The American Geriatrics Society Health Care Systems Committee. Journal of the American Geriatrics Society, 52 (4), 556-557.
Dekker, S. (2007). Just Culture: Balancing Safety and Accountability (p.26). Burlington, VT: Ashgate Publishing Company.
Friedman, B., Jiang, H.J., & Elixhauser, A. (2008). Costly Hospital Readmissions and Complex Chronic Illness. Inquiry, 45 (4), 408-421.
Hernandez, A.F., Greiner, M.A., Fonarow, G.C., Hammill, B.G., Heidenreich, P.A., Yancy, C.W., Peterson, E.D., and Curtis, L.H. (2010). Relationship Between Early Physician Follow-up and 30-Day Readmission Among Medicare Beneficiaries Hospitalized for Heart Failure. The Journal of the American Medical Association, 303 (17), 1716-1722.
- 78

Huffman, M., (2007). Health Coaching: A New and Exciting Technique to Enhance Patient Self-management and Improve Outcomes. Home Healthcare Nurse, 25 (4), 271-276.
Jack, B.W., Chetty, V.K., Anthony, D., Greenwald, J.L., Sanchez, G.M., Johnson, A.E., Forsythe, S.R., O'Donnell, J.K., Paasche-Orlow, M.K., Manasseh, C., Martin, S., & Culpepper, L. (2009). A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Annals of Internal Medicine, 150 (3), 178-87.
Jencks, S.F., Williams, M.V., & Coleman, E.A. (2009). Rehospitalizations among Patients in the Medicare Fee-for-Service Program. The New England Journal of Medicine, 360 (14), 1418-1428. Retrieved from: http://www.nejm.org/doi/full/10.1056/nejmsa0803563#t=article
Marx, D. (2009). Whack.A.Mole . Plano, TX: By Your Side Studios.
Naylor, M.D., Brooten, D.A., Campbell, R.L. Maislin, G., McCauley, K.M., & Schwartz, J.S. (2004) Transitional Care of Older Adults Hospitalized with Heart Failure: A Randomized, Controlled Trial. Journal of the American Geriatrics Society, 52 (5), 675-684.
Naylor, M.D., Brooten, D., Campbell, R., Jacobsen, B.S., Mezey, M.D., Pauly, M.V. & Schwartz, J.S. (1999). Comprehensive Discharge Planning and Home Follow-up of Hospitalized Elders: A Randomized Clinical Trial. The Journal of the American Medical Association, 281 (7), 613-620.
Naylor M, Brooten D, Jones R, Lavizzo-Mourey R, Mezey M, Pauley M. (1994). Comprehensive Discharge Planning for the Hospitalized Elderly. Annals of Internal Medicine, 120 (12), 999-1006.
Parry, C., Coleman, E.A., Smith, J.D., Frank, J.C., & Kramer, A.M. (2003). The Care Transitions Intervention: A Patient-Centered Approach to Facilitating Effective Transfers Between Sites of Geriatric Care. Home Health Services Quarterly. 22 (3), 1-18.
Parry, C., Min, S.J., M., Chugh, A., Chalmers, S., and Coleman, E.A. (2009). Further Application of The Care Transitions Intervention: Results of a Randomized Controlled Trial conducted in a Medicare Fee-For-Service Setting. Home Health Care Services Quarterly. 28 (2-3), 84-99.
- 79