Embed Size (px)
Citation preview

Short Communication
Journal of Neuroimaging Vol 13 No 2 April 2003Aly et al: Brain Microembolism
Brain Microembolism Ahmed Aly, MD
Viken L. Babikian, MD
Glenn Barest, MD
Mihran Artinian, MD
Alejandro Forteza, MD
Carlos S. Kase, MD
A B S T R A C T
Purpose. To alert clinicians about the occurrence of a subtype ofbrain infarction, its suspected etiology, and its detection by spe-cific neuroimaging techniques. Methods. The article presents 5nonconsecutive patients admitted to the stroke services of 2tertiary care hospitals, who presented with acute or subacutesymptoms suspicious, but at times atypical, of brain ischemia.Findings. Each patient had evidence of 3 to > 20 small areas ofrecent brain infarction detected by diffusion-weighted imaging(DWI). When available, brain computerized tomography imageswere not helpful for the diagnosis of these recent infarcts. Mostlesions were present on magnetic resonance imaging fluid-attenuated inversion recovery sequences, but the diffusion-weighted images allowed the determination of their acuity. Fur-ther evaluation revealed a potential source of embolism in eachpatient. Brain microembolism was suspected in all cases. Con-clusion. Small and multiple areas of acute or subacute braininfarction occasionally present with clinical features atypical forbrain embolism. They can be detected by magnetic resonanceDWI studies.
Key words: Brain, embolism, stroke.
Aly A, Babikian VL, Barest G,Artinian M, Forteza A, Kase CS.
Brain microembolism.J Neuroimaging 2003;13:140-146DOI: 10.1177/1051228403251187
An “embolic stroke” is usually suspected when a patientpresents with a focal neurological deficit of sudden onsetand is found to have a source of emboli such as atrial fibril-lation. In most emergency rooms today, the clinical fea-
tures of stroke, usually supported by brain computerizedtomography (CT) findings, form the basis of the initialtherapeutic plan. The main clinical, angiographic, andbrain CT features of the major stroke syndromes havenow been established for several decades. They were fur-ther refined during the past decade by the introduction ofnew magnetic resonance imaging (MRI) and CT tech-niques, particularly those pertaining to changes observedduring the first 6 hours after stroke onset.
Not unexpectedly, MRI has enhanced the clinician’sability to image and understand the complex set of eventsthat lead to brain infarction, and to categorize stroke sub-types. The purpose of this article is to alert clinicians aboutthe occurrence of a subtype of brain embolism that causesmultiple small areas of brain infarction and about the abil-ity to detect it with MRI diffusion-weighted imaging(DWI).
Methods
The patients presented herein were selected from admis-sions to the stroke services of the Boston Medical Centerand the Boston Veterans Administration Medical Center
140 Copyright © 2003 by the American Society of Neuroimaging
Received August 23, 2002, and in revised form October 30,2002. Accepted for publication November 5, 2002.
From the Department of Neurology (AA, VLB, CSK) andthe Department of Radiology (GB), Boston UniversitySchool of Medicine; the Department of Radiology, Har-vard Medical School (MA); and the Department of Neu-rology, University of Miami (AF).
Address correspondence to Viken L. Babikian, MD,Stroke Service, Department of Neurology, Boston Uni-versity School of Medicine, 715 Albany Street, D-315,Boston, MA 02118. E-mail: [email protected].

during a 12-month period. They do not represent a con-secutive series.
MRI studies were performed using 1.5-T Philips NT,Intera, and Signa LX General Electric scanners. DWIsequences were obtained on the basis of the single-shot,echo-planar imaging technique with b values of 0 and 800or 0 and 1000. To avoid the T2 “shine-through” effect,apparent diffusion coefficient (ADC) maps werereviewed in all cases. They showed corresponding areasof reduced ADCs and restricted diffusion in all lesionsreported as acute infarcts. Any lesion with an equivocal,normal, or elevated ADC value was considered chronicand preexisting. Some lesions showed increased signal onthe corresponding T2-weighted images. Each study wasindependently reviewed by a neuroradiologist and astroke neurologist.
Patients
Patient 1
This 82-year-old man had a 5-minute episode of “poorcontrol” of his right hand, having difficulty placing lettersin a crossword puzzle even though he was able to hold hispencil and write. The following day, he had a < 5-minuteepisode of mild numbness of the right leg, below the calflevel, in addition to poor control of the leg while walking.This recurred 3 days later, but the numbness extended upto the level of the groin. Although the weakness resolvedcompletely, the numbness persisted after the initial im-provement.
Nine days after the first attack, the patient experienceda < 30-minute episode of visual symptoms. When lookingout of a window, he felt “the tops of the trees wereblurred.” Two similar episodes occurred during the subse-
quent days, leading to his hospitalization. The patient washypertensive, and there was a past history of atrial fibrilla-tion of short duration. He was receiving aspirin (325 mg/d)at the time of these attacks. The principal findings onadmission consisted of a blood pressure of 181/98 mmHg, a regular pulse of 63 beats/min, left-sided neck bruit,and decreased light touch perception below the right calflevel.
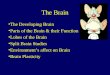
Brain CT was normal on the day of admission, 12 daysafter the initial episode. An MRI study on the day preced-ing admission revealed 6 small areas of restricted diffu-sion consistent with recent infarcts in the left occipital andboth parietal lobes (Fig 1). Five lesions were seen on thefluid-attenuated inversion recovery (FLAIR) sequences,but several were missed on the T2-weighted sequences.Magnetic resonance angiography (MRA) showed a >80% stenosis of the left internal carotid artery (ICA). Arepeat MRI study was unchanged on the day after admis-sion. A transesophageal echocardiogram showed a 5-mm,nonmobile plaque of the ascending aorta.
Patient 2
A 71-year-old woman presented with a 3-day history ofback pain radiating to the left leg. Some left leg weaknesswas detected 1 day prior to admission. One day after ad-mission, she developed left arm weakness, followed 12hours later by left facial weakness. The past history wassignificant for hypertension, hyperlipidemia, diabetesmellitus, and cardiomyopathy. She was receiving daily as-pirin, but the exact daily dose could not be determined.Examination showed a blood pressure of 192/100 mmHg; a regular pulse; and a mild (3/5) left hemiparesis in-volving the face, arm, and leg. There was minor sensoryextinction of the left side in response to visual or tactile si-multaneous bilateral stimulation.
Aly et al: Brain Microembolism 141
Fig 1. Diffusion-weighted images in patient 1. Areas of restricted diffusion are detected in the left occipital lobe and both pari-etal lobes.

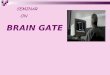
Brain CT was normal on the day of admission. MRIwas obtained hours after the arm weakness developed.The DWI sequences showed 20 areas of restricted diffu-sion. These recent infarcts were < 1.5 cm in diameter andinvolved cortical and subcortical regions of the right fron-tal, parietal, temporal, and occipital lobes (Fig 2). Not alllesions were seen on the T2 sequences, and although allwere detected by the FLAIR sequences, they were not asconspicuously delineated as in the DWI sequences. Non-specific hyperintensities, thought to represent chronicsmall vessel disease, were present in the T2 and FLAIRsequences. There was no stenosis of the right ICA andonly mild to moderate disease of the left ICA.Transthoracic echocardiography showed a hypokineticleft ventricle with an ejection fraction of 20%.
Patient 3
This 79-year-old woman was admitted for evaluation ofintermittent confusion. Four weeks prior to admission, aright index finger atraumatic necrotic lesion was ob-served. During the 3-week period preceding admission,cognitive changes with episodes of staring, fatigue, loss ofappetite, and difficulties with gait were reported. The pastmedical history was significant for chronic obstructivepulmonary disease, congestive heart failure with reducedleft ventricular ejection fraction, and smoking. She was onaspirin (325 mg/d). On admission, her blood pressure was130/64 mm Hg, and her pulse of 84 beats/min was regu-lar. She was alert, fluent, disoriented, and easilydistractable. The neurological examination was otherwiseunremarkable. Two necrotic ulcers of the right index fin-ger were still present. They were thought to be secondaryto thromboembolism.
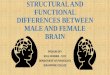
Brain CT was not done. An electroencephalogramshowed bilateral frontal slowing. DWI MRI on the day ofadmission revealed > 10 recent small infarcts in the pons,left centrum semiovale, and right periventricular region.There was extracranial occlusion of the left ICA. Intrave-nous anticoagulation was initiated. Several transient epi-sodes of decreased responsiveness occurred during thehospitalization, but there were no other focal changes onthe neurological examination. A repeat MRI examina-tion, 4 days after the first, showed > 15 small, subcorticalDWI lesions of the right occipital lobe, periventricularregion, as well as the centrum semiovale (Fig 3). At least 5of these lesions were not detected at the time of the firststudy. Again, the majority of lesions were not seen in theT2 sequences, and although most were identified in theFLAIR sequences, they were not as conspicuous. Atransesophageal echocardiogram showed mobileatherosclerotic plaques in the ascending and descendingaorta.
Patient 4
This 50-year-old man presented with a 24-hour history ofmental status changes, slurring of speech, and difficultywalking of sudden onset. The past medical history was sig-nificant for hypertension, diabetes mellitus, cirrhosis withupper gastrointestinal bleeding, and remote cocaine use.He was not receiving antiplatelet agents. His blood pres-sure on admission was 102/62 mm Hg, with a regularpulse of 113 beats/min. The patient was confused and dis-oriented to time, and he had gaze deviation to the rightwith left visual field neglect. A mild (4/5) left hemiparesisinvolved the face, arm, and leg.
142 Journal of Neuroimaging Vol 13 No 2 April 2003
Fig 2. Diffusion-weighted images in patient 2 showing left temporal, periventricular, and corona radiata areas of restricteddiffusion.
A B C

Emergent brain CT showed 5 bilateral periventricularand corona radiata lucencies of undetermined age. Therewas no change on a repeat study 2 days later. Bilateralslowing was present on electroencephalography. Atransesophageal echocardiogram showed a patent fora-men ovale. More than 20 areas of brain infarction involv-ing the periventricular and corona radiata regions bilater-ally, as well as the right temporal and left occipital lobes,were seen on the MRI DWI study (Fig 4) obtained on theday of repeat brain CT. These lesions were either notidentified at all or not as clearly seen in the T2 images, butall were detected by the FLAIR sequences. MRA showedno substantial stenosis of the intracranial and extracranialarteries.
Patient 5
A 68-year-old man was admitted with a 1-week history ofrecurrent episodes of transient word-finding difficulty.Episodes occurred as often as 3 times daily, and eachlasted up to 1 hour. The patient understood what he wastold and knew what he wanted to say, but he “just couldnot say it.” There were no other associated neurologicalsymptoms. Moreover, during the 2-week period preced-ing admission, 3 episodes of left-sided monocular visualloss, described as “a curtain dropping down,” were re-ported. Episodes were painless, and each lasted secondsto minutes. The past medical history was remarkable forhypertension, diabetes mellitus, and throat cancer treatedwith radiation therapy > 25 years prior to admission. Epi-sodes occurred while the patient was on aspirin at 325mg/d. On admission, his blood pressure was 125/59 mmHg, and his pulse was regular. The neurological examina-
tion was non-revealing. A transient episode of word-find-ing difficulty occurred 2 days after admission.
A contrast-enhanced brain CT was normal on admis-sion. The DWI sequences of the MRI study obtained 48hours later showed a small left insular infarct and 3 areasof restricted diffusion involving the left temporal andperiventricular white matter (Fig 5). These lesions weremost clearly identified in the DWI sequences, and somewere missed in the T2 and FLAIR sequences. In addition,nonspecific hyperintensities, thought to be secondary tochronic small vessel disease, were present in the T2 andFLAIR images. MRA showed a severely stenotic lesioninvolving the distal 2 cm of the left common carotidartery, with diminished caliber of the left ICA throughoutits course. This was subsequently confirmed by catheterangiography.
Aly et al: Brain Microembolism 143
Fig 3. Patient 3. Areas of restricted diffusion are detected in the pons, right occipital lobe, and the corona radiata bilaterally.
BA C
Discussion
The patients described in the preceding paragraphs pre-sented to medical attention with a variety of neurologicalsymptoms, most suggestive of brain ischemia. Brain CTscans were nondiagnostic, and MRI DWI sequences re-vealed relatively small areas of brain infarction in allcases. When taken together, these cases present evidencethat multiple and small areas of brain infarction occasion-ally present with clinical features atypical for brain embo-lism. They can be detected by MRI DWI sequences.
What were the causes of brain infarction in thesepatients? Analysis of data available from the case studiesdoes not provide a definitive answer. Lacunar disease,vasculitis, and other processes may have been the causesof some of these strokes. However, the multiplicity of

144 Journal of Neuroimaging Vol 13 No 2 April 2003
Fig 5. Left temporal, insular, and periventricular areas of restricted diffusion in patient 5.
Fig 4. Patient 4. (A) Brain computerized tomography shows small and hypodense lesions in the periventricular area and cor-pus callosum. (B) The corresponding magnetic resonance imaging shows areas of restricted diffusion involving theperiventricular white matter, corpus callosum, and corona radiata.
A
B

MRI DWI lesions in all 5 cases and their distribution in >1 arterial territory in cases 1, 3, and 4; evidence of sys-temic embolism in case 3; and the finding of potentialsources for emboli in all patients, provide indirect evi-dence that these lesions were secondary to brain embo-lism. Similar areas of restricted diffusion in DWI can alsobe seen in other conditions associated with brain embo-lism. Patients who receive aneurysm embolization treat-ment with Gugliemi detachable coils,1 those undergoingangioplasty and stenting,2 and those with fat embolismsyndrome3,4 all have similar MRI findings, lending fur-ther support to the notion of embolism in our cases. Giventhe relatively small sizes of these infarcts, we have electedto use the term brain microembolism to refer to this condi-tion. The impact of decreased clearance of emboli in thiscontext remains unknown.5
The term cerebral microembolic state was originallycoined by Kamenar and Burger6 to describe the conditionof the brain in fat embolism. In that condition, ischemicinfarcts and perivascular hemorrhages < 2 mm in diame-ter are scattered throughout the brain. They are second-ary to massive embolism of fat particles.6 Brainmicroembolism is also a feature of cholesterol embolism,a condition in which multiple brain microemboli to arteri-oles < 300 µm in diameter are common.7 Encephalopathyand visual symptoms can frequently be seen in that disor-der.7,8 The composition of embolic particles remainsunknown in this series, but there was no clinical evidenceof fat embolism. Rather, atherosclerotic disease withplatelet-fibrin or cholesterol embolism was suspected.
Although most patients described in the precedingparagraphs presented with symptoms suggestive of brainischemia, some had mild or atypical symptoms, such aspoor control or confusion, not consistently fitting the clas-sical symptoms of the major stroke syndromes. Withoutappropriate imaging studies, such patients might not be asreadily diagnosed by unsuspecting clinicians, and the pat-tern of brain infarction might not be recognized. Unfortu-nately, the data presented in this article do not permit acomplete characterization of the clinical features of brainmicroembolism, because the selected patients do not rep-resent consecutive cases from a prospective database.They do offer insight into a subtype of ischemic stroke.The diversity and variability of symptoms are the mainfeatures observed in this series. Small MRI DWI lesionsare associated with relatively mild neurological deficits,such as isolated hand weakness.9,10 Thus, further study willbe necessary to ascertain whether this disorder has char-acteristic and recognizable clinical features and whetherthey differ from embolism in other conditions such as
atrial fibrillation.11 The treatment of this condition isbeyond the present study’s scope.
Brain CT scans were obtained for 4 of the selectedpatients, and they were nondiagnostic. MRI T2sequences did not detect all infarcts. FLAIR sequenceswere more helpful, but they did not allow discriminationbetween new and chronic infarcts that were often seen inthese patients. This is one of the principal benefits ofDWI, which is sensitive for the detection of hyperacute(<6 hours), acute (<24 hours), and subacute (generallywithin 2 weeks) infarcts. DWI findings gradually fadeafter several weeks, whereas most FLAIR findings persist.Although brain ischemia was clinically suspected in allcases, it was not until the DWI and ADC studies wereobtained that definitive diagnoses of infarction weremade. In addition, the DWI studies clarified the subtypeof stroke because this pattern of microembolism andbrain infarction was never anticipated clinically. Thus,until more is known about the clinical features of brainmicroembolism, an MRI study with a DWI sequence isindicated in patients with atypical clinical presentationsand a high clinical suspicion for brain ischemia. It shouldbe noted that similar microembolic infarcts have previ-ously been reported as satellites of large areas of infarc-tion,12 and they have been considered markers of embolicdisease.
References
1. Rordorf G, Bellon RJ, Budzik RF, et al . Silentthromboembolic events associated with the treatment ofunruptured cerebral aneurysms by use of Gugliemi detach-able coils: prospective study applying diffusion-weightedimaging. Am J Neuroradiol 2001;22:5-10.
2. Jaeger HJ, Mathias KD, Drescher R, et al. Diffusion-weighted MR imaging after angioplasty or angioplasty plusstenting of arteries supplying the brain. Am J Neuroradiol2001;22:1251-1259.
3. Parizel PM, Demey HE, Veeckmans G, et al. Early diagnosisof cerebral fat-embolism syndrome by diffusion-weightedMRI (starfield pattern). Stroke 2001;32:2942-2944.
4. Forteza AM, Koch S, Romano JG, et al. Transcranial Dopp-ler detection of fat microemboli. Stroke 1999;30:2687-2691.
5. Caplan LR, Hennerici M. Impaired clearance of emboli(washout) is an important link between hypoperfusion,embolism, and ischemic stroke. Arch Neurol 1998;55:1475-1482.
6. Kamenar E, Burger PC. Cerebral fat embolism: aneuropathological study of a microembolic state. Stroke1980;11:477-484.
7. Ezzedine MA, Primavera JM, Rosand J, Hedley-White ET,Rordorf G. Clinical characteristics of pathologically provedcholesterol emboli to the brain. Neurology 2000;54:1681-1683.
Aly et al: Brain Microembolism 145

8. Gittenger JW, Kershaw GR. Retinal cholesterol emboli inthe diagnosis of renal atheroembolism. Arch Intern Med1998;158:1265-1267.
9. Kim JS. Predominant involvement of a particular group offingers due to small, cortical infarction. Neurology2001;56:1677-1682.
10. Gass A, Szabo K, Behrens S, Rossmanith C, Hennerici M. Adiffusion-weighted MRI study of acute ischemic distal armparesis. Neurology 2001;57:1589-1594.
11. Lin HJ, Wolf PA, Kelly-Hayes M, et al. Stroke severity inatrial fibrillation. Stroke 1996;27:1760-1764.
12. Baird AE, Lovblad KO, Schlaug G, Edelman RR, Warach S.Multiple acute stroke syndrome. Marker of embolic dis-ease? Neurology 2000;54:674-678.
146 Journal of Neuroimaging Vol 13 No 2 April 2003