-
Primary malignant brain tumors in adults exist in a
dizzyingarray of forms. Find out about the types of tumors,
theirsigns and symptoms, treatment options, and effectivepatient
management.DAWN CAMP-SORRELL, FNP, AOCN, MSNOncology Nurse
Practitioner • Hematology and Oncology Associates • Sylacauga,
Ala.
The author has disclosed that she has no significant
relationships with or financial interest in any commercial
companies that pertain to this educational activity.
ONE OF THE most chilling pronouncements anyone canhear is, “You
have a brain tumor.” The fear this declarationcauses the patient is
often justified, especially when thetumor’s malignant, invasive,
fast-growing, and life-threat-ening. Existing treatments can be
ineffective.
Tumors that originate in the brain vary widely by tissuetype,
site of occurrence, growth potential, tendency toprogress, tendency
to recur, and treatment response.According to the Pediatric Brain
Tumor Foundation of theUnited States, brain tumors are the
deadliest of childhoodcancers. And just because a brain tumor is
benign doesn’tmean it’s harmless; a benign tumor in the wrong place
canbe deadly. Regardless of their characteristics and point
oforigin, however, malignant brain tumors have the highest
morbidity and mortalityrates.
Tumors originatingfrom structures withinthe brain are called
pri-mary brain tumors.Those that spread fromother areas in the
bodyto the brain are calledsecondary, or metastatic,brain tumors.
In this
20 Nursing made Incredibly Easy! May/June 2006
Brain tumorsFacing trouble head-on
By the numbersPrimary brain tumors represent 1.4% of allcancers
diagnosed in the United States.About 18,500 primary malignant brain
tumorsare diagnosed each year. If you include all pri-mary brain
tumors, the number rises toaround 41,000 new cases each year.
Almost13,000 deaths annually are caused by braintumors.
22..55ANCC/AACN
CONTACT HOURS
No easy wayaround thisdiagnosis,that’s for
sure!
-
May/June 2006 Nursing made Incredibly Easy! 21
s
-
article, I’ll focus principally on primarymalignant tumors in
adults. I’ll discusscauses, pathophysiology, clinical
presenta-tion, diagnosis, and treatment options, aswell as go over
some important new treat-ment options.
First, let’s review the brain’s anatomy.
Central processingunitThe brain consists of soft,spongy tissue
divided intothree major structures: thecerebrum, the cerebellum,
andthe brain stem. It’s coveredand protected by the skin, theskull,
and the meninges. Cere-
brospinal fluid bathes the tissueand cushions it from shocks.The
outer layer of the cerebrum, the
cerebral cortex, consists of unmyelinatednerve fibers called
gray matter. Within thecerebrum are myelinated nerve cells
calledwhite matter. Basal ganglia, which controlmotor coordination
and steadiness, are
found in the white matter.The undulating surface of the cerebrum
is
made up of gyri (convolutions) and sulci(creases). The cerebrum
has a right and lefthemisphere. The corpus callosum, a mass ofnerve
fibers, bridges the hemispheres, allow-ing communication between
correspondingcenters on each side. Some of the large sulcidivide
the surface into lobes: the frontal, theleft and right parietal,
the left and right tem-poral, and the occipital. The lobes are
namedafter the cranial bones that cover them.
The cerebellum is underneath the backpart of the cerebrum. It
also has two hemi-spheres, each having an outer cortex ofgray
matter and an inner core of white mat-ter. This part of the brain
maintains muscletone, coordinates muscle movement, andcontrols
balance.
The brain stem lies just below the cere-brum, in front of the
cerebellum. It runs fromthe cerebrum and connects to the
spinalcord, and it consists of the midbrain, thepons, and the
medulla oblongata. Its func-tion is threefold: (1) to mediate
autonomiccardiac, respiratory, and vasomotor function;(2) to
provide two-way communication linesfor nerve signals; and (3) to
serve as the ori-gin for 10 of the 12 pairs of cranial nerves.
22 Nursing made Incredibly Easy! May/June 2006
Where the trouble startsPrimary brain tumors are classified
accordingto histology (tissue of origin), as follows:• Tumors
originating in neuroepithelial tissue
—astrocytomas—glioblastomas—oligodendrogliomas—mixed
gliomas—ependymal tumors• Tumors originating in cranial and
spinalnerves
—central nervous system lymphoma• Tumors of sellar region
—pituitary adenomas—pituitary
carcinomas—craniopharyngiomas—chordomas, chondrosarcomas.
Let’s take acloser look at what’s
inside you.
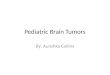
Gyri
Central sulcus
Lateral sulcus
Parietal lobe
Occipitallobe
CerebellumSpinal cord
Medullaoblongata
Pons
Temporal lobe
Frontal lobe
Frontal lobe
Anatomy of the brain
-
The diencephalon is the part of the brainlocated between the
cerebrum and the mid-brain. It consists of the thalamus, the
hypo-thalamus, the subthalamus, and the epithala-mus, which lie
deep in the cerebral hemi-spheres. All sensory information
(exceptfor olfactory information) has to check in atthe thalamus
before it can be transmittedappropriately to the brain. The
hypothala-mus helps to power autonomic functions,like regulating
body temperature, hunger,hormone output, and the sleep/wake
cycle.
Those are the parts. Now let’s briefly lookmore closely at the
types of cells that makeup the various brain structures.
The nervous system contains two types ofcells: neurons and glial
cells. The neurons arethe basic anatomic and functional units ofthe
nerves. The glial cells provide nourish-ment, structural support,
and protection for
the neurons. Within the brain and spinalcord, glial cells
surround nerve cells andhold them in place. They’re subdivided
intofour main types: astrocytes, oligodendro-cytes, ependymal
cells, and microglia.Astrocytes and oligodendrocytes are
specifictypes of neuroglial cells (nonneural support-ing elements).
Oligodendrocytes formmyelin in the central nervous system
(CNS).
Now that we’ve got the architecture inplace, it’s time for a
look at what can gowrong when a tumor arises in one or moreof these
structures.
Invasion forceExperts haven’t yet found any positivecauses or
risk factors for primary braintumors. In a few rare hereditary
syn-dromes—NF1, NF2, Turcots, Gorlins,tuberous sclerosis, and
Li-Fraumeni—
May/June 2006 Nursing made Incredibly Easy! 23
Making the gradeBecause the tumor-node-metastases (TNM) staging
system used for many other cancers doesn’twork very well for brain
tumors, classification is based on alternate systems. Following are
two of themost widely used: the World Health Organization (WHO)
classification of nervous system tumors andthe National Cancer
Institute’s (NCI) grading system for adult brain tumors.
WHO grade Characteristics
I Discrete lesions with low proliferative potential. May be
curable with surgical resection.
II Infiltrating lesions that are low in mitotic activity but
recur. Some tumor types tend to progress to or recur at higher
grades of malignancy.
III Lesions with histologic evidence of malignancy in the form
of mitotic activity, clearly expressed infiltrative capabilities,
and anaplasia.
IV Lesions that are mitotically active, necrosis-prone, and
associated with a rapid preoperative and postoperative evolution of
disease.
NCI grade Characteristics
I The tumor grows slowly, has cells that look similar to normal
cells, and rarely spreads into nearby tissues. It may be possible
to remove the entire tumor by surgery.
II The tumor grows slowly, but may spread into nearby tissue and
may become a higher-grade tumor.
III The tumor grows quickly, is likely to spread into nearby
tissue, and the tumor cells look very different from normal
cells.
IV The tumor grows very aggressively, has cells that look very
different from normal cells, and is difficult to treat
successfully.
-
there’s a genetic link to brain tumor devel-opment. Links to
environmental exposuresare under scrutiny; only one, exposure
toionizing radiation, is known to increasethe risk of a primary
brain tumor.
Primary brain tumors are classifiedaccording to the tissue of
origin or histol-ogy—how it looks under a microscope (seeWhere the
trouble starts). Two grading sys-tems are commonly used (see Making
thegrade). The higher the grade, the moreaggressive the tumor will
be. Tumors oftencontain several grades of cells: the highestgrade
determines the grade by which thetumor is classified. Further
classification isbased on genetic tumor markers and molec-ular
biologic abnormalities.
The signs and symptoms of a brain tumordepend on its size, type,
and location.
Tumors can arise from the brain tis-sue itself or from the
meninges,
pituitary gland, or cranial bloodvessels (see A glossary of
com-
mon tumor types). Symptoms,often characterized by insidious
onset, are typically caused by an
increase in intracranial pressure (ICP) andblockage of
cerebrospinal fluid. Some of themost common signs and symptoms
include:n frequent headachesn decreased motor strength and
coordina-tionn seizuresn altered vital signsn vomiting with or
without nausean papilledeman anorexian changes in mood/personalityn
changes in the ability to think andlearn.
Most patients present with a headachethat won’t go away with
pain medication.Headaches occurring on awakening can bean early
symptom of brain tumor. They maybe associated with projectile
vomiting, whichsuggests an increase in ICP. The headachesmay be
dull or sharp and, as the ICP rises,tend to be frontal or
occipital.
Some patients have changes in mentalstatus, mood, or
personality. They may alsosuffer memory loss, lose the ability to
con-centrate, or exhibit focal neurologic signs.
24 Nursing made Incredibly Easy! May/June 2006
A glossary of common tumor types
Tumor type Description
Gliomas (account for Tumors of the neuroepithelial/glial
cells40% to 50% of intracranial neoplasms)
• Astrocytomas • Overgrowth of astrocyte cells (the brain’s
connective tissue)
• Oligodendrogliomas • Overgrowth of oligodendrocyte cells with
calcification
• Ependymomas • Overgrowth of the ependymal cells
• Mixed gliomas • Two or more cell types within a tumor
• Medulloblastomas • Most common pediatric malignant tumor.
Rapid growth pattern, highly invasive with a high risk of
metastases
Meningiomas Arise from the linings (meninges) of the brain and
can involve the skull
Peripheral nerve tumors Include acoustic neuroma, schwannoma,
and Von Recklinghausen’s(type 1) neurofibromatosis and type 2
neurofibromatosis
Pituitary adenomas Can be secreting or nonsecreting
Germ cell tumors Dermoid cysts, epidermoid cysts, pineal tumors,
and chordomas
Hematopoietic tumors Primary malignant lymphomas
I haven’tbeen
myselflately!
-
Delirium and dementia are often indicatorsof a brain tumor.
These symptoms are poor-ly understood, and they can cause
distressfor the patient and his family.
Brain tumors can produce irritation thatcauses seizures. Common
types of seizuresthat arise from brain tumors include simplefocal,
complex partial, and generalizedtonic-clonic. Simple focal seizures
are local-ized; that is, they’re produced in a specificpart of the
brain. These seizures involvesimple sensory or motor functions.
Com-plex seizures occur when the brain irritationspreads into the
frontal and temporal lobes.In a generalized seizure, the irritation
isspread over both sides of the brain; thepatient may lose
consciousness and hisarms and legs will move uncontrollably.Loss of
bladder and/or bowel control mayoccur (see Brainstorm: Managing a
seizure).
These signs and symptoms may point toa brain tumor, but they’re
not definitive.Let’s look next at ways to diagnose a
braintumor.
Picture thisDiagnosis begins with a thorough history.Ask the
patient to describe his symptoms,calculate how long he’s had them,
whenthey occur, whether he sees a connectionto an activity or
circumstance, and if theyseem to be worsening.
A neurologic exam is the next order ofbusiness. This involves
various tests ofmovement, vision, touch, hearing, smell,reflexes,
eye response, balance and coordina-tion, abstract thinking, mental
status, andmemory. Abnormal findings may be able tohelp pinpoint
the area of the brain that’saffected.
Computed tomography (CT) scan is themost widely used diagnostic
imaging test.Magnetic resonance imaging (MRI) is alsoused; it’s
more sensitive for detecting intra-parenchymal brain tumors like
ependymo-mas, the most common brain tumor in chil-dren. Hemodynamic
imaging combines CTscan or MRI with the ability to gauge the
speed of contrast dye uptake; it’s useful forshowing tumor
neovascularization.
Cytologic studies of cerebrospinal fluidcan be used to detect
the presence of malig-nant cells shed by the tumor. An
electroen-cephalogram can detect areas where abnor-mal brain waves
occur and evaluate tempo-ral lobe seizures. It can also be used to
helprule out other disorders.
Once a lesion is pinpointed, a neurosur-geon will obtain a
biopsy specimen via cra-niotomy to determine the histology or the
tis-sue type of the tumor. Stereotactic (computer-directed) biopsy
is an option when the lesionis too deep or in an area where
craniotomy istoo risky or when the patient can’t tolerategeneral
anesthesia.
Next up: treatments.
Reducing planWhenever feasible, treatment for a braintumor
begins with surgery. The primarygoal is to excise as much of the
tumor aspossible to reduce the severity of signsand symptoms while
optimally preservingneurologic function (see Craniotomy: A holein
the head for postsurgical management).Let’s look at the other
options that goalong with surgery.
May/June 2006 Nursing made Incredibly Easy! 25
Craniotomy: A hole in the headAfter a craniotomy, the patient is
closely monitored in the intensive careunit. Be particularly aware
of potential complications, like intracranialbleeding, cerebral
edema, and water intoxication. A thorough neurologicassessment can
detect the patient’s level of consciousness, intracranialpressure
(ICP), and motor dysfunction. Decreased strength or level of
con-sciousness and pupil changes may indicate increased ICP and
cerebraledema.
• Monitor vital signs. Increasing temperature may indicate
infection;increased heart rate or blood pressure may indicate
increased ICP.
• Discourage activities that may increase ICP, such as
straining.
• Monitor for seizure activity.
• Assess for signs of intracranial bleeding, such as swelling
over the inci-sion, changes in mental status, nausea, or
vomiting.
• Provide support to the patient and family during the immediate
postop-erative period.
-
n Radiation. Radiation therapy is usefulfor improving cure rates
and prolongingsurvival for most types of primary braintumors. The
type of radiation technique
used and the amount given de-pends on tumor histology, grade,and
location and the patient’sphysical status. Ionizing radia-tion
targeting the tumor is deliv-
ered so as to minimize injuryto the surroundinghealthy tissue.
The most
common technique usedis external beam radia-tion therapy. As
the
name implies, the radia-tion comes from a machine
outside of the body. Treat-ment is generally given 5
days a week for 4 to 6 weeks for a totaldose ranging from 40 to
70 Gy. Adverseeffects may include hair loss, fatigue, nau-sea,
vomiting, scalp dermatitis, andheadache. Somnolence syndrome,
charac-terized by mild drowsiness and fatigue tomarked lethargy, is
common after brain ir-radiation. It usually subsides 2 to 3
weeksafter the start of therapy.
Stereotactic radiosurgery allows deliveryof high-dose radiation
in a single dose to a
precise area in the brain. The goal of thistechnique is to
eradicate the tumor cellswithin a targeted area and minimize
dam-age to the surrounding tissues. Adverseeffects may include
headache. Also, theframe used to immobilize the patient’shead
during this procedure may be uncom-fortable.n Chemotherapy.
Chemotherapy has beenshown to boost survival in patients
withgliomas, medulloblastomas, and certainother tumors. How well it
works dependson the ability of the chemotherapeuticagent to cross
the blood-brain barrier, aprotective mechanism the body uses tostop
potentially damaging substances frominfiltrating the CNS. A few
brain tumorsactually serve to break down the barrier.Chemotherapy
is generally used as adju-vant therapy to surgery and radiation.
Itcan also be used for recurrent brain tumors. n Drug therapies.
The combination of a corticosteroid like dexamethasone(Decadron),
an osmotic diuretic like man-nitol, and a loop diuretic like
furosemide(Lasix) is used to reduce edema aroundthe tumor.
Otherwise, the swelling couldcause brain structures to shift and
increaseICP. The osmotic diuretic pulls fluid outof the space
surrounding the tumor and
26 Nursing made Incredibly Easy! May/June 2006
Match the treatment to the tumor type
Tumor type Radiation/surgery Chemotherapy
Lymphomas Whole-brain X-ray therapy Intrathecal ethotrexate,
procarbazine, vincristine, high-dose cytarabine
Medulloblastomas Surgery, craniospinal radiation Lomustine,
cyclophosphamide, vincristine, cisplatin, etoposide
Gliomas Surgery, radiation Temozolomide, carmustine,
procarbazine, carboplatin, irinotecan, etoposide
Astrocytomas Surgery, radiation Temozolomide, carmustine,
procarbazine, carboplatin, irinotecan, etoposide
Oligodendrogliomas Surgery, radiation Procarbazine, lomustine,
vincristine
Meningiomas Surgery, external beam or Hydroxyurea, alpha
interferon stereotactic radiation
With braintumors,
smaller isbetter.
-
into the intravascular space, where theloop diuretic can push
the kidney to ex-crete it. A steroid can also help to
relieveheadaches by lowering the ICP. Patientstaking a steroid will
need ulcer prophy-laxis with a histamine2-receptor blockerlike
famotidine (Pepcid) or a proton pumpinhibitor like lansoprazole
(Prevacid).Seizure medication may also be used. As-pirin and
anticoagulation medications arestopped to avoid intracranial
bleeds.
Medications can be used in the nonspecifictreatment of
concentration and memory dis-turbances to manage coexisting
depression,anxiety, or agitation.
See Match the treatment to the tumor typeand Plan B for more
information.
Handling the tough jobsA major part of your job is to help the
pa-tient manage his symptoms in a way thatwill best preserve his
quality of life. Fol-lowing are some guidelines for
symptommanagement.n Monitor headache onset, intensity, andsymptoms.
Advise the patient about med-ications, like steroids and
analgesics, thatwill relieve the pain.
n Monitor seizure activity and the type ofseizure. Instruct the
patient about appro-priate antiseizure medications,
includingadministration and adverse effects. Seealso Brainstorm:
Managing a seizure.n The patient with a brain tumor may ex-perience
significant fatigue from the tumor
May/June 2006 Nursing made Incredibly Easy! 27
Plan BStandard treatment sometimes falls short of improving the
5-year survival rate for certain tumor types. According to the
NationalCancer Institute, new biologic therapies being looked at
include dendritic cell vaccination, tyrosine kinase receptor
inhibitors, far-nesyl transferase inhibitors, viral-based gene
therapy, and oncolytic viruses. Patients with tumors that are
unresectable or infre-quently curable may benefit from
radiosensitizers, hyperthermia, or interstitial brachytherapy used
along with external beam radi-ation therapy to boost its benefit.
Following are some of the other new treatment options in clinical
trials.
Tumor type Standard treatment Treatment options under study
Pilocytic astrocytomas Surgery or surgery and radiation
Nitrosourea-based chemotherapy, temozolomide
Anaplastic astrocytomas Surgery plus radiation or surgery plus
Hyperfractionated irradiation, accelerated-fractionradiation and
chemotherapy irradiation, stereotactic radiosurgery
Glioblastoma Surgery plus radiation or surgery plus
Hyperfractionated irradiation, accelerated-fractionradiation and
chemotherapy, carmustine irradiation, stereotactic
radiosurgery(BCNU)-impregnated polymer (Gliadel wafer), radiation
plus temozolomide
Oligodendroglial Surgery or surgery plus radiation Temozolomide,
procarbazine-lomustine-vincristine (PCV) therapy
Brainstorm: Managing a seizure
• Have the patient lie down immediately if hefeels a seizure
coming on. Some patients willhave a warning symptom, like a visual
aura or asmell.
• Loosen clothing around the neck andabdomen.
• Clear away all objects close to the patientthat could injure
him.
• Stay with the patient to provide support andto document
manifestations of the seizure.
• Ensure airway patency. Never force apatient’s mouth open
during a seizure.
• Once the seizure has subsided, providereassurance and reorient
the patient to time,place, and person.
-
itself or from the treatments.Advise him to get adequate
rest, food, and fluids. Con-sult with a dietitian if nausea
and vomiting or anorexia make it im-possible for the patient to
take inproper nutrition. n The patient may experience cogni-
tive impairment and/or memory loss. Theprovider may order
medications that willreduce these distressing symptoms.
Providing plenty of good, understand-able information so that
the patient canmake informed decisions about his care isone of the
best ways you can help him copewith a diagnosis of brain tumor and
itsaftermath. “Is there anything you’d like toask?” can be a key
phrase in avoiding mis-apprehension. Often, you can use his
ques-tions as an indication of how much infor-mation he really
wants to know.
Be on the lookout for symptoms of majordepression in a long-term
patient. Once the
hectic back-and-forth of tests and chemotreatments disappears,
the full implicationsof having a brain tumor may finally sink inand
be overwhelming. Refer the patientand his family to hospital social
services,which will provide them with informationon the many brain
tumor support groupsavailable. n
Learn more about itArmstrong TS, et al. Seize the moment to
learn aboutepilepsy in people with cancer. Clinical Journal of
OncologyNursing. 7(2):163-169, March-April 2003.
National Cancer Institute. Adult brain tumors (PDQ):Treatment:
Health Professional Version.
http://www.nci.nih.gov/cancertopics/pdq/treatment/adultbrain/healthprofessional/allpages.
Accessed February 17, 2006.
Ree A, et al. Direct infiltration of brainstem glioma alongthe
cranial nerves. Journal of Neuroimaging. 15(2):197-199,April
2005.
Smeltzer SC, Bare BG. Brunner & Suddarth’s Textbook
ofMedical-Surgical Nursing, 10th edition. Philadelphia,
Pa.,Lippincott Williams & Wilkins, 2004.
Whittle IR, et al. Gliadel therapy given for first resectionof
malignant glioma: A single centre study of the poten-tial use of
Gliadel. British Journal of Neurosurgery.17(4):352-354, August
2003.
28 Nursing made Incredibly Easy! May/June 2006
INSTRUCTIONS
Brain tumors: Facing trouble head-onTEST INSTRUCTIONS• To take
the test online, go to our secure Web site at
www.nursingcenter.com/ce/nmie.• On the print form, record your
answers in the test answer sectionof the CE enrollment form on page
54. Each question has only onecorrect answer. You may make copies
of these forms.• Complete the registration information and course
evaluation. Mailthe completed form and registration fee of $19.95
to: LippincottWilliams & Wilkins, CE Group, 2710 Yorktowne
Blvd., Brick, NJ08723. We will mail your certificate in 4 to 6
weeks. For faster service,include a fax number and we will fax your
certificate within 2 businessdays of receiving your enrollment
form. Deadline is June 30, 2008.• You will receive your CE
certificate of earned contact hours and ananswer key to review your
results. There is no minimum passinggrade.
DISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any
nursing journal published byLippincott Williams & Wilkins
together and deduct $0.95 from the
price of each test.• We also offer CE accounts for hospitals and
other health care facili-ties on nursingcenter.com. Call
1-800-787-8985 for details.
PROVIDER ACCREDITATION:Lippincott Williams & Wilkins, the
publisher of Nursing madeIncredibly Easy!, will award 2.5 contact
hours for this continuingnursing education activity. Lippincott
Williams & Wilkins is accred-ited as a provider of continuing
nursing education by theAmerican Nurses Credentialing Center’s
Commission onAccreditation. This activity is also provider approved
by theCalifornia Board of Registered Nursing, Provider Number
CEP11749 for 2.5 contact hours. Lippincott Williams & Wilkins
is alsoan approved provider by the American Association of
Critical-CareNurses (AACN 00012278, CERP Category A),
Alabama#ABNP0114, Florida #FBN2454, and Iowa #75.
LippincottWilliams & Wilkins home study activities are
classified for Texasnursing continuing education requirements as
Type 1. Your certifi-cate is valid in all states.
Earn CE credit online: Go to
http://www.nursingcenter.com/CE/nmie and receive a certificate
within minutes.
Eating 3 squaremeals a day
could be toughfor your patient.