Embed Size (px)
Citation preview

Do you know what’s in people’s Do you know what’s in people’s head?head?

Brain tumorsBrain tumors
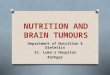
72 male72 male HPI: presents to E.R. with history of HPI: presents to E.R. with history of
confusion, change of personality, left confusion, change of personality, left sided H/Asided H/A
P/E: disorientation and P/E: disorientation and aggressiveness, no focal signsaggressiveness, no focal signs
Labs: WNLLabs: WNL Imaging:Imaging:

Brain tumorsBrain tumors

Brain tumorsBrain tumors
anatomyanatomy

Brain tumorsBrain tumors

Brain tumorsBrain tumors

Brain tumorsBrain tumors

Brain tumorsBrain tumors
DDx:DDx: BenignBenign
CongenitalCongenital AVM/aneurismAVM/aneurism
Acquired Acquired Infectious (toxoplasmosis, cyst)Infectious (toxoplasmosis, cyst) strokestroke
MalignantMalignant PrimaryPrimary metastaticmetastatic

Brain tumorsBrain tumors
Glioblastoma Glioblastoma multiformemultiforme
AstrocytomaAstrocytoma OligodendrogliomaOligodendroglioma MeningiomaMeningioma Brain stem tumorsBrain stem tumors MedulloblastomaMedulloblastoma Ependymoma Ependymoma
SarcomaSarcoma LymphomaLymphoma CraniopharyngiomaCraniopharyngioma NeurofibromaNeurofibroma Germ cell tumorsGerm cell tumors SchwannomaSchwannoma Pituitary tumorsPituitary tumors meningiomameningioma

Brain tumorsBrain tumors
MetastasesMetastases SingleSingle Multiple Multiple

Brain tumorsBrain tumors

Brain tumorBrain tumor

Brain tumorsBrain tumors

Brain tumorsBrain tumors
Management:Management: Medical support (steroids + PPI)Medical support (steroids + PPI) Staging Staging Surgical resection if indicatedSurgical resection if indicated Adjuvant therapiesAdjuvant therapies

Brain tumorsBrain tumors

Brain tumorsBrain tumors

GBMGBM
Radiation therapyRadiation therapy Standard dose: 60 Gy / 30 fractionsStandard dose: 60 Gy / 30 fractions O.S. = 42 weeks (1979 study)O.S. = 42 weeks (1979 study)
Radiation therapy + chemotherapyRadiation therapy + chemotherapy Meta analysis shows improvement in Meta analysis shows improvement in
generalgeneral

GBMGBM
Best results to Best results to date:date: Combination with Combination with
temozolomidetemozolomide 75 mg/m2 po od x 6 75 mg/m2 po od x 6
weeks (concurrent weeks (concurrent with xrt), then 150 with xrt), then 150 mg/m2 po od on d1-mg/m2 po od on d1-5 every 28 days x 6 5 every 28 days x 6 cyclescycles
RTRT RT/TMZRT/TMZ
Median Median OS OS (months(months))
12.112.1 14.614.6
2 yr 2 yr survivalsurvival
10%10% 26%26%

GBMGBM
If poor performance statusIf poor performance status Hypofractionated xrt:Hypofractionated xrt:
40/1540/15 35/1035/10

Brain tumorsBrain tumors
57 male 57 male HPI: known lung cancer; developped HPI: known lung cancer; developped
gait instabilitygait instability P/E: cerebellar exam abnormalP/E: cerebellar exam abnormal ImagingImaging

Brain tumorsBrain tumors
Cerebellar metastasis on CT scanCerebellar metastasis on CT scan
Management: Management: Supportive careSupportive care Decadron (10 mg stat, then 4 mg po Decadron (10 mg stat, then 4 mg po
QID) + PPIQID) + PPI

Brain metsBrain mets
Depends on stability of peripheral Depends on stability of peripheral disease and extend of intra cerebral disease and extend of intra cerebral disease:disease:
Peripheral disease stable: Peripheral disease stable: confirm solitary status with MRIconfirm solitary status with MRI If solitary: If solitary:
consider surgical resection or stereotactic consider surgical resection or stereotactic radiosurgeryradiosurgery
Whole Brain Radiation Therapy (WBRT)Whole Brain Radiation Therapy (WBRT)

Brain metsBrain mets
SurgerySurgery DiagnosticDiagnostic Quicker steroid Quicker steroid
tapertaper Quicker symptom Quicker symptom
reliefrelief
Limited by Limited by localisationlocalisation
SRSSRS Non invasiveNon invasive Less riskLess risk Less expensiveLess expensive
Limited by sizeLimited by size RadioresistanceRadioresistance
MelanomaMelanoma Sarcoma Sarcoma

Brain metsBrain mets
peripheral disease stableperipheral disease stable More than 1 lesionMore than 1 lesion
Surgery less of a considerationSurgery less of a consideration WBRT +/- stereotactic radiosurgery boostWBRT +/- stereotactic radiosurgery boost
Criteria:Criteria: < or = 3 lesions< or = 3 lesions Volume: < 4 cmVolume: < 4 cm Prognostic > 3 monthsPrognostic > 3 months KPS >70KPS >70

Brain metsBrain metsSurvivalSurvival WBRT + WBRT +
SRSSRSWBRTWBRT p valuep value
OverallOverall 6.56.5 5.75.7 0.130.13
1 met1 met 6.56.5 4.94.9 0.040.04
1-3, 1-3, age<50age<50
9.99.9 8.38.3 0.040.04
1-3, NSCLC1-3, NSCLC 5.95.9 3.93.9 0.050.05
1-3, RPA1-3, RPA 11.611.6 9.69.6 0.050.05

Brain metsBrain mets
peripheral disease not stableperipheral disease not stable Palliative radiation therapyPalliative radiation therapy Re-irradiation on a case by case basisRe-irradiation on a case by case basis

Brain metsBrain mets

Brain metsBrain mets
Prognostic:Prognostic: Untreated: 1 monthUntreated: 1 month Steroids: 2 monthsSteroids: 2 months

Brain metsBrain mets
Radiation therapyRadiation therapyKPSKPS >70>70 >70>70 <70<70
AgeAge <65<65 >65>65
Primary Primary controlcontrol
YesYes nono
MetsMets Brain Brain onlyonly
Multi Multi organorgan
SurvivalSurvival 7.17.1 4.24.2 2.32.3

Brain metsBrain mets
Side effectsSide effects AlopeciaAlopecia Skin erythemaSkin erythema Fatigue Fatigue Neurocognitive changesNeurocognitive changes

Brain metsBrain metsSingle metSingle metSymptomatic,ResectableSymptomatic,Resectable
First/only metFirst/only met
Surgery + WBRTSurgery + WBRT
Single metSingle metLittle / no symptomLittle / no symptom
Non resectable / surgery Non resectable / surgery refusedrefused
SRS + WBRTSRS + WBRT
2-3 mets, KPS>702-3 mets, KPS>70RPA 1, NSCLC, <50 yoRPA 1, NSCLC, <50 yo
SRS + WBRTSRS + WBRT
2-3 mets, KPS>702-3 mets, KPS>70None of favorable Px factorsNone of favorable Px factors
WBRT +/- SRSWBRT +/- SRS
4 mets, KPS>704 mets, KPS>70RPA 1, NSCLC, <50 yoRPA 1, NSCLC, <50 yo
WBRT +/- SRSWBRT +/- SRS

Brain metsBrain mets
Role of WBRTRole of WBRTDecrease rate of new mets Decrease rate of new mets (50% to 25%)(50% to 25%)
Does not increase OSDoes not increase OS
Some histologies have less Some histologies have less distant failures (RCC, distant failures (RCC, melanoma, sarcoma)melanoma, sarcoma)
No increase in toxicity No increase in toxicity (objectively)(objectively)
Subjective increase in Subjective increase in toxicitytoxicity
Case where Dx is in doubt Case where Dx is in doubt (meningioma)(meningioma)