Embed Size (px)
Citation preview

Pediatric Dermatology Vol. 12 No. 1 24-27
Branchio-Oculo-Facial Syndrome and DermalThymus: Case Report and Review of
the LiteratureRenata Rizzo, M.D., Giuseppe Micali, M.D.,* Stefano Calvieri, M.D.,t
Giovanni Sorge, M.D., and Domenko Mazzone, M.D.
Clinica Pediatrica e ^Dermatologica. Universita di Catania, Catania, and TLstitiito di Dermalologia eVenereologia, Universita La Sapienza, Roma, Italia
Abstract: we report a patient affected by the rare branchio-oculo-facialsyndrome. Histologic study of the branchial clefts showed thymic rem-nants. A scanning electron microscopic study of the hair was also per-formed. The clinical features of the patient were compared with those ofother patients reported in the literature.
In 1982 Lee et al (1) reported a mother and sonwith similar peculiar features consisting of bilateralbranchial sinuses and an unusual facial appearance.The son also had inlrauterine and postnatal growthretardation; premature aging was observed in themother.
One year later. Hall et al (2) reported two unre-lated children with similar clinical manifestationsand incitided this syndrome in the group of bran-chial cleft syndromes. Fujimoto called it branchio-oculo-facial syndrome (3).
We report a patient affected by this rare syn-drome in whom histologic examination of the bran-chial clefts and morphological hair analysis wereperformed.
CASE REPORT
This was the only child of young, unrelated parents.He was born at term by cesarean section. Birth-weight was 2450 g (3rd percentile). height 48 cm(10th percentile), and head circumference 33 cm(3rd percentile). He had a peculiar facies with asmall cranium and forehead, a low-set anterior hair-
line, and light brown, fine, dry, curly hair. He hadupward-slanting palpebrai fissures, left ptosis, andthick, long eyelashes. His nose was short with abroad bridge, flattened tip. and hypoplastic alae.The philtrum was short and prominent with thick,fibrous, vertical ridges producing a pseudocleft(Fig. 1). The palate was cleft, narrow, and higharched. The ears were angulated posteriorly withhypoplastic helices, hypertrophic anthelices, verylarge lobes, and deep conchae. and bilateral ulcerson the upper side. A subcutaneous, nodular, elon-gated lesion measuring approximately 4 x 2 cm waspresent symmetrically on each side of the neck. Theoverlying skin was erythematous and abraded insome areas (Fig. 2). The patient is now 24 monthsold, his weight is 9500 g (lOth percentile), height 79cm (50th percentile), and head circumference 45 cm(3rd percentile). Psychomotor development is nor-mal.
Routine laboratory test results were normal, in-cluding lymphocyte subpopulations and particularlyT4 and T8 lymphocytes, T4:T8 ratio, B cells, total Tcells, and immunoglobulins. High-resolution chro-
Address correspondence to Renata Rizzo, M.D., Clinica Pe-diatrica, Policlinico, Viale A. Doria 6, Catania 95125. Italia.
24

Rizzo et al: BOF Syndrome and Dermal Thymus 25
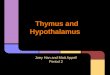
Figure 1. The patient's peculiar facies: the nose has abroad bridge and hypoplastic alae, and the thick, fi-brous, vertical ridges of the phiitrum produce apseudocieft.
mosomes, electrocardiogram, eiectroencephalo-gram. and evoked visual potential were normal.Bone age was mildly retarded. Ophthalmologic ex-amination revealed partial right aniridia. Magneticresonance imaging showed a cerebellar anomalyconsisting of partial hypoplasia of Ihe vermis anddilatation of the cisterna magna.
Histologic examination of the culaneous lesionshowed an epidermis with numerous invaginationslined by respiratory-type epithelium. In the subcu-taneous tissue there was a well-demarcated mass
Figure 3. Histologic section of cutaneous neck lesionshows an epidermis with numerous invaginationslined by respiratory-type epithelium and a well-demarcated mass consisting of heterotopic thymus inthe subcutaneous tissue.
consisting of beterotopic thymus tissue of normalstructure divided into cortical and medullary com-partments (Fig. 3). In the cortical portion the cellpopulation was more packed and composed of smalland medium-size iymphoid cells. Immunobistologicstudies revealed the presence of T lymphocytes(UCHL! + ). Celiularity was rarer in tbe medullarycompartmenl and consisted of a population ofsmall-size lymphoid cells, mainly B lymphocytes(CD20 +) with aggregations of epithelial cells andHassal's corpuscles. Hair analysis showed a diffusehypopigmentation with reduced diameter (Fig. 4).Tbe mother's hair had canallike grooving along thelongitudinal axis of the shaft and fracturing withoutother pigmentary anomalies (Fig. 5).
DISCUSSION
This patient had the peculiar findings of thebranchio-oculo-facial (BOF) syndrome. Clinical
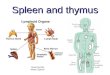
Figure 2. Malformed ears, and an elongated lesion onthe lateral neck with erythematous and, in some areas,abraded skin.
Figure 4. Scanning electron micrograph of the pa-tient's hair shows a diffuse hypopigmentation and re-duced diameter. (Magnification 625x.)

26 Pediatrie Dermatology Vol. 12 No. 1 March 1995
Figure 5. Scanning electron micrograph of tlie hair ofthe patient's mother shows canaliike grooving andfracturing. (Magnification 1250x.)
signs of 19 cases from the literature as well as thoseof our patient are shown in Table 1 (2.3,5,6,8-10).Although their clinical features were not fully de-scribed, the patients of Farmer and Maxman (4) and
TABLE 1. Manifesiations of theBranchio-Ociilo-Facial Syndrome
Growth deficiencyPrenatalPostnatal
Craniofacial anomaliesSubcutaneous cysts of scalpPremature graying of hairLacrimal duct obstructionColobomaAnophthalmiaMicrophthalmiaCataractMyopiaStrabismusOrbital cystsMalformed earsAuricular pitsConductive hearing deficitMalformed noseUpper lip abnormalityLip pitsDental abnormalityHigh arched palateBranchial clefts or variants
Atrophic skin lesionHemangiomatous lesionBranchial sinusUlcers or erosion
OthersHand anomaliesMental retardation
No. ofPatients/TotalNumber inLiteratureReports
6/1.^3/14
3/il5/10
15/186/142/195/9
3/123/9
3/i62/19
12/175/156/9
14/1718/!93/165/124/50
18/192/197/196/6
6/15
6/133/15
OurPatient
+-f.
-—
+
-—————+—+++—+—+—+++
—
Tom et al (7) are included, as they most likely rep-resent BOF syndrome.
Patients with BOF syndrome share some fea-tures with the bratichio-oto-renal (BOR) syndrome{Table 2) (11). Distinguishing features are the upperlip abnormalities, abnormal nose, retroauricularskin abnormalities, microphthalmia, and prematuregraying in the BOF syndrome, and facial asymme-try, and renal and ureteral abnormalities in the BORsyndrome. Until now the two have been consideredseparate entities. Recently, however, Legius et al(12) reported a family in which the father and sonhad manifestations of both syndromes. This sug-gests that the clinical characteristics ofthe two syn-dromes would result from the effect of mutations ofa single autosomal dominant gene.
This hypothesis is supported by Hing et al (14)who recently reported a patient with branchial cleftsinuses, microphthalmia, nasomaxillary dysplasia.and cardiovascular and central nervous system ab-normalities. They suggest that the nasoschisis, na-somaxillary dysplasia, and long philtrum may re-flect an extreme variation of the facial featuresnoted in BOF syndrome. Hence the syndrome isthought to be a pleiotropic anomaly in which muta-tions of a single autosomal dominant gene may leadto perturbations in the development of the anteriorpole of the embryo to a markedly variable degree(14).
ln our patient, histologic examination ofthe necklesion revealed thymic remnants. To our knowl-edge, only two cases of dermal thymus have beenreported in the literature (6,13) and only one ofthese individuals had BOF syndrome.
The presence of lymphocytes and epithelial cellsconfined to HassaFs corpuscle-like areas has anembryologic explanation. The thymus arises towardthe end of the sixth week of fetal life from each ofthe third pharyngeal pouches. The epithelium oftheelongate ventral portions of the two pouches prolif-
TABLE 2. Discriminating Features of BOR andBOF Syndromes
Clinica! Features BOR BOF
Upper lip abnormalitiesAbnorrnal nosePostauricular skin abnormalitiesMicrophthalmiaPremature grayingFacial asymmetryRenal and uretera! abnormalitiesBilateral branchial cleftHearing lossAbnormal ears
-I-++++

Rizzo et al: BOF Syndrome and Dermal Thymus 27
crates, obliterating their cavities. These primordiaof the thymus migrate medially and fuse to form thebilobate thymus. The primordia soon lose their con-nections with the pharynx and slowly migrate cau-dally (15), An anomaly in the development of thefirst three pairs of the branchial arches and the thirdpouch explain the anomalies seen in BOF syn-drome.
Patients with BOE syndrome are reported tohave premature graying of the hair. To our knowl-edge, our patient is the first in whom a scanningelectron microscopic study of the hair has been per-formed. It showed that the pigmentary anomaly thatwill reflect in premature graying later in life is evi-dent from early childhood; its pathogenesis is un-known, Ultrastructural study of the mother's hairshowed structural anomalies different from thoseseen in her son. Whether these anomalies are re-lated to the syndrome is not clear. Due to the smallnumber of reported cases of BOE, an ultrastructuralinvestigation of the hair of affected patients as wellas their relatives is recommended,
REFERENCES
1, Lee WK, Root AW, Fenske N, Bilateral branchialcleft sinuses associated with intrauterine and postna-tal growth retardation, premature aging, and unusualfacial appearance: a new syndrome with dominanttransmission. Am J Med Genet 1982;11:345-352.
2, Hall BD, De Lorimier A, Foster LH. A new syn-drome of hemangiomatous branchial clefts, lippseudoclefts, and unusual facial appearance. Am JMed Genet I983;14:135-138,
3, Fujimoto A, Lipson M, Laero RV. et al. New auto-
somal dominant branchio-oculo-facial syndrome. AmJ Med Genet 19B7;27:943-951,
4, Farmer AW, Maxman MD, Congenital absence ofskin, Plast Reconstr Surg 1960;25:291-297,
5, Harrison MS, The Treacher-Collins-Franceschettisyndrome, J Laryngol Otol I957;71:597-6O3,
6, Barr RJ, Santa Cruz DJ, Pearl RM, Derma! thymus.A light microscopic and immunohistochemical study.Arch Dermatol 1989;125:1681-i684,
7, Tom DWK, Alper JC, Bogaars H, Inflammatory lin-ear epidermal nevus caused by branchial cleft sinusesin a woman with numerous congenital anomalies, Pe-diatr Dermatol 1985;2:318-321,
8, Fielding DW, Fryer .\E. Recurrence of orbital cystsin the branchio-oculo-facial syndrome, J Med Genet1992;29:430-43L
9, Schweckendiek W, Hort W, Nauth HF, Doppelseit-ige retro-und subaurikulare fisteln mit Ektropium desFistelgangepithels, Laryngol Rhinol 1977;56:795-800,
10, Schmerler S, Kushnick T, Desposito F, Long-termevaluation of a child with the branchio-oculo-facialsyndrome, AmJ Med Genet 1992:44:177-178,
11, Melnick M, Bixler D, Walter E, Nance E, Silk K,Yune H, Familial branchio-oto-renal dyspiasia: anew addition to the branchial arch syndromes, ClinGenet 1976;9:25-34,
12, Legius E, Fryns JP, Van Den Berghe H, Dominantbranchial cleft syndrome with characteristics of bothbranchio-oto-renal and branchio-oculo-facia! svn-drome, Clin Genet 1990;37:347-350.
13, Civi I, Kurtay M, Civi S, Bilateral thymus found inassociation with unilateral cleft lip and palate, PlastReconstr Surg 1989;83:143-147,
14, Hing .AV, Torack R, Dowton SB, A lethal syndromeresembling brancbio-oculo-facial syndrome. ClinGenet 1992:41:74-73,
15, Moore KL, The developing human. In: Clinically ori-ented embryology, 3rd ed, Philadelphia: WB Saun-ders. 1982:179-193,