Embed Size (px)
Citation preview

Breast Cancer Genetics Module
M. Kent Froberg, M.D.
2009

Objectives
• Learn the basic genetics for sporadic and familial forms of breast cancer
• Learn the Bloom-Richardson grading system for breast cancer
• Learn the significance of ER, PR and HER2 proteomics in the Rx and prognosis of breast cancer





Sporadic Breast Cancer
• ~95% of cases
• Usually NL by cytogenetics
• Alterations include– Activation of oncogenes– Inactivation of tumor suppressor genes– Include gene mutations, deletions,
hypermethylation

Sporadic Breast Cancer
• Amplified Oncogenes:1. Human epidermal growth factor receptor-2
(ERBB2, HER2) at 17q12, tyrosine kinase activity. Overexpression in 25-30% of
breast tumors
Associated with a worse prognosis

HER 2 Targeted Therapy
• Herceptin (trastuzumab) mouse monoclonal Ab vs HER2
12-20% response rate alone, 30-50% response in combination RxBinding internalizes receptors & NK cell-mediated killing
• Tykerb (lapatinib) tyrosine kinase inhibitor of HER2
Approved by FDA (March 2007) in combination with Capectabine for HER2 + breast cancerSmall molecule enters cell and blocks signal transductionDelayed progression in women that had failed anthracycline, Taxane and trastuzumab


More Oncogenes
2. Myc at 8qOverexpressed in ~20% of breast CANuclear protein involved in regulation of growth & apoptosis
3. CCND1 (cyclin D1) Overexpression in 15-20% of breast CA (& 80% of invasive lobular carcinomas at protein level)Can bind and activate estrogen receptors

Tumor Suppressor Genes in Breast Cancer
• Inactivated tumor suppressor genes1. p53 at 17p13
nuclear protein that induces cell cycle arrest or apoptosis ~20% of invasive breast carcinomas most are missense mutations, some frameshift with loss of wild type allele May be present by IHC because of failure to degrade p53

More Tumor Suppressor genes
2. RB1CC1 at 8q11
regulator of RB1 gene
seen in ~20% of breast Ca
3. CDH1 at 16q22
cell-cell adhesion molecule E-cadherin
seen in 60% of invasive lobular CA, not ductal

Breast Biopsy
• Needle core or mammatome bx
• Routine:– Dx: Type of Ca (infiltrating ductal, lobular,
intraductal, etc.) – Tumor grade– Lymphovascular permeation– ER/PR/HER2 testing

Lumpectomy or Mastectomy
• Routine pathology:– Confirm Dx of invasive CA, intraductal
– Margins + or -
– Tumor grade
– Lymphatic/vascular invasion + or -
– Maximum dimension (or multifocality)
– Sentinel node or axillary LN metastasis + or -

Histologic Grade
• Bloom/Scarff/Richardson:Tubule formation Nuclear pleomorphism Mitosis (per hpf)
>75% 1 Mild 1 <8 1
10-75% 2 Moderate 2 8-14 2
<10% 3 Marked 3 >14 3
___ ___ ___
Total score of each 3 to 9 used to establish

Bloom/Scarff/Richardson
Grade Description 5yr survival 10yr survival
1 Well-differentiated (3-5) 95% 90%
2 Moderately-differentiated (6,7) 75% 63%
3 Poorly-differentiated (8,9) 50% 45%

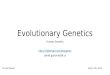
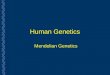
Histopathology of well- (A), moderately- (B) and poorly-differentiated infiltrating ductal carcinoma of the breast. “A” shows abundant tubules without pleomorphism or mitotic activity, while “C” shows lack of tubules with numerous mitotic figures and nuclear pleomorphism. The tumor in “B” is intermediate.

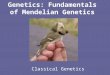
Routine Proteomics
• ER/PR: ER+ = better prognosis– IHC, also true if PR+– >10% of cells with nuclear staining = positive– <5% nuclear staining = neg
• Her2 (IHC, ELISA, FISH, mRNA)– >30% of cells with membrane staining =
positive

ER+ breast cancer cells

PR+

HER2+

Genetic Assessment for Familial Cancer
• When?
• Who?
• What?

When?
• ASCO recommends testing for cancer predisposition when there is:
1. Strong family Hx/early onset
2. Tests can be adequately interpreted
3. Results may influence medical mgt
4. >10% probability of detectable mutation in a family

Who?
• Proband and 1st & 2nd degree relatives of the proband

What?
• Family Hx of specific cancers
• Deleterious mutation in gene of interest

Familial Cancer Syndromes
• Characteristics:1. 5% of all cancers
2. Earlier presentation
3. Vertical transmission within a family
4. lifetime risk

Familial Cancer Syndromes
• More red flags1. Clustering of unusual or rare cancer
2. Multifocal disease
3. Bilateral disease in paired organs
4. Multiple 1 cancers

Familial Cancer Syndromes
• Genetic heterogeneity: same disease from alterations in different genes
• Breast Cancer Syndromes:BRCA1, BRCA2, Li-Fraumeni (p53), Cowden
Disease (PTEN), Ataxia-telangiectasia (ATM)

Breast Cancer
• General: 1 in 10 females by age 70• If familial cancer: lifetime risk is 40-87%• RR depends on:
– age at Dx,
– specific penetrance (as determined by epidemiologic studies),
– specific genes (& mutations) involved,
– carrier rate in population,
– environmental factors

Familial Breast Cancer Syndromes
1. Cowden’s Disease: multiple hamartoma syndrome, mandibular hypoplasia, acral keratoses, scoliosis, tumors
• Breast CA, 25-50% lifetime risk• Thyroid CA (& benign adenomas)• Gene PTEN (10q23.3): phosphatase
(dephosphorylates PI3P) and tensin-like (adhesion)• Tumor suppressor gene seen in ~70% glioblastomas
& 60% prostate CA

More Breast CA Syndromes
2. Ataxia-telangiectasia: autosomal recessive progressive neurologic disorder (cerebellar degeneration), risk cancer
– 50-150 X risk of CA– 70% are lymphomas & T-cell leukemias– Also CA of stomach, ovary & skin (melanomas) – Heterozygotes have 3-8 fold risk of breast CA– Gene ATM (11q22-23): role in sensing & signaling
DNA double-strand breaks, also may have PI3K-like function and binds p53, BRCA1 & CHEK2 proteins

More
3. Li-Fraumeni Syndrome: autosomal dominant associated with multiple 1 neoplasms in children and young adults– Sarcoma prior to age 45 + 1st degree relative
with CA before 45 risk breast CA, soft tissue sarcomas,
osteosarcomas, & brain tumors– Gene TP53 (17p13.1):



More4. BRCA2: autosomal dominant trait with risk of
early onset breast CA & male breast CA (less frequently pancreatic or ovarian CA)
• prevalence ~1/1000, Ashkenazi Jews ~1.5%, Icelanders ~0.6%
• Risk of breast CA by age 70 is ~27%, 80% penetrance
• BRCA2 (13q12.3): 27 exons, exon 11 has BRC repeats which controls RAD51, a recombinase enzyme

More BRCA2
• Mutations lead to chromosomal abberations from defective double-stranded DNA repair
• Mutations in both BRCA2 alleles Fanconi Anemia
• Male familial breast CA also associated with mutations in DHTR (androgen receptor)




More
5. BRCA1: autosomal dominant trait with markedly susceptibility to breast & ovarian CA
• Breast CA prior to age 40 without DCIS component
• Prevalence 1 in 883 Caucasians, ~1% of Ashkenazi Jews
• Penetrance ~50-60%, cumulative life time risk ~87% of breast CA, 44% for ovarian CA
• Cancers usually higher-grade & stage

BRCA1
• Large gene: 24 exons at 17q21, protein 220-kDa• NH2 terminus RING finger domain (ubiquitin
ligase activity) & carboxy-terminus BRCT repeats are highly conserved
• BRCA1 complexes with proteins involved in DNA repair, transcription, chromatin remodeling, & protein ubiquination
• DNA damage leads to hyperphosphorylation of BRCA1

BRCA1
• BRCA1 colocalizes with BRCA2 & RAD51 proteins during S-phase
• BRCT domain is protein-protein interaction module involved in DNA repair & cell cycle control
• Mutations in mouse Brca1 lead to -irradiation hypersensitivity & genetic instability




Screening for Familial Breast Cancer
• Consider for presentation <50 with two first degree relatives <50 with breast or ovarian CA
• Bilateral breast cancer
• Breast and ovarian in same patient

BRCA1
• ~50% of familial breast CA if 4 family members <60 with breast CA
• ~80% if both breast and ovarian Ca
• Tumor suppressor gene > 100 mutations described

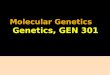
Risk Assessment
• References:– Couch FJ, et al. BRCA1 mutations in women attending
clinics that evaluate the risk of breast cancer. NEJM 1997;336:1409-15.
– Gail MH, et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Nat Cancer Inst 1989;81:1879-86.
– Colditz GA, et al. Family history, age, and risk of breast cancer: prospective data from the Nurses’ Health Study. JAMA 1993;270:338-43.

Probability of Detecting BRCA1 Mutation in Families

Treatment
• Selective estrogen receptor modulators = tamoxifen
• Aromatase inhibitors= anastrozole, letrozole– Improved disease-free survival compared to tamoxifen
• HER2 inhibition = Herceptin (trastuzumab)• Zinc-binding inhibitors, tyrosine kinase inhibitors
(Tykerb), anti-VEGF & other HER2 directed drugs all in clinical trials

Treatment
• Tamoxifen: breast cancer trial 45% reduction in incidence compared to placebo
• Prophylactic mastectomy: 85% reduction in risk, life expectancy 2.9-5.3 yrs, but may still develop breast CA