Embed Size (px)
Citation preview

Breast Cancer Survivorship
Melissa Accordino, MD
Assistant Professor of Medicine
Herbert Irving Comprehensive Cancer Center
Columbia University Medical Center

Who are the Cancer Survivors?
• More than 1 in 3 Americans will be
diagnosed with cancer in their lifetime
• 15.5 million Americans have a personal
history of cancer; >4% of the US
population
• More than 28 million survivors worldwide

Cancer Survivorship Facts
• Prevalence will increase sharply during the next
25 years with aging of the population
• 60% of survivors are over the age of 65
• Breast, Prostate, and Colorectal are the 3 most
prevalent cancer sites
• Approximately 14% of survivors were diagnosed
20 years ago

Estimated and Projected # of Survivors
by Year Since Diagnosis in the US
Source: de Moor JS, et al. CEBP Annual Report 2013;22:561-570

Estimated Number of Survivors by
Cancer Site in the US (2012)
Source: de Moor JS, et al. CEBP Annual Report 2013;22:561-570

No Clear Consensus on Survivor Definition
Disease-free after
5 years
Not sure
How do you define a cancer survivor (n=144)
Disease-free after 2-3 years From the moment of
diagnosis and for the
balance of life
From diagnosis to
recurrence Following completion of
active treatment
Source: P De Fusco, et al. SABCS 2007, ASCO 2009

Definition of a Cancer Survivor
“From time of diagnosis, through the balance of his
or her life”
– NCCN
“Anyone with a history of cancer, from the time of
diagnosis and for the remainder of life, whether that
is days or decades.”
– National Coalition for Cancer Survivorship

What Has Led to our Success?
• Earlier detection
• Novel treatments
• Combined modality therapy
• Prolonged adjuvant and/or maintenance
therapies
• Prevention of second malignancies

For Many Patients, Cancer is now a
Chronic Disease…

The Effects of Cancer and Its
Treatment
• Physical and/or psychosocial Effects
• Long-term effects
• Late effects
• Range in severity
• Some improve over time, while others
progress or become permanent

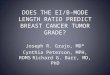
Health Status Significantly Poorer in
Cancer Survivors
Excellent
Very Good
Good
Fair
Poor
Excellent
Very Good
Good
Fair
Poor
31% Fair & Poor 18% Fair & Poor
Cancer Survivors
(n=1,817) Non-cancer Controls
(n=1,817)
Source: Yabroff KR, et al. JNCI 2004;96:1322-30

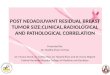
Loss of Productivity Significantly
Poorer in Cancer Survivors
0
10
20
30
40
50
60
70
80
90
100
Held job in past12 months
Unable to workdue to health
problems
Limited in amountof work due to
health
Lost days fromwork in past 12months (mean)
% o
f patients
with lost pro
ductivity
Breast Cancer Survivors (n=301) Matched Controls (n=1,479)
*
*
* *
* p<0.02
Source: Yabroff KR, et al. JNCI 2004;96:1322-30

IOM Findings: Survivorship Care
• Survivorship care is a
neglected phase of the
cancer care trajectory
• Recurrence, second cancers,
and treatment late effects
concern survivors
• Few guidelines on follow-up
care
• Providers lack education and
training

IOM Findings: Survivorship Care
• Survivors may:
• Be unaware of risk
• Have no plan for follow-up
• Opportunities to intervene
may be missed
• Care is often not coordinated
• Models of survivorship care
not tested

Why is Cancer Different from other
Chronic Diseases?
Cancer treatment is…
Complex
Multi-modal
Multi-disciplinary
Toxic
Expensive
Often poorly coordinated
Cancer treatment usually occurs in isolation from
primary health care delivery

Other Challenges
• Limited systematic study of the late effects of
cancer therapy
• Follow-up care plans have been ad hoc, with
focus on surveillance for recurrence
• When should health promotion and chronic
disease prevention become the focus?
• Infertility?

What is Needed to Implement the
Survivorship Care Plan?
• Acceptance of cancer as a chronic disease – following
an initial period of extraordinarily complex therapy
• Staff support for time required to prepare and
communicate the plan
• Expand the evidence-base of knowledge re: late
effects, follow-up needs, and survivorship care
• Train all health professions in the needs of the
growing number of cancer survivors – how to act on
the care plan recommendations

Survivorship Care Plans: A model for
Integration of QOL & QOC
Quality of Life
Quality of Care

Breast Cancer as a Model for Study of
Late & Long-term Effects
• Most common cancer in women
• Occurs across the lifespan
• Complex treatments, high rates of cure
• Treatment affects menopausal status and
endocrine milieu of the woman
• Potential for substantial impact on physical and
emotional health

Surveillance Testing after Breast Cancer
• Breast cancer adjuvant clinical trials abandoned routine
monitoring with chest, liver, and bone imaging in the
1990s – recurrence detection rare before clinical
symptoms
• Two randomized trials conducted in the 1990s did not find
a difference in survival outcomes in women who had
routine clinical visits and mammograms compared to
women with more intensive surveillance including blood
work, chest films, scans, and ultrasounds
Sources: ASCO Guidelines 2006, 2013
Rojas et al. Cohrane Review 2005

Tumor Marker Surveillance after
Breast Cancer
• No RCT data to support use of tumor markers for breast
cancer monitoring (CEA, CA 15-3, CA 27.29) for effect on
survival outcome, i.e. that detection of recurrence earlier
makes a difference
• The rate of false negative or false findings for these
markers are not known
• Normal or abnormal tumor marker results can contribute
to false reassurance and/or increased anxiety for patients,
as well as unnecessary medical evaluations

Source: Schnipper LE, et al. JCO 2012;30:1715-24

Surveillance Testing Utilization Women with early stage breast cancer diagnosed 2001-2009 (n=258)
at an academic medical center
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% of sample who received at least one % for pure surveillance testing
Source: Han EE, et al. Cancer 2013;15:4316-24

Surveillance Testing Utilization Women ≥65 with locoregional breast cancer diagnosed 2001-2007
(n=39,650) using SEER-Medicare
Tumor Marker Use
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Months 3-12after
Diagnosis
Months 13-24 after
diagnosis
35% 28%
% In
cre
ase
d C
osts
of C
are
*
Costs of Care Increased in
Patients who had TMs
*
* p<0.001
Source: Ramsey SD, et al. JCO 2015;32:149-55

Common Survivorship Care Concerns
• Pain
• Fatigue
• Depression
• Physical limitations
• Cognitive changes
• Lymphedema
• Sexual dysfunction
• Menopause related symptoms
• Body Image / Weight Gain
• Secondary cancers
• Late effects of therapy
• Osteoporosis, cardiac, infertility

Cancer-related Fatigue
• Most common side effect of cancer and its treatment
• Occurs in 60-96% of patients during treatment (Wagner &
Cella, 2004)
• Fatigue may persist for months or years after successful
treatment completion
• 30% of breast cancer survivors report fatigue 1-5 years
post-diagnosis (Bower et al.;2000)
• 63% of fatigued survivors continue to report fatigue 5-10
years post-diagnosis (Bower et al., 2006)

Cancer-related Fatigue
• Different than “normal” fatigue due to lack of sleep or over-
exertion
• More pervasive, debilitating, longer-lasting
• Involves physical, mental, and emotional components
• Not relieved by adequate sleep or rest
• Fatigue occurs across different types of cancer and different
types of cancer treatment
• Mechanisms underlying cancer-related fatigue have not
been determined

What Causes Fatigue?
Comorbid
medical
conditions
•Cardiovascular
disease
•BMI
Comorbid
symptoms
•Pain
•Menopausal sx
•Sleep disturbance
Fatigue
Biological factors
•Anemia
•Inflammation
Demographic
factors
•Age
•Income
•Marital status
Psychosocial
factors
•Depression
•Catastrophizing
coping style
Health
behaviors
•Physical activity

Cognitive Complaints
• Self-reported complaints don’t always match performance
on neurophysiological (NP) testing
• Tests of memory, attention, reasoning, visual-spatial abilities
• Some studies document impairment on NP tests in cancer
patients that pre-exist cancer treatment
• 20-30% of breast cancer patients
• Biology of cancer (e.g. inflammation related)?
• Common risk factors for both cancer and cognitive impairment (e.g.
poor DNA repair mechanisms?)
• True incidence of cognitive decline is uncertain
• Estimates range from 15-25%; some percentages as high as 61%

Risk Factors
• Age
• Cognitive reserve or
vulnerability
• Age and medication
• Genetic predisposition/
vulnerability to
chemotherapy or
cognitive impairment:
• APOE, COMPT
• Poor DNA repair
• Menopause
• Hormone therapy
• Anxiety/Depression
• Supportive Care meds
• Comorbid medical
conditions
• Surgery and anesthesia
• Sleep disturbance

Candidate Mechanisms for Cognitive
and Brain Changes
Blood-brain
barrier integrity
Changes in cognition, and
brain structure and function
DNA damage
and telomere
length
Cytokine
deregulation
Estrogen or
testosterone
reduction
Genetic
susceptibility
Source: Ahles and Saykin Nature Reviews Cancer 2007;7:192-201

The Effect of Modafinil on Cognitive
Function in Breast Cancer Survivors
Open label cancer survivors >30 days post chemo and/or RT with fatigue
(n=76) those with improvement after 4 weeks (n=68) randomized to
Modafinil vs. Placebo x 4 weeks
Open label portion significant effect on:
• Speed of memory (p=0.007)
• Quality of episodic memory (p<0.0001)
After randomization, relative to placebo, improvement
of:
• Speed of memory (p=0.03)
• Quality of episodic memory (p=0.02)
• Mean continuity of attention (p=0.02)
Source: Kohil S, et al. Cancer 2009;115:2605-16

Patient Factors and Interaction with
Treatment & Survivorship Outcomes
• Effects of tobacco use on drug metabolism and treatment
efficacy
• Weight and weight gain and its effect on treatment efficacy,
comorbid conditions, and survivorship outcomes
• Physical activity influence on survival and other outcomes
• Concomitant medications and their effects on outcomes,
e.g. metformin, aspirin, statins
• Comorbid conditions, e.g., hypertension or DM, and their
effect on outcomes

Obesity at Diagnosis Associated with Inferior
Outcomes in HR+ Breast Cancer (E1199)
N=4,770 node positive & high risk node negative Br CA patients who
received AC, taxanes, and hormonal treatment. Median age 49, 37% obese
DFS for obesity (HR positive/HER-2 negative/unknown
Multivariable analysis HR 1.24 p=0.008
Source: Sparano JA, Cancer 2012;118:5937-46

Obesity at Diagnosis Associated with Inferior
Outcomes in HR+ Breast Cancer (E1199)
N=4,770 node positive & high risk node negative Br CA patients who
received AC, taxanes, and hormonal treatment. Median age 49, 37% obese
OS for obesity (HR positive/HER-2 negative/unknown
Multivariable analysis HR 1.37 p=0.002
Source: Sparano JA, Cancer 2012;118:5937-46

Lifestyle Modifications & Br CA Prognosis
• Observational studies suggest:
• Higher physical activity may improve survival
• High fruit/veg and low fat diet may improve
survival
• Higher BMI is associated with poorer outcomes
• Clinical trials suggest:
• High fruit/veg and low fat diet may improve
survival in ER- Br CA (WINS)
• Potential mechanisms include insulin-IGF-1 axis,
inflammatory pathways, and hormonal pathways
Chlebowski JCO 2002, Holmes JAMA 2005, Pierce JCO 2007, Chlebowski JNCI 2006

Physical Activity & Mortality After BC Diagnosis
Nurses’ Health Study (n=2,987)
MET-hrs/wk RR (95% CI)*
<3 Ref
3-8.9 0.71 (0.56-0.89)
9-14.9 0.59 (0.41-0.84)
15-23.9 0.56 (0.41-0.77)
24+ 0.65 (0.48-0.88)
*Adjusted for age, time since
diagnosis, smoking, BMI,
menopausal status, HRT use, age at
1st birth, parity, OC use, energy
intake, stage, treatment
Source: Holmes MD, et al. JAMA 2005;293:2479-86

Diet, Physical Activity and Survival Women’s Healthy Eating and Living (WHEL) Study (n=1,490)
Source: Pierce JP, et al. JCO 2007;25:2345-51

Women’s Intervention Nutrition Study (WINS) (n=2,437)
Chlebowski JNCI 2006
ER+ subjects
ER- subjects

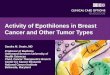
Insulin and Breast Cancer Prognosis
0
0.5
1
1.5
2
2.5
3
3.5
< 27 27-35.3 35.3-51.9 > 51.9
HR
Distant Recurrence p=0.007
Insulin Quartiles (pmol/L)
Death p=0.001
Source: Goodwin PJ, et al. JCO 2002;20:42-51

SUMMARY
• Increasing number of cancer survivors
• Breast, Prostate, and Colon = 50%
• Successes in outcome have come at a cost:
• Financial
• Physical
• Functional
• Psychological
• Much research to be done!

THANK YOU