Embed Size (px)
Citation preview

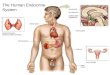
BreastBreast

Modified sweat glands.Modified sweat glands.Lobes and lobules of gland Lobes and lobules of gland in fat tissue stroma.in fat tissue stroma.
Ducts emerge from acini of glandsDucts emerge from acini of glandsSmaller ducts join to form lactiferous ductsSmaller ducts join to form lactiferous ducts
Lactiferous ducts merge just Lactiferous ducts merge just beneath he nipple to form a beneath he nipple to form a lactiferous sinus. Then lactiferous sinus. Then individually open on nippleindividually open on nipple

Ducts emerge from acini of glandsDucts emerge from acini of glandsSmaller ducts join to form lactiferous ductsSmaller ducts join to form lactiferous ducts
Lobes and lobules Lobes and lobules of gland of gland in fat tissue stroma.in fat tissue stroma.

Axillary A lateral thoracicInternal mammary A perforatingIntercostal lateral
Axillary veinInternal mammary VIntercostal veins
Supraclavicular nerveItercostal Nsympathatic





Benign Breast DiseaseBenign Breast Disease Congenital ConditionsCongenital Conditions Traumatic ConditionsTraumatic Conditions InfectionsInfections Aberrations of Normal Development Aberrations of Normal Development
and Involution (ANDI)and Involution (ANDI) NeoplasticNeoplastic
Benign - FibroadenomaBenign - Fibroadenoma

Congenital ConditionsCongenital Conditions
CongenitalCongenital Supernumerary Supernumerary
nipple along nipple nipple along nipple lineline
Supernumerary Supernumerary breastbreast
Aplasia – turners, Aplasia – turners, Juvenile Juvenile hypertrophyhypertrophy


Traumatic ConditionsTraumatic Conditions
Traumatic fat necrosisTraumatic fat necrosis Cracks of nippleCracks of nipple HematomaHematoma Traumatic mastitisTraumatic mastitis Milk fistulaMilk fistula

Traumatic Conditions (Fat Traumatic Conditions (Fat Necrosis)Necrosis)
Follows trauma, Follows trauma, surgery or radiationsurgery or radiation
Small, hard mass - Small, hard mass - confused with confused with carcinomacarcinoma
Focal necrosis of fat Focal necrosis of fat with inflammationwith inflammation
Foamy lipid-laden Foamy lipid-laden macrophagesmacrophages
Later fibrosis, Later fibrosis, calcificationcalcification

Mammary fistulaMammary fistula
Congenital (rare)Congenital (rare) AcquiredAcquired
Varient of MDEVarient of MDE Incision and Incision and
drainage of abcess drainage of abcess in lactating breastin lactating breast

InfectionsInfections
AcuteAcute Mastitis neonatorumMastitis neonatorum Pubertal mastitisPubertal mastitis Traumatic mastitisTraumatic mastitis Metastatic mastitsMetastatic mastits Mammary duct Mammary duct
ectasiaectasia Lactational mastitsLactational mastits Acute suppurative Acute suppurative
mastitismastitis
ChronicChronic Chronic non specific Chronic non specific
chronic breast chronic breast abscessabscess
HidradenitisHidradenitis Pilonidal DiseasePilonidal Disease Postoperative Postoperative
Wound InfectionsWound Infections specificspecific
TuberculosisTuberculosis SyphillisSyphillis ActinomycosisActinomycosis

Duct Ectasia and Duct Ectasia and Periductal MastitisPeriductal Mastitis
? Aetiology, age 40s - 50s, smokers ? Aetiology, age 40s - 50s, smokers Dilatation of breast ducts - fill with Dilatation of breast ducts - fill with
stagnant brown/green secretion - atrophy stagnant brown/green secretion - atrophy and loss of ductal epithelium - secretion and loss of ductal epithelium - secretion spills into periductal tissues - inflammatory spills into periductal tissues - inflammatory reaction (‘mastitis’)reaction (‘mastitis’)
Micro - lyphocytes, histiocytes, plasma Micro - lyphocytes, histiocytes, plasma cellscells
Secondary anaerobic infection, abscessSecondary anaerobic infection, abscess Fibrosis - slit-like nipple retractionFibrosis - slit-like nipple retraction

DuctDuct Ectasia andEctasia andPeriductal MastitisPeriductal Mastitis
PresentationPresentation Nipple discharge - any Nipple discharge - any
colourcolour Nipple RetractionNipple Retraction Subareolar massSubareolar mass AbscessAbscess Mammary duct fistulaMammary duct fistula
May mimic carcinomaMay mimic carcinoma

Duct ectasiaDuct ectasia
Nipple retraction
Lump
Abscess
Nipple discharge - any colourNipple discharge - any colour
Mammary duct fistulaMammary duct fistula

•Antibiotics • Flucloxacillin & • Metronidaziole
• NSAID
Central duct excision(Hadfield operation)


Operations - Hadfield’s Operations - Hadfield’s Major Duct ExcisionMajor Duct Excision
IndicationsIndications : : duct ectasia (periductal mastitis) with duct ectasia (periductal mastitis) with
recurrent episodes +/- fistulaerecurrent episodes +/- fistulae blood stained discharge from one or more blood stained discharge from one or more
ducts in women > 40ducts in women > 40 IncisionIncision : :
circumareolar but < 3/5 the areolar circumareolar but < 3/5 the areolar circumference to allow enough blood circumference to allow enough blood
supplysupply include the orifice of any sinus or fistulainclude the orifice of any sinus or fistula

Operations - Hadfield’s Operations - Hadfield’s Major Duct ExcisionMajor Duct Excision
TechniqueTechnique : : cut the subcutaneous cut the subcutaneous
tissue down to the ductstissue down to the ducts dissect in a plane dissect in a plane
circumfentially around circumfentially around the terminal lactiferous the terminal lactiferous ducts ducts
divide the ducts close to divide the ducts close to the nipple and remove the nipple and remove with a small conical with a small conical wedge of tissuewedge of tissue
include fistulous tracts include fistulous tracts with all granulation with with all granulation with excisionexcision
+/- DT closure 4/0 +/- DT closure 4/0 subcuticularsubcuticular

Lactational MastitisLactational Mastitis

Bacterial MastitisBacterial Mastitis
Cracks and fissures Cracks and fissures form in early form in early breastfeeding breastfeeding
Secondary infection Secondary infection with Staph. aureuswith Staph. aureus
Carried by Carried by nasopharynx of infantnasopharynx of infant AbscessAbscess Chronic scarChronic scar

Fever
Throbbing pain
Skin oedema
Aspiration of pus


Operation - Incision & drainage breast Operation - Incision & drainage breast abscessabscess
Breast abscess :Breast abscess : most occur during lactationmost occur during lactation empty the breast , allowing the baby to feed by the other breastempty the breast , allowing the baby to feed by the other breast drain early when there is a point of maximal tenderness - drain early when there is a point of maximal tenderness - needle needle
aspiration + antibiotics may be more appropriateaspiration + antibiotics may be more appropriate TechniqueTechnique : :
1.1. General anaesthesiaGeneral anaesthesia2.2. incise incise
over point of maximal tenderness or fluctuance over point of maximal tenderness or fluctuance if near the nipple use circumareolar incision if near the nipple use circumareolar incision deepen the incision until drain pus, send for M/C/Sdeepen the incision until drain pus, send for M/C/S Use counter incision in upper breastUse counter incision in upper breast
3.3. break down loculations & take Bx (exclude inflam Ca)break down loculations & take Bx (exclude inflam Ca)4.4. +/- DT +/- kaltostat packing+/- DT +/- kaltostat packing5.5. supportive bra, breast feed when comfortablesupportive bra, breast feed when comfortable


IndicationIndication : solid breast lump that is clinically benign : solid breast lump that is clinically benign
AimAim : to extract the lesion with minimal margin and least : to extract the lesion with minimal margin and least cosmetic defect to establish a histological Dx and remove the cosmetic defect to establish a histological Dx and remove the palpable lump.palpable lump.
Operations - Breast Operations - Breast Excisional BiopsyExcisional Biopsy


Breast Excisional BiopsyBreast Excisional Biopsy Incisions Incisions ::
incise over the lump - adequate excision 1st priority incise over the lump - adequate excision 1st priority 2nd comes aesthetic position2nd comes aesthetic position if possible scar hidden by braif possible scar hidden by bra medial incisions more likely to develop keloidmedial incisions more likely to develop keloid avoid radial incisions except mediallyavoid radial incisions except medially make incision within skin that would be removed if make incision within skin that would be removed if
patient subsequently required a mastectomypatient subsequently required a mastectomy
• Technique : excise lump completely without cutting into ithold specimen with Lane or Allis tissue
forcepscareful haemostasis +/- DT + L.A.subcuticular closure

Caseous form
Sclerosing form
Fibrocaseous
Suppurative form

TuberculosisTuberculosis
Antituberculous Antituberculous drugsdrugs
Cold abscessCold abscess Valvular incisionValvular incision Local anti TBLocal anti TB
FibrocaseousFibrocaseous Simple mastectomySimple mastectomy Anti TBAnti TB

ANDI( Fibrocystic Disease)ANDI( Fibrocystic Disease)
Developed by LE Hughes at Cardiff 1987Developed by LE Hughes at Cardiff 1987 Replaces fibrocystic disease, fibroadenosis, etc.Replaces fibrocystic disease, fibroadenosis, etc. Main Histological Features:Main Histological Features:
Epithelial proliferationEpithelial proliferation Adenosis (increase in no. of acinar units per lobule)Adenosis (increase in no. of acinar units per lobule) Epithelial Hyperplasia ( of cells) Epithelial Hyperplasia ( of cells) ++ Papilloma Papilloma
formationformation FibrosisFibrosis CystsCysts
Retention cystsRetention cysts Blue –domed cyst of Bloodgood (macrocysts)Blue –domed cyst of Bloodgood (macrocysts) Brodie’s tumor (microcysts)Brodie’s tumor (microcysts)

PresentationPresentation
MastalgiaMastalgia CyclicalCyclical Non-CyclicalNon-Cyclical
Lump - many causesLump - many causes Periareolar DisorderPeriareolar Disorder
Nipple DischargeNipple Discharge Nipple RetractionNipple Retraction

Cyclical MastalgiaCyclical Mastalgia
PresentationPresentation Median age 35 yrsMedian age 35 yrs Premenstrual breast discomfort Premenstrual breast discomfort Upper outer quadrant (often bilateral)Upper outer quadrant (often bilateral) Relief during menstruationRelief during menstruation Associated with nodularityAssociated with nodularity Aetiology presumably hormonalAetiology presumably hormonal

Non-Cyclical MastalgiaNon-Cyclical Mastalgia
Not related to menstrual cycleNot related to menstrual cycle Median age 45yrs (pre- or postmenopausal)Median age 45yrs (pre- or postmenopausal) Unilateral, well-localised, ‘trigger spot’Unilateral, well-localised, ‘trigger spot’ Multiple CausesMultiple Causes
Carcinoma Carcinoma Mammary Duct EctasiaMammary Duct Ectasia Sclerosing Adenosis (ANDI)Sclerosing Adenosis (ANDI) Painful ScarPainful Scar Musculoskeletal PainMusculoskeletal Pain Mondor’s DiseaseMondor’s Disease

LumpsLumps TraumaticTraumatic
Fat NecrosisFat Necrosis Organized hematomaOrganized hematoma
InflammatoryInflammatory Mammary Duct Ectasia/Periductal MastitisMammary Duct Ectasia/Periductal Mastitis Chronic breast abcessChronic breast abcess
ANIDANID NodularityNodularity Cysts (Galactocele)Cysts (Galactocele) Sclerosing AdenosisSclerosing Adenosis
Neoplastic Neoplastic BenignBenign
LipomaLipoma Hard FibroadenomaHard Fibroadenoma Giant fibroadenomaGiant fibroadenoma Phyllodes TumourPhyllodes Tumour
MalignantMalignant

NodularityNodularity
Often bilateral, upper outer quadrantOften bilateral, upper outer quadrant May be cyclicalMay be cyclical Associated with mastalgiaAssociated with mastalgia Histology (ANDI)Histology (ANDI)
CystsCysts FibrosisFibrosis AdenosisAdenosis

CystsCysts
Common, 30s-40sCommon, 30s-40s Often multiple, bilateralOften multiple, bilateral Present suddenly (fluid) Present suddenly (fluid)
++ pain, nodularity pain, nodularity Tense, less mobile than Tense, less mobile than
FibroadenomaFibroadenoma Involution of stroma and Involution of stroma and
epitheliumepithelium Turbid fluid (blue)Turbid fluid (blue) Apocrine or simple Apocrine or simple
cuboidal epithelial liningcuboidal epithelial lining

GalactoceleGalactocele
Solitary subareolar Solitary subareolar cystcyst
Dates from lactationDates from lactation Contains milkContains milk Can calcifyCan calcify Can greatly increase Can greatly increase
in sizein size

Cysts of the breastCysts of the breast
Cysts of the breast
Cysts of the breast
Ductal systemDuctal systemNeoplasticNeoplastic
ANIDANID
Macrocysts
Macrocysts
Microcysts
Microcysts
StromaStroma
Duct papilloma
Papillary cystadenoma
Duct papilloma
Papillary cystadenoma
BenignBenign
Degeneration of carcinoma
Degeneration of sarcoma
Intracystic carcinoma
Degeneration of carcinoma
Degeneration of sarcoma
Intracystic carcinoma
Serous
Lymphatic
Blood
Inflammatory
TB cold abscess
Chronic abscess
Hyadatid
Serous
Lymphatic
Blood
Inflammatory
TB cold abscess
Chronic abscess
Hyadatid
GalactoceleGalactocele
Skin cystsSkin cysts
MalignantMalignant
Sebaceous
Dermoid
Sebaceous
Dermoid

Nipple DischargeNipple Discharge
Physiological - pregnancy/lactationPhysiological - pregnancy/lactation Duct EctasiaDuct Ectasia GalactorrhoeaGalactorrhoea Duct PapillomaDuct Papilloma CarcinomaCarcinoma CystsCysts IdiopathicIdiopathic

GalactorrhoeaGalactorrhoea
Milky discharge unrelated to lactationMilky discharge unrelated to lactation Primary PhysiologicalPrimary Physiological
MenarcheMenarche MenopauseMenopause StressStress Mechanical StimulationMechanical Stimulation
SecondarySecondary Drugs: haloperidol, metoclopramideDrugs: haloperidol, metoclopramide Increased Prolactin: pituitary tumour, Increased Prolactin: pituitary tumour,
paraneoplasticparaneoplastic

Management of Breast Management of Breast SymptomsSymptoms
Breast Lump - always need to exclude Breast Lump - always need to exclude CaCa
Breast examination - Is there a lump or Breast examination - Is there a lump or localised nodularity?localised nodularity?
Is there no lump or diffuse nodularity?Is there no lump or diffuse nodularity? Triple AssessmentTriple Assessment
1. FNA1. FNA 2. U/S2. U/S 3. Mammography3. Mammography

Breast Lump – Cyst and Breast Lump – Cyst and MxMx
O/E discrete lump or localised nodularity presentO/E discrete lump or localised nodularity present
FNAFNA
cysticcystic
no bloodno residual lumpthen no cytology
no bloodno residual lumpthen no cytology
solidsolid
re-examine in 6/12
reassure
re-examine in 6/12
reassure
bloody fluid
residual lump
then do cytology
& mammography
bloody fluid
residual lump
then do cytology
& mammography
excisional biopsyexcisional biopsy
no lump or diffuse nodularity
no lump or diffuse nodularity

Palpable Breast Lump - Solid Palpable Breast Lump - Solid MxMx
FNA solid lumpFNA solid lump
CytologyMammography > 35U/STru-cut biopsy (lump > 2cm)
CytologyMammography > 35U/STru-cut biopsy (lump > 2cm)
suspicious or carcinomasuspicious or carcinoma
benignbenign
observe but excise if :• age >35• Pt requests• pain• increasing size• equivocal cytology
observe but excise if :• age >35• Pt requests• pain• increasing size• equivocal cytology
Manage as for breast cancerManage as for breast cancer
Panel comment :
If pt 25 - 35 need FNA/ trucut Dx of fibroadenoma otherwise need exc Bx.
If tru-cut = normal breast tissue then still need histology of the lump.

No Palpable Breast Lump No Palpable Breast Lump MxMx
no lump or diffuse nodularity
no lump or diffuse nodularity
age < 40age < 40age > 40age > 40
re-examine 6/52re-examine 6/52
reassurereassure
benignbenign
Cytology
MammographyU/S
Cytology
MammographyU/S
reassurereassure
benignbenign
suspicious or carcinomasuspicious or carcinoma
Manage as for breast cancerManage as for breast cancer

Nipple dischargeNipple discharge
Nipple dischargeNipple discharge
Bilateral (multiductal)Bilateral (multiductal) UnilateralUnilateral
Physiological
Pathological
Fibroadenosis
Papillomatosis
Duct ectasia
Physiological
Pathological
Fibroadenosis
Papillomatosis
Duct ectasia
Mammography
U/S
Mammography
U/S
Uniductal Uniductal
Fibroadenosis
Papillomatosis
Duct ectasia
?? carcinoma
Fibroadenosis
Papillomatosis
Duct ectasia
?? carcinoma
MultiductalMultiductal
Duct papilloma
Duct carcinoma
Duct ectasia
Chronic absces
??? fibroadenosis
Duct papilloma
Duct carcinoma
Duct ectasia
Chronic absces
??? fibroadenosis
Cytology,prolactin,ductographyCytology,prolactin,ductographyMicrodochectomyMicrodochectomy

FibroadenomaFibroadenoma
Peak incidence 15-25 yrsPeak incidence 15-25 yrs Smooth, highly mobileSmooth, highly mobile 2-3 cm occasionally multiple2-3 cm occasionally multiple Benign tumour of fibrous and glandular tissueBenign tumour of fibrous and glandular tissue Mono- or polyclonal (cyclosporin)Mono- or polyclonal (cyclosporin)

Fibroadenoma - Fibroadenoma - histopathologyhistopathology
Well formed capsuleWell formed capsule Delicate stroma Delicate stroma
surrounding glandular surrounding glandular and cystic spacesand cystic spaces
Epithelium Epithelium compressed and compressed and distorted by the distorted by the stromastroma
++ Coarse calcification Coarse calcification

Benign tumorsBenign tumors

Giant FibroadenomaGiant Fibroadenoma
Peripubertal age Peripubertal age groupgroup
> 5cm > 5cm Rapid growingRapid growing Esp. Asian, black Esp. Asian, black
womenwomen Benign tumourBenign tumour Occasional atypiaOccasional atypia

Phylloides TumourPhylloides Tumour
Present later - 6th decadePresent later - 6th decade Mostly benign, few highly Mostly benign, few highly
malignant with metastasesmalignant with metastases PathologyPathology
Variable size up to 15cm Variable size up to 15cm ++ skin ulcerationskin ulceration
Bulbous projections (‘leaf-Bulbous projections (‘leaf-like’)like’)
Stroma has greater Stroma has greater cellularity, mitoses, nuclear cellularity, mitoses, nuclear pleomorphism than pleomorphism than fibroadenomafibroadenoma
Higher grade lesions Higher grade lesions resemble sarcomaresemble sarcoma







Duct PapillomaDuct Papilloma
Solitary benign tumour Solitary benign tumour in single large duct in single large duct
PresentationPresentation Discharge (Discharge (++ blood) blood) Mass (clinical or XR)Mass (clinical or XR)
Multiple papillae with Multiple papillae with connective tissue axis, connective tissue axis, covered with epithelial covered with epithelial and myoepithelial cellsand myoepithelial cells
Considered benignConsidered benign



Operations - Operations - MicrodochectomyMicrodochectomy
IndicationsIndications : persistent blood stained : persistent blood stained discharge from a single duct opening on discharge from a single duct opening on the nipple -- often find papilloma of duct the nipple -- often find papilloma of duct causing the bleedingcausing the bleeding
TechniqueTechnique : squeeze the breast and : squeeze the breast and nipple until a drop of discharge is seennipple until a drop of discharge is seen
cannulate the duct using a lacrimal probe and secure in place with 3/0 suture passed through the skin along side the duct opening

Operations - Operations - MicrodochectomyMicrodochectomy
TechniqueTechnique : make a radial incision into the : make a radial incision into the nipple along the line of the probe encircling nipple along the line of the probe encircling the duct orificethe duct orifice
Dissect the skin of the areolaaway from the underlying breast for approx 1cm on each side of the probe and excise the breastsegment containing the probe using scissors commencing behind the duct orifice andcontinuing into the breast.
haemostasis & closure

Breast Procedures & Breast Procedures & OperationsOperations
ProceduresProcedures FNAFNA Tru-cutTru-cut needle biopsy - superceded by gun needle biopsy - superceded by gun
BxBx
OperationsOperations Excisional biopsyExcisional biopsy MicrodochectomyMicrodochectomy Hadfield’s Major Duct excisionHadfield’s Major Duct excision Incision and drainage of breast abscess - often Incision and drainage of breast abscess - often
needle aspiration with antibiotics is usedneedle aspiration with antibiotics is used

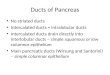
GynecomastiaGynecomastia
Enlargement of the Enlargement of the glandular tissue of glandular tissue of the breastthe breast
Unilateral or bilateral Unilateral or bilateral enlargement forming enlargement forming a disc like lesion a disc like lesion under the nipple and under the nipple and areola which is freely areola which is freely mobilemobile

Gynecomastia (etiology)Gynecomastia (etiology)
PhysiologicalPhysiological NeonatalNeonatal PubertalPubertal Involutional Involutional
(senescent)(senescent) PathologicalPathological Decrease Decrease
production or action production or action of testosteroneof testosterone

GynecomastiaGynecomastia PathologicalPathological
Decrease production or action of Decrease production or action of testosteronetestosterone
Klinfelter’s syndromeKlinfelter’s syndrome Testicular feminization syndromeTesticular feminization syndrome AnorchismAnorchism
Increase production or action of estrogenIncrease production or action of estrogen Pituitary tumorsPituitary tumors Adrenal hypoplasia( addisson’s)Adrenal hypoplasia( addisson’s) Testicular tumors ( Teratoma)Testicular tumors ( Teratoma) Liver failureLiver failure HyperthyroidismHyperthyroidism Estrogen treatmentEstrogen treatment DrugsDrugs
Reserpine, methyldopaReserpine, methyldopa IsoniazidIsoniazid SpironolactoneSpironolactone Tagment, primperan, H2 blockersTagment, primperan, H2 blockers
IdiopathicIdiopathic

Gynecomastia (treatment)Gynecomastia (treatment) PhysiologicalPhysiological No No
treatmenttreatment PathologicalPathological
Treatment of the Treatment of the cause cause
if persist excisionif persist excision Idiopathic Idiopathic
excisionexcision Sub mammarySub mammary Circum areolarCircum areolar

GynecomastiaGynecomastia