Embed Size (px)
Citation preview

Breathe Easier: Using Clinical Education Breathe Easier: Using Clinical Education and Redesign Techniques to Improve and Redesign Techniques to Improve
Pediatric Asthma CarePediatric Asthma Care
Lalit BajajLalit Bajaj, MD, MPH, MD, MPHThe ChildrenThe Children’’s Hospital, Denvers Hospital, Denver
Hoke StappHoke Stapp, MD, FAAP, MD, FAAPColorado Pediatric Partners, LLCColorado Pediatric Partners, LLC
Angela Stowe, MSAngela Stowe, MSPhysician Health Partners, LLCPhysician Health Partners, LLC

IntroductionsIntroductions

ObjectivesObjectives
Understand how clinical education and disease-specific registries can improve implementation of asthma guidelinesIllustrate how the Chronic Care Model and LEAN techniques enhance the redesign of practice office workflow to optimize adherence to evidence based guidelinesApply concepts learned to your health care delivery environment in order to foster collaboration between primary care providers, specialists and hospitals

OutlineOutline
Scope of the ProblemHistorical Perspective on the Development of the CPP Asthma Quality Improvement ProjectProgram DesignData Lessons LearnedOpen Discussion

What problem are we trying to What problem are we trying to solve?solve?
Asthma – prevalenceCosts – direct, indirectDo we follow published guidelines?Is this a problem that we can solve with the current practice environment?

The direct cost of treating childhood asthma is estimated at $3.2 billion annually.1
Children with asthma have 3.5 times as many hospitalizations, 3.1 times as many medication prescriptions, and 1.9 times as many physician office visits as do children without asthma.2
1 Raskin 2003, 2 Raskin 2003
How much does it cost?How much does it cost?

Each year approximately 10.1 million school days are lost due to asthma.1
Between 1990 and 2000 the costs associated with the time adults lost from work due to care for a child sick from asthma increased by 88%.2
And in 1994 alone, the last year for which there is data, children age 5-17 missed 11.8 million school days costing employers $957 million for parents/ caregivers’ lost work time.3
1 AON 2001, 2 AAFA 2001, 3 Williams & Powell 2001
Is this all the cost?Is this all the cost?

Do practitioners use the guidelines?Do practitioners use the guidelines?
http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdfAdherence to published guidelines variesICS for persistent asthma: 25-50%Influenza vaccine: 25-40%Action plans: 9-40%Barriers:
Lack of familiarityLack of agreementLack of self-efficacyLack of timeLack of support staff
440 pagesCabana, 2001

Is there a way to fix the problem?Is there a way to fix the problem?

Is there a way to fix the problem?Is there a way to fix the problem?
Studies all show significant increases in process measures (ICS, action plans, influenza vaccines)More importantly, they are all showing decreases in ED visits and hospitalizationsInterventions vary from guideline implementation to more complex interventions utilizing disease registries, case workers, etc.Some study designs utilize CQI analytic techniques, while other utilize chart reviews

BackgroundBackground
Why invest in quality improvement?Why now?Why asthma?Goals of the program

Challenges to PCPChallenges to PCP
Reimbursement EHR implementationContinuity of carePhysician shortagesRetail-based clinicsVolume of clinical informationTimeIncreasing attention to quality

Asthma Quality InitiativeAsthma Quality Initiative
Collaborative PartnershipColorado Pediatric Partners (CPP)Physician Health Partners (PHP)The Children’s Hospital (TCH)Colorado Allergy and Asthma Centers (CAAC)
Planning, implementation and evaluation team

PopulationPopulationTarget population
Pediatric primary care practices (CPP)19 practices, 68 physicians, 140,000 patients
Pediatric patients with asthma7,000 patients (estimated 5% prevalence)
Geographic areaFront Range

Overarching GoalsOverarching GoalsRedesign underlying systems to achieve sustainable improvementsProvide consistent and evidence based treatmentEmpower PCPs/asthma champions/families to take the best care of the patients

Measurable GoalsMeasurable GoalsProcess outcomesSeverity assessmentController medsInfluenzaAction planClinical outcomesED utilization and hospitalizationMissed days of work and school for parents and patientsCaregiver confidence

Key ComponentsKey Components
Clinical Education and Access to SpecialistsAsthma education for providers and staff
Guidelines into practiceDevice training
Asthma nurse specialist hotlineAsthma consultation or specialist referral
Improved communication b/w PCPs and specialists

Key Components (continued)Key Components (continued)
Practice Redesign and ImprovementDedicated practice coachPractice assessmentImprovement teamChronic Care ModelPDSA, Lean


Key Components (continued)Key Components (continued)
Asthma RegistryTraining and supportRegistry processRegular reportingUsing data to drive improvement


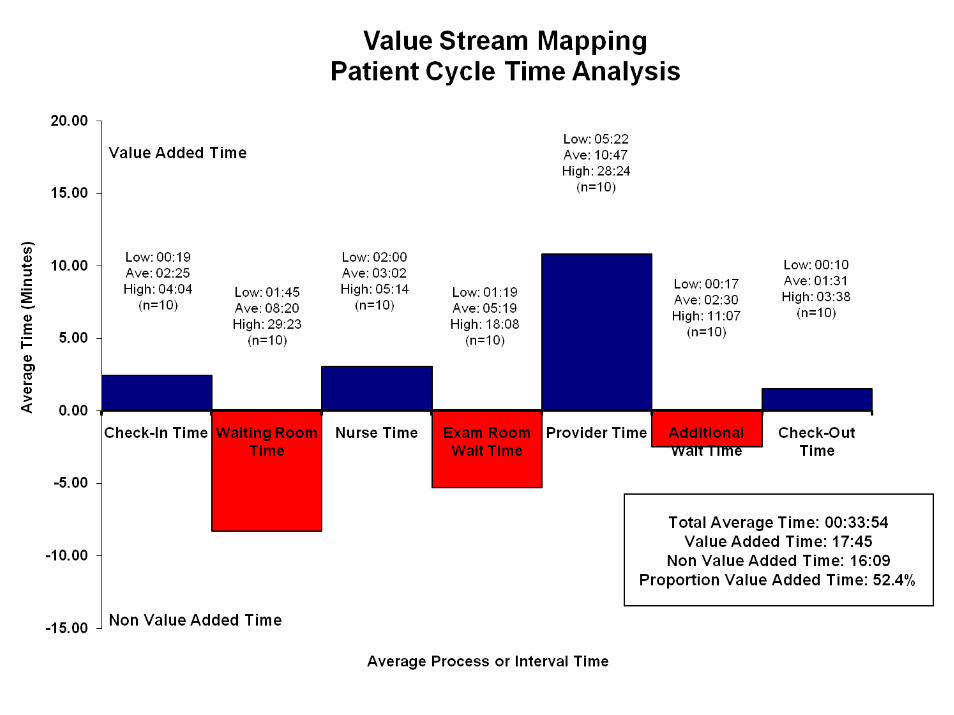
Process MappingProcess Mapping

DataData







Evaluation/MonitoringEvaluation/Monitoring
Follow-up with practice coachPlanning team and board review of IPA and practice-level registry reports
Use data to identify gaps in care and drive future educational sessions
Collaboration with TCH informatics on data analysis

Keys to SuccessKeys to Success
Keys to SuccessPartnershipPlanning and implementation infrastructure
Curriculum buildingRegistry and tool developmentDiscussions with payers
Team members with clearly defined rolesIPA commitmentRigorous data evaluation

ChallengesChallenges
ChallengesHard decisionsBuy-inTime commitmentLong term investmentEMRs

Next Steps Next Steps
Developing IPA-wide educational sessions targeted at improving process outcomes
Action plansAsthma Initiative Users Group
Better understand practice barriers and how to enhance registry functionality
Examine clinical outcomes and patient satisfaction measures

Next Steps (continued)Next Steps (continued)Using framework for additional disease statesGrowth and dissemination
Topic of CPP Board discussionBest practice for implementing best practiceIntegration with other programs
Partnership with TCH and CAACTCH Asthma ClinicsIMPACT Network
Collaboration with IPIP30% of CPP practices currently participating
Linking information systems

How is the office impacted?How is the office impacted?

ScenariosScenarios
Practice is meeting significant resistance from one of the “more senior” partners that he is resistant to changing his practice to incorporate the program. “My patients get all of the asthma care they need.”
Same provider, nine months later, with sense of accomplishment on the number of patients he has activated in registry, and noting improvement in patient care

ScenariosScenariosMother of persistent asthmatic, having difficulty keeping her child's asthma symptoms under control prior to instituting Asthma Quality Control Program. Unsure what medicines to use when.
Since program onset, she now receives updated, written action plan to take home for review when her child’s asthma flares. She feels increased sense of competence and confidence in maintaining her child’s health.

ScenariosScenariosTrials of office implementation. Staff concerned about possible increased workload, how will this fit into workflow, does this make a difference for the patient.
Establish initiative champions, process development group. Seek input from affected staff, develop processes, continually refine processes.
Use Asthma Registry reports to highlight accomplishments of team effort. Meeting or exceeding goals and relationship to improved care.

Open DiscussionOpen Discussion
What is the current patient care environment in terms of care for a patient with asthma?
Is the care focused on chronic or episodic care?What do the most current guidelines recommend?
Severity assessment - do you use a validated tool?Are controllers used appropriately?Flu shotsAction plans - are you comfortable with the content?

Open DiscussionOpen Discussion
How do you know how you’re doing?Do you measure adherence to guidelines?
Is there adequate communication with specialist/hospitalist?
What tools do we need to What tools do we need to improve asthma care?improve asthma care?
Clinical educationKnow who the patients areThe right information at the right timeA way to measure performanceA way to incorporate into practice so we don’t dieFrequent feedbackSome moneyPartners (can’t do it alone)





























