Embed Size (px)
Citation preview
Breathlessness in the ED
Palliative care workshop for EM residentsJuly 29, 2015

DisclosuresNo disclosures
Case“CTAS 1 to the resus room”
mid 70s female in acute respiratory distress
Has been placed on O2 by FM by EHS but despite this still only has O2 sats of 88% and significant WOB
Hx of severe COPD, on home O2 and max medical therapy. Frequent hospitalizations in past 3 months and steadily declining, now fully bed bound at home due to symptoms
What do you do next?
What is dyspnea?
“I feel like I am suffocating.”
“I am afraid and feel like I am drowning.”
“I have a tightness in the chest”
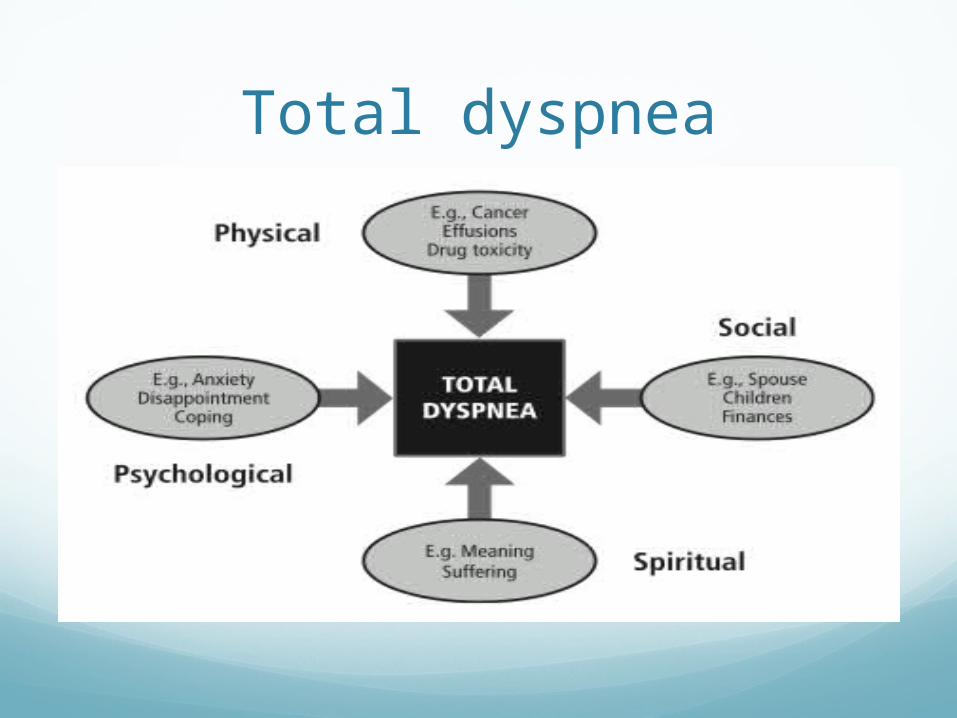
Total dyspnea
Cancer pts: lung, GI (esophagus), Breast, ENT, lung mets most common to have symptoms
CHF: 65% will have some dyspnea
COPD: 90% will have some dyspnea
IPF
Motor diseases: ALS, MS
Any patient with a life-threatening illness

When to think of palliative care?
Cancer, especially if metastatic or if lung, esophagus or ENT cancer
Advanced COPD: on home 02
CHF with EF <25%
Other significant co-morbidities
Recurrent ED visits/admissions for same problem in last 3 months
Poor functional status: ie ECOG 3 or 4
Pt expresses wish for comfort care or DNR
Surprise question

Goals of CareConcurrently treat the symptom while
addressing the underlying cause (if appropriate)
Outcomes are better when a palliative approach is adopted earlier in the disease process
Once those causes are no longer treatable, managing the symptom becomes the main priority
Non-pharmacologic options
fans directed towards face, open windows, cold compresses on face can help
pulmonary rehab
Acupuncture
breathing training (upright forward leaning position, controlled breathing, pursed-lip breathing)
relaxation strategies
walking aides


Home O2 criteria Arterial oxygen saturation (SpO2) less
than 88% for 6 min
Ambulatory Desaturation to less than 88% for 1 min

O2 delivery systemsNasal Prongs (NP) : 1-6 lpm , 22-40% Fi02
Simple Mask (SM) : 5-12 lpm, 35-50% FiO2
Non Rebreather Mask : 15lpm, 60-90% Fi02
High Flow Face Mask : up to 95 % Fi02
High Flow Nasal Prongs (HFNP) : 100% Fi02 with very high flowrates
Bi-Level Positive Airway Pressure (Bipap) : set Fi02 plus ventilatory support ( aka non invasive ventilation )

High Flow Nasal Prongs
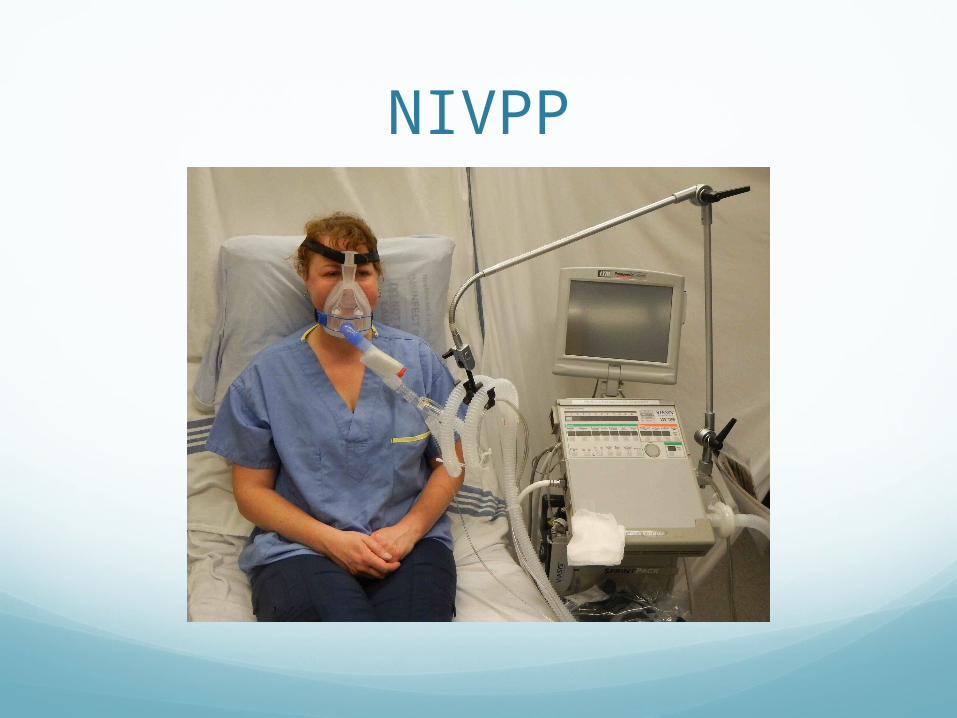
NIVPP

Situations to consider HFNP/BiPAP
Time-limited trial
Goal-limited trial


Back to our casePatient’s symptom are controlled with HFNP and
opioids.
Goals of care are discussed with patient and family
Patient is clear that she does not want further life prolonging treatment
Symptoms are managed with opioids and midazolam
Patient passes away 2 days later on the palliative unit
SummaryDetermine patient’s values/goals of care
Investigate and treat underlying cause if appropriate
Oxygen has a role in palliative care, but only use it if it is helping to achieve the patient’s goals
Opioids are main treatment for refractory dyspnea and will not hasten death when used appropriately
Concept of total dyspnea – address other factors which may be contributing