Embed Size (px)
Citation preview

Breech Breech PresentationPresentation
Breech Breech PresentationPresentation
Name: Pritiss NairName: Pritiss NairGroup No: 2Group No: 2

Definition• Breech presentation is the
entrance of the fetal buttocks or lower extremities into the maternal pelvic inlet.
• It is the most commonest form of malpresentation.

Introduction
Breech presentation occurs in 3-4% of all
deliveries. The occurrence of breech presentation decreases with advancing gestational age.
Breech presentation occurs in 25% of births that occur before 28 weeks’ gestation, in 7% of births
that occur at 32 weeks, and 1-3% of births that
occur at term. .
Perinatal mortality is increased 2- to 4-fold with breech presentation, regardless of the mode of delivery. Deaths most often are associated with
malformations, prematurity, and intrauterine fetal
demise.

Types of breech Presentation 1. Complete (Flexed breech)- Normal attitude of full flexion is
maintained.- The thighs are flexed at the hips and
the legs at the knees.- The presenting part consists of 2
buttocks, external genitalia and 2 feet.- It is commonly present in multiparae.

2. Incomplete
- This is due to varying degrees of extension of thighs or legs at the podalic pole.
- There are 3 types:
a) Breech with extended legs( Frank Breech)
- The thighs are flexed on the trunk and the legs extended at the knee joints.
- The presenting part is the 2 buttocks and external genitalia.
- Usually occurs in primigravidae due to tight abdominal wall, good uterine tone and early engagement of breech.

• b) Footling presentation- Both the thighs and legs are partially
extended bringing the legs to present at the brim.
c) Knee Presentation- Thighs are extended but knees are flexed,
bringing the knees down to present at the brim.




EtiologyEtiology PrematurityPrematurity Factors preventing spontaneous Factors preventing spontaneous
version:version:-Twins-Twins-Oligohydramnios-Oligohydramnios-Septate or bicornuate uterus-Septate or bicornuate uterus-Short cord-Short cord-Intrauterine death of fetus-Intrauterine death of fetus Favourable adaptation:Favourable adaptation:-Hydrocephalus-Hydrocephalus-Placenta previa-Placenta previa-Contracted pelvis-Contracted pelvis-Cornufundal attachment of placenta-Cornufundal attachment of placenta

Undue mobility of the fetus:Undue mobility of the fetus:
-Hydramnios-Hydramnios
-Multiparae with flax abdominal wall-Multiparae with flax abdominal wall
Fetal Abnormalities:Fetal Abnormalities:
-Trisomies 13, 18, 21-Trisomies 13, 18, 21
-Myotonic dystrophy-Myotonic dystrophy

Positions• The sacrum is the denominator of breech
and there are 6 positions:a)Right sacro posteriorb)Left sacro posteriorc)Right sacro laterald)Left sacro laterale)Right sacro anteriorf)Left sacro anterior
The commonest position is assumed at left
\ sacro anterior.


Mechanism of Labour Sacro anterior position: The principal movements
occurs in 3 places- the buttocks, shoulders and head.
Buttocksa) The engaging diameter is bi-trochanteric = 10cm
with the sacrum directed towards ilio-pubic eminence.When the diameter passes the pelvic brim, the breech is engaged.
b) Descent of buttocks until ant. buttock touches pelvic floor.
c) Internal rotation of ant. Buttocks by1/8th of a circle placing it behind pubic symphysis.
d) Further descent with lateral flexion of the trunk until ant. hip hinges under symphysis pubis.
e) Delivery of the trunk and lower limbs.f) Restitution occurs so that buttocks occupy the
original oblique position.

Shoulders
a) Bisacromial diameter =12cm engages in the same oblique diameter occupied by buttocks.
b) Descent occurs with internal rotation of shoulders causing shoulders to lie in AP diameter of pelvic outlet. Trunk simultaneously rotates externally by 1/8th of circle.
c) Delivery of posterior shoulder followed by ant. shoulder by ant. flexion of delivered trunk.
d) Restitution and external rotation: Untwisting of trunk occurs putting anterior shoulder towards right thigh in L.S.A and left thigh in R.S.A. External rotation of shoulders occur to the same direction because of internal rotation of occiput 1/8th of circlr anteriorly.
e) Fetal trunk is now positioned as dorso-anterior.

Head
a) Engagement occurs through oblique diamter occupied by buttocks or through transverse diameter. The engaging diameter of head is suboccipito-frontal= 10cm
b) Descent with increasing flexion
c) Internal rotation of occiput anteriorly through 1/8 or 2/8 of circle, placing occiput behind symphysis pubis.
d) Further descent until sub-occiput hinges under symphysis pubis.
e) Head is born by flexion- the chin, mouth, nose, forehead, vertex & occiput.

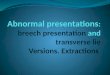
A)Mechanism of breech delivery.Right sacrum transverse(RST) at the onset of labor;engagement of the buttocks usually occurs in the oblique or tranverse diameter of the pelvic brim.

B)Early second stage.The buttocks have reached the pelvic floor and internal rotation has occurred so that the bitrochanteric diameter lies in the AP diameter of the pelvic outlet

C)Late second stage.The anterior buttock appears at the vulva by lateral flexion of the trunk around the pubic symphysis.The shoulders have not yet engagement in the pelvis.

D)The buttocks have been delivered,and the shoulders are adjusting to engage in the transverse diameter of the brim.This movement causes external rotation of the delivered buttocks so that fetal back become uppermost.

E)The shoulder have reached the pelvic floor and have undergo internal rotation so that the bisacromial diameter lies in the AP diameter of the pelvic outlet. Simultaneously, the buttocks rotate anteriorly through 90 degree. this is called Restitution.the head is engaging in the pelvic breim,and the sagittal suture is lying in the transverse diameter of the brim.

F)The anterior shoulder is born from behind the pubic symphysis by lateral flexion of the delivered trunk

Partial Breech Presentation
Partial breech extraction is employed when the operator discerns that spontananeous delivery will not occur or that expeditious delivery is indicated for fetal or maternal reason.The body is allowed to deliver spontaneously up to the level of the umbilicus

A) Shoulder engaged, posterior (left) shoulder at lower level in pelvis that anterior shoulder.

B)Rotation of trunk causing posterior shoulder to rotate to anterior and slip beneath the pubic symphysis

C)Maneuver for delivery of the head.The fingers of the hand are inserted into the infant’s mouth or over mandible;the right hand exerts pressure on the head from above.

D)Mauriceau-Smellie-Veit maneuver for delivery of the head.The finger of the left hand are inserted into the infant’s mouth or over the mandible;the fingers of the right hand curve over the shoulders.An assistant exerts suprapubic pressure on the head.

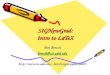
Extraction Of Breech

• A)Abduction of thigh and pressure in popliteal fossa causes the knee to flex and become accessible.

• B)Delivery of leg by traction on the foot

• C)application of Piper forceps, employing towel sling support. The forceps are introduced from below, left blade first, aiming directly at intended position on sides of the head.

• D)Buttocks brought to hollow of sacrum

• E)Traction on anterior leg causes buttocks to advance and rotate into direct AP diameter of pelvis.Continued downward traction causes the back to rotate anteriorly.

• F) further downward traction causes the shoulder to engage on the transverse diameter of the inlet.

• Delivery of breech with one finger in the groin. The wrist is supported with the other hand. When the posterior groin is accessible, the index finger of the other hand is placed in it to complete delivery of the breech.

• Flexion and abduction of thigh to deliver extended leg.

Criteria for VD or CS
VDFrank positionGA>34wFW=2000-3500grAdequate pelvisFlexed headNonviable fetusNo contraindication Good progress labor
CSFW> 3500grFootlingSmall pelvisDeflexed headArrest of laborGA24-34wElderly PGInf or poor historyFetal distress

Diagnosis
Diagnosis can be:
a) Clinicalb) Sonographyc) Radiology

Complete Breech Frank BreechPer abdomen:
Fundal grip
Lateral grip
Pelvic grip
F.H.S
Head- suggested by hard and globular mass.
Head is ballotable. Fetal back is to one side and irregular limbs on the other side.Breech- suggested by soft, broad & irregular mass.Breech is usually not engaged during pregnancy.Usually located at higher level round about the umbilicus.
HeadIrregular small parts of feet may be felt.Head is non-ballottable.Irregular parts are felt less.
Small, hard, conical mass is felt.Breech is usually engaged.
Located at a lower level in the midline due to early engagement of breech.
Per vaginum:During pregnancyDuring labour
Soft & irregular parts are felt through the fornix.Palpation of ishial tuberosities,sacrum & feet by the sides of buttocks.The foot felt is identified by the prominence of the heel and lesser mobility of the great toe.
Hard feel of the sacrum, often mistaken as the head.Palpation of ischial tuberosities, anal opening and sacrum only.

Zatuchni-Andros Breech Scoring
Add 0 Points Add 1 Point Add 2 Points
Parity 0 1 2
Gestational age (wk)
39+ 38 <37
EFW (lb) 8 7-8 <7
Previous breech
0 1 2
Dilatation 2 3 4
Station -3 -2 -1
If the score is 0-4, cesarean delivery is recommended.

• Ultrasonography is most informative.a) It confirms the clinical diagnosis-
specially in primigravidae with engaged frank breech or with tense abdominal wall and irritable uterus.
b) Detect fetal congenital abnormalityc) Measure biparietal diameter, gestational
weight and approximate weight of fetusd) Localises placentae) Acessment of liquor volumeAttitude of head-flexion or hyperextension

Complications• During pregnancya) Birth anoxiab) Injuryc) sepsisd) Genital edema and ecchymoses due to caput
formatione) Hypoxiaf) Prolapsed cordg) Fracture of femur inflexionh) Placenta previai) Difficulty in delivery of shoulders, can cause
damage to brachial plexus of fetusj) Difficulty in delivery of head, intracranial bleeding
due to tear of tentoriumk) Prolonged compression of umbilical cord and
asphyxia

• During delivery a) Intracranial haemorrhage- compression
followed by decompression during delivery of the unmoulded after-coming head results in tear of the tentorium cerebelli and haemorrhage in subarachnoid space.
b) Asphyxia due to:-cord compression-Retraction of placental site-premature attempt at respiration while head is
still inside- Delayed delivery of the head- - cord prolapse

c)Injuries:- Hematoma on sternomastoid or on thighs- Fractures- Visceral injuries- rupture of liver, kidneys,
suprarenal glands, lungs- Nerve- medullary coning, spinal cord
injury, Erb’s or Klumpke’s palsy due to stretching of the brachial plexus

Thank you!!