Embed Size (px)
Citation preview

i
Title
They didn’t ask the question … An inquiry into the learning experiences of
students with spina bifida and hydrocephalus
Name
Barbara Rissman, MEd, BEd (AWE), ATCL (Tchr), AMusA, AYMF (Pforte),
AYMF (ElOrgan)
Centre
Centre for Learning Innovation
Academic qualification for which thesis is submitted
Doctor of Philosophy
Year submitted
2006

ii
ABSTRACT
They didn’t ask the question … An inquiry into the learning experiences of
students with hydrocephalus related to spina bifida
The researcher has a daughter who was born with an encephalocele and her
neuropsychological assessment indicates a Nonverbal Learning Disability (NLD). The
difficulties of the educational experiences that emerged over time, mainly because her
learning profile was not understood, prompted reflection on the consequences for other
students who present with this profile. A concern for the long-term implications for students
and parents of the frequent misunderstandings of the NLD has inspired this study.
A review of the literature suggested a need to raise educator awareness about the subtle
but disabling nature of the NLD syndrome. This study explored the perceptions of teachers,
teacher aides and parents involved with 5 students who showed hallmark signs of an NLD.
The theoretical foundation rests in the understanding that a student’s learning experiences
are influenced by past and present school experiences, the attitudes of peers, and parental
expectations.
The purpose of this thesis is to help parents, teachers and others appreciate the school
experiences of children at Level 1 risk of developing an NLD, those with a hydrocephalic
condition. It does not purport to offer ultimate solutions or to contribute to diagnosis but
rather to act as a starting point for a body of theory to guide development of suitable learning
environments for such children. Of further importance is emphasis on the need for similar
studies to be conducted into the learning experiences of other children who demonstrate
specific syndromes or mosaic forms of those syndromes.
Naturalistic Inquiry methodology was used to explore the educational experiences of
five students who attended different Australian schools. After completion of all interviews,
psychological testing assessed general intelligence and the NLD status of each student. All
students were found to be severely learning disabled and all were high on the NLD
parameter. Educators generally did not reveal understanding of the NLD syndrome
“Nonverbal, what is it? So is it a visual …” Some teachers devised innovative strategies to
help the student cope in class while others expressed frustration … if the traditional
instruction “doesn’t work either, what does?” What stood out was an absence of
understanding about nonverbal deficits. Frustration about poor organisation, decision-

iii
making, task completion and problem-solving was expressed and a mixture of concern and
criticism was levelled at social incompetence. Students who could not work independently
were perceived by some teachers and aides as “lazy” or “molly-coddled” and problems with
everyday living skills were sometimes blamed on the student’s family.
Findings revealed a compelling need to raise educator awareness about the range of
cognitive, learning and social problems associated with shunted hydrocephalus and spina
bifida. They also highlighted a need for teachers to question “Why can’t this student do
things one would expect they could do” and demand answers that explicate the serious
difficulties being experienced.
Educate teachers, aides, school psychologists
= detection
= assessment
= know what they’re dealing with

iv
Key words
Nonverbal Learning Disability, NLD, NLD profile, spina bifida, hydrocephalus, shunted
hydrocephalus, teacher, aide, parent, student, educator, Education Queensland, Acquired
Brain Injury, ABI, assets, deficits, strengths, weaknesses, perception, phenotype,
psychological, psychometric, assessment.

v
STATEMENT OF ORIGINAL AUTHORSHIP
The work contained in this thesis has not been previously submitted to meet
requirements for an award at this or any other higher education institution. To the best of my
knowledge and belief, the thesis contains no material previously published or written by
another person except where due reference is made.
Signature _________________________________________
Date __________________________
vi
ACKNOWLEDGEMENTS
This thesis is dedicated to the courageous children who have sometimes suffered in
silence when their longing to fit in and keep up at school, and their desire to please and to
achieve, were misunderstood. I acknowledge the plight of parents and carers whose
advocacy, fears and heartfelt desires to help their child achieve independent life skills within
a realistic framework was not always recognised by educators.
I want to thank my beautiful daughter for her constant concern for me over the past 42
months. It was her journey through mainstream school that inspired this project. Her
wrestle with her own unrealised dreams and her ongoing adjustment to the reality of life
today makes her stoic and gutsy in my eyes.
Thank you to my brother John who has always encouraged me and believed that I could
illuminate the learning struggles of children with shunted hydrocephalus and spina bifida and
the pain that students and families can experience during the long school experience.
Thank you to a special neuropsychologist called Maggie who always found time to
discuss and offer advice to me about the world of neuropsychological testing.
Last and by no means least, it is my two supervisors John and Michael to whom I feel
indebted. Their patience and encouragement have seen me to completion and their big-
picture thinking and academic knowledge and experience have helped to clarify my thinking
many times. I am privileged to have had the opportunity to work with these two highly
respected academics. John and Michael are fine exemplars of human understanding.

vii
LIST OF TABLES
Table 4.1. Coding System 78
Table 4.2. Test Battery 85
Table 4.3. Criteria for NLD Phenotype 95
Table 4.4. Algorithm: NLD Profile Score 96
Table 4.5. Diagnosis of NLD Profile 97
Table 4.6. Summary of Functional Profile 98
Table 4.7. Spiralling cycle of deficiency 268
viii
LIST OF FIGURES
Figure A1. Neural tube closure 303
Figure A2. The normal bony spine 304
Figure A3. Spina bifida occulta 305
Figure A4. Normal spine, meningocele, myelomeningocele 306
Figure A5. Myelomeningocele 306
Figure A6. Encephalocele 308
Figure A7. Encephalocele 308
Figure A8. Lipomyelomeningocele 308
Figure A9. The Holter shunting system 309
Figure A10. Shunt system to the abdominal cavity 310
Figure A11. Neuron and Myelin sheath 313

ix
LIST OF ABBREVIATIONS
ABAS Adaptive Behaviour Assessment System
ABI Acquired Brain Injury
ADHD Attention Deficit Hyperactivity Disorder
ASBHA Australian Spina Bifida and Hydrocephalus Association
BRIEF Behaviour Rating Inventory of Executive Function
CELF Clinical Evaluation of Language Fundamentals
CPS Cocktail Party Syndrome
EF Executive Function
FSIQ Full Scale Intelligence Quotient
HPE Health and Physical Education
IEP Individual Education Plan
IQ Intelligence Quotient
JLO Judgment of Line Orientation
NLD Nonverbal Learning Disability
OT Occupational Therapist
PI Physical Impairment
PIQ Performance Intelligence Quotient
SBHQ Spina Bifida and Hydrocephalus Queensland
SEC Special Education Class
SEU Special Education Unit
SOSE Studies of Society and Environment
TOPS-R Test of Problem Solving - Revised
VIQ Verbal Intelligence Quotient
VMI Visual-Motor Integration
V-P Verbal-Performance
WCST Wisconsin Card Sorting Test
WIAT Wechsler Individual Achievement Test
WISC Wechsler Intelligence Scales for Children

x
TABLE OF CONTENTS
ABSTRACT ii
KEY WORDS iv
DECLARATION v
ACKNOWLEDGEMENTS vi
LIST OF TABLES vii
LIST OF FIGURES viii
LIST OF ABBREVIATIONS ix
TABLE OF CONTENTS x
Researcher Background 1
1. Overview of study
Current research: NLD associated with hydrocephalus and spina bifida 4
Research problem 5
Purpose of study 7
Application of findings to other groups 8
Purposeful selection 9
Methodology 9
Member checks 9
Data analysis 10
Case study reporting and audit 10
Research Question 10
2. Literature Review I
Nonverbal Learning Disability 11
Part 1
Common NLD characteristics 12 What is NLD? 13
NLD assets and deficits 14
Problems common to mathematics and social functioning 18
Relationship of NLD to other disabilities 18
Clinical incidence of NLD 19
What causes NLD? 20
Explaining the title “Nonverbal Learning Disability” 21
Summary 22
Part 11
How hydrocephalus is linked to an NLD 22
Summary 24

xi
3. Literature Review II
NLD characteristics in individuals with Hydrocephalus and Spina Bifida 25
Verbal learning and memory 25 Tactile perception 26
Motor and psychomotor functioning 26
Visual perception 28
Visual-motor perception 28
Visual-spatial perception 29
Executive Function 29
Language 31
Language and Distractibility 31
Academic skills 33
Adaptive Behaviour 34
Summary 35
Research Question 37
Implications for this research 37
4. Methodology
Part 1 Theoretical underpinnings 39
Philosophical position towards reality 40
Recruitment process 40
Purposeful recruitment strategy 41
Final subgroup 41
Naturalistic Inquiry: Strengths and Weaknesses 42
Axioms that underpin Naturalistic Inquiry 43
Significance of context 45
Trustworthiness 45
The human data collection instrument 48
Preferable human-as-instrument qualities 49
Summary 50
Data collection 50
Interviewing 51
Listening skills 51
Observation 52
Nonverbal communication 52
Interview questions 52
Interview Guide 53
Note-taking 53
Tape-recording 53
Member checks 54
Data Analysis 54
Data Interpretation 54
Grounded theory 55
Case Study mode 55
Thick description 56
Audit process 56
Part 11
Method 58
Qualitative problem 58
Research Question 58
Determining selection site 59

xii
Primary participant selection 59
Participant selection 60
Data Collection 61
Human data collector 62
Gaining consent from parents and students 63
Setting up teacher and teacher aide interviews 63
Consent mechanism 64
Building rapport 64
Building rapport with students 65
Shared interests and reciprocity 66
Tape recording 66
Starting parent and teacher interviews 67
Listening skills 67
Self-introduction for teacher and teacher aide interviews 67
Self-introduction for parent interviews 68
Interviewing students 68
Starting student interviews 69
Self-introduction for student interviews 69
Listening to students 69
Observation 69
Nonverbal communication 70
Noting techniques 70
Interview Process Phase 1 70
Phase 1 open-ended questions 71
Phase 2 Interview Guide 71
Phase 2 Interview Guide questions for parents 72
Phase 2 Interview Guide questions for students 74
Phase 2 Interview Guide questions for teachers and teacher aides 75
Closing the interviews 76
Transcribing interviews 77
Member Checks 77
Coding System 77
Table 4.1 Coding 78
Analysis of qualitative data 79
Stage 1 Unitising 79
Stage 2 Categorising Units of Information 80
Stage 3 Indexing 81
Triangulating data 81
Interpreting content 81
Reflexivity and bias 82
Psychometric testing 83
Administration of test measures 84
Table 4.2 Test Battery 85
Description of test instruments 86
General intelligence assessment 86
Supplementary tests 87
Understanding V-P discrepancy 93
Diagnosing the NLD profile 94
Table 4.3 Criteria for NLD phenotype 95
Table 4.4 Algorithm: NLD Profile score 96
Table 4.5 Diagnosis of NLD Profile 97
Diagnosis of Executive Function (EF) Profile 98
Table 4.6 Summary of Functional Profile 98

xiii
Case Study Reports 99
Writing the Report 99
Audit Trail 100
5. Case Study reports
Personal interest in case studies 101
Recruitment 103
Data Collection 103
Data Analysis 103
Interpretation and reporting 104
Jenny’s Case Study 106
Context of Jenny 106
A day in the life of Jenny 108
Jenny at school 111
Teacher and Aide perceptions of Jenny as a person with a disability 115
Summary of 2005 Psychological and Speech Assessments 116
Interpretative discussion 117
Conclusion 118
Ryan’s Case Study 120
Context of Ryan 120
A day in the life of Ryan 123
Ryan at School 128
Teacher and aide perceptions of Ryan as a person with a disability 137
Summary of 2005 Psychological and Speech Assessments 139
Interpretative discussion 139
Conclusion 142
Clair’s Case Study 144
Context of Clair 144
A day in the life of Clair 146
Clair at School 149
Teacher and aide perceptions of Clair as a person with a disability 160
Summary of 2005 Psychological and Speech Assessments 162
Interpretative discussion 162
Conclusion 166
Mel’s Case Study 168
Context of Mel 168
A day in the life of Mel 171
Mel at School 176
Teacher and aide perceptions of Mel as a person with a disability 187
Summary of 2005 Psychological and Speech Assessments 191
Interpretative discussion 192
Conclusion 197
Josie’s Case Study 199
Context of Josie 199
A day in the life of Josie 204
Josie at School 209
Teacher and aide perceptions of Josie as a person with a disability 223
Summary of 2004 Neuropsychological Assessment and
2005 Psychological and Speech Assessments 227
Interpretative discussion 228
Conclusion 234

xiv
Cross Case Analysis: Synopses 235
Jenny 235
Ryan 236
Clair 238
Mel 239
Josie 241
Cross Case Analysis 242
Perceptions of NLD assets 243
Perceptions of NLD deficits 245
Academic deficits 247
How did Education Queensland, teachers, aides and peers perceive students? 258
Summary 264
Personal understanding of how impaired nonverbal skills lead to maladaptive
social skills? 265
Table 4.7 Spiralling Cycle of Deficiency 268
6. Summary of study and conclusions
Problem 269
Methodology 269
Credibility of findings 270
Limitations of study 270
Findings 271
How teachers and aides understood learning difficulties? 273
Did teachers, aides, parents and students know about a
Nonverbal Learning Disability? 275
Recommendations resulting from the study 275
To help students 275
Parental help for students 278
Restatement of what is important 278
Recommendations for education systems 279
Conclusion 280
Future research 284
Reference List 285
Appendix A
Chapter Two Part 11: NLD associated with shunted hydrocephalus and
spina bifida 300
Figure A1: Neural tube closure 303
Figure A2: The normal bony spine 304
Figure A3: Spina Bifida Occulta 305
Figure A4: Normal spina, Meningocele, Myelomeningocele 306
Figure A5: Meningocele 306
Figure A6: Encephalocele 308
Figure A7: Encephalocele 308
Figure A8: Lipomyelomeningocele 308
Figure A9: The Holter shunting system 309
Figure A10: Shunt system to the abdominal cavity 310
Figure A11: Neuron and myelin sheath 313
Summary 314

xv
Appendix B
Study summaries
Intelligence and achievement in children with myelomeningocele (Wills, Holmbeck & McLone, 1990) 315
Early hydrocephalus
(Fletcher, Brookshire, Bohan & Timothy, 1995) 316
The Intelligence of hydrocephalic children
(Dennis, Fitz, Netley, Sugar, Harwood-Hash, Hendrick, Hoffman,
& Humphreys, 1981) 319
Cognitive functioning in patients with spina bifida, hydrocephalus
and the “Cocktail Party Syndrome”
(Hurley, Dorman, Bell & D’Avignon, 1990) 320
Distractibility and vocabulary deficits in children with spina
bifida and hydrocephalus
(Horn, Lorch, Lorch & Culatta 1985) 322
Cognitive and achievement status of children with myelomeningocele
(Shaffer, Friedrich, Shurtleff & Wolf, 1985) 324
The clinical and psychological characteristics of children with the
“Cocktail Party Syndrome”
(Tew & Laurence, 1979) 326
Neuropsychological and adaptive functioning in younger versus
older children shunted for early hydrocephalus
(Holler, Fennell, Crosson, Boggs, Mickle & Parker, 1995) 327
Syndrome of Nonverbal Learning disabilities: Age difference in
personality/behavioural functioning
(Rourke & Casey, 1989). 329
Appendix C
Background to verbal-performance discrepancies in individuals with
hydrocephalus and spina bifida 330
Verbal-performance discrepancies in previous studies 331
Appendix D
Definitions 334
Nonverbal Learning Disability 334
Executive Function Disorder 334
Mild Intellectual Impairment 335
Borderline Intellectual Functioning 335
Appendix E
Glossary 336

xvi
Appendix F
Students with NLD and inclusive education 342
Background 342
Benefits of inclusive education for all students 343
An ecological approach 344
Strategies for a student with an NLD 345
Selected hints from this study for other teachers and teacher aides 348
Appendix G
Information Packs 351
Letter of Introduction, Study Description and Consent forms (Parents) 351
Letter of Introduction, Study Description and Assent forms (Students) 357
Letter of Introduction, Study Description and Consent forms (Principals,
teachers and teacher aides) 363

1
Researcher background
The researcher is the mother of a young person born with a form of spina bifida called
an encephalocele. Early childhood years were plagued by shunt dysfunctions that each time
required urgent surgical intervention, seizures, repair of alternating strabismus (squints) and
constant vigilance to prevent a bump to the head. Progress was closely monitored by a team
of medical professionals which comprised a neurosurgeon, paediatrician, ophthalmologist,
physiotherapist and occupational therapist. Fletcher, Brookshire, Bohan and Timothy (1995)
empathise with this account when they say “parents of a child with hydrocephalus face a
lifetime of monitoring the child’s condition with recurrent concerns about possible relapse,
shunt dysfunction and the need for additional surgery” (p.210). As specialised care and daily
physical therapies were prescribed from an early age, the mother resumed the study of music
to gain qualifications and build a teaching practice from the home base. In retrospect, the
study and practice provided a cathartic outlet from the constant monitoring.
Impressive verbal skills at an early age created hopes, dreams and ambitions that were
kept alive by ongoing achievement in the early school years and sustained by strong
conviction that “if we work harder, she’ll catch up” in the maths and assignment tasks. Field
visual deficits were undetected until post school despite return visits to a specialist physician
to inquire about classroom difficulties. Repeated assurance that “her eyes are fine” because
she could read the smallest legible print in direct vision, difficulties with reading and
copying from the blackboard, crossing roads and frequent near-misses persisted. Clumsiness
and co-ordination problems were attributed to the primary problem at birth. As a child and
student, she was cooperative and eager to learn and with sufficient one-on-one support and
small-step instruction, she was able to complete tasks in the early school years. Reading and
speech were intelligible and articulate from a young age. Repetition was our ticket to
success and she thrived on sameness and predictability. Changes to routines, class outings,
school camps and new situations caused extreme anxiety, sometimes illness.
To extend cognitive, fine-motor, eye-hand and visual memory skills, the mother taught
her daughter piano and theory of music for a five-year period. Grades 1 and 2 Theory of
Music examinations (AMEB) involved much rote learning at which she excelled and
achieved “Honours” grades, 97/100 and 96/100. Despite the increased complexity of Grade
3 theory, well-practiced strategies and a formal extension of time helped her achieve 83/100.

2
A medical certificate to explain right-sided weakness was provided for three practical
examinations and for each an “Honours” grade was awarded. Several other developmental
activities were introduced over the years to fulfil mutually-shared dreams and complement
therapies and formal school.
With increasing age and year levels, as school demands became more complex and
required comprehension, integration of information, adaptability and problem solving skills,
age-appropriate expectations could not be realised. In retrospect, success with school and
music rote memory tasks created an impression of competence and fluent speech caused
misperception. Unrealistic parent and teacher expectations were coupled with increasing
difficulty in the social arena. A neuropsychological assessment at age 15 years indicated
NLD characteristics, a verbal intelligence quotient (VIQ) of 73 and a performance
intelligence quotient (PIQ) of 57 reflecting a 16-point discrepancy and a full-scale
intelligence quotient (FSIQ) of 62. Abandoning the dreams and accepting the reality was a
painful process.
The difficulties of the educational experiences that emerged over time for child and
parent, mainly because the learning profile was not understood, prompted much reflection on
the consequences for other students in the educational system at large who present with this
profile. The long-term implications for students and parents inspired this investigation into
teacher, teacher aide, parent and student perceptions. The personal dilemma, confusion and
disillusionment experienced are expected to enhance ability to explore the phenomena of
research interest. However, it could be equally argued that personal experience makes the
task of detached researcher more difficult. Although Lincoln and Guba (1985) say the
investigator who possesses a “great deal of tacit knowledge germane to the phenomenon”
being studied has a distinct advantage, the limiting effects to objectivity are here
acknowledged (p.209).
“What became Mum’s life became her passion”
Tony

3
CHAPTER ONE
Overview of study
This study explored how teachers, teacher aides, parents and students understood the
schooling experiences of 5 students with hydrocephalus and spina bifida who showed
characteristic signs of a Nonverbal Learning Disability (NLD). An NLD is a serious
developmental disability that has potential to influence the academic, social and emotional
aspects of a person’s life and threaten their ability to achieve economic and personal
independence. Synonymous with a developmental disability is a gap between perceived
competencies and a person’s real ability to function in the world which becomes wider and
more obvious with age. The cornerstone of thinking about a nonverbal learning disorder is
that individuals cannot be categorised but rather that each person’s unique blend of strengths
and weaknesses places them somewhere on a continuum of neurodevelopmental disorders.
Nonverbal Learning Disorders first came to the attention of researchers in the field of
neuropsychology in the early 1970s when they noticed that some children with learning
disabilities displayed significant discrepancies between verbal and performance intelligence
scores that differentiated them from other youngsters with learning disabilities (Myklebust,
1975). Investigative efforts by Rourke, Young and Flewelling (1971) and Rourke, Dietrich
and Young (1973) led to identification of the NLD syndrome and formulation of the current
working model. An NLD is believed to be caused by damage, disorder or destruction of
neuronal white matter in the brain’s right hemisphere and may be seen in persons suffering
from a wide range of neurological diseases such as hydrocephalus and other types of brain
injury (Harnadek & Rourke, 1994).
The pervasive nature of the NLD profile presents a dilemma for teachers because
functional difficulties present within a context of relatively better speech. Despite a well-
developed vocabulary, a student with an NLD has cognitive and functional limitations that
affect ability to interpret nonverbal communication, develop social competence, handle new
situations and acquire age-appropriate motor coordination, perceptual skills and higher-level
language skills. Dysfunctional reactions or behaviours may result in a student being branded
as “a problem”, “lazy” or “emotionally disturbed” (Tanguay, 2002).
Twenty-five years after research into the NLD syndrome began, Thompson (1997)
reported that educational professionals are largely uninformed or unfamiliar with its long-

4
lasting effects. Foss (1991) explored school records and parental anecdotal information of
adolescents with deficits in nonverbal aspects of learning which indicated “little
understanding of the nature of the difficulties” young people faced nor did they receive
appropriate instruction to address their areas of weakness (p.128). The majority of teacher
training programs “offer little, if any, training in the area of interventions for the student with
a Nonverbal Learning Disability” says Tanguay (2002, p.10).
This study purposely selected 5 students from a population that Rourke (1989) says
manifests the NLD syndrome most exactly – those with a hydrocephalic condition.
Hydrocephalus is a major complication of spina bifida, a neural tube defect that results from
failure of the spine to close properly. Today, ninety-five percent of individuals with spina
bifida have hydrocephalus that is treated with a shunting procedure and the quality of
surgical intervention has resulted in significantly increased rates of survival (Lutkenhoff &
Oppenheimer, 1997).
A review of the literature suggested a need to raise educator awareness about the subtle
but increasingly disabling nature of a Nonverbal Learning Disability. While abundant
literature and reports of teacher misunderstanding emanated from the United States and
Canada, there was no reason to assume the learning experiences of Australian children who
display the NLD profile were the same. This study probed allegations by Thompson (1997),
Roman (1998), Russell (2004) and Tanguay (2002) that educators are unfamiliar with the
NLD syndrome. It explored the perceptions of teachers, aides and parents involved with 5
students who shared aspects of the NLD profile, the aim being to engage contributors to the
whole context of the child’s life (Parlett & Hamilton, 1972). The theoretical foundation rests
in the understanding that a student’s learning experiences are influenced by past and present
school experiences, the attitudes of peers and parental expectations.
Current research: NLD associated with hydrocephalus and spina bifida
This introductory section highlights studies that have investigated the prevalence of
NLD in populations with hydrocephalus and spina bifida. Holler, Fennell, Crosson, Boggs,
and Parker (1995) used a sample of 28 children with shunted early-onset hydrocephalus and
spina bifida to administer tests to assess neuropsychological and adaptive functioning in
younger versus older children. Results indicated that children with shunted hydrocephalus
“may be conceptualised as exhibiting the NLD syndrome” (p.63). A final sample of 145
children aged 5-14 years with hydrocephalus and related medical conditions was recruited by

5
Fletcher et al. (1995) to address neurobehavioral characteristics of hydrocephalus in relation
to NLD. Findings revealed that “hydrocephalus per se is clearly associated with significant
deficiencies in a variety of nonverbal skills including motor, perceptual-motor and visual-
spatial skills”. Some aspects of language were found to be intact while language at the level
of discourse was problematic (p.211-212). Lindsay (1997) recruited a sample of 38 adults
with spina bifida in 1997 to investigate whether Rourke’s NLD model applied to subjects in
adulthood. Administration of a battery of intelligence, neuropsychological and self-report
tests revealed that the spina bifida group as a whole did meet the criteria for NLD. Eleven
subjects who had shunted hydrocephalus related to spina bifida were assessed by Hommet,
Billard, Gillet, Barthez, Lourmiere, Santini et al. (1999) to determine whether the NLD
syndrome described in children with hydrocephalus was observed in adulthood.
Neuropsychological performance revealed that the group with shunted hydrocephalus related
to spina bifida was more affected by the “extensive and longer-lasting Nonverbal Learning
Disabilities syndrome” (p.149).
A search of current journal articles did not reveal any investigation into how teachers,
aides and parents perceive a child who presents with the NLD phenotype. An Australian
study by Backhouse and Rodger (1999) explored parent and student perceptions of the
transition from school to employment for young people with an Acquired Brain Injury
(ABI). Individuals in this population may display traits of the NLD profile. Findings
revealed that individuals with ABI were generally not well understood and consequently
their needs were not met. Parents also reported high levels of stress in relation to schooling
and future employment.
Research problem
In the Western world today, most scholastic accomplishments are measured and defined
through language-based communication. Nonverbal learning disorders routinely go
unrecognised because parents and educators consider language-based skills an indication of
ability to learn (Thompson, 1997). Students who do well at reading, spelling and oral
presentations may be considered more academically and socially capable than they are. A
well-developed vocabulary coupled with the appearance of competence may present a “false
illusion of giftedness” which makes it difficult for school personnel to appreciate the
debilitating nature of an NLD (Tanguay, 2002, p.26). What is not obvious is that the child
copes by relying almost exclusively on language, therefore vocabulary is disproportionately
developed (Tanguay, 2002). Excessive speech may be largely free of content with pragmatic
aspects almost at a simplistic level (Rourke, 1989). Despite apparent facility with language,

6
a student who falls somewhere on the NLD continuum experiences many functional
limitations. When tasks require focused attention, superficial communication can mask
functional difficulties and fuel teacher misunderstanding when expectations are not reached.
A favourable prognosis for the student with NLD depends on early identification and
intervention if serious functional and long-term adjustment problems are to be minimised
(Rourke, Fisk & Strang, 1986). According to Rourke (1989), the NLD syndrome in addition
to other biological, sociocultural and interpersonal components “appears to predispose those
so afflicted to suicide risk” (p.149), a situation that is intensified by teacher and peer
misunderstanding over the prolonged school experience. Strong auditory memory skills
which allow negative remarks to be stored verbatim may add to depressive episodes. Levine
(1994) says the immediate short-term effects of repeated “failure and exasperation” through
school may be minimal “compared to the durable impacts” of misinterpretation (p.272).
Despite notable publications and journal articles by American authors and pre-eminent
researcher in the field, Byron Rourke, Roman (1998) and Russell (2004) claim the NLD
syndrome is unfamiliar to many educators, psychologists, therapists and other professionals.
Possible explanations are that few text books used in teacher preparation courses mention the
syndrome which limits exposure to its characteristics (Telzrow & Bonar, 2002). Much NLD
literature is also found in Neuropsychology, Child Psychiatry, Developmental Medicine and
Child Neurology journals not routinely accessed by educators.
Lack of training in the area of intervention and ignorance about the profile may cause
teachers to impose the same expectations established for all students on a child with an NLD.
Whitney (2002) says most teachers in the United States are trained to believe behavioural
problems are emotionally based therefore every piece of evidence gathered on a particular
student is skewed by misperception “their intentions were good, but their particular frames
of reference narrowed their focus and limited their field of vision” (p.6). Some teachers
were reported to say “it’s not neurological, it’s just spoiled behaviour” or “I’ve never heard
of NLD. It’s just one more thing parents have come up with to excuse the child who won’t
do the work” (p.220).
Intelligence measures evaluate verbal and nonverbal aspects of intelligence yet
Thompson (1997) claims many educators ignore evidence of nonverbal deficiencies. If
labelled “uncooperative”, a student with an NLD will believe it even though he or she is
working ten times harder than peers to achieve much less (Thompson, 1997). Contra wise, a
student who is verbally fluent and achieves excellent spelling and tables scores does not

7
prompt the teacher to consider a learning disorder. Rourke (1995) believes such children are
rarely involved in educational programs that address their special learning needs hence an
acute need to identify students and prevent generalised feelings of despair resulting from
overestimates of ability (Thompson, 1997). Thompson says paediatricians, teachers and
special educational professionals should take time to listen to parental concerns which may
indicate an NLD. If treatment is not introduced fairly early “on all appropriate academic and
behavioural fronts”, the prognosis tends to be “quite bleak” (Rourke, van der Vlugt &
Rourke 2002, p.236).
This study initially selected individuals whose parents perceived had good verbal skills
but who experienced trouble with mathematics and handwriting. A telephone interview was
conducted with each parent and current psychological assessments were requested to aid
identification of the final subgroup. Informal interviews with teachers, aides, parents and
students then explored how they generally perceived the educational experiences of students.
At the conclusion of all interviewing, a psychological test battery or supplementary tests
were administered to participating students.
Purpose of Study
The purpose of this thesis was to assist parents, teachers and others to appreciate the
learning and schooling experiences of children with hydrocephalus and spina bifida. It did
not purport to offer solutions or to contribute to diagnosis but rather to act as a starting point
for the development of a body of theory to guide further development of appropriate learning
environments for such children. A further importance of this study is emphasis on the need
for similar studies to be conducted into the learning experiences of other children who may
demonstrate specific syndromes or mosaic forms of those syndromes.
The intention was to gather multiple perspectives from stakeholders on the educational
experiences of 5 young people with shunted hydrocephalus and spina bifida who displayed
NLD characteristics. It sought to fill a void in the literature by investigating allegations that
educators are unfamiliar with this learning disability. In the context of five Queensland
schools and families, this study “gave voice” to forty-three teachers, aides, students and
parents or caregivers.
Families were expected to offer history of educational experiences and how they
believed young people were perceived at school. Since nonverbal deficits become more

8
noticeable with age, it was thought a greater emphasis on life skills, friendships and social
isolation may emerge from older students. The project sought to probe understanding of
impaired ability to perform many daily tasks which teachers, aides, parents, even physicians,
are at a loss to explain.
The ultimate goal is to increase understanding with intent for that increase to “be
noticeable to a variety of audiences” (Lincoln & Guba, 1985, p.225), educators,
psychologists and school counsellors so that early identification and intervention can
generate appropriate expectations before educational and social difficulties lead to anxiety or
worse. As a consequence, the significance of verbal and nonverbal abilities for academic,
social and emotional functioning will gain ascendancy in the minds of professionals and
parents. A confirmed learning need for educators may stimulate inclusion of NLD
information in teacher training programs. As well, findings have relevance to other groups
whose neurological ailments cause NLD characteristics (Molenaar-Klumper, 2002).
Application of findings to other groups
Children with NLD have characteristics in common with individuals with Asperger’s
Syndrome. Molenaar-Klumper (2002) quotes Paternotte (2000) as saying 9 out of 10
children with NLD have Asperger’s Syndrome though “the opposite does not seem to apply”
(p.67). A majority of children with acute Leukaemia and Foetal Alcohol Syndrome show
many traits of NLD and Multiple Sclerosis is a disability that results in some traits of NLD
(Molenaar-Klumper, 2002). Some NLD assets and deficits are mirrored in individuals with
an Acquired Brain Injury (ABI). In 1998, the Brain Injury Association of Queensland said
63 400 Queenslanders reported a disability from an ABI that interfered with areas of
schooling, employment, communication, mobility and self care. Individuals with shunted
hydrocephalus and spina bifida may be subsumed under the ABI rubric due to damage
sustained post-birth from shunt malfunction, infection and/or a seizure condition. Subject to
the area of damage, commonalities between persons with an ABI and those with spina bifida
and hydrocephalus may involve memory, concentration and retention skills, sensory, motor,
perceptual, visuospatial, executive functioning, language and communication, social,
behavioural and emotional abilities (Brain Injury Association of Queensland, 2006).

9
Purposeful selection
Certain individuals were recruited because they possessed similar traits or
characteristics, referred to in this context as a homogeneous subgroup (Cresswell, 2002).
The researcher identified certain characteristics then found individuals who possessed them.
A primary group of students aged 9-16 years with shunted hydrocephalus and spina bifida
was recruited through Spina Bifida and Hydrocephalus Queensland, the Mater Hospital
Spina Bifida Clinic and the Royal Children’s Hospital Spina Bifida Clinic. A process of
continuous refinement focused more and more sharply on salient NLD characteristics until
the final homogeneous subgroup was identified.
Methodology
This qualitative study used naturalistic inquiry methodology to explore the educational
experiences of children with shunted hydrocephalus and spina bifida. An inquiry into
perceptions demanded an approach that emphasised adaptability, open-endedness and
flexibility, one that allowed the unexpected to expand the inquiry’s scope by catering for the
multiple realities presented by informants. Two phases of informal conversational
interviews explored perceptions. Phase 1 used open-ended questions to survey the
“territory”. Phase 2 followed-up significant issues and a semi-structured interview guide
delved particular areas of research interest.
On completion of interviews, a psychological test battery determined the NLD status of
each student. Test results added to the richness of case study descriptions and provided a
contextual background for case study reports. This sequence allowed exploration of
perceptions without influence of researcher bias, prejudice or predetermined views derived
from test findings.
Member checks
Member checks involved sending a verbatim transcript of each interview to the
individual for them to confirm, correct or extend. On-site engagement, contextual
observation, supervisor collaboration and debriefing, a reflexive journal and strategies to
address subjectivity and bias were used to strengthen credibility of findings.

10
Data analysis
During analysis, a constructivist-perceptual view of reality was adopted because it
acknowledged that multiple realities reside in the human mind, all capable of different
interpretation from other vantage points. Phase 1 and Phase 2 content were analysed and
units of information were identified. Each unit was the smallest piece of stand-alone
information that led to new understanding. Through constant comparison, units were
assembled under categories derived from open-ended questioning and topic headings in the
interview guide to form a provisional category set. Review of provisional category headings
involved supervisor collaboration to formulate a logically sequential case study framework.
To generate trustworthiness and confidence in findings, data were triangulated by teacher,
aide parent and/or student perceptions to ensure multiple realities were reported in each case
study. Inquiry content was interpreted in terms of the inquiry’s basic axioms and in the
context of psychometric test data.
Case study reporting and audit
To explore the intricacies within each bounded system, case study reporting focused on
the individual complexity of each case rather than a population of cases (Burns, 2000).
Cross-case analysis moved to a higher level of abstraction by cutting across case studies in
search of similar and divergent views. Finally, examination of the audit trail established that
all checks and balances were carried out in ways that fell “within the bounds of good
professional practice” and findings were consistent with raw data (Lincoln & Guba, 1985,
p.109).
The following research question was developed to address the primary objective of this
study:
Research question
How do teachers, teacher aides, parents and students perceive the educational experiences of
5 students with shunted hydrocephalus and spina bifida?

11
CHAPTER TWO
LITERATURE REVIEW 1
Nonverbal Learning Disability
A Nonverbal Learning Disability (NLD) is a silent, complex and serious problem and
“management can only be effective if based on a thorough understanding of the disorder”
(McDowell, 2003). The NLD syndrome is manifested most clearly on a developmental basis
(Harnadek & Rourke, 1994). This means that characteristics are seen in terms of a child
afflicted since his or her earliest developmental stages rather than a child whose early
months and years of cognitive development were normal until a neurological disease or
damage was “superimposed upon a normally developing brain” (Rourke, 1989, p.86). In a
majority of cases, children with a developmental disability do not grow out of it because the
damage or destruction sustained cannot be cured (McDowell, 2001). Dysfunctions
associated with the NLD syndrome are less apparent at 7-8 years of age than at 10-14 years
and become more obvious and “debilitating as adulthood approaches” (Rourke, 1989, p.117),
as Thompson says “a child grows into NLD” (1997, p.19).
Rourke et al. (2002) report that individuals at Level 1 risk of manifesting virtually all of
the NLD assets and deficits are those with:
1. Hydrocephalus (early, shunted) (Fletcher et al., 1995; Fletcher, Francis,
Thompson, Brookshire, Bohan, Landry et al. 1992; Rourke, Bakker, Fisk &
Strang, 1983)
2. Aspergers Syndrome (Rourke & Tsatsanis, 2000)
3. Williams Syndrome (Anderson & Rourke, 1995)
4. De Lange Syndrome (Tsatsanis & Rourke, 1995b)
5. Turner Syndrome (45, X) (Rovet, 1995b)
6. Callosal Agenesis (uncomplicated) (Smith & Rourke, 1987)
7. Velocardiofacial Syndrome (Fuerst, Dool, & Rourke, 1995)
8. Significant damage or dysfunction of the Right Cerebral Hemisphere (Rourke,
Bakker, Fisk & Strang, 1983)
This research focused on students with a hydrocephalic condition treated by early
shunting. After examining the psychosocial, neuropsychological and neuropathological
characteristics of children with hydrocephalus, Fletcher et al. (1995) found that

12
“hydrocephalus represents a prototypical NLD disorder”. Further, it is one of the “only
disorders identified at Level 1 for which the neurobehavioral characteristics have been
thoroughly investigated” (p.232-233). In children under two years, hydrocephalus presents
in association with a congenital central nervous system (CNS) deficit such as spina bifida.
In this event, hydrocephalus is secondary to a structural malformation (Fletcher & Levin
1988) and it is a major complication in 95% of spina bifida cases. In most cases today, the
hydrocephalic condition is treated with a shunt mechanism to prevent the condition
becoming worse. The following literature reviews are presented as Part Ι and a Summary of
Part II. The medical nature of Part II literature review has determined its placement in
Appendix A.
Part I
The following review discusses common NLD characteristics, the NLD syndrome,
NLD assets and deficits, problems common to mathematics and social functioning,
relationship of NLD to other developmental disabilities, what causes an NLD and an
explanation of the title “Nonverbal Learning Disability”.
Common NLD characteristics
Common characteristics of the NLD syndrome include good rote memory, reading and
spelling skills, fluent speech, a wide-ranging vocabulary, poor gross and fine motor, visual
memory and recall skills, spatial perceptions and spatial relations, understanding of
nonverbal communication, adjustment to new situations and significant trouble with social
judgment and interaction (Thompson, 1997).
Researchers estimate that 65-93% of all communication is nonverbal. According to
Whitney (2002), 55% of the emotional meaning of a message is expressed in nonverbal cues
such as facial expression, posture and gesture, 38% is transmitted through tone of voice, and
only 7% of the emotional meaning of a message is expressed in the words we speak. For a
person with NLD who attends to words only, up to 93% of the emotional meaning may be
missed. The long-term effects on socioemotional functioning of such a disability should not
be underestimated and if not addressed with early intervention, will lead to significant
impairment. Socioemotional ineptness refers to deficits in social judgment, visual-spatial-
organisational skills needed to recognise faces, expressions of emotion and variations in tone
of voice, tactile-perceptual and psychomotor skills required for smooth affectionate
encounters, and adaptability to novel interpersonal situations (Rourke, 1989).

13
When investigating socioemotional functioning in a group of children with language
deficiency and a group who exhibited the NLD profile of assets and deficits, Rourke and
associates (1989) found that children who demonstrated NLD characteristics were at higher
risk of developing some sort of socioemotional disturbance than the language deficient
children, but that is not to imply that “the language deficient children will never experience
socioemotional disturbance” (p.55). They claim there is something in addition to a language
deficiency that causes disturbed socioemotional functioning to occur. Additional factors
may include teacher-pupil personality conflicts, unrealistic demands by parents and teachers
and inappropriate social expectancies (Rourke, 1989). When such difficulties are coupled
with trouble interpreting up to 93% of emotional meaning from social interaction, they have
potential to encourage “problems in the socioemotional functioning of even normally
achieving children” (p.56).
What is an NLD?
The possibility of an NLD was first described by Myklebust in 1968 as deficits in the
concept of right-left, direction, time, size, speed, distance, height, and ability to interpret the
meaning of human behaviour. Rourke (1989) called this constellation of symptoms a
Nonverbal Learning Disability (NLD) and proposed a model for its aetiology, neurological
bases and developmental course that would later be named the “White Matter Model”. He
believed this model would account for a consistent pattern of deficits observed in children
with a history of early generalised cerebral dysfunction while acknowledging that other
neurodevelopmental disorders might share some but not all NLD characteristics. The NLD
syndrome has been described as a breakdown in ability to process information due to lack of
mental coordination (Molenaar-Klumper, 2002). Rourke (1989) describes it as the non-
cooperation of neuropsychological, academic, socioemotional, and adaptive functions.
Children with nonverbal learning disabilities are often described as poorly coordinated
in fine and gross motor skills and as adults may be extremely awkward and disorganised in
physical activities. Because they experience great difficulty adapting to new vocational,
personal or social situations, Rourke (1989) suggests the evidence is strongest for a
disturbance in the right hemisphere. Obrzut and Hynd (1991) explain that a direct result of
these deficits and the poor social perception of students with NLD may limit the student’s
resulting inner experience with consequential effects on reasoning and adaptive behaviour.
Much of the child’s prelanguage learning of environmental sounds, visual-motor
patterns, relations and rhythms done through visual and auditory perceptions is
“disproportionately stored and processed in the right hemisphere” in early life say Obrzut

14
and Hynd (1991, p.605). Between 18-23 months of age, the right hemisphere develops faster
than the left, reflecting greater right hemisphere involvement during this period (Semrud-
Clikeman & Hynd, 1990). It is reasonable to expect that students who cannot recognise,
interpret, evaluate and integrate speech intonation, facial expressions, and experiences from
visual and auditory stimuli will be at greater risk of developing deficits in social competence.
For an individual whose nonverbal abilities are in the average or above range but who has
limited verbal abilities, “the capacity to take responsibility for oneself in society remains at a
high level” says Myklebust (1978, p.96). But for the student with NLD, reduced ability to
integrate the nonverbal aspects of life will result in impaired perception and imagery which
distorts the total life experience.
NLD assets and deficits
Primary assets include simple repetitive motor skills, auditory perception and mastery
of rote material especially through the auditory modality, but not confined to it. Primary
deficits include visual, spatial and tactile perception, arithmetic deficits, complex
psychomotor skills and difficulty dealing with novel and complex tasks and information
(Rourke, 1995).
Assets
1. Simple repetitive motor skills. Repetitious simple-motor tasks are generally
intact especially at older age levels (middle childhood and beyond) although
handwriting may remain a slow arduous task for some (Fletcher et al., 1995;
Rourke, 1989).
2. Auditory perception. Delayed speech development in some individuals with
NLD during the first months and years may raise concern about the integrity of
the auditory system but once speech and language development begins, it
seems to develop at an above-average rate (Rourke, 1989). On the other hand,
some children with NLD may speak at a very young age, even before one
(Whitney, 2002, p.21). Capacity to deal with information presented through the
auditory modality becomes a primary asset and provides a “basic strength from
which all other assets flow” (Rourke, 1989, p.87). For a child with NLD, the
capacity to hear is far better developed than the capacity to see or feel
(Molenaar-Kulmper, 2002). Well-developed capacities for auditory perception,
attention and memory lead to “good-to-excellent verbal reception, verbal
repetition, verbal storage” and word-recognition skills (Rourke, 1989, p.93).
Good attention to auditory and verbal stimuli promotes advanced auditory and
verbal memory, accurate pronunciation and fluent verbatim repetition of what
is heard. Children with an NLD prefer to use good auditory perception to

15
explore through listening and asking questions rather than through looking,
moving and manipulating which limits environmental awareness and impairs
spatial relations, concept formation, problem solving and mathematical
abilities.
3. Mastery of rote material. The child with NLD confidently handles repetition of
material received through the auditory modality and has good use of routine
and already memorised information (Whitney, 2002). A characteristic feature
of children with an NLD is their well-developed rote verbal capacities and this
ability to memorise words results in a large vocabulary at a young age. Verbal
output may be verbose and of a repetitive straightforward nature and it may
lack content with the main point often omitted.
Deficits
4. Tactile perception brings incoming signals through the skin of both hands
which Goldstein (1997) believes is a great deficit experienced by students with
an NLD. Inability to understand and profit from information perceived from
the sense of touch impairs performance of everyday tasks. Persons with an
NLD may exhibit bilateral tactile perceptual deficits, often more marked on the
left side of the body. Simple tactile imperception may improve with age
whereas complex tactile imperception tends to persist (Rourke et al., 2002).
Tactile sensitivity is basically undervalued in most interventions to aid
adolescent and adult psychosocial competencies in favour of emphasis on
linguistic competencies (Rourke, 1989). Adult interactions of the intimate
variety require “smooth, coordinated, integrated sensorimotor functioning” and
spontaneous adaptive transitions to meet quickly changing social situations
(Rourke, 1989, p.143). Such interactions not only involve intact sensorimotor
functions but interpretation of nonverbal behaviours. Individuals with NLD
may have great difficulty deploying such behaviours which may cause them to
be viewed as “misfits”, a situation which increases the chance of social
isolation, withdrawal and depression (p.143).
5. Visual perception is the ability to recognise and understand what is seen.
According to physician, L. Kleinschmidt (personal communication July 7,
2001), incoming messages bring raw material for the brain to process which
requires the student to examine an object, discern its important features, then
integrate and relate new information to previous experience. A child with NLD
may have a good eye for detail but have trouble separating details from the
whole object being perceived. For example, they may be able to describe a
house in detail but not know where the house is (Molenaar-Klumper, 2002).

16
This failure to grasp the total picture is caused by inability to form visual
images (Thompson, 1997). If a child cannot envisage something seen
previously to mentally dissect, rearrange or reconfigure parts in relation to the
whole, he or she will have great trouble with assembly tasks, decision-making
and problem solving. Impaired ability to discriminate and recognise visual
detail and visual relationships together with outstanding deficiencies in spatial-
organisational abilities, particularly within a novel situation, are primary NLD
deficits likely to increase with age (Rourke, 1995).
6. Spatial perception is an aspect of visual perception. According to physician, L.
Kleinschmidt (personal communication July 7, 2001), spatial perception
defines the ability to perceive oneself in relation to surroundings, to identify
objects in relation to one another and see differences between them. A limited
wish to discover reduces exploratory behaviour and few environmental
impressions reflect a preference for known situations and familiar things.
Students who experience this form of perceptual disturbance often have a poor
understanding of in-out, under-over, right-left concepts, telling the time and
map reading will have great difficulty in classroom learning, particularly
following instructions (Rowley-Kelly & Reigel, 1993). Difficulty with spatial
relations impairs ability to synthesise visual-spatial information such as
recognising faces, interpreting gestures and reading facial expressions. Poor
spatial orientation and reduced physical rhythm affects performance in social
interactions, conversations and abstract academic endeavours including group
work which demands transition from one activity or location to another.
Visual-spatial-organisational deficits cause tremendous difficulty with
organising schoolwork and completing assignments to meet timelines.
7. Arithmetic deficits define difficulty distinguishing variations in shapes, sizes,
amounts and lengths and are present early in life because children with an NLD
infrequently play with puzzles, blocks or construction-type toys (Obrzut &
Hynd, 1991). A lack of desire to explore and discover the spatial and physical
attributes of objects influences acquisition of basic number concepts for a
student with NLD. Compared to reading and spelling, most students with an
NLD struggle with maths, especially problem solving. To solve a maths
problem, they must visualise a problem, consider different approaches and
choose the best resolution. Maths-based life skills that involve time, money
and measurement are problematic as are doubling and halving of size (Whitney,
2002).

17
8. Complex psychomotor skills refer to the mental origin of muscular movement.
Such skills require a psychological interpretation of an action followed by a
motor response, says physician L. Kleinschmidt (personal communication July
7, 2001). A deficit that is often more marked on the left side of the body may
cause the child with NLD to avoid crossing arms or legs. Further, he or she
may have trouble maintaining balance, walk with a wide gait and be accident-
prone (Molenaar-Klumper, 2002). Basic coordination and fine motor skills
“develop very slowly and lag behind” in the average child with an NLD
(Molenaar-Klumper, 2002, p.26). It may take years not weeks to learn to ride a
bike and even if balance and coordination are mastered, safety may be
compromised by problems with visual, visuospatial and decision-making.
Using cutlery, scissors and tying shoelaces are initially difficult tasks that may
improve with practice. A person with NLD may often be referred to as
“clumsy” or “awkward” because movements are not smooth and well-
integrated (Whitney, 2002, p.17). They do not outgrow this awkwardness as
happens with most children but instead, awkwardness becomes worse as motor
challenges increase.
9. Adapting to novel situations requires the ability to generalise which is the
hallmark of high-level intellectual functioning, says physician L. Kleinschmidt
(personal communication July 7, 2001). It requires ability to adapt previously
learned patterns of behaviour to new situations. Due to an over-reliance on
routinised behaviours, a student with NLD may use inappropriate responses in
new situations where new information must be integrated with previous
learning and experience. A poor memory for novel information that is not easy
to code verbally combined with difficulty interpreting the subtle aspects of
communication found in humour and difficulty “reading between the lines”
makes new situations highly stressful and fearful for a person with an NLD.
They do not understand deceit, cunning or manipulation but instead take
everyone at face value and translate all communication literally (Thompson,
1997). As age increases and verbal and nonverbal situations in school and
society become more complex, the adolescent with NLD finds he or she can no
longer rely on behaviours and responses previously found adequate. As a
result, social skills fail to develop over time and the student becomes more
isolated as he or she moves into adulthood (Anderson, Northam, Hendy &
Wrennall, 2001).
18
Problems common to mathematics and social functioning
When the qualitative aspects of performance in mathematics and social incompetence
were examined with children who exhibit an NLD, Rourke (1995a), Rourke and Conway
(1997) and Strang and Rourke (1985) found that the assets and deficits that seem to underlie
problems with mathematics such as visual-perceptual-organisational, psychomotor, concept
formation and ability to deal with novel problem solving situations, stemmed from the same
deficits as those which cause maladaptive social behaviour (See Table 4.7).
Relationship of NLD to other disabilities
Molenaar-Klumper (2002) raises an important point of discussion and that is, whether
NLD characteristics are clearly different from other developmental disorders or whether they
overlap with other known developmental disorders. She presents a hierarchy of ailments in
which white matter plays a part:
Ailments that show NLD characteristics some coincide with it
Hydrocephalus
Asperger’s Syndrome
Williams Syndrome
Right Hemisphere damage
Incomplete development of corpus callosum
Many NLD traits found among others in a majority of children with
Acute Lymphatic Leukaemia
Foetal Alcohol Syndrome
Some NLD traits among them
Traumatic Brain Injury
Multiple Sclerosis
Tsatsanis and Rourke (1995) hypothesise that developmental disorders “fall along a
continuum of neurodevelopmental disease”, each disorder characterised by varying degrees
of severity and its proposed relationship to white matter damage or dysfunction (p.476).
Because there are many levels of NLD, not every child will show all the characteristics
(Molenaar-Klumper, 2002).
It is interesting to consider differing professional attitudes towards the syndrome. From
a speech pathology perspective, Volden (2002) acknowledges the comprehension and

19
pragmatic language difficulties experienced by a child with NLD but says there is no reason
to believe the syndrome is a new phenomenon. It may be just a new way of thinking about
and categorising children already seen by speech pathologists. From a paediatric
occupational therapy perspective, Whitney (2002) suggests an over-developed left
hemisphere may suppress development of other parts of the brain. Changes in lifestyle,
education and family life over the past half century may also account for the rise in NLD
characteristics presenting in school populations. She further suggests that the syndrome did
not manifest severely fifty years ago because the roles of children provided sufficient
opportunity and challenge to develop deficient areas of performance. Activities such as
skipping, climbing trees and playing hopscotch served to develop motor sequencing and
psychomotor skills and because peer circles and extended families lived in relative close
proximity, caregivers were on hand to provide social skills training.
Clinical incidence of NLD
When asked if NLD was “too rare to be the focus of concerted research and clinical
efforts”, Rourke et al. (2002) said “autism, a disorder much rarer than NLD, has been the
subject of such concerted efforts – there is evidence that the ‘incidence’ of NLD is
increasing” (p.165). In the past, the clinical incidence of NLD in children referred for
assessment because of suspected learning disabilities was “one school-identified child who
exhibited NLD” to about 20 children who exhibited a language learning disability. In recent
times, this ratio has been halved to approximately 10 with a more ‘standard’ learning
disability to every one who exhibits NLD “and there are indications that this trend toward a
higher incidence of NLD among the population of children with learning disability is
continuing”, with a sex ratio of 1:1 with NLD (pp.165-166).
An explanation for the 1:1 gender ratio of clinical incidence since the 1980s is the
“gender role expectation revolution” where girls are now expected to engage in roughly the
same tasks and meet the same developmental demands as boys. Because girls now engage in
contact sports and strenuous track-and-field events and they are expected to match boys in
school subjects involving mathematics and science, difficulties with motor and psychomotor
skills, visual-spatial-organisational skills, concept formation and scientific activities are now
more pronounced (Rourke et al., 2002, p.166).

20
What causes NLD?
Current evidence and theories suggest destruction, damage or dysfunction of white
matter in the brain’s right hemisphere may be the cause of NLD (Thompson, 1997).
Rourke’s (1989) theoretical principles argue (i) the more dysfunctional or damaged the white
matter is, the bigger the chance an NLD will be present and (ii) the developmental stage and
type of white matter damage sustained has significant influence on manifestation of the NLD
syndrome.
It is recognised that both hemispheres are suited for different types of processing, but
typically complement each other in functioning. While neuroscientists are not in complete
agreement about the cause of the disorder, Rourke’s (1995) “White Matter, Right
Hemisphere Deficit” hypothesis is commonly accepted as a way to understand the
syndrome’s confusing manifestations (Vacca, 2001). Rourke’s explanation for NLD is based
on the Goldberg and Costa (1981) model constructed from data and speculations derived
from investigations of human adults. Goldberg and Costa claim the right hemisphere is
particularly equipped to handle tasks that involve inter-modal integration whereas the left
hemisphere is predominantly suited to intra-modal processing (Rourke, 1989).
This view involves right hemisphere facility to deal with abstract novel information
demands for which no task-relevant or pre-existing behaviour exists “in the person’s
cognitive repertoire” while the left hemisphere is adept at handling the routinised,
automated, stereotypic application of a particular plan once “assembled” by the right
hemisphere (Rourke, 1989, pp.63-64). This notion suggests the right hemisphere can
integrate information from several senses simultaneously such as interpreting gestures and
facial expressions with spoken language to clarify full meaning, whereas the left hemisphere
best handles well-practiced or rote learning presented in a step-by-step manner. These
functional hemisphere differences were addressed by Goldberg and Costa (1981 in Rourke,
1989) when they concluded:
1. The ratio of grey-white matter is higher in the left hemisphere than in the right,
meaning there is relatively more white matter than grey in the right hemisphere
(Rourke, 1989, p.62);
2. The grey-white ratio can be used as “a marker of prevailing organising ability of a
structure in reference to intra versus inter-regional integration” (p.63).
This indicates a relatively greater emphasis on inter-regional integration of the right
hemisphere and on intra-regional integration in the left. Tanguay (2002) suggests the
dysfunction caused by a disproportionate amount of white matter in the right hemisphere
21
versus the left explains why NLD is often referred to as a Right Hemisphere Syndrome. The
intra-regional pattern of connectivity that characterises the left implies excellence in tasks
that require focus on a single mode of performance. The right hemisphere’s inter-regional
pattern of connectivity constitutes a greater capacity to process many modes of
representation within a single task, in other words, complexity. Molenaar-Klumper (2002)
explains these functional hemisphere differences by suggesting that information stored in the
left side of the brain is more easily accessed because of a simpler structure whereas
information stored in the right hemisphere’s branch-like structure appears more complex and
obscure to access.
Empirical studies of the Goldberg and Costa (1981) model were carried out on a group
of children who exhibited extremely “well-developed word-recognition and spelling skills
but outstandingly poor performance in mechanical arithmetic” (Rourke, 1989, p.66).
Observations and generalisations drawn sufficiently illustrated that the group exhibited
deficiencies in inter-modal integration, problem solving and concept formation especially in
new situations and the group had extreme difficulty benefiting from experiences that did not
blend with known and practiced behaviours. They exhibited quite deficient right hemisphere
capacities within a context of clear verbal strengths and single mode intra-modal left
hemisphere skills. Conclusions and formulations drawn from research into right hemisphere
developmental learning disabilities by other researchers such as Tranel, Hall, Olson and
Tranel (1987), Voeller (1986), Weintraub and Mesulam (1983) bear a “more than passing
similarity” to those outlined in Rourke’s 1982 model (Rourke, 1989, p.79).
Explaining the title “Nonverbal Learning Disability”
“Nonverbal” in the title denotes a disability that originates from deficits in the
nonverbal processing domains. From this perspective, “the pattern of assets and deficits in
speech and language development displayed by the child with NLD is thought to arise from
interactions within and between a characteristic set of more basic nonverbal
neuropsychological assets and deficits” (Rourke & Tsatsanis, 1996, p.30). These
interactions are understood to be those within and between good auditory, rote memory,
simple repetitive motor skills and poor tactile-visual-organisational, complex psychomotor
and concept formation skills.
All learning involves verbal and nonverbal processes and deficits in visual-spatial-
tactile and psychomotor abilities will restrict exploratory behaviour, impede understanding
of cause-and-affect relationships in the environment and hamper ability to deal with new

22
situations. Such deprivation leads to impaired concept formation, nonverbal problem
solving, hypothesis testing and ability to profit from environmental feedback. These skills
require both hemispheres to integrate complex information which is difficult for a child with
NLD because one hemisphere is somewhat dysfunctional.
Summary
Children and adolescents with the NLD syndrome present a pattern of assets and
deficits that is characterised by well-developed verbal skills and poor psychomotor, tactile,
visual-spatial-organisational perceptual and problem solving abilities. Socioemotional
problems arise from limited understanding of higher-level language, age-appropriate social
skills and inability to adjust to changing social circumstances. Although compensatory
strategies may reduce deficits in some areas, any combination of these problems will affect
every aspect of daily life in one way or another and place the individual at substantially
increased risk of emotional problems with increasing age.
Working on Goldberg and Costa’s (1981) hemispheric specialisation, Rourke (1989)
theorised that the right hemisphere’s higher white-grey ratio than the left affords it greater
capacity to deal with inter-modal demands of complex work, personal or social information
and new situations. The left hemisphere’s greater grey-white ratio implies effective
functioning on tasks that require intra-regional activity such as routinised practiced
behaviours. The extent of compromise is influenced by the degree and age that white matter
damage was sustained. Individuals with right hemisphere compromise would not be
expected to score well on test measures that demand complex psychomotor, visual-spatial-
organisation, problem solving and task changing skills.
Part II
How hydrocephalus is linked to an NLD
Byron Rourke developed the “White Matter” model in 1987-1988 to account for
neuropsychological development within the areas believed to characterise all children who
display the NLD syndrome (1989, p.113). The principles that underpin the model claim that
a significant insult to the right cerebral hemisphere is “sufficient” to cause the NLD
syndrome, the “necessary” condition being damage or destruction of the neuronal white
23
matter which facilitates the transmission of information between hemispheres (Rourke, 1989,
114). In this study, the “necessary” condition is hydrocephalus.
Hydrocephalus is a condition characterised by excessive cerebrospinal fluid (CSF)
within the ventricles or “caves of the brain” (Rowley-Kelly & Reigel, 1993, p.10). Three
brain ventricles produce about 600ml of CSF each day. Cerebrospinal fluid keeps the brain
tissue buoyant, acts as a vehicle to deliver nutrients to the brain and remove waste, and it
flows between the head and spine to compensate for changes in the amount of blood within
the brain (National Institute of Neurological Disorders and Stroke, 2001). Hydrocephalus
occurs when an obstruction disrupts the flow of CSF through normal circulation pathways.
The area around the ventricles receives the greatest stress and as it yields, the “ventricles
enlarge which increases the pressure” on brain tissue (Dennis, 1996, p.407). Hydrocephalus
results from a number of congenital conditions which include spina bifida.
Spina bifida is a defect in the neural tube closure that may cause a complex congenital
disability when bones in the vertebral column or skull fail to fuse (Fletcher et al., 1992).
Fusion of vertebrae arches is an important step in embryonic development when the two
sides of the spinal canal in the back grow together “to form the cavity for the spinal cord”
(Andrews & Elkin, 1981, p.6). Neural tube malformations such as encephalocele and
anencephalocele are included in the term spina bifida (Andrews & Elkin, 1981, Year Book
Australia, 2001). These defects occur “when there is a failure to fuse at the head end of the
nerve cord” (Anderson & Spain, 1977, p.14). Spina Bifida presents with several degrees of
severity.
Spina Bifida Occulta is the most common, innocent and concealed form which is
characterised by absence of a small piece of vertebrae. The occulta type does not involve
herniation of meninges or contents of spinal cord (Eynon, Knighten, Kruse, Lee et al., 2002).
It rarely requires treatment and it is of little or no consequence to the person (Rowley-Kelly
& Reigel, 1993).
Spina Bifida Meningocele is an abnormality present at birth which is identified by a
smooth sac protruding from a defect in the skull or the vertebral column. The herniated cyst
is filled with CSF and either cerebral or spinal meninges but a meningocele does not contain
any neural tissue. Once the cyst is removed surgically, the patient rarely develops
hydrocephalus. There is usually no loss to neurologic function and the prognosis for normal
development is very good (Rowley-Kelly & Reigel, 1993).

24
A Lipomyelomeningocele is a closed neural tube defect in the lumbar region. Although
motor or sensory impairments may not be evident at birth, “subtle, progressive neurologic
deterioration” may become evident in later childhood or adulthood (Sandler, 1997). Spina
Bifida Myelomeningocele is the most severe form of spina bifida present at birth. It is
characterised by a split in the outer part of the vertebrae and the baby’s spinal canal remains
open along several vertebrae in the lower or middle back. Myelomeningocele involves the
lining or meninges of the spinal canal, the spinal cord and nerves, and almost all children are
treated with an operation to remove the cyst and close the opening in the spine to reduce risk
of infection (Rowley-Kelly & Reigel, 1993). There is always partial or complete paralysis
and loss of sensation in the lower part of the body and the degree of severity is determined
by the site and nature of the defect (Dunning, 1992).
In 95% of spina bifida cases today, progressive hydrocephalus develops which requires
shunting (Lutkenhoff & Oppenheimer, 1997). Excessive fluid in the brain’s ventricles is
treated by a shunting procedure which drains hydrocephalic fluid from the head to the heart
or abdomen. According to Dennis (1996), excessive pressure that is not relieved with 12
hours of obstruction will cause brain damage. See Appendix A for more information about
shunted hydrocephalus and spina bifida.
Summary
Rourke and associates found that a group afflicted with a hydrocephalic condition who
manifested the NLD syndrome most exactly did sustain significant destruction of right
hemisphere white matter from lesions caused by the hydrocephalus. Damaged nerve fibres
cause inter-communication problems which characterise a student with NLD and such
damage highlights the salience of white matter integrity for integration of new and complex
information between hemispheres. This relationship provides the “final common pathway”
that links residual damage from a hydrocephalic condition to a Nonverbal Learning
Disability (Rourke & Del Dotto 1994, p.37). The next chapter discusses the prevalence of
NLD characteristics in persons with hydrocephalus and spina bifida.

25
CHAPTER THREE
LITERATURE REVIEW II
NLD characteristics in individuals with hydrocephalus and spina bifida
Much literature that relates to the cognitive functioning of individuals with
hydrocephalus and spina bifida described heterogeneous groups where findings did not
discriminate between shunted and unshunted hydrocephalus despite well documented
evidence on the effects of shunted hydrocephalus on right hemisphere systems and cognitive
functioning. This review has sought to isolate studies that involved individuals with shunted
hydrocephalus and spina bifida and the characteristics that frequently constitute their unusual
cognitive profile. See Appendix B for Summary of Studies.
Learning difficulties in the child with spina bifida and hydrocephalus can be subtle and
difficult to diagnose (Rowley-Kelly, 1993). They may be well-masked by language-based
achievements which are usually applauded by parents and educators. The following
discussion will focus on the effects of auditory, tactile, motor and psychomotor, visual,
visual-motor and visual-spatial perception, problem solving and language on verbal and
nonverbal performance and their affects on academic skills and adaptive behaviours.
Impressive verbal strengths are consistently reported to cause unrealistic expectations and
misperceptions of competency and educational achievement lags behind “expectations raised
by the child’s fluency” (Tew & Laurence, 1979, p.360). The discrepancy between clear
ability with language and communicative content causes overestimation of the person’s real
capacity (Anderson et al., 2001). The frequency of such reports justifies investigation into
the relative verbal strengths of the student with shunted hydrocephalus and spina bifida
(Shaffer et al., 1985). The reported influence of distractibility on understanding of word
meanings merits inclusion of the distractibility factor.
Verbal Learning and Memory
Good auditory, verbal and rote memory skills and well-articulated speech are reported
strengths of students with shunted hydrocephalus and spina bifida though comprehension of
language may be poor (Dunning, 1992). Good auditory skills allow many students to
become fluent talkers with a good vocabulary who can pick up adult speech with ease
(Dunning, 1992). For individuals who display an NLD, auditory perception is a primary

26
asset that converts to good auditory and verbal memory and precise articulation of what is
heard.
Tactile perception
Findings from different assessment tools used to measure tactile-perceptual abilities of
children with hydrocephalus and spina bifida indicate that individuals were found to have
difficulties with tactile and visuospatial perception tasks (Wills, 1993). Mattson (1982)
reports that it is not unusual for children with spina bifida to have “pudgy, undeveloped and
weak” hands (p.227). Through the course of normal childhood development, children learn
about objects in the environment through physical exploration. They pick up objects, throw
them, drop them and pick them up again. Because children with NLD are relatively inactive
and have impaired tactile perception, they are content to investigate by asking questions and
relying on others to describe objects rather than employing physical movement, tactile and
visual sensory inputs. As a result of limited exploratory behaviour and inadequate
information from the tactile sensory system, they fail to make connections between objects
in the environment with obvious consequences for occupational performance (Whitney,
2002).
Motor and psychomotor functioning
Rourke’s (1989) NLD model is partly based on the role of early motor-based
deficiencies which characterise the child with hydrocephalus and limit exploratory
behaviour. When investigating the incidence of NLD in the student with spina bifida and
hydrocephalus, it is therefore important to assess motor system functioning. In many
students with spina bifida and hydrocephalus, abnormal brain development, spinal cord
problems and hydrocephalus cause impaired motor control of arms and hands in addition to
problems with lower limbs. Motor disorders may be due to malformation of cerebellum
which is critically involved in fine motor control of voluntary movement and proprioceptive
skills (awareness of body movements in space) that influence hand control and bimanual
motor control (Dennis, 1981). Development of fine motor skills may be delayed in the early
years because the arms and hands may be needed to support upper extremity functions thus
hindering opportunity to practice manipulation and coordination skills (Turner, 1986).
Visual-motor functioning may be affected by ocular problems such as squint, near
sightedness and poor visual tracking. As a consequence, poor eye-hand coordination may
cause students to perform poorly on tasks that require persistent motor control, execution of
fine motor tasks or tasks that involve time constraints with the speed of production. An
increased incidence of left-handedness or ambidexterity due to the effects of hydrocephalus

27
on motor centres of the brain does not “influence the pattern of intelligence” (Dennis et al,
1981, p.614). They report no differences between right and left handed children on VIQ,
PIQ and FSIQ and verbal-performance discrepancies (p.608) though Lonton’s (1976) study
of children born with myelomeningocele found children without a clearly established hand
preference tended to experience greater difficulty on academic and IQ tests.
Poor penmanship found to be common in students with spina bifida and hydrocephalus
causes handwriting to be extremely difficult. On copying or drawing tasks that require
visual-motor skills, Wills, Holmbeck and McLone (1990) found children with
myelomeningocele obtained much lower scores than other groups. Rourke (1989) considers
the graphomotor problems that cause slow and laboriously-produced script to be a tertiary
academic deficit with a child with NLD. Anderson and Spain (1977) found children with
spina bifida took the same time to write two sentences as controls took to write three, even
when pressed for time.
Dennis et al. (1981) categorised children according to whether motor problems were
severe, moderate or mild. All three groups with different levels of motor impairment
showed lower PIQ and as a result, lower FSIQ scores. However, all three motor impaired
groups showed a similar degree of nonverbal deficit and PIQ was equally poor regardless of
whether motor impairment was mild, moderate or severe indicating that “even a mild degree
of motor impairment limits the absolute level of nonverbal intelligence” (p.609). Degree of
reduced movement is therefore not critical to a nonverbal deficit because mobile and non-
mobile children were found to have similarly low nonverbal intelligence.
Hydrocephalus, a presence of the Arnold-Chiari malformation (variable cerebellum
displacement) and lack of exploratory behaviour due to reduced mobility affect the visual-
motor skills of 80-90% of students with spina bifida (Hurley, 1993). A study of
neuropsychological and adaptive functioning in younger and older children with shunted
hydrocephalus and spina bifida observed that depressed scores in motor speed and
visuomotor integration compared to norms may be attributable to the impact of higher level
lesions (Holler et al., 1995).
Fletcher and Levin (1988) report an experimental measure of motor learning
administered to 20 children with spina bifida and hydrocephalus by Anderson and Plewis
(1977). The task required children to place a dot between two circles as fast as possible for
twelve trials. Children with hydrocephalus were slower and less accurate than controls and
were more affected by restriction of visual feedback. Deficiencies in children with spina

28
bifida and hydrocephalus were attributed to poorer manipulative skills and visual-spatial
abilities (Fletcher & Levin, 1988).
Visual perception
Individuals with spina bifida and hydrocephalus frequently experience visual perception
problems (Rogosky-Grassi, 1993, p.200). Common visual defects experienced by the
student with spina bifida and hydrocephalus are abnormal eye gaze, poor visual acuity and
strabismus or squint. Such abnormalities that occur during early development and are
associated with “poor nonverbal but not verbal intelligence” contribute to impaired
development of visual perception skills and depressed FSIQ score (Dennis et al. 1981,
p.609). Strabismus is common in students with spina bifida and hydrocephalus and if left
untreated will result in loss of vision in the affected eye (Hurley, 1993). Because the eyes
may appear “normal”, teachers may be unaware of visual impairment (p.113). Visual and
upper extremity motor problems impair manipulative tasks such as cutting with scissors and
using assembly objects, a deficit which Hurley (1993) says may relate to a general nonverbal
learning disability.
Two areas of particular difficulty are discriminating “figure” from background and in
making spatial judgments (Dunning, 1992, p.16). Visual perception requires visual acuity
and eye muscle control if the eyes are to gain a good visual image and an appropriate
attention span for task focus is essential. Fletcher and Levin (1988) report Woods’ (1979)
finding that 35% of a group of spina bifida children had a vision defect while Clements and
Kaushal (1970) found vision problems in 50% of a mixed group with spina bifida and
hydrocephalus. Dennis et al. (1981) examined the relationship between ocular abnormalities
and psychometric intelligence and concluded that visual abnormalities were associated with
lower PIQ but not VIQ.
Visual-motor perception
Abercrombie, Lindon, Gardiner, Tyson and Jonckheere (1964) argue that visuomotor
disorders cannot be explained by lack of spatial experience because children with a spastic
condition and children “similarly handicapped” with respect to movement in space had
visuomotor disorders (p.206). Although deprivation of movement does not cause
visuomotor disorder, deprivation of movement or movement disorders do affect “general
mental development, particularly perception” (Abercombie, 1968, p.206). Abercrombie
(1968) reports the significant importance of motor activity for mental functioning. An
experiment in short-term exposure to prisms conducted by Held (1965) illustrated a close

29
one-on-one relationship between movement and visual feedback. Hypothesis testing
confirmed that ability to adjust impaired visual input was critically reliant upon active
movement. Holler et al. (1995) found the number of shunt revisions “negatively related to
PIQ and visual-motor integration” (p.70) though Hunt and Holmes (1975) concluded that
number of shunt revisions was not related to cognitive functioning.
Fletcher (1995) compared visual-motor performance on motor-based Visual-Motor
Integration (VMI) and motor-free Judgment of Line Orientation (JLO) with a hydrocephalic
group of children and found they obtained significantly lower scores on both measures.
Wills et al. (1990) used the VMI with a myelomeningocele group when assessing
intelligence and academic achievement. Strong correlations were found between PIQ, VMI
and arithmetic measures.
Visual-spatial perception
Students with spina bifida and hydrocephalus experience difficulty with spatial
awareness (Hurley, 1993). Inability to appreciate or judge distances between oneself and
objects in the environment before organising a sequence of movements has consequential
effects on independent living skills, road crossing, driving a motor vehicle, map reading and
following directions. Abercrombie et al. (1964) suggest limited spatial experience,
especially if it occurs in early life as a result of deficient mobility of the hands or whole
body, may affect development of skill in “understanding spatial relationships and
manipulating them” (p.575).
The significant visual-spatial problems in children with spina bifida and hydrocephalus
in Fletcher et al. (1995) tempted investigators to propose that a task’s motor component may
explain deficiencies observed in children with hydrocephalus. Comparison of motor-based
and motor-free spatial tasks showed children with shunted hydrocephalus “were significantly
impaired” on the motor-based test indicating that a testing tool sensitive to visual-spatial
difficulties is more appropriate for the child with spina bifida and hydrocephalus (p.217).
Deficits in these nonverbal measures are consistent with Rourke’s (1989) suggestion that
impaired visuospatial skills may be partially a consequence of right hemisphere shunt
placement.
Executive Function
Executive functioning refers to a range of loosely related higher-order cognitive
processes including planning, organisation, problem solving, hypothesis testing, mental
flexibility, decision making, feedback utilisation and self-perception and any combination of

30
these difficulties will interfere with day-to-day functioning in a range of areas (Spreen &
Strauss, 1998). These functions may be conceptualised as a group of processes that guide
and manage cognitive, emotional and behavioural functions, especially during active novel,
problem solving activities (Gioia, Isquith, Guy & Kenworthy, 2000). Social interaction, for
example, requires a response to a series of nonverbal cues in addition to any verbal
information. Nonverbal feedback that is not accurately interpreted and integrated with
verbal input may result in an inappropriate response and inhibit social interaction (Anderson,
2001).
The ability to organise is an “extremely active process” and highly problematic for a
child with limited mobility and/or severe coordination problems (Rowley-Kelly, 1993,
p.223). It requires visual and tactile exploration and complex psychomotor manipulation to
effectively deal with novel information which may speculate a link between visual motor,
psychomotor, organisation and cognitive skills. Students with spina bifida and
hydrocephalus have a fundamental difficulty with planning and organisation which Mattson
(1982) explains as “the ability of the brain to conceive of, organise, and carry out a sequence
of unfamiliar actions” (p.227).
Fletcher et al. (1995) interpreted the Wisconsin Card Sorting Test (WCST) as a
measure of ability to shift attention, this ability considered to be a significant mark of a well-
functioning brain (Tsatsanis & Rourke, 1995). They found the total number of 145 children
with arrested, shunted or no hydrocephalus aged 5-14 years, the groups with shunted and
arrested hydrocephalus completed significantly fewer categories on the WCST than other
groups. Apparent reliance of the WCST upon integrity of right hemisphere systems
influenced Fisher, DeLuca and Rourke (1997) to use it with fifteen 9-17 year-olds who
exhibited the NLD syndrome. They found NLD subjects demonstrated inferior WCST
performance thus extending the domain of problem solving performance impairment to
include executive functioning. Hurley et al. (1990) considered WCST scores to be most
indicative of brain damage and level of daily functioning. Additionally, they chose the
WCST because of its ability to (i) assess and use environmental feedback to develop
problem solving strategies, (ii) shift set and suppress inappropriate responding and (iii)
selectively attend to relevant stimulus dimensions without distraction. These extended
findings that involve deficits in dealing with novelty, ambiguity and non-routinised situation,
support Rourke’s model of NLD (Rourke, 1981; Rourke, 1989).

31
Language
Because many children with hydrocephalus and spina bifida can freely generate
sentences with good articulation, they are not considered to need special educational support
(Hurley, 1993). Evidence and discussion has highlighted a consistent pattern of better-
developed verbal than nonverbal abilities which supports a commonly held belief that verbal
skills are a strength of children with spina bifida and hydrocephalus and initially their most
impressive characteristic. Language of children with hydrocephalus is often described as
being “an effective vehicle for social contact but an unsuccessful way of conveying
meaning” (Dennis, 1996, p.410). There is now growing consensus among researchers that
the language of children with hydrocephalus is not normal (Fletcher et al. 1995; Wills,
1993).
Fletcher et al. (1995) administered four language tests to 40 children aged 5-14 years
with shunted hydrocephalus and spina bifida and compared results to normal children. On
tests that addressed verbal fluency, rapid naming, timed word retrieval, automaticity and
word finding skills, the spina bifida group “scored well below the normal children” (p.221).
Worth noting are the skills demanded by these timed tests. Poor performance may reflect
slower processing speed of groups with hydrocephalus and spina bifida, a “deficit to be
expected from a population known to suffer significant white matter compromise rather than
language deficit” (Anderson et al., 2001, p.199). Further, the automaticity naming test
requires attaching a name to picture information. The visual information presented and
processed by the right hemisphere must cross to the left hemisphere’s naming centres, the
conduct of such transmission between hemispheres impaired in many children with
hydrocephalus due to damaged or destroyed white matter.
When assessing the abstract demands of verbal ability, Culatta and Young (1992) found
IQ tests reflected no differences between children with spina bifida and hydrocephalus and
normal controls in the more concrete use of language but when judging the abstract demands
of verbal ability, children with spina bifida and hydrocephalus tended to have a higher rate of
irrelevant utterances and poorer performance. Horn et al. (1985) suggest that excessive
verbiage is partly due to difficulty attending to relevant features while ignoring irrelevant
elements that occur in the environment which may indicate a link between language and
distractibility.
Language and distractibility
Frequently, children with spina bifida and hydrocephalus show difficulties in applying
sustained attention to a task (Abercrombie, 1968; Horn et al., 1985; Shaffer et al., 1985).

32
Horn et al. (1985) sought to confirm a relationship between language deficits and
distractibility in children with spina bifida and hydrocephalus. They hypothesised that if
distractibility affects language comprehension, subjects with spina bifida and hydrocephalus
should perform relatively poorly on vocabulary items presented with irrelevant information
and in the absence of irrelevant information, they should perform similarly to matched
controls. They suggest that difficulty distinguishing between the relevant and irrelevant
aspects of a situation may partially account for deficits in the pragmatic aspects of language
discussed by Rourke (1989), which posits a relationship between language-distractibility-
comprehension and verbal responses.
Culatta and Culatta (1978) found that standardised tests often overestimate language
comprehension of children with spina bifida. They report examples of children who were
unable to identify examples of words used in their own speech. Assessors should not be
deceived by clear articulation and grammatical patterns of the speech of a typical child with
spina bifida but should observe dissonance between a word and the situation in which it is
used and whether the child understands the language he or she is generating. To use a word
appropriately, one needs to attend to its recurring relevant features while ignoring contextual
features not relevant to the word meaning (Horn et al., 1985).
The fact that children with spina bifida and hydrocephalus performed similarly to
controls on vocabulary comprehension in the absence of irrelevant information indicates they
grasped the initial concept, yet results showed that distractibility affected receptive language
use after initial acquisition of word meaning when selective attention must sort relevant from
irrelevant background stimuli (Horn et al., 1985). If a child with spina bifida and
hydrocephalus has difficulty recognising the relevant features of a task, relevant and
irrelevant features may be considered in decision-making. A tendency for irrelevant items to
claim “some share of attention” may cause the child to lose track of the relevant task (Horn
et al., 1985, p.718). Increased distractibility was found to be partly responsible for deficits in
vocabulary comprehension after initial word acquisition, which may explain use of a word
without understanding of its meaning and use of vocabulary above the mental level of the
child (Fletcher et al., 1995).
Culatta (1993) offers three possible reasons why the child with hydrocephalus and spina
bifida may use irrelevant and inappropriate language:
1. When perceptual task demands became complex and they wished to end the
activity, Kozbelt-Culatta (1975) found students used expressive language and
frequently changed the topic of conversation;

33
2. A child with hydrocephalus and spina bifida might use a word because it sounds
interesting, although this may also be a trait of children with no disability. Words
used in an inappropriate context were found to be those which students failed to
recognise on a subsequent comprehension test (Culatta & Culatta, 1978);
3. Personality characteristics of children with spina bifida and hydrocephalus and the
Cocktail Party Syndrome (CPS) indicate “they revel in the opportunity to use large
words and display their memorising ability”, but intellectual limitations become
apparent if asked to define words used in conversations (Tew & Laurence, 1979,
p.361);
4. Difficulty maintaining sufficient attention to follow topical conversation causes the
student with spina bifida to produce irrelevant responses rather than expand the
topic (Williamson, 1987). As irrelevant utterances increase, attentional
performance decreases (Culatta & Egolf, 1980). Other relative influences upon
language usage now emerge. Distractibility reduces selective attention and ability
to attend to a word’s salient features in concert with its environmental aspects;
reduced word understanding inhibits ability to maintain focused attention on a
conversational topic; impaired perceptual skills reduce ability to attend to task
demands causing an increase in irrelevant language. This amalgam of factors no
doubt contributes to the verbal-pragmatic language deficits that Rourke (1989) says
are “notably absent” from spoken and written language of persons with NLD
(p.94).
Academic skills
Children with spina bifida may be passed along in school for years while falling further
behind in academic skills. “Parents and educators may have unrealistic expectations that the
child fails to meet” (Hurley, 1993, p.107). Poor academic skills are seen among many
individuals with spina bifida with and without CPS (Shaffer et al., 1985). Studies discussed
clearly show hydrocephalus is a factor in the development of cognitive skills. Based on
verbal and performance IQ levels, academic achievement has consistently been reported to
be lower than that of peers with PIQ below expectations when compared to VIQ. Although
basic reading is usually intact, deficits in selective attention, visual-field and visual scanning
impact upon word understanding and passage comprehension. It may be that children with
spina bifida and hydrocephalus rely only on superficial word knowledge and novel usage and
exclude integration of contextual information. Difficulty with the pragmatic aspects of
language and ability to distinguish between the relevant and irrelevant aspects of a situation
discussed by Culatta (1993), Horn et al. (1985) and Rourke (1989) indicate a link between
language, distractibility, word comprehension and verbal behaviour.

34
Arithmetic deficits were consistently reported in children with spina bifida and
hydrocephalus. The arrangement of precise numbers into sequences, lines or columns
requires computation skills that tap visuospatial and serial-ordering skills. Such deficits may
be due to limited early exploratory experience with size, shape, weight and quantity (Wills et
al., 1993). Further, slow arduous graphomotor skills restrict their rate of productivity and
academic achievement, such characteristics consistent with predictions in the Rourke (1989)
NLD model.
Adaptive Behaviour
A condition such as hydrocephalus related to a neural tube defect may interfere with
acquiring developmental skills and adaptive behaviours necessary for successful coping
strategies. To cope with the needs of a changing environment, a child needs to manage in
the physical environment, interact with objects in the environment and adapt to changing
social situations (Williamson, 1987). Coping strategies rely on such variables as level of
intelligence, language, temperament and social skills which collectively contribute to
integrative ways of managing. As children who exhibit NLD characteristics become older,
they experience greater difficulty coping with novel or complex tasks that require problem
solving and concept-formation abilities (Casey & Rourke, 1991). Such children demonstrate
increased levels of socioemotional disturbance “particularly of the internalised variety”
(p.288).
Fletcher et al. (1995) administered the Vineland Adaptive Behaviour Scales to parents
to gather information about their child’s behavioural adjustment. Findings revealed that
assessment of psychosocial adjustment of the same cohort at a younger age showed
hydrocephalus and its treatment were related to an emergence of behaviour problems. Holler
et al. (1995) found adaptive and social behaviours were impaired in older versus younger
children and as social behaviour demanded more content-rich language with increasing age,
parents reported older children fell behind peers.
Rourke, Fisk and Strang (1986) raised concern about the personality status of children
with an NLD which caused them to collect data regarding parental perceptions. Parents
reported poor socialisation skills, poor peer relations and a tendency to gravitate towards
younger or older playmates, withdrawal and isolation in social situations, inappropriate
behaviour especially in unstructured social situations and a poor appreciation for social
distance. As adolescence approached and task and social demands became more
sophisticated and complex, parents reported a shift toward internalised personality
maladjustment with children feeling increasingly more anxious in novel situations.

35
Academic and adaptive behaviour deficiencies of children with an NLD were evidenced in
home, school and community settings and the type and range of academic, basic self-help
and communicative difficulties reported render such children at risk of “serious adjustment
problems throughout their development” (Rourke et al., 1986, p.240). A repertoire of key
social and adaptive behaviour skills is indispensable to social acceptance and “effective
mainstreaming” (Rowley-Kelly, 1993, p.269).
Paediatrician Dr Mel Levine (1999) claims:
From the moment school-age children emerge from the bed covers each day until their
safe return to that security, they are preoccupied with the avoidance of humiliation at all
cost. They have the constant need to look good, to sidestep embarrassment, and to gain
respect, especially from their peers … The child with a learning disorder faces an
especially daunting challenge in the quest to feel respected among peers, admired by
parents, and reasonably satisfied with the track record achieved by his steadily evolving
mind (p.2-3).
Possession of key social and adaptive behaviour skills by a person with spina bifida is
by no means guaranteed given the harmful effects of hydrocephalus on ability to handle the
increasingly more complex tasks and social demands that accompany the journey through
school to adulthood and personal independence.
Summary
Literature reviews discussed characteristics of the Nonverbal Learning Disability
syndrome and the syndrome’s principle features as reported in individuals with shunted
hydrocephalus and spina bifida. Fletcher et al. (1995), Holler et al. (1995) and Wills et al.
(1990) reported relationships between cognitive skills development and Rourke’s (1989)
NLD model in cohorts with hydrocephalus and spina bifida. A focus on major areas of
functional difficulty for individuals in this population, visual, visual-motor, visual-spatial,
psychomotor and language, their cumulative influence on verbal and nonverbal intelligence
and their association with the NLD syndrome dictates that appropriate test measures be
utilised to assess the NLD status of each student who participated in this study. Deficits are
not global because the individual may present with a “wide range of behaviours and
abilities” (Thompson, 1997, p.44):

36
Strengths
Verbal fluency and clear articulation
Skilful rote verbal and rote memory skills
Impressive vocabulary
Early reading skills development
Co-exist with
Severe balance problems and lack co-ordination
Visual, spatial, organisational and tactile perception problems
Difficulty with fine motor skills
Difficulty with problem solving, planning and organisation
Difficulty with language comprehension
Difficulty with social judgment and interaction
This unique combination may be displayed by a student with shunted hydrocephalus
and spina bifida whose profile equates with uneven cognitive growth due to hydrocephalus
in the first months of life. The literature has frequently said that the occurrence of
hydrocephalus may cause a significant difference between verbal and nonverbal intelligence
which is often confusing for teachers. This discrepancy may result in an overall intellectual
disability. Early onset of hydrocephalus and subsequent management of the condition
therefore have a major influence on the development of cognitive, motor and visual abilities
and social skills (Fletcher & Levin, 1988). Learning difficulties of children with
hydrocephalus and spina bifida are different from those shared by other children with
learning disabilities. Language is generally well-developed and auditory memory can be
outstanding compared to other areas of functioning. In this regard, they are different from
“low-ability children without physical disabilities whose language tends to be retarded in
comparison with performance skills” (Dunning, 1992, p.15). See Appendix C for
Background to V-P discrepancies in individuals with shunted hydrocephalus and spina
bifida.
Because right hemisphere deficits do not significantly impact on performance in the
early grades, Thompson (1997) says young students with NLD usually do not receive
services. If the student is to receive the necessary support to experience success through
school and be prepared to meet the social and adaptive demands of post-school life, early
identification and intervention are imperative. The best outcomes reportedly result from
early identification and intervention which places heavy reliance on the knowledge and
understanding of teachers and parents as those who are in the best position to shape and
enhance the child’s development (Rourke, Young, Strang & Russell, 1986). Once identified,

37
difficulties across academic parameters must be managed by effective inclusive education
strategies. See Appendix F for Strategies to aid Inclusive Education Practice.
Such responsibility provides good reason to explore the perception phenomenon.
Unstructured conversational interviews will gather perspectives from teachers, aides and
parents on the educational experiences of students who share NLD characteristics.
Assimilation of in-depth interview data with assessment data is expected to provide
comprehensive insight and new understanding of the research problem. The following
research question is derived and formulated from preceding literature reviews. It represents
a transparent need and the worthiness of findings has been scrutinised.
Implications for this research
Literature emanating from the United States and Canada reports that teacher
unfamiliarity with the NLD syndrome and its long-lasting effects may cause them to assume
a child presenting with this profile is “emotionally disturbed”, “bright but doesn’t apply
himself”, “will be fine once he/she learns to better organise him/herself” (Thompson, 1997,
p.10) or the child is “simply immature” (Rourke et al. 1986, p.252). Exploration of
perceptions may induce collaborative discourse, challenge existing assumptions and lead to
better understanding. If awareness of the NLD paradoxical presentation convinces teachers
to refer students they presume are “lazy” or “unmotivated” for assessment, the long-term
effects of misperception and/or labelling through the long school experience will be
minimised. Levine (1994) believes the “immediate short-term effects may be minimal
compared to the durable impacts of their misinterpretation” (p.272).
Research question
How do teachers, teacher aides, parents and students perceive the educational experiences of
5 students with shunted hydrocephalus and spina bifida?

38
Findings may benefit children who share some but not all characteristics of children
with shunted hydrocephalus and spina bifida. For example, individuals with an ABI,
Asperger’s Syndrome, Acute Leukaemia, Foetal Alcohol Syndrome and Multiple Sclerosis
may display a pattern of similar strengths and weaknesses due to damaged or destroyed right
hemisphere white matter. Depending on the “geographical focus” of damage and the age
damage was sustained, common areas of difficulty in home, school or vocational settings
may include impaired cognitive, sensory, memory, language and social abilities (Rourke,
Bakker, Fisk & Strang, 1983).
This study makes a significant contribution to existing literature. In particular, it
responds to allegations that teachers and other professionals are uninformed about the NLD
syndrome. To gain a comprehensive understanding of the true state of affairs, the original
intention was to interview significant stakeholders in each student’s life, teachers, parents
and students themselves. After teachers suggested that aides may know “more than us”, the
researcher sought additional permission from all school principals to interview teacher aides.
By including those individuals who provided the one-on-one support, the study’s approach
was expanded to incorporate another layer of understanding. The following chapter will
discuss the study’s theoretical framework and the processes that were utilised to recruit
participants and collect, analyse, interpret and report data.

39
CHAPTER FOUR
METHODOLOGY
This chapter comprises two parts. Part I addresses the theoretical underpinnings of this
study, the researcher’s philosophical position towards the reality of perceptions, the
recruitment process and naturalistic inquiry methodology. Part II describes the strategies and
activities that were used to initiate and conduct the project to completion.
Part I
Theoretical underpinnings
A methodology outlines the direction, theoretical principles and framework to guide
how research will be done in the context of a particular paradigm. Given the complexity of
educational problems, some approaches are more holistic and able to embrace greater
complexity than others (Keeves, 1999). Quantitative research uses standardised measures to
gather data for analysis and comparison according to predetermined rules and procedures.
On the other hand, qualitative research allows investigation into specific issues in depth and
detail in the field without constraint of predetermined categories. It lends itself to thick
description and depending on the complexity of interactions, may become intense.
Qualitative researchers are committed to a naturalistic viewpoint, interpretative
understanding of human experience and the situational constraints that shape inquiry (Denzin
& Lincoln, 1994). Each paradigm or model examines the world differently through its
unique set of beliefs, creates phenomena to which beliefs are perceived to apply, proposes
questions that may be answered and submits different kinds of knowledge, the validity of
which is justified by the method from which it was derived (Salomon, 1991).
Qualitative research is largely unstructured, results are unpredictable and the outcomes
are uncertain (Denzin & Lincoln, 1994). The researcher has no governance over what data
will emerge. A qualitative method was used to investigate the perception phenomenon
because it typically seeks to explore meaning and understanding gathered in the field with
the “entity-in-context” for fullest understanding (Lincoln & Guba, 1985, p.39). “Perception”
was used as a conversational term to express personal insight and experience.

40
Philosophical position towards reality
Any social inquiry requires the researcher to have an “image of the situation”, a
yardstick by which evaluation and new knowledge may be measured. The researcher
approaches any social inquiry with a set of assumptions that explain how he or she perceives
the world, how knowledge is constructed and the reason for conducting research. These may
constitute a formal philosophical stance or they may simply be “crude mental models”
(Smith 1997, p.74). Inherent in the inquirer’s mental models is the power to determine what
counts as knowledge, such authority permitting one to discriminate “warrantable knowledge
claims from unwarrantable ones”. These should never go uncontested if the “voices of the
minority” are to be heard (Greene & Carecelli, 2003, p.95).
A constructivist-perceptual position towards reality was adopted. The constructivist-
realist posture believes the multiple realities that reside in the minds of people are best
studied in a holistic idiosyncratic way while perceptual realists concede reality may be
appreciated from certain vantage points which some call perception (Guba & Lincoln, 1999).
Although real to the owner, the perceptual realist views a perception as a partial incomplete
view of a phenomenon, capable of different interpretation if viewed from another
perspective. Although teachers and aides had limited knowledge about each student’s
aetiological background and information about NLD characteristics, perceptions were
considered an expression of understanding at a particular point in time.
Basic to all real-world inquiry is adoption of a hermeneutical approach towards
interpreting perceptions which involves revelation of different views and making sense of
what was observed in a way that communicates understanding (Denzin & Lincoln, 2000).
The major purpose of this process was not to justify one’s own constructions but to expose,
clarify, compare and contrast divergent views to promote a connection between them and
“mutual exploration by all parties” (Guba & Lincoln, 1989, p.149). Hermeneutics
philosophy pays attention to context and what the respondent intended to communicate. It
theoretically argues that the researcher interprets another perspective from a particular
standpoint or situational context. For this reason, one must know about the researcher and
informants to place the study in a proper hermeneutic context (Patton, 1990).
Recruitment process
“In research, sampling is destiny” (Kempster, Stringfield & Teddlie, 2003, p.275).
Sampling refers to selecting people in a manner that will maximise the researcher’s ability to

41
generate a thorough database to explore the phenomenon of interest, make inferences from
the data to produce credible explanations, use tacit knowledge of what may or may not work
and “where theory meets the hard reality of time and resources” (p.273). Purposeful
recruitment maximised researcher ability to develop theory that took account of local
conditions, influences and values.
Purposeful recruitment strategy
The inherent practical nature of recruitment issues invariably forces pragmatic choices
to be made. To encompass the demands of any single or mixed method, Curtis, Gesler,
Smith and Washburn (2002) adapted the following Miles and Huberman’s (1994) criteria to
evaluate a recruitment strategy:
1. The recruitment strategy should stem from the researcher’s conceptual framework
as well as from the research question being addressed;
2. The final subgroup and associated others should be able to generate a
comprehensive database on the phenomenon under study and allow for the
possibility of drawing clear inferences and credible explanations from the data;
3. The recruitment strategy must be ethical, feasible and practical.
This scheme allowed qualitative inquiry to comprehensively address the research
question. A subgroup that displayed the characteristics of research interest was expected to
provide richly descriptive data and findings that were rich in understanding.
Final subgroup
The power of purposeful recruitment lies in selecting information-rich cases from
which a great deal can be learned. In qualitative research, there are no rules for group size,
the number entirely dependent upon the issue under investigation with a focus on quality and
information-richness (Erlandson, Harris, Skipper & Allen, 1993; Patton, 1990). A
contingent and serial approach allowed the refinement of a homogeneous subgroup. The
contingent and serial approach meant that additional attributes were tapped only after
predecessor attributes are identified and tapped (Lincoln & Guba, 1985). In terms of a
qualitative study, a homogeneous group required the researcher to purposefully select
individuals who shared defining characteristics. The final subgroup comprised those
individuals who displayed the “blueprint” of characteristics needed to generate data that
were rich in content and inclusive in scope, data that revealed valuable new “portraits” and
understanding (Patton, 1990).

42
Naturalistic Inquiry Methodology
Strengths and weaknesses
Naturalistic Inquiry methodology suited the purpose of this study since the intention
was to explore the reality of perceptions by eliciting teacher, aide and parent perceptions of
students’ learning experiences. Naturalistic Inquiry methodology was chosen for the
following reasons:
1. It resonated with an interpretive predisposed view towards conducting inquiry
whereby perceptions were represented by multiple complex constructions;
2. It embodied assumptions and values that matched the researcher’s view of seeing
the world (Glesne, 1999);
3. It allowed respondents to be forthcoming and willing to express personal
understandings about the phenomenon;
4. It provided flexibility to follow new leads and scope to explore perceptions to
whatever depth the informant deemed apposite;
5. It allowed the researcher to sense salient and sensitive issues, bring tacit
understandings to bear upon the best means of follow-up and to be infinitely
adaptable while remaining actively engaged in the inquiry process;
6. It endorsed personal experience, insight and tacit understandings as a means of
promoting inquirer-respondent interactivity, appreciating nuances, and shedding
light on case study discussions;
7. The degree of uncertainty created by inquirer-respondent interaction was minimal
due to “insider” experience with students who had similar aetiological
backgrounds;
8. Insider knowledge and experience raised contextual awareness of factors and
influences that interacted to mutually shape student behaviours.
The elements of naturalistic inquiry most relevant to this study are captured by Wolf
and Tymitz (1977). Naturalistic inquiry is geared to uncovering many personal but
nonetheless important stories “told by real people, about real events, in real and natural
ways”. It attempts to present segments of life in the informant’s natural language that
represent as closely as possible how they feel, what they know and what their “concerns,
beliefs, perceptions and understandings are” (p.7).

43
Naturalistic Inquiry methodology translated interpretivist principles into research
language to show how perceptions were explored, gathered, analysed and explained. The
purpose of naturalistic inquiry was to understand and reconstruct the multiple realities that
informants, including the researcher, held while remaining open to new interpretations as the
“scope of the inquiry” expands (Guba & Lincoln, p.142). Such open-endedness would have
made a definitive inquiry impossible before commencement, a principle characteristic of
naturalistic inquiry being that steps be repeated as often as necessary to clarify the picture,
like the layers of an opinion, multiple realities “nest within or complement one another.
Each layer provides a different perspective of reality and none could be considered more true
than any other” (Guba & Lincoln, 1981, p.57). Naturalists therefore take an expansionist
position, building outward from the point of entry into the inquiry field, each new layer
peeled back with the sum of insights gleaned from the previous layer.
A principal weakness of Naturalistic Inquiry methodology is potential for copious
amounts of data resulting from open-endedness, adaptability, flexibility and expansion which
may threaten in-depth analysis. A further limitation may be that generalisations or “truth
statements free from both time and context” are not a possibility (Lincoln & Guba, 1985,
p.38). Rather, the aim of inquiry may be seen as developing a body of knowledge that
describes individual cases in the specific context under investigation.
The following discussion outlines the inquiry’s framework, the axioms that underpin
naturalistic inquiry, the significance of context and the operational techniques employed to
address trustworthiness standards. The credibility standard was addressed by on-site
engagement, contextual observation and triangulation activities. Dependability and
confirmability standards were mutually addressed and communicated through examination
of the audit trail. In the context of this study, the transferability standard was not considered
pertinent to the exploration of perceptions.
Axioms that underpin Naturalistic Inquiry
Naturalistic Inquiry Methodology is based on a set of basic axioms or principles that
inquirers contend are more meaningful and a “better fit” to most social phenomena (Guba &
Lincoln, 1999, p.141).
Axiom 1. This principle contends that multiple realities exist in the minds of people; an
assumption that is compatible with a constructivist view of reality. Interpretation and
understanding rely on holistic individual analysis of context and responses (Green,
2002). “No phenomenon can be understood out of relationship to the time and context
that spawned, harboured and supported it” (Lincoln & Guba, 1985, p.189). An inquiry

44
into human interactions and settings requires the naturalistic researcher to merge a basic
posture of “not knowing what is not known” with humility and willingness to learn what
was never imagined to be learnable at the outset (p.235). As multiple realities emerge
for further exploration, naturalistic inquiry diverges rather than converges which means a
predetermined plan is supplanted with general directions to be filled out as the inquiry
proceeds (p.236). Even with general boundaries in mind, initial stages of inquiry into
multiple constructions with wide “sweeps of the data collection net” dredge up much
information that is interesting but irrelevant (p.228).
Axiom 2. The inquirer-respondent relationship emphasises that an accurate presentation
of the respondent’s voice is critical to inquiry and a truthful account of the informant’s
opinion and experiences depends on the inquirer’s ability for “detached reporting”
(p.39). Lincoln and Guba (1999) believe the inquirer-respondent interactivity should be
exploited to stimulate engagement and insight. The researcher acknowledged past
experiences and remained aware of forces that helped shape interpretations and
subscribe to her theoretical stance.
Axiom 3. The possibility of generalisation in naturalistic inquiry may be seen as
developing a body of knowledge that describes individual cases in the context under
investigation. This premise drew the researcher to naturalistic inquiry because it “gave
voice” to a group generally not heard, 5 individuals with hydrocephalus and spina bifida,
their parents and teachers. Lincoln and Guba (1985) say “if you want people to
understand better than they otherwise might, provide them information in the form in
which they usually experience it. They will be able, both tacitly and propositionally, to
derive naturalistic generalisations that will prove to be useful extensions of their
understandings” (p.120).
Axiom 4. At best, the inquirer hoped to establish a reasonable pattern of influence by
identifying the meaning and understanding being sought (Lincoln & Guba 1999, p.143).
It is impossible to distinguish cause from effect because entities are in a state of “mutual
simultaneous shaping” that may be compared with the brain’s “interconnected mass of
neurons where every neuron is connected to every other neuron in a seemingly trackless
fashion” (Lincoln & Guba, 1985, pp.38, 151). All interrelated parts of reality represent
the “whole” with general unclear boundaries but a wealth of central meaning about
interrelationships between parts.
Axiom 5. Naturalistic inquirers assert that personal values and assumptions influenced
initial problem selection, choice of methodology, values and culture that characterise
subjects and the inherent values in the inquiry context. All are mutually interdependent
and interlock with each other, akin to what Salomon (1991) calls reciprocal determinism.
Interaction between researcher and respondents created subjective understandings

45
mediated by personal values. The value-ladenness of inquiry therefore demanded early
identification and declaration of researcher values to strengthen the trustworthiness of
dialogue (Green, 2002).
Significance of context
In naturalistic inquiry, context grounds the “neuronal” web of interrelationships.
Because subjects take their meaning “as much from their context as from themselves”, all
studies should be conducted in their natural setting (Lincoln & Guba, 1985, p.189). To
ignore the complexity of the social environment is to “impoverish the evaluation” say
Frechtling and Sharp (1997, p.1-8). The inquirer’s plan to interact personally and
environmentally with the context gave rise to “profound responsivity and interactivity”
which allowed informants to recount “histories, anecdotes, experiences, perspectives,
retrospectives, introspections, hopes, fears, dreams and beliefs” in their own language based
on their own experience, a posture that supported emergence of greater in-depth emotive
data (Guba & Lincoln, 1981, p.130; Lincoln & Guba, 1985).
Trustworthiness
Any valid inquiry must be able to demonstrate its truth value, provide the foundation
for applying it and allow for external judgments to be made about consistency and
transparency of procedures, neutrality of findings and decisions. These combined qualities
are what Lincoln and Guba (1985) call trustworthiness which is a matter of concern to
readers of the inquiry’s final report. “Integrity is everything” says Delahaye (2000) and the
qualitative researcher should endeavour to observe, report and interpret the multiple realities
of informants “as accurately and as faithfully as possible” (p.161). If naturalistic inquiry is
to add to an overall body of knowledge, it must guarantee some measure of credibility about
the inquiry and report findings in a way that allows its audience to check on findings and the
process by which they were obtained (Erlandson et al., 1993). Any person wishing to use
findings as a basis to formulate recommendations must be convinced that the study is worthy
of confidence. To engender such confidence, credibility, dependability and confirmability
standards were built into the inquiry process.
1. Credibility was seen as an ongoing check between the interpretations of research
data and the multiple realities presented by informants. Pertinent to a naturalistic
inquiry is compatibility of these realities with those attributed to them by the
researcher. This relationship is called credibility. Credibility had to be established
with informants who provided data to ensure transcriptions rang true with members
of that setting. A credible outcome was one that adequately represented both the
areas in which realities converged and the points on which they diverged

46
(Erlandson et al., 1993). A credible inquiry was expected to be imprecise in terms
of definite boundaries and specific relationships but rich in deep meaning and
understanding. Engagement with the inquiry context, building trust, observation,
addressing personal bias and triangulation are field activities that increased the
prospect of high credibility. (a) Engagement with the inquiry context was intended
to build trust which required the researcher to reduce social distance and use
“middle-of-the-road strategies” to preserve integrity of the persons and situations
being studied (Erlandson et al., 1993, p.135). (b) Building trust and rapport
required the researcher to spend enough time at the inquiry site to overcome any
distortions due to her presence, become oriented to the context and generally allow
her to understand daily affairs in the way informants interpreted them. Building
trust was a developmental time-consuming process that involved reaffirming
informants that their confidences and close-to-the-heart secrets would not be used
against them, anonymity and third party identification issues would be safeguarded,
their interests would be honoured and they would be given opportunity to offer
input that may influence the inquiry process (Lincoln & Guba, 1985). As daily
activities became more predictable, the researcher tried not to lose sensitivity to
daily events or lose objectivity towards the setting and its members. She guarded
against becoming involved with informants to the degree that the research agenda
became merged with thoughts as an “insider” causing informant opinions, beliefs
and experiences to become indistinguishable from her own (Denzin & Lincoln,
1994). (c) Observation required the researcher’s notes to become the eyes, ears and
perceptual senses of the reader (Patton, 1990). Contextual observation allowed the
researcher to actively seek new leads and new sources of data. This demanded
researcher ability to seize the moment and take personal risks to expend energy,
driven by a strong sense of purpose and assertiveness (Lightfoot, 1983). (d)
Researcher bias based on prior values was addressed by the researcher. The best
cure for biases was to become increasingly aware of how they slant and shape what
we hear and how they can interfere with our reproduction of the informant’s reality
(Guba & Lincoln, 1981). Lack of researcher bias was essential to avoid evidence
being interpreted “to support a preconceived position” (Burns, 2000, p.470). The
researcher as investigator, perceiver, selector and interpreter had to be constantly
vigilant to guard against “distortions of bias and prejudice” (Lightfoot, 1983,
p.370). Douglas (1976) believes that society is a mixture of “the highly patterned
and the highly unpatterned, the cooperative and the conflictful, the open and
obvious and the secret and obscure” (p.56). Given the profound conflicts of
interest, values, feelings and actions that pervade social life, many people one deals

47
with have something to hide. The social researcher therefore relies on a
combination of cooperative and investigative methods, spending enough time in the
context to become oriented and overcome distortions caused by personal presence
so that daily affairs may be understood in the way informants interpret them. Since
the truth lay in the integration of various perspectives rather than in the choice of
one dominant voice, a deviant opinion was seen as an important version of the truth
and a useful indicator of what the culture defines as normal (Lightfoot, 1983, p.13-
14). (e) Triangulation seeks to check the accuracy of an item of information
derived from one source against one or more other sources. It may be viewed as a
corroborative technique that is useful for establishing credibility of findings and
interpretations (Eisner, 1979). When various bits of information all lean in one
direction, “that direction assumes far greater credibility” (Guba & Lincoln, 1981,
p.107). Conceding no observations or interpretations are perfectly repeatable,
triangulation serves to clarify meaning by identifying different ways the
phenomenon is being seen to confirm the story holds up, the pieces fit and make
sense and the facts are consistent (Flick, 1992). The best way to achieve this was to
gather information about different situations and relationships from different
vantage points with each piece of information expanded by at least one other source
(Erlandson et al., 1993, p.31). The greater the convergence attained through
triangulation of multiple data sources, the greater the confidence in observed
findings. Triangulation techniques included member checks, cross-case analysis
and research team collaboration and debriefing. (i) Member checks allowed
verbatim transcripts to be checked with those who provided the data. This allowed
the informant to confirm, correct or extend the information solicited. Member
checks put the informant on record as having agreed to the accuracy of the
researcher’s transcript of events thus making a future claim of misunderstanding or
investigator error more difficult (Lincoln & Guba, 1985, p.314). Member checks
should not be confused with triangulation though superficially, they appear
identical. Triangulation seeks to check the accuracy of an item of information
derived from one source against one or more other sources while member checks
test the credibility of the researcher’s transcript with the informants who provided
them (Lincoln & Guba, 1985). (ii) Cross-case analysis involved cutting across
individual cases in search of similar and different views. Researcher willingness to
openly consider other possibilities was essential to an overall constructivist-
perceptual view towards interpreting reality. Readers will make their own
decisions about divergent views and Patton (1990) believes the reporting of
alternative views is often among the most interesting section of the research report.

48
(iii) Research team collaboration and debriefing provided external checks on the
inquiry process. As researcher biases were probed, meanings explored and the
basis for interpretations clarified, team debriefers shored up credibility by ensuring
the investigator was aware of personal posture and values (Lincoln & Guba, 1985).
Engagement and observation at the inquiry site and triangulation activities were
considered the best means of operationalising the credibility criterion to ensure
interpretation of realities were verified by those who have afforded them
(Erlandson et al., 1993).
2. Dependability allowed for instability factors such as reality shifts and better
insights that may cause change but could be taken as error, to be taken into account.
Dependability was assessed from a meticulous audit trail which verified a record of
the inquirer’s judgments that were “not readily apparent to readers of an inquiry
report” (Guba & Lincoln, 1981, p.145).
3. Confirmability required the auditor to assess whether findings were grounded in the
data, inferences were logical, the category structure was logical and disconfirming
data were accounted for. Triangulation techniques and maintenance of a reflexive
journal that displayed the researcher’s mind processes, philosophical position and
bases for inquiry decisions discreetly dovetailed with the dependability and
confirmability audit trail (Lincoln & Guba, 1985, pp.327).
The human data-collection instrument
Naturalistic Inquiry uses the human investigator to identify salient elements through
interviews, observations and noting nonverbal cues transmitted through the interview process
(Lincoln & Guba, 1985). The potential of the human instrument is imbedded in their ability
to observe, categorise, discriminate and process many forms of data on explicit and tacit
levels. The ability to be responsive, flexible and view social entities holistically, to process
explicit and tacit knowledge and to seek out the usual and unusual is uniquely human.
Further, a human inquirer has unique opportunity to probe, delve, scrutinise or cross-
examine those statements that are unclear or need amplification. The “talking person” can
explain exactly what his last comment meant, the influences that framed the comment and
the background information that expands understanding of a particular event, feeling,
perception or situation (Guba & Lincoln, 1981, p.136).
Humans have one virtue lacking from all objective instruments and that is judgment,
along with the flexibility to use it (Guba & Lincoln, 1981). Moreover, the human instrument

49
can bring to bear all the power of his or her tacit understandings. For these understandings
to be used to their fullest extent there was frequent and meaningful interactions between
researcher and informants so that insights and experience inherent in tacit understandings
could be shared through interpersonal contact, without the researcher shaping participant
responses. Tacit knowledge is difficult to articulate, personal in origin, valued by the owner,
related to context, known in part and unknown in part by the owner and best transmitted
through personal interaction (Nonaka & Takeuchi, 1995). Liberty to tap this valuable
resource was highly dependent upon a trusting relationship between inquirer and informant.
Whether interviewing or observing, the naturalistic inquirer employs explicit
(conscious) and tacit knowledge (known only to the owner) simultaneously. Humans
capture, filter, sift, sort and process literally thousands of bits of explicit and tacit knowledge
every day to form a complex and meaningful whole (Guba & Lincoln, 1981, p.135).
Extending awareness of a situation beyond conscious knowledge to the realm of the felt
involves an internalisation process (Nonaka & Takeuchi, 1995). Once explicit knowledge is
lived or experienced by the individual, it becomes internalised or felt. It may produce new
insights for the researcher and lend depth and richness to understanding of social settings
which in turn may be communicated to the study’s audience.
Preferable human-as-instrument qualities
Empathy is the human characteristic most applicable to naturalistic inquiry and the
extent to which interviewers are able to communicate warmth and empathy often marks them
as good or not-so-good data collectors (Guba & Lincoln, 1981). It requires ability to
understand what the other person is experiencing, to feel some of what he feels and to share
to some degree “his view of his experiences” (Dexter, 1970, p.62). Empathy promotes
understanding and achieving understanding builds greater empathy in a reciprocal way
(Guba & Lincoln, 1981). Sensitive data usually involves recounting personal stories and is
made easier by an empathetic, warm, responsive listener. Without being aware of it, most
people would rather retain their own conclusions than learn anything contrary to them. A
good listener needs a genuine desire to hear what others have to say (Webb & Webb, 1975).
Failure to hear certain things and not others, to see or read something into a person’s actions
that is not there or failing to note what is clearly there by using “filters and selective
perceptions” undermines reliability (Guba & Lincoln, 1981, p.147).
The naturalistic inquirer needs ability to deal with the psychological stresses of work in
the field, the loneliness and isolation involved with data reflection and analysis, constant
examination of personal feelings and actions and their impact upon the research setting and

50
informants, the realisation that personal change is part and parcel of social inquiry and
willingness to undergo that change. Another valuable trait is willingness to talk and listen to
many different types of people and their views including individuals the researcher dislikes
and mistrusts (Guba & Lincoln, 1981). Information can come from unexpected sources.
Curiosity about everyone, the weak and the powerful, the ordinary and extraordinary and
those who initially do not seem central to the setting is more likely to strengthen rigor and
credibility by providing information that reliably depicts complexities in the social context.
A shortcoming of the human instrument with respect to dependability can be overcome by
adequate training and experience, various triangulation techniques and auditing processes,
any limitations more than compensated for by the richness of the data gathered. Only the
human instrument can describe situations and cultures that provide the reader with an
“empathetic and vicarious experience of what is must have been like to be on site” (Guba &
Lincoln, 1981, p.148).
Summary
Naturalistic Inquiry’s belief that context is the key to meaning demands a human
instrument who is capable of adapting to the complex dynamics inherent in that context.
Essential to this discovery-oriented approach is the inquirer’s intention to minimise
manipulation of the contextual setting by placing no restriction on what the research outcome
should be (Guba & Lincoln, 1981). The admission of informants’ tacit understanding is
highly significant and serves to strengthen and deepen understanding of the focus under
investigation. As the inquiry’s truth value is a matter of concern for readership of the study’s
final report and to any person wishing to use findings as a basis to formulate
recommendations, neutrality of findings and decisions must demonstrate consistency and
transparency of procedures. The credibility, dependability and confirmability standards
discussed are critical to generating such confidence and trustworthiness.
Data collection
Opportunity to tap into the knowledge, experience and insights of others in their natural
language and context is virtually impossible without face-to-face verbal interaction (Guba &
Lincoln, 1981). In this context, an interview is defined as a “conversation with a purpose”
(Back & Gergen 1963, p284). The data collection phase involved interviewing and
observation of contextual influences and nonverbal communication.

51
Interviewing
Naturalistic Inquiry presupposes that social contexts have pluralistic sets of values. The
interview structure must allow value systems and multiple perspectives to “arise from the
context in whatever way the respondents express them” (Guba & Lincoln, 1981, p.156).
Informal conversational interviews took the form of a conversation between informant and
researcher and focused on the informant’s perception of their experiences in their own
language (Burns, 2000). Free-flowing dialogue relied on the quality of interaction between
researcher and interviewee and direction was minimally controlled by the researcher to
ensure conversation stayed relevant to the interest of inquiry. The rationale behind informal
conversational interviewing was that the only person who understands the social reality in
which they live is that person (Burns, 2000). Conversational interviews allowed people to
share their stories, experiences, anecdotes and perceptions and they were made unobtrusive
by the way the inquirer proceeded. Allowing people to feel comfortable that their views
were legitimate, talking their language, addressing points of significance to them and
providing continuous reassurance to allay concern of evaluation encouraged openness and
natural interactions that were not seen as intrusive and intimidating (Wolf & Tymitz, 1977).
A strength of this flexible approach was its responsiveness to individual differences and
situational changes given researcher ability to interact easily with people, generate rapid
insight, formulate questions quickly and guard against asking questions that impose
interpretations upon the contextual situation (Patton, 1990). A major disadvantage of open-
ended interviewing was that the researcher was exposed to the informant’s interpretations
and presentations of reality. A further drawback was the time needed to collect data, as
Patton (1990) says “the gathering of field data involves very little glory and an abundance of
nose-to-the-grindstone drudgery” (p.265).
Phase 1 used conversational interviewing techniques because they allowed people to
share their perceptions in an unobtrusive way. Interviews were exploratory, a continuing
process of discovery as the researcher learned what issues were salient to the informant and
which needed further exploration in Phase 2.
Listening skills
Displaying empathy and acceptance, showing respect and creating an atmosphere of
trust encouraged the informant to enter a relationship in which it was safe to reveal real
feelings, thoughts and emotions (Burns, 2000). Good listening skills and attention to what
the interviewee was saying and feeling were considered the most important attributes of the
interviewer. Two levels of listening were involved (a) listening to the content of what was

52
expressed in words and (b) being sensitive to what was not stated in words but conveyed by
nonverbal signs (Delahaye, 2000). Since the informant provided the raw data about the
phenomenon under investigation, the inquirer listened very carefully and was at ease with
silence so as not to contaminate the outcome by intruding on the informant’s thinking time.
Burns’ (2000) caution against jumping to conclusions and allowing prejudices to impede
understanding was acknowledged.
Observation
The implied assumption behind observation was that the informant’s behaviour
expressed deeper values and beliefs (Burns, 2000). Dexter (1970) believes the interview is
more successful when the interviewer can obtain clues not only through verbal reporting of
personal experience but from “incidental observation of informant behaviours which allow
further insight into experience” (p.84). The interviewer tried to see the world from the
informant’s perspective and capture the perception phenomenon “in and on its own terms, in
its own culture and context” (Guba & Lincoln, 1981, p.193). There is no pure, objective,
detached observation say Denzin and Lincoln (2000) therefore all observation required the
researcher to become immersed in the world of the informant whilst managing her role as
interviewer and eliciting trust, openness and acceptance (Burns, 2000).
Nonverbal communication
Nonverbal communication was defined as the intentional or unintentional exchange of
information through non-linguistic signs (Guba & Lincoln, 1981). These speak louder than
words and are a valuable part of interview data (Burns, 2000). “It is not what one gains by
adding them but what one loses by ignoring them, for they are always there to be tapped”
(Guba & Lincoln, 1981, p.223). Collection of nonverbal data supplemented other collection
techniques because they acted as an immediate cross-check on everything else that was
observed or heard. If one considers that 66%-93% of all communication is nonverbal, a
good naturalistic inquirer should possess trained receptive capability to interpret these
unconsciously sent signals.
Interview questions
Two interview phases were conducted in one session. The Phase 1 overview phase
aimed to gather enough information from informants to understand what elements were
salient to them for follow-up. Phase 2 explored elements deemed salient in Phase 1 and an
interview guide was used to delve specific areas of research interest (Lincoln & Guba, 1985.

53
The object of conversational interviews was to get people to talk about experiences,
feelings and opinions and questions allowed informants to respond in their own language.
As questions became more specific as the interview proceeded, the interviewer had to decide
what questions to ask, how to word them and how much to solicit (Lincoln & Guba 1985).
Opinion or value questions were aimed at understanding a person’s cognitive and
interpretative processes “what do you think about …” while feeling questions aimed to
understand the person’s emotional response to experience (Patton, 1990, p.291). “What is
your opinion about that” demanded an analytical interpretative reply while “how do you feel
about that” was a question about feeling. Phase 1 open-ended questions relied on the
inquirer’s ability to paraphrase important points for probing in Phase 2. Paraphrasing
involved repeating key points in the informant’s message back to them to assure them that
their message was understood. Key points for follow-up in Phase 2 were carefully noted.
Interview guide
An interview guide is an inventory of specific points of interest that the interviewer
wishes to explore, probe and ask questions about to illuminate a particular topic (Loftland &
Loftland, 1995). It ensured that the same basic lines of inquiry were pursued with each
person (Patton, 2002). The interview guide used a semi-structured format and for this
reason, Phase 2 interviews were regarded as guided conversations (Loftland & Loftland,
1995). To elicit in-depth data, an important point raised in Phase 1 was used as the “stem”
of a Phase 2 question (Delahaye, 2000, p.170). Answers to secondary questions were
paraphrased until the researcher was satisfied the point has been fully explored.
Note-taking
Note-taking was not so extensive and absorbing that it deflected attention from the
interviewee (Dexter, 1970) nor did it cause the pace of the interview to become non-
conversational (Patton, 1990). “The best notes in the world will never achieve the same
results as the listener who is able to immerse himself in the respondent’s frames of reference
… and hear clearly and accurately what another is saying without overlays of values,
attitudes, preconceptions, stereotypes, beliefs or prejudices … ” (Guba & Lincoln 1981,
p.176).
Tape recording
Erlandson et al. (1993) suggest gathering data in a way that presents the most complete
picture without allowing procedures to obstruct access to additional data that may be needed.
A tape recorded interview eliminates a major source of interviewer bias, that conscious and

54
unconscious selection of what material to note. Judicious use of a tape recorder ensured
interview completeness by capturing all that is spoken together with nuances, direct
quotations, examples and nonverbal cues to improve reliability and accuracy. Tape
recording also afforded the interviewer opportunity to remain focused during the interview.
Advantages were expected to outweigh disadvantages but nevertheless the researcher
remained sensitive to any sign of boredom or intimidation.
Member checks
Naturalistic inquiry takes its strength from the separate realities constructed by different
individuals which must be “given status” in the lives of those individuals and in the contexts
in which they operate (Guba & Lincoln, 1989). Interview transcriptions were clarified and
checked through the member checking process in a fair and unbiased way. Corroboration
with each informant tested the accuracy of interview transcripts and provided opportunity for
expansion before the data analysis phase.
Data analysis
Data analysis involves description and interpretation. Objective descriptive analysis
comes first and demands detailed hard work to put together coherent answers to descriptive
questions (Patton, 1990). Analysis began with the very first data collected and this
facilitated later data collection phases. This interaction between collection and analysis is a
distinguishing feature of naturalistic research that continues until the study’s end. In a sense,
tomorrow’s work was “refashioned on the basis of today’s insights” (p.273). Data collected
was viewed as constructions of informants that lead to reconstructions when analysed.
Inductive analysis attempted to make sense of a situation without presupposing in advance
what main issues would emerge from the cases under study. An inductive approach
therefore allowed a focus on the individual’s experiences without imposition of prior
expectation in advance of the fieldwork (Patton, 1990).
Data interpretation
Interpretation goes beyond descriptive data. It involved attaching meaning, value or
significance to what was found, offering explanations, answering “why” questions and
dealing with conflicting explanations and data irregularities as part of testing the viability of
an interpretation (Patton, 1990). To strengthen trustworthiness of dialogue, the value-
ladenness of data interpretation demanded early declaration of researcher values (Green,

55
2002). Because observational interpretation was shaped by the mood, experience and
intention of the researcher, Stake (1995) believes “research is not helped by making it appear
value free. It is better to give the reader a good look at the researcher” (p.95). The
researcher’s theoretical lens was made explicit to the extent to which personal experience
and insights were relevant to informing the study’s purpose, the topics explored and
interpretation of data.
Grounded theory
Grounded theory takes the researcher into the real world of informants. It works
because such theory fits the practical situation from which data have emerged. It is
understandable to sociologist and laymen and cannot be derived without the openness that
characterises naturalistic inquiry. The generation of categories was a contribution to theory.
Ideas and concepts discovered in the data and categories that became apparent were woven
by the researcher into “fabrics of theory” (Denzin & Lincoln, 1994, p.447). Tacit knowledge
played a part by allowing the researcher to articulate theory based on units of information
judged valid for inclusion, units that may have otherwise been omitted. Explanations,
triangulating tests, little ideas “hardly worth calling theories”, once identified as units of
information, were hung onto. Together, they linked with other theories to provide
understanding of the text and “make the story” (p.449). This network of concepts, evidence,
relations of concepts where theory data and explanation unite, resembles the human
explanatory belief system where a person reflectively “constructs an explanation, a story for
and from data” (p.449).
Case study mode
Case studies resonate with the principles that underpin naturalistic inquiry. They are
primarily directed towards an “emic posture” and their capacity to seek out, interpret and
reconstruct meanings held by insiders is strong (Lincoln & Guba, 1985, p.359). By assisting
readers to construct new knowledge, case study mode asserts knowledge is socially
constructed. Each unit of information entered into the case provides another “point of
leverage from which to test interpretations” and thus affords the reader opportunity to probe
trustworthiness and factual consistency (Lincoln & Guba, 1985, pp.359-360). Case study
reporting provided opportunity for the researcher to demonstrate interaction with the inquiry
site and state personal values and perspectives so that personal biases could be made explicit.

56
Most naturalistic case studies emphasise “objective description and personalistic
interpretation” mediated by respect and curiosity for diverse perceptions and realistic
description of the local context (Denzin & Lincoln, 1994, p.242). A distinguishing feature of
case study mode is belief that each human system is an individual entity whose characteristic
wholeness requires a thorough investigation of the interdependency of parts (Sturman, 1999).
Case study reports resemble portraits for they must capture the essence and multiple aspects
of the informant, situational features, values and connections between persons and can
provide very engaging, rich explorations of a phenomenon in its real-world setting
(Flechtling & Sharp, 1997). Due to a need for thick description and integration of data from
multiple sources (Lincoln & Guba, 1989), case study reports are longer than those typically
encountered and researcher prerogative ultimately decides what is necessary for an
understanding of the case and what of the case’s own story will be reported. Cases may be
similar or dissimilar, “redundancy and variety each having voice” (Denzin & Lincoln, 1994,
p.237). Each examined multiple realities and thick description provided “a window of
meaning” into the lives of informants to allow the reader to connect with common
experiences and unique differences, the real business of any case study being
particularisation not generalisation (Green, 2002, p.14).
Thick description
Thick description may be defined as “generous, fertile, abundant and above all accurate
portrayal of the events, persons and contexts” that forms the inquiry site (Guba & Lincoln,
1981, p.152). It must have depth and detail with sufficient factual and accurate descriptions
for the reader to enter the situation under study. It should depict contextual interrelationships
and complexities by describing everything the reader needs to know to understand findings
(Erlandson, et al., 1993). This meaningful way of sharing rich detail and insight invites a
more active role for the reader by creating a scene remarkably close to that gained by direct
contact with the site (Erlandson et al., 1993). If findings are interpreted in terms of thickly
described contextual factors and influences, the researcher must use all senses to “look,
listen, smell and feel the surroundings and interaction” (Guba & Lincoln, 1981, p.146), in
other words, one must see the forest and the trees.
Audit process
The audit trail required a deposit of records stemming from the inquiry (Lincoln &
Guba, 1985). Files that represented the phenomenon under study contained the sum total of
information from which findings were derived and since these were the closest the auditor
57
could get to the context, the study’s credibility was strongly influenced by them (Erlandson
et al., 1993). Access to six types of files that provided documentation and a running account
of the inquiry were built into the trail.
Three files represented the phenomenon under study:
1. Raw data included audiotapes, verbatim interview transcripts and reflexive journal
notes;
2. The unitising process displayed units of information typed in text boxes;
3. Data reconstruction showed synthesis of journal notes with units of information
already allocated to provisional categories.
Two files represented the inquiry procedures:
1. Methodological journal notes described decisions and accompanying rationale,
daily schedules and logistics of the study;
2. Personal diary notes described the researcher’s intentions and motivations.
This audit process allowed the auditor to attest that the inquiry’s category system was
derived from generally approved procedures, the category set made sense in view of the data
from which it emerged and that data were appropriately assigned within that set (Guba &
Lincoln, 1981, p.97). Once all steps were concluded, the auditor reviewed all findings with
the researcher to allow any errors of omission to be rectified. Of critical importance to the
audit trail was that no fact was reported without noting its source and no claim was made
without supporting data (Erlandson et al., 1993).

58
METHOD
Part II
This section explicates the methods that were used during recruitment, data collection,
member checking, analysis and interpretation phases, culminating with a final audit to check
that all practices and procedures fell within the bounds of good professional practice.
Qualitative problem
The general impression of children with shunted hydrocephalus and spina bifida is they
are fluent talkers, very sociable, good at memorising auditory information and they learn best
with verbally presented information with high levels of repetition (Dunning, 1992).
Practicing paediatrician and psychologist Loomis (2003) says these children normally do
well during the early years of primary school but fall behind as task demands become more
complex and abstract, and many struggle with a Nonverbal Learning Disability. Right
hemisphere dysfunction is believed to affect planning, organising and problem solving
abilities, the ability to process social cues and follow multi-step directions and the ability to
generalise. These interacting factors present a confusing state for educators.
Based on clear ability to generate fluent speech, educators and parents develop
expectations and goals that often cannot be achieved without extensions of time and/or one-
on-one support. A review of literature indicates the clearly articulated speech that
characterises individuals with shunted hydrocephalus and spina bifida causes misperception
of real performance ability. For teachers and aides, the difference between an illusion of
competence and on-the-job ability is difficult to explain. This state of affairs may be
considered a conceptual problem that begs additional understanding (Guba & Lincoln, 1981,
p.88). Given that all forms of inquiry emerge in response to perceived problems, the
following research question was created to include significant contributors to the quality of
each student’s learning experiences.
Research question
How do teachers, teacher aides, parents and students perceive the educational experiences of
5 students with shunted hydrocephalus and spina bifida?
59
Determining selection site
In terms of a qualitative study, a homogeneous group dictated that purposefully selected
participants be recruited from a site where members share the defining characteristics of
interest (Cresswell, 2002). Consent was granted from Spina Bifida and Hydrocephalus
Queensland to recruit through the association’s membership database. Ethical approvals
were later granted from the Mater Hospital and Royal Children’s Hospital to recruit through
hospital spinal clinics.
Primary participant selection
Primary selection criteria:
1. Aged between 9-16 years in mainstream schooling;
2. With shunted hydrocephalus related to spina bifida;
3. Who speak and read well;
4. Who have trouble with maths and handwriting;
5. Who live in southern Queensland.
Rationale:
1. Aged between 9-16 years in mainstream schooling. Ages 9-16 years covers
the age-range of proposed students in primary and secondary classes which
incorporates transitional periods of a young person’s life. Of interest was the
transition from primary to secondary school. The research focus was on children
who present atypical profiles in mainstream classes;
2. With shunted hydrocephalus related to spina bifida. Individuals with shunted
hydrocephalus were expected to exhibit virtually all assets and deficits that
underpin manifestations of the NLD syndrome (Tsatsanis & Rourke, 1995);
3. Who speak and read well. Good speaking and reading abilities are primary
assets of a student with an NLD;
4. Who have trouble with maths and handwriting. These identifying features
increased the likelihood that each individual would have some degree of an NLD;
5. Live in southern Queensland was chosen for practical data collection reasons. This
criterion permitted a visit to each participant’s home to conduct interviews and it
made access to the Mater Hospital for psychological assessment easier.

60
Participant selection
A final subgroup of 5 students aged 9-16 years who shared defining characteristics was
recruited. A four-tiered approach was adopted to achieve a homogeneous subgroup with
defining features. Each successive stage extended information already obtained only after
previous characteristics were assessed and analysed.
1. Initial telephone conversation. Parents of individuals who met these criteria
were invited to contact the researcher. This conversation permitted the researcher
to explain her role, confirm the purpose of the study, and discuss the data
collection process, informed consent, and ethical issues. It provided opportunity
for the researcher to confirm (a) a presence of a shunt for hydrocephalus (b) spina
bifida classification (c) age, school and year level (d) school-ascertainment
conducted (e) identifying attributes such as:
• Did the student speak well?
• Did the student have trouble with maths for example; could he or she
calculate $50 - $16.50?
• Did the student have trouble completing school and homework tasks?
• Does the student have trouble with handwriting; can he or she write a
whole page?
• Did the student have trouble with planning, organisation and managing
time?
• Did the student have trouble with coordination e.g. clumsy, awkward?
• Did the student have trouble with many everyday tasks for example,
tying shoelaces, following directions, using scissors?
• Did the student have trouble with crossing roads?
• What about concentration and memory?
• What about friendships?
• Developmental history (a) walking and talking age, (b) level of
mobility, educational experiences
• What assessments were conducted and the year conducted?
• Would the parent give the researcher access to assessment information
for the research purpose?
• Would the parent give permission for student to participate in some
additional testing?
• Would the child be willing to participate in one test session at the Mater
Hospital?

61
A good informant was one who had the characteristics the researcher required, the
ability to articulate experiences, time to be interviewed and who was willing to participate.
The following outlines the continuous refinement process:
1. Homogeneous group. Individuals who showed strength in the areas of auditory
perception, rote memory and simple motor skills and limitations in visual-spatial-
organisational perception, psychomotor, problem solving, language and academic
areas were identified;
2. Identifying the students for the study. The focus of investigation was on
perceptions of children who appear verbally bright but share features of an NLD.
Because children with NLD are keen readers and usually display a good
vocabulary, teachers are not prompted to consider a learning disability. Excellent
rote memory skills add to the dilemma for teachers and parents and because
language-based skills are highly regarded by the community at large, a learning
disability that involves the nonverbal areas of functioning is not identified. An in-
depth exploration of teacher, aide and parent perceptions of this profile therefore
depended on selection of students whose strengths and weaknesses bore
resemblance to the NLD profile. Current psychological assessments and
telephone responses were reviewed by the research team and used to identify
suitable students. Potentially suitable students without assessment conducted
within the past 24 months were included on the basis of parental telephone
responses;
3. Final homogeneous subgroup. The final homogeneous subgroup of 5 students
whose psychological profile resembled the NLD profile were selected and invited
to participate. Having met the blueprint of characteristics, it was hoped the
subgroup would remain constant but in the event of early attrition, contact details
of other willing young people were retained.
Data Collection
Researching student perceptions was a potent way of challenging assumptions
(Dawtrey, Holland & Hammer, 1995). “Those who have researched student perspectives
over the years have been astonished at the mature and serious way the vast majority talk
about their school and learning experiences” (Hargreaves, 2004). Perceptions of students
are unique to themselves and exclusion of the young person’s articulation of their learning
experiences from this study would severely undermine the validity of teacher and parent
perceptions. Ruddock, Chaplain and Wallace (1996) argue with conviction that the voice of

62
students is of fundamental importance in developing improvements to school strategies yet it
is infrequently reported in an overt manner. Despite concern about reliability of information
gathered, Crozier and Tracey (2000) say there has been “increasing and overdue interest in
hearing the voices of young people themselves about their educational experiences” (p.174).
What should be endorsed is a structure of agency where children are recognised as people in
their own right and should therefore been seen as active constructors of their own social
worlds, capable of reflection and understanding about its meaning and importance to their
own lives (James & Prout, 1996).
As consumers of school policy and curricula, young people are capable of analytical
and constructive observations and of responsibly identifying factors that hinder their learning
(Ruddock et al., 1996). Implications for policy, school and classroom practice are therefore
flawed if based only on teacher, teacher aide and parent assumptions about students’
educational experiences without seriously listening to the versions of young people. Because
the meaning that students attach to educational experiences may not necessarily be the same
as that of teachers, aides and parents, it was an inconceivable proposition to exclude the
voice of students as active participants from this study.
Traditionally, children’s thinking has been viewed from the vantage point of adult
perspectives and according to Mayall (1996), it is commonplace to find that the child’s voice
is “simply omitted from academic sociology” (p.163). To make the young person the centre
of focus, the researcher recognised and accepted that children are competent reporters of
their experiences and capable of reflecting upon them. When analysing data from students,
children’s views were taken seriously, the aim of “doing the research and writing it up was to
work for children rather than on them” (Mayall, 1996, p.12).
Human data collector
The researcher utilised informal conversational interviews, observation and nonverbal
cues to collect data. The purpose was to elicit information about parent, student, teacher and
aide concerns, beliefs and understandings. Qualities such as empathy, warmth, careful
listening and ability to “shift gears” were continuously cultivated, sharpened and refined by
the researcher (Dexter, 1970, p.62).

63
Gaining consent from parents and students
The initial contact with parents was a Letter of Introduction, Study Description and
Consent Form sent out by Spina Bifida and Hydrocephalus Queensland, the Royal
Children’s Hospital and the Mater Children’s Hospital. See Appendix G.
If children are seen as a social group within society, they have rights and entitlements
of their own including the right to speak for themselves and to be listened to as a group
(Mayall, 1996). Reliance on the consent of others denies a child informant information
considered essential to an adult participating in research. Further, it denies the child
opportunity to clarify the aims of the research and how he or she might contribute and to
decide whether or not they want to participate (Masson, 2000). For these reasons, the
researcher afforded due respect for the student’s rights to understand the purpose and nature
of the study before making a voluntary choice to participate. To do this, a Letter of
Introduction, Information Sheet and Statement of Assent were forwarded to each student in
addition to gaining consent from the parent or caregiver. Although this kind of
documentation had no standing as an informed consent mechanism, it was intended to
provide students with a greater sense of ownership. See Appendix G for Information packs.
Setting up teacher and teacher aide interviews
Ethical approvals to contact school principals regarding communication with teachers
and aides were granted by Education Queensland and Catholic Education. A Letter of
Introduction, Study Description and Consent Form was forwarded to each principal together
with a Teacher Information Pack for his or her approval. Once permission from the school
principal, parents and students was granted, the researcher sent information packs to
respective teachers.
At the start of each interview with parents, students, teachers and aides, the researcher
answered questions and explained benefits and risk protection. Exploration of teachers and
parent and student perceptions of the educational experiences of young people with shunted
hydrocephalus and spina bifida gave voice to all informants. Responses revealed
impressions and insights foremost in the informant’s mind considered worthy of reporting.
The researcher provided assurance that measures to safeguard ethical and confidentiality
issues were approved by the University Human Resource Ethics Committee (UHREC).

64
Consent mechanism
Informal conversational interviews, note taking, tape recording and observation
techniques all raised ethical issues about researcher conflict of interest, intellectual disability,
health risks, reciprocity, respondent identity, informed consent and confidentiality with
respect to school identity, confidentiality, anonymity and third party identification.
1. Researcher conflict of interest. The researcher and her daughter are members of
SBHQ. To guard against a conflict of interest, the researcher explained that her
role as data collector was to explore how learning experiences were perceived in
school and home settings.
2. Disability. Students’ intellectual status was unknown at the time of interview. This
was addressed by including a Letter of Introduction and Information Sheet in each
Information Package written in comprehensible language to the student.
3. Health risks. Because all students who attended the Mater Hospital for testing had
shunted hydrocephalus and spina bifida, a parent or caregiver was invited to
accompany the student. This allowed Adaptive Behaviour and Executive Function
questionnaires to be completed by the parent or caregiver.
4. Respondent identity: Every precaution was taken to ensure confidentiality.
Personal names and names of schools were substituted with pseudonyms.
5. Confidentiality. All reasonable precautions to protect confidentiality of interview
data during analysis, integration and interpretation phases were exercised.
6. Anonymity. When reporting and using direct quotations, anonymity was protected
by not making any informant recognisable through some contextual reference.
Denzin and Lincoln (1994) advised to present demographic data “in aggregates” so
that identifiers such as gender, age, class were not linked and consistently
associated with the same participant through the study even though a pseudonym
was used (p.232). Before entry into the final report, identification of persons,
places and contexts was scrutinised so that dramatic changes could be made “for
the sake of the more general readership” (Lincoln & Guba, 1985, pp.370-372).
Building rapport
Developing and keeping rapport was a process of continuous negotiation that required
the researcher to make conscious adjustments to meet the emerging needs of the inquirer-
informant relationship. The goal of establishing rapport was to reduce distance, anxiety and
build trust so the researcher could achieve ends determined by the research purpose. This
65
relationship was therefore asymmetrical as the researcher worked to achieve rapport to
accomplish ends shaped by the research needs (Glesne, 1999).
Maintaining rapport required the researcher to become familiar with the “landscape”,
the social and political structures of the site that shape behaviour. During initial contact with
parents and school principals, she was sensitive to family and school protocols, and to
reception of her visit. Fitting in was not a challenge and the researcher ensured she
constantly monitored her behaviour, facial expressions and tone of voice and she always
agreed with informants even if their views offended her personal values and beliefs. Measor
(1985) suggested presenting as sweet and trustworthy “but ultimately rather bland” (p.62).
Building rapport with students
Feeling empowered to speak required a supportive environment and researcher
willingness to recognise certain factors that create differences between adults and youth
(Lloyd-Smith & Tarr, 2000). Accessing and understanding the complexity of the student’s
world (France, Bendelow & Williams, 2000) and how the researcher was perceived by the
student were crucial to bridging this gap. Four key factors were considered before
interacting with young people:
1. The inquirer talked informally with the young person before starting the interview
to help build the relationship. She asked questions about everyday events to show
she was interested in what the young person had to say;
2. The inquirer presented in a role of “naïve curiosity which was honest, open and
empathetic” and without tendency towards patronage (p.152);
3. The inquirer avoided a judgmental attitude about people’s behaviour and beliefs.
4. The inquirer encouraged views that were challenging or different and provide
opportunities to explore the complexity of issues.
Twenty-two years of individual and group music teaching and many coaching
relationships that spanned 7, 8 or 9 years of tuition for individual students afforded
opportunity for the researcher to work with a wide range of abilities in the 6-89 year age-
range. The success of working relationships could be quantitatively measured by a high
percentage of honours grades and many high distinctions awarded to approximately 200
students over a 22-year period. A combination of teaching experience and familiarity with
students who experienced sensory, intellectual and physical disabilities equipped the inquirer
with enough understanding to build rapport and respond to any uncertain situations that may
have arisen.

66
Shared interests and reciprocity
Sharing interests and getting people to talk about them was an important element in
building the research relationship because it got people talking (Measor, 1985). To
compensate for time constraints and to help the informant to feel comfortable, a short period
of time was allocated to have a chat with each teacher, aide, parent and student before
starting the “Self Introduction and Starting the Interview” phase.
As teacher, parents and students willingly gave time, shared stories, feelings and views,
the researcher was concerned about ability to reciprocate. Glesne’s advice was aptly used
“What you do have that they value is the means to be grateful by acknowledging how
important their time, cooperation, and words are by expressing your dependence upon what
they have to offer and by elaborating your pleasure with their company” (1999, p.127).
Giving feedback depended on the nature of the relationship between interviewee and
researcher. The researcher erred on the side of less rather than more feedback, noting
Patton’s warning that if negative feedback was wrong, “it is long remembered and often
recounted” (1990, p.269). The researcher adopted a non-directive role to learn participant
and respondent beliefs, experiences and views. On occasions, opportunity to express
personal views offered therapeutic benefit and given the researcher’s background, it was part
of what she could offer back to informants (Patton, 1990).
Tape recording
Tape recording ensured no verbal productions were lost and it provided opportunity to
review whenever necessary to reach full understanding. Prudent use ensured the researcher
remained sensitive to any sign of intimidation, intrusion or constrained responses. The
irreplaceable nature of interview data dictated that two copies of each original recording
were made. One copy was stored immediately after each interview. The researcher
transcribed the tape recording as soon as possible after the interview.

67
Starting teacher and parent interviews
To help the teacher or parent feel comfortable when starting the interview, the
researcher explained the study’s purpose and her interest in the inquiry and consent to
participate and tape record the conversation were affirmed. Each parent and teacher was
advised (a) how he or she came to be selected, (b) that personal names and name of school
would be replaced with pseudonyms, (c) that all information in the final report would be in a
de-identified form,
(d) that he or she could interrupt, ask questions or ask for something to be made more clear,
(e) that he or she could withdraw and the decision would be respected, (f) that a transcript of
each interview would be offered and he or she had the right to change things in it (Measor,
1985).
Listening skills
To communicate active listening, the researcher focused attention on the informant.
One needed to think about further probes, link current talk with what had already been said
and think ahead to frame new questions that arose from new data (Lofland, 1971). Issues
raised in the initial phase were expanded in the interview guide to take account of new leads
as the interviewer solicited more depth and description. To enhance listening and attention
to what the informant was saying, the inquirer employed attending, responding and
understanding skills (Brockett, 1983).
Attending required active listening, eye contact, showing genuine concern, paying
attention to nonverbal behaviour and promoting an atmosphere of relaxation. The inquirer
sat facing the informant to give the message that she was paying full attention. She sat with
a gentle lean forward to indicate she wanted to understand the informant’s message and was
willing to accept all information in a non-defensive way. Eye contact distance between
informant and inquirer was approximately one metre (Delahaye, 2000). Responding
involved being sincere, empathetic and responsive to what was spoken, showing respect, and
being non-judgmental. Understanding between both parties resulted from establishing good
rapport with the interviewee (Brockett, 1983).
Self-introduction for teacher and teacher aide interviews
“My name is Barbara Rissman. I used to be music teacher but now I’m doing research
at QUT. I have worked with students with sensory, physical and intellectual impairments
and many who were not physically or intellectually challenged and I used to prepare them

68
for state music examinations. I find students with hydrocephalus and spina bifida interesting
because the ones I know have good verbal and rote memory skills but they have trouble with
writing tasks, mathematical concepts and handling some everyday tasks. Research studies
frequently report these characteristics. I am interested to hear your perceptions of …
learning experiences and the valuable insights and experience you have gained that may be
helpful to young teachers ‘learning the ropes’. I’ll also be talking with other teachers of
students who have hydrocephalus and spina bifida”.
Self-introduction for parent interviews
“My name is Barbara Rissman. I used to be a music teacher but now I’m doing
research at QUT. When I was a music teacher, some of my students had difficulty with
hearing, vision and learning new theory concepts. I find children with hydrocephalus and
spina bifida interesting because the ones I know speak well but they find handwriting,
mathematical concepts and some everyday tasks quite difficult. Research studies frequently
report these problems with children who have a hydrocephalic condition. I am really
interested to hear how you understand … learning experiences and the methods you have
found useful when teaching … something new. I’ll also be talking to other parents of
children with this condition”.
Interviewing students
Interviews with parents and students were conducted on the student’s home ground
(Nesbitt, 2000), one advantage being that the student was not be influenced by the proximity
of teachers, teacher aides and classmates (Christensen & James, 2000). As a guest in the
family’s home and with a desire to fit in, the inquirer reassured parents by allowing them to
be present at the interview if they wished, while being aware that children’s answers may be
influenced by the presence of parents or siblings (Christensen & James, 2000). Observable
benefits were that parent and student discussions sometimes triggered recall of buried events
which provided further insight and description of happenings.
The opening questions in Phase 1 were designed to relax the student and build
confidence. In designing Phase 2 questions, attention was given to posing questions that
explored areas of importance in a non-threatening and unambiguous way, for example “Tell
me about …” Interviews were interposed with pauses and prompts. Some of the best
insights into children’s perspective were stimulated not by the questions designed to explore
that aspect of experience but by some other question. In this event, attentive listening
facilitated shifting gears with the student (Dexter, 1970). To increase internal validity with
respect to contentious responses, the researcher occasionally asked similar questions at

69
different points in the interview to ensure the student gave similar answers (Costley, 2000).
Care was taken to ensure questions related to the child’s developmental status at the time of
interview.
Starting student interviews
The researcher explained the study’s purpose and her interest in the inquiry. The
student’s consent to participate and tape record the conversation was affirmed. The
researcher advised the student (a) how he or she came to be selected (b) that personal names
and name of school would replaced with false names (c) that all information in the final
report would be in a de-identified form, (d) that he or she could interrupt, ask questions or
ask for something to be made more clear, (e) that he or she could withdraw and his or her
decision would be respected, (f) that a transcript of each interview would be offered for him
or her to check, change or extend.
Self-introduction for student interviews
“My name is Barbara Rissman. I used to be a music teacher but now I’m doing
research at QUT. During the 22 years that I was a music teacher, I worked with children
who had difficulties with hearing, sight and learning new theory concepts. I find children
with hydrocephalus and spina bifida very interesting because the ones I know speak really
well but they find writing and some everyday tasks quite difficult. I’m going to be talking
about learning experiences with other children who have shunted hydrocephalus and I
wonder if you would mind helping me with my work?”
Listening to students
Good listening skills and comfortable pauses and prompts such as “ah”, “cool”,
“awesome” and “really” were important when interviewing young people. They allowed the
student to feel there was time for them to think and they provided reassurance that the
researcher was paying attention without shaping their responses (Nesbitt, 2000, p.146).
Attentive listening familiarised the researcher with the student’s language and “patterns of
idiom”, some of which were adopted by the researcher to reduce distance (p.146).
Observation
Participant observation was interpolated with the interview process in the early stages
as the inquirer became immersed into the informant’s world. It involved directly observing
the setting and participating in the sense that interviews with informants were considered
part of the process of observation with both parties aware of their inquiry relationship (Guba
70
& Lincoln, 1981). Concrete and detailed observational notes were made by the researcher
(Denzin & Lincoln, 2000).
After each day of interviewing, the researcher reflected, analysed and noted personal
feelings and impressions in a reflexive journal (Glesne, 1999). Reflective and analytic
thoughts and wonderings that came to mind at other times were also recorded because they
contributed to identifying problems and developing new questions (p.53).
Nonverbal communication
Different observers may attribute different meaning to a particular nonverbal sign and
caution was exercised during interpretation. Fidgeting, moving about, getting comfortable
are nonverbal cues that could indicate attention and concentration difficulties, rolling the
head and/or the eyes and slow responses may indicate information-processing difficulties.
After leaving the data collection site, additional observations and relevant aspects of
nonverbal communication were noted.
Noting techniques
Sparse notes, key words and names used during the course of the interview were written
which allowed the researcher to keep a close eye on what had been talked about and what
remained to be talked about (Lofland & Lofland, 1995).
Interview Process Phase 1
In Phase 1, questions were the “grand tour” type (Spradley, 1979, p.86). They did not
presuppose which feelings or thoughts should be salient for the interview. To keep the
interview productive, the researcher remembered that the person being interviewed was the
expert on what he or she knew, understood, and felt (Erlandson et al., 1993). Questions were
asked in an open-ended fashion that established the territory being explored but allowed the
interviewee to use whatever words they wanted to express their thoughts (Patton, 1990).
An attitude that was interactive and responsive allowed informants to relate their
stories, experiences, views, hopes and fears in their own language based on their own
experiences (Lincoln & Guba, 1985). This inspired greater in-depth descriptive and emotive
data to enrich understanding and provide vivid detail of real-world experiences. The
interviewer tried to speak in the informant’s language and think about what would make
sense and be most acceptable to them. Concentrated attention on the informant allowed cues

71
and hints that may indicate a jump to another topic to be noted and keen listening allowed
the researcher to make any transition with the informant (Dexter, 1970). Flexibility to
follow new leads or return to earlier points was maintained by an easy rhythm and a great
deal of talk time for the respondent.
Phase 1 open-ended questions
Parents
“What’s a normal day like for …?”
“Are there any critical issues that I should ask you about first?”
“What sorts of things does … enjoy doing most?”
“What sorts of things tasks does … find most difficult?”
Students
“I’d really like to know what you think about school”
“Tell me some things I should ask you about”
“Tell me about the things you like doing most?”
“Tell me about the things you don’t like doing?”
Teachers
“What’s a normal school day like for …?”
“Are there any critical issues that I should ask you about first?”
“What tasks does … enjoy doing most?”
“What tasks does … find most difficult?”
Phase 2 Interview Guide
Phase 2 interviews followed Phase 1 interviews on the same day. The rationale for
using an interview guide was to gather teacher and parent perceptions about the student’s
ability to handle the cognitive and functional tasks that underpin the NLD profile. Semi-
structured protocols followed up important issues raised in Phase 1 before investigating
activities that had an NLD focus. Question order was flexible to allow a smooth flow of
discussion (Costley, 2000). When potentially sensitive or embarrassing issues arose, the
interviewer tried to follow these up towards the end of the interview in the hope that trust
and rapport had built up through the course of the interview (Lofland & Lofland, 1995).
Probes such as “Tell me more about …”, “You mentioned …”, “What happened next?”
were used to expand previously raised topics of interest. Incoherent pumps such as “umm”,
72
“uh-hah” and calls for reactions to the researcher’s version of what was said “Do I
understand you to say …” were used to increase confidence and elicit greater detail (Patton,
1990, p.271). Minimal encouragers combined with nonverbal communication techniques
such as eye contact and head nods were used to reassure the informant that the interview
context was warm and accepting (Burns, 2000). At times, comment was invited by
introducing topics with “Some people believe that …”, “I’ve been talking to some other
people and they’ve mentioned some things we haven’t talked about. I’m wondering if you
would mind reacting to these” (Guba & Lincoln, 1981, p.179). The researcher tried to avoid
leading questions or questions that communicated what she believed to be a preferable
answer such as “don’t you think that …” instead of “what do you think about …” (Glesne,
1999).
Phase 2 Interview Guide questions for parents
The set of issues to be explored was outlined before interviewing began – classroom
activities, homework, group work, everyday tasks, friendships, relationships with teachers
and classmates, anxiety and parent observations. Issues raised in Phase 1 and new questions
were introduced with “Tell me how … manages with …”
Classroom activities
Handwriting tasks
Maths
Concentration and memory
Homework
Getting started and getting it finished
Assignments
Planning, organisation and managing time
Working in groups
In the classroom
Everyday tasks
Scissors
Getting dressed and undressed
Preparing food in the kitchen
Home Economics classes
Crossing roads and keeping safe in the community
Lunchtimes and social
Friendships (special friend, invitations to parties, school socials)
“Does … go on school camps and does he/she enjoy them?”

73
“Does the school have a policy about who should/should not push the wheelchair?”
Relationships at school
“How do you feel … gets along with teachers?”
“How do you feel … gets along with teacher aides?”
“How do you feel … gets along with classmates?”
“How do you feel teachers and teacher aides understand …?”
“Do you go to IEP meetings for …?”
“How do you feel classmates understand …?”
“Do you have much opportunity to talk with teachers and teacher aides about …
needs and progress and any difficulties he/she may experience?”
“Do you feel … is getting the help he/she needs at school?”
“Have teachers and teacher aides had some help with classroom strategies that might
help …?”
“What do you think would help teachers and teacher aides to understand … learning
needs better?”
“Has anyone from the Spina Bifida Association visited the school?”
Anxiety
“Does … experience any anxiety-related problems eg getting to sleep?”
“As parents, how do you deal with issues that cause … anxiety?”
“Does she have somebody to talk with about school issues that cause her anxiety?”
“Can you tell me about the school’s approach towards independence for …?”
“What perceptions do you think the wheelchair creates in the minds of teachers and
students?”
Parent observations
“Does … appear confused or lost when entering a new situation?”
“Is he/she slow to become familiar with a new physical location?”
“Does she tend to interpret what you say literally eg “he’s a chip off the old block?”
“From your in-depth understanding of …, what do you think are his or her strengths?”
“How would you like to see these used post school?”
“Tell me what you think about post-school for …”
“Have you heard about the NLD syndrome?”
“How did you come to hear about it?”
“Has your knowledge helped you (a) to understand … learning needs better,
(b) understand why … has trouble with many “taken-for-granted” tasks, (c) advocate
for appropriate help”
“Have you discussed the NLD syndrome with other parents?”

74
“Would you like to know more about this learning disorder?”
“Is there anything else you’d like to tell me that might help other parents?”
Phase 2 Interview Guide questions for students
The quality of data gathered from children depended on relevance of the topic to the
child’s life and the measures used to collect information. At a minimum, questions needed
to measure the concept of interest, be unambiguous and worded in such a way that students
understood them in the way intended (Christensen & James, 2000). One concern was to
ensure information gathered was valid and whether it represented the child’s perspectives at
a particular time or whether it represents a more permanent attitude (Lewis & Lindsay,
2000). To check internal consistency of students’ views at the time of interview, the
researcher checked important points with the student “You said that … Have I understood
you correctly?” To provide a further check, the verbatim interview transcript was offered
post-interview to each student and their parents.
The set of issues to be explored was outlined before interviewing began – classroom
activities, homework, group work, everyday tasks, friendships, relationships with teachers,
anxiety and anything else the student wanted to talk about.
Classroom activities
“Tell me about the class work that you’re good at.”
“Tell me about the things you have trouble with in class.”
“Tell me how you manage with (a) following directions, (b) copying from board,
(c) getting work finished, (d) changing from one task to another, (e) writing tasks,
(f) maths”
“What about memory and concentration?”
“Tell me about planning tasks, getting organised and managing time”.
“Can you remember things that you hear really well?”
“How do you feel when you enter a new location?”
Homework
“What about getting homework finished and remembering to take the right books
home?”
“How do you go with researching information for assignments?”
“What about doing group work with other kids in class?”
“How your think teachers and aides understand any difficulties you have?”
Lunchtimes and social
“Tell me about lunchtimes.”

75
“Tell me about friendships.”
“Do you have a special friend or buddy?”
“What about school camps, birthday parties and things like that?”
“Is there a policy at school about who should or should not push your chair?”
Everyday tasks
“Tell me about everyday tasks that you find easy.”
“Tell me about everyday tasks that you find hard.”
Relationships with teachers
“Do you think the teachers and teacher aides understand you?”
“What do you think would help them to understand you better?”
Anxiety
“What about anxiety?”
“What things would you like more help with at school?”
“Is there anything else you want to tell me about?”
Phase 2 Interview Guide questions for teachers and teacher aides
Topics, issues and concerns raised in Phase 1 were followed up. The issues to be
explored were outlined before interviewing began – classroom activities, homework, group
work, everyday tasks, friendships, relationships with teachers and classmates, anxiety and
teacher observations. Issues raised in Phase 1 and new questions were introduced with “Tell
me how … manages with …”, “I’m interested to know how … manages with …”
Classroom activities
Getting class work finished
Following directions e.g. changing from one subject or one room to another
Copying from the blackboard
Handwriting tasks
Planning and organisation
Time management
“What about concentration and memory?”
“What about rote memory skills?”
“Do you find that … can remember things that he/she hears well?”
“How do you feel … handles any new or novel task?”
“How is … when she enters any new physical local location. Does he or she appear
confused or lost or can he/she reorient?”
Homework
“Does … remember to take the right books home?”

76
“Does he/she seem to get homework finished?”
Assignments
“How does … manage with (a) researching information for assignments and (b) getting
assignments finished and handed in?”
Everyday tasks
“How does … manage with using scissors?”
“What everyday tasks do you think … finds most difficult?”
Group work
“How does … manage group work with peers?”
Lunchtimes and social
“Does … have a special friend or buddy?”
Relationships with teachers
“How do you think … gets along with teachers and aides?”
“Does she appear to get anxious about school?”
Teacher observations
“From your experience working with … what do you consider are his or her
strengths?”
“How could he/she use these post-school?”
“What advice would you offer to other teachers working with a student with
hydrocephalus and spina bifida?”
“Would you like to know more about the nature of … learning difficulties?”
“I’ve read that some children with SB/HC have a Nonverbal Learning Disability”.
“Have you heard of that?”
“If yes, how did you come to hear about the NLD syndrome?”
“Has your knowledge helped you to (a) understand … learning needs better, (b)
advocate for appropriate help?”
“Would you like to know more about this learning disorder?”
“How is the best way to inform teachers about students with this learning profile?”
“Is there anything else you’d like to tell me that might help other teachers or the
study?
Closing the interviews
One strategy used to facilitate the closing of the interview session was to say “I think
we have covered all the topics I planned in the guide. Do you have any final comments?”
(Delahaye, 2000, p.167). The inquirer made sure she thanked the informant “Thank you for
your involvement. Your time and contribution is really helping this project and they are very
appreciated” (Burns, 2000, p.429).

77
Transcribing interviews
Tape recorded interviews were transcribed as soon as possible after the interview’s end.
Lofland and Lofland (1995) recommended spending, at minimum, as much time studying
and analysing material as was spent on the interview itself. Listening to the tape recording
piece by piece served to stimulate analysis and allowed the researcher to consider what had
been accomplished in the interview.
Member Checks
As dictated by conventional good practice, verbatim transcriptions of the 1st and 2nd
interview phases were offered back to the informant for him or her to confirm, correct and/or
extend. A stamped-addressed envelope was attached for return of the corrected version to
the researcher.
Validating data from students did not present challenges. To increase validity of what
was said, transcripts were addressed to the student and parent because the parent’s
understanding of the young person’s language and intent was expected to overcome any
ambiguity.
Coding system
On return of transcripts, the researcher de-identified and coded all persons and places
named to protect confidentiality and anonymity. Each item of information was numbered in
the transcript’s left margin for quick location during the audit trail. Whole numbers were
assigned to students and letters were assigned to teachers, aides and parents. Where more
than one teacher aide was assigned to a student, a bracketed lower case roman numeral was
used, for example, TA (ii) denoted the 2nd teacher aide assigned to a student. See Table 4.1
Coding System.

78
Table 4.1. Coding System
Primary Students
S.1 – S.3
Secondary Students
S.9 – S.10
Parents Carer
P C
Teachers and aides - Primary Class Teacher Primary Relief Teacher Maths Teacher Physical Tutorial Teacher Home Economics Teacher English Teacher Drama Teacher Science Teacher Art Teacher Practical Art Teacher Computer Studies Teacher Learning Support Teacher Teacher in Charge: Students with Disabilities Special Needs Teacher Teacher Aides 1-3
PCT PRT MT PTT HEcT ET DT ST AT PAT CST LST TIC:SD SNT TA(i), (ii), (iii)
Site - state school state high school catholic primary school catholic secondary school classroom resource room special education unit music room family home interviewer home
ss shs cps css cr rr seu mr fh erh
Site visit episode - Site visit e.g. 2
sv-2

79
Analysis of qualitative data
The first step of analysis was to simplify the complexity of reality into a manageable
classification scheme (Patton, 1990). Three stages of data analysis were involved with
developing a provisional category set - Unitising, Categorising and Indexing.
Stage 1 Unitising
Units of information were identified from corrected and de-identified transcripts of
Phase 1 and Phase 2 interviews. A single unit was identified by two characteristics:
1. It had to be heuristic, that is, lead to new understanding;
2. It had to be the smallest piece of information able to stand alone and be interpreted
without additional information other than broad understanding of the inquiry’s
context (Lincoln & Guba, 1985, p.345).
Units did not bear dual content and each unit was allotted a separate number to prevent
ambiguity. For each informant, units of information were typed into text boxes with the
student number, informant letter code, school description and site visit number at the head of
each box and a response number was entered against the text, for example, S.10/U.7-LST-
shs-sv1 = Student 10, Unit of information 7, Learning Support Teacher, state high school,
site visit 1, as illustrated below.
Later reference to this unit during individual case study reporting was abbreviated to
(S.10/U.7-LST-135). Lincoln and Guba (1985) advised over inclusion of units of
information in the unitising phase because it was easier to reject what later appeared
irrelevant than to retrieve information earlier discarded.
S.10/U.7-LST-shs-sv1. I’m interested to know how she manages with
getting class work finished.
135. Um … when I had her for ICT, very rarely did she finish anything. It would take a long time for her to do a task. Um I think it’s also one of the things that probably prohibited her getting it done was that she would go off into her own little world and it wasn’t really daydreaming it was I don’t know how to explain it. She would just not be there and then you’d say “come on S.10, let’s…” you know “get on the task” and then she’d be in a big fluster and then get confused….very rarely she’d get a task finished unless there was one-on-one so ... and always pushing. I have read that they need continual prompting.

80
Stage 2 Categorising Units of Information
Categories needed to represent the data being studied and be “able to explain the
behaviour under study” (Glaser & Strauss, 1967, p.3). The aim was to bring units that
appeared related to the same content together. The interview guide constituted a “descriptive
analytical framework” where answers from different people were grouped by question topic
and classified under categories (Patton, 1990, p.376). The following guidelines were
adapted from Lincoln and Guba (1985).
1. Each text box was read and cut out. The researcher determined on tacit or intuitive
grounds which units looked or felt alike. Were their contents “essentially similar”?
Such units from Phase 1 responses were assembled under tentative headings and
Phase 2 responses were assembled under interview guide headings (Lincoln &
Guba, 1985, p.347). Parent and student responses were segregated from teacher
and aide responses. The contents of each pile were reread and key points were
noted to aid the formulation of new headings. At this point, collaboration with the
Principal Supervisor took place to discuss a provisional category set that would
represent all data and provide a logical and comprehensive framework for case
study reporting. Successive text boxes were similarly cut and read to determine
whether units looked or felt like those already placed or whether they depicted a
new category (Lincoln & Guba, 1989, p.347). All items under one heading needed
to look alike, be logically related and “dovetail” in a meaningful way to form a
single concept. If viewed externally, category differences had to be “bold and
clear” with heterogeneity clearly evident (p.93). When viewed internally,
individual categories had to show homogeneity among items. Units that neither
fitted into provisional categories nor constituted a new heading were entered into a
“miscellaneous” category for later review.
2. Once a meaningful category set was established, the miscellaneous category was
reviewed. The number of unresolved units numbered less than .01 of the total and
those classified were relatively free from ambiguity. This confirmed
comprehensiveness of case study framework. Some issues “buried” in a large
category needed further subdivision; others were subsumable under existing
categories. At this stage, a set of “discreet categories with no ordinality” (Lincoln
& Guba, 1989, p.94) was acceptable, its inclusiveness indicated by an absence of
unassignable items.
3. The entire category set was then reviewed to check that no category was missing
and that nothing was overlooked.

81
Stage 3 Indexing
All items of information were indexed so they could be retrieved and traced to their
original source as quickly as needed, the major portion of this task completed through the
analysis and unitising phases. All coded and unitised data from text boxes was copied to
another document where reflexive journal notes about each informant were added at the
head.
Three copies of corrected transcripts were made since master computer files become a
key resource for locating materials and maintaining the context of raw data:
1. A master copy was stored in a secure place;
2. A copy was stored on a personal computer hard drive;
3. A copy was stored on a portable disc.
Triangulating data
Triangulation techniques attempted to explain more fully the richness and complexity
of each case by studying it from more than one perspective. It contributed to verification and
validation of analysis by “checking out the consistency” of different data sources within the
same method (Burns, 2000, p.419). Each piece of data was triangulated by at least one,
sometimes two, three or four other sources. This back and forth process between data sets
was considered the best way to ensure saturation and promote credibility of findings.
Meticulous and detailed coding allowed each unit of information to be traced back to its
original source.
Interpreting content
Inquiry content was interpreted in terms of the inquiry’s basic axioms and in the context
of measured test data. Tacit knowledge, insight and experience aided interpretation and
allowed the researcher to suggest more than one plausible interpretation of teacher, teacher
aide, parent and/or student perceptions. This study was designed to incorporate congruent
and dissonant views, all mediated by the researcher’s personal values, predispositions and
the contextual factors declared at the outset and prior to case study reporting.
The highs and lows of mainstream schooling, verbal strengths that fuelled illusions of
accomplishment and the disillusionment experienced when expectations could not be
realised afforded the researcher appreciation for multiple perceptions of the student’s

82
learning experiences. Experience with the language characteristics of an individual with
hydrocephalus and spina bifida provided “tools” to make sense of intended meaning. This
theoretical lens was made explicit to the extent to which personal experience and insights
were relevant to informing the study’s purpose, the topics explored, and the interpretation of
data. The admission of tacit understandings was highly significant with respect to parent
perceptions because their intuitive knowledge of students’ strengths, weaknesses, gullibility
and vulnerability served to strengthen and deepen understanding.
Reflexivity and bias
Reflexivity meant the researcher was aware of and openly discussed her role in the study
in a way that honoured and respected the people being studied while adhering to her primary
obligation to tell the stories of people (Creswell, 2002). Feeling angry, irritable, happy,
excited or sad indicated that subjectivity was at work and when emotions were attuned to the
researcher’s subjective lenses, they helped identify when subjectivity was “being engaged”
(p.105). Rather than give the audience reason to consider the biases, the juxtaposition of self
and subject matter enriched case study discussion and final reporting (Denzin & Lincoln,
2000). The following lists strategies used to generate trustworthiness and confidence in data
analysis and reporting:
1. A verbatim transcript of each interview was sent to the informant for them to
confirm, correct or extend;
2. In each case study report, data were triangulated by teacher, aide, parent and/or
student perceptions to ensure the multiple views of informants were reported;
3. Cross-case analysis cut across individual cases in search of similar and divergent
views. Core inconsistencies were identified and discussed in the light of
researcher insight and experience;
4. To circumvent layers of personal interpretation, direct quotations were preferred to
paraphrasing;
5. A meticulous coding system allowed all quotations to be traced back to their
original source;
6. Examination of the audit trail established that all checks and balances were carried
out in ways that fell “within the bounds of good professional practice” and
findings were consistent with raw data (Lincoln & Guba, 1985, p.109).
To guard against contamination of interview data by the powerful impact of having a
child with hydrocephalus and spina bifida, the influences of personal investment, feelings,
values and experiences, three measures were adopted:

83
1. Supervisor debriefing probed contentious and emotional issues to shore up rational
interpretation and reporting;
2. Personal insights, feelings and values that may have contaminated analysis of
interview data were declared at the outset, during case study discussion and before
case study reporting;
3. The researcher wrote personal feelings in a reflexive journal and asked how they
influenced questions asked through the interview phases.
Explicit disclosure of personal insights, experiences and feelings not only heightened
awareness of personal subjectivity during analysis and reporting but it contributed to
trustworthiness by providing greater understanding of self and personal investment in the
research. Although techniques used did not guarantee balance and fairness, they provided a
process of useful checks and balances. Ultimately, methodological strategies and acts of
reflexivity ask the reader to accept the researcher’s account as a conscientious effort to “tell
the truth” (Denzin & Lincoln, 2000, p.1028).
Psychometric Testing
Visual, visual-spatial, visual-motor perception, complex psychomotor and problem
solving skills mediate execution of many daily living and classroom tasks that are
problematic for individuals with shunted hydrocephalus and spina bifida. These “difficult-
to-explain” areas of difficulty that pervade the everyday life of individuals in this population
were assessed because such deficits are primary NLD characteristics. They are the principle
variables that distinguish individuals with NLD from those with a general learning disability.
Harnadek and Rourke (1994) say the most significant characteristics of NLD in children
correspond to those skills and abilities “found to be amongst the least developed initially,
and that continue to worsen (relative to age-peers) as children with NLD grow older” (p.8).
Test results that confirmed areas of difficulty highlight a need for appropriate intervention
before failure in academic or vocational domains causes long-term problems for the
individual (Rourke et al., 1983).
Psychometric testing to establish the NLD status of each student was conducted at the
conclusion of qualitative data collection. Intelligence tests proven to be reliable predictors of
achievement in traditional school subjects justified their use in an academic setting. To fully
comprehend a child’s ability range and learning potential, Kaufman (1994) believes
intelligence tests are best used in conjunction with other measures and the results interpreted
with regard to national norms.

84
Despite the difficulties of using standard tests with individuals with physical or
cognitive deficits, Sattler (1974) claims it is still important to compare performance with that
of a normal child because the “latter sets the standards in the world at large” (p.83). The test
selection was designed to measure the most significant dimensions of the NLD syndrome
and Adaptive Behaviour and Executive Function scales were used to evaluate the student’s
ability to function independently in school, home and community environments.
Supplementary tests ensured that the range of assets and limitations were assessed.
Administration of test measures
Psychometric tests were administered when all interviewing was complete. Well-
validated, reliable and normed measures quantified verbal and nonverbal abilities of
individuals whose medical condition constitutes a “sufficient condition” to produce the NLD
syndrome (Rourke, 1989, p.114). A clinical psychologist who had experience administering
tests to children with spina bifida and hydrocephalus conducted testing. A speech
pathologist conducted language assessment. The duration of the supplementary test session
was 2 hours and the full test battery lasted 4-6 hours. During these sessions, parents were
invited to complete Adaptive Behaviour and Executive Function questionnaires.
Because “clearly defined clinical criteria for use in ‘diagnosing’ the NLD syndrome
have not yet been established” (Harnadek & Rourke, 1994), areas of testing were guided by a
review of studies that recruited individuals with hydrocephalus and spina bifida and
assessment protocols recommended by McDowell (2003) and Rourke et al. (2002). The
following test battery was developed by a neuropsychologist, psychologist, speech language
pathologist, developmental paediatrician and the researcher. All tests were standardised
well-established measures listed in the University Register of approved procedures. Results
were analysed and scored by the test administrator according to standardised rules. Detailed
interpretation was conducted by the neuropsychologist, developmental paediatrician and the
researcher.

85
Table 4.2. Test Battery
Test Session: Supplementary Testing
Test Battery: Duration: 4-6 hours
Verbal-Performance discrepancy
Wechsler Intelligence Scale for Children (WISC III)
Verbal learning and memory
Rey Auditory Verbal Learning Test (RAVLT) Multilingual Aphasic examination of verbal fluency
Tactile perception
Finger-Tip Number Writing (Halstead-Reitan Battery) Tactile Form Recognition (Halstead-Reitan Battery)
Motor and psychomotor
Dynamometer (Halstead-Reitan Battery) Grooved Pegboard Test (Halstead-Reitan Battery)
Visual-Motor Perception
Test of Visual-Motor Integration (VMI) (Beery)
Visual-spatial perception, Planning and Organisation
Rey-Osterreith Complex Figure
Language
Clinical Evaluation of Language Fundamentals (CELF 3)
Problem Solving
Test of Problem Solving – Revised (TOPS-R)
Academic skills
Wechsler Individual Achieve Test (WIAT II) Subtests: Reading, Spelling, Maths (reasoning)
Adaptive Behaviour
Adaptive Behaviour Assessment System (ABAS)
Executive Function
Behaviour Rating Inventory of Executive Function (BRIEF)

86
Description of Test Instruments
General intelligence assessment
Test measure: Wechsler Intelligence Scale for Children (WISC III) for subjects under
16.11 years (Wechsler, 1989).
WISC III subtests assessed verbal and performance intelligence and comparison of
clustered results ascertained the presence of a V-P discrepancy. WISC III verbal scale
comprised 6 subtests – Information, Vocabulary, Digit Span, Comprehension, Arithmetic
and Similarities. WISC III performance scale comprised 5 subtests – Object assembly,
Block Design, Picture Completion, Picture Arrangement and Coding.
Administration time: 90-120 minutes approximately.
WISC 111 subtests - NLD assets and deficits
The Object Assembly, Block Design, Digit Span and Comprehension subtests were
included in general intelligence assessment. Subtest scores aided assessment of visual-
spatial-organisational, auditory perceptual and language comprehension skills.
The Object Assembly and Block Design subtests assessed visual-spatial-organisation
skills (Rourke, 1989). Visual perceptual skills allow a child to form visual images of what is
seen and inability to form visual images will cause difficulty with assembly tasks. Impaired
visual-spatial-organisational skills cause great difficulty in classroom learning, particularly
following instructions (Rourke, 1989).
The Digit Span (forward and backward) subtest assessed auditory perceptual ability
(Rourke, 1989). Auditory perception is a primary asset of children who exhibit the NLD
syndrome and their capacity to deal with information presented through the auditory
modality provides a “basic strength from which all other assets flow” (Rourke, 1989, p.88).
“Verbatim memory for oral and written verbal material can be outstanding in the middle to
late elementary school years and thereafter” (p.83). According to Dunning (1992) students
with shunted hydrocephalus and spina bifida do not appear to experience deficient auditory
skills and they have good memorising abilities.
The Comprehension subtest assessed complex language understanding. Although
individuals with shunted hydrocephalus and spina bifida are fluent talkers and their reading

87
accuracy may improve to above chronological age, comprehension of what they have read or
been told may be poor (Dunning, 1992). It is therefore important to distinguish between
vocabulary scores and comprehension of what is said and heard (Dunning, 1992). Difficulty
with reading comprehension, especially novel material, is an NLD academic deficit which
tends to increase with age (Rourke, 1989).
Supplementary tests
Verbal learning and memory
Test Measure: Rey Auditory Verbal Learning Test (RAVLT) (Schmidt, M.)
Test Measure: Multilingual Aphasic examination (Benton, Hamsher & de S. Sivan
(1989)
The Rey Auditory Verbal Learning Test is useful for evaluating verbal learning and
memory including proactive inhibition, retractive inhibition, retention, encoding versus
retrieval and subjective organisation (http://www3.parinc.com). In a child with NLD, the
capacity to deal with information presented through the auditory modality is a primary
neuropsychological asset (Rourke, 1989, p.87). The language of individuals with
hydrocephalus and spina bifida is generally well-developed and good attention to auditory
and verbal stimuli promotes advanced auditory and verbal memory, accurate pronunciation
and fluent verbatim repetition of what is heard (Dunning, 1992).
Age range: 7-89 years
Administration time: less than 5 minutes
Qualification: “C” level
The Multilingual Aphasic examination is most frequently used to assess verbal fluency.
This verbal fluency test required the subject to produce as many words beginning with the
letters “F” “A” and “S” as he/she could generate over a one-minute period. Importantly,
rules applied regarding proper nouns, repeats, derivative forms etc. (www2.psy.mq.edu.au)
Age range: 6-13+ years
Administration time: 5-10 minutes
Qualification: No restriction
88
Motor and psychomotor
Test Measure: Dynamometer from Halstead-Reitan Battery (Reitan & Wolfson, 1993)
Test Measure: Grooved Pegboard Test (GPT) from Halstead-Reitan Battery (Reitan &
Wolfson, 1993)
The Hand Dynamometer is a test of grip strength. As with other tests of manual
abilities, strength between hands is expected to vary widely in individuals with lateralized
brain damage. The Hand Dynamometer or Grip Strength Test calls for two trials for each
hand alternating between hands. The score is the force exerted in kilograms for each hand
averaged for the two trials (Lezak, 1995, p.684).
Deficits in motor and psychomotor coordination skills are primary NLD characteristics
that tend to increase with age (Rourke, 1989). Problems with psychomotor and visuomotor
skills broadly characterise individuals with hydrocephalus due to abnormal brain
development and/or spinal cord lesions. Deficits in speed and manipulation skills are
associated with limited exploratory behaviour in the early years and these deficits will
impede performance in everyday life.
Age range: Child to adult
Administration time: 5 minutes approximately
Qualification: “A” level
The Grooved Pegboard Test is a test of static steadiness. It is an assessment protocol
recommended by Rourke to assess complex motor and psychomotor skills in individuals
suspected of NLD. The individual is required to fit keyhole-shaped pegs into similarly
shaped holes on a 4″ x 4″ board beginning at the left side with the right hand and at the right
side with the left hand. The person is urged to fit all 25 pegs in as rapidly as possible. One
trial is performed with the dominant hand followed by one trial with the non-dominant hand.
The scores obtained are the length of time required to complete the task with each hand and
the total number of times the pegs are dropped with each.
Visual-motor and Grooved Pegboard tests are important because Rourke’s (1989) NLD
model is partly predicted on the role of early motor-based deficiencies that limit exploratory
behaviour and characterise hydrocephalic children.
Age range: Child to adult
Administration time: 3 minutes
Qualification: “B” level

89
Tactile Perception
Test measure: Finger-tip Number Writing from Halstead-Reitan Battery (Reitan &
Wolfson, 1993)
Test measure: Tactile Form Recognition from Halstead-Reitan Battery (Reitan &
Wolfson, 1993)
Finger-tip Number Writing requires the individual to verbalise without the aid of vision
which of the numbers 3, 4, 5, or 6 has been written on his or her fingertips. A different
finger of the right hand is used for each trial until four trials have been given for each finger.
The procedure is then repeated for the left hand. The score is the number of errors made
with each finger for each hand (Rourke, 1989, p.227).
A Tactile Form recognition test requires the participant to close their eyes and to
recognise by touch such common object as a coin, a paper clip, a pencil or a key. Each hand
is examined separately (Lezak, 1995, p.425).
Bilateral tactile-perceptual deficits are evident in individuals with NLD. Tactile-
perceptual skills commonly present problems for children with hydrocephalus, particularly
those with spina bifida (Fletcher et al., 1995). Although no “hard” signs of simple tactile
deficiency may be evident, “complex tactile input tends to persist” (Rourke et al. 1995,
p.157). Individuals with suspected NLD may show more marked deficits on the left side of
the body and there is a tendency for these to become less prominent as age increases
(Rourke, 1989).
Age range: Child to adult
Administration time: 5 minutes approximately
Qualification: “C” level
Visual-motor perception
Test measure: Test of Visual-Motor Integration (5th Edition) (Beery, Buktenica &
Beery, 1997)
Visual-motor integration is the degree to which visual perception and finger-hand
movements are well coordinated (Beery et al., 1997). The VMI is a motor-based task that
requires writing skills. It measures eye-hand coordination by asking the student to copy
increasingly complex geometric designs with pencil and paper and helps to assess the extent
to which individuals can integrate their visual and motor abilities
(www.pearsonassessments.com).

90
Visual-motor skills employ efficient use of arms and hands for visually directed reach,
grasp and manipulation. Poor visual-motor coordination will interfere with writing skills
development, ability to copy from the blackboard and impair playground and physical
education activities. A student with spina bifida is likely to have poor or delayed visual-
motor skills and because these involve eye-hand coordination, they tend to be related to
visual perceptual and organising deficits (Hurley, 1993).
Age range: Child to adult
Administration time: 10-15 minutes
“C” level qualification required
Visual-spatial perception, planning and organisation
Test measure: Rey-Osterreith Complex Figure (ROCF) (Osterrieth, 1944)
The Rey-Osterreith Complex Figure test assesses visual-memory, visuoperceptual and
constructional skills and spatial organisational skills (Mitrushina, Boone & D’Elia, 1999). It
consists of a complex two-dimensional line drawing containing 18 details including crosses,
squares, triangles and a circle arranged around a central rectangle. The participant is
presented the stimulus figure with the isosceles triangle and circle oriented to the right and is
instructed to “make a copy of this design as best as possible” on a plain sheet of paper with a
coloured pencil (Mitrushina et al., 1999, p.157).
Attention to visual input is poor in individuals with NLD and except for repetitive
verbal input delivered through the auditory modality, deficient visual attention increases with
age (Rourke, 1989). For individuals with spina bifida and hydrocephalus, attention problems
may be more evident on measures that require visual scanning and analysis (Wills, 1993)
though some selective attention tests may reflect differences between sustained attention for
rule-guided tasks and tasks that demand active scanning, sequencing, planning and shifting
attention (Lezak, 1983).
Age range: 6-89 years
Administration time: 15 minutes approximately, excluding delay
Qualification: “C” level
Language
Test Measure: Clinical Evaluation of Language Fundamentals (CELF 3rd edition)
(Semel, Wiig & Second, 1980). Receptive language subtests used: Concepts and Directions,
Word classes, Semantic Relationships. Expressive language subtests used: Formulated

91
sentences, Recalling sentences and Sentence Assembly. Supplementary subtest used:
Listening to paragraphs.
The CELF-3 core and supplementary subtests was used to evaluate the student’s
language strengths and weaknesses and measure the student’s academic and social language
performance at school and at home (http://marketplace.psychcorp.com).
Individuals with an NLD display well-developed receptive language, a high volume of
speech output and strong rote verbal capacities (Rourke, 1989). The language skills of
individuals with shunted hydrocephalus and spina bifida are generally well-developed and
impressive verbal fluency often causes overestimation of true ability (Dunning, 1992).
Exploration of functional language understanding beyond the superficial expressive level
would explain unusual features and the “grossly deficient content and pragmatics” notably
absent from the language of NLD individuals (Rourke, 1989, p.94).
Age range: 5-21 years
Administration time: 30-45 minutes
Qualification: “B” level
Problem Solving
Test measure: Test of Problem Solving - Elementary Revised (TOPS-R) (Bowers,
Huisingh, Barrett, Orman & LoGiudice, 1994)
Test measure: Test of Problem Solving - Adolescent (Bowers et al., 1994)
The Test of Problem Solving assesses how students use language to think, reason and
solve problems. Both levels use age-appropriate tasks to determine strengths and
weaknesses in a number of areas: clarifying, analysing, generating solutions, empathising,
affective thinking, using context cues and vocabulary comprehension (www.psychtest.com).
Ability to handle novel information and situations is a primary NLD deficit with
severity expected to increase with age. Ability to analyse, organise and synthesise
information “constitute the basic building blocks” that allow one to form and modify
concepts, generate and test a solution to a problem then deal systemically with
environmental feedback regarding suitability of the solution (Rourke, 1989, p.93). These are
particularly difficult areas for individuals with hydrocephalus and spina bifida due to severe
coordination problems (Rowley-Kelly, 1993).
Age range: Elementary Revised 6-11 years; Adolescent 12-17 years
Administration time: 35-40 minutes
Qualification: “B” level

92
Academic skills - Reading, Spelling, Maths Reasoning
Test Measure: Wechsler Individual Achievement Tests (2nd Edition) (WIAT ΙΙ)
(Wechsler, 2001). Subtests: Reading, Spelling and Maths Reasoning
WIAT II battery is empirically linked with WISC III. Subtests allow evaluation of
response correctness as well as examination of what strategies were employed to solve
problems. Reading involves naming letters, working with sounds in words and reading
words aloud from lists. Only accuracy of pronunciation is scored, not word comprehension.
Spelling involves writing the spelling of dictated letters, sounds and words that are dictated
and read in sentences. Maths Reasoning involves counting, identifying shapes and solving
verbally framed “word problems” presented orally and in writing or with illustrations. Paper
and pencil are allowed (http://alpha.fdu.edu/psychology).
Good to excellent single-word reading skills are considered an NLD academic asset
(Rourke, 1989). Though many are poor readers or at risk of reading difficulties (Mattson,
1982), individuals with hydrocephalus and spina bifida usually develop a reading ability that
is more than adequate despite initial slowness of acquisition (Dunning, 1992). Excellent rote
memory skills usually ensure that spelling of phonetically regular words is almost always a
strength for individuals with NLD (Rourke, 1989). Difficulty with maths is an NLD deficit
that increases with age (Rourke, 1989). Maths are problematic for individuals with
hydrocephalus and spina bifida due to visual defects, sensory and motor organisation
difficulties and poor spatial ability (Dunning, 1992). Handwriting is slow and arduous for
many individuals with hydrocephalus and spina bifida though well-practiced simple tasks
may be an asset for some.
Age range: 4 years to adult
Administration time: 40 minutes approximately
Qualification: “B” level
Adaptive Behaviour
Test Measure: Adaptive Behaviour Assessment System (ABAS 2nd Edition) (Harrison
& Oakland, 2003)
The ABAS is used to assess individuals with learning difficulties, their adaptive skills
functioning and to determine how the student is responding to the demands of daily life
(http://harcourtassessment.com). This test comprehensively assesses all 10 areas of adaptive
behaviours as specified by DSM-IV in relation to learning difficulties - communication,

93
community use, functional academics, home living, health and safety, leisure, self-care, self-
direction, social and work.
The ABAS will provide valuable information about the functional capacity of a child
with spina bifida and hydrocephalus in relation to his or her peers by assessing skills needed
to function independently in home, school and social settings.
Age range: Birth to 89 years
Individual administration time: 15 minutes
Qualification: CL2
Executive Function
Test Measure: Behaviour Rating Inventory of Executive Function (BRIEF) (Gioia,
Isquith, Guy & Kenworthy, 2000)
The BRIEF consists of two rating forms – a parent questionnaire and a teacher
questionnaire designed to assess executive functioning in the home and school environments.
The BRIEF is useful in evaluating children with a wide spectrum of developmental and
acquired neurological conditions including pervasive developmental disorders
(http://ww3.parinc.com)
Executive functioning refers to a range of loosely related higher-order cognitive
processes including initiation, planning, hypothesis generation, cognitive flexibility, decision
making, regulation, judgment, feedback utilisation and self-perception which are necessary
for effective and contextually appropriate behaviour (Spreen & Strauss, 1998) which are
reported to be problematic for students with hydrocephalus and spina bifida.
Age range: Child-adolescent
Individual administration time: 10-15 minutes
Qualification: “B” level
Understanding a V-P discrepancy
The stronger verbal than nonverbal intelligence of individuals with hydrocephalus and
spina bifida reflects normal performance on rote verbal, rote memory and simple motor tasks
and below normal performance on tasks that require tactile, visual-spatial-organisation and
visual-motor perception, manual dexterity and problem solving abilities (Anderson & Spain,
1977; Dunning, 1992; Fletcher et al., 1992; Fletcher et al., 1995; Fletcher & Levin, 1988;
Holler et al., 1995; Hommet et al., 1999; Hurley, 1993; Hurley et al., 1990; Mattson, 1982;
Rogosky-Grassi, 1993; Rourke, 1989; Shaffer et al., 1985; Wills et al., 1990; Wills, 1993).

94
Although the VIQ > PIQ profile may be a indicator of an NLD, Tanguay (1999) says it is not
always present because more difficult questions and more subtle cues may depress
comprehension and arithmetic subtest scores thus suppressing the overall verbal score.
Children who are less gifted may display a “less extreme” difference between verbal and
nonverbal intelligence and for this reason, Molenaar-Klumper (2002) says a discrepancy
should not be a concluding factor in diagnosing an NLD but should rather indicate that
further investigation and testing is necessary (p.61).
Appendix C of this thesis reports the incidence of verbal-performance (V-P)
discrepancies in individuals with hydrocephalus and spina bifida. The literature considered a
discrepancy of at least 10 points significant and a prime indicator of an NLD. More recent
literature sheds new light. Pelletier, Ahmad and Rourke (2001) found a V-P discrepancy of
at least 10 points evident only 27.3% of the time. If this criterion was used in isolation from
other criteria for selecting persons with NLD, “it would be likely to miss 72.7% of the
Definite and Probable NLD population in the 9-15 age range”. “It would appear that
dropping a V-P discrepancy of at least 10 points as a criterion would, in all likelihood, have
no appreciable effect on ‘diagnostic’ accuracy” ( p.95). In this study, past and current
research findings were considered and a V-P discrepancy was regarded as a contributing, but
not essential, factor to NLD diagnosis.
Diagnosing the NLD profile
It is hypothesised that nonverbal learning disorders fall within a continuum of
neurodevelopmental disorders by varying degrees of severity and their relationship to white
matter damage or dysfunction (Tsatsanis & Rourke, 1995). Although a particular
neuropsychological pattern is present, the combination of strengths and weaknesses comes
together somewhat uniquely in each individual. Some children may be “more physically
awkward, others may have more social deficits while others may experience “significant
impairment in all deficit areas of the syndrome” (Tanguay, 2002, p.16). It is therefore
central and critical to diagnosis that involved professionals have in-depth knowledge of
variations in the severity of expression of the syndrome.
An interdisciplinary team diagnosed the NLD status of each student. The team
comprised a developmental paediatrician who had extensive experience with the diagnosis
and management of children with developmental disorders, a neuropsychologist who had
vast experience with the diagnosis of developmental disorders, the psychological test
administrator, the speech language pathologist and the researcher as educator and parent of
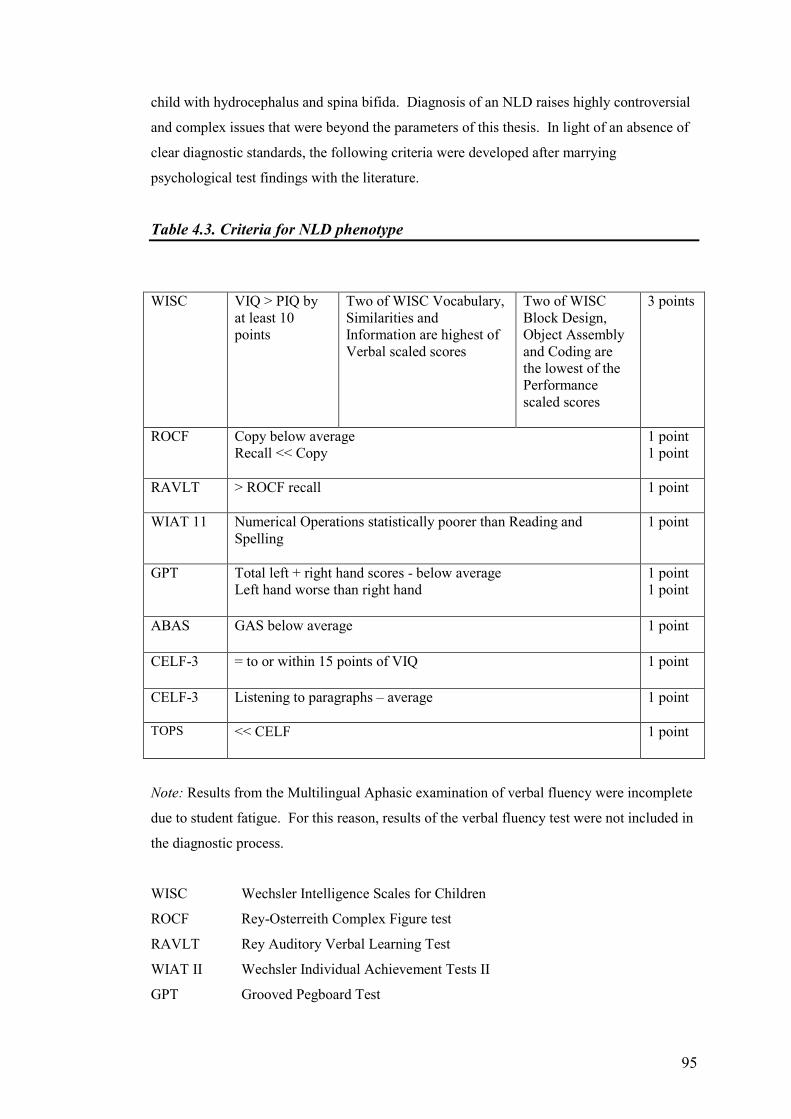
95
child with hydrocephalus and spina bifida. Diagnosis of an NLD raises highly controversial
and complex issues that were beyond the parameters of this thesis. In light of an absence of
clear diagnostic standards, the following criteria were developed after marrying
psychological test findings with the literature.
Table 4.3. Criteria for NLD phenotype
WISC VIQ > PIQ by at least 10 points
Two of WISC Vocabulary, Similarities and Information are highest of Verbal scaled scores
Two of WISC Block Design, Object Assembly and Coding are the lowest of the Performance scaled scores
3 points
ROCF Copy below average Recall << Copy
1 point 1 point
RAVLT > ROCF recall
1 point
WIAT 11 Numerical Operations statistically poorer than Reading and Spelling
1 point
GPT Total left + right hand scores - below average Left hand worse than right hand
1 point 1 point
ABAS GAS below average
1 point
CELF-3 = to or within 15 points of VIQ
1 point
CELF-3 Listening to paragraphs – average
1 point
TOPS << CELF
1 point
Note: Results from the Multilingual Aphasic examination of verbal fluency were incomplete
due to student fatigue. For this reason, results of the verbal fluency test were not included in
the diagnostic process.
WISC Wechsler Intelligence Scales for Children
ROCF Rey-Osterreith Complex Figure test
RAVLT Rey Auditory Verbal Learning Test
WIAT II Wechsler Individual Achievement Tests II
GPT Grooved Pegboard Test
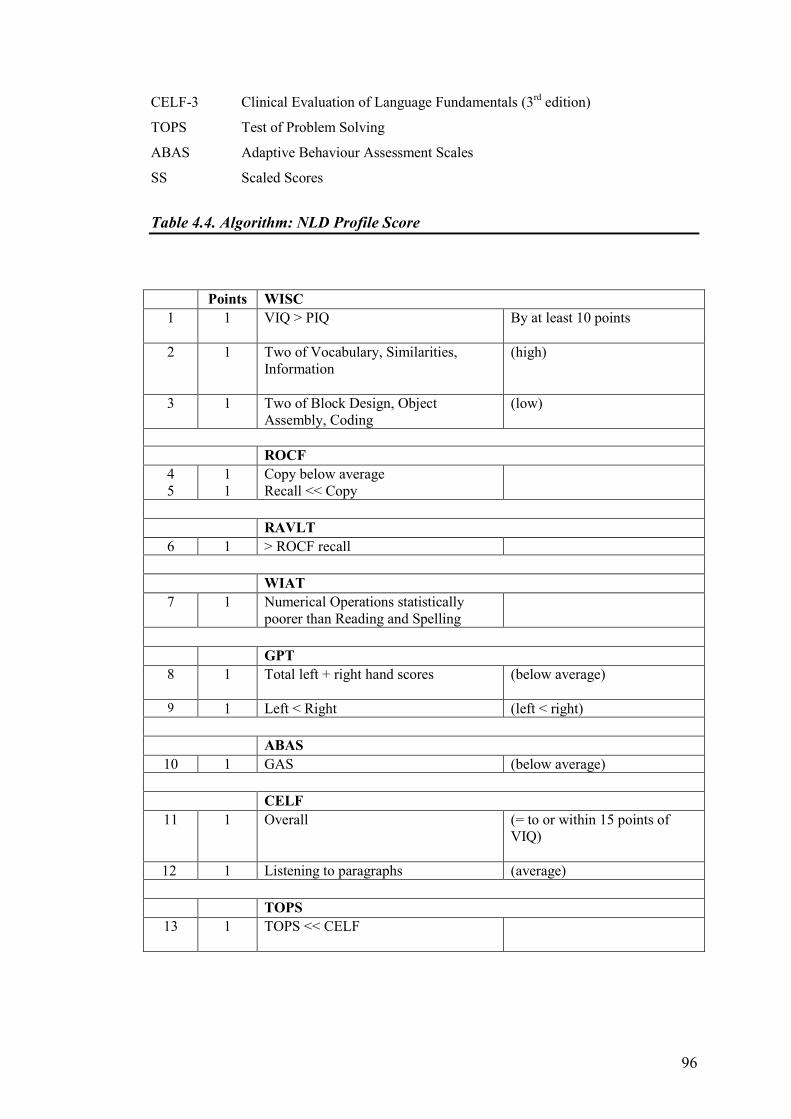
96
CELF-3 Clinical Evaluation of Language Fundamentals (3rd edition)
TOPS Test of Problem Solving
ABAS Adaptive Behaviour Assessment Scales
SS Scaled Scores
Table 4.4. Algorithm: NLD Profile Score
Points WISC 1 1 VIQ > PIQ
By at least 10 points
2 1 Two of Vocabulary, Similarities, Information
(high)
3 1 Two of Block Design, Object Assembly, Coding
(low)
ROCF
4 5
1 1
Copy below average Recall << Copy
RAVLT 6 1 > ROCF recall
WIAT 7 1 Numerical Operations statistically
poorer than Reading and Spelling
GPT 8 1 Total left + right hand scores
(below average)
9 1 Left < Right (left < right)
ABAS 10 1 GAS (below average)
CELF 11
1 Overall
(= to or within 15 points of VIQ)
12 1 Listening to paragraphs (average)
TOPS 13 1 TOPS << CELF

97
Table 4.5. Diagnosis of NLD Profile
Points Mel Josie Ryan Jenny Clair 1 √ X X X X 2 √ √ √ X √ 3 √ √ X X X 4 √ √ X √ √ 5 √ √ √ X √ 6 X X X X X 7 √ √ √ X √ 8 √ √ X √ √ 9 √ X X √ X 10 √ √ √ √ √ 11 √ √ √ √ √ 12 √ √ √ √ X 13 √ √ √ √ X
Total 12 13
10 13
7
13
7
13
7 13
▼ ▼ ▼ ▼ ▼ NLD NLD Partial Partial I I
NLD NLD
A student who exhibits total scores of 10 - 13 points = NLD
6 - 9 points = Partial NLD
2 - 5 points = No NLD
I I = Intellectual Impairment

98
Diagnosis of Executive Function (EF) Disorder
The Behaviour Rating Inventory of Executive Function questionnaires were completed
by parents and teachers. This data and selected test battery data were used to confirm an
assemblage of executive function deficits in the areas of planning, organisation, ability to
change mental set, make decisions, test hypotheses to problem solve, generate ideas and
regulate appropriate emotional responses, utilise feedback for effective and contextually
appropriate behaviour, initiate and complete tasks. All 5 students were diagnosed with an
Executive Function Disorder. The following table summarises the multiple problems that
were confirmed by psychological testing which challenge these 5 students in school, home
and community environments on a daily basis.
Table 4.6. Summary of Functional Profile
Mel Josie Ryan Jenny Clair · SB and HC · Borderline Intellectual Impairment · Significant V-P discrepancy · NLD · EF · Slow information processing · Severely impaired adaptive living skills
· SB and HC · Borderline Intellectual Impairment · NLD · EF · Slow information processing · Severely impaired learning and memory · Severely impaired adaptive living skills
· SB and HC · Low average intelligence · Partial NLD · EF · Slow information processing · Specific memory Problems · Severely impaired adaptive living skills
· SB and HC · Low average Intelligence · Significant P<V discrepancy · Partial NLD · EF · Specific language disorder · Difficulty with most areas of daily living
· SB and HC · Intellectual Impairment · Severe difficulties in all areas of learning · EF · Severely impaired adaptive living skills

99
Case Study Reports
Each case study draws attention to what can be learned from the individual case
(Denzin & Lincoln, 2000). Case studies comprise data from the student and parents in the
context of family, data from educators in the context of school, a summary of psychological
testing, interpretative discussion and conclusion. All accumulated information about each
particular case has gone into that case study. Each case study gave the researched a voice.
Each reports perceptions in a temporal and sequential fashion (history) and provides
contextual descriptions that permit a vicarious experience for readers to raise understanding
and illuminate issues that need consideration for change. This iterative process involved
revisiting category files and raw data to check, question and/or support various
inconsistencies for articulation in the report (Delahaye, 2000).
Each study contains three sections – objective description, interpretation discussion and
a conclusion. The purpose of the study, the problem that gave rise to it, the researcher’s
personal interest in the study, philosophical orientation, recruitment, data collection,
analysis, interpretation and reporting techniques are outlined prior to case study reporting.
Objective description presents and triangulates data from Phase 1 and Phase 2 interviews. A
summary of psychometric test results precedes interpretative discussion. Interpretative
discussion is written subjectively in the light of researcher insight and test findings. The
conclusion summarises the student’s learning experiences as voiced by stakeholders.
Writing the report
A major task that accompanied writing was maintaining an audit trail. No item of
information or assertion was noted without supportive data and each fact was triangulated by
at least one other source. Objective segments were free of the inquirer’s interpretation and
judgment so the reader could make his or her own interpretations (Erlandson et al., 1993).
These sections were written informally in third person, using direct quotations from
informants to add flavour and zest with an approximate 60/40 split between description,
triangulation of data and quotations, and conceptual understanding (Burns, 2000). Data was
organised by category or topic heading. The interview guide constituted a “descriptive
analytical framework” where answers from different people were grouped by question topic
(Patton, 1990, p.376). This early commitment to topic headings facilitated cross-case
analysis later (Stake, 1995). Cross-referencing of indexed items of information to each case
study needed detailed care so that materials from which to write could be easily found
(Lincoln & Guba, 1985).

100
Discussion of inquiry content allowed subjective interpretation. It was written in first
person with researcher interpretations interpolated with those of the respondent “it is not just
what the data say, but what you and the data say” says Pugach in Glesne, (1998, p.165).
The story endeavours to see the world through the informant’s eyes to give readers a sense of
walking “in the shoes of local actors” (Lightfoot, 1983, p.223). Interpretative discussion and
conclusion of each report give details of the case study’s contribution to increased
understanding with intent for that increase to be noticeable to a range of audiences (Lincoln
& Guba, 1985).
Audit trail
The audit trail provided an adequate amount of evidence to verify that the techniques
used strengthened integrity and trustworthiness of findings. For this reason, diligent
attention was given to maintenance of files that represented the phenomenon under study -
methodological journal notes, the rationale that accompanies decisions, personal diary notes
and notes about daily logistics. Careful documentation allows interested persons to
reconstruct the developmental history of the study and the processes from which decisions
and conclusions were reached.

101
CHAPTER FIVE
CASE STUDY REPORTS
The focus of these case studies was to explore how teachers, teacher aides, parents and
students perceived the learning experiences of 5 students with shunted hydrocephalus and
spina bifida who shared signs of a Nonverbal Learning Disability (NLD). Selection of this
participant group supports the view that students’ learning experiences are influenced by
parental and teacher expectations, previous school experiences and the attitudes of peers.
The primary intention was to illuminate new portraits of insight and awareness about the
school experiences of each student as conveyed by significant stakeholders. Perceptions
were regarded as expressions of understanding at a particular point in time, similar and
divergent views sharing equal value in a quest to uncover new insight. Findings seek to fill a
gap identified in the literature about the need to explore educator understanding of the NLD
syndrome. Children who display this atypical profile are rarely involved in educational
programs that address their learning needs hence the need to investigate and raise awareness
so that students afflicted can be identified before loneliness and academic failure become
internalised problems with age (Rourke, 1995; Thompson, 1997). Personal interest in the
study has been declared at the outset and below to provide the reader with a good look at the
writer’s theoretical lens.
Personal interest in case studies
A 12-year journey through mainstream schooling has inspired this research. The
writer’s daughter was born with an encephalocele, a defect included in the term spina bifida
because all share failure of the bone to fuse along the vertebral column or bones of the skull
(Anderson & Spain, 1977; Menkes, 1995). The first neuropsychological assessment at 15
years of age diagnosed intellectual impairment which was difficult to accept. No
professional had ever suggested intellectual compromise. Because she did achieve with
individual support, I theorised that “if we work harder, she’ll catch up”. Daily therapies
focused on physical and visual issues related to the primary problem at birth.
During close liaison with primary teachers, the mother encouraged them to make
allowances for many surgical interventions. In-class support and provision of tuition and
musical accompaniment for class and liturgical activities made the mother a school
“regular”. With much one-on-one help, repetition and structured routines at home, the

102
young student kept abreast with her peers up to Year 5. In other words, she managed the
concrete tasks and predictable situations in the early years but anything new required step-
by-step instruction and psychological preparation. The first “lazy” accusation was observed
on a Year 5 report and such comments became frequent. Every year got harder, much
harder, in every area. One year, a peer told her to read a script which contained offensive
language. She willingly complied and was reprimanded by the teacher. She does not
understand manipulation, cunning or deceit. She is trusting and impeccably honest, to the
point of being tactless at times.
She still has unpleasant dreams about teachers who gave detentions for not completing
class work and one teacher who said “don’t roll your eyes at me” which at the time, may
have signalled information processing difficulties and bewilderment. She recalls the mean
reactions of peers when she could not grasp the underlying meanings in sarcasm or humour
and did not respond appropriately. She is vulnerable to being taken advantage of because
she translates most communication literally. To the casual observer at her current age of 24
years, she presents as an attractive well-spoken girl. In retrospect, her clearly articulated
speech, friendliness and the support from home helped ‘carry’ her through primary school to
about Grade 6 when social and cognitive gaps became wider.
A summons to the school in Year 10 advised the mother that the school could no longer
meet her daughter’s learning needs and another school was suggested. The deputy at the
second college refused to read the neuropsychological assessment provided and the mother
had much trouble dealing with the Learning Support Teacher but class teachers were
approachable. Abstract maths concepts like algebra, area and distance, assignments,
vocational and hospitality subjects and social interaction became unbearably hard to handle
to the extent that, in Year 12, she said she would shoot herself if she had a gun. She was
very lonely at lunch times and at school socials and she was unable to understand the cross-
fire communication within groups. As well, she did not receive invitations to parties or
sleep-overs. Life is lonely without age-appropriate friends. Shopping and going to the
movies is lonely without a friend. Driving a car is not an option for all due to impaired
peripheral vision, planning, organisation, decision-making and problem solving skills which
slow responsivity. The bottom line was, no one really understood the academic or social
problems, let alone could we put a name to them. The mother eventually found a chapter in
Rourke (1989) that talked about Aunt Gertrude’s vase and that was the start of the writer’s
interest in an NLD. By this time, the mother had found an adolescent psychiatrist who
helped mother and daughter adjust psychologically to the change of school and the
realisation that hopes dreams and the future may evolve differently from that planned.

103
Diagnosis of NLD in Australia is relatively new and the young person has not been
formally diagnosed but after comparing neuropsychological test results, personal experience
and understandings with literature reviews, she does appear to “fit” the profile. As an insider
of the NLD world then, the writer’s ears were attuned to what people were saying and her
experience enhanced sensitivity to the plight of parents, teachers, aides and students. Having
walked in the “shoes of local actors” (Lightfoot, 1983, p.223), the writer did not seek to find
fault or pass judgement but rather probe understanding at a given point in time. Whilst
interpreting and reporting data at all times, she endeavoured to “bracket” personal
experiences to prevent them colouring her judgement of the story being told.
Recruitment
As described in detail in Chapter Four Part II, parental responses to an invitation to
participate and review of existing psychometric data by a developmental paediatrician were
used to identify a homogeneous subgroup of 5 students aged 9-16 years with hydrocephalus
and spina bifida. All parents perceived that their child had good verbal skills but
experienced trouble with maths and handwriting.
Data collection
Data collection comprised two interview phases conducted in one session. Phase 1
used open-ended questioning to gain an overview of a normal day in the life of each student.
Phase 2 explored issues raised in greater depth and an interview guide provided focus,
direction and questions that targeted specific areas of research interest.
While the importance of the child’s voice is commonly acknowledged in research
literature, these case studies involved children with spina bifida and hydrocephalus.
Psychological testing revealed that four students had difficulties with speed of information
processing, attention and concentration and one student had trouble with verbal
comprehension. These difficulties together with fatigue may have contributed to the quality
of responses from younger students.
Data analysis
To activate the credibility criterion, interview transcripts were corroborated by
informants before commencing analysis. Transcripts were then analysed to identify units of

104
information. Stage 1 units were allocated under tentative headings according to a presence
of look-alike feel-alike qualities. State 2 units were assigned under topic headings from the
interview guide. During a collaborative meeting with the Principal Supervisor, it was agreed
that data suited the assimilation of thirty-four category headings into the following sub-
sections to form a provisional category set:
Family life
This section incorporated data from parent telephone interviews, open-ended interview
questions with the family, and other contextually-relevant data.
Rules for inclusion in this category:
1. Voices of parents, grandparents and students;
2. Perceptions of past and present school experiences and friendships;
3. Critical issues.
A day in the life of the student based on parent, grandparent and student reports
Rules for inclusion in this category:
1. Perceptions of the mornings, at-school activities, homework and friendships.
The student at school based on teacher and teacher aide reports.
Rules for inclusion in this category:
1. Perceptions of the mornings, at-school activities, homework and friendships.
Teacher and teacher aide perceptions of the student as having a disability
Rules for inclusion in this category:
1. Teacher and aide understandings of learning difficulties;
2. Advice for other teachers and aides;
3. Awareness of NLD.
The contents of each category were then synthesised in a coherent way for entry into
the case study report. Analysis of data was enhanced by additional techniques which
included cross-case analysis, supervisor collaboration and debriefing and the maintenance of
a reflexive journal.
Interpretation and reporting
Inquiry content was interpreted in terms of the inquiry’s basic axioms. Interpretative
discussion and conclusion includes researcher insight and experience to stimulate thought
and transcend the objective content presented earlier. They demonstrate the contribution to
knowledge by comparative analysis of data with test findings and literature reviews to raise
the present conceptual level of understanding. A constructivist-perceptual view of reality

105
was adopted because it acknowledges that multiple realities exist in the minds of informants
and all may be interpreted differently if viewed from other vantage points. Perceptions were
considered an expression of understanding at a particular point in time and their exploration
is congruent with a hermeneutical approach towards revealing and making sense of different
views in a way that communicates understanding (Denzin & Lincoln, 2000). Theory was
grounded in close analysis of data from concrete settings. Grounded theory alone cannot
entirely reflect the constructivist-perceptual view of reality but, together with the flexibility
that characterises naturalistic inquiry, it allowed “multiple points of view to be generated
from the research – for ‘truth’ to be subjective and complex” (Tashakkori & Teddlie, 2003,
p.563).
Each case study contains objective and interpretative sections. Objective reporting
includes triangulation of data. Verbatim quotations were used liberally to add flavouring and
to preserve the accuracy and integrity of individual viewpoints. Although quotations are
verbal transcripts of what was said, hesitations such as “um”, “you know”, “you know what I
mean”, “yeah” and “like” were removed to enhance readability of the text.
The purpose of each case study was to give the researched a voice, to provide
opportunity for teachers, parents and students to share their understanding of the learning
experiences of 5 students with hydrocephalus and spina bifida. The aim was to increase
understanding not to pass judgement and the fine line that differentiates “finding fault and
finding meaning” was acknowledged (Glesne, 1999, p.170). There was no intention to offer
advice, but rather to present alternative viewpoints interpreted in the light of personal
experience and psychological test results. To take account of the interpretative aspect and
the researcher as “human agent” who lived through the research experience, the presence of
“I” throughout discussion and conclusion texts reflects the researcher’s presence in the
research setting (Glesne, 1999, p.169).
Prudent advice offered by Nagel was accepted “writing about another person’s life is an
awesome task so one must proceed with a gentleness born from knowing that the subject and
the author share the frailties of human mortality” (1988, p.115). Pseudonyms are used for
names and places to preserve confidentiality and commitment to anonymity.
Forty-three interviews were conducted for this study: • 19 with teachers; • 6 with teacher aides; • 11 with parents (including initial telephone interview); • 2 with grandparents; • 5 with students.
106
JENNY’S CASE STUDY
Context of Jenny
Family life
Jenny is a Year 5 student at a state primary school which has an enrolment of about
651 students. She was born with a lipomyelomeningocele lesion in the lumbar region of the
vertebral column which was repaired at 9 months of age. The parent said Jenny slept for the
first 2 years of her life and only woke for feeds. A ventriculoperitoneal (VP) shunt was
inserted when Jenny was 8 years 11 months. She has a tethered cord and has had ongoing
difficulties with toileting. Tethered cord refers to scar tissue that forms following back
surgery and “attaches itself to the spinal cord and to nearby bone, causing the spinal cord to
be pulled on” during periods of growth (Lutkenhoff & Oppenheimer, 1997, p.5). Jenny
underwent cord detherings in 2000 and 2003 following more frequent falls and deterioration
in her bladder and bowel control. She has not experienced seizures.
Despite being told that Jenny would not walk, the parent spent “a lot of time in the pool
doing physio with her”. She walked around 2 years of age and is still independently mobile
(U.5contd-P-64). During sessions in the pool, she would go to sleep in an inflatable ring
with a seat insert and the mother would continue with the physio (U.6contd-P-80). She
started talking around 18 months. Jenny lives with her mother, stepfather and two older
sisters and she has had a very close relationship with her Grandma since babyhood (diary
notes). “There’s only been me doing it and my Mum … her father didn’t support me with
her at all”. When he found out she had spina bifida “he couldn’t help” said the mother
(U.14-P-Gma-197). She also mentioned another daughter “who’s ADD ADHD Aspergers”
(U.8-P/Gma-102).
During initial conversation, the mother said Jenny speaks well, likes reading but she
struggles with maths. Handwriting is tiresome and when she gets sore hands at school, she is
given an Alfa Smart computer. Jenny is forgetful. Apart from a couple of chores, she is
“hopeless” with routine everyday tasks. She can ride a bike but she has no road sense and
“there’ll be cars coming and it’s like ‘O! Get off the road’” (U.18contd-P-200). She is
clumsy and awkward “when things are starting to go bad and then I know she’s got to go and
have a scan, like there’s tethering” (U.19-P-204). At these times, she may fall over a lot,
walk into things and have wetting and soiling accidents and the mother knows she must

107
contact the neurosurgeon (U.19-P-206). Concentration was average but Jenny gets
distracted. Short term memory is “bad … in la-la land” said the mother. Jenny has a few
friends. She is “fine” with dressing, undressing, buttoning, doing zips but not at the back,
tying shoelaces and she can make a snack in the kitchen (U.18-P-180-92).
Past school experiences
Jenny has an Individualized Education Plan (IEP) and the mother attends the IEP
meeting every 3-4 months (U.24-P-254). Initially, “they did not understand about spina
bifida” and they thought Jenny “should be able to do what other kids do” (U.33contd-P-370).
Visits from the Spina Bifida Association were arranged to explain the condition and show
videos and the mother said “they’re a lot better now” (U.22-P-228) and they monitor Jenny
(U.16-P/Gma-234). Jenny spoke about the teachers she gets along with and she did not
report any untoward experiences with teachers (U.20-S-181) but she worries about falling
over and said “the school’s very rough” because some children push her (U.22-S-189-92).
Perceptions of Jenny at home and outside
During a power outage, Grandma sent Jenny to buy hot chips. As she watched her
cross the road, “the power guy said ‘clumsy’”. Grandma replied “that little girl’s spina
bifida” and he was “absolutely dumbfounded” (U.12-P/Gma-165-7). He could not believe
Jenny had spina bifida and she could walk. The mother said people expect her to be in a
wheelchair or using splints or a walking frame and even when she shows them the scars on
Jenny’s back, “it’s like ‘wow how come she can run and jump and she can walk like this’”
(U.5contd-P-52).
The three girls have chores after school but Jenny’s are often not done. Grandma said
“you can see it if a child’s in a wheelchair. Well she can’t do this and she can’t do that. Just
because Jenny walks around, there’s some things she can’t do or not as good” (U.6-P/Gma-
62). The mother and grandmother now give single instructions to Jenny but her sisters
consider it unfair that she gets reminders and they lose their allowance if chores are not done
without reminders (U.6-P/Gma-65-74).

108
A day in the life of Jenny based on Jenny, parent and grandparent reports
Getting ready and going to school
“She’s the one we’re always telling to do things … reminding her to brush her teeth,
get dressed” (U.1-P-2) and when she is with Grandma, she must be reminded to do her bed,
her room, have breakfast then after breakfast “now go and do your teeth” (U.5-P-47). When
she is finished one task, she must be moved on to the next and “I find that hard because if
you look at Jenny, she’s a normal child” (U.5-P-47-56) but the mother said “I’ve still got to
give her that chance ‘cause it can be taken away from her at any time” (U.2-P-10). Jenny
said she was “pretty okay” with getting dressed but finds most of her chores difficult (U.19-
S-165). They are sometimes late getting to school “and sometimes we get there on time”
said Jenny (U.14-S-127-31).
At school
Jenny missed 14 weeks of school the previous year because of hospitalisation. She
enjoys going to school and she is top of the lowest group in maths (U.7-S-188; U.1-S-18).
The mother reported a very good bond between Jenny and her teacher and the school said
“Jenny’s not a problem at school, she’s caught up” (U.7-P/Gma-84-94). She can remember
things that she really has to, for example, if asked to do quiet reading then retell the story to
the class, she will remember that “sort of stuff” (U.10-P-132-8). Jenny explained a volcano
and red lava she made in a Studies of Society and Environment class (SOSE) and she offered
to write out the recipe (U.10-S-266). Copying from the blackboard was “easy” and she can
now do cursive writing on the line (U.5-S-42; U.10-S-78). Group work was “really really
easy, we’ve done it before” and Jenny said she can count money (U.17-S-145; U.12-S-98).
Jenny gets “picked on a little bit, she does get teased. It’s only because kids can’t see
her disability so when she does have a mistake, she does get teased” and that really upsets
her. She refuses to wear the pull-up pants “I’m not a baby” she says. If she was in a
wheelchair, “that’d be fine but because she’s not, if she runs around and does everything like
a normal child, they think well there’s nothing wrong with her” said the parent (U.10-
P/Gma-120-4). Jenny is not allowed to play on monkey bars, do running, high-jump or long-
jump but she can play a ball game until she gets tired (U.15-P/Gma-214).
The Principal put a large picture of Jenny in the Teacher’s Lunch Room with a note that
emphasises her spina bifida and advises an action plan if “she’s fallen or been pushed”. This

109
followed many accidents where uninformed teachers would “just pick her up without even
realising it”. Now “they won’t touch her. They’ll just ring straight an ambulance” said the
mother (U.23contd-P-242-7).
Coming home and homework
Jenny is very good with doing homework after school “then she does her spelling and
gets them all right … she’s a good little speller” said the mother (U.11-P-146-155).
Sometimes she gets side-tracked before school and forgets to take homework to school so
the mother will “run it down to the school” (U.14-P-168).
Loneliness, friendships and anxiety
This year she did not have a special friend or buddy (U.18-S-151). The mother said
Jenny was good with friendships but special friends and invitations to parties, she is “no
good like that” (U.20-P-211-6). At lunchtimes, she sometimes plays with friends or plays on
her own “but it’s really boring on my own” (U.18-S-147). She has one friend less because
one girl moved away “and I’ve got others who can’t play with me” (U.2-S-22).
Tasks Jenny enjoys
She is good at art, handwriting, spelling, maths and tables (U.2-S-26-8) and she uses
triangular pencils to aid her grip and control (U.22-P/Gma-139-151). She likes drawing
unicorns and a map of Australia and when in hospital, she copied 3 horses freehand for her
Mum “because this big machine was on me and it was pretty awful” (U.3-S-65-81). The
mother said she is a good swimmer and when she gets tired “she’ll turn herself over and
float” (U.15-P/Gma-212-220). Jenny likes to climb trees and do “all the things she’s not
supposed to do like running, playing normally with kids on forts, ride her bike, play tiggy,
ride horses” but she must be watched for safety reasons, for example, her older sister leads
the horse to give Jenny the sense of “Oh! I’ve been on a horse” (U.3-P-12-4). According to
Grandma, she can be quite conniving. After a bout in hospital, she came home with 53
staples in her back and fell off either her bike or the clothes line. She dragged herself onto
concrete but “she couldn’t tell us what she’d been doing”. She said “‘she’d tripped’ but
Grandma said “she won’t stand still” (U.16-P/Gma-223-228). The mother and grandmother
“just take her as she comes … you give up after a while” (U.13-P/Gma-179). When she is
older and her sister gets a horse, Jenny would like to “get a motorbike” and “I want to get a
puppy” (U.3-S-127).

110
Strengths reported by the parent and grandmother
Her mind, her body “because if it wasn’t for her herself, she wouldn’t be where she is.
So just her full body, she’s full of strength, very like pig-headed sort of thing. She won’t let
anything beat her. She’s very strong-minded like that ‘I’m not going to be in a wheelchair,
don’t be silly’” said the parent (U.27-P-294).
Tasks Jenny finds difficult
Memory is a problem and little accidents may happen if playing with friends and Jenny
forgets toileting (U.5-P-38-44). Each day she has three house chores (a) to make her bed,
(b) brush her teeth and (c) empty her rubbish but finds it very hard to get all three done.
“She can do one but gets side-tracked” (U.5-P-38). Holding a pencil for too long gives her
very sore hands (U.4-P-24), finishing class work and tasks that involve planning,
organisation and time management are difficult (U.6-S-44; U.14-P-164-6). Every task needs
a reminder which is what Jenny and her mother find the hardest (U.13-S-104; U.5-P-44).
Advice for teachers
Teachers cannot think children like Jenny are “like any other child if they get pushed
over. Their backs are very fragile. They are very fragile children. They just can’t be
roughed up like any other child. There have been some teachers at the school that haven’t
understood and I have gone right off at them and saying that ‘she can’t be pushed in the back
because her back is very very fragile’” said the mother (U.33-P-370). These teachers were
“not there all the time” and the mother said “there’s not a lot of schools who know a lot
about spina bifida. It’s not a known thing …” (U.33contd-P-370).
Have you heard of a Nonverbal Learning Disability?
The mother had heard about an NLD from other parents who spoke about their children
“with the hydrocephalus and the learning part” (U.32-P-326-328). She had also heard about
it from “a couple of the teachers at the school”. One was the Special Needs teacher who said
“Jenny doesn’t have it … she’s pretty good” (U.32contd-P-352). Psychological test results
indicate Jenny has Partial NLD, an Executive Function disorder, specific deficits in the
language domains and her intellectual functioning was in the low average range.

111
Jenny at school based on teacher and teacher aide reports
At school
Jenny was away for a whole term because of hospitalisation and up to the time of
interview, the class teacher had had “very little academic time with her” (U.23contd-PCT-
158). The teacher worked very hard to build a class culture of support and understanding
after Jenny returned to school because she was quite sick and “we could barely stay in the
room. She was soiling and it was a real sign that she needed that off” (U.7contd-PCT-30).
Some children would say “something really smells around their desk” but a few knew the
situation and would support her. The teacher stressed that she was a class member and
whatever happened “it was not focused on, it was none of your business, mind your own,
move away”, thus deflecting attention (U.7contd-PCT-30). There have been many class
discussions about Jenny’s shunt and her back and “we all know Jenny needs to go to the
head of the line because she can’t be bumped and it’s not putting her out there but it really is
an awareness that we have and we talk about it freely”. There is a whole lot of support in
that room “but we’ve had to work very hard to get that culture going”. Fitting into the class
was not difficult for Jenny because “she’s bubbly and very resilient and the class culture has
stamped out any of that sort of stuff and it’s encouraged for that sort of thing” (U.8contd-
PCT-36).
Despite very good routines, programs and timetables on the desk, the teacher described
a normal day as “a pattern of confusion that she tries to sort out what’s happening for the
day” (U.1-PCT-2). A lot of the time she operates by watching others to try and figure out
what is going on. Even with direct instruction, she is still “a bit confused” because she does
not retain a routine for a whole day. “So I think she has a fairly trying task all day to keep up
with the hum-drum of the classroom and what’s going on” (U.1-PCT-2).
Her spelling is “very poor” and “she certainly can’t write well enough to express what’s
in her head”. “She needs a lot of redefining, rephrasing and refocusing” so for her, it is
always an adapted level of work in most areas, said the teacher (U.2-PCT-8). Any event
that interests her that she can personally experience, “she grabs that, she goes with it, she’s
willing to talk, to write as much as she can to present whatever the findings are in her own
way”. However, it needs then to be deciphered by a teacher sitting with her to decode
because spelling-wise, some is not quite readable. Learning is tough for her and presenting a
finished product is a very time-consuming task but “she’s keen and when she clicks onto

112
something, she’s really keen to please and she really does it” (U.2contd-PCT-10). So her
days are tough days, said the teacher (U.1contd-PCT-14).
The most enjoyable tasks are writing, drawing a picture to match the writing or
presenting something personally like a poem, a letter to Mum or offering responses about a
story or characterisation of a book (U.3-PCT-16). Jenny is keen to talk about “relationship
stuff” and will outpour pages about personal issues in her diary but it needs deciphering
(U.3contd-PCT-16-24). She is “very empathetic to other kids” and very understanding of
more mature relationships between people than most students (U.3contd-PCT-16).
Loneliness, friendships and anxiety
Jenny makes sure she fits in, she tries, she knocks on doors and she will generally find
someone to be around and play with but “no” the teacher did not think she had a special
friend (U.23contd-PCT-146-50). She has friends but “I don’t think she’s got loyal staunch
‘you are my best friend, come to my house’” (U.23-PCT-144). “There’s always this round
of bitchy fighting stuff, no different to anyone else” but Jenny is “probably 60% more
involved than other kids”. She gets very heated and will lose her temper and lash out and hit
and she has a very strong sense of justice” said the teacher (U.9-PCT-36). Because of her
difference and her verbal skills, she can say some silly things that put her on the fringes “and
she doesn’t lie down and die. She works her way back in there …” Anxious … “in the hum-
drum of the room, I don’t see that. I don’t see her fiddling and sitting staring off into space
… no I don’t, no” said her teacher (U.12contd-PCT-64).
Overall, the teacher did not think Jenny could pick up nonverbal cues from her peers.
“If she picks it up, it’s probably the wrong message or it’s misinterpreted. There’s no
subtlety with her. It’s got to be very clear in black and white. There’s no real subtlety and I
think that’s what gets her into trouble because someone will say something that probably
shouldn’t have been taken as an offence but she gets on her high horse about it and goes with
it …” (U.10contd-PCT-46). Her mental processing is slow which could be “half the trouble
with relationships. It’s all happening too fast and ‘she said’ and ‘he said’ and then ‘I said’
and then she’s back with ‘I want to respond to that first bit’ (U.16-PCT-108).
Strengths reported by the teacher
“Her resilience, her happiness, her ability to try, her ability to come up smiling no
matter what. She will reach out to people, it may be inappropriate, it may be wrong and she
may fall flat on her face but she reaches out to say ‘hey I’m here … talk to me’”. She cares
for other kids and is very empathetic towards them. Her strength is “her knowing of and her

113
enjoyment of the emotions and the flow of the world around her. She’s very in tune … she’s
so unaffected about herself”. She gives praise, she gives credit when it’s due and she is
“very much reaching out with her arms wide open to embrace whatever comes her way and I
think that’s her strength”, and she is “very appreciative of anything you do for her, very
much” (U.24-PCT-160).
Special teaching arrangements
Jenny has 1 hour of SEU time per week. Because of her long hospitalisation and her
fragility in the playground, the teacher utilised SEU time for a gross and fine motor skills
programme done to music. Jenny is restricted where she can run freely at lunchtime and the
teacher “felt she needed the exercise in a safe place”. As far as academic support in the
classroom, the teacher said “no, I’m basically it” (U.4-PCT-20).
Changing mental set and getting class work finished.
Changing from one task to another in class is a very unsettling time for her. “It’s all too
quick for her”. She needs closure and if a task is unfinished, “she’ll just throw it in the desk
and never think about it again” (U.13-PCT-68).
Homework
“That’s been difficult. I don’t know if that’s Jenny or it’s home. Their life’s been very
hard this year” said the teacher who thought “Mum helps her to get through it” (U.19-PCT-
126). Homework sheets that have an easy section and a hard section are given out weekly
and students are asked to “have a go and practice doing something every week and handing
it in”. Jenny has handed in some homework which was not well presented “but it’s been
done” (U.19-PCT-128).
Copying from blackboard and handwriting
The teacher prefers students to work in small groups on the carpet using worksheets
rather than work from the blackboard. She is very slow, often does not finish board work
and “if she doesn’t know the word, she doesn’t have a clue what the writing is about so
you’d need to go really carefully”. She often says “I can’t see that” or “can I sit somewhere
else” (U.14contd-PCT-84; U.14-PCT-76). Asking Jenny to copy a draft of her work to a
good copy “is very hard for her” (U.14-PCT-72). Handwriting was big and “undecipherable
in the beginning” but with much teacher help and practice, it is down to a readable size with
readable formations of letters and spacing and she is now “handwriting pretty much
everything”. She works on readability not neatness and “I’ve seen her go very quickly

114
through a nice letter when she’s very involved” and she will write three pages. “It’s the
quality of the spelling and the quality of the concepts but it is hard for her, she really works
at it” (U.17contd-PCT-114). The teacher mentioned the Alpha Smart computer which “she
treats like a toy” (U.17contd-PCT-112).
Planning, organisation and time management
She does not have planning and organisational skills “no, she’s not good. Her desk is
an absolute mess. Despite how many times we clean it up, she can’t find things” and time
management “‘I just do spontaneously what I do until someone says stop’” said the teacher
(U.18-PCT-122).
Rote memory skills
Learning spelling and tables is tough on two counts because Jenny “won’t put her mind
to the task. She doesn’t want to sit down and do that over and over again … she doesn’t like
rote learning very much”. Although she will write things out a few times, the teacher said
she does not retain it at all (U.15-PCT-92).
Maths
She needs a lot of hands-on stuff and one-on-one work” and given that she is in that low
category of learning, she needs someone to work close to her who will catch her up, talk or
explain what is happening (U.1-PCT-8). Any maths activity is very difficult. She tries her
hardest but even with concrete materials, “we’re not there yet” (U.5-PCT-24).
Concentration and memory
Writing a response without a “lot of framing and contextual stuff is very difficult for
her. She can’t get started, she can’t think it through … it’s all too hard” (U.5-PCT-24).
Remembering and answering questions on test papers “doesn’t take it in so she finds that
difficult” (U.5contd-PCT-24). “What am I thinking and how do I say it on paper” was how
the teacher perceived Jenny’s approach to writing. “It’s not put together in a structure but
it’s just a flow of ideas from her mind” that recounts an excursion or a fight with a friend
(U.17-contd-PCT-118).
Verbal skills
The teacher perceived Jenny’s verbal skills and command of English as “very poor”
(U.9contd-PCT-36; U.2-PCT-8).

115
Everyday taken for granted skills
Academically, maths is the most difficult everyday task and functionally, “getting
organised, getting into class, finding out what’s going on, keeping tabs on how everything’s
running, what’s happening” which the teacher attributed to “her not cottoning on quick
enough. It’s that chaotic pattern of being in the classroom which is very difficult for her”
(U.22-PCT-134-6; U.22contd-PCT-140). Using scissors, cutting and pasting are “not
brilliant but it’s okay, it’s acceptable” (U.20-PCT-130).
Group work with peers
The teacher thought she had friends in the class but mentioned that “a lot of the kids
find her very trying, very trying indeed …” (U.8-PCT-30). Jenny is often the last one to get
grouped up but again “she just waits and she’s bubbling and someone comes along and they
group her up into a group”. Often people do not want to sit next to her, not the whole class
but just one or two and when they suddenly move, the teacher realises Jenny’s sitting there
so she must be very aware of where Jenny is supported. “It’s very complex to say how it
happens but you have to be very aware of Jenny” (U.8-PCT-30).
Critical Life skills as represented in school
Although she is very resilient, the teacher thought Jenny “needs relationship help within
the playground” (U.9contd-PCT-36).
Teacher perceptions of Jenny as a person with a disability
Advice for other teachers
“If they’re the same as Jenny, I would say don’t do it alone, get your class to help.
Build your class culture No. 1; you don’t have to do it on your own. You have to be very
firm about no, there will be no teasing and yes, there are special requirements for her like
anyone else with a broken leg or physical problem and give her some support that she can
feel she can rely on, slow, organised, routinised and make plenty of allowances for accepting
that ‘that is as much as I can do’ and say that. That is as much as she can do and that’s great
and that’s fine”.
“Get to know them really well” (U.25-PCT-166). “If you don’t know them and know
their quirks and know when to push and when to pull back, then you can’t work with them”

116
(U.21-PCT-132). Know them and provide a culture around them in the classroom that “you
don’t have to do that alone and she doesn’t have to do it alone” (U.25contd-168).
Jenny needs a routine; she needs it over and over again. She needs a lot of support.
“When she can’t produce something beautifully, I give her gel pens and I buy pretty paper
and that helps her by putting the border on to start with, just a pretty border and she gets a lot
of satisfaction from that too”. Work side by side rather than from the board. “Copy that
down” or “finish that … I’ve done this much you finish that much, that sort of stuff”
(U.25contd-PCT-168).
Teacher understanding of learning difficulties
Class work needs to be adapted because some students can do a whole activity while
“some fill in the beginning or ends of sentences”. For Jenny, the teacher obliterates
unnecessary information and she may “give her a bank of words at the bottom … ‘Choose
from these words’ rather than ‘You have to think up these words’”.
“It’s adaptation and protection I suppose but don’t do it alone. The class … they’re the
secret of having a kid like that in the class. They’ll do it for you. They’ll tell and they’ll
help her and they’re out of their seats to help her but she’s not special then really”. If a child
comes with a broken leg “I’ll make sure you’ve got a comfortable seat, I’ll make sure people
don’t bump you, I will make sure that you need to do what you need to do … anyone gets
that privilege. Jenny has this, she needs that, we need that, and that’s the culture. Everyone
gets what they need to have in the classroom … you’re pushing uphill otherwise”
(U.25contd-PCT-170-2).
Summary of 2005 Psychological and Speech Assessments
The following extract has been taken directly from assessment reports.
2005 (aged 10 yrs 4 mths) Full Scale IQ = 84
Verbal IQ = 72
Performance IQ = 102
VIQ-PIQ difference = 30 (clinically significant)
Language assessment age equivalent = 7 yrs 0 months
Problem Solving age equivalent = 6 yrs 1 months

117
On a test of general intellectual functioning, Jenny performed within the low average
range for a girl her age. Within this, general intellectual functioning is comprised of verbal
and non-verbal intellectual functioning. Jenny performed within the average range on the
non-verbal component of intellectual functioning, however performed within the borderline
range on the verbal component incurring a 30-point discrepancy between her non-verbal and
verbal abilities.
Jenny performed well on tasks assessing speed of information processing and
relationships between concrete items assessing visual spatial and motor skills. She
demonstrated great difficulty on a task of work meanings and verbal expression of them.
She also had difficulty determining relationships between specific words.
Jenny’s academic performance is within the expected range of her actual ability
predicted by her intellectual functioning. However, Jenny does have significant learning
difficulties that need to be considered in her academic programme. These areas are as
follows:
• Any task which involves an organisational component (e.g. having a tidy desk to
undertaking a project);
• Some tasks which involve visual perception;
• Most areas of verbal learning including knowledge of word meanings and expression
of them and relationships between verbal concepts.
Interpretative discussion
The teacher interview was conducted in the school Music/Arts Room during the
morning lunch break. The class teacher conveyed an impression of sensitivity towards the
personal and academic needs of class members and Jenny’s family spoke similarly. By
placing a large photo of Jenny in the Teachers’ Lunch Room with information about her
medical conditions, physical status and procedures to follow in the event of a bump to the
head or fall, the principal ensured that every staff member had the same crucial information.
This case had an unexpected outcome. Students were recruited according to age,
presence of spina bifida and shunted hydrocephalus, good verbal skills and trouble with
maths and handwriting. These criteria were verified during the initial telephone
conversation. Good verbal skills were confirmed by Jenny’s mother yet language
assessment indicates a specific disorder within the language domains. Results from

118
psychological and language assessments reveal that Jenny meets criteria for Partial NLD, an
Executive Function Disorder and her intellectual functioning was in the low average range.
In this case study, no contentious parent or teacher perception ignites discussion, quite the
reverse, but one public misperception reported by the mother and grandmother deserves
comment.
People expect her to be in a wheelchair or using splints or a walking frame
and even when the mother shows them the scars on Jenny’s back, “it’s like ‘wow
how come she can run and jump and she can walk like this’” (U.5contd-P-52). When
asked, Jenny’s parent and grandmother agreed that the general community appears to expect
people with spina bifida to be dependent on a wheelchair or walking aid. Jenny’s prognosis
for walking was grim but the mother persisted with physio in the pool. In an educational
context, mobility and verbal fluency plus the hiddenness of shunted hydrocephalus convey a
child who is “so normal in every way” (S.2-U.22-TA-232; U.6-P-56). For a child with NLD
characteristics, such misunderstanding about the primary condition and associated cognitive
and social implications can lead to unfair criticism and unachievable goal-setting in school
and vocational settings. According to the mother “there’s not a lot of schools who know a
lot about spina bifida. It’s not a known thing ...” (U.33contd-P-370).
Handwriting was big and “undecipherable in the beginning” but with much
teacher help and practice, it is down to a readable size with readable
formations of letters and spacing and was reported to be “handwriting pretty
much everything” (U.17contd-PCT-114). With teacher support, practice and patience,
Jenny’s writing has improved and it is now readable. This outcome confirms Rourke’s
(1995) proposition that handwriting is a stereotype task that can be “routinised” with
frequent repetition.
Conclusion
In the school context, Jenny had trouble with maths, handwriting, concentration,
memory, changing from one task to another, starting and finishing a task, homework,
changing a routine, misinterpreting peer social interaction and she did not have a special
friend … all characteristics of the NLD syndrome. The mother reported poor planning,
organisation and time management skills so mornings are difficult and Jenny is sometimes
late for school. Contrary to the literature (Rourke, 1989; Rourke et al., 2002; Thompson,

119
1997), her spelling and rote memory skills were poor. Despite the mother saying during
initial telephone contact “yes, Jenny speaks well”, test battery results and the Language
Assessment indicate that Jenny has a specific difficulties within the language domain.
Jenny’s teacher, in fact, reported a “very poor” command of English.
Jenny’s stronger nonverbal than verbal skills differentiates her from other study
participants whose verbal skills were stronger than nonverbal abilities. However, she still
displayed typical NLD deficits in the areas of maths, handwriting, planning and organisation,
visual perception, concentration, memory, ability to start and finish a task and social skills.
Test findings confirmed that the mother’s perception of Jenny’s verbal skills was inflated
while functional difficulties were perceived realistically. One explanation may be ongoing
willingness of the family to compensate for limitations and encourage small achievements
because parents are ever mindful of the challenges and setbacks overcome by their child.
Maybe the optimism generated by the mother and grandmother inspired Jenny to be
optimistic, to keep trying and wanting to please, to be caring and empathetic towards other
students, to be resilient, happy and willing to “embrace whatever comes her way”.
120
RYAN’S CASE STUDY
Context of Ryan
Family life
Ryan is a Year 4 student at a private primary school in southern Queensland which has
an enrolment of about 564 students. He was born with a myelomeningocele lesion in the
lumbar region of the vertebral column (L.4-L.5) and a ventriculoperitoneal (VP) shunt was
inserted 3 days after birth. The shunt was replaced at 3 years of age and revised at 9 years.
Ryan has an Arnold Chiari malformation but he has not experienced seizures. He walked at
about 2 years and started talking around 14 months. He lives with one parent and two
brothers.
Ryan is independently mobile and sometimes wears short leg braces called Ankle Foot
Orthoses (AFOs) to support the arch and ankle of each leg. These lightweight plastic
supports mould to the back of the leg and ankle and fit inside the shoes (Lutkenhoff &
Oppenheimer, 1997). Ryan is in a mainstream class and has been allocated 20 minutes of
aide time per day but the parent said “he doesn’t get it” because the time is utilised to
supervise toileting. Ascertainment from Level 5 to Level 4 Physical Impairment (PI 4)
prompted the parent to write to the State Minister for Education since PI 4 correlates with
reduced funding. The parent drew attention to the ascertainment of children with spina
bifida and literature that documents the “perceptual processing difficulties and other nuanced
cognitive effects of hydrocephalus which occur in 90% of children with spina bifida … The
typical uneven cognitive development, propensity for cognitive gaps and commonly
experienced learning disabilities experienced by kids with spina bifida and hydrocephalus
are ignored or considered of no consequence when assessing the level of assistance to
provide to these kids to ensure equity”. The essence of this letter was “why isn’t there
funding for cognitive issues associated with hydrocephalus” (from copy of letter provided,
dated 17.10.03; U.2contd-P-50).
During the initial telephone conversation, the parent confirmed that Ryan speaks well
and likes reading. He “started to read last Christmas and has not stopped. Vocabulary has
increased and he can express his thoughts clearly”. He is good at concrete maths and spatial
concepts were “good” at Grade 3 level but after the last shunt revision, homework tasks that
relate to congruency or rotating of shapes “fell right away” (U.14-P-178). At the time of

121
interview, Ryan was not considered clumsy and was “pretty steady with pouring drinks” but
would sometimes overfill the glass (U.15-P-190). The parent reported weak hands with
some tremor. Handwriting is tiresome and the left-hand shakes when writing. Planning,
organisation and time management were “awful” and rote memory skills were “good” up to
the time of shunt revision. Gross motor movements and visual perception were “not too
bad”. He can do some everyday tasks though buttoning is difficult and he cannot tie
shoelaces. Ryan is not able to complete any homework tasks without help. Short-term
memory is “awful” but long-term memory is better. His ability to pick up nonverbal cues
and read a situation is “pretty good” but verbal comprehension “is poor” (U.25contd-P-342).
Sometimes he is not vigilant when crossing the road so “I always cross the road with him”
but when playing locally, the parent has “people watching out for him” (U.22contd-P-298).
Ryan had one close friend at school and anxiety was not a problem that was reported. He is
a “pretty calm, happy, open” child with a wicked sense of humour but complains of aches
and pains when asked to do a task he does not enjoy.
Past school experiences
The father said educational experiences were “like walking, hazardous but he has had a
good run”. When asked about previous psychological assessment, the school reportedly did
not want to conduct assessment. The parent is frightened of Ryan “being left behind” and
“tries hard so school won’t be a negative experience”. “It’s really tough as a parent to watch
them get discouraged by not fitting in to the expectations that they hold for all students. All
students have to be able to write a sentence and he just can’t, he simply can’t and you feel
discouraged. It’s really hard to watch that” (U.27-P-384).
Critical issue
“It’s wrong that they fund him for physical disability and don’t recognise that he has
non-typical learning requirements”. The parent claimed that physical disability carries “no
funding for cognitive sort of issues and it should”. Ryan has definite cognitive gaps and
rather than say ‘o well he’s disabled so we’ll lower expectations’, resources should be
available to target those gaps to make the school experience more positive (U.2-P-20). He
believed schools were struggling to get resources for their core body of students and students
like Ryan are always going to be feeling deficient and at risk of falling behind (U.2-P-20).
When the parent specifically asked the school counsellor to assess Ryan’s learning abilities
and gaps, she initially “sounded keen” (U.2contd-P-24).
As part of the Individualized Education Plan (IEP) ascertainment process, a meeting
was convened for “people who could help with determining the full extent of Ryan’s needs”.

122
An advisory teacher from Education Queensland who allocates funding and recommends
resources for State and Catholic Education students with physical impairment was present
(U.2contd-P-30). After the meeting, the parent asked the school counsellor about
psychometric evaluation of Ryan and she said “no, we’re not going to do that” and it seemed
they were just going to concentrate on keyboarding (U.2-P-22). “My gut feeling was the
advisory teacher had already talked her out of doing anything extra or that someone had
talked her out of doing anything extra for Ryan to address his cognition or his educational
requirements” said the parent (U.2contd-P-24). “She and I have had fights in the past. She
is absolutely against providing … against supporting … asking for any funding at all for
addressing educational requirements (U.2contd-P-26). She’s nasty about it, she’s really
nasty” (U.2contd-P-28contd). When talking about literacy problems because Ryan is “not
fluent in writing”, the advisory teacher said that “his ability to access anything that she could
get for him depended a lot on me, on what I was willing to … on how committed I was as a
parent and whether I was willing to go and check out software, but software … she’s bloody-
minded”. The parent challenged her about denying Ryan something he needed by reducing
him from Level 5 to Level 4 and since that initial clash, “she is so defensive with me that she
is actually hurting Ryan’s cause” (U.2contd-P-28contd).
There is no funding available for people with cognitive difficulties unless ascertained
with Levels 3, 4, 5, 6 Intellectual Impairment said the parent. Classification as “learning
disabled” under the IEP ascertainment process does not carry funding and “it might be
assumed that the normal allocation of teacher aide time could be used” to help these students
(U.2contd-P-30). There is a medical reason why Ryan cannot fully access the school
curriculum and even though he is “not down lower than 10%”, his disability could be
compensated for by addressing it through the system rather than “trying to make him work
harder or tying to make me work harder at home” (U.2contd-P-38).
When asked whether Education Queensland may regard spina bifida as causing
physical impairment only … “Do they not recognise that spina bifida and hydrocephalus can
cause cognitive gaps?” The parent said “I think there’s a stumbling block there. I would say
definitely that this person who’s the one whose job it is to hand out funding, she’s got that
mindset” (U.2contd-P-42). A copy of the letter sent to the Education Minister was given to
the researcher with the comment “that’s sort of my feelings on the school system and how
they don’t look at the educational needs of children with spina bifida. They only look at
their physical needs” (U.2contd-P-52contd). “Some of the resources that come out of
Education Queensland deal with all the impairments and their levels and they list a few
physical impairments that can cause cognitive problems and spina bifida is not one of those

123
listed and yet you’ve seen the research and I’ve got my reference list here. It’s got lots of
research about ‘Hydrocephalus causes a specific type of learning disorder’. It’s out there,
the literature’s there, the body of knowledge is there and yet we just can’t get the Education
Department to say ‘yeah it does, let’s address it’ and I don’t know why” (U.2contd-P-56).
A day in the life of Ryan based on Ryan and parent reports
Getting ready and going to school
Ryan gets up at about 6.45 a.m. and generally has a shower before doing his initial
catheterisation (U.1-P-4). He has “pretty good skills now at dressing himself and getting his
shoes on but he can’t tie his shoelaces” said the parent (U.22-P-270). It took a long time to
establish a routine and he needs visual reminders and a list which tells him what days to wear
sports uniform (U.19-P-226). The three children are driven to school “usually by 8 but quite
often we’re late … sort of near the 2nd bell”. Permission was granted to drop Ryan near the
school’s front door because in winter his legs get stiff and he finds the flat path easier. The
parent ensures Ryan has his water bottle because if he does not drink all day and gets
dehydrated, “his toilet doesn’t work so well that evening” (U.1contd-P-4).
At school
Classroom and homework tasks that involve handwriting are very difficult. “If he can
hide, he just won’t even start them” said the parent. If students are asked to write a story,
Ryan would have ideas in his head but “organising those ideas coherently and physically
writing them down just seems too hard so he won’t. You’d have to be there with him a lot of
the time which is difficult and you can’t do that in a classroom with 25 kids” (U.7-P-86). To
help Ryan record his ideas without the effort of writing, the parent purchased a Pocket PC
with keyboard and scribe which he can speak into. “He starts recording, speaks near it, stops
it then it’s down and it helps him to sequence” (U.8-P-102). Ryan was asked what he
thought about school “Oh! It’s great, I really love it”. When asked about writing tasks, he
said “writing … pretty good” (U.10-S-128). Changing from one task to another in class and
copying from the blackboard were also “great” (U.1-S-2; U.8-S-114; U.9-S-124). He
enjoyed cooperative learning where children “team up with peers” whose different strengths
and weaknesses are used to complete certain tasks (Levine, 1994, p.276).
Reading is good but comprehension, especially with double meanings and figurative
language, “fell way down” after the last operation but renewed interest in reading indicates

124
improved comprehension (U.5-P-80). Keyboard skills are “getting better” and Ryan chooses
to type spelling rather than write them out for homework. Up to the time of shunt revision,
basic maths facts, 3, 4 and 5 times tables and doubling strategies were good but post surgery
he was unable to add three numbers. “He’s still struggling a lot with maths” but at school,
students march and recite tables which has helped Ryan (U.10-P-114). He enjoys concrete
maths and spelling, making title pages for his books and he described a volcano with “real
good lava” that he made at school (U.6-S-4 2). Ryan loves working in class groups but he
tends to socialise a lot and needs a strong group leader, said his parent (U.20-P-248).
He always joins in the Physical Education class but the parent thought it was becoming
more difficult and Ryan who had more aware of his disability. A classmate said to the father
“Oh Ryan! He walks really well but he’s really slow at running isn’t he”. He puts his heart
and soul into sports days and swimming carnivals and everyone knows him (U.21-P-252).
Ryan said he likes swimming (U.14-S-279). The class did not have any boys to swim the 50
metres so Ryan volunteered. “He would have been two-thirds of the way down when they
were almost winning the race at the other end so the race was basically almost over when he
got down to the first end and everyone’s waiting to clap for Ryan ‘cause that’s enough, he’s
done a good job’ and when he turned around and came back this cheer goes up from the
whole school” and from his brother’s high school classroom next door (U.21contd-P-254-
262). When he got to the other end about two and a half minutes later “this roar goes up.
There wasn’t a dry eye in the house”. He does know that he’s slower and he does feel bad
that he can’t run as fast as the others but it doesn’t stop him. He’s got such spirit” said his
parent (U.21contd-P-262contd).
Coming home and homework
The boys are collected at about 3.15 p.m. and taken them home for a snack before
getting Ryan relaxed to “get him on the toilet. While he’s on the toilet in the initial stages
nothing’s happening so we usually start the homework and for an ongoing period I’ll stay in
there with him and sometimes help with homework” said the parent (U.1contd-P-4). He is
on the toilet for about an hour, sometimes one and a half hours, and then he showers, gets
dressed and watches some television before dinner at about 6.30 p.m. Bedtime is 8 o’clock
and Ryan is always asleep by 8.30 p.m.
“Homework’s been a hassle” said the parent who had watched other children Ryan’s
age doing homework “and they’re much faster, always. It’s always a struggle to do his
homework” because it takes more time to process instructions, make a start, decide that he’s
actually going to do it, have that idea in his head and the plan and motor movement to do it.

125
“It’s a struggle because we’re half way through a sentence and he’ll stop”. He needs
constant redirection (U.16-P-196). The parent ensures the house is quiet with no visitors and
no television, that he has a drink and everything he needs. When set up, the parent says
“now do it … now … no, no, now … do it mate, pick your pencil up mate … good … do it”
(U.16contd-P-198). He generally attacks assignments “with a fair bit of gusto” but he is not
keen on writing a lot of words so he has prepared PowerPoint assignments with pictures and
the main ideas that he can verbally expand (U.17-P-202). Ryan was asked how he felt about
homework and what he enjoyed doing most. “It’s great when it’s just writing or like reading
or voice recording ‘cause I can record all the stuff I need into it” (U.12-S-136-40).
Loneliness, friendships and anxiety
Ryan has good friendships with his peers, his brothers’ friends and his younger
relatives. “He’s pretty good socially, he’s got some good friends” said the parent (U.23-P-
308). At school, “he can interact with girls and he’ll interact with some of the boys” but
some boys his own age are the hardest group to get along with. Their play is centred on
activities which Ryan cannot keep up with and though they like him, they “tend to exclude
him from those activities or treat him as an inferior in that respect” (U.6-P-84). He has a
close friend in his class, some good acquaintances and some groups he can say “hello” to,
said the parent (U.6-P-84). Ryan enjoys visiting his buddies at the preschool and on
weekends likes to visit the homes of two other friends (U.16-S-300-304).
Tasks that Ryan enjoys
He “loves to dance and he’ll even have a go at singing”. He likes music but found
learning the recorder difficult. The parent had not been able to interest him in music “and
it’s difficult to find the time when he’s got to spend an hour on the toilet a day and it’s really
difficult just to get enough time to do his homework and finish his assignments” (U.12contd-
P-158-172). He plays the computer at home, loves swimming and jumps on the trampoline
(U.12-P-144-8). He can break eggs and mix cakes but he must be watched because “if he’s
using a hand-held mixer, he’ll lose concentration and point it towards the ceiling” (U.22-P-
270). At mealtimes, Ryan likes to help out “‘O! I’ll get the sauce’ … ‘who’d like a drink?’”.
He gets the cups and water out but he will sometimes say “‘hello, it’s too heavy, I can’t lift
it’ but he’s got it all out” (U.22contd-P-292).
Strengths reported by the parent
Verbal skills will be a strength that can be capitalised on in high school and “there
needs to be care not to give him too many written assignments”. Access to technology like

126
PowerPoint provides incentive to do neat work and quantity that “he can’t produce by hand
and they’re going to want quantity. If they want a quantity of handwritten work, they’re not
going to get it from Ryan” (U.26-P-358-360). Reading, decoding skills and confidence with
oral presentations are also strengths (U.18-P-216). “He’s actually quite good in front of a
group” and captivating and “it gives him a real boost ‘cause he does persist, he is a persistor
but it’s not recognised that he is because it’s so difficult for him to maintain his constant
attention and to focus on a task. So people actually see him as lazy when he’s actually trying
really hard” (U.4-P-78).
Tasks that Ryan finds difficult
Organising his work, staying on task, working from a complex set of instructions given
once and processing purely verbal instructions are difficult for Ryan (U.3-P-60). Small
blocks of work with clearly highlighted instructions given as framework are “definitely
better” (U.3-P-60-76). Planning is “awful”, motor planning, getting books out of his desk
and planning a task “he just doesn’t know where to start, he’s dumbstruck” (U.19-P-226).
Memory is a problem and “remembering what he did on the weekend was always really
tough for him”, said the parent (U.13-P-176). The family worked really hard on getting him
to remember what he ate for dinner the previous night, what he did on the weekend and what
he did at school. Concentration is even worse. “He’s just not able to concentrate for too
long on one thing” (U.13-P-176) but if he’s interested in something and if it’s hands on, he
seems to be able to maintain a longer concentration and be less fatigued by the task” (U.4-P-
78).
The oven timer is used to manage time and ensure routine tasks are done at home.
“When the bell rings, I want you to have finished this this and this” and “when the bell rings
that’s the time you get off the toilet and into the shower”. This encourages independence
and ensures things get done, said the parent (U.19contd-P-240). Ryan cannot tie his
shoelaces. “He just hasn’t got strong enough hands”. He learnt the process of doing it but
the motor coordination and planning is a challenge and “when he does get there it doesn’t
work anyway ‘cause he hasn’t got the strength to make them actually work so there’s no
incentive for him to learn to tie them” (U.22-P-270). He can use scissors “terribly … it’s not
good but he can do it”. He can rule a line with a ruler but he has to really concentrate. The
parent purchased a ruler with a ridge so he “can hold it really straight and securely”. He can
butter bread with soft butter and can make a sandwich completely (U.22contd-P-282).

127
When asked what tasks were difficult, Ryan said “finding all my stuff” and “getting all
my books out. Sometimes I have to get three books out at a time. It’s the big books I’m
having trouble finding like my SOSE book, Science book and Religion book” (U.5-S-38;
U.15-S-290; U.7-S-98).
Advice for parents and teachers
The parent advised other parents to be involved and find a way to advocate without
upsetting people “but you can’t be passive. I’m not saying be aggressive but I’m saying be
assertive. You really have to or you lose even the feeling of control and then you realise that
nothing’s going well and you haven’t been able to help because they’re not going to
naturally tend to try to cater for these special needs … it’s too hard” (U.24-P-316). Staff
wants to help ‘but they haven’t got the resources to do it so you need to be assertive and
supportive”. Be willing to share information, get to know the teacher and aides and talk
informally about “what they’re doing” with your child (U.24-P-316). Teachers were advised
to focus on strategies that Ryan can use independently (U.24contd-P-320 contd.).
Although difficult to know “how much knowledge is too much knowledge”, the parent
considered it sensible if everyone knew “what was going on” but “it’s not good if people just
label and say ‘o well, he’s got this and that means he’ll have problems with maths so we
can’t expect too much there”. The parent was unsure of how much knowledge to give
teacher aides without them lowering expectations “if they think there’s a cognitive gap?”
Maybe the best outcome is for “some of the specialists and myself to know the traits of
hydrocephalic learners” (U.24contd-P-320).
The parent suggested teachers learn how to vary teaching methodology to cater for
different learning styles so that once “you get to know your kids” and know the learning
difficulties linked to spina bifida, “you’ve got the two things you need to be able to tailor
your general class. It’s not just a program, it’s not just a unit that you choose, it’s tailoring
the whole way your classroom runs to cater for people who don’t learn routines as well, who
don’t sequence instructions as well, who don’t see the blackboard as clearly as you imagine
everyone can see it”. Colour-coding and a neat clear blackboard “can make the world so
much brighter for some kids and they’re not dumb, they’re just not the easiest student to
teacher. It would be lovely if every student was easy to teach but they’re not” (U.28-P-388).
“I really think that the Education Department don’t do enough. They should be
teaching more skills in learning styles, in evaluating learning styles of students” and doing
more research and training based around how to cater for people’s learning styles” rather that

128
just giving teachers access to a range of tools. Schools should be given more funding to
make direct instruction methodology available to those who need it. One cannot hope that
teachers will “find out that hydrocephalus involves a learning disability and you’re relying
then on parents who might or might not be emotionally strong enough to go and advocate for
their son or daughter. I think the Education Department needs to do more but I don’t know”
(U.29-P-392).
Have you heard of a Nonverbal Learning Disability?
The parent had read about the NLD syndrome and had collected most of the fact sheets
about hydrocephalus and learning difficulties published by the Hydrocephalus Association in
America. Fact sheets were lent to Ryan’s teacher whom the parent presumed would pass
them on to the next year’s teacher.
Ryan at school based on teacher and teacher aide reports
At school
Late arrival by 5-10 minutes meant Ryan often missed notices about “what’s happening
during the day”. In many ways, his teacher said he was expected to have a normal day like
every other child in the class with the interruptions of toileting procedures (U.1-PCT-6). He
enjoyed being involved in activities, loved talking about them and he excelled at class
discussions but “very much disliked having to sit down and do any work”. The teacher
described two different extremes - loving and enjoying interaction with peers and then
having to do individual work which he found very difficult (U.1-PCT-6). He did not like
leaving the classroom for toileting and timetabling meant he often missed out on something
special. Except on Monday, he is collected for toileting halfway through music, sport,
computer or library lessons or assembly “and the children notice that as well so it makes him
stand out a bit” (U.1contd-PCT-6). A normal day for Ryan was more tiring and more
physically, intellectually and emotionally fatiguing than for others but generally he was
“pretty happy to be at school”. By the end of the day he could get quite crampy and achy
and “getting any written work out of him at the end of the day just wouldn’t happen,
wouldn’t happen” (U.1contd-PCT-14).
The class teacher ensured he sat centre-front because “he needed so much spoon-
feeding all day long. He needs sentence starters all the time and constant supervision to keep
him on task” (U.10-PCT-128; U.17-PCT-168). He enjoyed drawing and art and was

129
unaware of the fine motor problems he has until Grade 4 when he became “more aware of
the differences between his art and other people’s art and there was this time when he
became quite upset over his problems” (U.7contd-PCT-66). If asked to draw a tree “his
didn’t really look like everyone else’s and the aide said he used to get mad and he wouldn’t
try” (U.19-TA-170). The class teacher who had taught Ryan for three years sat him down
for a special drawing activity that used simple shapes to draw say, a bird. “He became one
of the best bird-drawers in the class because he learnt how to do it a special way. So he
enjoyed that, very much so” (U.7contd-PCT-66). He is a very imaginative child and “should
be able to write terrific stories” but writing them down is difficult (U.18-TA-164).
Ryan is quite a good little reader and enjoys talking about all kinds of topics such as
science, various books or a CD that Dad bought (U.7contd-PCT-72). He was “happy
enough” with basic maths addition but more complicated problem solving situations “no
hope at all … didn’t like that at all” (U.7contd-PCT-72). In the playground, he managed
“perfectly well. He was very very active before the shunt revision; a very active child in the
playground … ran, jumped and climbed up and down stairs and over rocks. He didn’t expect
anyone to give him special treatment because of his difficulties. He was out there with the
best of them” but over the last 12 months, he was not as active as he used to be (U.26-PCT-
297; U.5-TA-48; U.11-TA-78).
Loneliness, friendships and anxiety
Loneliness per se was not reported. In the Year 3-4 composite class, the teacher said
Ryan “tended to play with children who were outside the social norms, so those children
who were normally isolated, who were normally loners and have a few social difficulties of
their own” (U.1contd-PCT-8). One child was in Grade 3 “so a year younger than he who
had a lot of behavioural and emotional problems” and “a girl his own age but she has
obsessive compulsive disorder and a lot of depressive, emotional problems” (U.1contd-PCT-
8). The teacher felt Ryan struggled emotionally because “it’s pretty hard being friends with
those two kids but it was his choice … ” Because of his immaturity, “he tended to play more
with these children who were more accepting of the differences”. Ryan had a special friend
in another class, a “very intelligent child”, a different thinker who is quite happy to sit and
talk at length with Ryan and possibly an excellent pair-partner for Grade 5. “He’s the kind
of kid who could happily sit there and re-explain what the teacher has said or give Ryan
sentence beginnings. He’s a social misfit again because he is such a different thinker and
he’s an intellectual child” said the teacher (U.27-PCT-301).

130
Ryan was never ever teased, criticised or left out (U.1contd-PCT-8). He had “quite a
lot of good friends” and at lunchtimes, the aide said he does everything the same as other
students (U.13contd-TA-108). She ensures toileting is done before breaks so he can join his
peers (U.15-TA-131). Everyone knows him and he plays with the same group of children
and has done for quite a few years. “I’d say even when they’re in different classes they still
stay friends with him” (U.13-TA-100). When asked about Ryan’s relationship with teachers
and aides, the aide said “Oh well! Of course I love him to death so it’s different”. She had
been with him since Grade 1 and “he’s been fine with everybody” (U.8-TA-72). Friendships
cause Ryan to get anxious and worried and the aide reported “a few times when he’s been in
tears” because a student “won’t talk to me” or would not play at lunchtime. “He’s getting a
little bit older now but he is young in his head” (U.13-TA-98-100). Otherwise, she thought
he would only get anxious “if he’s going to miss out on something” (U.9-TA-74).
Strengths reported by teachers
Verbal skills, an incredible imagination, a great sense of humour and being very
thoughtful of others were strengths reported by his teacher (U.28-PCT-307). “In a lot of
ways he’s quite determined. He doesn’t let things beat him but in some respects he sits back
and lets you do things for him” said the aide. Mostly “he does whatever everyone else does
even if it is difficult for him so I suppose his determination” (U.17-TA-150).
Special teaching arrangements and sport
The twenty minutes of teacher aide time allotted to Ryan is used to supervise toileting,
ensure his hands are washed and that he follows the catheter cleaning procedure. The time
taken and any problems are recorded (U.3contd-TA-18; U.15-PCT-158). Class reward
programmes are used to keep his incentive alive. A tick or “5” for excellent work in the
morning builds up to being some kind of special reward such as extra computer time. The
idea of a pain scale worked well (U.35-PCT-371). When he talked about pain, the teacher
found it hard to gauge severity so she now asks “okay your pain, on a scale of 1-10” and if
above 5, she would know it was really bad and he was not “just winging” (U.36-PCT-371-3).
The aide did lots of keyboard skills with him in the past and the class teacher ensures he
gets at least ten minutes on the computer every day to comply with IEP goals (U.8contd-
PCT-182). The aide said he gets very tired doing bookwork and needs pushing the whole
time. “You virtually have to sit there one-on-one with him and say ‘write that’, ‘write that’
and ‘write that’”. He would know the answer but getting him to write it down … “I don’t
know whether that’s laziness or his disability”. She would say “I’ll write the next three

131
words and you write some more” (U.3-TA-10-12). She thought he did not like doing much
at all but considered him “quite capable of doing it … whether he gets tired or whether he’s
lazy is debatable …” (U.2-TA-6).
Ryan loves sport and although “he no longer plays like he used to at lunchtime”, he still
participates in formal sport activities such as the 800 metre fun run or two laps of the oval.
He was the last to finish “and the entire school cheered him on and he was just about ready
to fall over” said the teacher who ran the last 200 metres to get him over the line. He is quite
a good swimmer and even though his muscles tire easily, the teacher mentioned his readiness
to swim the 50 metres. “‘I know I’ll be last but I know I can do it’ and that encouraged other
boys to swim as well and they wouldn’t have done it if it wasn’t for Ryan and again he was
the last one to the finish line and the whole school, they’ve got a special cheer for Ryan. It’s
really lovely so he loves that” (U.7-PCT-64).
Getting class work finished
“Most classroom work isn’t finished” said the teacher and aide (U.11-PCT-142; U.11-
TA-78). People from the Spina Bifida Association suggested covering sections of visually
challenging pages to increase white space between activities and circling those to be done.
The aide often thought Ryan’s inability to finish a task from the board or in his books was
“just laziness and spoiltness” but she observed he got “a lot tireder quicker” and tardiness
with task completion may be due to his writing “‘cause he can’t sort of keep up with the
writing” (U.11-TA-78). His teacher considered him “a pretty happy-go-lucky little boy”
who would sometimes get disappointed and frustrated at not being able to complete activities
within a timeframe (U.15-PCT-158). He was unable to “get done what a normal child
without his difficulties would have gotten done in class so it was easier to manage it
beforehand and reduce the amount of work that he had to do”. Even with reduced
expectations and scaffolding, he tended not to finish and would tire, lose concentration and
get easily distracted (U.11contd-PCT-144). To give him a sense of “I’m finished the job”,
some work was taken home where Ryan conveyed ideas and his Dad would scribe them”
(U.11contd-PCT-144).
Homework and assignments
If he was too tired to work in the last hour of school, “he’s going to be too tired to do
homework” said the teacher. Ryan found it very difficult to finish homework but the parent
had good weeks where a lot got done and “other weeks where it wouldn’t” and that
depended on his tiredness at the end of the school day (U.22-PCT-252).

132
Copying from blackboard and handwriting
Copying from the blackboard is very laborious and the teacher used colour-coded dot
points to help students with eye, auditory processing and attention problems. This broke a
copying task into stages and Ryan “could do that much more easily” (U.17-PCT-168). The
teacher would circle or underline what Ryan should write as dot points “because he couldn’t
always read a sentence and take the key words out so he could not work from the board like
most children could” (U.17-PCT-168).
“As soon as you said ‘pick up a pencil’ he would talk about it, he would discuss it, he
would happily draw it, he would act it out but writing about it, he just couldn’t think of how
to start a sentence. He would be stuck. He had no hope of being able to” said the teacher
(U.8-PCT-72). Ryan would know the facts or answer but would not know how to write it. If
the teacher gave him two or three words of a sentence, he could finish the whole sentence
without hassle but thinking of how to start a sentence “he couldn’t do”. “‘On Christmas
morning, I …’” no hassle but as to how to start a sentence, he cannot do that. “There’s all
the ideas up here but he can’t put them into words” and into writing (U.8-PCT-74; U.1-PRT-
2). His writing is “quite large, poorly spaced and quite crammed together. He found it very
difficult to write on lines” and it tended to slant upwards (U.8contd-PCT-188; U.4-TA-40).
But when Year 4 students of the 3-4 composite were asked to “do all their joins”, Ryan
started doing cursive “and he was actually quite fluid when he was writing with joins”
whereas he was “really struggling with the actual manual printing of the words”. The
teacher spoke of writing “where he’s stopped, he hasn’t finished the sentence or he hasn’t
finished a word. He’s only halfway through a word and he’s stopped and I found this didn’t
tend to happen when he was doing cursive” (U.8contd-PCT-92). She spoke of reprimand
because she had inadvertently not read the IEP in detail which instructed “teaching him to
type rather than teaching him how to write” (U.8contd-PCT-86).
Comprehending and following instructions
Following instructions and shifting mental set were difficult for Ryan. If students were
to get out a maths book, the teacher would jot book name and page number on the board
“because by the time he finally found what he was looking for, he couldn’t remember the
page number” and this helped students to focus on the key message (U.14-PCT-152;
U.10contd-PCT-132). The teacher also used “the count of 5, so counting helped” but she
would forewarn Ryan about a task ending, read his last sentence or maths activity and say
how long he had to finish (U.14-PCT-152). He may get distracted during the introduction to
a new lesson “and it’s probably a mental difficulty, being on one wavelength and having to
think about something else so I had to make sure he was quite focused” (U.16-PCT-166).

133
Planning, organisation and time management
Ryan had a lot of difficulties with planning and organisation. “He needed to be told
what to do, when to do it and how to do it every time” said the teacher. His ability to
manage his desk was very limited despite trying all kinds of things. “At one stage we had 4
or 5 pencil cases, one for his writing pencils, one for his crayons one for his felt pens and
they were see-through then we tried a big one for everything to go into and that didn’t work
well either”. A big improvement was replacing the desk made for a child with physical
disability with a standard desk with fold-back lid which doubled as work space (U.18-PCT-
204). In Term 4 “he had a tidy desk and it was the biggest sense of pride for him”.
Everything was clean, tidy and organised and the different design made such a difference to
his life and his ability to find things. Sometimes he would almost be in tears because he
would spend 4 or 5 minutes looking for something that was there “but he couldn’t find it”.
The previous desk was “specially purchased for him but it wasn’t functional” because it
required him to “hold the lid up all the time” (U.18contd-PCT-204).
He is very forgetful of things he needs to do such as meeting the aide for toileting at
10.20 a.m. and 1.30 p.m. “but he couldn’t remember”. At the beginning of the year, he was
really good but in terms 3 and 4 he could not remember at all and could go for hours without
saying to himself “Oh! I haven’t been” (U.19-PCT-218).
Handling novel tasks or situations
Ryan “did like a strict routine, very much so he liked that” said his teacher. Before the
shunt revision, he was showing signs that he was “ready to look at learning multiplication
and understanding the concept. Afterwards, he just could not understand it. He had no hope
of understanding it. It was far too complex for him … So at the end of the year, the only
way for him to learn his multiplication was just as tables and regular practice and repetition”
(U.31-PCT-337).
Rote memory skills
Spelling was “actually very good … one of the best in the class”. By using rote
memory skills and counting patterns, Ryan could do his 2, 5 and 10 times tables but none of
the others (U.32-PCT-345-51).
Concentration and memory
Concentration and memory are quite poor. The teacher reported times when he could
sit and focus on a task he enjoyed for a long period of time but if it became physically or

134
mentally challenging, he would tire and be quickly distracted (U.21-PCT-250). In Term 1
“his memory was quite okay really and his ability to chatter away about what he’d done on
the weekend and he was always full of stories and he’d chat away to us whereas that stopped
in term 3 and 4. It was real difficult to draw information out of him” she said (U.5-PCT-38).
Short-term memory was “definitely much worse post than prior” shunt revision and he had
“such terrible headaches and was so lethargic and unwell” for a few weeks beforehand that
he was not functioning at all (U.5-PCT-38). As far as ability to work independently, his
short-term memory crashed. He could not remember what he did yesterday so in terms 3 and
4 when asked to write one or two sentences about the weekend, the teacher asked pointed
questions “did you do this” and he would sit there “so short-term memory was quite poor”.
Working memory was much poorer so ability to work with numbers was impaired. Ryan
and the teacher would work out a sentence starter and “he’d have to go sit down and write it
but by the time he’d sat down he’d forget what the sentence starter was. So I noticed that a
lot and he was very achy post operation, very achy for the whole of the year” (U.4-PCT-34).
“I reckon he’s got an excellent memory” said the aide but concentration to stay on task
is not always good but “a lot of times I put things down to being spoilt or lazy but I’m
probably wrong. I say that because I deal with normal children that don’t have any problems
and he’s so normal in every way to me that I suppose I jump on that and think he’s just being
lazy” (U.22-TA-232). The hardest thing at present was “keeping him on task in class” (U.6-
TA-68).
Verbal skills/vocabulary
Verbal language was “very well developed actually” but a relief teacher observed
during story writing that Ryan “had the ideas but he couldn’t actually write them into
sentences. He needs one-on-one or I’d actually tell him just to draw a picture of it in the
steps” (U.1-PRT-2). “He can talk about anything, has no trouble” and tells a lot of stories.
He mightn’t do that to everybody but he does to me” said the aide. Vocabulary was
excellent said his class teacher who recently scanned a piece of Ryan’s work – a short
conversation from an ancient Greek myth between Perseus and King Polydectus. “He had
some quite complex vocab for a child that age, really very good and all correctly spelt”
(U.33-PCT-353). The teacher encouraged Ryan to think and type draft work straight into the
computer because he used more interesting, mature vocabulary when typing than when
writing (U.9-PCT-116).

135
Everyday taken for granted skills
The most difficult everyday task for Ryan is writing “particularly if it doesn’t involve
any copying” and if asked to copy a whole paragraph from the board, “that’d be too much
and he would just emotionally and mentally collapse at the thought of it. He just wouldn’t
be able to start it” but would copy circled or underlined key words or bullet points “quite
happily” (U.24-PCT-262).
Using scissors is quite difficult and the teacher would sometimes cut things for him
“because he was quite a perfectionist” and he became frustrated and teary if he could not cut
things correctly. Ruling up lines on a page was very difficult because he could not keep the
ruler straight, “couldn’t hold it properly so when he went to move the pencil along, it would
just slip … he had no pressure” said the teacher (U.23-PCT-253; U.14-TA-122).
Ryan learnt to put on his shoes and socks in Year 4 “and it was a big thing for him to
learn to do”. He cannot do shoelaces and he finds the long school socks or ribbed sports
socks “quite difficult to put on” (U.24contd-PCT-268; U.16-TA-136). The teacher asked the
parent to provide him opportunity to learn these skills. She recognised this would slow him
down in the mornings “but I felt it was better for him to learn how to do some self-care
activities and also because he would need to go swimming” in terms 1 and 4. He wears a
swim shirt to cover his scars “but getting that up over his shoulders and manipulating his
shoulders and his arms is quite difficult” so the teacher or aide would help “but he found it
quite challenging to get changed” (U.24contd-PCT-270; U.16-TA-136).
Group work with peers
Ryan would want to work immediately with the children who had some social and
academic difficulties of their own said the teacher (U.25-PCT-284). The aide added “he
would be in there doing his thing whether it’d be right or not is another thing but he’d be in
there with the group. He would work with them” (U.12-TA-94). The class is mostly
cooperative but there were times where children got “a bit testy” and because he was
unlikely to write a great deal, some “perceived him to be the slacker in the group, not
contributing a great deal” (U.25-PCT-284). If a particular child was getting annoyed, the
teacher would take the student aside and quietly explain Ryan’s situation and the child would
be much better. It was very important to pair him up with the right children “and you
couldn’t choose the same children all the time because then they would tire” (U.25-PCT-
284). “There’s a lot to being a peer mentor, I mean they have to really understand the task
themselves to be able to ask him the kind of questions that would help him out” said the
teacher (U.25contd-PCT-288).

136
Critical life skills as represented in school
The teacher reported “quite a few soiling accidents” that Ryan was not always aware of
because “he doesn’t have a great deal of sensation in his lower half” (U.20-PCT-220; U.26-
TA-292). He once reported a “very obvious” accident that wet the front of his shorts and his
shoes. Both teacher and aide thought this was unusual because he normally needs a catheter.
The teacher contacted the aide and to save Ryan embarrassment, she told the class she was
sending him on an errand to the office. On arrival the aide said “take everything off, take
your shoes off”. “‘Ohhh’” and he smacked his face as he realised he had a container of
bubble mixture in his short’s front pocket “and he’d wet himself all over and it was bubble
mixture so from then on we’d just quietly call him ‘hey bubble boy!’. It was our little secret
joke but he didn’t have very many accidents really just a few where he was soiled and he
found it very difficult to wipe himself. He couldn’t see, couldn’t feel and he found it quite
difficult to balance himself” (U.20contd-PCT-228). At an IEP meeting, the teacher
suggested a mirror in the bathroom so he could actually see what he was doing and because
he is going into Year 5, the aide had said “‘there has to be a stage where he needs to become
more independent in wiping himself’” (U.20contd-PCT-228).
Although the aide has followed him from Infants to Year 4 (U.21contd-TA-230), it was
starting to bother her that she might still be helping Ryan with these tasks in Year 7 and “I
would like him to be more independent but I don’t think his Dad helps. I have no authority
but just talking to his Dad at meetings they’ve tried a lot of times and I really think he needs
to make him more independent” (U.21contd-TA-216contd). If there is soiling, “it’s really
hard when you’ve got those braces on your legs. You’ve got shoes and socks on, your pants
are there but you’ve pulled them down and your undies are dirty and how to get them off
over your shoes. It’s really hard but I try to make him do it himself and I just have wet ones
and things there and I say ‘there they are’ and it nearly breaks my heart sometimes but I have
to you know” (U.21-contd-TA-214).
An IEP meeting early in the year was convened and the class teacher was questioned
about toileting procedures. “‘Well I don’t do it, my teacher aide does it, she should be
here’”. The aide believed questions about toileting should be directed to her … “why ask
somebody that doesn’t even do it” (U.25-TA-252). “That upsets me about Ryan because
often there’ll be a big meeting and I won’t be invited” (U.24-TA-238). There might be 8
people, “all people you know specialists very educated, highly educated people and I feel a
little bit intimidated actually but still when you get down to the nitty-grittys, I’m the one
who’s wiping his bum aren’t I so if they want to ask anything about that sort of thing, it’s no
use asking anybody else”. “They just don’t understand that but they have no idea. I might

137
be late for something and they’ll say something and I’ll say ‘O I had a problem with Ryan’
and they look at you and they have no idea what you’re talking about. ‘Do I have to spell it
out … hhh’” (U.25contd-TA-260-66).
The teacher raised the family background and its impact on how Ryan deals with life.
She felt that the parent and older brothers “do tend to do a lot, too much for him at home”
(U.6-PCT-56). “There’s a few years difference between him and the older brothers. They
don’t always get on, definitely don’t always get on and it’s also probably very hard for the
older brothers as well because they are to a certain extent co-carers with Dad” (U.6contd-
PCT-60). She acknowledged there was a lot involved with caring for Ryan “so they’ve had
to grow up and deal with things that most kids their age wouldn’t have to deal with. So it’s
just a slightly difficult family background for him” (U.6contd-PCT-60).
Teacher and aide perceptions of Ryan as a person with a disability
Advice for other teachers
Use bullet points, help them to find key words and experiment with organisational
strategies to discover what will help them manage their materials. Transparent pencil cases
were good and Ryan’s parent put the name of every book on every corner of each book, top-
bottom-right-left, back and front “so if he’d put his book in upside down and back to front,
he’d simply have the word ‘Daypad’ there facing him. So he could just lift it up and he
didn’t have to turn every book over”. Colour-coded covers would also help, said the teacher
(U.29-PCT-309-11).
Different coloured chalks and laminated strips of cardboard for writing sentence starters
was helpful. Journaling may involve writing about the weekend. “If I then asked them to
move off and write about it, he couldn’t. But if we decided on three key ideas, I could jot
those ideas down and write three sentence starters. After that I felt he could write easily and
put those key ideas into those sentences” (U.29-PCT-313). The aide said “I think every kid’s
different and well every person’s different too aren’t they so they like … I can’t think of
anything else other than just love ‘em that’s all” (U.26-TA-286).
Teacher and aide understanding of learning difficulties
“Ryan has been perceived at times by some teachers as being lazy, as being a very
capable child, a bright child but perhaps molly-coddled at home, babied too much, too

138
dependent and because of that dependence that’s why he’s not able to do things
independently by himself. So because he’s so used to having everything done for him, the
perception is that he therefore can’t go off and write a short story about his weekend, which
he can’t, but for other reasons so the perception is that he can be lazy …” (U.2-PCT-22). A
relief teacher perceived Ryan as a “bright little boy, brighter than what he gives off as a
perception” (U.1-PRT-8).
The aide puts difficulty staying on task down to “being spoilt or lazy … I say that
because I deal with normal children that don’t have any problems and he’s so normal in
every way to me that I suppose I jump on that and think he’s just being lazy. But from when
I go to meetings with all the hoo-ha when everyone comes and assesses this and does that
and I hear things that I think ‘well maybe I’m wrong there about … maybe it’s a problem he
has” (U.22-TA-232). When the researcher asked if difficulty finishing tasks may be linked
to slow mental processing, the aide said “I don’t know that. I only see a little boy and I’m a
Mum. I only see what I think I see and I have no qualifications to see there might be a
reason for these things. I probably treat him the same as other kids. Maybe I don’t know
enough about his limitations” (U.11contd-TA-80). Speaking about support in and out of
class, the aide said she treats him like everyone else in class and “probably I’m harder on
him but the minute we walk out that door that’s different, toileting’s different” (U.21-TA-
198).
“One of the biggest things is how do I get him to work, how do I get him to want to
because he doesn’t simply want to” said the class teacher (U.12-PCT-146). She questioned
a connection between shunt revision, attitude change and being very achy. He was very tired
and he continued to be achy and tired for the whole of the year “and I imagine if I was
feeling tired and I was achy all day long and I had cramps in my legs and my muscles, then I
probably wouldn’t be particularly motivated to work and learn either” (U.13-PCT-146).
Have you heard of a Nonverbal Learning Disability?
“Nonverbal, what is it? So is it a visual …? Can you give me examples of how that
might manifest” asked the teacher. Characteristics of the syndrome were described and
causation was explained by the researcher. “He certainly has what you were saying when
you were describing it. It certainly matches what I find with him. I’m very glad that I’m not
teaching him next year ‘cause I need a break because it’s very exhausting. On the other hand
I’m really sad that I’m not teaching him next year because it’s very interesting, very
challenging, very very rewarding and he’s a lovely little boy, just a lovely boy” said the class
teacher (U.34-PCT-357).

139
Summary of 2005 Psychological and Speech Assessments
The following extract has been taken directly from the assessment reports.
2005 (aged 10 yrs 2 mths) Full Scale IQ = 88
Verbal IQ = 88
Performance IQ = 91
VIQ-PIQ difference = 3 (not significant)
Language assessment age equivalent = 8 yrs 0 months
Problem Solving age equivalent = 5 yrs 11 months
On a test of general intellectual functioning, Ryan performed within the low average
range for a boy his age. Ryan performed within the low average range on the verbal
component of intellectual functioning but performed with the average range on the non-
verbal component. Ryan experienced difficulty on a task of word meanings and ability to
express them verbally. He had difficulty with a task which assesses practical knowledge of
social situations. Ryan also had difficulty with a task assessing 2-dimensional visuomotor
skills. Finally, Ryan had difficulty with a task which assesses speed of information
processing.
Ryan does have significant learning difficulties that need to be considered in his
academic program. These areas are as follows:
• Acquiring new material as well as retrieving information from his memory;
• Any task which involves an organisational component (e.g. having a tidy desk to
undertaking a project);
• Processing information quickly (e.g. having to follow a set of instructions);
• Any task which involves speed of hand-eye co-ordination (e.g. undertaking work
from the blackboard);
• Attention and concentration;
• Knowledge of word meanings and expression of them;
Interpretative discussion
The class teacher appeared sensitive, understanding and constructively responsive to
Ryan’s educational and emotional needs. To support peer understanding and acceptance, she
wove a segment on “The Walking Miracles in our Class” into a Science lesson. This gave

140
each child opportunity to speak about any personal illness or surgery experienced and
undoubtedly enhanced empathy (diary notes). The following excerpts reflect on perceptions
of a student diagnosed with Partial NLD, an Executive Function Disorder, specific deficits in
the memory domains and whose intellectual functioning was in the low average range. Prior
to this study, there appeared to have been no formal assessment of Ryan’s intellectual and
functional impairments.
“As soon as you said ‘pick up a pencil’ he would talk about it, he would
discuss it, he would happily draw it, he would act it out but writing about it, he
just couldn’t think of how to start a sentence. He would be stuck. He had no
hope of being able to” said his teacher (U.26-P-358-360). The parent, class teacher
and aide reported problems with writing (U.8-PCT-72; U.3-TA-10-2). Handwriting for
children with spina bifida and NLD characteristics is a complex task because it involves
“thinking, memory, language, attention and fine motor skills” (Lutkenhoff & Oppenheimer,
1997). Ryan knows the answers and he has the ideas but as Sandler (1997) explains “the
strain of remembering and executing the letter formation, organising the words into
grammatical sentences and developing a narrative sequence can lead to fatigue, loss of
motivation and decreasing academic self-esteem” (p.88). The teacher noticed Ryan would
stop halfway through a word but this did not happen when he was doing cursive writing. I
queried whether the continuous contact of pencil on paper kept him focused whereas the
lifting between letters when printing may increase distractibility. The teacher said “that’s
exactly what I think it was” (U.8contd-PCT-88). Rourke (1995) says the writing skills of
children like Ryan “are usually very poor during the primary grades of school” but may
become “smooth and effortless” because of the child’s ability to routinise this activity
completely since “routinisation and stereotypic application is thought to be a process for
which left hemisphere systems are particularly geared” (p.14). With practice, time and
endurance, Ryan’s handwriting skills may develop further.
“He couldn’t always read a sentence and take the key words out”. So he
could not work from the board like most children could, said the teacher (U.17-
PCT-168). The parent, class teacher and aide spoke of Ryan’s difficulties copying work
from the board (U.18-P-388; U.21-TA-198). Test results report that visual-motor perception
were in the “average range for a boy his age” but any task which involved speed of hand-eye
coordination (e.g. undertaking work from the blackboard) was an area of significant
difficulty together with slowed ability to process information, understand word meanings

141
and express them verbally. The age equivalent of Ryan’s language assessment was 8 years,
2 years 2 months below his chronological age. If difficulties with visual, motor,
comprehension and extracting key words from a sentence are combined, the handwriting task
becomes a painstaking job for this little boy. Fortunately, his teacher managed these
difficulties beforehand by circling or underlining what he should write as dot points.
“He never finishes a task from the board or in his books. I sort of, well I
often thought it was just laziness and spoiltness but I think he does get a lot
tireder over the years he’s been getting a lot tireder quicker” (U.11-TA-78). The
aide wondered if difficulties completing work from the board or bookwork was “just laziness
and spoiltness” but she thought he got “a lot tireder quicker”. For a child with spina bifida
and hydrocephalus, it takes their full psychological and physical energy just to get through
the day. They are often exhausted at the end of a school day. The aide spoke of seeing only
what she thought she saw and of having “no qualifications to see there might be a reason for
these things” (U.21-TA-198). The father questioned how much information should be
provided to aides. Regardless of whether teacher aide time is used for toileting or class
support, should she not have the same information about a student with special needs
available to her as teachers and why is this aide not invited to planning meetings since she is
“on call” to attend to whatever personal or classroom issues arise with Ryan?
He is very forgetful of things he needs to do such as meeting the aide for
toileting at 10.20 and 1.30 “but he couldn’t remember” (U.19-PCT-218). The parent
also said “memory is a difficult issue” (U.13-P-176) yet the aide thought Ryan had an
“excellent memory” (U.22-TA-232). Testing revealed Ryan had great difficulty with verbal
learning and memory. He could retain a certain amount of the information presented but at a
level much lower than that expected of a typically developing child. Forgetfulness and poor
concept of time cause frustration for teachers and families especially if an important school
or telephone message was forgotten. Time may be considered a vague, abstract and
intangible concept. Rourke et al. (2002) speak provisionally about an “extremely distorted
sense of time” because it has not yet been thoroughly investigated, but they suggest it may be
evident in alertness to time of day and time taken to manage common everyday activities
(p.160).
142
“Nonverbal, what is it? So is it a visual …? Can you give me examples of
how that might manifest” (U.34-PCT-357). The parent provided most fact sheets about
hydrocephalus and learning difficulties from the Hydrocephalus Association in America to
Ryan’s teacher but when asked about NLD, the teacher was unaware of the syndrome.
Fortunately for Ryan, this astute teacher identified and addressed problems as they arose.
Should not all teachers and aides be made aware of the syndrome’s profile to avoid the
“lazy”, “spoilt”, “babied” labels being applied to a student who genuinely wants to please,
achieve and succeed? I believe that teachers and aides are generally caring, conscientious
people who want students to succeed but they have insufficient time or energy to research
this learning disability. Given these constraints, it would make good sense to teach
prospective teachers about an NLD during pre-service training and inform practicing
teachers during in-service training.
Conclusion
In the school context, Ryan does not have any behavioural problems. He reads well, he
has an excellent vocabulary and he enjoys talking about all kinds of topics. He is a good
speller, he can handle basic maths but word problems “no hope at all”. Although he has a
special friend and he visits buddies in the preschool, he gets anxious and worried about
friendships. A teacher said he tends to play with children outside the social norms who are
more accepting of the differences. Problems with handwriting, copying from board,
planning, organisation, time management, fine motor, finding things in his desk,
comprehending and following instructions for any new task, handling any change to routine,
concentration and memory, starting and finishing class work without help and completing
homework present a severe range of impediments. School day mornings are difficult
because Ryan needs constant reminders but he is still late for school sometimes.
Language assessment said “there is much in his world that he doesn’t comprehend
fully” and “there is much in communicating his ideas that he finds difficult”. Ryan also
“struggles to integrate the many parts to a social situation and formulate that information into
a main idea”. On a Test of Problem solving, Ryan’s age equivalent was 5 years 11 months,
well below his chronological age of 10 years 2 months. The going must be tough yet the
teacher said this little boy has a great sense of humour and he is very thoughtful of others.
Educators are ready to blame parents for their child’s deficient self-help skills yet it is
reasonable to suggest that all parents dream of personal independence, happiness and
autonomy for their child. Ryan’s teacher acknowledged that his older siblings were to an

143
extent, co-carers with the parent “so they’ve had to grow up and deal with things that most
kids their age wouldn’t have to deal with (U.6contd-PCT-60). This little boy needs to be
catheterised and showered every morning before school and family life may revolve around
these routines. Staff asked the parent to provide opportunity for Ryan to learn some self-
help skills but before school, time and the needs of other family members are also critical.
The mornings can be exhausting because the child also needs help with tasks that age-peers
do automatically. Siblings often stand aside because the parent is preoccupied with
attending to such needs. The pressure is on parents to get children to school on time and
teaching staff complain if they are late. Parents feel very responsible when they arrive late,
as the parent said “you feel terrible” (U.19cntd-P-246). If common sense and fairness to
Ryan, his family, teachers and aides is to prevail, it appears that a meeting at the start of each
school year would benefit all, a meeting where collaborative discourse can lead to new
understanding of the full picture.

144
CLAIR’S CASE STUDY
Context of Clair
Family life
Clair is a Year 6 student at a state primary school which has an enrolment of about 626
students. She was born with a “quite big” myelomeningocele (T.12) which was closed at 7
days of age. A ventriculoperitoneal (VP) shunt was inserted on the left side of the head at
around the same time (U.30-C¹&S-628). Over the years, Clair has had two shunt revisions at
age 3 years and 4-5 years of age (U.27-C¹&S-589). She lives with her grandparents who are
retired and they have cared for her for the past four years. Clair visits her mother and older
brother and sister on weekends and a carer brings her back for the school week. Grandma
said the brother is a “looker-afterer” kind of boy. The sister and Clair used to play well
together but the sister is now quite “advanced” and they do not seem to share the same
interests. Clair uses a wheelchair because she is paralysed below the waist. The school she
attends has a Special Education Class (SEC) where Clair spends 3 days per week and the
other 2 days are spent in her mainstream class. Five students including Clair attend SEC
classes. She is ascertained as Level 5 Physical Impairment (PI 5) and the Special Needs
Teacher proposes to advocate for Level 6 (PI 6) on entry to high school (U.2contd-SNT-
10contd). As an integral part of this study, Clair undertook psychological assessment.
Unbeknown to the school counsellor, he conducted psychological assessment with Clair just
10 days later and she did not mention the first assessment. The school counsellor is reported
to be considering Special School for Clair from Year 8.
Clair has an active complex partial seizure condition which started after major back
surgery when she was 6 years old. The seizures occur at random and each one lasts about 60
seconds. The back surgery, which took about 6 hours, was to arrest kyphosis and insert a rod
into the back. Kyphosis is an “abnormal condition of the vertebral column characterised by
a convexity in the curvature of the thoracic spine” (Mosby, 2002, p.965). The operation
could not be done “while there was any speck of broken skin” which caused the grandparents
to protect her from any kind of accident (U.21contd-C¹&S-483). The grandmother worries
about the seizures and Clair’s future and she sometimes feels the school think the medical
professionals “aren’t waving the magic wand … see it’s the epilepsy that’s the big thing”
(U.26-C¹&S-581). She spoke of communications with doctors about Clair’s seizures and the
possibility that “at puberty they may disappear which is what we’re hoping for because if it
weren’t for that, her learning would be much better” (U.26-C¹&S-583). Risk factors that

145
precipitate seizures are tiredness, hot weather and stress. Clair does not like the sun or hot
weather “but swimming, we’re working on” (U.21contd-C¹&S-487). The grandmother said
“she doesn’t seem to perspire and the heat builds up” which could be a side-effect of
medication for bladder incontinence (U.27contd-C¹&S-595-601). When a seizure occurs at
school, Clair is taken to lie down in the SEC where she is supervised until well enough to
leave.
During the initial telephone discussion, Grandma said Clair speaks well, is good at
spelling and likes reading “on good days”. She knows her times tables but Grandma needs
to sit with her for homework tasks. A funding package provides for a carer to come for 2
hours twice per week to help with homework. An IEP is in place at school. Organisational
skills were being worked on at school and these have improved. Clair can manage some
taken-for-granted tasks such as doing her hair, buttons and hooks and concentration is “not
too bad if she likes it”. Grandma said Clair can remember difficult words such as
“discriminating” and “predictive” and she would ask their meaning rather than look them up
in the dictionary. She has friends and is a chatty girl “but tends to be bossy”.
The grandmother raised concern about Clair’s “withdrawn” moods at times. Normally
she is chatty and bouncy but in the last 6 months “she has been sometimes disinterested and I
think that’s all to do with disability and epilepsy so that’s why we ended up in the hospital in
January because we just didn’t know what to do”. The hospital said symptoms were anxiety-
related but Grandma considered them to be depression or “bordering on depression” (U.32-
C¹&S-640). Clair has been attending a local child mental health clinic to learn self-help
techniques for getting to sleep. The clinic also helps children with social interaction skills.
Grandma said Clair likes male company and this has been a concern because Clair likes to
hug people. She told Clair that she should not lie on anyone because she is no longer a little
girl. Clair said she does not do this anymore. Educational experiences so far have been
satisfactory and Grandma reported that all teachers at the present school including the SEC
“have been very good but I think they are put off by the fact that Clair verbally is very
expressive and may not catch things sometimes” (U.2-C¹&S-8).
Past school experiences
Clair used to get in trouble a lot in Year 1 and was sent to the Responsible Thinking
Chair (RTC) every day. When asked why she had to go there, Clair said “‘cause the teacher
thinks I was doing the wrong thing and I didn’t do anything wrong … remember I hate that
school so much”. The teacher thought Clair was ‘yapping and thinking of other things’ “but
I didn’t do it” said Clair. “I hate that teacher. She’s a mean, angry, poopy, grumpy teacher”.

146
Grandma thought Clair was the only child in a wheelchair at this school and toilet facilities
did not cater for her special needs. Clair started at the present school in the middle of Year
3. “I like this school better now. I’ve got billions and billions of friends” (U.18-C¹&S-395-
414). Clair said that after Year 7 she would be going to the high school next door which
Grandma said has a “proper disability unit” U.19-C¹&S-427).
A day in the life of Clair based on Clair and grandparent reports
Getting ready and going to school
Clair does not have trouble getting up in fact she is “at her best at 7 or 8 o’clock in the
morning”. She has a chair beside her bed and she gets herself out of bed without falling
over. “We’ve got it all down to minute by minute … military precision” said Grandma
(U.6contd-C¹&S-73-82). After picking up 5 other students, a school bus collects Clair at
about 8 o’clock. “When the bus arrives, I usually just get ready and go without running into
anyone” she said (U.6contd-C¹&S-69).
At school
Once at school, she goes straight to the Year 6 classroom and has a short talk with the
teacher (U.6contd- C¹&S-87). Clair was invited to talk about a normal day for her. “I
forget” she said. Grandma said “you describe it”. “Well um I don’t really get any pains in
the stomach or backache or headache. They used to hurt me” said Clair. Examination and
blood tests conducted had attributed symptoms to anxiety but Clair does not get these pains
now (U.4-C¹; S-30-5). Since attending the child mental health clinic, the psychiatrist has
been encouraging her to play in the playground with the other students instead of spending
time with the teacher aides. Grandma thought this was still happening but Clair maintained
she now plays with friends (U.7-C¹; S-96).
As far as the teachers are concerned, the main worry is Clair’s seizure condition. To
aid peer understanding, the school nurse who visits weekly was asked to explain warning
signs to students and suggest they call for help if Clair has a petit mal. Grandma reported
teacher concern about deterioration in learning over the past 8 months which prompted them
to request permission for the Guidance Officer to assess her intelligence (U.7- C¹; S-100-4).
When in the mainstream class, Clair sits near the board at a desk to the side of the room
“in case they’ve got to take her to the SEC if she has a little seizure” (U.10- C¹; S-197-200).
147
An Occupational Therapist from Spina Bifida and Hydrocephalus Queensland recently
conducted a sensory profile assessment. It reported sensitivity to noise and recommended
one-on-one support and quietness in the classroom (U.10contd-C¹; S-207). Clair can
navigate her way around the school independently. She can manage level but not raised
gutters and she is apprehensive about falling forward on grassy slopes (U.22contd- C¹; S-
492-503). The grandmother thought school staff was “really in tune” with Clair’s needs and
the mainstream class teacher has been “excellent so Clair’s been lucky” (U.24-C¹; S-565-
571). There were no reports of jokes about the wheelchair. “The children are used to it
because there’s several kids in wheelchairs there” said Grandma (U.25-C¹; S-575).
Coming home and homework
The school bus brings Clair home at 3.15 p.m. and a carer comes to help with
homework (U.2-C¹; S-8). The carer is also a support person for the grandmother who said “I
can do everything else it’s just the homework … being so far removed from it all that was
my concern” (U.2-C¹; S-14-6). Clair’s homework folder is compiled and marked by the
Year 6 teacher which Grandma thought was preferable to Year 5 when students swapped
books to mark homework “and some kids would say ‘try harder’” (U.11-C¹; S-218-223).
Homework sheets consist of questions which Clair reads interprets and then inserts the
answers (U.11contd-C¹; S-261). Long-term memory is excellent but short-term memory is
weak. If asked what she did at school Clair will say “I can’t remember”. Grandma
wondered if this was an excuse but Clair said “hey, like I do say but I can’t remember what I
did”.
Loneliness, friendships and anxiety
Clair spoke about her friendship with another girl. “They have their little spats” said
Grandma though not as often as last year and they seem to resolve their problems. Clair
goes to the SEC at morning tea time. At big lunchtime, she may invite a friend to “play
ballgames and puzzles and stuff”. Her friend tells her who to invite and Clair usually agrees
(U.16-C¹; S-338-49). When asked if she thought classmates understood her at this school,
Clair said “they don’t think I’m mean to them”. Grandma felt they were more understanding
this year because they may be more mature but last year there was lots of squabbles and
Clair would come home and talk about meanness from children. “But there’s never any
invitations or vice versa” said Grandma. Even though the class teacher says the children are
“really very good”, Grandma said “it’s more like a caring type of thing not on a friend level”
(U.20-C¹; S-453-70). Clair “would love to have a friend and that’s what this friendship
group is all about. All the children there have a problem but all of them are able-bodied”

148
said Grandma (U.21-C¹; S-477). Clair tries to ask people home and Grandma wondered if
it’s “because it’s in a different suburb and we’re so much older” that invites are not accepted
(U.21-C¹; S-477).
Over the last Christmas holidays, Clair “was having about 2 hours of sleep a night and
next day no sleep”. The grandmother said she had to sleep beside her on the floor until her
doctor said “no” and also advised no music and no lights when Clair was going to sleep.
When going to sleep now, Grandma has trained Clair to think about something good, to
make up stories and pictures in her mind and to “think about something nice that you did that
day” (U.23contd-C¹; S-539). Clair said nothing worries her about school now but Grandma
said she keeps things to herself which probably results in insomnia. To help relax Clair, the
grandmother purchased Geranium, Nereli and Ylang Ylang which she burns in an oil burner
in Clair’s bedroom for an hour before bedtime. She also massages Clair with cream to help
relax her (U.23-C¹; S-506-10).
Tasks Clair enjoys
Each Thursday, the SEC does cooking and Clair enjoys chopping carrot which she does
very neatly. She likes grating carrot and cheese and she can distinguish the sharp side from
the blunt side of the knife (U.14-C¹; S-307-26). Playing Solitaire on the computer, drawing
and writing notes to people are tasks she enjoys. “When you’re feeling good, you do
beautiful writing” but if she is tired or had a seizure, “then you can tell the difference” (U.8-
C¹; S-138-46). At about 10 years of age, the grandparents bought some legos for Clair “but
she seems to like writing and drawing more than building” (U.8- C¹; S-151-7). She can use
scissors well and likes cutting, “I’m good with the shaking stuff to make something”, and she
can use a peeler to peel an apple but she is unable to cut an apple in half (U.17- C¹; S-359-
75).
Strengths reported by the grandparent
Clair attends to her own personal care and self-catheterises four times each day.
Grandma said this is something she has to take responsibility for if she is somewhere else
and Clair has learnt to say “Oh! It’s time for me to go to the toilet. Can I use your
bathroom?” (U.28-C¹; S-605-15). Clair’s rote memory skills are also a strength. She gets all
spelling correct or only one wrong and in the maths test “one wrong and nine right but I
always say this … ‘it doesn’t matter just try your best’” (U.12-C¹; S-239).

149
Tasks that Clair finds difficult
Cleaning up the school desk “is annoying … I find it irritating. It gets messy again
about every 5 minutes” said Clair (U.9-C¹; S-171-7). To help organisational skills, a
checklist on the desktop reminds her when to get the ruler or pencils out. But Clair said this
reminder is not there now and “I keep finding my things disappear everywhere”. She often
forgets to bring her jumper home “I can’t remember it, everything” she said (U.9contd-C¹; S-
184-89).
Have you heard of a Nonverbal Learning Disability?
Grandma was not explicitly asked if she had heard of an NLD but she did not express
awareness during brief description of the syndrome’s characteristics (U.31-C¹-S-634).
Clair at school based on teacher and teacher aide reports
At school
Clair is dropped off at school at about 8.50 a.m. and she “often pops into the classroom
to have a chat before school starts” (U.1-PCT-2; U.1-TA-2). The teacher looks forward to
these times because it allows some one-on-one which is not always possible in a class
situation (U.1-PCT-2). She sits with a group of able-bodied children and has her own set of
work which she normally takes out and gets on with. Two teachers agreed that
organisational skills have “changed significantly” but the SEC teacher said she still needs
monitoring because “all the strategies for getting her to restate what you’ve asked her to do
are unsuccessful because she’s not retaining more than a very short instruction” (U.1-PCT-2;
U.3-SNT-30; U.12-SNT-75). The class teacher tries to involve Clair with general classroom
discussions “but she’s not into it. She’s more into working on her own” (U.1-PCT-2) and
the SEC teacher said she worked at a “much lower level than the rest of the class”
(U.7contd-SNT-50).
The importance of assessing Clair’s level of intellectual and functional performance
was stressed by a SEC teacher. Difficulties with language-based functioning which affects
every curriculum area is causing major problems in her functioning within a standard
curriculum and assessment before high school is important “it’s just that she wasn’t due for
review and the downturn has occurred quite recently” (U.2contd-SNT-10contd). The area of
extreme difficulty is with “language functioning and in processing and in retention of even
very short sentences” (U.2contd-SNT-16). Clair is unable to manage questioning aimed at

150
much younger students who have a range of difficulties and “of course she develops the
social nuances of ‘silly me’ and the roll of the eyes and the tap of the thigh” and just lately
she has been saying ‘I don’t know what’s the matter with my brain’” (U.2contd-SNT-16).
To raise awareness of what was happening with Clair’s seizures so students could show
some empathy, the school gained Grandma’s permission to enlist the school nurse to talk to
students about her epilepsy, spina bifida and hydrocephalus and “how Clair needs to be
catheterised when she goes to the toilet” (U.2-PCT-12; U.4-PCT-20). The epilepsy was the
predominant focus because “that’s the one they see more. They actually don’t see Clair
particularly as a disabled kid; she’s just a kid that happens to be in a wheelchair. The thing
that makes the difference is the epilepsy not the spina bifida. I know that sounds weird but
that’s the reality and it’s the one that makes her very different to them and that they are more
cautious of” said teachers (U.4contd-SNT-34; U.2-PCT-12). “The kids are very accepting
and sometimes I’m not aware that she is having a seizure until one the kids says ‘Clair needs
you’. That’s all they say and I’ll just go over to stand beside her and I can see that all is not
well. So I think that as a class we’ve handled that quite well. Nobody gets uptight about it
and I think it’s possibly because they’re not terribly defined seizures” (U.2contd-PCT-14;
U.3contd-SNT-30contd). When asked about any cruel jokes, sarcasm or jokes about the
wheelchair, the teacher said “no, I’ve never heard any kids at this school say anything
derogatory to those kids or about those kids and she’s never complained to me about
anything either so that’s really good” (U.3-PCT-18). If an incredibly negative response
towards Clair was sustained, the school would ensure she was not placed in the same class as
that child to prevent “a domino effect on the remainder of the class”. So within Clair’s class,
the school tries to include “some people that we know are good peer tutors” not just for Clair
but for others (U.4contd-SNT-34).
In the SEC, she predominantly works independently with a small group approach and a
differentiated mode of delivery. “We demand a very high standard of Clair. She’s capable
of working well and producing some nice quality work but we also allow her to work in lots
of different modes such as pencil and paper tasks on the desk and keyboard tasks on the
Alpha Smart keyboard (U.7contd-SNT-50contd). A lot of her assignments are done on
computer and “we’ve got programmes that actually will speak to her and we can write and
transpose worksheets and activities” (U.7contd-SNT-50contd).
Loneliness, friendships and humour
One aim at school is to encourage Clair to socialise more and develop some of her
leisure time activities (U.1-SNT-4; U.1contd-PCT-2contd). “She will at the moment just sit

151
and literally withdraw” and she can be quite rude if people try to push her to play with others
(U.1-TA-2contd; U.12-SNT-75). She does not interact well with her peers and an aide
wondered whether this was due to the “horrendous” 11-12 year age-group or “the social
impairment that she has and not being able to interact well with others” (U.1-TA-2contd).
She relates well to the aides and “relies on us too much for her socialising. She will hang
round the aides rather than her peers” (U.3-TA-6). Sometimes she is a little rude which was
considered due to her inability to socialise on a competent level (U.3-TA-6). Somebody
commented “it’s almost like cocktail talk, this parrot fashion” which after a while “it’s
repetitive ‘Oh! You’re funny, oh! You’re funny, oh! You’re silly, you’re crazy’ but the
next day she’ll say exactly the same thing and it’s almost as if ‘I know these phrases and I
know that these work for me to be able to talk to people so I’ll just say these things’, the
same thing over and over again”. If asked what she did on the weekend “you’ve really got to
push and prompt to get answers from her because she doesn’t live with her mother … It’s a
big thing for her ‘Mum’s coming up for the weekend or I’m going to Mum’s for the
weekend’”. Another “real parrot thing for her is ‘what did you have for dinner last night’,
and she’ll ask everybody ‘what did you have for dinner last night’”. She is able to recall
what she had “so dinner must be a very important thing” but the funny little phrases and
questions that she asks cause one to think “Oo! She’s a chirpy little ...” but after a month
one thinks “Oh my gosh! She’s asked me this a hundred times” (U.3contd-TA-6contd).
Clair has “a good rapport with the kids in the classroom, they really love her and she
gets on well” said the teacher. She had never seen Clair at odds with any classmate and
“they’re very caring” and accepting of physically impaired children (U.1contd-PCT-2contd).
When a Special Needs teacher brought Clair and “other wheelie kids” to ask questions about
what kids eat for breakfast, Clair asked some questions “which was a huge thing for her to
do”. When she left, some of the kids said “wasn’t it good that Clair did that” because she is
normally uncomfortable doing things by herself. She is very quiet, does not do a lot of
interacting and “she’s not a centre of the stage person at all” said the class teacher (U.8contd-
PCT-59).
Social interaction and friendships are an issue and the teacher wondered if this was due
to Clair’s isolation from classmates during lunch times when she is at the SEC where she can
invite a friend but usually does not. After getting her tablet and sometimes tuckshop, she is
“quite happy to be up here and sit” (U.1contd-TA-2contd). “But the social side of having to
ask, ‘how do I ask’ and rejection and all of that comes into the whole thing”. Sometimes she
says inappropriate things … “she doesn’t understand that the things that she says might not
be appropriate for other people so I would think there is a difficulty with the social skills”

152
(U.16-PCT-128; U.1-TA-2contd). “She just doesn’t get it how people are with each other,
what’s rude and what’s not rude” (U.13-TA-36).
Understanding jokes is an ongoing problem “because we always muck around with the
children”. When an aide pretended to “pinch” some of her morning tea, Clair got very angry
“give me it, give me it” and she went away and just glared and she said “I’m not talking to
you anymore, just stay away from me”. The aide said “it was just a joke and you’ve just got
to realise that things like that are just a joke sometimes”. Clair sat there with a frown on her
face and would not talk to anybody and it took the entire morning break for her to come out
of this little tantrum then she said “I’m sorry I wasn’t very nice at morning tea” (U.13-TA-
36-8). The aide explained that whoever was joking would not eat her morning tea “but she
then didn’t know how to get herself out of it”. Now the aide says “you know I’m only
joking” and Clair has got into the habit of saying “I know you’re only joking” but she takes
everything literally and believes they are going to take her lunch (U.13contd-TA-38). She
can be “rude to her peers in the same way that they might be having a joke with her and she
threw a pencil at one of her friends the other day and it hit them on the side of the head.
They were upset and said ‘Oh! I was only joking’”. Her “social skills are so poor that she
doesn’t understand when anybody else is joking and then she thinks that when she does
something that’s quite nasty, it is a joke” (U.13contd-TA-38contd).
Clair is “great in a one-on-one situation with an adult” and will want all of that adult’s
attention but if offered a bunch of cards to play a game, she would be excited about playing
with an adult but would “either refuse or withdraw very swiftly” from playing in a one-to-
one setting with a peer which is a big concern of staff (U.1contd-SNT-4). Clair was “a bit
anxious” at the beginning of the year possibly because of a new class composition but now
“she’s the most relaxed I’ve ever seen her” said the class teacher (U.17-PCT-134).
Strengths reported by teachers
“A delightful little girl … yeah she’s lovely” (U.10contd-PCT-92). She “desperately
wants to please, she desperately wants to belong, she desperately wants to be successful so
she will try her hardest” (U.12-SNT-75). She “loves all the functional things that we do”
such as cooking, art work and anything where she has close one-to-one interaction with
others and is not required to compute and respond in any “higher order manner whatsoever
so she likes simple familiar games” (U.5-SNT-40). Staff noticed that Clair extremely enjoys
working with younger children and given a selection of books would “go for things that
would be age-inappropriate”. Her performance of reading “is actually way beyond that
standard but her comprehension of the text isn’t there”. She obviously uses the visuals and

153
reports from home say she chooses television programmes more suited to younger children
(U.5-SNT-40).
Clair is physically very independent in her wheelchair and is quite strong with her arms
(U.4-TA-8). She is “quite able to get herself from A to B” but if going to the oval or on
uneven terrain, she will ask for help (U.6-PCT-32). When asked if peers are allowed to
assist, the teacher said she had never really asked if “that’s not a good thing to be doing. I’ve
just sort of taken it as a natural course of events that it’s okay to do it but it could be possible
that it’s not”. By asking for help “I do think sometimes Clair could use it to her advantage”
when she may be quite able to do it herself (U.6-PCT-32-44) but the teacher believed this
was the “friendliest thing to do because you’d like to encourage the kids to do basic things”
(U.6contd-PCT-51).
Clair likes to be able to do things for herself. She takes medication at school daily to
control bladder infections and “goes up to the office on her own and gets that”. Office staff
administer the medication so she is independent with catheterisation and getting her tablet
but needs reminding “that she’s got 5 minutes” because she is slow and may get involved in
looking at wall pictures and forget to come back (U.1contd-TA-2contd).
Special teaching arrangements and sport
The school week comprises two different days for Clair. She spends Monday and
Friday in her Year 6 class where she is supported intermittently by an aide and on Friday
afternoon she takes part in an alternate Health and Physical Education (HPE) activity while
other students play off-campus sport. Tuesday, Wednesday and Thursday she starts the day
in her Year 6 classroom and from 9.30 a.m.-1 p.m. she works on core activities in the SEC.
Because it is a mainstream school not a Special School, the SEC takes a differentiated
approach to the curriculum. “We look at where the children are at, what they need to learn
and how we can all augment that within the environment”. Working within a small group
allows SEC staff “to tweak the pupil-teacher ratio very much into favour of students who
require a lot more visual and verbal prompting and so forth” said the teacher (U.1contd-
SNT-4). This approach will “augment the willingness of the children to actually take part in
activities”. It mimics what would be provided in the mainstream class but teaching is
tailored to suit student needs at the time. Clair is “currently working at about the top end of
Grade 3 early Grade 4 level and she’s in a Grade 6 class but is actually at a Grade 7 age” so
if working on core subjects in the mainstream class, she would be substantially below her
peers. Clair’s time in the SEC can also be utilised to focus on outside therapy without
interrupting classroom time thereby reducing the number of in-out processes (U.1contd-

154
SNT-4). On SEC days, she returns to her Year 6 at 1.30 p.m. with the understanding that she
is firmly a member of her mainstream class but supplements her core curriculum subjects
whilst in the SEC (U.1contd-SNT-4). Memory and recall were “fairly poor” so the SEC
modifies what she is doing in class with plenty of enforcement and repetition (U.1-TA-2).
A functional session on Healthy Eating has been introduced to involve students with
cooking meals. The idea is “to develop a skill to allow them to function or to at least
appreciate the food that’s provided for them” and as a socialisation issue to encourage them
to share with somebody outside the SEC. Clair also takes part in a specific SEC-based
programme designed to help the student’s gross and fine motor skills (U.1-SNT-4). Visual
and spatial perceptions were not too bad but it “depends on how she is on the day as well.
She can have a really good day and be really sparky and other times you really would think
she’s half asleep. You get some days when she’s really really got her finger on the pulse and
other days well there’s not much pulse going on there” said the aide (U.12-TA-34).
Clair went on the Year 6 camp “which was really great” and some girls in the class
“fight over accompanying her to wherever she needs to go” (U.5-PCT-26). A focus on body
systems and nutrition in Term 2 meant the class did 15 minutes daily fitness and when she is
with the class, they borrow gear like skittles and quoits from the SEC. Classmates are
delighted to be in Clair’s group “to experience the sort of things that she uses” (U.5-PCT-
26).
Getting class work finished
The class teacher does not “actually apply a lot of pressure” but says “this is what we
will do this week”. She does not say “well if you’re not finished at the end of the week you
have to stay behind to finish it” but instead, she lets Clair work at her own pace “and she’s
quite good. She really sticks to it, she doesn’t waste time” though sometimes she has “a
little bit of a daydream but a lot of other kids waste more time than Clair does” (U.11-PCT-
102). She is incredibly tired at times which may be due to a task that needs focused attention
or a degree of excitement (U.10contd-PCT-92).
Homework and assignments
Negotiation between class teacher and family over the last couple of years has reduced
the amount of homework because Clair is very tired by the end of the day (U.7contd-SNT-
50contd; U.10-PCT-79). After speaking with her carer, the teacher compiled a booklet of

155
reading and comprehension activities which Clair hands to the teacher when finished “and
that seems to be working well” (U.10contd-PCT-86).
Copying from blackboard and handwriting
“Her handwriting is beautiful. She can be a bit pedantic about it being perfect and can
be quite slow. We’ve had to work really hard and it’s no longer in the IEP as a goal” said
the teacher (U.9-SNT-56) but the “content probably leaves a lot to be desired because she’s
so repetitive”. “What you’ll get is almost a loop where she will actually continue to repeat
the same thing” (U.9-SNT-58; U.9-TA-14). Clair wrote in a recent Mother’s Day card “I
like my Mum because she is good to me. She takes me shopping. She buys me things and I
love her and she is so good to me and she takes me shopping and I love her so much …” and
the aide said a lot of her story-telling is also very repetitive (U.9-TA-14).
Comprehending and following instructions
Comprehension-based activities, whether reading or any form of comprehension where
she has to read, remember, and answer questions, are difficult. Formal mathematics like
addition and subtraction are not a problem but problem solving activities are hard (U.6-SNT-
44; U.8-PCT-53). The class teacher selects “low level but high interest” activities for Clair
(U.8-PCT-53). Following directions is difficult so when she gets her tablet from the office,
the aide says “you have 5 minutes to get back here”, shows her 5 fingers then “off she goes
… wheel wheel wheel really quickly … and she usually comes back in 5 minutes”. She is
“not very good at time but I think she knows 5 minutes is a short period of time, that’s all she
would look at it as” (U.19-contd-TA-60-2contd; U.18-TA-58).
Planning, organisation and time management
“Tasks to do with organising, decision-making, probably problem solving, anything
that’s a little bit too abstract is very difficult for her to grasp” but straight-forward tasks ‘put
the answer in here’ she’s not too bad with” said the aide (U.130contd-TA-40). “Whilst I
wouldn’t claim for one minute for her to be totally organised, it is a lot better but it’s taken a
lot of direct teaching, a lot of additional cues both visual and verbal” (U.10-SNT-65; U.12-
PCT-108). “I’m not standing beside her at the beginning of the day saying ‘take this out, do
that, do that, do that’ … she knows”. In a folder labelled “Clair’s work”, she bundles
completed work and keeps work in progress separate in the same folder (U.12-PCT-108).
During one SEC activity about time, children were asked how long it would take to go to the
office and to the pool and they were all way out … just thought that it would take ½ an hour

156
to get there”. They did minutes and seconds and Clair was a little better than some but
“didn’t really have that concept” (U.19-TA-60).
Handling novel tasks or situations and anxiety
Spontaneous events and changes to routines are difficult for Clair. “We’re going to the
library now ... ‘Oh hec!’ She could quite easily go to the library without a book if it wasn’t
at the time that we always go” (U.11-SNT-65). As long as she has a base of familiarity
whether that be a person or an environment “she is less concerned” but a situation where
both the environment and the people interacting with her are new is a bigger concern “but
it’s not something that we see very regularly because she is very comfortable with us and
she’ll always have us there and seek us out” (U.11contd-SNT-73). Staff has worked very
hard with Clair’s swimming lessons. “The first couple of years literally she would grip hold
of my arms so hard that she would bruise them and she would be screaming at me the entire
time and being at times very rude but it was that she didn’t want to be in there” (U.11contd-
SNT-73contd). With very careful teaching and keeping the same 2 people working with her
in the pool, she has become much more confident. For the first few weeks of swimming in
terms 1 and 4, the same 2 people are kept working with Clair but after that she is “much
more relaxed and will allow only one of us to be there and for me to take a couple of steps
back” so she can go in a supported float which is dramatic progress but it’s taken a
considerable period” (U.11contd-SNT-73contd). She had to know who was swimming with
her “you could see she was anxious …” and if unable to give her an answer, she would say
“‘but you must know who, can you find out who’… but she is an anxious little thing’” said
the aide (U.5-TA-8contd). Once in the pool, Clair assesses her behaviour as being rude and
having caused pain. She will apologise but the apology gets overly profusive “‘I’m really
really really sorry … please don’t be angry I’m really really … ’” until asked to “stop … it
hurt but I’m over it” (U.11contd-SNT-73contd).
Preparing a list of things that she needs for the day, a pencil, rubber, ruler and maybe a
structure of the day is helpful and reassuring because it allows Clair to come into class and
say “Oh! It’s Monday and we’re going to music and we’re going to library and oh I know
that I’m going to do all those things today” whereas if she was a little bit concerned about
anything as with swimming, “she just wouldn’t let up until she found out who it was. So it
became a stressful thing for her” (U.11-TA-22). Who is taking her to the bus is a big
problem “‘are you with me today’” so she likes to know who’s with her” said the aide
(U.11contd-TA-28; U.5-TA-8contd).

157
Clair finds it difficult to answer a question. To help reading comprehension, she is
asked to read maybe 3 sentences. “On Tuesday morning, so and so were running late for
school”. When asked “when did it happen” Clair was unable to say ‘when’ so the sentences
are repeated. “Tell me what I just said” and she could repeat if back. It was almost like the
processing of it and the anxiety of ‘I’ve been asked a question, I just don’t know that answer,
I don’t know that answer’ and she’ll sit there and say ‘I’m thinking, I’m thinking’ and you
can see that it’s all too overwhelming for her”. After repeating back the phrase, the teacher
stopped her and said ‘when … on Tuesday morning … so that is the answer to the question’
and she sort of went ‘O!’ and it’s almost as if ‘well I didn’t even realise that’ so her
processing of quite a simple question and recall and being able to relay what is the answer is
really difficult for her” (U.1contd-TA-2contd iv).
Rote memory skill
“Oh! She can spell” though the class teacher was unsure of the extent of Clair’s rote
memory skills (U.15-PCT-124) but she reported that Clair had learned tables and spelling at
the previous school by saying them out loud every day (U.20-TA-66).
Maths
Clair is given lots of copied maths tasks that are fun but low level. “She’s nowhere
near her same-age peers academically, she’s not” (U.7-PCT-53). She handles mechanical
type maths “quite well” but problem solving maths that require comprehension are “not as
easy” (U.7-PCT-53).
Memory and concentration
A teacher and aide perceived Clair to have a problem with memory and recall “though
she can remember some of the things she’s done work wise”. She has an ability to
concentrate and the class teacher did not report issues with concentration span (U.1contd-
TA-2contd; U.14-PCT-120). Reading is good and a programme has been introduced “to get
her to do more recall”. Clair reads a book of about Year 2 level which has limited text and a
simple story and after every page; she is asked a question “now what was the boy’s name”.
After reading the second page, Clair would be asked pages 1 and 2 questions “and we’d get
to the end of the book. Now by the end of the book, oh yes she could remember all those
things because we’d said them after every page”. Clair remembered most of the book the
next day but when asked a month later “couldn’t even remember the book … didn’t
remember reading that one at all” said the aide (U.10contd-TA-18).
158
Verbal skills and orals
“She’s got a great speaking voice, there’s no doubt about that”. Clair is a bit shy and
“she doesn’t have a buddy up here” (U.9-PCT-65). Last year she had a little friend who has
since left the school “so maybe that has implications for her not coming out of herself as
much as we’d like her to” said a teacher (U.9contd-PCT-73). She did one oral in Year 5 and
was very nervous but an aide sat beside her and the teacher prompted and encouraged her but
“she’s not very confident with that type of thing” (U.15-TA-44). Clair does not like to gets
things wrong but is encouraged to “have a go … it doesn’t matter if it’s wrong, have a go”.
She repeats a lot of “what you’ve said in the past” so if she does not know the answer to a
question now, she will say ‘it doesn’t matter if I got that wrong does it, it doesn’t matter
because I’m trying, at least I’m trying aren’t I’” (U.15-TA-44).
Everyday taken for granted skills
Chopping tasks in the cooking class are not difficult because Clair has good dexterity
and can chop chunky pieces of carrot into centimetre square cubes (U.11contd-SNT-73).
She can do her hair, buttons and hooks and she self-catheterises. She manages scissors well
and can peel an apple with a peeler but she cannot cut the apple in half. Organisational skills
are still difficult but a checklist on the desk at school and a routine have helped them to
improve.
Group work with peers
A lot of group work done in the mainstream class “is not geared to where she’s at and a
lot of it takes place when she’s not there” said her teacher (U.18-PCT-138). Clair was
thought to feel “a little bit embarrassed about being part of a group and maybe not being able
to keep up as well as the other kids” and her understanding of group interaction is “not as
well developed as her same-age peers”. The teacher wondered if this was “because her
opportunities for interacting in that way are so limited” (U.18-PCT-140). In the SEC, a
group of 4 or 5 starts off with “a generalised teaching point then we take it to a higher level
for Clair and another child and a lower level for students working at a lower level”. Clair
then works in partnership with another Year 6 student in the sense that they are on similar
tasks or on the same task. But at that point, the instruction for Clair and partner separates
because Clair has a higher level of experience but lower ability to process and the other
student has low level experience but higher ability to process information. So the mode of
delivery has to alter (U.7-SNT-48-9). Clair is capable of working and propelling herself
independently through tasks and appreciates interaction but “we’re all working around the
same point” which allows cross-discussion to continue to occur (U.7contd-SNT-50). A large

159
section of Clair’s IEP focuses on social pragmatics which can be integrated in the SEC
“because we’ve got 4 or 5 students compared to 30 in the mainstream so it allows us to be
more interactive with the students” (U.7contd-SNT-50).
Critical life skills as represented in school
There is a basic split between critical issues as to whether they are academic-based
issues as in higher order thinking and complex processing which are not occurring, and
social pragmatics and health care issues. Her seizures come and go and over the last 2 years,
they have increased dramatically in number, complexity and duration (U.4-SNT-32).
“Grandma actually had to come and explain it to us what a seizure or an event would be
because they were so fleeting. It was very difficult to spot one” … “sometimes they go on
for a long time but not incredibly severe” (U.2-PCT-12). They are “something we’re always
monitoring. We always keep a record of how long they lasted” and what actually happened
during the seizure (U.8-TA-10). There can be 2 a day, 3 a day, maybe one a week or one a
fortnight. They do interfere with her schoolwork because after a seizure “she’ll be extremely
tired, really worn out”. Often she is taken to the SEC to lie down on the bed but “now her
seizures seem to have taken on a phase 2 where she’s becoming agitated and a little
aggressive” (U.7-SNT-8). She will have uncontrollable movements and salivating but “then
she may go into trying to wheel herself away if she’s sitting in her wheelchair and you’ll go
to stop her and she’ll grab your hand and say ‘stop it, let me go, let me go’ but she’s actually
still in the seizure state” and she gets quite aggressive. Staff now put Clair on the floor
instead of the bed because one time she tried to get back in the wheelchair by herself (U.7-
TA-8).
“Being careful of her physically because she has a rod in her back” is a safety issue
when Clair is being lifted or transferring herself from her chair to the toilet. An aide must
always be present. She can be a “little bit lax with herself” and needs to be reminded to be
careful of herself because she is not able to feel her legs. She could easily bang or cut
herself and she would not know “so we’re always aware that she’s got to be careful and
watch for those transfers over because it’s a bit like lug, lug, lug with her legs” (U.8-TA-10).
Because of the shunt, Clair and staff are mindful that any hit or bang to the head, major
headaches, dizziness or fainting could be something to do with the shunt which is always an
issue” (U.8-TA-10). She needs encouragement to drink more water though she is good at
eating but she will forget to ask someone to get her lunchbox out. She may just sit there for
10 minutes doing nothing; just sit happily as she does at the office waiting for somebody to
get her tablet (U.8contd-TA-10contd).

160
Teacher and aide perceptions of Clair as a person with a disability
Advice for other teachers
“One of the very difficult things that you tend to get with students with spina bifida and
hydrocephalus is in those early years because they can function very well on a concrete
level, the disparity between themselves and their peers is actually much lower” and the gaps
widen in middle and upper primary school with demands of more complex higher order
processing (U.2-SNT-6). Any teacher working with a student with hydrocephalus should be
told “they’re not disorganised to annoy you and they cannot take responsibility for doing
things” (S.13-SNT-77). In a lower grade, there was an issue with Clair taking home the
school newsletter because Grandma did not receive one for several weeks. As her transport
comes 10 minutes before the end of a school day before the newsletter is handed out, the
teacher said “well it’s up to her to remember to ask me”. The SEC teacher replied “well
that’s not going to happen, be realistic about … it’s almost the same as what you do as a
mother … you pick your battles ... you work on the organisation but there are certain things
that it really is not worth wasting Clair’s energy levels on attempting to do ... ”
The school worked on organisational goals for 2 years “but I’ve seen teachers get
incredibly annoyed with her and other students for being disorganised and unprepared and
it’s not her fault”. The teacher wished she had a dollar for every time “I’d said to somebody
‘it’s actually a part of the condition, she’s not doing it to upset you, please just build the
extra prompt into your day” (U.13-SNT-77). “I’d say that’s my biggest” piece of advice and
“my next one would be is that you need to check on these kids more often. You can’t
assume that because they’re not disrupting your lesson that they are performing at their
optimum level because the chances are that they’re not. I’d say that those are the two
biggest things” (U.13-SNT-79).
“Keep asking till you find out what you need to know really until you feel comfortable
about it” said the class teacher (U.19contd-PCT-154). There is nothing worse than having a
child in your class who doesn’t feel comfortable with you and it can be a nightmare I think
for both parties” (U.19contd-PCT-160). “I’ve read everything that I can get my hands on”
and colleagues have provided further reading to increase understanding about the medical
condition. The teacher knew what spina bifida was but did not know about the
hydrocephalus component. Clair has cerebral palsy also and the teacher said it had “been an
eye-opener” to learn about Clair’s need for catheterisation. “You can’t really teach them

161
unless you know what’s going on there in the background’ she said (U.19-PCT-144).
Teachers should also talk with the aides and the Special Needs Teacher who always comes if
the class teacher has a concern (U.19contd-PCT-146).
Patience and a sense of humour are needed because sometimes “they can be a bit
wearing” and compassion helps one to realise their struggle because their little minds do
think in a different way to ours. Be flexible but modify things to the way it’s going to work
for them and don’t try to fit them in with everyone else because they’re not going to, no”
advised the aide (U.21-TA-72).
Teacher understanding of learning difficulties
Clair’s desire to please makes her “a very easy person to teach in that way, not easy
because she’s incredibly complex but easy in the fact that she will always try her best and
it’s a case of you sitting there and puzzling through how best to go about what she needs to
know”. This teacher said “I loved working with her, she’s complex but she’s interesting”
(U.15-SNT123).
Have you heard of a Nonverbal Learning Disability?
The researcher spoke about the NLD syndrome and explained the negative affects that
hydrocephalus may have on daily functioning. Two teachers had heard of an NLD, one
“only recently” which prompted an internet search. “I haven’t spent a lot of time looking at
that but I understand there’ll be huge differences in performance in different areas and that
you can actually have an extremely high performance in some of the areas and an incredibly
low performance in other areas which obviously dramatically affects what’s going on in the
classroom … well not just in the classroom, in life” (U.14-SNT-83). After explaining the
effect of damaged myelin on ability to make decisions and problem solve, this teacher said
“that’s classic for Clair” (U.14contd-SNT-91). She was interested to know more NLD (diary
notes). The other teacher said “what surprised me most of all was the social skill inability. I
just thought as if there isn’t enough physically going on for these children for them not to be
able to cope with social interactions and have real meaningful friendships is not fair, it’s
awful” (U.20-PCT-166). The aide had not heard of an NLD but said “Oh okay! That’s
interesting isn’t it … well that seems to be Clair down to a tee but yeah she’s a good little
talker” (U.22-TA-76, 94-6).

162
Summary of 2005 Psychological and Speech Assessments
The following extract has been taken directly from the assessment reports.
2005 (aged 12 yrs 4 mths) Full Scale IQ = 57
Verbal IQ = 60
Performance IQ = 62
VIQ-PIQ difference = 2
Language assessment age equivalent = 5 yrs 0 months
Problem Solving age equivalent = 5 yrs 6 months
On a test of general intellectual functioning, Clair performed within the mild range of
intellectual impairment for a girl her age. Both verbal and non-verbal intellectual
functioning was consistent with her general intellectual functioning. Within this, Clair
demonstrated a number of relative strengths and weaknesses. She performed well on a task
assessing immediate auditory memory. She had difficulty on a task of word meanings and
ability to express them verbally, comprehension of social situations and she also had
difficulty with a task assessing 2-dimensional visuomotor skills.
Clair has severe difficulties across all areas of learning. These include:
• Any task which requires attention and concentration;
• Any task which requires organisation and planning;
• Learning new material and memory of it;
• Word retrieval and fluency (verbal expression);
• Processing information quickly;
• Most tasks which involve speed of hand-eye co-ordination (e.g. undertaking work
from the blackboard);
• All academic subjects.
Interpretative discussion
Interviews were held in the SEU which was sub-divided into therapy and teaching
areas. The environment was noisy and there were seven interruptions during interviews. I
was impressed with the Special Needs Teacher’s understanding of Clair’s learning
difficulties and her willingness to share knowledge with teachers, advocate for Clair and
promote flexibility with classroom teaching strategies and expectations of Clair. She pointed

163
out that teachers are already very busy and modifying lessons for even one student with
special needs adds to the teacher’s workload and sometimes burn-out (diary notes). “This
department could not run without the wonderful teacher aides that we have got” and
Education Queensland should recognise Special Teacher Aides as paraprofessionals over and
above the standard recognition of what a teacher aide is. “These people are not mixing paint.
These people are not totally at the direction of somebody else. They are having to think on
their feet” (U.16contd-SNT-131-3).
Grandma and Clair’s interviews were held at the family home. Clair presented very
well and spoke clearly and expressively. Interview questions did not bring lengthy responses
from Clair. Grandma spoke of concern about Clair’s future and offered advice on herbal
potions that may help other children suffering from insomnia.
This case study is about a girl who has good reading and spelling skills and “very
expressive” verbal fluency (U.2-C¹&S-8). Severely impaired adaptive behaviour skills such
as inability to use community facilities, personal care and hygiene, home living skills,
responsibility for herself, functional academic, language and listening skills have been
camouflaged by her NLD way of interacting with the world. This means her expressive
verbal and communication skills have caused misperception about her true level of ability.
Staff from the Special Education Class and the class teacher appeared astute and sensitive
towards Clair’s needs. Their readiness to share observations, knowledge and experience in
order to establish her developmental status before designing a program that addressed and
compensated areas of deficiency appeared to work well. Psychological testing for this study
revealed that Clair’s primary diagnosis was mild intellectual impairment. However, there
was an NLD profile of strengths and weaknesses which made the problem even more
functionally disabling whilst making it hard for people to appreciate how disabled she really
was. Clair was also diagnosed with an Executive Function Disorder. Prior to this study, it
appears that assessment of the extent of Clair’s intellectual and functional impediments at a
school level had not been conducted recently.
Somebody once said “it’s almost like cocktail talk, this parrot fashion”
which becomes repetitive “’Oh! You’re funny, oh! You’re funny, oh! You’re silly,
you’re crazy’ but the next day she’ll say exactly the same thing and it’s almost
as if ‘I know these phrases and I know that these work for me to be able to
talk to people so I’ll just say these things’, the same thing over and over again …
these funny little phrases and questions that she always asks when you meet

164
her you think ‘Oo! She’s a chirpy little’ and then after about a month you go ‘Oh
my gosh! She’s asked me this a hundred times’” (U.3contd-TA-6contd). These
speech characteristics were reported by an aide who had worked with Clair for three years.
They draw attention to the Cocktail Party Syndrome (CPS). “This syndrome represents the
ability to produce fluent expressive language that is tangential and irrelevant to the context
of the conversation” (Fletcher et al. 1995, p.220). About 30% of children with spina bifida
and hydrocephalus who use stereotypic phrases and vocabulary above the apparent mental
level of the child, well-articulated speech, verbal perseveration, irrelevant verbosity and
display over-familiarity of manner may have the CPS (Fletcher et al., 1995; Tew &
Laurence, 1979). Hurley et al. (1990) found 15 children with spina bifida hydrocephalus and
CPS had difficulties with visual-spatial-organisational perception, low IQ and poor academic
skills. Similarly, Clair has been diagnosed with an intellectual impairment, her performance
of tasks using visual-spatial-organisation and planning skills was in the severely impaired
range and four of the five CPS diagnostic criteria were reported here. Diagnosis of CPS was
not a focus here and speculation would be unethical.
The class teacher tries to involve Clair with general classroom discussions
“but she’s not into it. She’s more into working on her own” (U.1-PCT-2). She is
working at a “much lower level than the rest of the class” (U.7contd-SNT-50).
Both teachers displayed sensitivity to Clair’s limitations and her embarrassment about being
part of a group and being unable to keep up and understand group interaction. Clair
demonstrated significantly impaired language skills across both comprehension and
expression and her age equivalent was 5 years 0 months which is 7 years 4 months below her
chronological age. Her responses to scenarios presented in a problem solving test indicate
that “she doesn’t always interpret situations as the majority would”. Her age equivalent
problem solving ability was assessed at 5 years 6 months, 6 years 10 months below her
chronological age. “There is much in her world that she doesn’t comprehend fully” and
“there is much in communicating her ideas that she finds difficult” reported the Speech
Pathologist. This complex range of difficulties would make it reasonable to suggest that
group work in a mainstream class would present cognitive and social demands beyond
Clair’s level of competence.

165
“The first couple of years literally she would grip hold of my arm so hard
that she would bruise them and she would be screaming at me the entire time
and being at times very rude but it was that she didn’t want to be in there”
(U.11contd-SNT-73contd). With very careful teaching and keeping the same 2
people working with her in the pool, she has become much more confident. Two
teachers reported Clair’s difficulty with handling any new task, event or situation (U.11-
SNT-65; U.11-TA-22). Clair relies on routine, sameness and predictability and any new task
or situation will require her to integrate new information, stimulus and/or environment with
previous learning and experience. During assessment, Clair was unable to move freely from
one situation to another and she had difficulty regulating appropriate emotional responses.
Her difficulty understanding the subtle aspects of communication embedded in humour and
sarcasm would make anything different to the norm highly stressful and fearful for her. Staff
appeared insightful and perceptive about Clair’s fears which had an obvious influence on
their gentle supportive approach towards slowly building her confidence.
“It was just a joke and you’ve just got to realise that things like that are
just a joke sometimes”. Clair “really takes everything literally and she thinks
that they are going to take her lunch” (U.13contd-TA-36-8). She can be “rude to
her peers in the same way that they might be having a joke with her and she
threw a pencil at one of her friends the other day and it hit them on the side
of the head and they were upset and said ‘Oh! I was only joking’”. Her “social
skills are so poor that she doesn’t understand when anybody else is joking and
then she thinks that when she does something that’s quite nasty, it is a joke”
(U.13contd-TA-38contd). A failure to deal with humour is a failure to understand or
effectively handle incongruity says Rourke (2002) and such inability stops a person from
“judging and reacting to an event as humourous” (p.164). It is caused by a concept
formation deficit which means the person has difficulty organising a variety of information
to form thoughts or ideas. Rourke et al. (2002) believe inability to recognise and deal with
humour is “an earmark of persons with NLD” (p.164).
Failure to recognise and deal with humour is a social disability that may draw ridicule
from peers. Because children like Clair interpret speech literally, they only hear the words
spoken without inference or implied meanings. They may appear confused, roll their eyes
and say “I don’t get it” when everyone else is laughing. They feel embarrassed, silly and left

166
out until maybe a family member dilutes and rephrases the joke until the child grasps the
core wit. Understanding jokes is an ongoing problem for Clair and her inability to integrate
underlying meanings with nonverbal behaviours and environmental factors may cause an
inappropriate response that sounds obnoxious or rude which may expose her to further
rejection. “She just doesn’t get it you know how people are with each other, what’s rude and
what’s not rude” said the aide (U.13-TA-36). Her social withdrawal and preference to work
alone rather than with age-peers is understandable but lonely and may exacerbate Clair’s
anxiety and insomnia over time.
Conclusion
Usually, mornings are not difficult for Clair. She is a “good little talker”, reading
spelling and tables are good but reading comprehension is poor. Speech is very repetitive
“parrot fashion” with repeated phrases and questions. Social interaction and friendships are
an issue and she does not have a special friend but she attends a friendship group to help
social competence. Clair relates well to aides and enjoys working with younger children
more than with age-peers. Recognising and understanding humour, comprehending and
following instructions, handling any change or anything abstract are difficult. Handwriting
is beautiful if she feels good but slow. Organisation has improved and she can manage basic
maths but not problem solving maths. Short-term memory and ability to handle spontaneous
events or answer questions are difficult for Clair. She enjoys fine motor tasks and
homework is modified without any pressure being applied from school.
I believe the strategies developed to help Clair were based on judicious identification of
her level of language functioning, social ineptitude, educational loneliness and fear of the
unknown, and the driving force behind this insightful approach was the Special Needs
Teacher. As a result, all involved with Clair were on the same wave length though not
obviously every year since teachers who got incredibly annoyed with Clair’s disorganisation
were reported. The SNT wished she “had a dollar” for every time she had said to a teacher
“it’s actually a part of the condition, she’s not doing it to upset you, please just build the
extra prompt into your day” (U.13-SNT-77). What instilled such intuition into the Special
Needs Teacher and would her efforts to raise understanding be easier if teachers were
exposed to the NLD phenotype through pre or in-service training? Clair is 12 years of age
and has reached Year 6 before the full extent of her intellectual and functional impairments
was formally ascertained. This reinforces the need to inform teachers and school
psychologists that frequently “below average cognitive ability, and mild degrees of mental

167
retardation are not uncommon” with individuals with spina and hydrocephalus (Sandler,
1997, p.23).

168
MEL’S CASE STUDY
Context of Mel
Family life
Mel is a Year 10 student at a state high school in southern Queensland which has an
enrolment of about 639 students. She was born with thoracolumbar myelomeningocele
(T.10) which was closed at two weeks of age. Associated hydrocephalus required placement
of a right-sided ventriculoperitoneal (VP) shunt at 3 weeks of age. Her shunt has been
revised once and she has had a spinal fusion to correct kyphosis. A head scan in 1993
showed features of an Arnold Chiari malformation. Mel was born with congenital absence
of the corpus callosum which comprises the largest set of nerve fibres in the head’s midline
region (Rourke, 1989). She uses a wheelchair because she is paralysed below the waist. She
lives with her mother, father, younger brother and sister. The father and mother both work.
The school has a Special Education Unit (SEU) and Mel is ascertained at Level 6 Physical
Impairment (PI 6). Mel has not been diagnosed with a seizure condition.
During the initial telephone discussion, a parent revealed that Mel spoke well though
she “doesn’t always understand what she’s said” and she likes reading. She struggles with
maths and completing homework tasks and handwriting was “terrible”. Planning and
organisation were difficult and time management was “terrible”. She seemed to manage
Home Economics quite well and the school kitchen was fully wheelchair accessible with the
sink and stove at an appropriate height for Mel. She could manage some everyday tasks like
buttoning and dressing herself. Her concentration was fine when listening to music or
watching the Bold and the Beautiful … “anything else … forget it”. The mother thought
short-term memory was “pretty good” but long-term memory “depends”. She thought Mel’s
maintenance of friendships was “slack”.
Mel has a mixture of mainstream and SEU classes. She receives teacher aide support in
most classes and the SEU has physical education classes for children with disabilities. In the
physical tutorial, exercises such as balancing on the back two wheels of the wheelchair are
taught to assist independent skills in the community such as negotiating gutters. “It’s great”
said a parent and Mel enjoys these classes. The parent said that ever since Mel had her first
wheelchair, there had been an expectation of independence “because we felt that it was
important for her not to have that feeling of learned helplessness. We wanted her to be
independent as much as she possibly can and we’ve pushed that all the way” (U.17-P-164-

169
166). Mel is independent with her toileting. When asked if anybody was allowed to push
Mel’s chair, the parents have stipulated a rule that no matter whether it is a teacher, aide or
student “you must ask her because it’s her chair and it’s the only way she can get around and
you wouldn’t like it if someone pushed you” (U.17-P-176). If Mel is pushing, one must ask
if it’s okay and if she says “yeah, fine” you must say “okay hands up” because it is really
“quite wrong for the person in the chair to be pushing and someone else be pushing because
they have no control over the chair” (U.17-P-182). Mel agreed that a student must first “ask
my permission first so that I know whether I can trust them or not” (U.1-S-10). When asked
about problem areas, Mel said she finds “it difficult dealing with social things and her
brother, sister and parents” and she was seeing two counsellors at the time (diary notes
6.2.05).
Past school experiences
The mother and researcher agreed that wheelchair help that allowed Mel to join friends
in the playground did encourage friendships. In primary school, “that’s when a lot of issues
started”. Mel would go around the playground but would not go very far because it was “so
physically tiring for her so the children she befriended were quietly-spoken children who
weren’t physically active so she would tend to hang around the covered areas or go to
library” (U.17-P-192).
By Year 4, Mel was experiencing organisational problems with separate subject books.
The mother purchased a 5-subject book with dividers between sections and plastic pages for
handouts. The mother and Mel agreed that the 5-subject book had helped over the years. To
help her keep numbers aligned for high school maths, the mother ruled up quad lines or
pulled a quad book apart then glued the pages into the maths section of the 5-subject book.
When asked if Mel was getting the help she needs at school, one parent said
“seemingly” though she had a “rough start” in Year 8. Despite having had one transition day
for 5 weeks, when full-time school started the mother received a phone call two weeks into
the term saying “we’ve got these issues” to which she replied “well, I’m really concerned”.
On the first day of school, Mel was given her timetable with the floor plan of the school,
1-6 subject periods, classroom codes, subject codes and teacher codes set out. “I looked at it
and I struggled and I’m quite map-good” (U.23-306). She “cut out all the unnecessary stuff”
and colour-coded each subject to that classroom so Mel knew that pink was English, green
was Maths and Science was red. That really helped her “but I couldn’t believe that they had
all that information yet they still couldn’t simplify it for her. It was just too much overload”

170
(U.23-P-306). On the whole though, she thought educational experiences had been positive
and helpful.
The mother thought teacher aides understood Mel because they had dealt with several
other children with spina bifida before. “They seem to have a good understanding of the
expectation that I have for Mel and the level of output that I think is achievable for her
without me putting too much pressure on her … ” The mother attends IEP meeting where
any concerns can be raised or she would telephone the school about an immediate issue
(U.33-P-450). When asked if teachers and aides had received help with classroom strategies
to help Mel, the mother replied “I don’t believe that they’ve had any help with classroom
strategies. However they could possibly pick each other’s brains, go up to the unit and see if
they had any strategies. When she was in primary school, they often used to pick my brain”
(U.36-P-490). When asked if anybody had come to talk with teachers about the nature of
Mel’s learning needs, the mother said someone from the Spina Bifida Association had come
in Year 8 and she expected another visit by Year 10 “but apart from that, not that I’m aware
of” (U.30-P-418).
When asked if she thought peers understood Mel, the mother said “I don’t think that her
classmates probably understand very much about her at all. I think if they did then the
dynamics that she’s had in the past couple of years probably wouldn’t have ever happened”
(U.34-P-454). The researcher asked if student differences were overtly talked about at
school. “When she was in Grade 2 they did but no, not in the time that she was in primary
school, only Grade 2” (U.34-P-456).
When the researcher mentioned the teacher who spoke about the walking miracles in
the class, the mother said “that’s a good idea because I think if the children in the class have
a bit of an understanding about what a child’s disability is regardless of what the disability is
… they don’t have to have a great deal of knowledge just a little bit so that they have a little
bit more of an understanding at a tolerance level” (U.34-P-462). The researcher and the
mother considered the merit of teachers talking about individual differences to their class to
build a culture of caring and understanding. Students’ sensitivity to teacher vibes will likely
carry over to the workforce which can be as notoriously cruel towards individual difference
if such is not addressed early. “If you don’t pick up anything straight away, you’re seen to
be incapable or you’re a dummy whatever” said the mother (U.35-P-482).

171
A day in the life of Mel based on Mel and her parent’s reports
Getting ready for school
In Mel’s home, a normal day is “rushed in the morning, calm in the afternoon unless
she has somewhere to go” (U.1-P-2). The most critical issue raised by the mother was Mel’s
lack of organisation with getting ready to go places … “just doesn’t seem to understand that
there’s a time frame that you have to get organised in” (U.2-P-6). The parents set Mel’s
bedtime the same as her younger brother and sister “because it takes so long for her to get
organised in the morning … she is hard to wake up. That day the mother “woke her up at
half past 6 and it was a quarter past 7 before she was up and in the toilet to go into the
shower and the bus comes at about 10 to 8” (U.32-P-436). Sometimes she has trouble
getting to sleep and she may be still awake at 10.30 p.m. The mother wondered if this was
related to lack of mobility “the brain may still be wanting to work but the body’s a bit tired
so they can’t switch off” (U.32-P-440). With tasks around the home like drying the dishes,
Mel is organised and gets them done (U.3-P-10). Planning and time management skills were
described as “poor” and strategies used in primary school included the oven alarm and an
egg-timer. Mel can dress herself and the mother said she doesn’t buy anything with a zip.
Pull-up pants without a zip are easier and these increase her independence (U.18-P-198).
At school
Frequent room changes means Mel does not have an allocated desk but she chooses a
seat in the first or second row which allows her to see everything on the board and is “close
enough to the door that I can get out in case of an emergency, hopefully before everyone
tramples me” (U.13 contd.-S-126). All students are given a certain amount of time to move
from one class to the next irrespective of whether they have a disability or not “so if we’re
late, we’ll probably have to make up that time” (U.30-S-325). Group work in class is quite
easy because Mel gets along with most of the students but if in a group with no teacher aide,
she finds some members “are trailing off into their own conversations about certain things”.
She tries to get them back on track “but nobody seems to listen so …” (U.16-S-152). Group
work in the Physical Tutorial usually includes students in wheelchairs “and I get on with
pretty much all of them” (U.17-S-160). School is “pretty good but it could be a lot better ….
not the education side of things so much it’s more of the social side of things …. outside of
the classroom”(U.1-S-2-6). She felt teachers and aides understood her quite well and “I get
on quite well with both. I can work quite easily with both so it makes that aspect of school
easy” (U.22-S-222).
172
Coming home and homework
A taxi bus transports Mel home after school. She constantly tells her mother she has
no homework but if there is something important, a teacher or aide will ring and say “she’s
doing so well in English can you make sure this is done so that she can get a mark for it”
(U.10-P-72). Assignments often require a “bit of pushing from me to help her complete
those tasks” but over the years the mother has found it best to do the handwriting if Mel gave
the ideas “because it’s got to be up to her” (U.11-P-88). By Year 7, the mother felt it
important for her to start having ownership of her school life to gain that sense of
achievement (U.11-P-90). When asked if she remembers homework instructions, Mel said
she may enter these in her diary, write them on a separate piece of paper or in the allocated
section of my 5-subject book” (U.15-S-136). Researching information on the internet or in
the library was not a problem “I do get books out quite easily to find the information that I
need” (U.15-S-142).
Loneliness and friendships
Over the years, Mel has spent a lot of time with adults, probably more so than
interacting with other children. When her grandparents are over, she sits at the table and
chats and “when her great Grandma is over, she just sits beside Nan in the chair and holds
Nan’s hand and they talk … She’s got a great, really close friendship with her great Nan and
it’s really special, it’s really special” (U.38contd-P-512).
Mel has had quite a number of friends over the years but she does not pursue
friendships, for example, she will not ring or write to two friends who have relocated. A
local friend who has an intellectual disability “rings Mel all the time but Mel never rings
her” (U.25-P-362). The mother knew she had some friends at school “that aren’t disabled
children but none of them ever ring her … ask her out” (U.25-P-374) and “she’s never been
to any parties since she’s been at school … in high school” (U.26-P-376). She is struggling
with a couple of friendship dynamics at school and recently came to a conclusion that “if
they’re not going to talk to me then I’m not going to waste my time with them”. The mother
said “but that’s great you have to come to a stage when you say enough’s enough” (U.29-P-
412). When asked if Mel worries about what other kids are saying or what they’re thinking
the mother said “not that she’s passed on” but on a couple of recent clinic visits, the
paediatricians were concerned that “she’s clinically depressed” and the mother attributed
this to friendship dynamics with a particular group of children (U.31-P-430).
Mel spoke about lunchtimes at school. She has two or three friends that she sits with
and she recently had another good friend who she is “having quite a big amount of trouble

173
with” (U.18-S-164). When asked what sorts of things were happening, Mel said “leaving me
out and ignoring me and when they eventually do speak to me, the so-called leader of the
group she bosses me around and tells me what not to say and what to say and when to say it
and all of that and I had a big argument with her last year but it’s been going on a lot longer
than that” (U.18-S-168). But there are three or four students in the group who still talk to
Mel (U.18contd-S-176). She did not express feelings of anxiety but conceded she gets a
little nervous with some aspects of drama if required to perform things “but I cope with that”
(U.23-S-228). “So you’ve done the study about how people like myself interact with the
teachers and aides and how we learn. What about … have you done much study on the
social side of how people like myself interact with friends” asked Mel (U.27-S-274). The
researcher mentioned some study findings. She also spoke about the hiddenness of the
hydrocephalic condition and the difficulty for people to realise its implications. Mel said
“and the spina bifida part of it as well. They think that we can do everything but what they
don’t know is that we can’t” (U.27contd-S-296-8).
Mel does not have any problems inside of class because she was getting plenty of help
but “because of what’s been happening on the social side of things, I am getting counselling.
I have been having to get more from another lady and the guidance officer at school but of
course I’ve got to decide who, I mean, is the counsellor” (U.27-S-300). She felt the lady will
“understand more about the things I’m going through as opposed to my guidance counsellor
who’s a male” (U.27contd-S-302).
Tasks that Mel enjoys
“Music, drama, soapies, soap books and goss magazines” said the mother (U.4-P-14)
and Mel said “I like watching a lot of TV and listening to a lot of music and I sit with two or
three … my only three friends at lunch so that’s all of that” (U.2-S-14). At school, Mel is
reasonably good at English, reasonably good in Home Economics, Science, quite good at
Drama ‘cause I do that at the moment and Physical Tutorial I’m pretty good at that” (U.2-S-
29). Two or three days before a drama performance, everyone including Mel still had scripts
in their hands. When it came to the performance, half the class was still using scripts but not
Mel … she knew her lines (U.25-S-238). She was confident about copying from the board
(U.9-S-62) and changing from one task to another (U.10-S-70). To these assets the mother
added tables which have had much input (U.8-P-50) and Mel spoke about the “one very
good oral that I’ve done in my whole entire high school life” (U.24-S-234). Mel has done
abseiling and she was also a Girl Guide (U.19-P-206).

174
Strengths reported by mother
“Her tolerance, her love for her grandparents and her great Grandma. She’s extremely
understanding when it comes to other people, not her mother. Socially with adults, she’s
quite adept and she’ll try new things” and she will not panic about going to a new place or
say “what will people think” (U.37-P-498).
Tasks that Mel finds difficult
Probably tolerating input from her brother and sister and sometimes Mel gets frustrated
with her disability and how it impedes on her life, said a parent (U.5-P-16). Mel’s response
was “having to put up with my brother and sister, having to put up with my parents … that’s
pretty much it” (U.3-S-24). At home “I can’t reach … I can barely reach the bathroom sink.
I can’t reach the kitchen sink that’s why I don’t have to do the cleaning up after dinner so
I’m always stuck with the drying up” (U.21-S-218). She can trundle up to make a sandwich
if items are put out because some facilities are not wheelchair-friendly. She can get to the
bedroom but she needs to be lifted into the toilet or shower by someone (U.21-P-246). She
can chop a carrot “albeit not very well” and would probably struggle with a potato but she
would have a go (U.21-P-256).
Handwriting is very poor and she tires very easily, said the parent. “I am reasonably
slow depending on how much writing there is to do and it can be quite hard to read” said Mel
(U.6-P-28; U.11-S-74). Aides are very understanding and have tried to put handouts in place
to save large amounts of writing. An Alpha Smart is available but sometimes the physical
management of that on the back of her chair as well as her school bag can be difficult
because she has to take the bag off then take the Alpha smart off, set if up and then repeat
those steps to pack up and go to the next class (U.6-P-30). “I’m absolutely horrible at
maths” said Mel (U.4-S-29) and according to her mother “it’s taken a lot of input in primary
school to get to the level that she is … nothing too abstract but she’s got basic maths skills”
(U.7-P-46). Last year “I did have a bit of trouble concentrating on maths for I don’t know
what reason but I was usually just staring into space but this year that hasn’t happened in any
of my classes but we’ll see what happens as the year goes on” (U.12-S-104). Problem
solving “would be alright but in some aspects it can be a little bit difficult”. “I have a
reasonable amount of trouble with pretty much everything” but multiplication, division and
subtracting are considerably easier than “things like long division, perimeter, area and
algebra … yeah those kind of things can be considerably harder” (U.5-S-38-40).
Concentration and memory when learning anything new “takes its time. If it’s
something she’s interested in, recall is good but if it’s something she’s not really interested

175
in …” (U.9-P-60). To speed up Mel’s slow information processing over the years, “I would
say to her ‘I need an answer by the time I get to 5’ otherwise she would just ‘um’ and ‘ah’ all
the time or when she was really young she’d go off on a totally different tangent” (U.13-P-
118). When asked if she rolls her head and eyes … “mm all the time for sure. If she was
disgusted with something she would be throwing the head and roll the eyes and when she
was in primary school she was a real drama queen” said the mother (U.13-P-120-2). Mel
also rolls her head and eyes at home and she can go into another little world. She will hum
to herself and “you can hear her in the lounge room and she’ll be ‘rrrrr …” (U.13-P-128).
In a group situation, she may not always be able to keep up with cross-fire conversation
“she would possibly retreat not physically but presence wise” and if the pace was rapid, Mel
would get lost (U.15-P-152-6). She struggles with fine-motor things “because she is
missing the corpus callosum”. When she has something in one hand, the other hand will
move as well and this happens when she is writing. When a baby, the family used to think it
was cute when she waved because the other hand would wave also “‘till we discovered what
it means” (U.19-P-200).
Manipulative tasks are difficult. She can do buttons but they are difficult for her.
Writing and anything fiddly arty-crafty, cutting out or gluing is a little bit difficult for Mel
but she can knit. They did knitting as part of their Physical Tutorial though what she
produced was more like fishing net. She ended up with twice as many stitches as she needed
but a relative “tidied it all up for her” (U.19contd-P-226). Fine motor skills and using
scissors “are quite good” but gluing and pasting “it’s a shame I can’t cut straight or glue
anything on a piece of paper straight so that it lines up one underneath the other and in
corners and things” said Mel (U.21contd-S-210-14). She can cross the road “albeit very
gingerly”. She is very cautious and will look and then seem to dawdle getting to the other
side. “She’ll just sort of amble across” said the parent (U.22-P-264). Slowed mental
processing, spatial difficulties and inability to judge the distance of oncoming traffic impairs
her ability to cross quickly and horizontal nystagmus (spasmodic movement of the eyeballs)
may add to difficulties (U.22-P-276).
With a completely new task, Mel finds it hard to grasp the initial concept but with
enough practice it does get considerably easier (U.6-S-44). She complained about her
“horrible memory” (U.8-S-56). She can handle names and ages of people and places but
remembering how to do particular sections of maths is more difficult (U.8-S-58).
176
Post-school
The mother felt her idea and Mel’s idea might differ. “I think it will be challenging. I
think she’ll get extremely frustrated. I think her levels of depression will be extremely high”
(U.40-540). She thought Mel would probably not gain full-time employment. “No, I think
she’ll probably do a variety of voluntary work and probably a small percentage of paid work
realistically. I’m not trying to be negative on this but speaking realistically” (U.40-P-540).
Mel said “if I was good at art, I would have liked to have gone into the fashion industry as a
fashion designer and the other ones were, I may like to become a singer or an actress”.
Voice projection is quite good because she does inter-school drama and has done
recreational drama (U.16contd-S-273). “That’s still on the ‘maybe’ pile … otherwise a
writer or something to do with animals. It’s a very broad decision of occupations that are
still on the ‘maybe’ pile” and no definite decision has been made (U.26-S-246).
Advice for teachers or aides
Mel was asked if she had any hints that might help teacher or aides. She suggested we
all “pitch in together … if we can try and have the teachers and aides, well not so much the
aides, the teachers have a better understanding of our disabilities and what kind of
difficulties we have then they may be able to try and sort out a better way of teaching us so
that we can understand” (U.29-S-313).
Have you heard of a Nonverbal Learning Disability?
The mother and Mel were asked if they had heard of the syndrome and if not, if they
would like to know about it. “No, I haven’t heard of it” said the mother (U.41-P-566) and
“yeah, I think if we can find out about the whole range of things that are impacting on these
things for our children, the better we are and the more we can help and it also flows over to
other children” (U.41contd-P-590). Mel had not heard of an NLD (U.28-S-304).
Mel at school based on teacher and teacher aide reports
At school
Mel enjoys working on computers and doing science projects but cannot do some
practical tasks because standard bench heights create safety issues. The science teacher
therefore tries to incorporate tasks she can do (U.3-ST-22-6; U.1-ET-2). Mel seems to “cope
really really well” with Drama apart from needing help to secure her bag on or off her chair.
Her verbal skills “are excellent and she’s got a good grasp of vocabulary” and her wheelchair

177
does not appear to make any difference to her performances said the teacher (U.1-DT-4).
Getting into English classes can be difficult because Mel has to manoeuvre the furniture and
“manipulate her way through the crowd” to find a spot but the teacher tries to run in and
move the chair to make space for her and the aide along one side “out of the scrum” (U.1-
ET-1; U.1-MT-1). A normal English class requires the student to “come in, fight your way
in, fight your way out. No one gave her special treatment but by the same token didn’t really
give her any hassles either” (U.1-ET-2). Alphabetical seating means a boy ends up beside
Mel. He was not keen to sit next to her but the teacher did not think it was related to her
being in a wheelchair. “He sort of always moved his desk out of the way and kind of had his
back half to her so that wouldn’t have really helped but I didn’t move him because no matter
who I put there, I don’t think the situation would have been terribly different” (U.1-ET-2).
Maths …“nothing stands out particularly. She seems to have reasonable number skills and
overall performance on other units worked on “has been fairly even over the whole lot.
Some things she’s passed and some she hasn’t. She hasn’t done outstandingly well on the
whole” (U.19-MT-83).
She loves team sports organised by the SEU though it took a while to gain confidence.
Backward balancing was difficult at first but she allows the Physical Tutorial teacher to keep
pushing her. She likes to attempt things for herself and does not like anyone to automatically
do things for her (U.5-TA-23). Mel will always try to achieve a new goal and team members
are very supportive (U.3-PTT-6). “She’s like a dog with a bone. She doesn’t shy away from
an issue. She won’t verbally consent but will give it a go … “we’ll see” (U.18-PTT-6). Her
determination is a strength but she can be obstinate (U.18-PTT-36). “She is determined and
she’ll persevere if she wants to. I think she’ll give up as easily if she’s not interested too
(U.29-HEcT-215).
Mel has got better at moving around the school and getting to classes quicker but
getting “ready to start” is a problem (U.22contd-HEcT-105). She “fusses around” in Home
Economics classes and at washing up time “they can call her back and call her and ‘I just
have to stir this three more times before I’m ready’” (U.11-HEcT-109).
Loneliness and friendships
Mel “doesn’t seem to do well in that area” and her sense of humour and interests are
probably more adult (U.28-HEcT-211; U.14-TA-128). “You can see she’s had a lot of
difficulties to deal with, a lot of hardships that other people never go through and mostly
contact with adults and that may be part of the reason that she doesn’t have these friends
particularly here in this school”. Even if she was open enough to make lots of friends, it may

178
be difficult for her “to find someone who’s really at her level” (U.28-ET-188-192-6). She
did not seem to have a special friend or buddy though “I dare say she does have special
friends up in the unit” (U.17-MT-73). One aide said “she’s not a loner. She does mix with
other SEU student and other girls as well” (U.11-TA-93) but another observed “a problem
with friendships” (U.14-TA-128). “She wasn’t like the rest of the kids. They’d muck around
and joke and she wouldn’t find that humorous at all … she’s so serious” (U.14-TA-128).
After working regularly with Mel, two aides “got to joking with her and she would laugh”
and share a private joke (U.14contd-TA-132; U.24-TA-114). She used to be by herself
sometimes “but I think a bit of it was because she seemed really old for her years” (U.14-
TA-128). She is always going or coming on her own and “she’s always alone and isolated”
(U.1-ET-2; U.28-ET-215). “I think it’s a fairly lonely existence in life that she leads and yet
the kids responded really positively to her when they heard her speak because I think like
me, they had never really heard her speak”. She is a lovely girl, very shy and quiet and with
the arbitrary type of core subject grouping, “I would say that she’s quite lonely” (U.26-ET-
182-4).
Mel enjoys talking and just being able to sit with other students and listen to them tell
silly stories and sometimes she raises her eyebrows. She “doesn’t seem to make friends
easily” because she speaks as an adult and does not enjoy silliness with a lot of the teenage
students in class” (U.5-HEcT-44). At lunchtime she sits with students from the SEU and
was reported to “mother” a very high-needs student who understands everything but he is
himself, nonverbal (U.15-PTT-30). Mel would often sit, talk and read to him (U.14contd-
TA-132). One aide considered he was her special friend but “I don’t think she has a
girlfriend”. She is accepted in the SEU “but there are no sleepovers and the teacher
wondered whether this could be due to friendship or transport restraint (U.17-PTT-34; U.28-
TA-304). In the SEU, she did not have a special friend but rather “a general friend” (U.17-
PTT-34). She did not have a special friend in another class “but they do help her. If I asked
‘would you like to work with Mel today, she’s very cool she doesn’t bite’ … no, they’re
always very good to her so that’s good” said the teacher (U.17-ST-147-9).
Two aides perceived Mel to be a very calm, unphased, laid back sort of girl (U.22-TA-
211-3; U.13-TA-126) while another said she gets anxious about friends. “I haven’t seen her
angry” but for one presentation, Mel wrote a story about school, friends and falling out of
friendships and bitchiness. She used fictional names but then said “Oh! Would you believe
that some of this has happened to me?” The aide thought this alluded to the fact that Mel’s
account was based on a real-life story that she had experienced but said she did not show any
great distress during presentation (U.16-TA-82).

179
Strengths reported by teachers
Mel is a mature young lady who has a good grasp of language (U.2-PTT-4). She is a
very well-behaved student with an even temperament who never seems to be in a bad mood
(U.1-MT-2). One of her strengths is her mature attitude and the fact that she seems to be
able to cope with whatever is thrown up without herself getting thrown by it. “She copes a
lot better than half the class” (U.19-MT-81). She is very independent, cooperative, patient,
dedicated and tries very hard (U.5-MT-12-4; U.18-ST-151; U.21-TA-306). She knows
exactly what she wants and she will not be swayed. When comfortable with people, “she’s
got a really nice sort of caring side to her and she’s very concerned but I think it takes her a
while for that to come out. She was very standoffish when she first came here and we
thought ‘Oh quite rude’. She did not mean to be rude but came across as being very blunt
(U.21-TA-206).
“Strengths … a very good mind, a very wide-ranging vocabulary. Her oral skills really
surprised me” (U.30-ET-233). She is extremely polite, pleasant and extremely cooperative
generally at having a go at things but “they don’t quite get finished”. With a teacher aide,
there is certainly less for her to do in the classroom and she always held her own (U.30-ET-
233). She does exceptionally well in the area of conversation and communicating with
people and one aide found it quite frustrating when she would say “some things that you
would expect perhaps a mum or her parents to say. She’s quite adult in that way” (U.24-TA-
114; U.5-TA-23). Mel is not “a shrinking violet”. She is very good orally. She will say
what she thinks and “will have a go at someone for not working or staying on task and she’ll
like roll her eyes when the boys are being stupid” because she is quite mature (U.22-DT-
108).
Independent Education Plan (IEP)
Mel attends the SEU three times each week where she partakes in the Physical Tute
class. The focus of Physical Tutorial is on the child’s disability and most students have
trouble with fine motor skills (U.1-PTT-2). The aim is to make students fully independent
around the school and for Mel, teaching her to get in and out of her wheelchair. She gives
this class her full concentration. Mel plays wheelchair basketball and as she does not have
good eye-hand coordination, they use small, softer balls and lower the goals (U.16-PTT-32).
In a mainstream class, Mel “still manages to do the ball games and things but often kids
mightn’t include her because she’s obviously going to be slower than some of the others”
(U.19-DT-94). In the Shop class, Mel is supported by an aide to safeguard her safety (U.36-
TA-402).

180
Getting class work finished
“She’s usually still writing right to the end of the lesson” and uses whatever extra time
is allocated to catch up (U.8-MT-28-32). Although Mel has been repeatedly asked to put up
her hand for help, she never does and even when asked for suggestions about help “she
doesn’t seem to have anything to offer there” (U.2-MT-2). Fortunately an aide comes in one
day out of three to assist “but for the rest of the time she pretty much works on her own with
just occasionally help from me” said the teacher (U.2-MT-2). Getting work finished is an
issue (U.13-ET-64; U.6-ST-64). Even with the help of an aide, she never seems to complete
anything (U.13-ET-64). “She’s lovely. She’s really light and happy to chat with but she
doesn’t seem to meet deadlines”. When work is almost complete, “it’s all those issues as to
why she can’t print if out and why she can’t hand it in”. The teacher felt it might be a total
lack of confidence on Mel’s part … “She doesn’t want to make that commitment to submit
something for it to be rated by anyone” (U.7-ET-14).
In English class, the aide encourages Mel to do some writing then communicate her
ideas for the aide to scribe. “If I wrote something down in a way that she didn’t want it said,
then she would just say ‘change the word’ so we would do that” (U.8-TA-40). She “always
seems to be disorganised, always saying she’ll get it finished or saying she’d work on it …
the work always looked like it was all being done but it never really came to fruition. It
never really finalised itself to the point where it was handed in or whatever” (U.29contd-ET-
218). In the SEU, Mel “is an intelligent young lady” who gets her tasks done and the teacher
makes sure students get the time they need to finish (U.5-PTT-10). In one practical class
where tasks had to be finished, the teacher said you “feel like you’re pulling teeth but it
happens. Well she’s handed her work in and she’s done what’s required” (U.15-HEcT-139).
Mel has trouble getting long tasks finished said another teacher (U.5-ST-60-2). In some
classes Mel has no teacher aide but “when we’re there, we make sure that she’s finished”
because she is a slow writer and the timeframe is difficult for her (U.14-TA-121; U.6-TA-
50). If there is no aide, she may “battle on” for too long before asking for help (U.35-TA-
384). “She definitely needs monitoring and she definitely needs teacher aide assistance in
any practical classes” (U.35-TA-384).
Homework and assignments
“Not good, not very good, not on time. I think the vast majority of them were late
unless they’re actually able to be done in class. A lot of them are at least started in class”
said an aide (U.24-TA-233-9). Mel needs frequent reminders “well she rarely does her
homework when it’s due” and without an aide “she just couldn’t do it in Home Economics.”

181
(U.17-TA-143-5). Big assignments can be “tricky” and are often modified for Mel (U.14-
TA-121). If an assignment was almost finished except for the conclusion, the aide would ask
Mel to do the conclusion but this did not happen. She could not complete assignments and
hand them in on time and “even though she was good at English, she did struggle to get her
assignments in on time” (U.18-TA-86).
A teacher gave spelling homework each week to teach students something “about
meeting a deadline, making a commitment and doing the right thing” (U.15-ET-74). They
were asked to write out 12 words 10 times each over 5 days “about 20 minutes work for a
week” said the teacher (U.15-ET-74). Mel “only did hers probably not even 50% of the time
and that really disappointed me”. Students who did not comply had to do the spelling in the
computer room at lunchtime and those who skipped received an administration detention
(U.13contd-ET-66). Despite numerous contacts with her mother, spelling homework and
some assignments were not handed in or did not “come in until very late in the piece” (U.9-
ET-34; U.18-TA-86; U.15-TA-162). Because she did not do the lunchtime work, Mel got
quite a few administration detentions. “I couldn’t treat her any differently to anyone else” so
she would get a 45” administration detention manned by the deputy which lasts a whole
lunchtime. This misdemeanour is permanently recorded on the student’s file (U.13contd-
ET-66).
She could research basic information on the internet but “putting it in her own words
would probably be the hard thing to do” (U.24contd-TA-247). Mel handles the computer
well but is slow to skim through data and isolate what is relevant (U.10-ST-90). She
struggles more if researching from books said an aide (U.18-TA-86).
Copying from the blackboard and handwriting
Mel can copy from the board “but slowly” and what she copies seems to be correct
(U.10-MT-38-40; U.7-ST-72; U.10-DT-36). Accuracy was gauged at about 80-90%
(U.10contd-TA-60) though she needs to keep looking at the board (U.16-TA-131).
Sometimes Mel would read from the board while the aide scribed which allowed her to
initially process the new data (U.8contd-TA-42; U.10-TA-80).
The most difficult task “is written” (U.7-DT-19, 72). Handwriting is “really big and
scrawly”, “very spidery” and looks like it’s taking up two lines not one” (U.16-TA-133; U.8-
TA-53; U.2-ET-2; U.12-ET-56). She “hates writing and it’s very messy and untidy and if I
go over and have a look at what she’s doing, I find it quite difficult to read it”. She speaks
very well but writing what she could verbalise and putting it into sentences was difficult and

182
some of it was illegible, said aides (U.5-TA-18; U.10-TA-56). She is “so very slow with
writing” and “the re-reading of it can be a bit dicey” so the aide provides a handout for
revision (U.4-MT-2; U.7-TA-47). Other teachers said handwriting was not so difficult “that
it’s a minefield”, “it’s not completely unreadable but it is very messy” and “it’s the actual
mechanics of her handwriting that’s not good (U.17-HEcT-159-161; U.8-ST-78; U.3-DT-
12). When she tries to draw activities made in a maths lesson, “the drawings are very hard to
understand” (U.4-MT-2).
Comprehension and following instructions
“Certainly the everyday language is not a problem” but mathematical language may
sometimes cause a blank look that calls for more explanation (U.22-MT-93). Mel could
comprehend instructions that were verbally explained but “she didn’t seem too proficient at
reading instructions” like following a recipe (U.3-TA-8). In one practical class where tasks
involved a series of steps, she needed help “so if there was no one there to tell her, she would
be lost” (U.7-TA-60) but the Special Needs teacher knew to give only one instruction at a
time (U.6-PTT-12). An aide reported times when Mel would misinterpret text but when two
scenarios were presented, explained and compared, “the penny would drop and she’s say
‘Oh, now I see!’” (U.27-TA-170).
Planning, organisation and time management
“I would say poor” (U.11-TA-62). “That’s a problem” (U.9-ST-86). “Definitely needs
help with that. If she didn’t get help with that, I think she’d just give up or just feel like she
was getting nowhere because I think she’d just fuss around the whole time and miss the point
of everything”(U.18-HEcT-163). Her 5-subject work book was very poorly organised and
she had no consistency with where she wrote subject notes from class to class (U.13-TA-64-
6). When Mel shares personal things with one teacher “they won’t make a lot of sense
because it’s really holding up her organisation …” She takes a long time to get organised
with her bag and drops lots of things and if the teacher did not make time to get to know her,
“you’d only know her as someone who’s always dropping her bag on her way to class”. The
SEU has a set routine and Mel was said to be self-motivated (U.9-PTT-18). She definitely
responds well to the toileting routine “and if she gets out of routine, you have to go up to
remind her” (U.12-TA-109-110).
One teacher attributed Mel’s poor planning, organisation and time management skills to
expectations. “I think she’s used to having people, other people organise her and other
people think for her and I think that at her stage in life, she needs probably to take on some
responsibility there for that”. An aide offered to phone Mel’s mother about work due but the

183
teacher “felt that Mel was more than capable of managing that herself” (U.21-ET-118).
Students intending to do the work had got it in but Mel’s was one that had to be passed to the
head of department to ring home. The work that eventually came in was not passed because
only about one-third was done “… it was just not acceptable” (U.21-ET-118-126).
Handling novel tasks or situations
Aides said Mel needs constant prompting with any new task and if slow to start, she
may need guided instruction or she may watch another student first (U.33-TA-366; U.7-TA-
34).
Rote memory skills
Mel would know all of her script whereas half of the class had scripts in their hands
“she’s fine with that sort of thing” (U.2-DT-10; U.26-DT-128). When doing long
multiplication without a calculator, 90% of her times tables would be right, said an aide
(U.21-TA-187).
Maths
Mainstream maths is the hardest area for her (U.2-TA-25). She has trouble
remembering to bring tools like her calculator and “never ever has them” for class but she
always has pens (U.2-TA-33; U.19-TA-167). Mel is willing to try problem solving maths
but she needs some assistance to interpret questions. Activities done in pairs overcomes this
to some extent (U.7-MT-20-4).
Concentration and memory
Memory “is not the greatest” and Mel finds intimate concepts such as toileting hard to
remember. “An avoidance behaviour may be to pretend to have memory loss to avoid going
to the toilet” said one teacher (U.10-PTT-20). She remembered to bring a vase from home
for a practical class without notes or phone calls from staff (U.10contd-HEcT-91) but would
never bring in the sewing equipment needed from home ‘I’ve forgotten again’” and she did
not write reminder notes (U.13-TA-115). But her memory “isn’t terribly good from one
lesson to the next” especially where task planning was involved. She was slow to locate all
craft materials for decoupage and found it difficult to “work out the advantages and
disadvantages of what they were going to make” (U.12-TA-108). Concentration and
memory “needs help”. She tries to concentrate but “she’ll lose it if someone talks or she’ll
sort of get into this little dream world where she’s just staring up into space”. Recall …
“she will forget” and needs lots of reminders (U.19-HEcT-167).

184
Mel achieved excellent results in a recent science test and in fact did much better than a
lot of the class so from that point of view “her memory is excellent” said two teachers (U.11-
ST-96; U.22-ET-146). Apart from the handwriting, “she looks like any other student to me
in fact she was one I would call bright. She would be one of the brightest in the class … I
didn’t see any problems with short term memory or difficulty with comprehension or
anything” (U.23-ET-150-2). The aide said Mel likes English and excelled at the oral work.
“She did very well. She got voted the best in the class for an oral presentation but her
memory’s obviously quite poor” (U.14-TA-76).
Verbal skills, vocabulary and orals
Mel is a mature young lady who has excellent verbal skills and a good grasp of
language (U.4-DT-4; U.2-PTT-4; U.5-HEcT-44). She speaks well and verbally seems to be
able to communicate with no trouble at all … “perhaps she seems to understand better than
those around her” (U.21-MT-89). Mel is best at performing an oral and is “interested in the
sense that she’ll give you information”. She has a very clear voice, very precise in her
choice of language and she is a good conversationalist (U.6-DT-18, 110; U.27-DT-132). She
is quite mature for her age” (U.27-DT-132) and is very concise and adult with her choice of
words in orals (U.2-TA-10).
The English teacher reported “very very good” oral skills. The class had two orals that
semester and names were drawn out of the hat for order of presentation. The teacher was
unsure about Mel’s response to an oral so deliberately kept her name aside until last. “She
ended up being virtually the last person to do it and hers was absolutely magnificent” (U.5-
ET-10). Students sat there and said nothing whereas normally half of them are still talking to
each other and need quietening by the teacher (U.33contd-ET-243). What she did “which
many of the others didn’t was she actually put on the accent of the character that she was
doing and no one else did that” (U.33-ET-243). “No one said a word from the very first
minute. She got their attention and kept it through the quality of what she was saying and
her attempt … which takes a lot of guts … to actually go into role and put on a voice”
(U.33contd-ET-243).
To provide opportunity to praise Mel, the teacher said to the class “we’ve heard all of
them now, who’s do you think was the best” and everyone said ‘Mel’s’. She was “thrilled to
bits” and after class the teacher said “look you’re always really quiet in class. I was just so
impressed with your oral presentation”. Mel said she had been having private Confidence
Building or Assertiveness training which “obviously has paid off” said the teacher. With the
second oral, she got up quite confidently and “did a really good job again” (U.5-ET-10).

185
Mel has a great command of the English language “in fact some of the kids said ‘you know
what I liked about Mel’s … Oh, all those big words! I didn’t know what they meant but they
impressed me’. She has a very very good command of the English language and is able to
use big words appropriately and there’s obviously a lot more going on there than you see
from the front you know” (U.5contd-ET-12).
Group work with peers
She sits back and is extremely quiet and withdrawn and she doesn’t usually say
anything. She may write things down but would not voice her opinions and if asked in class
“have you got any questions” will always say “no” (U.26-HEcT-207; U.14-ST-129). But if
in a class with other students with special needs “she would work with them but she didn’t
generally do things with other kids”. If she was the only special need student and “she had
to pair with someone, she very often wouldn’t … ‘I can do it myself’ or she’d work with a
teacher aide” (U.18-TA-192). One aide thought Mel could understand group interaction
“with the special needs students, not so much with the other ones because if they’re mucking
around she’ll tell them to stop mucking around” (U.26-TA-282-4). In a social setting, she
will listen “but she’ll do what she wants to do” (U.26-HEcT-207). The SEU teacher said she
may come across as a little bit bossy and “other kids may think of her as rude” (U.14-PTT-
28). In mainstream class groups, she can probably comprehend bits and pieces of the
interaction “but overall it needs to be much slower for her but it is not a major issues because
she still picks up the things that are important but they could be fairly quick for her”
(U.14contd-ST-131).
With group selection, Mel does not take the initiative and put herself into a group but
waits for the teacher to place her. She sometimes finds it hard to compromise and can be a
little stubborn and gets annoyed “if kids aren’t focused and on task which is good” said a
teacher (U.17-DT-26, 74, 84). “To be honest, my picture of kids in the group is more of her
working while the others stop to talk. She really does stay on task very well” (U.23-MT-95).
Two other teachers perceived Mel’s difficulty with group work as being due to her maturity
from the amount of time spent with adults and health professionals (U.27-ET-188; U.5-DT-
16). She gets easily bored with the other kids like immature boys in the class and “gets
almost disdainful of them which I don’t blame her because I do too”. She sticks up for
herself in a subversive way and will ignore and roll her eyes at any student who considers
giving her a hard time (U.5-DT-16).

186
Everyday taken-for-granted tasks
Moving around in a wheelchair “might be constraining in some ways” (U.13-ST-111)
and learning new physical tasks “would probably be the worst things for her to try and do”
like learning to balance on the back two wheels to get up and down gutters (U.6-TA-37;
U.29contd-TA-309). Fine motor skills such as using scissors and writing skills are difficult
(U.12-PTT-24). Information processing is slow and “because people don’t always
understand, they may think she is rude” (U.4-PTT-8). Toileting is time-consuming and Mel
self-catheterises at the start of the second lunch break and then meets her friends afterwards
(U.11-TA-97). “She is very determined and goes at her own speed, like the train!” (U.13-
PTT-26). She often turns up to class without the “tools that she needed to work through the
day” and once settled, she is “very very slow” to get books out (U.19-TA-96). Using the
sewing machine is very difficult because the school does not have elbow press-starters. Mel
“manages quite well” if the foot pedal is put on the table and she can “use her elbows to run
the machine” but if an aide uses the pedal for her, it raises a safety concern (U.3-HEcT-16-
18).
One aide helps Mel and other students with special needs in the cooking class (U.14-
HEcT-127) and her most difficult task is following the recipe (U.4contd-TA-14). She is
“very very slow with any chopping” and is determined to have everything the same size. If
asked to “chop roughly it’s still got to be all precise even though she has difficulty with the
knife” (U.13-HEcT-123; U.25-TA-264). Coordinated ability to hold with one hand and chop
with the other is slower than a lot of students. She gets it done but not in the timeframe
(U.4contd-TA-14). “I mean there’s a lot of gnashing of teeth and time and stress involved
with it but once again, her nature of ‘ah, it’ll be right’” is good but it can be frustrating
(U.13-HEcT-123). Decision-making in the kitchen takes a long time and the teacher
wondered if Mel likes to hear what other people are doing and gather all information before
making a decision (U.7-HEcT-48). She was very slow to make decisions in the decoupage
class and would say “no, I’m still thinking” and seem to go into another little world (U.9-
TA-76-78). She manages to get everything done in the Home Economics class with
assistance. “I don’t think she could cope without the assistance. I think she would be too
frustrated with the fine motor and organisational parts of it”. (U.24contd-HEcT-197).
Carrying things is difficult because “she doesn’t often put them in her bag. She tries to
carry things on her lap and they roll off”. But “once again that’s just an organisational thing
in that she often wants to do it quickly and stop and reach around to get her bag or get
someone to open it and put it in for her” (U.24-HEcT-195). Everything is everywhere in her
schoolbag and when she tries to get something out, everything would come out “so it’s

187
probably just like organisation and stuff like that” thought an aide (U.17-TA-184). Dropping
papers in class can be a problem and one teacher picked sheets of paper Mel had dropped
“probably four times before the end of the lesson” (U.11contd-HEcT-113). “Just being
down that low is an issue because the world is set up for people who are another three feet
higher” remarked one teacher. Everyday life tasks are quite difficult at that height regardless
of whether you have quite good manipulation in your hands or quite an active brain and “I
think everything is pretty difficult for her in terms of having a bag with everything in it
behind her” (U.25-ET-174).
Critical life skills as represented in school
Written work is difficult for Mel and “she takes a very long time to do tests because she
takes a long time to write things down” (U.4-ST-16, 46, 50). “She can sometimes be a little
bit lazy with the written work, a battle but it’s nothing major” (U.5-DT-16). An aide
observed that Mel eats her breakfast and lunch when she gets to school at about 8.15 a.m.
“so I don’t know what she does in her lunch break although she does have to toilet and that
can sometimes take 20-25 minutes (U.23-TA-104). When asked once, she had not had any
breakfast. “We get 2 breaks so I don’t know if she saves anything but she eats things like
donuts at ¼ past 8 in the morning. So I talked to her about eating healthy food for herself
and she was tucking into a donut!” (U.23-TA-112).
Teacher and aide perceptions of Mel as a person with a disability
Advice for other teachers
“Keep checking on her because she does not ask for help and she does need it” advised
one teacher (U.24-MT-103) while another said “time is the most major issue because she has
everything else”. Give handouts instead of asking her to do copious amounts of writing
which is very difficult for her (U.24-DT-116) and have a chat and a joke with her at the end
of class. “It’s nice because they know that you care for them and they might actually try
even harder which is excellent” (U.20-ST-166). Another teacher said “you’ve got to sit and
talk to students in a wheelchair … find that talking time otherwise she’s not going to initiate
it” (U.31-HEcT-223).
In a Drama class, the teacher advised not to modify activities “just keep everything
equal and that’s why I think that I haven’t had any issues with them because I haven’t treated
them any differently. I’ve made allowances but I haven’t treated her as anything special.

188
It’s just she’s one of the class. I think it’s really important that teachers don’t single her out
and don’t say ‘Ah well! You don’t need to do this’”. Treating students exactly the same so
“they do extend themselves further …” was said to work well (U.24contd-DT-116). Try to
integrate them as much as possible so they don’t feel different and “click into something
they’re good at … that self-esteem issue is the biggest factor that is going to help promote
their learning”. Try to arrange the room and activities so they can participate and “try and
find something where they can get praise just as other students would do” (U.32-ET-239,
241). Work with the child’s personality and with Mel, her determination. Find their
strengths “and hone in on them (U.20-PTT-40).
An aide suggested trying to deflate situations with humour “then you relax”
(U.25contd-TA-124). “Get to know the student, accepting them as they are and trying to
work the best way that suits them and their personality …” (U.25contd-TA-124). If the
student appears to need help, ask “are you having trouble, can I help you” because Mel
“doesn’t like it at all if you just take over” (U.30-TA-326). Each student is so different and
the aide needs to “work out what they’re capable of”. Get to know the child first and let
them have a go first before you “rush in and do stuff for them” (U.23-TA-222-6).
Anything else you want to tell me?
In the classroom, “there is a lot of writing and there needs to be a solution to the
slowness there”. It can be printed material or someone to write for her, carbon copies or
even a little machine but “whether she’d be any faster typing things rather than writing them
down, I don’t know” said a teacher (U.27-MT-137). One teacher who knew Mel the
previous year said “she’s very friendly and apart from being a teenager with all the teenage
problems, she seems like she’s maturing quite happily and I imagine that she’ll be carried
along” (U.34contd-HEcT-251). The teacher who witnessed Mel’s excellent oral
presentations said “if I hadn’t taught her for English and I only had her for the computing
subject, I might not have been able to give you the insights that I have” (U.36-ET-259)
whereas other teachers may “see her as someone whose writing and perhaps personal
interaction, which is quite shy and doesn’t say a lot, would be all they would have to go by”
(U.36contd-ET-265).
Teacher understanding of learning difficulties
Mel has a very very good command of the English language. She is able to use “big”
words appropriately and “there’s obviously a lot more going on there than you see from the
front”. “She’s lovely … she’s really light and happy to chat with or whatever but she

189
doesn’t seem to meet deadlines” (U.6-ET-12-14). A SEU teacher said she appears vague
“and I explain that this is because she needs extra time to process information. Teachers
might find her rude so I try to make sure that people know Mel needs extra time to process”
(U.2-PTT-4). One practical teacher hones in on safety issues because “safety is such a part
of being confident” and she wants all students to succeed. “You have to give them the
latitude to find their own confidence otherwise they can also be a bit jumpy with the knives”
(U.25-HEcT-203-5).
“She’s quite a capable student. I didn’t have much time one-on-one with her because I
was so tied up with the rest of the class but my perceptions are that she’s quite bright. She’s
very capable and without the handicap that she obviously has stopping her from writing well
or whatever, I think there’s plenty going on up top (U.11-ET-72; U.4-TA-8-10). But I felt
that Mel has plenty of brains, plenty of ability but was probably getting away with more than
she … I think there’s overcompensation somewhere along the way ‘Oh, we won’t make Mel
do that’ and that’s why I said ‘No, if she hasn’t done the right thing, she’ll get the detention
the same as everyone else’”. “I had very little real interaction with her … sometimes I think
that being on the peripheral of things you can actually see a lot more than if you go right in”
(U.16-ET-78, 86). If the teacher aide was called away, “she was not keen to do much on her
own. I think she’s become a bit reliant … my belief is a little bit pampered and a bit
mollycoddled and I don’t think people are, because she’s in a wheelchair, I don’t think she’s
being pushed the way she should be ‘cause as I keep saying, I think she’s really quite
capable” (U.18-ET-88-92). “Anyone who can sit there and give the two oral presentations
that she gave to me, the language that she used … the kids were right, it was quite
sophisticated language and it said to me here’s someone who’s quite bright but not showing
her true potential for whatever reason” (U.19-ET-92). “She’s a good kid and she’s got lots
of potential but I don’t think it’s really being tapped and promoted as much as it needs to be”
(U.24-ET-166).
An aide thought Mel did not listen very carefully because she had a tendency to think
she knew everything. “Sometimes I found her to be quite stubborn which was frustrating
because I knew that she didn’t know what she was doing but she would just keep going
anyway” until the atmosphere became relaxed then they would go back (U.6-TA-26-8). “I
think she’s a lot more capable than we saw. She needed a lot of prompting to start the
lesson and to get the stuff out but I found it a little bit frustrating with her” (U.5-TA-24).
Mel did not usually come to class and get set up “whereas I felt that just to get out your
pencil case and your book and that would have been okay for her” (U.5-TA-26).

190
Teachers were asked how Mel’s strengths could be used post-school. Her oral skills
they are really quite quite outstanding … her forte is going to be the verbal. I could see her
as a radio announcer” (U.31-ET-235). This teacher expressed concern about Mel’s “lack of
ability to finish anything and completion rate is very very poor and organisational skills
generally. It’s a mystery in life that it always seems to be going along okay but it never kind
of gets there” (U.34-ET-247). Teachers suggested a job which dealt with people (U.20-MT-
87), some sort of teaching because of good oral skills and ability to explain things (U.21-DT-
100) or continuation from school to tertiary study if Mel could cope with the pace of work
presented (U.19contd-ST-163).
Have you ever heard of a Nonverbal Learning Disability?
“What” said the first teacher asked “that would be like a spatial … I guess people have
all sorts of learning disabilities don’t they. I don’t know that I’ve heard anything about it in
any great depth”. The researcher spoke about reports in the literature that some children in
this population do have an NLD. “Yes, I think I read that last night too … and that seems to
tie in with what I mentioned before about the diagrams she draws” but when it comes to
manoeuvring her chair into place between furniture, there doesn’t seem to be any spatial
problem at all. She seems to be able to judge that well” (U.26-MT-117-129).
The next teacher said “I may have in other, like in a broader sense”. After explaining
that difficulties are in the nonverbal domains and students have relatively better verbal skills,
the teacher said “well I think that would be quite accurate because she can verbalise but she
doesn’t want to interpret things clinically” (U.34-HEcT-225-7). The researcher was asked
how this disability would exhibit itself and what behaviours would be displayed. She spoke
about functional difficulties, fine motor, and trouble handling new situations but good verbal
skills that convey an impression of competence. The teacher perceived Mel to experience
such difficulties “so perhaps that is that condition or that aspect of it … I’d say that’s Mel”
(U.34contd-HEcT-229-249).
After explaining the consequences of white matter damage in layman’s terms, another
teacher said she could see a bit of a pattern when Mel does her tests. Questions that require
thought about “what might happen to this, this and that” she will usually leave blank. So
that’s interesting because it correlates with what you’ve said” (U.22contd-ST-197). Two
aides had not heard of an NLD while a third said (U.26-TA-128; U.32-TA-340; U.24contd-
TA-260-264) the good verbal skills cause one to think “they know everything … you think
they’re very high functioning” (U.26contd-TA-162-166-sv3). Whilst one teacher noted an
association between hydrocephalus and a spatial difficulty from the internet the night before

191
interview and another “may have heard of it in a broader sense”, one may speculate that no
teacher or aide expressed bona fide understanding of the NLD syndrome.
Summary of 2005 Psychological and Speech Assessments
The following extract has been taken directly from assessment reports.
2005 (aged 14 yrs 11 mths) Full Scale IQ = 74
Verbal IQ = 89
Performance IQ = 63
VIQ-PIQ difference = 26 (clinically significant)
Language assessment age equivalent = 11 yrs 11 months
Problem Solving age equivalent = 11 yrs 4 months
Mel does not fall into the category of intellectual impairment. On a test of general
intellectual functioning, she performed within the borderline range for a girl her age.
However, her performance on verbal intellectual functioning was in the low average range
whilst her performance on non-verbal functioning was in the severely impaired range for a
girl her age. The difference in magnitude between her verbal and non-verbal intellectual
functioning is clinically significant with only 2% of girl’s Mel’s age having a difference of
this magnitude. Such a difference however is not uncommon in children with spina bifida
and hydrocephalus and can be attributed to the neurological difficulties associated with these
conditions. Due to the difference between her verbal and non-verbal intellectual functioning,
Mel’s general intellectual functioning is not a good indicator of her intellectual abilities and
so should be interpreted with caution.
Mel did however demonstrate some relative strengths and weaknesses. Mel
demonstrated good general knowledge, knowledge of word meanings and ability to express
them verbally. She also demonstrated a good understanding of relationships between verbal
concepts. Mel had greatest difficulty with tasks of sequential reasoning and speed of
information processing.
The results of academic testing indicate that Mel is performing above that predicted by
her intellectual functioning regarding areas of verbal development such as spelling and word
reading. However, she does experience great difficulty in a number of other areas which
need to be considered in her academic program. These areas are as follows:

192
• Any task which involves an organisational component (e.g. having a tidy desk to
undertaking a project);
• Tasks which involve visual perception and motor coordination;
• Learning new material;
• Working memory (ability to manipulate data in mind and produce an output);
• Tasks which require Mel to work at a fast pace;
• Most areas of non-verbal learning.
Interpretative discussion
Mel’s mother was the second person to respond to a recruitment mail out. At that time,
she considered Mel’s educational experiences had been “positive and helpful” on the whole.
At the mother’s request, parent and student interviews were conducted on different days in
the lounge room of the researcher’s home. The mother dropped Mel off for her interview
and Mel said she was comfortable to do the interview alone. I was very impressed with Mel.
She spoke in a sensible and mature manner for a girl her age. When asked about potential
problem areas, she said it was difficult dealing with social things, her brother, sister and
parents. She mentioned seeing two counsellors. During casual conversation later, the
mother and Mel expressed a difference of opinion regarding Mel’s time management skills.
The purpose-built school that she attended was designed to cater for students with or
without a physical or intellectual disability. Interviews were held in the school chaplain’s
office in the administration block. On the whole, teachers and aides were relaxed and at
times seemed imprecise when talking about Mel. Two teachers were a little guarded at the
beginning of the interview. After working through transcripts, I felt practical teachers
offered more detailed insight than teachers of academic subjects which may have been due to
a need for individual checking on progress of practical tasks. I sensed a tone of
accommodation and acceptance at this school, congeniality amongst staff and there was an
absence of bullying reports from the staff I spoke with.
Apart from the teacher who saw NLD mentioned on the internet “last night” and the
one who may have heard of it “in a broader sense”, no teacher or aide was familiar with the
syndrome. An aide thought staff would be interested to know more about the disability and
suggested that an in-service program would be one way since advisors come to talk about
disabilities that cause behavioural problems. The following discussion reflects on teacher
and aide perceptions of a student who has been diagnosed with an NLD, an Executive

193
Function Disorder and whose intellectual functioning was within the borderline range. Prior
to this study, there appeared to have been no formal assessment of the extent of Mel’s
intellectual and functional impairments.
“I wouldn’t say she makes close friends. She doesn’t seem to do well in
that area … I think that probably as an adult in a more adult environment she’ll
probably find that her sense of humour and things that she likes are probably
more adult” (U.28-HEcT-211). Mel was described by teaching staff as mature, old for her
years, speaks like an adult and if open enough to make a lot of friends, may find it difficult to
find someone who’s really at her level (U.2-PTT-4; U.28-ET-188-196; U.14-TA-128; U.5-
HEcT-44). These descriptors create impression of a student who functions beyond their
chronological age but in terms of clinical assessment, Mel’s expressive language skills were
assessed in the low-below average range, age equivalent 11 years 11 months, 3 years below
her chronological age (Communication Assessment Report, 2005, p.3). Mel speaks like an
adult, she has a wide-ranging vocabulary and her spelling and reading age equivalent was 19
years yet her Communication Assessment Report states “there is much in her world that she
doesn’t comprehend fully” and “there is much in communicating her ideas that she finds
difficult” (2005, p.2).
The misperception generated by Mel’s verbal competence is borne out in the above
quotation. Maybe teachers and parents do not recognise that mature speech and poor
nonverbal skills create a paradox. Mel needed help to interpret word problems yet she gave
excellent orals and used big words, which adds credence to the Rourke and Tsatsanis (1996)
claim that “linguistic functioning is an integral component of the NLD syndrome both as an
area of significant strength and weakness” (p.39). Children with an NLD can speak like an
adult. They may have pockets of knowledge in specific interest areas which also impress but
they have trouble transferring or adapting this knowledge to a new task or situation.
Nonverbal learning disorders routinely go unrecognised because parents and educators alike
consider language-based skills an indication of ability to learn (Thompson, 1997).
Misperception of ability leads to unrealistic demands by parents and teachers and inability to
meet expectations may lead to unfair criticism over the long school experience and increase
the risk of depression. It is important for parents and teachers to understand that their
difficulties are genuine. They have a neurological basis and verbal skills and vocabulary are
well-developed because the child has unimpaired access to that part of the brain.

194
If teachers, parents and guidance officers are not aware of this learning profile in the
early years so that assessment can be advised, consequences post-school can be gloomy.
Failure to recognise and diagnose an NLD may cause labelling and low self-esteem and will
likely manifest as an internalised problem as hopes, dreams and ambitions nurtured by home
and school are not realised. At the time of interview, Mel was seeing two counsellors. She
talked about difficulty handling the social side of life and friendships. The mother said there
had been no invitations to parties in high school. The weekends get very lonely for these
children for they constantly compare their achievements and social calendar to those of their
peers.
“I couldn’t treat her any differently to anyone else so she would get an
administration detention which is manned by the deputy and in the 45 minute
detention in their lunch taking up their whole lunchtime ... Usually in 20 minutes
if they race, they could get it done but no they choose not to come and they’d
get an administration detention which would be recorded on their file
permanently (U.13contd-ET-66). I felt this teacher believed that Mel could do the spelling
homework. She did not realise how intensely arduous the handwriting task can be for a child
with spina bifida and hydrocephalus. Mel has “plenty of brains, plenty of ability” but there
was “overcompensation somewhere along the way” (U.13contd-ET-66). This teacher gave
up her lunchtimes to supervise students who had come to do spelling homework because this
would teach them something about “meeting a deadline, making a commitment and doing
the right thing” (U.15-ET-74). Her intentions were honourable for a typical student but not
for a child with NLD. Punitive punishment will “destroy this child’s sense of hope and make
her feel she is a bad person if she is unable to follow through” says Thompson (1997, p.113).
Mel would not have been able to “race” through the spelling homework in 20 minutes
like other students. Almost every teacher and aide reported very slow, laborious, scratchy,
messy and sometimes illegible writing. Mel and her mother said handwriting was difficult
(U.6-P-28; U.11-S-74). She struggles with handwriting because the task is complex. The
word must be visually located on the sheet, held in working memory then recalled and
physically transferred to paper. This complex physical process involves much concentration
and effort which is often taken-for-granted especially if the person speaks well. Such
complexity may cause Mel to sit staring at the paper or drift into her own world because
starting is too hard. Mel’s copy of a geometric design was assessed in the severely impaired
195
range. She meets the criteria for an NLD and teachers need to understand that her
difficulties have a neurological basis. They are not a form of defiance or laziness.
“I think she’s used to having people, other people organise her and other
people think for her and I think that at her stage in life, she needs probably to
take on some responsibility there for that” (U.21-ET-118). Three teachers, three
aides and the parent reported problems with planning, organisation and time management
(U.11-TA-62; U.9-ST-86; U.13-TA-64-6; U.18-HEcT-163, 223; U.12-TA-109-10; U.21-ET-
118-126; U.2-P-6). Children with an NLD have trouble with abstract or non-tangible
concepts such as time management and getting organised to finish a task within a timeframe.
It may be difficult to break down a large assignment into component parts and even if
sections are attempted with step-by-step instruction, it may be difficult to pull out the focal
points of each section to write a conclusion as may have been the case when the aide asked
Mel to write a conclusion. Testing revealed that Mel experiences great difficulty in most
areas of nonverbal learning, any task which involves an organisational component, motor co-
ordination and tasks that involve visual awareness of the happenings and environment
around her. Visual imagery and memory are also necessary for effective planning and
organisation since they allow one to acquire the whole picture then mentally dissect and
reorganise parts in relation to the whole. Limited exploratory behaviour as a youngster
would no doubt compromise such skills needed for effective hypothesis-testing, decision-
making and problem solving. All of these areas are difficult for Mel. I would suggest the
mother would like nothing more than for Mel to be well-organised, unforgetful and
discerning about the duration of time at nearly 15 years of age. Acquisition of such daily
living skills is paramount in the minds of parents who are acutely aware of their own
mortality.
Group work “she sits back. She’s not keen on it. She would much much
prefer to do it herself. She gets frustrated …” “She can come across as a
little bit bossy and “other kids may think of her as rude” (U.26-HEcT-207; U.14-
PTT-8, 28; U.21-TA-206). Mel does not take the initiative to put herself into a group (U.26-
HEcT-207; U.14-ST-129; U.17-DT-26, 74, 84). Some teachers thought this was because she
was quite mature and got bored with immature behaviour from boys or got annoyed when
members became unfocused (U.27-ET-188; U.5-DT-16). When asked to pair up, Mel would
choose to work alone, with an aide or with another special needs student rather than with
other students. One difficulty for Mel is keeping abreast with verbal exchanges within the

196
group and if running at rapid rate, she would “retreat not physically but presence wise”
(U.15-P-152-6). This could be Mel’s rationale for trying to keep students focused, so she
could hang onto the threads of conversation. It may have been difficult to mentally reorient
to quick changes of topic and integrate underlying meanings, humour and sarcasm. Failure
to comprehend the full picture may result in an inappropriate verbal response and/or
nonverbal reaction which may render her vulnerable to peer ridicule. At times of
withdrawal, she may roll her eyes or appear distant. These involuntary behaviours may
reflect difficulty with processing a myriad of social cues. There is no intention to be “rude”
or “blunt” and if an inappropriate verbal response is offered, it will likely be one learned and
used previously but not adapted to the new situation and its dynamics.
“But she eats things like donuts at ¼ past 8 in the morning. So I talked to
her about eating healthy food for herself and she was tucking into a donut”
(U.23-TA-112). There could be two reasons why Mel eats her breakfast when she gets to
school. Firstly, poor organisation and time management problems in the morning means she
may not have time for breakfast before getting picked up at 7.50 a.m. Secondly, if she has
the Arnold Chiari 11 malformation, difficulties with swallowing may reflect a preference for
predictable soft textured foods like donuts.
“Anyone who can sit there and give the sort of two oral presentation that
she gave to me, the language that she used … the kids were right, it was quite
sophisticated language and it said to me here’s someone who’s quite bright but
not showing her true potential for whatever reason” (U.19-ET-92). The teachers
and aides who were privy to Mel’s oral presentations and script learning abilities were in
unique positions to commend her verbal skills and sophisticated language. On this basis,
Mel was often described as “a smart girl”, “mature”, “quite bright”, is “very precise in her
choice of language and is a good conversationalist”, “a lot more capable than we saw”, “has
plenty of brains, plenty of ability” … (U.16-ET-78-86; U.6-DT-18, 110; U.27-DT-132; U.5-
TA-24; U.4-TA-8-10; U.5-TA-24(edited). Mel herself spoke of trouble with the social side
of life yet to listen to her speak, one does not suspect difficulty with any form of
communication. Demonstrated verbal skills convey competence. They lead to unrealistic
expectations on the part of parents and teachers. It is interpretation of the nonverbal aspects
of communication and inability to grasp the whole picture within the context of a social
setting that are difficult. One aide said Mel could understand group interaction with the
special needs students yet the speech and vocabulary skills of these students may be inferior

197
to Mel’s. Compromised ability to interpret the nonverbal aspects of communication may be
compounded by misinterpretation of text (U.27-TA-170). The following perception shores
up the misunderstanding generated by Mel’s language skills “my belief is she’s a little bit
pampered and a bit mollycoddled and I don’t think people are … because she’s in a
wheelchair … I don’t think she’s being pushed the way she should be ‘cause as I keep saying
I think she’s really quite capable” (U.18-ET-88-92).
Chopping … ”she was very slow but she manages in the end but not in the
timeframe” “ I mean there’s a lot of gnashing of teeth and time and stress
involved with it but once again, her nature of ‘ah, it’ll be right’ is good but it can
be frustrating (U.4contd-TA-14; U.13-HEcT-123). The parent completed a questionnaire
that assessed Mel’s adaptive living skills. Her overall performance was scored in the
severely impaired range for a girl her age and her ability to process information was also in
the severely impaired range. Assessment of Mel’s tactile perception was within the normal
range but when a speed component was added, she has great difficulty. Results confirmed
she will have difficulty undertaking most tasks which involve a component of speed.
Deficient psychomotor functioning, information processing and visual-spatial skills will
have negative effects on self-help skills and will also impede decision-making and problem
solving abilities.
Conclusion
Mornings were difficult and rushed because Mel does not realise she has to get ready
within a timeframe. In the context of school, good verbal skills, excellent vocabulary and
spelling co-exist with poor handwriting and poor planning, organisation and time
management skills. Completing homework was difficult and she needed constant prompting
with every new task. Basic maths was manageable but she needed help to interpret problem
solving maths. Concentration, memory, decision-making were not good and fine motor tasks
were slow. Mel had trouble with the social side of school, she did not have a special friend
and she found group work difficult but she would group with SEU students.
Ability to adapt learned behaviours to new and complex learning requirements is the
“raison d être” of brain-behaviour development and “deficiencies in adaptability are
essentially, deficiencies in learning” says Rourke (2002, p.162). From a psychological
perspective, Rourke says the “rather devastating set of learning problems experienced by the

198
person who exhibits an NLD are among the very worst that can be imagined from a
psychological perspective. The social and vocational incompetence, the withdrawal, the
psychic pain are all terminal adaptive manifestations of learning failures. These are all
manifestations of the fact that ‘talk is very cheap’ when compared to the richness of adaptive
learning’. At the very least, talk is no substitute for learning” (p.162). If teachers and
parents remain uninformed about the extent and significance of NLD deficiencies, it will
confirm the Rourke, Young, Strang and Russell (1986) hypothesis that the needs of these
students are not “well understood by those who are in the best position to shape and enhance
their development, thus rendering such children at further risk for serious adult adjustment
difficulties” (p.237).

199
JOSIE’S CASE STUDY
Context of Josie
Family life
Josie is a Year 11 student at a state high school in southern Queensland which has an
enrolment of about 230 students. She was born with thoracic myelomeningocele (T.5) and
uses a wheelchair because she is paralysed below the waist. Associated hydrocephalus
required placement of a ventriculoperitoneal (VP) shunt soon after birth. To date Josie has
not been afflicted with a seizure disorder. She lives with her mother, father and younger
brother and her both parents work.
The mother said that at age 11 years, Josie had had an operation for every year of her
life. She shared some effects of Josie’s surgery on the family, in particular two stages of
major surgery undertaken by Josie in Year 6 to insert rods into her back to arrest scoliosis
and to fuse vertebrae. Doctors advised there was a chance that Josie “could not make it
through theatre because when they were doing the rods or fusion, there was a chance that she
could haemorrhage”. She was hospitalised for 2 weeks and her younger brother was cared
for by relatives. For the 2-week period Josie was in hospital she had to lay totally flat on her
back and eat and drink while lying down. There was to be no rotation of the spine for a 3
month period after discharge which meant a 2-person lift in and out of the wheelchair, in and
out of the car and in and out of the bed. “Nothing prepared us for this. It was one of our
worst experiences” said the mother. “We’ve been through some operations with Josie but
there wasn’t the education for parents” (P-255). On one occasion, the father said he’d rather
have his two arms amputated if he could just prevent Josie from these major bouts of
surgery. On return home from the major back surgery, severe stress caused hospitalisation
for the father.
The school has no Special Education Unit but it employs a Learning Support Teacher, a
Special Needs Teacher and two teacher aides. Academic and vocational subjects are
available to students and the school adopts a very strong approach towards Josie’s
wheelchair and independence (U.2-retnd by post). Josie has been classified as Level 5
Physical Impairment (PI 5) and the mother said she receives support in most classes. Josie
has chosen fewer electives than other students so that spares through the day allow her to
focus on life skills, kitchen skills and other areas of observed difficulty. A normal day
therefore comprises a mixture of core classes where Josie is supported by a teacher aide and
200
withdrawal lessons which focus on life skills with teacher or aide support. At 11.20 a.m.
each day, the nurse comes to assist with toileting procedures.
The mother confirmed that Josie speaks “very clearly but does not always understand
and doesn’t have recall of what she’s told people”. Josie relates better to adults and the
mother believes this stems from toddler days when she spent a lot of time growing up with
adults and did not learn interaction skills. Handwriting was considered “bad” and she would
have difficulty writing an A-4 page. Maths is a struggle and she has no comprehension of
the duration of time or judging distance when crossing the road. Concentration was “poor”
and depended on whether the topic was an area of interest. Short-term memory was also
“poor” though long-term memory was not a problem. Completing school and homework
tasks required supervision and constant prompting to remain on task and Josie had difficulty
remembering what was taught in class when doing homework. Some everyday tasks such as
buttoning and zips were do-able and Josie could dress and undress herself from the wait
upwards. Her mother mentioned the need to lay Josie on the bed to dress her for a recent
function and this may be an everyday occurrence given her condition. She was not good at
hand sewing and would find sewing on a button difficult. On the whole, the mother reported
that educational experiences in high school for Josie were difficult due to frequent changes
in both subjects and teachers.
The mother expressed strong “frustration dealing with teachers. Society hasn’t changed
… the frustration with school is exclusion not inclusion”. She feels Josie “suffers in silence”
because she is not able to verbally confront anybody. People don’t see her daughter as Josie
“but only see the wheelchair”. Who should and should not push the wheelchair became a
contentious issue which caused the mother to write a letter to all school staff requesting that
staff push Josie on carpet or grass. A girl once offered to help Josie in the classroom and
“one of the teacher aides just doesn’t politely say anything just goes off at her saying ‘Josie’s
meant to get over it herself, you’re not meant to be helping her’”. The mother tried pushing
Josie over the carpet and she found it difficult to direct the chair. “It seems to be off course
and it takes a lot to get through” and she was unsure whether the nylon reacts to the rubber
wheels (U.4-P¹-S-P²-116). “Independence has got her nowhere only loneliness and
heartache” said the mother. Lack of friends and ability to socialise were causing increasing
anxiety and the mother reports that friends are now 200% more important to Josie than
independence. At the start of that year she had “been back at school 5 days and has seen the
chaplain every day”. Despite the mother’s best efforts to advocate for Josie, the mother
believes teachers consider she is only the parent who wouldn’t know anything yet the mother
is the one confronted with Josie’s “sadness, unhappiness and the hard time she has accepting

201
her disability”. As well she has to answer questions about why Josie has no friends and
whether she will ever get a boyfriend.
Past school experiences
Every year that Josie had a new teacher in primary school, the mother would “have to
sit and go through everything, the medical history and the learning difficulties”. The mother
believed that primary school teachers would have advance knowledge of class composition
and if aware that Josie was in their class and that she depended on a wheelchair for mobility,
they would think “is there anything else I need to do, is there anything I need to know?”
There was “no continuity or communication from one year level to the next” said the parent
(U.14-P¹-S-P²-339). Many issues had involved young 1st year teachers. Because Josie “has
a stoma on for the bladder”, a local nurse would come to the particular class to assist with the
toileting procedure and “Josie used to just leave her class”, as Josie said “‘cause I knew what
was going on”. She would be gone for 5-10 minutes and would then return to class. The
mother spoke about the nurse’s visit with the class teacher who said ‘what … well I’ve often
wondered. This woman comes to the door, Josie just sees her and she goes out and then
Josie comes back about 10 minutes later’. The mother replied “well darling haven’t you ever
questioned what is going on like is it normal that students just leave the classroom with this
stranger” and she explained that this was the nurse who had come to help with toileting.
“But I think that came about because they don’t read the student’s file when they have the
student-free days” (U.14-P¹-S-P²-526-527).
“We ran into lots of issues of bad planning” said the mother. In Grade 2, Josie was sent
to back to collect textas from a classroom in the 150 year-old school building. To access the
classroom, she had to use a pull-chain to unlock the main double door. Unable to reach the
pull-chain to access the room and textas, Josie was given a detention. “But this is an
example of Josie having to do something by herself and at that time she didn’t have that skill
to work by herself and just not planning things properly” said the parent (U.14-P¹-S-P²-534).
Another time Josie had to do French in an upstairs classroom. The school eventually secured
a stair-walker from Education Queensland “and the only way Josie could get up was if she
had someone to operate it for her” once it was retrieved from a storage room. Josie was late
for a French class and received a detention. At the time, Josie was struggling with maths and
the mother asked if Josie could “do a bit more research on maths or read or something else
that’s going to be more beneficial” since she believed Josie would never use French post-
school but French was in the curriculum and French had to be done. “But you eventually
pulled me out of French” said Josie (U.2-P¹-S-P²-51-54).

202
One task required students to pick a country they would like to visit. With aide support,
Josie wrote in beautiful handwriting ‘One day I’d like to go and visit America and I’d like to
go to Disneyland …’ She had written half of the story and the teacher aide left Josie to
finish it. “Well she didn’t know what to do so she just wrote ‘and I’d like to see more and
more and more and more and more and more and more and more and more … things’”. The
draft had to be converted to good copy at home. “We sat up until about 9 or 10 o’clock that
night and Josie was doing her beautifulest handwriting and that bitch in the morning didn’t
even look at Josie’s. She was so proud that she’d done it and completed it” (U.14-P¹-S-P²-
621-637). At this point the father said “teachers don’t realise and you can’t really blame
them I suppose of what is actually involved over these sorts of kids you know, there hasn’t
been the training” (U.14-P¹-S-P²-653)
Early in Year 7, a teacher asked “what’s happening with the Year 7 camp because we
start planning it now for July”. The mother said “well you need 2 things. You need to get a
car ‘cause Josie can … ‘no’ said the teacher ‘I’m talking about the camp’. Oh yes well I’d
like Josie to go on the camp and about 3 weeks later the teacher said to me ‘Oh, we booked
the bus after we realised that Josie was going’ and I went ‘Oh, that’s alright’”. I was very
calm. “‘That’s alright all you need to do is get a car because when we go away we go in our
car and Josie can transfer in and out of a car, we don’t have a bus”. For many months “there
was always an obstacle and I just dig my heels in and I thought ‘nu she’s going on camp’”.
The mother said if funding was an issue, she could raise money through the Service Clubs …
‘Oh no no no no funding’s not an issue’ then “this stupid OT and Phsyio came” to try doing
a 2-person island lift to get Josie into the bus and then expected her to bottom-lift up the aisle
and be lifted onto the seat. “This is crazy” said the mother “you could visit two or three
places a day in Brisbane and you’d have 4-8 lifts a day. ‘What about the steps’ they said and
I went ‘no you’re going to have 30 other kids tripping up and down these steps with either
dog poo on their shoes or chewing gum and then you expect my daughter to have to lift. It
was basically like putting a dog in the back of a ute’” said the mother. She then sought a
third party to represent herself and Josie at the next meeting with the Principal. The
Principal phoned the following day and said “Oh, we’ve got a car” and she replied “That’s
all you had to do from the beginning”. Josie went on camp to Brisbane and had wonderful
time with the rest of the school. “It’s poor organisation and poor communication” said the
mother and since Josie was a pupil from pre-school to Year 7, the school had 8 years to plan
for the camp (U.14-P¹-S-P²-537-546).
At the end of Year 7, Josie’s mother presented a “little seminar” at the high school for
the prospective Year 8 staff. A handbook from the Spina Bifida Association was used to

203
describe in detail the sections relevant to Josie’s form of spina bifida … “didn’t even bother
to listen basically” said Josie. The mother offered to answer questions and considered this
an important information-sharing forum. The handbook was left at the school for staff
reference (P¹-S-216). “If you’re a teacher and you have a student in your class with a
disability you’d also start seeing some issues with that student wouldn’t you. You would be
able to look and say ‘Oh, they haven’t done much work today’ so wouldn’t you think that
you would sort of research yourself on this student’s condition and find out what it’s about”
said the mother (P¹-220).
When the mother visited the Year 10 maths teacher to discuss Josie’s trouble with
algebra, the teacher said “but Josie we went through this, we’ve been working on this for the
last two weeks. We did it this morning”. The mother spoke about Josie’s short-term
memory and recall problems and said “‘what was taught at 9 o’clock this morning, she’s not
going to recall or remember any of that sometimes or when she gets home at 3 o’clock’ and
trying to get that through to those teachers that have her for those subjects” (U.14-P¹-S-P²-
726). One Year 11 assignment was to design a menu and work out the exact cost per slice of
the end product. “It was very in-depth for Josie to follow and understand” said the parent.
She spoke of lack of teacher understanding when one day Josie arrived late at school and had
forgotten to bring her cooking. The repair of wheelchair tyres made Josie late and she had
forgotten cooking ingredients so the teacher said she would have to do “baby Grade 8 Find-
a-Word work instead” (U.3-retnd by post-M-6).
The researcher spoke about a need for raised awareness of the effect of hydrocephalus
on learning and daily life which is sometimes camouflaged by good verbal skills. Mobility
problems can be obvious but the effects of hydrocephalus are quite subtle, sort of hidden.
Josie said “yeah … how do they expect me to go around every new teacher and point out that
I’ve got a shunt. I’m sick of doing that … I’ve done that since Grade 1” (P¹-S-227-229).
The mother and researcher agreed that since the shunting system to control hydrocephalus is
concealed, the casual observer sees Josie as having a physical disability only. People are not
aware of the shunt and the mother reiterated that one study goal here is to highlight the
effects of hydrocephalus on learning and everyday life and Josie added “the fact that it’s
basically two disabilities” (P¹-S-252).

204
A day in the life of Josie based on Josie and her parents’ reports
Getting ready for school
A normal day for Josie means “I sort of do the normal things that people do like get up,
get everything ready for school and there are a couple of things that I may need help with
due to my spina bifida which are things like getting dressed” (U.1-S-2). During the school
week, her mother said there is a lot of rushing because Josie does not have a good concept of
time. She can tell the time but she has no idea of the length of time. “Most school days I’m
always prodding … quick hurry up, have you eaten your breakfast up … after you do that
you’ve got to do this and that … (U.1-P-2). Strategies used to improve Josie’s concept of
time include using the egg-timer, the mother making her own clock with 5-past, 10-past the
hour and explaining “if you’ve lost ½ an hour of this lesson, that’s the time it takes you to
watch Home and Away, ads and all, and that duration of time is equivalent to what you have
lost from your lesson (U.1-P-37). Josie is sometimes aware of punctuality which leads the
mother to think she will improve as she matures. The worst days are school days “I just hate
school mornings” said the mother (U.1-P-53).
Even though Josie is nearly 16, the mother is still doing a lot of things that she thought
Josie should be doing herself, “I think she still needs for me to do them … at least I can get
her to school a bit earlier or on time” (U.1-P-6). It took “a hell of a lot of years of every
morning ‘you have to do your teeth, face and hair’” before she could remember those tasks
(U.8-P-307). We had a checklist stuck on the table that she would tick off as she completed
jobs and it was “repetitive for quite a few years before it became set in here”. When in the
bathroom for a prolonged period, the mother would enter and “she’d be just looking around,
looking in the mirror … ‘Josie you’re supposed to be brushing your teeth’”. The mother gets
frustrated because she knows that if Josie goes to the bathroom to do her teeth “that’s what
you do and it’s not only her teeth that’s got to be done but she’s got hair to do and her face to
do and she’s like ‘I’ve got to finish putting my socks and shoes on ‘cause I haven’t done
that’”. And if her teeth are not well cleaned, we have an argument about that” (U.8-P-309).
Television is forbidden in the morning because it “slows you down” and the children are
asked to get books, timetable and tuckshop order packed the night before. Josie’s brother
has been diagnosed with ADHD so he also benefits from a routine but as in any household,
uncontrollable interruptions may cause delay.

205
Going to school
The family lives close to the school. Josie could wheel herself along the cement path
but the mother prefers to drive or push her each day. “The concept of time does not worry
Josie. If she sees someone along the road, she’ll stop and talk. She will wave to someone
and when asked who that was she’ll say “Oh, I don’t know I was just being polite”.
Although aware of Stranger Danger, the mother feels that if sent to school independently,
Josie would dilly-dally along the way. One day she got to school by 9.15 a.m. and the
mother said it was because “I was like power-walking … ‘Mum why don’t you slow down’
and it’s like Josie you’re arriving at 9.15 and you’ve missed ½ an hour of a lesson and it’s
that understanding of ‘Oh well, what’s ½ an hour’. Half an hour to Josie could be 10
minutes or it could be 3 hours” (U.1-P-8).
Coming home, homework and assignments
No television or Sony games are allowed after school until homework is done (U.1-P-
105). This year is a lot different because Josie has not had homework or at-home
assignments from any of her subjects “so we’ve been pretty relaxed in that area” said the
mother (U.1-P-2). She has never ever been able to go in and just do her maths homework or
work on assignments “she’s never ever worked on and completed a full assignment by
herself. It’s always had input with me” (U.8-P-307).
Loneliness and friendships
A recent bullying incident by Year 8 students caused Josie “to get very very upset …
‘O Josie another student wants his car back, hand us over your wheelie’. They implied Josie
was stealing another student’s car which was the wheelchair and Josie was quite offended
and upset by it which wasn’t good”. Four girls took Josie to the teacher who talked her
through it. “You’re a lot older and mature, don’t take it to heart” and the teacher felt Josie
was an easy target. Josie regained her composure “then I went and yelled at the other kids”
said the teacher (U.16-LST-207). Josie felt these students took advantage of her having
spina bifida and being in a wheelchair. “They make really cruel jokes about it like they seem
to think my wheelchair’s a car and it was a Year 9 student who came and said ‘I want my car
back’. Josie said she was not good with “smart comebacks” and her mother said that
sometimes kids aim to upset her and “when they’ve done that they just walk away” (U.1-S-8,
19). “Generally outside of me it’s alright yeah … school’s yeah I’m enjoying it” said Josie
and her mother added “this year” (U.1-S-22). Josie said to the researcher “I’m just sick of
my disability, like it’s in charge of my life like … do you know what I mean?” (P¹-197).

206
“You can get a really good teacher or teacher aide who is compassionate and
understanding or a terrible one” said the parent “I think it comes back to continuity of
communication ... every student and staff member at that school should be on the same
wavelength about Josie regardless of whether they have her in their classroom or not or
whether they only just see her in the tuckshop area. They should all be aware of her physical
disability, what it incurs, what it means. If they see her sitting by herself … stop … find out
if something … One year a teacher did stop and said ‘haven’t you got any friends to go and
sit with Josie’ and that was the truth. Josie didn’t have any friends to go and sit with because
she couldn’t get to where they were but that comes down again to ‘is there somewhere you
want to go Josie … can we help you’”. That is never offered. As I was saying, in the
classroom I think it just comes down to the teacher aides though, the person themselves …”
The mother suggested sitting at eye level so the person in a wheelchair so they do not “feel
they’re being towered over by someone”. “But those teachers they all do that to me, they
think they’re better than everyone else” said Josie (U.20-P¹-S-P²-817-834). “They don’t stop
and think … they’re not aware”. Overall the mother believed there was a very poor lack of
communication. “It’s never going to change” said Josie (U.20-P¹-S-P²-834).
When asked about group work at school, Josie said “well I find it a bit tricky to answer
because I don’t get to interact that well like I don’t get to socialise like at lunchtime. I don’t
get to hang out with people so I just presume that because I don’t get to hang out with them
they won’t want me to work with them” (U.24-P¹-S-P²-944-946). The mother believed
group work was difficult and it was best if the teacher just put Josie into a group (U.24-P¹-S-
P²-949).
Tasks that Josie enjoys
Josie “adores” animals and she has two dogs and three pet birds. She handles
Calligraphy well “I love that ‘cause it’s practical stuff, yeah no homework again” said Josie
(U.13-P¹-S-515). She finds maths “pretty easy because the teacher that I’ve got this year
doesn’t believe in things like algebra … doesn’t believe in teaching that, no homework, no
assignments” (U.13-P¹-S-P²-509) and the mother said for the first time in many years, Josie
was enjoying maths which was wonderful to hear (U.13-P¹-S-P²-512). English has always
been a favourite class subject and this year’s teacher is another that “doesn’t believe in
giving homework” (U.13-P¹-S-P²-515).

207
Strengths reported by mother
Her strengths are her wonderful happy personality and caring nature and her love for
music and the mother thought singing lessons could help Josie if she had the right teacher
(U.5-retnd by post-P-11).
Tasks that Josie finds difficult
Learning algebra in Year 10 was very complicated and Josie reported her mother saying
“they still have to shove it down our throats … she will never use algebra or coordinates”
(U.2-P¹-S-P²-24). Her mother repeatedly wrote notes saying “sorry, Josie didn’t do her
homework last night because she didn’t understand it” until one day the teacher said to Josie
“I don’t think it’s you don’t understand it, I just think you’re lazy”. The mother “spurred up
‘cause she doesn’t understand it, I don’t even understand it, her father doesn’t even
understand it. We’re adults, we’re highly educated and I don’t even understand algebra so I
went and met with her and said ‘why does she have to do it?’” (U.2-P¹-S-P²-25-27). The
mother believed Josie would have no use for algebra in her post-school career but “it was
easy to teach that because it was part of the Year 10 curriculum. It was easier to do that than
write a whole new program for Josie. “Stuff this, can’t do it so just … couldn’t do lots” said
Josie. Year 10 algebra tasks were later modified for Josie.
On one occasion, a maths class was given a “very in-depth assignment” which
comprised three sections on Statistics, Chance, Data and Measurement. The Statistics
portion required students to record on bar, pie and line graphs each player’s height, weight,
number of games played and the games lost by Queensland and New South Wales football
teams (U.2-P¹-S-P²-37). The Chance and Data part required students to estimate how many
times a 20c piece would need to be rolled to get a heads or tail result and the final
Measurement portion asked “how many wheat trucks would you need to use to cart x tonnes
of wheat from A to B then design a bloody fuel tank and use a dipstick to measure the depth
of fuel. I thought ‘this is just ridiculous’. It was just so way over Josie’s head” (U.2-P¹-S-
P²-39-41). The assignment was handed in with a notation from the mother “Josie found this
assignment very very difficult. We’ve only completed one type of chart or graph because it
was just so in-depth” and the teacher accepted that. “Thank God” said Josie (U.2-P¹-S-P²-
47-50).
Josie and her mum spoke unanimously about her difficulty copying from the board
(U.15-P¹-S-P²-878) and a lack of allowance for this. “She would have difficulty writing a lot
of stuff off the board” and the mother offered hints that would help Josie (U.15-P¹-S-P²-584).
Irregular aide support in upper primary and junior high school meant homework instructions

208
were often incomplete because the board had been wiped. One aide would scan blackboard
notes from class discussions and categorise as relevant or irrelevant for Josie to scribe or she
would copy and paste notes from another student’s book into Josie’s book (U.15-P¹-S-P²-
592). Another aide copied blackboard notes herself and sent them home with a request
“copy my notes into your book”. “This is crap” said the mother “why can’t I just stick in the
notes she’s written on a piece of paper in Josie’s book” which the mother did (U.15-P¹-S-P²-
605). Josie cannot process too many instructions at one time … “one instruction is a lot”
(U.8-P-303). In the morning, she tends to get flustered and very panicky if asked to eat
breakfast then do her teeth. “I find it difficult to process what I’ve got to do. It’s annoying.
That stuff’s really upsetting for me because that’s what causes me to get into trouble all the
time” said Josie (U.21-P¹-S-P²-925). New situations sometimes cause her to become very
stressed and confused and she then “finds it hard to ask for directions or assistance” said the
mother (U.9-P-8).
The mother spoke about organisation and short-term memory problems especially if
she’s been given a message at school “it’s like ‘why can’t I remember’ well who was it, was
it a boy or a girl ‘I can’t remember’ well did she have long hair or short hair ‘I can’t
remember’ which is frustrating for her and upsetting and it’s no good for me because it
might have been something that I needed to know” (U.9-P-314). To save Josie undoing her
schoolbag to find her diary, the mother attached a small notepad to a keychain worn around
the neck where Josie could jot important messages (U.9-P-328). It takes up to fourth term to
learn her class timetable and she finds any change difficult to remember. The mother
invented a “mini-timetable” worn around the neck on a keychain. It comprises five
laminated colour-coded cards that face inwards “so the rest of the school kids don’t see that
it is totally Josie’s timetable” (U.9-P-336). Each displays class period and time, name of
class, teacher name and room number. Lunch breaks and spares are also noted. “It’s good,
she wouldn’t survive without it because it probably takes her 6 months to learn her timetable
by heart and probably once a term her timetable could change so that means she’s got to
learn it all over again”. It’s been a “life-saver” said the mother (U.9-P-340).
Post School
Post school the mother hopes Josie will either further her schooling with TAFE,
university or obtain a traineeship in office administration or in a veterinary practice (U.5-
retnd by post-P-13). If the family stay in their present location, they have discussed a
business whereby the family makes cages level height with Josie for her to breed budgies
and supply a pet shop. Post school, the mother does not want Josie to stay at home without a
purpose (U.5-P-157).

209
Advice for parents
The mother advised parents to be strong advocates for their child “especially with the
education system as they do not seem to fully understand the hidden problems associated
with spina bifida. Parents should ask “if my child didn’t have a disability what would their
choices be”? If the choices are different to those presently available to the child, “ask
yourself why they are different” (U.7-M-retnd by post). Josie concluded by sharing “some
really good ideas I’ve come up with to have fun in my life … in my school life. Um actually
I still haven’t got around to doing it yet. I’ve got the Principal’s permission for it but I’m
thinking of starting my own cheer-leading squad … just haven’t got around to doing it yet”
(U.20-P¹-S-P²-970).
Have you heard of a Nonverbal Learning Disability?
The mother thought she had heard of the NLD syndrome through the Royal Children’s
Hospital and the Spina Bifida Association (U.8-retnd by post-14). Josie said she had never
heard about the syndrome (U.18- P¹-S-P²-745).
Josie at school based on teacher and teacher aide reports
Late arrival at school
A variable arrival time at school was offered to Josie but whatever the day, she is often
late. Even when timetabled not to be at school for the first 35-70 minutes, “she’s still usually
late for the next thing … there’s pretty much not a day that she’s not late for school” though
occasionally she does have accidents that cause her to be late (TIC:SD-4; TA-2; U.12-
TIC:SD-89). She could be 30-45 minutes late for the first scheduled lesson or she could
miss the whole lesson (TA-328; MT-4) so “I don’t think that that’s kind of a big priority”
(U.12-TIC:SD-93). Coming late to school is a big issue because Josie misses daily Care
Group meetings where notices about room changes, rehearsals and meetings are announced
prior to the first class. Non-attendance means this vital link is missed as well as the
camaraderie generated from vertical grouping (TA-312). On days when Josie is timetabled
to come late, the teacher aide usually scribes relevant notices for her (TA-328). If on time
on other days, Josie could jot down relevant notices “but she’s not and this sort of thing is
going to be breaking down the social interaction and leave her feeling as though she’s not
part of the school” (TA-332).
210
Loneliness and friendships
A concern frequently expressed was loneliness, trouble with making friends and Josie’s
relationship with the other students. “She really really wants and longs for someone really
close in friendship but doesn’t really have someone” (AT-36). Ability to function socially
with peers was a critical matter and the mother had written a letter to the school “and made it
an issue” (MT-20-24). Since she is not a very outgoing person, she is a bit of a target for
bullying which is unfortunate (MT-26; U.16-LST-207). It was really difficult to foresee a
pattern with her forming relationships because one day she would be sitting with a group of
peers but another day would have nobody around her. She did not seem to have strong
friendships and one teacher wondered whether these students were “putting up with her for
the day”. There seem to be more and more days when Josie is by herself “and that’s where I
can see the gap widening between their cognitive ability and hers as well as their different
levels of social development” (MT-80).
If alone “she’s almost like talking to herself. It’s probably more lips moving and sort of
a sound but there’s nobody else around … almost like she’s having a conversation with
somebody but there’s nobody there” (U.1-PAT-10). “I don’t know who it’s to, to an
imaginary friend I’m not sure …” but this does not happen in class because she’s not alone
in class (MT-20-24). Being a teenage girl going through puberty in high school and the fact
that she “really stands out so much more in a wheelchair and I think that’s her coping
strategy but I don’t know”. A bullying strategy was being implemented at the school and the
teacher felt that leaving Josie out was “an indirect form of bullying” (MT-26). When asked
if talking to herself was loud and whether it could be a form of stress relief, the teacher
replied “you can hear it if you’re walking past her. She’s not miming, she is actually
speaking. Yes, she looks tense. Yes, she looks uncomfortable” (MT-74).
An aide observed Josie was very depressed “sort of feeling as though she was going
against her disability. Up to now she has just accepted it but she now feels it is “really
getting in the road and I think she can understand the social problems that she’s having and
becoming much more aware of them” (U.2-TA-2). One day she found Josie in tears.
Students were allowed to shoot balls and the boys “just took it for granted that Josie couldn’t
shoot balls … well she can … but she got very upset because they gave the impression ‘Oh
well Josie won’t be interested in this, she can stay in the classroom with the teacher aide”.
By turning mad thoughts into glad thoughts, the aide helped Josie regain her composure
before they shared a shooting balls session (TA-6, 20).

211
She does a lot of sitting around in her wheelchair by herself and does not liaise well
with peers (U.1-MT-4). Pathways to other areas were reported but Josie chooses to sit in the
tuckshop area. She may expect people to come to her but she will not necessarily follow
them. Some Year 8 students were trying hard to socialise this year but some days she is
really tired and exhausted and “it’s been an effort to get through the day” (U.1-TA-8).
Because she is approaching sixteen “peers are moving to more adult-like pastimes like
drinking, boyfriends and Josie can’t relate to them” (U.1-MT-4). Lunchtimes are “probably
very lonely but she doesn’t always advocate for herself” (U.1-PAT-8). In Years 8, 9 and 10,
classmates would sit in a place she could access but now “they’re not doing that but I
personally don’t think that it’s much the fact that she can’t access them. Maybe they’re
going away ‘cause they know she can’t access them” (U.5-MT-110). Friends from previous
years who are fairly highly academically now spend lunchtimes doing virtual school or extra
work whereas the majority of students in the non-academic maths class for example have
behavioural problems “so in that class she’s with the really naughty drug-addicted and
sleeping-around kids swearing whereas Josie’s this nice girl who uses nice language has nice
manners and really doesn’t fit in with them. She’ll talk about her pets and talk about her
dolls and other 16 year-olds would say ‘I’m not interested in that at all’” (U.5-MT-114-124).
When peers speak with Josie she doesn’t appear very good at holding a conversation.
She lacks confidence and skill and “it’s very sad really because I think it’s her family and
herself that have held her back” (U.1-PAT-12). Some kids may talk to her for the wrong
reasons, trying to get a stir out of her and Josie may not recognise the difference between
who should and should not be ignored (U.1-PAT-12).
Most teachers did not think Josie had a special friend or buddy. “I could probably say
that one day a week she’s got company, she’s doing something, she’s got friends around her
but it’s certainly not every day” (U.28-MT-462). Sometimes she may be with a few different
students but no one on a regular basis or there might be one person for the moment then that
person will disappear and she will find someone else or be by herself (U.18-CST-116). A
small group of peers may seek her out but “I don’t think there’s any one person” (U.20-ET-
207). She had a group of friends in a present class “but they’re not what you’d call bosom
buddies … no I wouldn’t say she’s got one particular person that she’s really friendly with”
(U.30-PAT-398). She says she has certain people as friends but “at the same time she feels
very lonely and is concerned about friends” (U.25-TIC:SD-336). Access to other areas had
been discussed and Josie had practiced asking a peer to push her somewhere “but I don’t
think she’s used that yet … I think loneliness is a really big concern for her” said one teacher
(U.25-TIC:SD-336).

212
Strengths reported by teachers
Josie speaks very eloquently and her good conversational skills are one of her strengths
but these may be average if compared to every other 16 year-old in Queensland (U.17-MT-
335; U.31-MT-481). She can communicate though “she’s not overly articulate. She’s just a
very quiet person but will actively participate though not always with great enthusiasm”
(U.33-PAT-406). She loves her pets and gets most animated when talking about them or
becoming a vet or animal nurse (U.5-PAT-94). She loves being around family and friends
and being included and revels in the fact “that she gets her chance to have her say and to not
be alone” (U.6-MT-128). She is good at brainstorming and putting new ideas into words and
talking about them (U.26-AT-265) and her ability to memorise is a strength, especially in
Drama (U.26-AT-265). Rote memory skills tend to be good (U.16-MT-313). Josie is an
excellent speller and spelling has never been a problem (U.18-AT-171; U.15-TIC:SD-153;
U.20-TA-288). Her script-learning ability is also good. If other members in a group had
forgotten their lines, Josie “would always know everyone’s lines” (U.18-AT-173).
Computer tasks that allow freedom to integrate favourite interests were appealing (U.3-
CST-18). Hands-on art, craft and cooking tasks and a love of cultural activities like singing,
dancing, acting, drama and role play were easy tasks for Josie (U.4-LST-93; U.3-TIC:SD-
26). Speech and Drama provided a fertile milieu to hatch her script ideas (U.14-AT-145).
She displays enthusiasm, a very active imagination and is “good at improvising things” but is
a little hesitant about every new activity (U.3-AT-30). She likes writing short stories. Given
a topic, Josie has no trouble recalling an experience or movie she enjoyed. “She will get it
straight down, she’ll know exactly what she’s doing and I think she’ll actually sit there for a
while too and be reliving it in her mind before she’ll start writing”. Apart from a bit of
drama, role play and talking about her pets, Josie “doesn’t express any strong desire to do
things but she does express strong desires not to do things” said one teacher (U.3-TIC:SD-
26).
When asked to bring a packet pasta mix for lunch to prepare with the microwave, she
would turn up without anything (U.5-PAT-92). She enjoys IEP activities prepared by the
aide such as food shopping, counting money and telling the time. She likes taking part in
things that the other students do like the Cross-Country. This year she participated in the
same event as other students which was of utmost importance (U.8-TA-102, 110, 112, 114).
She hates feeling “no one’s thought about her and she’s been forgotten and just taken for
granted that she can’t attempt it or can’t do it (U.8-TA-120).

213
Josie was described as a very friendly, approachable, really happy nice personality who
is very calm and able to control her temper (U.31-MT-477; U.19-LST-237). She has
“impeccable manners really … she’s a really nice friendly student” (ET-U.2-10, 12). As far
as her behaviour is concerned, “you can’t fault her” (U.2-TA-110.). She is “lovely and
sweet” to have in class and although one teacher plans a lot of maths activities for her, “it’s
hard giving her that time when there are so many and I’m talking psychotic ratbags. You
take your eyes away for one second and they’re up on the tables and they’re running around
which is my biggest nightmare having this lot just running around like mad chooks”. This
teacher allocates planning time for Josie but “in the actual delivery I wouldn’t say that I’d
give her as much time as she really needs ‘cause I’m so focused on the behaviour in the class
… that’s when I need the teacher aide” (U.7-MT-164, 170).
Josie is enthusiastic and confident about the Performing Arts, cheer-leading and
dancing (U.31-MT-477) and though limited in what she can do with dancing, she still gets in
there and has a go (U.22-CST-154). Even if she doesn’t know how to do something, she will
try it and maybe give it a couple of attempts before giving up (U.22-CST-132). She seems
well-liked by classmates, is interested in classroom activities and she is willing to talk about
her own experiences (U.23-ET-229). Post school “I guess she’ll always be fine with talking
to people … well she can definitely speak well (U.27-AT-267) but another teacher said “a lot
of that’s got to be initiated by somebody else” (U.34-PAT-408). She has a career path …
she wants to work with animals (U.15-MT-296). She’s very good with her hands and she’s a
very caring person so she could definitely hone in on those outside of school” (U.19-LST-
333).
Independent Education Plan (IEP)
As part of the learning support program, Josie has one-on-one shopping excursions
where she has experienced difficulty with handling money. She was given access to the
family credit card for shopping trips which “really irked” the support person who had been
focusing on counting real money during withdrawal time (U.11-TA-128). Josie found it very
difficult to appreciate the concept of change and there was some concern about recent fund-
raising when somebody handed her a $5 note for a $1 bag and “she didn’t realise that that
person was waiting for their change” (U.11-TA-140).
Getting class work finished
Getting class work finished is a struggle. Task instructions are offered in a range of
ways – blackboard, handout, verbally to the class or individually. She tries very hard to keep
busy, participate and keep up with the class said an aide (U.1-TA-2). In a one-one-one

214
situation, Josie could complete an activity within a reasonable timeframe but in a class
situation, she needs constant monitoring to remind her of “what that task is about and how to
do it” (U.5-TIC:SD-36; U.5-ET-38). Without a teacher aide, she finds it very hard to stay on
task and keep up with the rest of the class (U.5-CST-34; U.13-PAT-190). She was not
unwilling to complete most tasks but rather she had difficulty “thinking it through and
remembering what the task was about and what the aim of the task was” (U.5-TIC:SD-36).
Two prohibiting factors were her reluctance to ask for help and a tendency to drift off into
her own little world (U.2-ET-10) and when asked if a task is finished, she will say “yes”
rather than “no” in case she gets in trouble (U.10-CST-68). If she “gets stuck she won’t ask
for help, she’ll just sit there and sort of space out” until asked about progress and when
refocused, she becomes flustered and confused (U.13-PAT-190; AT-97; U.4-TIC:SD-30).
“Very rarely she’d get a task finished unless there was one-on-one and always pushing”
(U.7-LST-135). She “definitely doesn’t catch” all verbal instructions given to the class and
when given individually, it helps if Josie repeats them back … “Oh, now I know what I have
to do” (U.5-TIC:SD-45). She would complete well-practiced tasks “very quickly” whereas
information not grasped because it was too difficult would normally not get finished “unless
there’s a teacher aide who’s helping to do the work and I think well she’s not learning it, this
is probably her fifth exposure to this and now you’re going to sit there and you’re pretty
much doing it for her and she’s not learning anything. I guess we’re just wasting some time”
(U.9-MT-212).
Homework and assignments
Some teachers did not give homework to students doing vocational subjects because
they attend school for 3 days and do traineeships for 2 days (U.10-ET-142). In-class
assignments had modified expectations for Josie in that she is allocated a teacher aide on the
days she works on the assignment (U.24-MT-420). Homework was not something that “she
kind of takes responsibility for independently. I think it’s something that there’s a lot of
support with from home and I think she’s not ever had consequences for not handing in or
completing work so she’s lucky that she’s got enough people supporting her in the
classroom” and finding out what is due. If a problem is anticipated “we kind of get on top of
it and help her get it done by giving her extra time or just acknowledging that there’s a
problem and giving her a bit of extra support. If things were pretty much independent and
she wasn’t receiving that support there would be huge issues with her getting things done on
time” (U.21-TIC:SD-280-300). “Over the years I don’t think she’s done much homework at
all to be honest and my gut feeling is Mum does the assignments and I’ve proved it at least
twice in that time that I’ve worked with Josie on assignments in class. I’ve seen the draft in

215
her book and the draft is completely different to the end result and it’s quite often not in
Josie’s language” (U.24-TA-370-374).
Copying from blackboard and handwriting
Josie normally sits near the front of the room. She can copy work including calligraphy
from the board though very slowly and she “works at her own pace” (U.12-AT-111; U.16-
PAT-216). Work copied was not extremely accurate. Words and points may be missed and
she needs help to finish before the board is wiped (U.10-LST-165; U.12-AT-115). Some
days Josie’s “attention and recall are good other days to put it horribly, she’s out with the
fairies and those days are very frustrating days … very frustrating” (U.6-TA-92). Instead of
adding one letter to the middle or end of a written word she will “cross it and start again and
just lately she’s back to pencils instead of biros” (U.6-TA-62-66). Two teachers did not
utilise the board because students could not be relied upon to copy … “these kids don’t copy
and behave. We don’t copy stuff down at all … they don’t cope” (U.7-ET-64; U.11-MT-
254). Josie and her mother said copying from the board was “difficult … I guess that’s the
easiest way to say it” (U.15-P¹-S-P²-878).
Handwriting was legible but very untidy, quite messy and childlike (U.6-TA-62-66;
U.13-AT-123; U.10-TIC:SD-75) and if in a hurry, it would not be readable (U.11-LST-173).
Josie enjoys Creative Writing and jotting down memories from an exciting event and one
teacher remarked that although writing may be “a bit scrappy, you can actually understand
what she’s saying and it’s quite thoughtful” (U.13-AT-123).
Comprehending and following instructions
Understanding and following instructions can vary from day to day depending on level
of fatigue and ability to mentally process directions. She has delayed comprehension skills
which means instructions are not necessarily understood when first articulated but if the task
is demonstrated and Josie repeats the steps back, she will say “Oh right, now I understand”
(U.6-TIC:SD-49). Changing from one task to another was not 100% because the first task
was not finished and she would get confused and flustered “then you’d lose her again” which
meant the teacher had to retrace steps with hands-on examples (U.12-LST-143). If a lesson
involved chopping and changing between three or four tasks, Josie may be on the second
task when the bell rang so “one thing and have it repetitive for her” was the best modus
operandi (U.12-LST-143).
When flustered, Josie may flip pages back and forth and read things very quickly
without slowing down. She “just had no idea what was happening really”. She may roll her

216
eyes and actually talk to herself when processing instructions but if unable to comprehend
she would be very quiet and “you’ll see her lips move then she’s talking to me but I think it’s
just the whole self-confidence I’m not quite sure …” (U.6-LST-123; U.6-TA-96). In
cooking classes, aide support was important for keeping her on track and preventing a drift
into her own little world … “a daydream type thing” (U.7-TA-100; U.13-PAT-190).
Following instructions is often delayed unless in a one-on-one situation. Small step-by-step
instruction works best and knowledge of the whole phenomenon was considered an aid to
end comprehension “because she’s got a very poor short-term memory as well, very very
poor and I’d say a very poor kind of middle term memory” (U.7-TIC:SD-51).
Planning and time management
Teachers who had worked with Josie in previous years reported her struggles with time
management, planning and organisation. Planning and organisation were described as very
poor, reasonably poor or “she’s got no planning skills” (U.11-TIC:SD-79; U.14-TA-172;
U.17-PAT-226). She needs constant monitoring about assignment due dates “today you
need to do these steps”. In one practical class, Josie was planning to draw the desk in her
bedroom but it took a long time for her to recall … “have a think about what’s in your room
… right, so you’ve got a bed … when you sit on your bed and you’re sitting on the side and
you look what can you see” asked the teacher. Josie agreed to take a digital photo of the
desk and bring it to school. “Well have you got it? ‘No I haven’t got that’”. The teacher had
not written this in Josie’s diary. After teaching Josie for 8 weeks, the teacher of a modified
English class said “everything’s done; she organised herself to get assessments done and
kept up to date with the assessments”. Time management was reasonable and Josie was in
the top three or four students in the class as far as completion of tasks … “doesn’t let things
drift, doesn’t stop work and doesn’t let herself get distracted by other kids” (U.10-ET-84).
Once in class, Josie does not think to open her bag and get out her book and pen but
needs prompting then she gets flustered (U.14-TA-172). She does not know whether her
diary or calculator is in her bag. “Mum actually packs her bag … she really didn’t know
what was in her bag until she opened it and had a look”. The teacher expected that by high
school, Josie would be in complete control of packing her own bag (U.18-TA-248). To
ensure cooking ingredients are brought to school, a teacher or aide phone the mother and
send a list home. She needs a lot of prompting “but I’m not sure whether part of it’s to do
with her upbringing in that Mum’s unwillingness to let her become independent and force
her to start making some of those decisions” (U.17-PAT-226). “She’s got no concept of time
and she doesn’t wear a watch anymore” although Josie was aware of the significance of
school bells (U.14-TA-252; U.1-P-2). In cooking class, she can sit and wait for the next

217
direction “she’s got to be nudged and pushed most of the time” said the teacher (U.17-PAT-
300). She always has aide support and does not have to work independently or manage her
own time and one teacher considered the consequences of such reliance post-school … “I
don’t know whether we’re really doing the best thing for her but the support helps her be
included” (U.14-MT-284-292).
Handling novel tasks or situations
She finds change confusing and depends on the timetable around her neck to plan her
school days (U.21-TA-300). Shopping expeditions were undertaken so Josie could
experience grocery and other shops. “When we came to somewhere we hadn’t tried before,
she was extremely nervous. She’d tense herself up and you could see the white on her
knuckles as she’s holding onto the arm and I would really have to talk fast to calm her down
and if she didn’t I’d just say okay close your eyes we’re going to do it”. Because it was
something new, she was not confident but next time “she’d still tense herself but it would be
nowhere near as bad” (U.23-TA-364).
She “needs a lot of reassuring for anything new that’s happening and feels a sense of relief
when it’s over”. Her first Virtual Schooling lesson went very well and the process was
discussed with Josie beforehand. She spoke clearly and loudly to the teacher despite a
tendency to speak very quietly in any new or different situation (U.17-TIC:SD-187). She is
enthusiastic and willing to try something new but gets flustered and “won’t put herself on a
limb” to ask for help. Aide support is therefore important to help her follow new directions
and change from one subject to another (U.15-PAT-212; U.12-LST-283).
Maths
Josie finds maths very difficult. She really struggles and had great difficulty with class
maths in previous high school years (U.15-TIC:SD-149; U.12-TA-148). A maths problem
that substituted words for numerical symbols was too difficult (U.4-CST-22; U.7-MT-140,
154). She currently does Consumer Maths which focuses its foundation to Level 2
Education Queensland maths outcomes. It provides grounding in basic numeracy such as
how to add, subtract, multiply, divide, how to use money and to some extent fractions,
percentages and measurement. She enjoys basic numeracy because she can do it and she
responds well to verbal praising “Oh excellent! Good stuff!” She was thought to enjoy
maths this year because “she really loves the games” (U.6-MT-132). She does not
understand place value, cannot read numbers in the billions, cannot problem solve and she
struggles with long multiplication, long division, fractions and percentages. Although she

218
can do some mental computations, staff was advised to develop her calculator skills (U.10-
MT-222).
Concentration and memory
Concentration span is generally short. Some days “there’s none at all, other days it’s
surprising how well she can concentrate” (U.7-TA-218). Some days she appears to be
concentrating but closer scrutiny may reveal otherwise (U.17-AT-169). Concentration was
thought to be 10-15 minutes and it would need to be a “fairly engaging task to engage her for
that 15 minutes” … maybe repetitive tasks that she can do (U.14-TIC:SD-139).
Problems with memory mean that everything must be written down and she is affected
by what she needs to remember, how important it is to her and obviously how often she
thinks about it, said one teacher and aide (U.7-TA-220; U.11-SID:SD-83,85). Instructions
written on the board then spoken are not remembered after the first hearing but “she
remembers it if you go over it and over it again. She’s learnt her times tables by rote
learning” said one teacher (U.16-MT-313). A computer assignment about developing
databases was manageable until entry of many different keys was required and she became
confused and needed one-on-one support. She was able to understand the steps but unable to
remember which process to follow (U.10-LST-169). One teacher routinely sat Josie next to
“one of the friendlier students” who would provide help but Josie “just spaces out and
doesn’t do anything” … just sits looking at the computer until the teacher comes (U.11-CST-
74).
Verbal skills, vocabulary and orals
She is quite articulated and softly-spoken and one has no trouble understanding what
she is saying (U.25-AT-261; U.24-ET-231). Language skills were perceived as better than
maths skills but again she was not confident to ask for help. (U.4-PAT-68-74). She can
communicate said another teacher but she is very quiet, hard to hear and “doesn’t know
really what she’s going to say” (U.20-LST-239). A teacher referred to other students with an
intellectual disability who “don’t have very good conversational skills” whereas Josie’s
conversational skills were an area of strength (U.17-MT-335). Josie is very quiet and tends
to withdraw a lot in practical classes “but I don’t know whether it’s related to an inability to
be confident as such or herself”. Her quietly-spoken voice was of no concern to one teacher
who felt class members should be more courteous about listening (U.24-ET-231). When
presenting an oral, comfort level was paramount and for Josie or any student who feared
intimidation by a non-positive culture, this teacher was flexible and open to presentation
before a smaller more sympathetic listening audience (U.12-ET-110).

219
Group work with peers
An observation reported by teachers was Josie’s reluctance with group work. She
would look around and look a little worried that she would not be included (U.4-AT-34, 36).
She is more reserved and tends to sit back and sit quietly until the teacher reminds students
“well don’t forget to include Josie” (U.14-LST-203). She is willing to be involved but
“there’s a natural barrier that she’s got to overcome with the other students … it would be up
to the peers to let her in” but once accepted, she would get in and try her very best but she
had not been observed doing a lot of group work happily (U.13-TA-406, 150). At times “the
kids aren’t always particularly willing to accept her as a group member but some of that
comes from her own reluctance … she’s not a particularly willing participant” and if not put
with certain students, she would probably be unwilling (U.27-PAT-376).
Josie has a lot of good ideas or a lot of perception about the group afterwards “‘I didn’t
like the way they did this’” but she finds it hard to keep up with crossfire verbal exchange
and the social interaction (U.27-TIC:SD-350; U.13-TA-156). She would miss large bits of
conversation and because “they’re all adding ideas and changing topics so fast” she can
switch off and go into her own thoughts and “she doesn’t really understand the way people
have a go at you” (U.23-AT-227). An aide may say something in a friendly way to cheer her
up or get things moving and Josie will look to see if she has a smile on her face and will say
‘Oh, Lucy Loo!’ but if a student did that, she would definitely take it the wrong way. I think
she’s been upset quite a few times with comments from students that to be honest, they
haven’t really meant what she thinks they’ve meant” (U.13-TA-152).
There is definitely that misunderstanding and Josie was thought to have great difficulty
communicating not just with her peers but with any student … “that’s probably why she’s
sitting in the covered area by herself because the other kids have given up on her really. I
know that sounds very cruel but they find it difficult to communicate with her and she finds
it hard to communicate back” (U.13-TA-156). Josie was thought to have had a sheltered life
in that she had not experienced a lot of things that other kids had experienced “therefore
they’ve got no subjects they can talk about or can relate about” (U.13-TA-166).
Everyday taken-for-granted tasks
Many daily tasks were difficult. Each cooking class requires a planning sheet. The first
thing is the name of the recipe and “then she’ll stop” and when asked about the next step, she
has to really think about it. As a practical aid to understanding fractions, students were
asked to make fried rice, “a fairly easy task for pre-vocational maths but it’s authentic and
she couldn’t do it”. The essence of the task was to measure ½ cup, ⅓ cup then double some
220
quantities. After three years of Home Economics, the teacher thought “she first of all would
know her way around the kitchen because she’d been in there so often and second that she’d
be able to follow the directions because it was step by step and I knew that she’d done that
before and she didn’t know what to do, she didn’t know what to do”. The teacher expected
“she would be able to recognise that this is a recipe and read the steps. I mean there’s only a
limited amount of vocabulary that you use in writing recipes, measure chop, stir. She had to
have me there telling her, pointing to the words ‘okay now this says ⅓ of a cup of …’ That
was a hard day, I didn’t have a teacher aide either” said the teacher (U.21-MT-394-444).
When cutting an onion, she may remember to put her fingers on top of the onion but
must be prompted to use her left hand or “the onion would take off”. One day, Josie was
using the cutting knife upside down. “Well I couldn’t wait too many times for that ‘cause
she was going to end up cutting her finger”. She could not tell the difference between the
sharp side and the blunt side said the aide (U.4-TA-46). Chopping, using scissors, gluing,
pasting and opening a flavouring sachet are awkward difficult tasks. With practice, Josie has
become good at cutting an apple into four pieces (U.17-TIC:SD-316; U.4-TA-46, 388, 400;
U.18-TA-230).
Manipulative tasks were difficult in the maths class. The teacher would instruct
students to use a ruler to mark off once then twice before cutting a piece of A4 paper into 8
even pieces (U.7-MT-132, 146). The marking off stages went well while the teacher was
showing Josie what to do but “as soon as I went away, she just had these lines that were this
thing and she was supposed to be doing something that was 9 cm apart” (U.7-MT-140).
Students in this class enjoyed hands-on activities and most were operating at somewhere
between current Level 2 and 4 to do tasks learned in preschool, Years 1 and 2, said the
teacher (U.7-MT-150).
Putting previously learned work into a new context is very challenging. “She’s been
taught to do fractions a certain way” and during the first week of prevocational maths,
students did a lot of cutting, colouring, fitting fractions into different areas, measuring and
talking but no actual writing which was completely new for Josie. There is nothing in that
maths class “that she’s never learned before … it’s just new context and she can’t do that”.
Josie can add and do her times tables but “give her a word problem about adding or times
tables and she can’t do it, so does she really understand what times tables mean” (U.21-MT-
361).

221
Organising her desk, getting things out of her bag, keeping a folder orderly and opening
it without the contents going everywhere, putting papers into a plastic pocket and folding a
letter before putting into an envelope are all difficult for Josie (U.17-TIC:SD-308-326).
Critical life skills as represented in school
Development of life skills and independence were raised as concerns and one teacher
did not know whether these were “Josie’s issues or a family dealing with Josie’s problems”
(PAT-48; TA-354). One teacher compared Josie with other students she had seen with a
physical disability who were “quite capable of doing things” that Josie did not seem very
willing to try by herself. In fact, she did not find Josie extremely independent (LST-39). A
critical issue for staff was Josie’s dependence on them for many things which they believe
she is capable of doing for herself, in particular her toileting which “we’ve observed on
numerous occasions that she can do” (TIC:SD-14). On days when the nurse is late or does
not arrive, offers of teacher help are refused. On those occasions, Josie does not do toileting
even though a checklist on the wall outlines the procedure which staff say she has
demonstrated she can do with little or no help (TIC:SD-14). To increase independence and
phase out the daily nurse visit, one teacher offered to take on that role but this was refused
(TIC:SD-20).
School infrastructure had been modified and improved to help Josie gain independent
life skills but “you can lead a horse to water but you can’t make it drink” (PAT-47). The
school purchased a hand-operated sewing machine and installed a new unit in the kitchen.
She started Hospitality but did not continue which caused staff to question whether “it’s a
family issue … ‘it might be a bit hard this week so we’re just going to drop it’”. A teacher
remarked that it may be part of her problem that she just doesn’t have the ability but the
teacher was “not privy to what she really is capable of” (PAT-47).
Coordinated use of both hands presented a problem for Josie in the classroom and in the
kitchen. Where the left hand is automatically used to steady a notepad or hold food being
chopped, Josie kept her left hand on her lap or tucked under her jumper. When cutting very
very thin slices of salami “she still wasn’t cutting all the way through to the board” … she
did not seem to understand that putting pressure on the point may be more effective (TA-40-
44). With respect to healthy eating, a teacher said the general opinion was that food
consumed by Josie was not “always good for her … not particularly healthy for her”. For
example, she goes through spates where she might have scotch finger biscuits for breakfast
(PAT-48).

222
If asked in the kitchen “what do you think we’ve got to do next, we’ve got all these
things here” she would have trouble and if something went wrong like the cake did not come
out of the tin properly or she forgot to add an ingredient, Josie would get “very defensive”
and “a bit more closeted if she strikes a problem she doesn’t want to deal with” (U.10-PAT-
180). She does not like to ask for help and although she does not express any desire in a
verbal way “I’m not going to do that”, one teacher said “it’s more kind of passive that she
just won’t do it” (U.4-TIC:SD-30). Anything out of her comfort zone that she has not dealt
with before is very difficult (U.9-TA-112). She finds cooking activities hard possibly
because it’s “a whole new world to her” if she does not do it at home (U.9-TA-112). Sewing
was very difficult. Initial shopping trips to the town, moving from shop to shop and
negotiating gutters were challenges “because she didn’t have enough confidence in herself”
but with reassurance and repetition over time, she learnt to navigate the town’s footpath
unaided (U.9-TA-114).
Decision-making and problem solving are difficult in class, in the kitchen and on
shopping expeditions (U.10-PAT-164; U.4-TIC:SD-155, 121). Whether “she’s worried that
she’s going to make the wrong decision or doesn’t like making choices … she’d be quite
happy for you to say do this” (U.10-PAT 160). She could probably offer solutions to a new
situation but if faced with the actual problem, she may not be able “to bring that across”. For
example, one activity required students to offer strategies for including someone in a group.
Josie could offer suggestions but if put in a situation that related to her life, the teacher
queried if “she could do the things that she suggested and I don’t know whether that comes
down to her confidence as well, like understanding what’s going on around her and being
able to pick up on those signs. Yes, I think decision-making is an issue” (U.10-PAT-166).
If asked “do you want a pink drink or a blue drink”, Josie automatically says “Oh oh, I don’t
know” and from there it will be a struggle. Her response to being put on the spot is “really
terrible” maybe ‘cause I thought if I said that I would get in trouble’” (U.4-TIC:SD-155,
121).
Josie can move from class to class quite independently but she likes people to do it with
her (AT-20; LST-23). A point of contention between family and school has been who
should and should not push Josie’s wheelchair if she needs help. The school had made
changes to enable access to any room or building she would need to enter but the mother
thought wheelchair wheels may be incompatible with carpet or grass (U.3contd-LST-63).
One teacher said “well we feel that she can do that but if she needs to get somewhere and
she’s having a great deal of trouble, we will ask if we can help her and if she says ‘yes’ we’ll
help her or she’s welcome to ask as well …” (U.13-TIC:SD-117).

223
Teacher and aide perceptions of Josie as a person with a disability
Advice for other teachers
Keep checking on progress, keep prompting to make sure the student is actually
understanding without letting them “slip off too much” (U.30-ET-281; U.23-CST-148).
Josie will just “sit there quietly looking at the computer so if you just glanced around, it
would look like she was doing something but actually she’s just sitting there”. One-on-one
instruction and help with the first activity then encouragement to continue without support
was advised. Physical scaffolding like worksheets and considering factors like font size and
type, background colour of paper and encouraging the student to ask questions and seek help
were found helpful (U.26-ET-245). Very short precise instructions, lots of repetitive work, a
lot of hands-on work, notes and handouts because “she doesn’t have the capability of writing
bodies and bodies of work” and peer-building were essential. Involving Josie with her own
learning, goal-setting, support and positive feedback “‘cause I notice she does thrive on
positive feedback and praise and probably modifying her tasks and her assessment work”
were advised (U.17-LST-217). “Persistence, checking, keeping on task … I don’t know how
to develop enthusiasm. I think it’s something that’s innate isn’t it … something that’s got to
come from you” thought one teacher (U.35-PAT-414). Being courteous and humourous
goes “a long way with Josie but be firm, don’t go soft on her” said an aide (U.32-TA-422).
Another teacher had no advice “I seem to be the person making all the mistakes
although I’m trying things at the moment and they don’t seem to be working like I’ve made
her happier but what’s she learnt. She thinks it’s fun. She used to hate maths and now she
likes coming and we do really good stuff but I don’t think she’s learnt anything”. Through
university and in-service training, this teacher learnt strategies to use with students with short
attention spans and behavioural problems “but I don’t know anything about what can I do for
Josie to get her learning. What do you do if the other stuff’s not working because the
traditional instruction doesn’t work with her and I guess the more visual hands-on, I use a lot
of multiple intelligences, we’re used to using these if we use computers. We use pictures,
making things and if that doesn’t work either, what does” (U.20-MT-387-487). The
prevocational maths class is presently doing Grade 8 work and “Josie’s really doing Grade 5
work and we’re only learning it and I’m only teaching it not because it’s going to get you a
job as a scientist but because it’s actually something you will need in your life. You need to
be able to tell the time, calculate the area, calculate the volume of paint and I don’t think
she’s going to finish Grade 12 really knowing the stuff that she should to get through life”

224
(U.20-MT-491). Josie finds it really hard to use the knowledge that she does have in new
contexts or situations “so relating adding and subtracting to going shopping or relating
adding and subtracting to sharing a pizza between her family members I’m not so sure that
I’m being very successful at those, in fact I don’t think that I have been successful at all”
(U.1contd-MT/3-26).
Anything else you want to tell me?
“The Special Needs teacher has told us that Josie has not been diagnosed with an
intellectual disability and yet there’s so like … we don’t … I don’t think any of us
understand. We’ve been told that she has no intellectual disability, there’s nothing wrong
with her, she hasn’t been ascertained, there’s nothing wrong with her mentally she only has a
physical disability when it’s quite plain to see that she doesn’t just have a physical disability
so we don’t know. What is it and why won’t anyone acknowledge there is something”
(U.33-MT-527).
Another teacher said “Oh well! I think your study’ll probably be really … I mean I’m
sure we’ll learn things from it as well. I think we’ve got lots to learn and lots to keep in
mind and I think there can be a frustration level as you say when you think especially when
people think she has a physical impairment she doesn’t necessarily have an intellectual
impairment. So I think teachers struggle with that ‘well why can’t she do this’ and I think
it’s hard in Josie’s case to know the decisions she can make or the processing she can do
because I think there’s such a high level of dependence there in a range of areas of her life,
not just physical dependence but the ability to solve all her own problems and even the
ability to choose her own friends and socialise in the way that she wants to. I think there’s a
lot of dependence in that area and I think that makes it hard to separate what is actually
really a problem for her or what is an easy way out” (U.31-TIC:SD-448).
Concerns were expressed about teacher aides and the assistance they provide. “When I
think of the teacher aide, I am looking for somebody not only to assist students in class but
also to be able to withdraw some students away from the other ones to be able to work on
something. It could be one-on-one or two-on-one specifically and I don’t think that happens.
Like sometimes you feel that you have to baby-sit the teacher aides too, that you’re not just
baby-sitting kids that you’re baby-sitting the teacher aides whereas I’m looking for a teacher
aide who’s got a little more autonomy and is able to think off their own back and not for me
to have to spoon-feed them” (U.4-MT-88).
225
Teacher understanding of learning difficulties
Maybe as teachers we don’t fully understand all the implications of her medical
condition on issues like decision-making and problem solving. We think that “spina bifida
has meant that she’s ended up in a wheelchair but we know she’s got some sort of
intellectual … but we would expect her to be able to make a decision ‘do you want this green
thing or do you want this red thing’ and we think that’s an easy decision to make. There’s
no right or wrong answer … and maybe we don’t understand … it’s not because she hasn’t
matured or grown up it’s just that she can’t like she’s not skilled in that area because of her
mental condition” (U.19-PAT-288).
“Oh gosh! Well she has some learning disability” and the major subjects like English,
Maths, Science and Computers “she’d probably find those difficult” (U.3-LST-97). Josie
“sometimes goes off in her own little world and she doesn’t really focus a lot of the time and
because she doesn’t have that confidence she won’t put her hand up and say ‘I don’t know
what I’m doing’”. Learning difficulties were thought to “stem from thought processing and
problem solving especially within her academic subjects. I don’t think she has any difficulty
with the actual work. I think she can complete most of the work and is really able to do
that”. Maths was the only subject where she thought some maths concepts had not been
grasped. Whatever the sign given, Josie will add instead of take away and if given a maths
word problem, “her automatic response is just to add everything, add all the numbers she can
see in that word problem up but I think any of her troubles in other classes come from not
being able to problem solve, ‘what do I do next’, probably time management, keeping
working and keeping focused” (U.28-TIC:SD-354).
Another teacher “wasn’t really sure exactly about her disability and how far it was with
her intellectual side of things”. When checked on she would say “‘O yep that’s fine’ but
you’d have to look at her work because she would be nodding and agreeing but not really
catching up with things. With every new task she had great ideas, was enthusiastic and
excited to start but needed to be checked on and she’s very forgetful too. It was quite
deceiving because you thought she was quite switched on and doing really well and yeah
there’s just a few things you needed to remind her of constantly” (U.1-AT-10).
She tries very hard (U.3-LST-125) but needs small precise point by point instruction
“do this, do this, do this” which can be difficult and frustrating for the teacher if no aide is
present and there are twenty other students to consider. Verbal instructions given to the class
are difficult to follow. “It’s like she’s day-dreaming … it’s almost as if she thinks I’m
talking to everyone else except her” and because the teacher always gave one-on-one to
226
ensure she was on task “one step … stop … give a step … stop wait till she does that, give
another step”, she wondered whether Josie now relied on this (U.7-MT-154, 164).
Although aware Josie needs assistance, “I also want her to become independent as well
and I’m getting to that point where I feel I shouldn’t help her as much because she’s got to
learn to get on in life herself. I know that sounds a bit mean but that’s the way I feel at the
moment. I’ve helped her I think to the full capacity but now is the time to cut the apron
strings and let her try things out herself. Sometimes it becomes very frustrating for me and I
will step in and say “well come on Josie let’s keep moving. She needs encouragement to be
a bit more assertive and do things and not just sit back and wait for things to happen” (U.2-
TA-420). When asked if Josie’s disability was explained to students, one teacher said “no, I
would assume that a lot of work would have been done with her in primary school but I’m a
new teacher and to some extent it really hasn’t been explained that much to me. I’ve had
Josie’s Mum talk to me about it but there’s some kids in Grade 11 who have no idea what’s
wrong with Josie” (MT-36).
Have you heard of a Nonverbal Learning Disability?
Seven out of eight of Josie’s teachers had not heard of the NLD syndrome (U.28-CST-
178; U.31-AT-285; U.34-MT-529; U.27-ET-300; U.30-LST-388; U.36-PAT-516-538; U.33-
TA-438). One teacher said “yeah I have read some information on that” (U.31-TIC:SD-471-
471). When the shunting device was mentioned, another teacher said “is that always there is
it … no I don’t think … Josie doesn’t have that” (U.30-LST-400).
Teachers were interested to “know what’s out there and what can be affecting kids” so
they can try to help them better” (U.28-CST-178) and another queried how much they really
knew about “what she’s got and what effects it can have”. After speaking about the NLD
syndrome, an aide said “so would that explain why Josie can’t form an opinion about
anything. If you ask her opinion of something, she will automatically turn to the next person
as though they could give her an answer ... You see it’s hard for us to distinguish whether
she can express an opinion or whether she just hasn’t got the depth of knowledge to make an
opinion or whether she’s so used to Mum making decisions for her that she’s used to going
home and asking Mum for her opinion and Mum’s opinion’s the opinion. It’s very difficult
to work out what it could be” (U.33-TA-438).

227
Summary of 2004 Neuropsychological Assessment and 2005 Psychological
and Speech assessments –
The following extract has been taken directly from assessment reports.
2004 (aged 14 yrs 9 mths) Full Scale IQ = 72
Verbal IQ = 78
Performance IQ = 71
VIQ-PIQ difference = 7
2005 (aged 15 yrs 9 mths) Language assessment age equivalent = 12 yrs 10 months
Problem Solving age equivalent = 11 yrs 4 months
Based on performance in 2005 assessment and information obtained from the previous
assessment, Josie does not fall into the category of intellectual impairment. However, her
level of intellectual functioning only falls just above that of intellectual impairment.
Furthermore, there is not a significant difference in the discrepancy between her verbal and
non-verbal skills but she does have significant deficits in both areas.
As a result of her deficits, Josie will have difficulty in a number of areas which will
affect her functioning both at home and in the school environment as follows:
• All areas of academic learning;
• Acquiring new material as well as retrieving information from her memory;
• Any task which involves an organisational component;
• Processing information quickly e.g. having to follow a set of instructions;
• Any task which involves a component of hand-eye coordination e.g. undertaking
work from the blackboard;
• Attention, concentration and ability to hold information long enough to complete a
task.
Her social communication skills are a relative strength for her, although this may lead to
under-estimation of Josie’s cognitive impairments. Her vocabulary, semantic verbal fluency,
fund of general knowledge and her verbal abstraction and reasoning were relative strengths
for her as were her sequencing with visual material (2004 Assessment). Josie obtained
average total language skill scores for comprehension and expression though some subtest
scores within total scores were significantly below average. “There is much in her world

228
that she does not comprehend fully” and “there is much in communicating her ideas that she
finds difficult” (Communication Assessment Report, 2005, pp.3,4).
Interpretative discussion
Family interviews were conducted in the family home and they lasted 4½ hours. I
found that once people began to talk, they became oblivious to time. Focused interview
guide questions provided further response triggers. Josie’s mother was the first person to
respond to a recruitment mail out. She conveyed many concerns with school staff and their
lack of understanding about Josie’s learning difficulties.
Teacher and aide interviews were held in the high school’s audio visual room. All
educators recognised limitations caused by the physical disability but planning, organisation,
decision making and problem solving difficulties perplexed them. Based on diary notes and
recollections, I believe all teachers and aides were caring people who wanted to help Josie
but at times their intentions were skewed by misperception and little or no knowledge about
the effects of hydrocephalus on learning and daily functioning. I suspected some teachers
implied a problem with Josie’s mother which at times may have had a rippling affect on
Josie. Almost all teachers wanted more information. The Special Needs teacher said “she’d
heard of NLD and read stuff about it” but no other teacher interviewed had heard of an NLD.
This case study is about a failure by educators to understand the neurological cause of this
student’s functional and learning difficulties. Josie was diagnosed with an NLD, an
Executive Function Disorder and her intellectual functioning was within the borderline
range.
“There’s pretty much not a day that she’s not late for school” (TIC:SD-4;
TA-2; U.12-TIC:SD-89). No amount of prodding and forward-planning seem to solve the
morning problems on a consistent basis. Getting clothes ready, tuckshop and bag packed the
night before should help but poor memory, concentration and distractibility interfere unless
you supervise and even then, repetition does not ensure practiced routines will continue.
Maybe hydrocephalus impedes retention of a practiced sequence like breakfast-teeth-
dressing-hair. Children with hydrocephalus are frequently reported to drift into their own
little world with the fairies. They don’t want to be a nuisance and they don’t want to be late
for school, class or appointments. They generally want to please and not cause tension at
home “why are you angry at me?” One instruction is a lot for Josie to process at one time so
if asked to eat breakfast then do teeth, she gets “herself flustered and very panicky in the

229
mornings” (U.8-P-303). Whitney (2002) reports the effects of daily stressors on a child with
NLD “I feel every day the way other people feel in a crowded shopping mall just before
Christmas” (p.34).
The mornings are tough and tiring for the most organised households. Imagine the
accumulated affect on the child and family. One teacher personally thought Josie’s Mum
packs her bag and by high school, she thought “Josie would be in complete control of her
own school bag” (U.18-TA-248). If she doesn’t have good planning, organisation and time
management skills, it may come time to leave for school and she is not packed up so the
mother does it. Parents tend not to talk about the mornings unless asked. They become an
accepted part of daily life but they take their toll on the primary caregiver, while siblings
tend to move on with time.
Neuropsychological testing done in 2004 revealed that Josie could focus attention for
brief periods of time but she had difficulty sustaining that attention. Her ability to divide her
attention between tasks was severely impaired. Her ability to comprehend, process, and hold
information in mind for the purpose of completing a task was impaired and she performed in
the severely impaired range on a task of planning and organisation. The discrepancy
between teacher perceptions of Josie’s lateness and the mother and daughter reports of
school mornings is significant. Despite receiving a copy of Josie’s prior assessment,
teachers seemed unaware that planning, organisation and time management problems might
contribute to late arrival at school. Although an occasional accident may sometimes be the
reason, those interviewed did not consider punctuality to be “a big priority at home”.
“Over the years I don’t think she’s done much homework at all to be honest
and my gut feeling is Mum does the assignments …” (U.24-TA-370-374). The
absence of homework this year had a positive influence on Josie and her mother’s opinions
of school but the stress, quantity and challenge of previous years’ homework and
assignments on Josie and family were reported. Slowness copying from the board, inability
to comprehend, decode and write verbal directions, short-term memory, planning
organisation and information processing problems mean task instructions are often
misinterpreted or incomplete. Researching information in the library or on the internet is a
task affected by poor visual perception and ability to sort relevant from irrelevant data.
Assignments require weaving together information from various sources and completion is a
complicated cycle of steps which make the task complex and painstaking for the family and
student with an NLD, without mention of the concentration and effort required for the final

230
type-up. Is it any wonder “she’s never ever worked on and completed a full assignment by
herself … it’s always had input with me” said the mother (U.8-P-307).
Aide support to plan and prepare the first draft of an assignment in class and modified
expectations are now in place which allows Josie to feel a sense of achievement and closure
on task completion. Two teachers inferred a lack of independent responsibility while
another teacher believed Josie would attempt homework with a lot of scaffolding, one-on-
one support and help from home. In addition to the aforementioned difficulties, Josie’s 2004
assessment confirm that concentration, task completion, logical sequential reasoning with
visual information and information processing abilities were impaired which generates the
question “Is assessment data shared with relevant teachers and aides and if it is, do they
understand the implications?” There appears to be ample evidence to verify that Josie’s need
for constant prompting, small-step instruction and one-on-one support to initiate and
complete tasks is genuine.
“I guess the one thing I’ve noticed is her relationship with the other
students mostly. She really really wants and longs for someone really close in
friendship but doesn’t really have someone” (AT-34). Children with an NLD
encounter their biggest problems in the social arena. With increasing grades as tasks and
expectations become more complex and require the student to take more initiative for
decision-making and problem solving in school and personal life, these children just cannot
cope. Gaps start to widen around Grade 6 as peers approach teenage years and interests and
emotions begin to change. They need people around them who understand their dilemma and
the emotional fragility that results from difficulty coping with peer interaction and
developing friendships. With advancing grades, the child may be teased and regarded as
“weird” or “a nerd” because they don’t recognise or interpret the nonverbal aspects of
communication. They may roll their eyes, not understand jokes and sarcasm and have
trouble keeping up with cross-fire conversation generated within social groups. As peers get
older, the subtleties and underlying meanings increase “well they would be lost on her I’d
say … that’s probably why she’s sitting in the covered area by herself because the other kids
have given up on her really” (U.13-TA-156). Josie’s severely impaired visual-spatial
perception may hinder her ability to gain the ‘full picture’, to recognise faces, interpret
gestures and read facial expressions which would make social interaction and group work
tough. These children bring the problems home, anxiety is taken to bed and it is still there
next morning when the child has to again face the music.
231
Social, communication and manual skills develop as children play, negotiate over
games and toys and share interests and responsibilities but as social complexities increase,
the adolescent with NLD finds it hard to cope with the constantly changing milieu. Friends
become fewer, there may be no invitations to parties and as social isolation increases and
gainful employment fails to materialise, anxiety and depression may well intensify.
Assessment of Josie’s ability to generate appropriate responses to certain scenarios indicated
she did not always interpret situations as the majority would, “there is much in her world that
she does not fully comprehend” and “there is much in communicating her ideas that she
finds difficult” (Communication Assessment Report, 2005, pp3,4). The aide said Josie has
been upset and had misunderstood comments from students quite a few times. To be
effective at understanding communication, Levine (1994) says a student must “use active
working memory to store the gist of one sentence while processing the subsequent sentences
and drawing appropriate inferences” (p.88). Test results report that Josie had impaired
ability to hold information in mind and process information quickly. Does anyone at school
really understand how lonely she must feel at lunchtime? Josie felt lack of peer interaction
meant kids wouldn’t want to group with her. What does it feel like not to have one special
friend? Does it affect one’s confidence and ability to function in the world and feel part of a
community? Educational loneliness carries through to post-school. If an acceptable niche is
not found and career goals developed through school do not eventuate, feelings of failure
may result. It is therefore reasonable to stress the need for early identification, assessment
and understanding of the NLD profile by teachers, aides and guidance officers to avoid this
outcome.
“Maybe those life skills should have been started way back when they first
started school so that they’ve had lots and lots of practice” (U.4-TA-214).
Lengthy discussion revealed teacher and aide concern about Josie’s ability to cope in the
world post-school and the timeframe left at school to achieve essential skills. Some staff
spoke of creative strategies they had developed to help Josie learn basic skills such as
remembering and reporting a message, shopping and navigating footpaths and gutters in her
wheelchair and buying groceries. Some elements of preparing a convenience meal were
unbelievably difficult for her like cutting the flavouring sachet and pouring boiling water
into a cup. These are genuine difficulties for a child with Josie’s functional profile.
Psychological assessment reported that Josie could use scissors and her grip strength was
equivalent for both hands but on a task that required speed and dexterity, her psychomotor
performance was poor. Her ability to pour boiling water from a jug to a cup was
compromised by severely impaired visual-spatial-organisational skills, a reported fear of

232
boiling water and the skills needed to mediate efficient use of arms and hands for visually
directed reach, grasp and manipulation were impaired “so yes that little 2-minute noodles
took ½ an hour” said the aide (U.15-TA-176).
Everyday tasks like preparing 2-minute noodles, handling money and being able to
decipher coins in a purse, ability to gauge and check change at the checkout are difficult for
students with an NLD and I expect the mother was aware of this when she gave Josie a credit
card to take on the shopping excursion. I understand the aide’s displeasure since the focus
had been on counting real money at school but if the mother was aware of Josie’s money
handling difficulties, she may have trained her to use the credit card to speed up the checkout
process and save her embarrassment and delay. Having said that, it is important to ensure
Josie understands the concept of credit and potential implications. Borrowing and the
abstract nature of bank interest may also be difficult concepts for Josie to understand.
Folding a piece of paper and putting into an envelope, tearing a piece of alfoil or
gladwrap, unwrapping a parcel, unlocking the door or using scissors may be difficult for a
person with hydrocephalus and spina bifida. These functional difficulties are mediated by
visual perception, visual-spatial, visual-motor and manual dexterity skills and limited
exploratory play hinders understanding of cause-and-effect relationships in the environment.
Such “hidden” impairments may be difficult for educators to fathom when they are
accompanied by verbal fluency.
“How terrible she can’t decide whether she wants green or blue” (U.36-PAT-
516; U.4-TIC:SD-121, 155). Children like Josie have a penchant for sameness and
predictability which correlates with their problem solving, hypothesis-testing and decision
making difficulties. “If I do this, that will happen or if I decide this, that will happen”.
Limited environmental experience and knowledge of consequences combined with inability
to fully interpret a situation’s nonverbal aspects will impede hypothesis-testing. If they
cannot make comparisons, it is probably hard to decide. Making a decision and being able to
come up with a solution is difficult for Josie and “she’d be quite happy for you to say ‘I want
you to do this’” (U.10-PAT-164). On the Executive Functions questionnaire, the mother
noted that Josie often had difficulty coming up with different ways to solve a problem. The
age-equivalent of Josie’s ability to interpret and solve problems was 11years 4 months, 4½
years less than her chronological age (Communication Assessment Report, 2005, p.4).

233
“When we came to somewhere we hadn’t tried before she was extremely
nervous. (U.23-TA-364; U.9-TA-114). Restricted early mobility that limited experience in
home and community environments are mirrored in Josie’s preference for known situations
and familiar things. Social ineptness is more obvious in new situations which require
integration of a multitude of stimuli. Is it any wonder why a youngster with nonverbal
deficits becomes fearful of a new experience or situation?
“She’s sort of big on sausage rolls, toasted sandwiches … and scotch finger
biscuits for breakfast” (U.18-PAT-234). One teacher spoke of collective concerns about
Josie’s eating habits and she was interested to hear a possible explanation. Ninety-five
percent of persons born with a myelomeningocele are born with the Arnold-Chiari 2
malformation. Josie has this anomaly which means a tongue of tissue “usually derived from
the lower lobes of the cerebellum extends down into the upper spinal canal” to cause
frequent gagging and difficult swallowing (Anderson & Spain, 1977, p.40). There may be a
tendency therefore to avoid new or course foods.
“I’ve helped her I think to the full capacity but now is the time to cut the
apron strings and let her try things out herself” (U.31(contd)-TA-420). Concern
about Josie’s acquisition of life skills is understandable if one compares her with an able-
bodied 16 year-old. Getting through the school day can be a huge challenge for a child with
hydrocephalus and spina bifida and the child may begin many days with fatigue. Any
combination of the aforementioned difficulties which confronts Josie on a daily basis would
exhaust her without incorporating wheelchair dependence. Given her difficulties with
information processing, memory, concentration and manipulative skills, imagine the energy
she must expend to process, plan, initiate and complete a task. Sheer coping with the
complexities of school life may cause stress and anxiety that disrupt sleep and add to fatigue.
Post-school, when the weight of school pressure subsides, Josie will probably acquire skills
at an older age through individualized training that is tailored to her needs. It is at this time
that the true gap between Josie’s ability to function in the real world and that of her peers
may become more apparent.
When asked ‘how do you understand the difficulties Josie has in or out of
the class”, I felt the initial responses from two staff members who interacted with Josie the
most were somewhat guarded “what do you mean by that? I think most of her difficulties do
stem from thought processing and problem solving especially within her academic subjects.

234
I don’t think she has any difficulty with the actual work. I think she can complete most of
the work and is really able to do that. Maths is the only subject where I think some of the
basic maths concepts she hasn’t grasped …” (U.28-TIC:SD-354-6). The second response
“I’m lost for words there I’m sorry. I know she needs assistance but I also want her to
become independent as well and I’m getting to that point where I feel I shouldn’t help her as
much as I used to because she’s got to learn to get on in life herself ...” (U.2-TA-420).
Other teachers repeated earlier-raised problems.
Conclusion
At home, the mornings are very rushed. In the context of school, Josie has a negotiated
starting time but whatever the day, she is late. Late arrival and loneliness were critical issues
for school staff. Josie’s caring, happy, friendly and approachable personality, her refined
speech, good spelling, tables and script-learning abilities are distinct assets. She can manage
basic maths but cannot problem solve or deal with abstract concepts like algebra or
measurement. Manipulative kitchen tasks are difficult, handwriting and copying from the
board are laborious, planning, organisation, time management and short-term memory are
poor and it takes up to fourth term to learn her class timetable. Any change is difficult to
handle and she gets stressed and confused about new situations. One instruction at a time
works best and most teachers said she needs constant reminders to complete a task within a
timeframe. Understanding social interaction and developing friendships with peers has
become a critical issue. Josie longs for a special friend and talking to herself in lunch breaks
may be her way of dealing with anxiety and loneliness.
Teachers need to know that Josie’s profile constitutes an identifiable learning disability.
If they were informed about it in undergraduate, postgraduate and in-service courses, the
importance of nonverbal abilities for daily functioning would become prominent in the
minds of educators and other professionals. Students who present with the NLD phenotype
could then be recommended for assessment and given support that adequately addresses their
learning needs. Raised awareness may be the ultimate weapon against frustration and
negative commentary on the part of teachers, aides and peers and as an annual event, open
class discussion about individual differences should occur to nurture a culture of support,
understanding and acceptance … an ethos that will extend beyond the school gate to the
wider community and workplace.

235
CROSS-CASE ANALYSIS
Synopses
To ensure stakeholder perceptions are contextually grounded, this segment will précis
background data offered by parents, teachers, teacher aides and students. To do this, case
study texts were meticulously scanned to retrieve relevant data not previously used in case
study reports. Cross-case analysis then cut across individual cases in search of similar and
divergent views about the strengths and weaknesses that represent the NLD phenotype. A
constructivist perceptual view of reality acknowledges that stakeholder perceptions express
understanding at a point in time, all subject to interpretation from other perspectives.
Jenny
Jenny is in Year 5 and she lives with her mother, stepfather, 2 older sisters and she has
a close relationship with her Grandma. She walks independently, she is a very good
swimmer, likes doing all the things she’s not supposed to do like running, playing with kids
on forts and she loves riding her bike but is “not good on road sense”.
The mother lets her do as much as she can because “I’ve still got to give her that chance
‘cause it can be taken away from her at any time”. Her mobility, strong-mindedness, spirit
and enthusiasm to run around and “do everything like a normal child” leads outsiders and
kids to think “there’s nothing wrong with her” which causes her to get picked on and teased
after a soiling accident at school. “It’s only because they can’t see her disability. If she was
in a wheelchair, that’d be fine” said Grandma. Daily living skills such as shopping, washing
clothes, personal hygiene, working memory and some social, health and safety issues are
difficult. School mornings are difficult and Jenny has trouble with most chores at home.
She can dress and undress and do one morning chore but gets side-tracked with the others
though she got all three chores done before school for one week when offered a $50
incentive! Jenny said “it’s very hard to remember things … I can’t remember anything a
long time ago”.
The mother heard about NLD from teachers at school and from other parents whose
children had hydrocephalus. A Special Education teacher was aware of the syndrome but
“he was saying that Jenny doesn’t have it. She’s pretty good”. The mother and grandmother
thought Jenny was “a pretty good student at school” and she had caught up after missing 14
weeks from hospitalisation. The school displays a large picture of Jenny in the staffroom
which highlights her medical conditions. Her class have open discussions about Jenny’s

236
shunt and her back and everyone knows she must go to the head of the line to avoid a bump
or push. The class teacher “is absolutely lovely” and understanding about Jenny’s care needs
and the mother attributes this to the teacher’s husband being dependent on a wheelchair for
mobility. Jenny finds the school “very rough” and the kids are not very good about not
pushing and she worries about falling over. In class, the teacher is “basically it” and she has
no aide support for Jenny and 7 or 8 other students.
School days represent a pattern of chaos because Jenny cannot retain the class routine
in her head for a whole day despite good routines and a timetable on her desk. She tries very
hard to keep up, sometimes by watching others to figure out what is happening and at other
times “letting it wash over her head and doing her own thing”. Most areas of class work are
modified but work still needs much framing. She is in the lowest maths group and “I’m top
of the group”. Jenny likes drawing unicorns and writing about personal experiences but
writing is “really hard” when her hands get sore and tired. She has friends but not a best
friend and although her mother considered she was good with friendships, there were no
invitations to parties. Her happy resilient disposition helps her to fit in and any soiling
incidents are sensitively handled by the teacher who calls an aide and deflects attention from
the unpleasantness. “She’s always out there, always trying, always wanting to join in, angry,
upset, but not sitting around sulking and depressed or left out” said the teacher. Jenny gets
very heated and has been known to hit and her strong sense of justice means she gets 60%
more involved with conflicts than other kids. Some trouble with relationships may be due to
misinterpreting cues and communication with peers and inability to resist acting on impulse.
The teacher described Jenny’s days as “tough”. Psychological testing diagnosed Jenny with
Partial NLD, an Executive Function Disorder, specific impairments in the language domains
and her intellectual functioning was in the low average range.
Ryan
Ryan is in Year 4. He lives with one parent and 2 older brothers and he sometimes
visits the other parent. His shunt has been in place from 3 days of age. He needs constant
reminders in the mornings and the parent said “you feel terrible” when he is late for school
because he may miss the first 5 or 10 minutes of school “which is a really important time to
just get settled in and know what’s happening during the day”. Ryan walks independently
and said school is “great … I really love it”. School days had two different extremes, loving
and enjoying interaction with the kids and the teacher then having to sit down and do
individual work which he found “really very difficult”. There is no in-class support because
reassessment reduced aide time to 20 minutes per day which is used for special toileting.
The parent was critical of Education Queensland’s failure to acknowledge cognitive

237
difficulties associated with hydrocephalus despite well-documented literature. “It’s wrong
that they fund him for physical disability and that they don’t recognise that he has non-
typical learning requirements”.
A normal day for Ryan is physically, intellectually and emotionally more tiring than for
others. “He could get quite crampy and achy by the end of the day and intellectually very
tired”. His teacher integrated an open discussion about the “Walking Miracles” in our class
into a Science lesson. The benefits may have been twofold, classroom and playground,
because there were no reported incidents of bullying, teasing or meanness. He loves
playtime most “when I go to visit my buddies, the preschoolers” and he interacts with girls
and some of the boys. He has no problems in the playground and said most kids “know who
I am”. He is young for his years and finds some boys his own age the hardest group to get
along with because he is unable to manage high-activity play and they tend to exclude him or
treat him as an inferior in that respect said the parent.
Ryan enjoys basic maths and spelling but finding the big books in his desk is difficult.
Writing is tiresome and his left hand shakes so the parent bought a portable computer with
keyboard, scribe and voice recorder which he uses to record homework sentences. Science
presentations are impressive but his effort and persistence to stay focused is not recognised
and “people see him as lazy when he’s actually trying really hard” said the parent. The
teacher said colleagues sometimes perceived Ryan “as being lazy, as being a highly … a
very capable child, a bright child but perhaps molly-coddled at home, babied too much, too
dependent and because of that dependence that’s why he’s not able to do things
independently by himself. So because he’s so used to having everything done for him, the
perception is that he therefore can’t go off and write a short story about his weekend, which
he can’t, but for other reasons …” The aide felt he was quite capable of doing the work …
he knows the answer but getting him to write it down “I don’t know whether that’s laziness
or his disability”. Ryan had a lot of difficulties … “he needed to be told what to do, when to
do it and how to do it every time” said the teacher. He is very forgetful and his ability to
manage his desk is very limited. He also gets anxious and worried about friendships.
Skills needed for daily living such as memory, language and listening skills,
community usage, functional academics, helping around the house, personal care and
hygiene, independence, responsibility and self-control were reported to be severely impaired
and Ryan finds it hard to plan, start and finish any task alone or develop problem solving
strategies. The period leading up to recent surgery made Year 4 “a hard year for him … it
was a really tough year” said the teacher. When asked about an NLD, this teacher said

238
“Nonverbal, what is it? So is it a visual …? Can you give me examples of how that might
manifest”. Characteristics and cause of the syndrome were explained in layman’s terms and
the teacher said “he certainly has what you were saying when you were describing it. It
certainly matches what I find with him”. Psychological test results indicate that Ryan has
Partial NLD, an Executive Function Disorder, specific deficits in the memory domains and
his intellectual functioning was in the low average range.
Clair
Clair is in Year 6 and spends school weeks with her grandparents who take Clair to visit
her Mum, brother and sister on the weekend. She is usually at her best early in the day and
ready when the school bus calls. She uses a wheelchair and is physically very independent.
Clair experiences complex partial seizures which are a great concern to her grandparents and
school staff. Her shunt has been in place since 7 days of age. Clair was unhappy at her first
school and was sent to the Responsible Thinking Chair (RTC) every day for “yapping and
thinking of other things”. The school had no Special Education class or SEU. An aide
helped with toileting and special facilities were built after Clair left the school.
Clair likes the present school much better and said she has “billions and billions of
friends” and “they don’t think I’m mean”. The school gained permission for the nurse to talk
to Clair’s class about her medical conditions and how they can identify and respond if she
has a seizure. The teacher felt this would help students to “show some empathy towards her
because they knew what she was going through”. Classmates “love her”. They are very
accepting of children with physical impairment and the teacher had never heard any insults
to or about children in wheelchairs. Classmates don’t actually see Clair “particularly as a
disabled kid, she’s just a kid who happens to be in a wheelchair. The thing that makes the
difference is the epilepsy not the spina bifida. I know that sounds weird but that’s the
reality” said the SEC teacher. Grandma said the class teacher and SEC staff are excellent
and really in tune but they are sometimes “put off” by Clair’s expressive speech because she
does not always “catch things”. To ease Grandma’s concerns about homework, a carer
comes for 2 hours 2 days per week which is a considerable help. Handwriting as an isolated
task has become “perfect” with much practice but without close direction, “what you’ll get is
almost a loop where she will actually continue to repeat the same thing” said the SEC
teacher. Reading performance is way beyond book standard “but her comprehension of the
text isn’t there”. The class teacher thought Clair felt a little embarrassed about being part of
a group and being unable to keep up because “her opportunities for interacting in that way
are so limited”. The SEC adopts a differentiated approach to teaching which allows students
work in many different modes.

239
Clair attends a Friendship Group run by Queensland Health to help with social skills
which it is hoped will lessen her anxiety. She seems to keep things to herself which
probably caused her insomnia said Grandma. Social interaction is a big issue and the class
teacher did not think she had appropriate social skills to build friendships and her inability to
understand humour is an “ongoing problem”. Language functioning, even processing a
simple question is very difficult and anything new makes her very anxious so teachers try to
avoid changing staff and environment when planning a new activity. Daily living skills such
as using community facilities, personal care and hygiene, home living skills, responsibility
for herself, functional academics, language and listening skills were reported to be severely
impaired. She is unable to resist or not act on impulse and she finds it hard to generate ideas
independently, problem solve, plan, start and finish a task or regulate appropriate emotional
responses when changing tasks or situations.
The “wonderful teacher aides” at this school were valued as paraprofessionals. Two
teachers had heard of the NLD syndrome, one “only recently”. After explaining the effect of
damaged myelin on ability to make decisions and problem solve, this teacher said “that’s
classic for Clair”. One aide had not heard of an NLD but said “Oh okay, that’s interesting
isn’t it …? Well that seems to be Clair down to a tee but yeah she’s a good little talker”.
Clair’s primary developmental diagnosis was mild intellectual impairment and she was
diagnosed with an Executive Function Disorder. There was also an NLD profile of strengths
and weaknesses which made the problem even more functionally disabling and difficult for
people to appreciate how disabled she was.
Mel
Mel is in Year 9 and she lives with her parents and younger brother and sister and she
has a “really close relationship” with her great Nan. Her shunt has been in place since 3
weeks of age. Mel relies on a wheelchair for mobility and the parents have pushed
independence “all the way” and any teacher or student must ask first before pushing her
wheelchair. She finds it hard to tolerate input from her siblings and she gets “frustrated”
with the way her disability inhibits her life. The mornings are “rushed” and getting
organised within a timeframe are critical issues. The mother has observed Mel going into
her own little world and she hums to herself at home. The SEU at Mel’s school concentrates
on developing the student’s functional skills to promote mobility at school and in the
community and Mel enjoys these Physical Tute classes. She felt school was “pretty good so
far but it could be a lot better … not the education side of things so much it’s more of the
social side of things”. She gets on with “pretty much” with all of the wheelchair kids in the
SEU but sometimes kids in a group will ignore her and leave her out. Mel felt she got on

240
“quite well” with teachers and aides and can work quite easily with both which makes that
aspect of school easy.
Mel asked if I had done “much study on the social side of how people like myself
interact with friends”. At a recent clinic visit, doctors were concerned about clinical
depression which may have been partly due to “dynamics of friendships” she is struggling
with at school said the mother. Daily living skills such as handling money, leisure, using
community facilities, home living, social skills, and health and safety issues were reported to
be severely impaired. She finds it difficult to independently generate ideas, plan, initiate and
complete a task, problem solve and manage appropriate emotional responses. The mother
felt a culture of care and understanding for different learning styles should be developed at
school … “it might be another way to explain the differences between people”. To her
knowledge, there had been no class discussion or explanation of Mel’s disability since
Year 2. There were no reports of bullying or teasing but Mel found friendships difficult “she
has a fairly lonely existence in life” said one teacher. She had a general friend not a special
friend. The mother did not think school staff had received help with classroom strategies
but they could “pick each other’s brains”, “pick my brains” or visit the SEU for advice.
Oral skills are excellent, she has a “wide-ranging vocabulary” and she “tries very hard”.
A teacher who witnessed her presentations described Mel as intelligent, capable and bright
but said she finds organisation, working within a timeframe, starting and finishing tasks
alone, difficult. Teachers and aides remarked that Mel does not ask for help. Aides help
with all practical classes and they do the close one-on-one work. Some described her as a
“bit pampered, bit mollycoddled” and “more capable than we saw”. Mel said she gets along
well with the teachers and aides but thought teachers needed to “have a better understanding
of our disabilities and what kind of difficulties we have” to sort out a better way of “teaching
us so that we can understand”. The mother had not heard of an NLD and said “I think if we
can find out about the whole range of things that are impacting on these things for our
children, the better we are and the more we can help and it also flows over to other children”.
Mel had not heard of an NLD. No teacher or aide expressed bona fide understanding of the
NLD syndrome. After brief outline of the NLD profile, one teacher said “well I think that
would be quite accurate because she can verbalise but she doesn’t want to interpret things
clinically” while another perceived Mel to experience such difficulties “so perhaps that is
that condition or that aspect of it … I’d say that’s Mel”. A Science teacher observed that
Mel usually leaves hypothesis-testing questions blank “so that’s interesting because it
correlates with what you’ve said”. Psychological test results indicate that Mel has an NLD,
an Executive Function Disorder and her intellectual functioning was in the borderline range.

241
Josie
Josie is in Year 11 and she lives with her parents and younger brother. She uses a
wheelchair and has had her shunt from soon after birth. There is a lot of rushing, prodding
and reminding on school mornings because Josie doesn’t understand the concept of time.
Worst days are school days and although the mother finds she is “still doing a lot of things
for her that she should be doing herself”, she feels Josie still needs her help. “At least I can
get her to school a bit earlier or on time” said the mother.
The school is very critical of her late arrival and even though the mother is up until
12.00-1.00 a.m. the previous night getting organised, Josie is still late for school. Josie’s
start time is variable but “there’s pretty much not a day that she’s not late for school” and
even with the later schedule, some staff did not consider “that that’s kind of a big priority at
home”. Daily living skills like self-care and personal hygiene, organisational tasks, home
living skills, getting around the community, keeping to a schedule and time limits were
reported to be severely impaired. Both teacher reports and parental reports indicated that
Josie had difficulty with working memory, ability to resist acting on impulse, move freely
from one situation to another, regulate appropriate emotional responses, generate ideas
independently, set goals and develop appropriate steps to carry out an activity.
The mother did not think Education Queensland fully understood “the hidden problems
associated with spina bifida” and to her knowledge, there had been no class discussion or
explanation of Josie’s disability since early primary school. The mother reported a lot of
issues with first year students and their understanding of spina bifida and special toileting
needs. Josie’s present school had a Learning Support teacher, a Special Needs teacher and
teacher aides but not a SEU. The school is “very strong with physical independence in
regards to Josie’s wheelchair” but Josie’s mother reported that “independence has got her
nowhere only loneliness and heartache”. The mother tries to advocate for Josie “but teachers
think she is only the parent who wouldn’t know anything” yet she is the one confronted with
Josie’s sadness, unhappiness and the hard time she has accepting her disability. She said it
was “frustrating dealing with teachers”. Some teachers were confused about Josie’s learning
difficulties and whether she had physical and cognitive disabilities since they had only been
advised of physical impairment. One teacher who considered Josie’s verbal skills a relative
strength remarked that other students with intellectual disability do not have good
conversational skills. Some teachers associated Josie’s difficulties with the family’s
handling of her disability while others accepted the mother’s advocacy and advice. One
teacher felt the school had done a lot to help Josie with respect to purchasing a special
sewing machine and modifying the kitchen “you can lead a horse to water but you can’t

242
make it drink” and added she did not know how to “develop enthusiasm, I think it’s
something that’s innate”.
Friendships are difficult and Josie longs for a special friend. Loneliness, no special
friend and Josie’s difficulty conversing with students without misinterpreting aspects of
communication were concerns of school staff. When asked about student understanding of
Josie’s disability, one teacher assumed “a lot of work would have been done with her in
primary school but to some extent it really hasn’t been explained that much to me”. Even
though Josie’s mother had discussed her disability “there’s some kids in Grade 11 who have
no idea what’s wrong with Josie” said the teacher. There were reports of bullying incidents
at this school. Some kids make “really cruel jokes” about her wheelchair “they seem to think
my wheelchair’s a car” said Josie. On one occasion a teacher said “you’re a lot older and
mature … don’t take it to heart” as she talked Josie through the incident. “But outside of me,
it’s alright yeah … school’s, yeah I’m enjoying it” said Josie while the mother felt Year 11
was Josie’s best year at school with little or no homework and no major issues with teachers.
Seven out of eight teachers had not heard of the NLD syndrome and the one that had said
“yeah I have read some information on that”. When the shunting device was mentioned,
another teacher said “is that always there is it … no I don’t think … Josie doesn’t have that”.
This teacher was unaware Josie had a shunt for the hydrocephalic condition. Psychological
test results revealed that Josie had an NLD, an Executive Function Disorder and her
intellectual functioning was in the borderline range.
Cross Case Analysis
The assets and deficits that constitute the NLD syndrome are best understood in terms
of cause and effect relationships, namely, primary assets and deficits lead to secondary and
secondary lead to tertiary. Interview guide questions were similarly aligned. Since the focus
of research was to explore understanding of the strengths and weaknesses that comprise the
NLD profile, there was no deviation from interview guide headings and additional category
headings that emerged from both interview phases. For ease of cross-case analysis then,
responses to questions about primary, secondary and tertiary assets and deficits will be
thematically aggregated under the following headings –
Assets
Auditory perception Rote material Simple motor
Deficits
Tactile-visual-spatial perception Complex psychomotor Academic: Handwriting, reading comprehension, mathematics Novel material or situations Social and friendships

243
Perceptions of NLD assets
Auditory perception
Good auditory perception leads to verbal fluency, accurate pronunciation and fluent
verbatim repetition of what is heard. Initially, all parents confirmed their child spoke well
but most noted verbal comprehension was poor. Some children did not always understand
what they had said to people. Excellent vocabulary and ability to remember difficult words
was mentioned and one child preferred to ask the meaning rather than use a dictionary. One
parent thought the child’s language strength could be “capitalised on in high school” and
another believed teachers were “put off” by very expressive speech because the child did not
always “catch things” and it tended to mask other difficulties. A child whose parent reported
“good” verbal skills was found to have specific deficits in the language domains. Students
enjoyed reading and largely verbal subjects like drama and role plays. One student was
asked to read at the Year 12 Graduation. “I wasn’t even nervous about that ... I didn’t even
have any practices of that” and the mother said she read brilliantly and fluently.
Most teachers and aides described verbal skills as “excellent”, “very well-developed”,
“really quite quite outstanding”, “can talk about anything, has no trouble … tells lots of
stories”, “a good-little talker”, “speaks very eloquently”, “fine in that area”, “her forte is
going to be the verbal … I could see her as a radio announcer” but two teachers said one
student could communicate but was “not overly articulate” or the student was very quiet,
hard to hear and “doesn’t know really what she’s going to say”. An aide said excellent
verbal skills conveyed an impression that the student knew everything … “you think they’re
very high functioning”. Except for the child with receptive and expressive language
problems, teachers reported great, interesting, mature complex vocabulary, good command
of the English language, very precise and adult in choice of language and ability to use big
words appropriately. Oral presentations drew praise with the exception of one teacher and
aide who said the student was shy, nervous and “not a centre of the stage person at all” but
the student had “a great speaking voice” and could present to the class with aide support. All
students could verbalise sentences and ideas but they could not write ideas in sentences and
one could not write a sentence at all. One teacher overcame this by asking the child to draw
the story ideas in steps. Another said that although “very good verbal skills” were a strength,
they may not rate as highly if compared with other 16 year olds. “I guess I say ‘very good’
because the child has a disability whereas if I compare them to every other 16 year-old in
Queensland I guess you would say they were average …”

244
Perceptions of verbal skills ranged from “can communicate” to “really quite quite
outstanding” and expectations were commensurate with impressions that is, a child who
presented a captivating oral impressed parents and teachers. The general feeling was that
verbal skills were better than maths. Interestingly, Levine (1994) says children who have
trouble understanding questions, explanations in class, maths word problems and reading
comprehension, which were all problems for this group, may experience difficulty with
processing at the sentence level. Impaired sentence understanding may impede
memorisation and recall and tedious handwriting compounds the writing task. Auditory
perception may be an NLD asset to the extent that it aids receptive language, verbatim
auditory memory, rote verbal memory and learning but there needs to be “close examination
of the qualitative aspects of their linguistic skills” (Rourke & Tsatsanis, 1996, p.30).
Core inconsistency
The only notable inconsistency was between one child’s mother and the teacher. The
mother perceived verbal skills as “good” but the teacher regarded command of English as
“very poor”. Test results for this child indicated specific language deficits.
Simple motor
Simple motor tasks that improve with practice and increase independence may include
dressing, undressing and personal care. Various levels of personal independence were
reported. To compensate for slowness and poor concept of time in these areas, parental help
was needed to get the child ready for school. Three children were often late for school and
for one student; this was a major issue for school staff. The mother hated school mornings
and the school believed getting the child to school on time was “not a big priority at home”.
Rote memory
Teachers and students reported good rote and script-learning ability especially for
drama and role-plays. Students knew their lines at performance time whereas “half the other
kids had scripts in their hands” and in a group situation “if other kids had forgotten their
lines, she would always know everyone’s lines”. Students became animated when talking
about Speech and Drama. “I really loved that because basically that’s what I can see myself
doing as a career … I want to be an actress” while another said “I may like to become a
singer or an actress …”

245
Spelling
All stakeholders reported good or excellent spellers with the exception of one child and
parent who said spelling was good “she’s a good little speller” but the teacher reported
spelling as “very poor”.
Tables
The same parent considered tables “good for her age” because they were better
than those of her older sister who had ADHD, though such comparison may be an unreliable
measure of ability. Some teachers agreed tables had been learnt well by repetition and rote
learning but there was a core inconsistency between two teachers at one school.
Core inconsistency
“She would not know her times tables and does not know her times tables no because
she finds maths very very very difficult, really really struggles which I know is really
common for students with spina bifida”. The student’s maths teacher said class work “she
has done before and she can do and has been really trained well and things like her times
tables she was very good at and she would finish that very quickly …” This teacher
converted the student’s hatred of maths to “she likes coming and we do really good stuff …”
One might query whether the first teacher drew on experiential knowledge or did she assume
that tables would not be good if maths was difficult? Maybe I should have probed her
perception of concrete maths as distinct from problem solving maths. The literature says
concrete maths based on tables and fixed routines are easier than problem solving maths
because the latter demands interpretation, adaptation and integration of previous knowledge
and experience. All students were found to enjoy basic or concrete maths but all
experienced great difficulty with problem solving maths.
Perceptions of NLD deficits
Tactile perception
Tactile perception allows one to put their hand into a purse and from messages received
through the fingers, discriminate between a purse and a biro. No simple tactile imperception
was reported here. Little effort is needed to engage the sense of touch because “it can be
developed within the proximate space of even a virtually immobile child” and children here
were immobile for at least the first 2 years of life (Rourke, 1995, p.10). Frequent use of the
246
hands even in a confined space will likely lead to no “hard” signs of tactile deficiency but
problems with “complex tactile input tend to persist” say Rourke et al. (2002, p.157).
Visual perception
Visual perception allows one to accurately scan and process what is seen through the
eyes and intact tactile-visual perception is needed to locate books and writing apparatus in
the desk. Finding things in the school desk was a problem for younger students but was not
reported for older because of subject room changes though secondary aides complained
about students not getting pad and pencil out before the start of lessons. Younger children
could not find things in their desk and all spoke of trouble finding their “stuff”. One student
would spend 4-5 minutes looking for something and would almost be in tears … “it would
be there but he couldn’t find it”. The teacher exchanged the desk made for a child with
physical disability to a standard desk and this gave the child a big sense of pride to have
everything clean, tidy and organised. All students sat up front or centre front because it
helped them to read the board and one teacher said because the child needed sentence
starters, constant supervision and “spoon-feeding all day long”
Visual-spatial abilities
Visual-spatial abilities which allow one to form visual images, copy accurately from the
board, organise notes on paper, organise paperwork and file papers within a folder were
problem tasks for all children. Difficulty forming visual images affects ability to remember
shapes, sequences, objects in the environment and awareness of self in relation to them.
Faulty concepts result which make word problems and abstract maths that involve
perceptions of area, size, spatial relationships, weight and distance almost impossible for the
student to fathom. Writing from the board involves visual-spatial processing, visual
memory, recall and fine motor skills and varying degrees of difficulty were reported with
slowness and legibility being the main problems. There was some doubt about accuracy
because students looked at the board frequently and work copied was either very untidy or
had several cross outs. It “depends on the day” because attention, memory and recall are
important and days when the student is “out with the fairies” were “very frustrating” for
aides. Some teachers and aides overcame difficulties by providing handouts, taking turns
with writing, asking the student to read from the board while the aide scribed, using coloured
chalk to highlight sections to be copied, circling or underlining key words and phrases for
the student to copy as dot points or providing a sentence starter on a laminated card for
sentence-writing.

247
Academic deficits
Handwriting
Handwriting is a simple motor task that Rourke says may become “smooth and
effortless” with practice (1995, p.14). The majority of teachers and parents described the
child’s writing as “scratchy”, “scrawly”, “spidery”, “terrible”, “messy”, “large, poorly
spaced, crammed”, “illegible”, “childlike”, “not fluent” and “laborious” though one teacher
said it was not so difficult that “it’s a minefield”. There were two exceptions where children
practiced and persisted to lift handwriting performance to “beautiful” if the child felt well or
a reasonable size with “readable formations of letters”. All students were very slow and all
got sore hands quickly. One student could not write a whole sentence independently.
Writing on lines was difficult, writing tended to slant upwards and one child’s hand shook
when writing but this child believed writing was “pretty good”. Writing about a personal
experience was easier than objective writing and teachers reported great ideas but trouble
writing them down. One teacher observed better application and writing fluidity with
cursive writing than with printing, which causes one to ponder the benefits of joining letters,
continuous pen-paper contact and more focused attention. One teacher perceived the child
as “very capable” and without the obvious disability that prevents good writing “I think
there’s plenty going on up … up top.” Some parents and aides did the handwriting if the
child provided the ideas. One student enjoyed drawing unicorns but drawings of other
students were difficult to understand. Verbal homework instructions not written down or
scantily done caused problems at home because they were incomplete or illegible.
Core inconsistency
The simple motor handwriting task that Rourke said may “reach good to excellent
levels” was not entirely the case here (1995, p.3). One child worked hard to improve
handwriting and it is no longer an IEP goal. The majority of teachers considered writing a
handicap either because of illegibility and/or slowness which, in concert with other issues,
hindered ability to start and finish writing tasks at all or within a timeframe. All children
were provided the same opportunity as peers to practice handwriting tasks but time
constraints often led to sharing the task, handouts or not getting finished. To encourage the
child’s engagement with class and homework, one parent purchased a digital notebook
device with a scribe and voice recorder. He believed this would utilise verbal skills, reduce
tiresome writing tasks and help the child to keep up. If used as a substitute for handwriting

248
at Year 4 level, one might question whether the device might hinder potential for writing
improvement given the advances from routine practice by two other students.
Comprehension
All children enjoyed reading but comprehension of the text was “not there” and for
older students, following a recipe or interpreting a word problem was very difficult. To
improve comprehension skills, some teachers modified reading level to focus on
interpretation through questioning. One teacher said the student could “verbalise but she
doesn’t want to interpret things clinically”. As text becomes complex, skills are needed to
interpret implied meanings, new vocabulary, spot key ideas, follow a storyline and integrate
new with old knowledge and experience. For children who interpret language literally, such
complexity can be beyond their realm of expertise.
Maths
Teachers, aides and parents said concrete maths that relied on learned tables and simple
procedures were better than problem solving maths. Skills were described as “low”,
“struggling”, “fairly poor”, “very very very difficult, really really struggles”, “manages quite
well but nowhere near her same-age peers”. To consolidate basic skills, one teacher used
games, puzzles and “we make things” to engage multiple intelligences. One student who
knew her adding and times tables could not use this knowledge in a word problem about
adding and times tables “so does she really understand what times tables mean. I would say
that no it was just rote learning”. Problem solving maths … “no hope at all”, “would have a
go … would need help with interpreting” and anything abstract like algebra or trigonometry
was beyond all students. One teacher grouped students in pairs to reduce problems with
interpretation. One student said she was “horrible” at maths while others enjoyed basic
maths.
“Mathematics may be considered to be a language in its own right” because it consists
of vocabulary, syntax, semantic content, symbolic representation and makes use of
contextual knowledge (Rourke & Tsatsanis, 1996, p.41). Vocabulary and syntax are not
difficult for children with NLD but “the way meaning is attached to words and how these
words are used to convey meaning”, conceptual understanding of underlying symbolic
representation and appropriate understanding of context are problematic for children with
NLD. Children could handle concrete maths but nothing abstract such as area, measurement,
time, volume, algebra or tasks that required visualisation of an experience or situation. This
reinforces the notion that deficient tactile-visual-psychomotor-concept formation skills that

249
result from inaccurate memory of tactile and visual input, limited exploratory, environmental
and personal experiences, underpin mathematical and social difficulties.
Memory
Short-term memory requires information to be initially heard and understood correctly.
All teachers said students could not comprehend or remember complex instructions.
Reduced visual-visuospatial-tactile skills and immobility that reduced early exploration
hinder ability to memorise nonverbal information and form concepts about objects in the
environment such as throw-drop-pick-up, in-out, above-below, light-heavy, left-right, and
short-long. The rippling effect of such deficits will influence effective hypothesis-testing,
decision-making and problem solving. We use such skills when confronted with a new task
or situation when learned knowledge and experience is retrieved, adapted and extended to
deal with the new circumstance. Teachers, aides, parents and students spoke about “poor” or
“very poor” short-term memory except one aide who thought the student had an “excellent”
memory. Children were unable to recall what was done at school that day or on the weekend
or what they ate for tea the previous night. Lesson requisites from home were often
forgotten.
Core inconsistency
“Well I reckon he’s got an excellent memory. Concentration like staying on task is not
always good” said an aide. A lot of times “I put things down to being spoilt or lazy but I’m
probably wrong. I say that because I deal with normal children that don’t have any problems
and he’s so normal in every way to me that I suppose I jump on that and think he’s just being
lazy” but when the aide attended meetings with all the “hoo-ha” and discussion about
assessments “and I hear things that I think well maybe I’m wrong there about … maybe it’s a
problem he has”. At the time of interview, I did not discriminate between short and
long-term memory and the aide may have offered a collective response based on one or more
incidents. Nevertheless, I felt she was searching for reasons why and since the student is “so
normal in every way” possibly because he walks, runs and jumps and can “talk about
anything, has no trouble”. The aide thought family life was “a bit chaotic at home. I could
be wrong about that” but such comments tend to put the family in the firing line for subtle
but persistent problems being experienced at school. If teachers and aides spent one week
with any family, they would become aware of a penchant for independence on everyone’s
part to ease the strain of maintaining daily routines. To save unfair apportion of blame, all
stakeholders have a vested interested in sharing their corner of the world at an annual
meeting between parents and school staff.

250
Planning, organisation and time management
Planning and organisational difficulties caused major problems for all students.
Teachers and parents described planning and organisation skills as “poor”, “shocking”,
“awful … even motor planning ‘how do I get these books out of my desk’ is difficult but
planning a task, just doesn’t know where to start, is dumbstruck … needs to be told what to
do, when to do it and how to do it every time”, “definitely needs help with that”, “really
struggles”, “organisational skills she’s lacking”, “no she’s not good. Her desk is an absolute
mess despite how many times we clean it up, she can’t find things …” Teachers spoke about
difficulty getting organised to start a task, stay on task, process and work from a set of
complex instructions given once. “It’s that chaotic pattern of being in the classroom” and
not cottoning on quickly enough to what’s happening next “now we’re going to the carpet,
‘right we’re going to the carpet, now where will I sit’, you’re sitting with me and then ‘why
are we on the carpet again, what’s happening here’”. All students needed individual support,
small-step instruction and constant supervision to stay on task and without it, they would
give up, feel they were getting nowhere and “fuss around the whole time and miss the point
of everything”. Individual support, structured routines and willingness to make plenty of
allowances helped them be included.
Teachers at one school worked on organisational skills for two years. It took strict class
routines, direct teaching, additional visual and verbal cues and checklists. The child now
rarely forgets to bring a pencil case to class. Previously, organisation skills were very poor
“Where’s your pencil ‘I don’t know … I’ve lost it’”. Forgetfulness with messages, constant
reminders and highlighted diary notes did not always ensure cooking or lesson requisites
were brought from home.
During an informal chat before class, one student would “babble about things” which
did not make a lot of sense and the teacher thought this reflected organisational problems.
The teacher used these times to get to know the student otherwise you would only know her
as “someone who’s always dropping her bag on the way to class”. Students in wheelchairs
seemed more prone to drop things off their lap and one parent reported a teacher saying
“you’ve got to be more organised”. One teacher picked papers up four times before the end
of lesson and another child often forget to close the ring binders with obvious consequences
when she dropped the folder. Poor assignment planning skills were compensated by aide
support, prompting and supervision but even then, some work was never finalised to the
point where it could be submitted but if the teacher or aide phoned home, work usually got
finished. Some staff wondered if trouble starting and finishing tasks was due to laziness,
spoiltness, having too much done for them at home or total lack of confidence and not

251
wanting to submit work for rating. Organising ideas coherently then physically writing them
down “just seems too hard so he won’t” said one parent. Another child had plenty of ideas
but “what am I thinking and how do I say it on paper”. Teachers and parents reported poor
ability to complete class work, homework or assignments within a timeframe. All teachers,
aides and parents said concept of time was “poor”, “difficult”, “struggles with that”, “not
wonderful … ‘I just do spontaneously what I do until someone says stop’”, “got no concept
of time and doesn’t wear a watch anymore”.
Parents said poor organisation, concept of time and short-term memory made mornings
troublesome for students and at times for the child who was “at her best at about 7 or 8
o’clock in the morning”. It took years to get children into a morning routine and still,
constant reminders, lists and alarm bells were needed. Organisation and time management
problems impede effective task planning and completion and impaired visual, spatial skills
and forgetfulness make it difficult to keep tabs on possessions, such problems compounded
for students in wheelchairs.
Core inconsistency
One Special Needs teacher made comments different to the others. “It’s not her fault
…”she would say to teachers who she had seen “get incredibly annoyed” about the
disorganisation and unpreparedness of the student with hydrocephalus. “If I’d had a dollar
for every time I’d said to somebody ‘it’s actually a part of the condition, she’s not doing it to
upset you, please just build the extra prompt into your day … They’re not disorganised to
annoy you and they cannot take responsibility for doing things”. Teachers and aides at two
another schools attributed poor ability to finish tasks to students having too much done for
them at home, other people organising and thinking for them and students needing to take
more responsibility for finishing homework and packing their schoolbag. The aide felt by
senior high school “you would be packing your own bag; bringing your own subject
notebooks … I would have thought you would be in complete control of your own school
bag”. One parent thought the 5-subject book worked well but in the school context, an aide
said it was a fair-size, quite heavy book and the student “wasn’t organised within herself to
keep that consistency from class to class” so maybe individual books with colour-coded
covers might be better. The latter worked for another student whose parent labelled each
corner front and back to help finding in the desk. Reduced grip strength, visuospatial
perception and poor organisation might make individual colour-coded subject books the best
option for students with hydrocephalus.

252
One teacher said it was difficult to judge time management skills because there was
always an aide present and the student did not have to manage her own time. Post-school
“I’m pretty certain there’s not always going to be an aide or a helper around so I sometimes
don’t know whether we’re really doing the best thing …” Post-school is when functional
difficulties become magnified when children lose aide support and try to enter the
employment market . If learning and task handling problems are blamed on laziness, being
babied or spoilt rather than addressed as neurological dysfunctions, how can teachers and
guidance officers recommend suitable employment options? The child may suffer dismay
and isolation as peers forge ahead vocationally and socially which leaves families struggling
to make life productive and fulfilling for their young people. Isn’t there a need to tell
teachers, guidance officers, parents and students about the NLD syndrome to prevent
unrealistic advice leading to disappointment in the workplace?
Complex psychomotor
Psychomotor skills involve both mental and muscle activity. Gross motor activities use
large muscle groups to coordinate body movements to walk, run, jump, skip, hop, ride a
bike, throw and catch a ball, cross the road and maintain balance. Fine motor tasks require
precise coordinated movements to do buttons, zips, shoelaces, cut with a knife or scissors,
glue, paste, hold a pencil correctly, write on lines, use a rubber effectively, dress, undress,
knit or sew. Two children walked independently and one of those could ride a bike but she
had issues with safety. All parents had reservations about their child’s ability to cross the
road safely and spoke of hesitance, extreme caution, clumsiness and poor road sense. Such
restraints could result from impaired visuospatial perception and impaired peripheral vision.
Level of fine motor competence varied and only one child could fully dress and undress, do
shoelaces, buttons and zips though not at the back. Another student had learnt to dress and
undress by age 10 but had trouble with buttons, a wet swimsuit and pulling socks “on and off
sweaty little feet” on swimming day. When shoelaces were done, hands were not strong
enough “to make them actually work so there’s no incentive for him to learn to tie them”.
An aide said one primary student should be able to tie shoelaces and asked repeatedly if a
parent could show the child. When the problem with shoelaces was raised by the parent, I
suggested toggles to help independence. Some parental help was needed for children in
wheelchairs although they could dress and undress from the waist upwards, do buttons with
some difficulty and one parent only bought “pull-on pants so that it increases again her
independence.”
During office training, teachers observed an older student struggling with organisation
on the desktop, folding paper before inserting into an envelope, opening a folder without

253
jumbling the contents and putting receipts in plastic pockets neatly but with practice, the
student “got a lot better”. All children could make a sandwich with soft butter but none
could lift anything very heavy in the kitchen … maybe a meal for one but not a saucepan of
potatoes and students in wheelchairs needed the stovetop to be at their level. “There’s a lot
of problems in there with a simple task … simple for us but it becomes more complicated
because she’s in a chair”. Using a ruler to draw a straight line was difficult and one parent
provided a ruler with a finger grip. Two students could handle scissors, glue and paste while
the skills of others were described as very awkward, “terrible”, “struggles”, “difficult”,
“slow”, “cautious”, “doesn’t like making things”, “it’s not brilliant but it’s okay”, “a little
difficult … it wouldn’t be neat”. During a practical lesson on fractions where colour-coded
step-by-step instructions were put on the board, one student “could not divide a piece of A4
paper into eight bits … it started off well when I was there showing her what to do and as
soon as I went away, she just had these lines that was this thing and she was supposed to be
doing something that was 9 cm apart”.
One student learnt to knit and although the end product looked like fishing net, a
relative tidied it up. Older students enjoyed chopping tasks in the kitchen but were slow and
determined to have everything the same size … “if I say ‘chop roughly’ it’s still got to be all
precise even though she has difficulty with the knife”. Another was tentative in the kitchen,
very awkward with some cutting, did not use her left hand unless prompted and recently the
aide “noticed she had the knife, the cutting knife upside down. Well I couldn’t wait too
many times for that ‘cause she was going to end up cutting her finger”. The essence of a
lesson on fractions was to measure ingredients, one-third of a cup of corn then double it, and
the student “couldn’t do it” nor could she follow the recipe without the teacher pointing to
the words on the packet. If cutting thin salami or cutting a sandwich in half, one student
needed reminding to apply pressure “down on the knife” to cut through to the board. In a
cooking lesson “the very first thing is just the name of the recipe” then the student would
stop until asked “‘well what have you got to do next’” and students really had to think about
it. One student could cut an apple in half and another could cut it into four once told “how to
cut and how to sit it”. Teachers and aides agreed that students could not cope without
assistance in the kitchen because of fine motor and organisational demands and time
constraints.
Core inconsistency
Measuring one-third of a cup of corn, doubling it and reading the recipe on the back of
a packet mix are complex tasks for a student with right hemisphere dysfunction. Maybe the
teacher did not take some “hidden” issues into account. This child only used her left hand

254
when prompted so manipulation and coordination were compromised. It is not uncommon
for children with spina bifida to have “pudgy, undeveloped and weak” hands and impaired
processing ability and manual dexterity would be a further hindrance (Mattson, 1982, p.227).
Although standard-type language is used on packet mixes, simply written instructions can be
overwhelming if they include opening a tin, tearing a flavouring sachet and pouring boiling
water because they utilise grip strength, coordination, dexterity plus visuospatial awareness
to pour boiling water. Such problems with “simple” everyday tasks can be frustrating and
the aide thought “everyday activities should have started a long long time ago right down the
track, not once a student gets to high school and we get into life skills. Maybe those life
skills should have been started way back when they first started school so that they’ve had
lots and lots of practice”. Parents may expect the child to pick up everyday tasks as other
children do by watching and trying and when problems arise, they allow for setbacks and
offer support to help the child meet deadlines and protect their place in mainstream. It
comes as a shock when the child reaches adolescence and their lack of everyday skills is
obvious. This is when accusations of laziness are used loosely, another reason to educate
parents, teachers and aides so that early identification of the NLD profile allows early
intervention on all fronts.
Novel material or situations
All students functioned best with a strict routine and all found any change to that
routine difficult to handle. If a library time changed, one child could quite easily go
“without a book if it wasn’t at the time that we always go” and if toileting routines were
interrupted, students needed reminders to get back on track. Responding to spontaneous
events and answering questions was difficult and responses were often delayed because of
slow mental processing. One teacher said this delay often caused people to perceive the
student as “rude”, but she needed extra processing time. Abstract or creative work was
difficult to grasp but “things that are straight ‘Put the Answer in Here’” were not too bad.
Work learned a certain way could not be transferred to a new context, for example, for the
first week of school, one teacher did not write a fraction on the board. “We did a lot of
cutting and colour and a lot of fitting fractions into different areas and measuring them and
talking about them but not actually any writing” which was completely new. All knowledge
was previously learned but the student could not transfer or adapt it to the new context. To
promote independence, one student was taken shopping to get wheelchair experience with
gutters, footpaths and shop entrances. The student was extremely nervous with every new
situation and would tense up to the point where the white on her knuckles could be seen as
she gripped the wheelchair arm. Another child became extremely anxious about swimming
lessons and each week insisted on knowing which staff member would accompany her in the

255
pool. She would hold onto that person so tightly that she caused bruising. To reduce anxiety
about any new situations, teachers now ensure this student “has a base of familiarity whether
that is a person or an environment”.
Social and friendships
Parents of younger students said their child had friends but only one had a special
friend and this child got anxious and worried and had been “in tears” about friendships.
Another child “would love to have a friend” and attends a Friendship Group to improve
social competence. Although she “gets on well with the kids in the class”, she is isolated
from classmates during play breaks because she prefers to visit the SEC where she is happy
to sit and watch others play games. The family felt the good relationship between student
and classmates was more “like a caring type of thing not on a friend level” and they said
“there’s never any invitations or vice versa”. The student did not seem to understand that
some things she says might not be appropriate for other people and the teacher thought social
skills were a major problem …“I wouldn’t think that she has appropriate social skills to build
friendships on”. Socialising was a difficult task said the aide because the child “just doesn’t
get it you know how people are with each other, what’s rude and what’s not rude” and has
much trouble recognising and responding to humour. To help the student, a large section of
the IEP focuses on social pragmatics and use of language, and a tweaked teacher-pupil ratio
allows staff to work closely with the child. Another student got on well in class but had
trouble in the playground and was “probably 60% more involved than other kids” with any
altercation. Overall, the teacher felt the child would not pick up nonverbal cues from her
peers and if she did “it’s probably the wrong message or it’s misinterpreted … it’s got to be
very clear in black and white”. Relationship help within the playground was considered a
need for this child. The parent observed there were no invitations to parties because the
child was “no good like that”.
Teachers of older students expressed concern about lack of friends and loneliness. One
parent said the child had had a number of friends over the years but she did not pursue
friendships. When two friends relocated, she would not ring them or write a card and when a
current student phoned, calls were not returned. The parent said “I know she’s got some
friends at school that aren’t disabled children but none of them ever ring her, ask her out”
and “she’s never been to any parties since she’s been at school … in high school”. The
parent added “as they get older that gap gets bigger”. This student expressed concern about
the social side of school and asked if I had “done much study on the social side of how
people like myself interact with friends”. I mentioned some literature reports that discussed
social interaction. Some staff thought the student had a group of friends but not one

256
particular friend. Part of the reason was attributed to the student having had “a lot of
difficulties to deal with, a lot of hardships that other people never go through and mostly
contact with adults”. This teacher thought she had a “fairly lonely existence in the life that
she leads” and part of it is that she herself is very shy in class. Even if she wanted to or was
open enough to make a lot of friends, she would find it perhaps difficult “to find someone
who’s really at her level”.
Staff at another school talked about another student’s loneliness, issues with friendships
and made comments like “she really really wants and longs for someone really close in
friendship but doesn’t really have someone”, “she’s probably very lonely … she says that
she has certain people as friends but I think at the same time she feels very lonely and she is
concerned about friends”. At lunch breaks, this student sits in her wheelchair in a central
covered area of the school where she was observed talking to herself “at lot” when alone.
One teacher thought the student had some friends but since she likes to sit in the same spot
and the other students like to wander around the school, she is left sitting by herself much of
the time. Two teachers said other parts of the school were wheelchair accessible but maybe
the student expects people to come to her rather than “she follow them”. “She doesn’t
always advocate for herself” and the one teacher taught the student how to ask for wheeling
help to access other areas. Teachers are careful about stopping to talk because “everyone’s
in a rush. If you are in a rush you can’t spend too much time with her because it will be a
very long conversation” but the mother said one year a teacher did stop and said “‘haven’t
you got any friends to go and sit with’ and that was the truth, she didn’t have any friends to
go and sit with”. She did not have a bosom buddy, anyone in particular or anyone on a
regular basis. Maybe “one day a week she’s got company, she’s doing something, she’s got
friends around her but it’s certainly not every day”.
During one lunch break, a group of younger students were bullying this student and she
became very upset. They regarded her wheelchair as their car and asked for it back.
Because she lacks confidence to confront someone verbally, the mother said her daughter
“suffers in silence”. Friendships were now 200% more important than independence and the
mother thought problems stemmed from toddler years when she spent a lot of time growing
up with adults and was “not exposed to groups of kids talking” to learn interaction skills.
Understanding humour and sarcasm was also difficult and this student had to check the
expression on the aide’s face if she said something cheerful but if a student did it, the aide
thought “she would definitely take it the wrong way … and I think she’s been upset quite a
few times with comments from students that to be honest, they haven’t really meant what she

257
thinks they’ve meant. So there is definitely that misunderstanding and I feel that she has
great difficulty communicating with her peers”.
Core inconsistency
Maybe the student sat in a central spot because she felt safe there or maybe she thought
more people might stop to chat. Fortunately, a teacher came to her aid after the bullying
incident and later “yelled” at the culpable students. She told the student she was a lot older
and mature and should not to take it to heart. When composed, it may have helped the
student to retell the incident so the teacher could explain different ways of interpreting and
responding in the future. From a constructivist-perceptual view of reality, this teacher felt a
senior high school student should be able to deal with the Year 8 students because “she was a
lot older and mature” but given the teacher aide’s understanding of the student, she may
consider the communication and situation misinterpreted by the student. Whichever is the
case, I don’t think either staff member realised the genuine difficulty experienced by the
student with interpreting and handling such situations. These students actually become
fearful and scared because they just don’t know what to say. The parent and one teacher
attributed friendship difficulties to frequent hospitalisation and insufficient exposure to age-
peers in the early years. No-one seemed to realise that problems with social interaction and
developing friendships can be tracked back to deficits in visual-tactile-organisational
perception and psychomotor domains. Deficits in these areas are the origin of dysfunctional
social skills which are discussed later.
There was a noticeable absence of bullying reports at schools where teachers had open
class discussions about the challenges faced by the student with spina bifida and
hydrocephalus. The teacher who assisted after a bullying incident was unaware that the
student had a shunt but she was interested to hear about hydrocephalus, its implications and
NLD. Speech assessment for all students revealed there was much in their world that the
child did not comprehend fully and there was much in communicating their ideas that each
child found difficult. I believe teachers do want to know more. The teachers, aides and
parents to whom I explained the link between hydrocephalus and an NLD, every one made
comments like … “well that makes so much sense”.

258
How did Education Queensland, teachers, aides and peers perceive students?
Education Queensland
One parent said Education Queensland do not recognise that a student with spina bifida
and hydrocephalus has non-typical learning requirements but only looks at physical needs
which carries “no funding for cognitive issues”. There is a medical reason why this student
cannot fully access the school curriculum and the disability could be addressed through the
system rather than trying to make the student work harder or tying to make the parent work
harder at home. Education Queensland website lists some physical impairments that may
cause cognitive problems and spina bifida is not one of those listed. The body of knowledge
is there yet “we just can’t get the Education Department to say ‘yeah it does, let’s address it’
and I don’t know why”.
Parents cannot hope teachers will “find out that hydrocephalus involves a learning
disability and you’re relying then on parents who might or might not be emotionally strong
enough to go and advocate for their son or daughter. It is tough to watch the child get
discouraged because of failure to meet expectations held for all students. One parent felt
Education Queensland should teach teachers more skills for evaluating different learning
styles rather that just give them access to a range of tools. They should also provide more
funding to make direct instruction methodology available to those who need it. Parents
believed they should be involved, assertive not aggressive and advocate strongly for their
child “especially with the Education system, as it does not seem to fully understand the
hidden problems associated with spina bifida”.
Past school experiences
A Year 2 child received a detention when unable to collect textas from a classroom.
She “couldn’t get into the classroom unassisted because she couldn’t reach this chain to pull
down and because she didn’t get to pick up the textas, she gave her a detention”. The same
child was placed in an upstairs language class which required a stair-walker and helper.
Delayed access to the storage room and walker caused lateness for class and the child was
given a detention. Another student got “quite a few administration detentions” for not doing
homework then failing to present at lunch break to do them. One family stayed up till 9-10
p.m. to help the child finish a writing task and the child was “so proud that she’d done it and
completed it” but the teacher did not look at the work next day. The father said “teachers
don’t realise, and you can’t really blame them I suppose, what is actually involved over these

259
sorts of kids you know, there hasn’t been the training”. A parent’s visit to the maths teacher
to discuss trouble with algebra revealed that the teacher did not understand the student’s
short-term memory and recall problems. Year 1 was a difficult year for one student because
she was always in the Responsible Thinking Chair (RTC) because the teacher “thinks I was
doing the wrong thing and I didn’t do anything wrong. Remember I hate that school”. Past
school experiences for another child were “like walking … hazardous but he has had a good
run”.
Teacher understanding of the medical condition
The family of an independently mobile child with a fragile back and a shunt said the
school expected she could do what other students do until people from the Spina Bifida
Association came to explain the condition. The family reported a perception that all people
with spina bifida depend on a wheelchair or walking aid and teachers must realise that even
if the child is mobile, they are not like any other child if pushed over. Lack of continuity and
communication, poor organisation, bad planning and many issues involving young first year
teachers who did not know or understand special toileting needs were reported. Every year
the child had a new primary teacher, one parent had “to sit and go through everything, the
medical history and the learning difficulties” because student information was not shared
between staff from one year to the next. Prior to starting high school, one parent presented a
seminar about the student’s medical condition for prospective teachers. Questions were
welcomed and a reference book left at the school but the student believed they “didn’t bother
to listen basically”.
Some parents said teachers acknowledged the obvious effects of spina bifida on
mobility but “they’re not aware that you’ve got the shunt”. The student said “yeah how do
they expect me to go around every new teacher and point out that I’ve got a shunt. I’m sick
of doing that … I’ve done that since Grade 1”. The subtle effects of hydrocephalus on
learning need to be highlighted to which the student added the “fact that it’s basically two
disabilities”. One teacher was unaware of the student’s shunt. “Is that always there is it …
no I don’t think … she doesn’t have that”. Another teacher’s lack of knowledge about
hydrocephalus led her to read all she could because “it can be a nightmare for both parties” if
the child is not comfortable with the teacher … keep asking till you find out what you need
to know until you feel comfortable”.

260
Teacher and aide understanding of learning difficulties
Teachers and aides observed a need for continual checking on all students. “You can’t
assume that because they’re not disrupting your lesson that they are performing at their
optimum level because the chances are that they’re not”. The secret of having a child with
spina bifida and hydrocephalus in the class was to get the class to help by developing a class
culture of support and understanding said one teacher. Adaptation and protection were
needed and firmness about “no, there will be no teasing” and “yes there are special
requirements for her like anyone else with a broken leg or physical problem”. Provide
support that the child can rely on and make plenty of allowances for accepting “that is as
much as she can do and that’s great and that’s fine”.
Difficulty understanding the disparity between younger and older students with spina
bifida and hydrocephalus was raised. Because younger students “function very well on a
concrete level”, the gap between them and age-peers is much lower but gaps widen in middle
and upper primary school with demands of “more complex higher order processing” said one
teacher. When colleagues showed incredible annoyance about disorganisation and
unpreparedness, she stressed “they’re not disorganised to annoy you and they cannot take
responsibility for doing things … it’s not her fault and it’s one of the things that if I’d had a
dollar for every time I’d said to somebody ‘it’s actually a part of the condition, she’s not
doing it to upset you, please just build the extra prompt into your day’”. The family believed
the child got on “very well now” with teachers and aides but thought staff was put off by
“very expressive” verbal skills because she does not always “catch things”. A desire to
please made this child easy to teach and teachers’ believed it was their responsibility to
devise the best way to teach what she needs to know. Flexibility and willingness to modify
tasks without trying to fit the child in with everyone else worked well and patience, a sense
of humour, and compassion help one to realise “that it is a struggle for them and that their
little minds do think in a different way to ours”. One teacher felt difficulty with social
interaction and meaningful friendships was unfair and “awful” given the physical issues the
child must deal with. Praise was heaped on “wonderful teacher aides” at this school. They
are “not mixing paint” nor are they “totally at the direction of somebody else. They are
having to think on their feet” and Education Queensland should recognise Special Teacher
Aides as paraprofessionals over and above the standard recognition of what a teacher aide is.
Some teachers at another school perceived the student to be “lazy”, “a very capable
child”, “a bright child but perhaps molly-coddled at home”, “babied too much, too dependent
and because of that dependence” was not able to do things independently. An aide who
blamed difficulty staying on task on being “spoilt or lazy” stated she may not know enough

261
about the child’s limitations. She did not know about the affects of slow mental processing
on task completion and said “I only see a little boy and I’m a Mum. I only see what I think I
see and I have no qualifications to see there might be a reason for these things”.
Educators of older students had trouble understanding difficulties with the nonverbal
aspects of school life. “Maybe as teachers we don’t fully understand all the implications of
her medical condition on issues like decision-making and problem solving”. They
understood that spina bifida had caused wheelchair-dependence but expected she could make
an easy decision such as “do you want this green thing or do you want this red thing.
There’s no right or wrong answer … and maybe we don’t understand … it’s not because she
hasn’t matured or grown up it’s just that she can’t like she’s not skilled in that area because
of her mental condition”. At one school, a teacher did not think the student had any
difficulty with the actual work … “I think she can complete most of the work and is really
able to do that” but some maths concepts were not grasped. Learning difficulties within
academic subjects were thought to stem from mental processing and problem solving “what
do I do next”, staying focused and managing time. Following verbal instructions given to
the class was difficult. “It’s like she’s day-dreaming … it’s almost as if she thinks I’m
talking to everyone else except her” and one teacher was concerned about the student relying
on individual teacher instruction to keep her on task. The teacher expressed frustration when
no aide was present and there were 20 other students to consider. One-on-one help was
needed to walk students through comprehension of written text and word problems. Older
students would not ask for help and were observed rolling their eyes, drifting into their own
little world and looking spaced out.
Based on a good command of the English language, quite outstanding oral skills and
sophisticated vocabulary, one high school student was perceived to have “lots of potential
but I don’t think it’s really being tapped and promoted as much as it needs to be”, “quite
bright but not showing her true potential for whatever reason”, “a very capable student … I
think there’s plenty going on up top”, “more capable than people are giving her credit for”
and there was “obviously a lot more going on there than you see from the front”. One
teacher felt the student had “plenty of brains, plenty of ability” but thought there was
overcompensation somewhere along the way which prompted her approach to unfinished
homework “no, if she hasn’t done the right thing, she’ll get the detention the same as
everyone else”. One student was thought to be a “little bit pampered and a bit
mollycoddled” and was not being pushed the way she should because she was in a
wheelchair. Older students were thought to have become too reliant on teacher aides and
when the aide was away, the student was not keen to do much on their own. Aide support

262
meant the student did not have to manage their own time or work independently but it helped
them be included. “I sometimes don’t know whether we’re really doing the best thing for
her” said one teacher.
Staff at one school spoke of frustration and some questioned the student’s intellectual
status. They found it deceiving because the student appeared “quite switched on and doing
really well” yet some things she needed constant reminders about. Lack of independence
received considerable focus and appeared a pressing issue for some. An aide felt she should
“cut the apron strings” and let the student try things out herself. At another school, aides
reported frustration with older students who needed prompting to get their pencil case and
book out before the start of a lesson. One aide spent time reflecting on her interaction with
the student and on ways she could improve her response to certain issues and her delivery of
new life skills. One teacher spoke collectively “I don’t think any of us understand. We’ve
been told she has no intellectual disability, there’s nothing wrong with her, she hasn’t been
ascertained, there’s nothing wrong with her mentally, she only has a physical disability when
it’s quite plain to see that she doesn’t just have a physical disability so we don’t know what
is it and why won’t anyone acknowledge there is something”. Another teacher felt they
would all learn from my study “I think we’ve got lots to learn and lots to keep in mind and I
think there can be a frustration level especially when people think she has a physical
impairment she doesn’t necessarily have an intellectual impairment so I think teachers
struggle with that ‘well why can’t she do this’ …”
Peer understanding
Primary students seemed to fare better than older students. One primary teacher asked
the school nurse to talk to classmates about the child’s medical problems, another designed a
Science lesson segment about the Walking Miracles in our Class to give every child
opportunity to speak about any significant illness, operation or disability and another teacher
facilitated open discussions about the student’s back and shunt. No derogatory comments to
or about younger students were reported but teasing occurred at one school if there was a
toileting accident.
Parents of older students did not think their child was understood by peers and no open
class discussions were reported “I don’t think that her classmates probably understand very
much about her at all. I think if they did then the dynamics that she’s had in the past couple
of years probably wouldn’t have ever happened”. The parent was not aware of any class
discussion about student differences and said students “don’t have to have a great deal of
knowledge just a little bit so that they have a little bit more of an understanding at a tolerance

263
level”. “When she was in Grade 2 they did but no, not in the time that she was in primary
school, only Grade 2”. At another school, some teachers thought much work would have
been done in primary school “but then to some extent it really hasn’t been explained that
much to me … There’s some kids in Grade 11 who have no idea what’s wrong with her”.
Another teacher did not think “they truly understand what it is that’s wrong with her” and
even if they did, she wondered “whether that would change anything particularly but it may
make you stop and think a little bit more”. Bullying “does happen but it doesn’t happen on a
day to day occurrence. It’s a one-off sort of thing and well not a one-off thing … it does
happen but not all the time and then she has students who do help her … she just needs to get
some confidence … ”
Wheelchairs
Students could manoeuvre wheelchairs around cement areas but sometimes needed help
on carpet or grass. One parent felt lots of issues started in primary school because it was too
physically tiring for the child to access where other kids were playing. Before pushing the
chair, this mother stressed that any teacher or student must first ask the student’s permission.
One teacher felt providing help to the student was “the friendliest thing to do because you’d
like to encourage the kids to do basic things”. A very strong school approach towards
wheelchair independence was reported by another parent. When the child was offered help
to navigate classroom carpet, the aide said the student was “meant to get over it herself,
you’re not meant to be helping her”. The family believed loneliness at lunchtimes was
because this student could not access areas where classmates were sitting though teachers
said these areas were wheelchair accessible and one teacher had been training the student
how to ask a peer to help her reach these areas. The mother wrote to all staff to “make it an
issue”.
Help for classroom teachers
Teachers and aides found it difficult to get students to want to work … “I don’t know
how to develop enthusiasm”, “how do I get … to want to because he doesn’t simply want
to”. A teacher spoke of in-service training that explains “kids with short attention spans and
behavioural difficulties learn a certain way and I know what those ways are”. “I learned at
uni how I can teach students like this but I don’t know anything about what can I do for … to
get her learning”. “What do you do if the traditional instruction doesn’t work with her and
the more visual hands-on work and using multiple intelligences “if that doesn’t work either,
what does?” There appeared to be no formalised help arrangement for teachers on an annual
basis. An occupational therapist from Spina Bifida and Hydrocephalus Queensland offered
advice to one primary teacher and a speech pathologist provided 6 weeks therapy to another

264
primary student. Apart from a visit in Year 8, another parent said “I don’t believe that
they’ve had any help with classroom strategies. However they could possibly “pick each
other’s brains” or “go up to the unit and see if they had any strategies”. In primary school
“they often used to pick my brain”. People from SBHQ visited one student in primary
school and wanted to visit before the high school transition “but that never happened”. A
visit to ease the junior-senior transition “wasn’t a very successful trip because it just stuffed
up” said the parent. See Appendix F for Helpful hints from this study for other teachers and
aides.
Summary
Parent, teacher and aide views were consistent with reports in the literature that students
with shunted hydrocephalus related to spina bifida display the NLD phenotype to varying
degrees. Good verbal skills and vocabulary were acknowledged though some teachers and
aides were more insightful than others because they probed below fluency and vocabulary to
examine content and meaning. Some educators seemed unaware that slowness with mental
processing, motor tasks that involve personal care and a poor concept of time influenced the
student getting to school on time. Good rote memory skills were acknowledged and inability
to use learned tables and simple procedures in a new context was observed.
Most teachers and aides had great difficulty understanding problems with the nonverbal
aspects of school life such as planning, organisation, initiating and completing a task,
decision-making, problem solving, managing time and comprehending and following
instructions. Poor decision-making ability was often blamed on the student having someone
to think and speak for them and inability to start and finish a task was sometimes blamed on
the student being lazy, babied, spoilt or having too much done for them at home. Some
parents and teachers attributed problems with the social side of school to frequent
hospitalisation and having spent younger years in adult company. Inability to converse with
peers at one school was blamed on the family and the student who have “held her back” and
deficient life skills were considered the student’s issues or a “family dealing with” the
student’s problems. It was hard for teachers to know what decisions a student could make
because there was “such a high level of dependence there in a range of areas of her life not
just physical dependence but the ability to solve all her own problems and even the ability
for her to choose her own friends and socialise in the way that she wants to. I think there’s a
lot of dependence in that area and I think that makes it hard to separate what is actually
really a problem for her or what is an easy way out”.

265
From each viewpoint, parents, teachers and aides are looking for answers … “I don’t
think we truly understand what exactly is wrong with her and what the implications are”.
People might say the student has spina bifida but nobody really says “this is exactly what
spina bifida is and this is how it affects you and she has these problems because of it. It’s
not really her fault, it’s not because she hasn’t matured or grown up or whatever it’s just that
she can’t like she’s not skilled in that area because of her mental condition”. At another
school, two teachers willingly shared knowledge about the student but accusations of
laziness and misunderstanding on the part of colleagues were reported.
All stakeholder comments suggest a thirst for more knowledge. Parents want educators
to listen to them. They want Education Queensland to acknowledge the volume of well-
documented literature about spina bifida, hydrocephalus and cognitive problems.
Psychological testing revealed a heterogeneous group. All students were found to be
severely learning disabled and the one common causal factor was neurological damage from
shunted hydrocephalus related to spina bifida. The following summarises the complex set of
learning difficulties experienced by students, none of which appeared to be formally
identified prior to this study.
1. NLD, Executive Function Disorder, Borderline Intellectual Functioning;
2. NLD, Executive Function Disorder, Borderline Intellectual Functioning;
3. Partial NLD, Executive Function Disorder, specific disorder in the memory
domains, Low Average Intellectual Functioning;
4. Partial NLD, Executive Function Disorder, specific disorder in the language
domains, Low Average Intellectual Functioning;
5. Mild Intellectual Impairment, NLD profile of strengths and weaknesses,
Executive Function Disorder. See Appendix D for Definitions.
Personal understanding of how impaired nonverbal skills lead to maladaptive
social skills
Although no simple tactile imperception was reported here, Rourke et al. (2002)
suggest tactile perceptual problems become less prominent with age but complex tactile
imperception tends to persist. All children had trouble with visual perception and all needed
to sit near the board. Problems with tactile and visual perception lead to an inaccurate
memory for information received through the sense of touch or through the eyes and
combined with immobility are expected to inhibit exploration and discovery. Children may

266
prefer to gather information by sitting and asking questions. Indifference towards
investigating surroundings leads to missed opportunities to profit from rich environmental
experience and interaction with peers.
In the early school years, tactile and visual skills are the most commonly used skills in
educational activities. Simple everyday tasks for a typically functioning child are not simple
for a child with neurological dysfunction. Turning on the tap at home may be different to
turning one on over the water trough at school. Shutting the toilet door at school will be
different to home. Generalising and adapting learned information is difficult and limited
exploration leads to limited experience with everyday differences. Don’t expect them to spot
differences because they don’t have the same level of environmental awareness as age peers.
These children need to be specifically taught many everyday skills such as tearing alfoil or
lunch paper, opening a tin, cutting an apple or opening the flavouring sachet for an instant
meal.
Children who do not physically explore the environment and learn to turn, twist,
handle, build, throw, lift and negotiate will not make accurate connections between objects
and consequences because of impaired perception of cause-and-effect relationships on a
physical or interpersonal level. Nonverbal behaviours such as gestures, facial expressions
and voice nuances may go unnoticed. Lack of practical understanding hinders ability to
form accurate concepts about a multitude of notions like shape, size, heavy-light, short-long,
above-below, in-out, up-down, personal exchanges and reactions. If perceptions of the
environment and the way objects and persons interact in it are impaired, such misperception
will hinder ability to ‘read’, integrate and interpret the whole picture and attach appropriate
meaning to language. This is where contextual meaning is attached to language. Good
auditory and rote memory skills allow children with hydrocephalus to remember
sophisticated words but perceptual difficulties can prevent observation and integration of the
nonverbal aspects needed to attach accurate contextual meaning to the word. Children may
use this word in the wrong context. Limited appreciation of word meanings, environmental
experiences and missed nonverbal information will make the inherent ambiguity in humour
and sarcasm difficult to recognise and manage.
Any new environmental or social situation requires one to decide on an appropriate
response and children with NLD tend to rely on something that has worked previously.
They need to compare what worked in the past with available options for the new
circumstance. Reliance on previously learned responses or behaviours is not always
effective as tasks and social interaction become less predictable and more complex. Hence

267
we have a scenario where a child’s developmental experiences have not sufficiently
equipped him or her to make reliable social judgements and deal effectively with new
scenarios. This state of affairs explains trepidation with new tasks/situations displayed by
students, their need for psychological, verbal and/or physical preparation and a strong
preference for sameness and routine “who is going to be swimming with me …”, “I’m going
to turn your wheelchair backwards and we’re going to go down the gutter”. The following
diagrammatically illustrates the spiralling cycle of deficiency that students with NLD may
experience.

268
Table 4.7. Spiralling cycle of deficiency
Start here Deficient – · Complex tactile · Visual perception · Organisation · Complex psychomotor
Impaired memory
for - · Information delivered through the hands and eyes · Hard to visualise and interpret word problems in class
Disinterest in – · Exploratory play leads to · Under-developed psychomotor skills (gross and fine motor) · Poor concept of size, weight, height, in-out, above-below etc.
Reduced – · Environmental and personal experiences · Experience with cause- and-effect relationships · Perception of nonverbal cues · Ability to form accurate concepts of objects and persons in the environment
Difficult to – · Handle complex psychomotor tasks · Attach appropriate contextual meaning to words · Recognise inconsistencies in humour and sarcasm · ‘Read’, integrate and interpret the whole picture
Impairs – · Ability to compare past experience to the present for hypotheses testing · Ability to make quick decisions · Ability to deal with humour and sarcasm
Difficulty with – · Problem solving maths · Planning, organisation, decision-making · Handling new tasks and new situations · Gauging appropriate responses in social settings
Maladaptive Social skills
and Problem solving
ability
Spiralling cycle of deficiency at an older
age

269
CHAPTER SIX
SUMMARY OF STUDY AND CONCLUSIONS
This study probed teacher, teacher aide, parent and student perceptions of the learning
experiences of 5 students with shunted hydrocephalus and spina bifida who shared NLD
characteristics. The theory underpinning selection of this participant group adheres to belief
that parents, teachers and aides significantly contribute to the quality of a student’s school
experiences. The voice of each stakeholder was given equal opportunity to be heard with
understanding that each viewpoint could be interpreted from different vantage points.
Problem
Students who do well at reading, spelling and oral presentations and display a wide-
ranging vocabulary may be assumed to be more academically and socially capable than they
are. A student with an NLD experiences severe limitations in the nonverbal areas of
functioning such as organisation, time management, decision-making, problem solving,
recognising and dealing with humour and understanding social interaction which teachers
often fail to recognise as genuine sequelae of the student’s medical conditions. This study
selected students at Level 1 risk of developing an NLD as a consequence of a hydrocephalic
condition then spoke with their parents, teachers, aides and students themselves. Since much
literature comes from Canada and the United States, understandings of 5 at-risk students
from five Australian schools were explored. The ultimate goal is to raise awareness and
understanding of the NLD profile with parents, teachers, aides and guidance officers so that
early identification, assessment and intervention can minimise failure on academic and social
fronts before disillusion and loneliness intensify with age.
Methodology
The openness of Naturalistic Inquiry methodology suited the researcher’s desire to
uncover important stories in people’s lives told in their own language before reporting
perceptions in a way that communicates understanding. A constructivist-perceptual position
towards reality was adopted because, like naturalistic inquiry, it accepts that each
individual’s realities are best studied in a holistic fashion in their natural context.

270
Initial recruitment of students through Spina Bifida Hydrocephalus Queensland did not
proceed as planned and twelve information packs were returned without address labels. It
then became necessary to recruit through public hospital clinics. From the total number of
16 responses, a homogeneous subgroup of 5 students who met tight selection criteria was
recruited. Five ethical approvals were granted for this study and the project was registered
on the Queensland Health Research registry. All recruitment protocols were diligently
followed and except for one teacher, all consent forms were duly signed, collected and filed.
This teacher gave verbal consent but declined to sign documentation. Access to interview
venues was trouble-free and all school principals, school staff, families and students were
accommodating, willing and interested in being involved. Data collection involved forty-
three interviews, each of about 1 hour, plus psychometric assessment of each student
involved in the study.
Credibility of findings
Member checking, cross-case analysis, supervisor collaboration, supervisor debriefing
and a reflexive journal were strategies used to strengthen credibility of findings. In addition
to strategies outlined under “Subjectivity and bias”, the researcher constantly monitored her
personal experiences through the data collection, analysis, interpretation and reporting
phases to offset the limiting effects to objectivity of having a child with hydrocephalus and
spina bifida. All verbatim interview transcripts were forwarded to informants for their
corroboration. Data was then de-identified and coded to preserve anonymity before
commencing the initial stage of data analysis. Items of information were identified and
numbered with special care taken to avoid dual content within any item of information. To
preserve the integrity of salient viewpoints, direct quotations were preferred to paraphrasing.
Limitations of study
Neuropsychological assessment which provides insight into brain-behaviour
relationships in the developing child was preferred but the cost of assessing an approximate
subgroup of 8-10 students was prohibitive. Before the final subgroup of 5 students was
refined, it was necessary to secure the services of a registered clinical psychologist for test
administration. To ensure comprehensive understanding of results, the expertise of a clinical
neuropsychologist and a developmental paediatrician were engaged to interpret test findings
prior to and during final diagnosis. Despite many advances, there is still a problem with the
diagnosis of an NLD. Firstly, there is no unanimity about a psychological test battery and

271
secondly, each person’s NLD status falls within a continuum. Rourke et al. (2002) confirm
that “there are varying degrees of expression of the syndrome” and some persons exhibit
some but not all of the neuropsychological assets and deficits (p.168). However, there was
sufficient agreement between members of the research team to confirm the similarities
between students and thus provide a foundation for the composite experiences of the children
described here.
Findings
Psychological testing revealed a heterogeneous group. All students were found to be
severely learning disabled and all were high on the NLD parameter. Two students were
diagnosed with NLD, two with Partial NLD and one with Mild Intellectual Impairment and
an NLD profile of strengths and weaknesses which made the degree of impairment more
difficult to ascertain. All 5 students were diagnosed with an Executive Function Disorder.
Of the two students with an NLD, one displayed a clinically significant V-P discrepancy of
26 points and the other had an insignificant V-P discrepancy of 7 points. One student with
Partial NLD displayed a clinically significant V-P discrepancy of 30 points favouring
performance and specific deficits in the language domains. The other student with Partial
NLD displayed a V-P discrepancy of 3 points favouring performance and specific deficits in
the memory domains. It is possible that the NLD characteristics of the two students with
Partial NLD will manifest and become more disabling with age, as Thompson (1997) says “a
child grows into NLD” (p.19).
The five case studies confirm previous literature that reports aspects of an NLD in
students with shunted hydrocephalus and spina bifida and different levels of severity fell
within a continuum. However, it was the NLD phenotype that appeared to confuse many
teachers and aides, the good oral presentations and wide-ranging vocabulary which in some
cases led to unrealistic expectations. What stood out was an absence of understanding about
nonverbal deficiencies particularly in the areas of organisation, time management, decision-
making, problem solving, ability to start and finish tasks and ability to develop friendships.
These five case studies demonstrate the varying degrees of expression of the syndrome and
the range of reactions by parents, teachers, aides and children themselves. With increasing
year levels as task and social interaction became more demanding and fewer allowances
were made, older students became more aware of their social difficulties and had sought
counselling.

272
Parents noted their child’s ability to converse better and build rapport quicker with
older or younger persons than with age-peers and for group work, all students had to be
placed by the teacher. One student was comfortable to group with age-peers if an aide was
present otherwise she preferred to work with Special Education students or work alone.
Another student said “I just presume that because I don’t get to hang out with them they
won’t want me to work with them”. Older students preferred “goss” magazines and “soapie”
television shows and given a selection of reading material, they would choose age-
inappropriate material. Teachers acknowledged good rote learning ability and good reading
skills but observed trouble with interpreting text … “she can verbalise but she doesn’t want
to interpret things clinically”. Older students enjoyed English and “really loved” Speech and
Drama “that’s what I can see myself doing as a career … I want to be an actress”. Verbal
skills impressed most teachers but some observed a lack of content and meaning and one
queried the student’s language skills if compared with other 16 year-olds without a physical
disability.
Teachers and aides often failed to understand the nonverbal aspects of school life and
did not link deficient planning, organisation and time management skills with late arrival at
school. Concerns about very poor organisational skills and poor completion rates were
expressed “doesn’t seem to meet deadlines … it’s a mystery in life that it always seems to be
going along okay but it never kind of gets there”. A child who could not work
independently was reportedly perceived by some teachers as “lazy”, “a very capable child, a
bright child but perhaps molly-coddled at home, babied too much, too dependent” and
because of that dependence, could not work alone. Lack of life skills was blamed on the
family’s dealing with the child’s problems or because “the family aren’t letting go”. One
parent said the effort and persistence put into oral presentations was not recognised and
because it was so difficult for the child to maintain constant attention on a task, people
actually considered the student “lazy” when actually, the child was “trying really hard”.
Poor organisation, decision-making and problem solving ability, inability to start and
finish a task and forgetfulness were sometimes blamed on the home situation, a need to “get
Mum organised”, laziness, or over-protective parents who thought and spoke for the child.
Teachers generally assigned responsibility for task completion to teacher aides though aides
did not appear to receive formal training and none were aware of the “Teacher Aide
Handbook: Assisting Students with Physical Disabilities” on the Education Queensland
website. If no in-class support was available, some teachers developed innovative teaching
strategies while others felt the teacher aide “knows more than us”.

273
All students needed a lot of prompting and had trouble making decisions “‘Oh oh! I
don’t know’ and from there it’ll be a struggle” said one teacher while another was unsure
“whether part of it’s to do with her upbringing in that Mum’s unwillingness to let her
become independent and force her to start making some of those decisions” about lesson
requirements. Interestingly, each student’s age equivalent on the Test of Problem Solving
ability was 3-7 years below their chronological age. Planning and organisation are a
fundamental difficulty for people with spina bifida and hydrocephalus because they require
the brain to envisage, arrange and carry out a series of unfamiliar actions. It is reasonable to
suggest that all parents want their children to become independent and receive opportunities
to reach their potential; therefore any claim of overprotection should be dispelled. Rourke et
al. (2002) say that “although sensitive caregivers are often accused of this, it is clear that
they may be the only ones who have an appreciation for the child’s vulnerability and lack of
appropriate skill development” (p.292).
Some teachers and aides had trouble understanding the student’s difficulty with
interpreting social communication and handling unexpected incidents. When confronted by
a Year 8 student who wanted “his car back”, one student in a wheelchair spoke with a
teacher “and do you know what I got from her ‘well you’re mature enough to know that
they’re only joking’”. The student’s age equivalent on Language Assessment was 3 years
below chronological age; indeed each student’s Language Assessment reported a disparity of
2-7 years below chronological age. As well, every report stated there was much in their
world that the student did not comprehend fully and there was much in communicating ideas
that each child found difficult. Failure by teachers and aides to understand struggles to plan,
organise, problem solve, make decisions, recognise and deal with peer interaction, humour
and novel situations can lead to unfair criticism, unreasonable expectations and inappropriate
advice from guidance officers on the student’s potential for post-school life and work.
How teachers and aides understood learning difficulties
Impaired decision-making ability caused frustration for teachers and aides. “Well spina
bifida it’s meant that she’s ended up in a wheelchair … but we would expect her to be able to
make a decision ‘do you want this green thing or do you want this red thing’ and we think
that’s an easy decision to make … and maybe we don’t understand … It’s not really her
fault, it’s not because she hasn’t matured or grown up it’s just that she can’t, she’s not skilled
in that area because of her mental condition”. Good conversational skills confused another
teacher because other students with an intellectual disability “don’t have very good
conversational skills”. Teachers and aides found it deceiving when “everyday activities that
we take for granted become a major operation” because the student seemed “quite switched

274
on and doing really well”. While aide support helped students be included, it meant they did
not have to work independently or manage their own time. Some staff did not think students
took independent responsibility for homework. One student received “quite a few admin
detentions” for non-compliance and each misdemeanour was grounds for a permanent record
on the student’s file.
Transferring previously learned information to a new context was very difficult and
students needed step-by-step instruction. Teachers were surprised when students could not
read and follow simple recipe instructions. An unexpected event in the kitchen would cause
one student to get “very defensive” and “a bit more closeted if she strikes a problem she
doesn’t want to deal with”. An aide was surprised when 2-minute noodles took 30 minutes
to prepare.
Some teachers expressed concern about motivating students to learn. University taught
them how to deal with attention and behaviour difficulties, but some teachers reportedly had
to “pick each other’s brains”, pick the mother’s brains or go to the Special Education unit for
ideas. Getting practical tasks finished caused much frustration for teachers and aides “you
feel like you’re pulling teeth but it happens”. Flexibility and willingness to adapt tasks
without trying to fit the child in with everyone else were accommodating approaches used at
two primary schools. Know them and surround them with a class culture they can rely on,
“that you don’t have to do that alone and she doesn’t have to do it alone”. At one school,
patience, compassion and a sense of humour helped Special Education staff to realise it is “a
struggle for them and that their little minds do think in a different way to ours”. A Special
Needs teacher had seen colleagues get “incredibly annoyed” about disorganisation … “it’s
not her fault and it’s one of the things that if I’d had a dollar for every time I’d said to
somebody ‘it’s actually a part of the condition, she’s not doing it to upset you, please just
build the extra prompt into your day’”. Because another child could not write about the
weekend, the child was considered “lazy” and “too dependent”. Difficulty staying on task
was blamed on being “spoilt or lazy” but one aide said she may not know enough about the
child’s limitations. Students who were not keen to work independently were described as
“pampered”, “mollycoddled” or “much more capable than people are giving her credit for”.
One teacher thought a student had “plenty of brains, plenty of ability” but there was
overcompensation somewhere along the way.

275
Did teachers, aides, parents and students know about a Nonverbal Learning
Disability?
No teacher expressed bona fide knowledge of the NLD syndrome. “Nonverbal, what is
it? So is it a visual …?”, “What … that would be like a spatial … I guess people have all
sorts of learning disabilities don’t they …” One teacher may have heard of an NLD “in a
broader sense”, one read about it on the internet the night before interview and another had
heard of the syndrome “only recently” from a friend. One teacher who had “read some
information on that” did not appear to relate reading to the student who was diagnosed with
an NLD. No aide had heard of an NLD though good verbal skills caused one to think “they
know everything … they’re very high functioning”. After describing the NLD in some
detail, teacher and aide responses included “… certainly has what you were saying when you
were describing it. It certainly matches what I find with …”, “that’s classic for …”, “well
that seems to be … down to a tee”, “I’d say that’s …” One teacher felt they would all learn
from this study “I think we’ve got lots to learn and lots to keep in mind and I think there can
be a frustration level especially when people think she has a physical impairment, she
doesn’t necessarily have an intellectual impairment so I think teachers struggle with that
‘well why can’t … do this’” Three parents had heard of the NLD syndrome, one had never
heard of it and another did not recognise the profile. Two students had never heard of an
NLD but were keen to know more. From these responses, it appears that no teacher, aide,
parent or student had genuine understanding or working knowledge of the syndrome.
Recommendations resulting from the study
Based on findings of this study, a number of recommendations can be made to assist
teachers, parents and the students themselves to benefit more from their educational
experiences.
For teachers and parents to help students
1. At the start of each school year, parents should request a meeting with all of their
child’s teachers and aides to explain the reality of school day mornings. Parents
should speak in detail about the stress involved with each school day to avoid blame
for late arrival on it not being “a big priority at home”. Such a forum would benefit
all. It could be designed to initiate collaborative discourse, challenge existing
assumptions and lead to new understanding of the full picture. Teachers and aides
need to listen to the parents and student. As demonstrated in case studies, the

276
parents have cared for this child since Day 1 which makes them and the child
valuable resources for school staff. Parents have observed the child in almost every
situation and know better than anyone about their child’s personal strengths,
vulnerabilities and deficient skill development.
2. At the start of each school year, parents, student and teachers could discuss the merit
of a class discussion about individual differences “I don’t think that her classmates
probably understand very much about … at all. If they did then the dynamics that
she’s had in the past couple of years probably wouldn’t have ever happened”,
“there’s some kids in Year 11 who have no idea what’s wrong with …” Parents said
teachers and students need to understand about different learning styles and
recognise that we all have a broad spectrum of learning styles. “If teachers push that
a little bit more in their classroom it might help. It might be another way to explain
the differences between people”. Teachers have a particular responsibility here and
they could engage the help of the class by building a culture that emphasizes:
a. care, consideration and support for classmates;
b. an understanding that some students have special requirements;
c. “there will be no teasing” and “yes” there are special requirements for a
student with a shunt just like anyone else with a physical problem;
d. no bumping the student who has a shunt; and
e. help for all children to do what they need to do.
3. At the start of each school year, parents and teachers should discuss an approach
towards wheelchair assistance that promotes friendship. An emphasis on
“independence has got her nowhere only loneliness and heartache” said one parent
and for another student, a lot of issues started in primary school because it was “so
physically tiring” for the child to access where peers sat or played. Parents could
stress the need for any teacher or student to first ask the student’s permission before
pushing the wheelchair.
4. At the start of each school year, parents and the school principal could discuss the
merit of hanging a large picture of the student in the Staff Lunch Room where the
student’s medical conditions are noted and the action plan to be followed in the
event of an accident or potential shunt problem. This would ensure all staff shares
the same information about the student.
5. Prior to high school transition, parents could meet with relevant teachers, aides,
school counsellor, Special Needs and Learning Support Teachers to discuss
problems in the nonverbal areas of functioning and potential difficulties the student
may have with following a complex timetable, getting lost in new surroundings,
disorganisation, forgetfulness and social incompetence.

277
6. Finding talk time before or after lessons was considered important to get to know the
student, build rapport and over time observe what the student is capable of.
7. Friendship situations need to be actively promoted by teachers and aides because a
child with hydrocephalus and spina bifida may have great difficulty initiating social
interaction and cultivating meaningful friendships. Older students were affected by
anxiety over social interaction and friendships. For such students, ability to function
socially with peers becomes a critical matter with age and dysfunction causes
anxiety and/or depression. Teachers and aides need to be aware of the progressive
effects of NLD deficits on social skill development. They need to realise that speech
fluency does not necessarily imply competence with understanding communication
and ability to perceive the subtleties of social interaction. The origin of these
problems is damage to right hemisphere functions from the hydrocephalic condition
not a family holding the child back and the implications of failing to appreciate that
leads to considerable problems for the child.
8. Overt or covert bullying behaviours need constant vigilance by teachers and aides in
and out of the classroom. A student with spina bifida and hydrocephalus may not be
able to recognise and respond to humour or sarcasm and this student may not
recognise the difference between who should and should not be ignored in the
playground. Students with hydrocephalus may need specific instruction on
appropriate “comebacks” to use in these situations.
9. Physically independent students with hydrocephalus and spina bifida should not be
overestimated by teachers and aides “they are very fragile children. They just can’t
be roughed up like any other child. You have to be very careful” because of a
fragile back and the shunt said one parent. If a mistake happens in class, one
student got teased “because kids can’t see” the child’s disability, they think there is
nothing wrong … but if the child was in a wheelchair “that would be fine”.
10. To reduce anxiety with any new activity or situation, teachers and aides could ensure
the student has a base of familiarity, whether that is a person or an environment.
11. To locate or reduce work to be copied from blackboard, teachers could:
a. use colour-coding to highlight;
b. circle, underline key words or phrases;
c. suggest student and aide take turns;
d. suggest student read while the aide scribes.
12. To aid sentence-writing, teachers and aides could write sentence-starters on
laminated cards.

278
Parental help for students
1. To compensate forgetfulness, one parent invented a mini-timetable to be worn
around the student’s neck on a keychain. It comprised five laminated colour-coded
cards that faced inwards “so the rest of the school kids” do not see that it was the
child’s timetable. Each card displayed name of class and time, teacher name and
room number. Lunch breaks and spares were also noted. The same parent provided
a small notepad and pencil to be worn around the student’s neck to jot down spoken
messages from the teacher.
2. To help the student find books and writing tools in desk, parents could provide:
a. transparent pencil cases;
b. colour-coded book covers;
c. subject name on all corners of every book, front and back, for quicker
identification.
See Appendix F for Helpful hints for teachers and aides from this study.
Restatement of what is important
The primary intention of this study was to explore the learning experiences of 5
students with hydrocephalus and spina bifida who showed signs of an NLD. Individuals
with a hydrocephalic condition are considered at Level 1 risk of manifesting virtually all of
the NLD assets and deficits. The study gave voice to 43 teachers, teacher aides, students and
parents who were believed to contribute significantly to the quality of the students’ learning
experiences.
The ultimate goal of the study is to raise awareness about this identifiable learning
profile so that early identification by parents, teachers, aides and school counsellors can lead
to appropriate assessment and intervention before failure on academic and social fronts
manifests as depression or worse with age. The significance of verbal and nonverbal
abilities for academic, social and emotional functioning will thus gain status in the minds of
professionals and parents. Findings from this study have confirmed a learning need for
educators. They justify further investigation with a view to teaching under-graduate, post-
graduate and current teachers about a Nonverbal Learning Disability and its ranges of
presentation and severity.

279
Recommendations for education systems
Data gathered and confirmed by psychometric testing reveals a compelling need to
educate teachers, aides, school psychologists and guidance officers about the continuum of
neurodevelopmental disorders of which NLD is one amalgam within a much wider spectrum.
The following recommendations have emerged from this study.
1. During undergraduate, postgraduate and in-service training, teachers could be
encouraged to develop pathways for parents and teachers to problem solve together.
2. Teachers and aides need to listen to their own disquiet about any student who is
struggling to do things one would expect them to be able to do. Further, teachers
need to listen to parental concerns that may indicate a neurodevelopmental disorder
so the child can be referred for immediate assessment.
3. Teachers, aides and school psychologists need to learn about the spectrum of
developmental disorders of which an NLD is one. The heterogeneity of students in
this study attests to this. Fundamental to understanding a developmental learning
disability is (a) assets and deficits become more obvious with age and (b) individuals
cannot be discreetly categorised but rather each person’s unique set of skills places
them somewhere on a continuum. Teachers, aides and diagnosticians must know
about the continuum of developmental disorders.
4. As well as assessing general intelligence, school psychologists should utilise test
measures that assess specific areas of nonverbal functioning such as tactile-visual-
organisational perception, psychomotor skills, adaptability, executive functioning
and social competence.
5. Education systems may consider:
a. allocating funds to make direct instruction methodology available to those
who need it;
b. psychometric testing for every student with shunted hydrocephalus, with or
without spina bifida, at timely intervals throughout the student’s school life.
6. In light of this study, it is hard to understand why there is not wider recognition that
shunted hydrocephalus, which occurs in 95% of spina bifida cases (Lutkenhoff &
Oppenheimer, 1997), may cause an identifiable learning disability. The “literature’s
there, the body of knowledge is there yet we just can’t get the Education Department
to say ‘yeah it does, let’s address it’ and I don’t know why” said one parent. Parents
want to be involved. They believed they should advocate strongly for their child
“especially with the Education system, as it does not seem to fully understand the
hidden problems associated with spina bifida”. “There’s not a lot of schools who
know a lot about spina bifida. It’s not a known thing”. The apparent non-

280
recognition by officialdom of primary and secondary problems is a source of
constant frustration for parents, as well as misunderstanding by teachers and aides.
7. More undergraduate, postgraduate and in-service training is obviously needed to
help teachers with the non-typical learning requirements of students with
hydrocephalus and spina bifida. Teachers had to “pick each other’s brains”, go to
the Special Education Unit for hints or “pick” the mother’s brains, said one parent.
“What do you do if the other stuff’s not working because the traditional instruction
doesn’t work and the more visual hands-on work and using multiple intelligences …
if that doesn’t work either, what does?” There appeared to be no formalised help as
that provided to teachers about attentional and behavioural difficulties.
8. Education systems may consider greater emphasis on the importance of enhancing
requirements for teacher aides to become well-versed in the specific problems of
students with diverse and mosaic disabilities. For example, in the present study, no
teacher or aide was aware of the booklet available the Education Queensland website
entitled “Teacher Aides Working with Students with Disabilities”, Booklets A-G
http://education.qld.gov.au/curriculum/learning/students/disabilities/resources/public
ations/taide.html
9. Education Queensland and other education systems could emphasise teacher aide
presence at all IEP meetings. One-on-one contact with a child with a disability will
provide useful feedback and suggestions for improvement. “When you get down to
the nitty-grittys, I’m the one who’s wiping …’s bum aren’t I so if they want to ask
anything about that sort of thing, it’s no use asking anybody else” said an aide.
Conclusion
The purpose of this thesis was to help parents, teachers and others to appreciate the
learning and schooling experiences of children with hydrocephalus and spina bifida. It does
not purport to offer ultimate solutions or to contribute to diagnosis but rather to act as a
starting point for the development of a body of theory that contributes to appropriate learning
environments for such children. A further importance of this study is emphasis on the need
for similar studies to be conducted into the learning experiences of other children who
demonstrate specific syndromes or variations of those syndromes.
The areas of functional deficiency that characterise students with an NLD are the areas
that distinguish them from those with a general learning disability. As illustrated earlier,
impaired fine and gross motor skills, planning, organisation, problem solving, decision-

281
making skills, difficulty handling new tasks and understanding social interaction can be
traced back to the skills least developed in early life and which continue to worsen with age.
As more autonomy, responsibility and self reliance is expected at home and school and
friendships became harder to sustain, everyday life for these children can be full of fear and
apprehension if the fundamental problem is not identified and managed. Teachers, aides
and parents must be cognizant of the NLD syndrome and its various expressions. They must
be willing to accept that contradictory presentations have a neurological basis, in the
presence or absence of a causal diagnosis. Current research emphasises that early
intervention offers a child the best chance of success through school but at the same time,
educators and others must remember that part of the problem with helping a student with an
NLD is a false belief that a student who reads, speaks and spells well and uses sophisticated
vocabulary could not have significant educational needs.
Overseas, the incidence of NLD is reportedly about 1 in every 10 young people with a
“standard” learning disability and indications are that the trend towards a higher incidence of
NLD is continuing (Rourke et al., 2002, p.165). In Australia, the 2006 Bureau of Statistics
says 185 800 children aged 0-14 years have some form of schooling restriction and 97,500 of
those are reported to have learning and intellectual problems. Furthermore, children in the
14+ age-range may reveal a large number of undiagnosed individuals with an NLD whose
learning, social and emotional problems are wreaking havoc on every aspect of school life, a
situation that makes edification to those who are in the best position to shape and promote
the student’s development, a moral imperative.
This study found that teachers willingly accommodated difficulties from obvious
physical limitations. Teachers acknowledged that learning problems existed but in the
absence of clear industry understanding of the NLD profile, many were unsure of what
strategies would help the student to learn since traditional instruction “doesn’t work”.
Educators did not conceptualise functionality in terms of verbal and nonverbal abilities and
reference to nonverbal skills caused confusion for some. If educators fail to realise that
problems handling new tasks and situations, organisation, time management, problem
solving, decision-making, forgetfulness, social interaction and humour reflect difficulties in
the nonverbal domains, blame will be apportioned to laziness, spoiltness, the family or home
life. This highlights a need for awareness about the significance of verbal and nonverbal
skills for everyday life. Also, assessment tools that target the verbal and nonverbal areas of
functioning must be utilised to enable psychological reports to explicate the true state of
affairs which is currently not always the case. The following possible sequence highlights a
chain of events that should lead to the asking of the “WHY” question.

282
Diagnostic sequence
1. Trouble with class stuff
√ √ √ √ √
2. WHY – Did not ask
3. Is it IQ? ↓ ↓ ↓ ↓ ↓
Low Low Low Average Low Average Bad
4. Is low IQ enough to explain Functioning << IQ - No
5. Does the student have a Learning Disability?
6. Is low IQ + LD enough to explain low functioning – No
All students had an Executive Function Disorder, varying degrees of an NLD and one
child had an Intellectual Impairment, previously missed. One child had a specific disorder in
the memory domains while another had a specific disorder in the language domains. Each
student’s intellectual functioning ranged from borderline to low average which spawns the
question “WHY are students performing so much poorer than we expect them to? Is it
related to spina bifida and hydrocephalus?” One parent said “if you’re a teacher and you
have a student in your class with a disability, you’d also start seeing some issues with that
student wouldn’t you. You would be able to look and say ‘Oh, they haven’t done much
work today’ so wouldn’t you think that you would sort of research yourself on this student’s
condition and find out what it’s about”. This raises questions about the processes that are
available to teachers to help them respond when they observe a student who is struggling
functionally and academically. An extract retrieved from the Education Queensland website
in 2006 entitled “Teacher Aides working with Students with Disabilities - Physical
Impairment” Book E states –
“In the school situation students with spina bifida and hydrocephalus may exhibit
specific learning difficulties such as -
• short concentration span
• difficulties with organising and planning a task
• limited abstract thinking” (p.9)
A recent search in Book D “Intellectual Impairment” revealed no mention of spina
bifida and/or hydrocephalus as causing intellectual damage. The Australian Spina Bifida and
Hydrocephalus Association (ASBHA) website reports many difficulties discussed here and
some advice is offered to teachers but why is there no mention of a Nonverbal Learning
283
Disability? Up to date information that takes account of current research findings and
academic literature is therefore not readily available on either website for those who pursue
the “WHY” question. This raises a separate set of questions about the processes that are
used to translate existing knowledge and research findings into a form that is available to,
and directly informs and influences professional teaching practice.
In this study, evidence gathered and verified by test findings confirmed that students
experienced a multitude of problems far in excess of those listed on the Education
Queensland website. All students were severely learning disabled and although some
parents, teachers and aides had intuitively developed useful measures to help students cope,
there appeared to be no formal classification at a school level of the extent of each student’s
learning impediments prior to this study. All students had shunted hydrocephalus and spina
bifida, a medical diagnosis known to be associated with neurodevelopmental problems.
Teachers had observed academic and functional struggles but apart from obvious physical
constraints, learning difficulties were not linked to medical conditions. So why is no one
asking whether learning and functional problems are related to spina bifida and
hydrocephalus? Rourke et al. (2002) and Fletcher et al. (1995) claim that hydrocephalus is
one of the only disorders identified at Level 1 risk of an NLD for which the neurobehavioral
characteristics have been thoroughly investigated. Educators must be informed that the
network of problems is serious and has far-reaching effects if not identified and managed.
Educators tend to guide students experiencing trouble with academic subjects towards
vocational fields such as hospitality, construction, automotive, tourism, retail, hairdressing or
horticulture. Such areas require fine and gross motor, visual, spatial, tactile, planning and
organisational skills that are problematic for these students and begs the question “What
happens post-school when aide support is withdrawn and students try to compete in the
workforce?” They appear bright but have trouble coping independently with everyday tasks
and they don’t quite “fit in” with peers. Are these students at risk of falling through the
cracks? If genuine difficulties on academic, social and emotional fronts are not identified
and addressed so career guidance can be couched within a realistic framework, the resultant
depression and dispirit can be severe and difficult to arrest as the young person grows older
and compares his or her real prospects with those of age-peers.
A Nonverbal Learning Disability is reported to be more common than Autistic
Spectrum Disorder in the United States and Canada (Rourke et al., 2002). In Australia,
autism has received much exposure in recent years yet this study has revealed less than
optimal awareness of a syndrome that has potential to shatter dreams and aspirations shaped

284
through the child’s developing years, a syndrome that affects not only those with
hydrocephalus but those with other types of brain injury and those without any known cause.
Teachers, aides and parents want to know more; they want to understand these children
so they can help them better. In the10th year of school, one student implied teachers did not
properly understand spina bifida and hydrocephalus and if they did, “they may be able to try
and sort out a better way of teaching us so that we can understand”. Everyone here would
profit from knowing about a syndrome which makes sense of the strengths and weaknesses
with which they deal on a daily basis, the NLD syndrome. Theories about educating
students with hydrocephalus and spina bifida need to take account of the range of cognitive,
learning and social problems that may result from the primary and secondary medical
conditions. If not identified and addressed, any combination of these problems will have a
profound effect upon the young person’s quality of life and the long term effects on
emotional well-being can be frightening and serious.
Future Research
Similar studies could be conducted into understanding of the learning experiences of
other children who demonstrate specific syndromes or mosaic forms of those syndromes. A
core problem that has emerged here is why educators did not associate complex learning
needs with the students’ medical conditions. Teachers accommodated physical limitations
but they did not understand cognitive difficulties despite the volume of literature that targets
learning difficulties associated with hydrocephalus and spina bifida. Struggles were
observed but why could students not do what teachers expected they could do? Up to date
answers would have minimised misunderstanding but why are teachers not asking why?
Furthermore, are teachers encouraged to seek, value and optimise parental experience and
tacit understanding of their child with a disability? These issues appear to be the crux and
foci of future research that need investigation with the aim of endorsing a forum for
collaborative discourse between parents and teachers that leads to shared experience and
problem solving. A unified front will promote understanding and reduce criticism of and by
all stakeholders. Targeted research to develop a range of learning strategies to help teachers
and aides deal with the needs of students who display various forms of an NLD would also
be optimal. Open pathways of communication between parents and teachers in concert with
an expansion of teacher education to include the NLD continuum and development of
appropriate intervention strategies may overcome any one-size-fits-all notion of education
and ease the plight and angst of many teachers, aides, parents and students.

285
REFERENCE LIST
Abercrombie, M. L. (1968). Some notes on spatial disability: Movement, intelligence
quotient and attentiveness. Developmental Medicine: Child Neurology, 10, 206-213.
American Accreditation Health Care Commission. (2002). Medical encyclopedia: Myelin
and nerve structure. Retrieved November 12, 2003, from
http://www.nlm.nih.gov/medlineplus/ency/imagespages/9682.htm
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th ed.). Text Revision. Washington, DC.
Anderson, V., Northam, E., Hendy, J., & Wrennall, J. (2001). Developmental
Neuropsychology: A Clinical Approach. East Sussex: Psychology Press.
Anderson, E. M., & Plewis, I. (1977). Impairment of a motor skill in children with spina
bifida cystica and hydrocephalus: An exploratory study. British Journal of Psychology,
68, 61-70.
Anderson, E., & Spain, B. (1977). The Child with spina bifida. London: Metheun.
Anderson, P., & Rourke, B. P. (1995). Williams syndrome. In B. P. Rourke (Ed.), Syndrome
of nonverbal learning disabilities. Neuro-developmental manifestations (pp. 138-
170). New York: Guilford Press.
Andrews, R., & Elkin, J. (1981). The Management and education of children with spina
bifida and hydrocephalus. ERDC Report No.32. Canberra: Australian Government
Printing Service.
Australian Bureau of Statistics. (2001). Child health since federation. Year Book Australia
2001. Retrieved May 10, 2004, from http://abs.gov.au/AUSSTATS
Australian Bureau of Statistics. (2006). Disability and disabling conditions, 1998. Retrieved
February 23, 2006, from http://www.abs.gov.au/AUSSTATS
Back, K. W., & Gergen, K. J. (1963). Idea orientation and ingratiation in the interview: A
dynamic model of response bias. Proceedings of the Social Statistics Section
(pp. 284-288).
Backhouse, M., & Rodger, S. (1999). The Transition from school to employment for young
people with acquired brain injury: Parent and student perceptions. Australian
Occupational Therapy Journal, 46, 99-109. Oxford, England: Blackwell.
Badell-Ribera, A, Shulman, K., & Paddock, N. (1966). The Relationship of non-progressive
hydrocephalus to intellectual functioning in children with spina bifida cystica.
Pediatric, 35, 787-793.
286
Baron, I. S., Fennell, E. B., & Voeller, K. K. (1995). Pediatric neuropsychology in the
medical setting: Hydrocephalus and myelomeningocele. New York: Oxford University
Press.
Beery, K. E., Buktenica, N. A., & Beery, N. A. (1997). Developmental test of visual-motor
integration (5th ed.). New York: Modern Curriculum Press.
Benda, C. E. (1952). Developmental disorders of mentation and cerebral palsies. New
York: Grune and Stratton.
Benton, A. L., Hamsher, K., & de S. Sivan, A. B. (1989). Multilingual aphasia examination.
Iowa City: AJA Associates.
Boehm, A. E. (1971). Boehm test of basic concepts. New York: Psychological Corporation.
Bohan, T. P., Dominguez, R., Fenstermacher, M., Kramer, L., Fletcher, J. M., Miner, M. E.
et al., (1994). Diffuse central nervous system anomalies associated with
myelomeningocele.
Bowers, L., Huisingh, R., Orman, J., & LoGiudice, C. (1991). TOPS-Adolescent: Test of
Problem Solving. Retrieved May 5, 2005, from www.linguisystems.com
Bowers, L., Huisingh, R., Orman, J., & LoGiudice, C. (1994). TOPS-R Elementary: Test of
Problem Solving. Retrieved May 5, 2005, from www.linguisystems.com
Brain Injury Association of Queensland. (2000). Acquired brain injury: An introduction.
Brain Injury Association of Queensland Inc.
Brain Injury Association of Queensland. (2003). ABI: Some statistics on the invisible
disability. Retrieved November 17, 2003, from www.biaq.com.au
Brain Injury Association of Queensland. (2004). The official journal of the brain injury
association of Australia: Synapse, Autumn, 2004, 2-5.
Brain Injury Association of Queensland. (2006). Fact Sheet: Statistics on ABI in
Queensland. Retrieved March 20, 2006, from www.biaq.com.au
Brockett, R. (1983). Facilitator roles and skills. Lifelong learning: The adult years 6,
(pp. 7- 9).
Burns, Robert B. (2000). Introduction to Research Methods (4th ed.). Australia:
Longman.
Burns, M. S., Halper, A. S., Mogil, S.I. (1985). Clinical Right Hemisphere Dysfunction.
USA: Aspen Publishing.
Casey, J. E., & Rourke, B. P. (1991). Neuropsychological validation of learning disability
subtypes. New York: Guilford.
Chelune, G. J., & Baer, R. A. (1986). Developmental norms for the Wisconsin card sorting
test. Journal of Clinical and Experimental Neuropsychology, 8, 219-228.
Christensen, P., & James, A. (2000). Research with children: Perspectives and practices.
London: Falmer.

287
Clements, D. B., & Kaushal, K. (1970). A study of the ocular complications of
hydrocephalus and meningomyelocele. Transactions of the Ophthalmological Society of
the United Kingdom, 90, 383-390.
Costley, D. (2000). Collecting the views of young people with moderate learning difficulties.
In Ann Lewis & Geoff Lindsay, Researching children’s perspective (pp. 63).
Buckingham: Open University Press.
Creswell, J. (1994). Research Design: Qualitative and quantitative Approaches. USA: Sage.
Creswell, J. (2002). Educational research: Planning, conducting, and evaluating
quantitative and qualitative research. Ohio: Prentice-Hall.
Crozier, J., & Tracey. (2000). Falling out of school: a young woman’s reflections on her
chequered experience of schooling. In Ann Lewis & Geoff Lindsay, Researching
children’s perspectives, 173-184. Buckingham: Open University Press.
Culatta, B. (1993). Intervening for language learning disabilities. In Fern L. Rowley-Kelly
& Donald H. Reigel, Teaching the student with spina bifida (pp. 171-188). Baltimore:
Brookes.
Culatta, B., & Culatta, R. (1978). Spina bifida children’s noncommunicative language:
Examples and identification guidelines. Allied Health and Behavioural Sciences, 1 (1),
22-30.
Culatta, B., & Egolf, D. (1980). Perpetual and linguistic performance of spina bifida. Spina
Bifida Therapy, 235-247.
Culatta, B., & Young, C. (1992). Linguistic Performance as a function of abstract task
demands in children with spina bifida. Developmental Medicine and Child Neurology,
34, 434-440. Retrieved from MEDLINE database.
Curtis, S., Gesler, W., Smith, G., & Washburn, S. (2000). Approaches to sampling and case
selection in qualitative research: examples in the geography of health. Social Science
and Medicine, 50, 1001-1014. Exeter: Elsevier Science.
Date, I. (1993). Long Term Outcome in surgically treated encephalocele. Journal of
Surgical Neurology, 40, 125-130. Retrieved November 5, 2003, from MEDLINE
database.
Dawtrey, L., Holland, J., & Hammer, M. (1995). Equality and inequality in education
policy. Adelaide: Open University.
Delahaye, B. L. (2000). Human resource development: Principles and practice. New York:
Wiley.
De Luca, J., Rourke, B. P., & Del Dotto, J. (1991). Subtypes of arithmetic-disabled
children: Cognitive and personality dimensions. New York: Guilford.
Dennis, M. (1996). Hydrocephalus: Treatment. In J. G. Beaumont, P. Kenealy & M. Rogers.
The Blackwell dictionary of neuropsychgology (pp. 406-411). USA: Blackwell.
288
Dennis, M, Fitz, C. R., Netley, C. T., Sugar, J., Harwood-Nash, C. F., Hendrick, E. B.,
Hoffman, H. J., & Humphreys, R. P. (1981). The Intelligence of hydrocephalic
children. Archives of Neurology 38, 607-661.
Dennis, M., Hendrick, E. B., Hoffman, H. J., & Humphreys, R. P. (1987). The language of
hydrocephalic children. Journal of Clinical and Experimental Neuropsychology, 9, 593-
621.
Denzin, N. K., & Lincoln, Y. S. (1994). Handbook of qualitative research. Thousand Oaks,
California: Sage.
Denzin, N. K., & Lincoln, Y. S. (2000). Handbook of qualitative research (2nd ed.).
Thousand Oaks, California: Sage.
Department of Education and the Arts. (2006). Inclusive education: Students with
disabilities. Individual education plans (IEPs). Retrieved May 4, 2006, from
http://education.qld.gov.au/curriculum/learning/students/disabilities/practice
Dexter, L. A. (1970). Elite and specialized interviewing. USA: North-western University
Press.
Douglas, J. D. (1976). Investigative social research: Individual and team field research.
Beverley Hills, California: Sage.
Dunning, D. (1992). Children with spina bifida and hydrocephalus at school. West Sussex:
Tappenden.
Education Queensland. (1998). Teacher aides working with students with disabilities –
physical impairment. Book E (p. 9). Retrieved May 2, 2006, from
http://education.qld.gov.au/curriculum/learning/students/disabilities/resources/publicati
ons/taidepi.pdf
Eisner, E. (1979). The Educational imagination: On the design and evaluation of
school programs. New York: Macmillan.
eMedicine Clinical Knowledge Base. (2004). Encephalocele. Retrieved May 15, 2004, from
http://author.emedicine.com/PED/topic2805.htm
Encyclopedia. (2003). Intelligence, psychology and psychiatry. Retrieved August 5, 2003,
from http://www.1upinfo.com/encyclopedia/1/intellig.html
Erlandson, D. A., Harris, E. L., Skipper, B. L., & Allen, S. D. (1993). Doing naturalistic
inquiry: A guide to methods. London: Sage.
Eynon T., Knighten D., Kruse Carolyn, Lee Matt., Downing, J. M., & Sparks, L. (Eds.).
(1998). Mosby’s medical nursing & allied health dictionary (6th ed.). USA: Mosby.
Fisher, N. J., DeLuca, J. W., & Rourke, B. P. (1997). Wisconsin card sorting test and
Halstead category test performances of children and adolescents who exhibit the
syndrome of nonverbal learning disabilities. Child Neuropsychology, 3, 61-70.

289
Fletcher, J. M. (1998). Learning Problems and the Central Nervous System deficits.
Reprinted in Spina Bifida Spinet (Autumn 1999 edition) with permission from Insights
USA, May/June 1998.
Fletcher, J. M., Bohan, T. P., Brandt, M. E., Kramer, L.A., Brookshire, B. L., Thorstad, K. et
al. (1996a). Morphometric evaluation of the hydrocephalic brain: Relationships with
cognitive development. Child’s Nervous System, 12, 192-199.
Fletcher, J. M., Brookshire, B. L., Bohan, T. P., & Timothy, P. (1995). Early
hydrocephalus. In B. P. Rourke (Ed.), Syndrome of nonverbal learning disabilities:
Neurodevelopmental manifestations (pp. 206-238). New York: Guilford Press.
Fletcher, J. M., Francis, D., Thompson, N., Brookshire, B. L., Bohan, T., Landry, S.
et al. (1992). Verbal and nonverbal skill discrepancies in hydrocephalic children.
Journal of Clinical and Experimental Neuropsychology, 14, 593-609.
Fletcher, J. M., Levin, H., & Butler, I. J. (1995). Neurobehavioural effects of brain injury in
children: Hydrocephalus, traumatic brain injury and cerebral palsy. In M. Roberts
(Ed.) Handbook of pediatric psychology (2nd ed., pp. 362-383). New York: Guilford.
Fletcher, J. M., & Levin, H. (1988). Neurobehavioural effects of brain injury in children. In
D.K. Routh (Ed.), Handbook of pediatric psychology (pp. 258-295). New York:
Guilford.
Flick, U. (1992). Triangulation revisited: Strategy of validation or alternative. Journal for the
Theory of Social Behaviour, 22, 175-198.
Foss, J. M. (1991). Nonverbal learning disabilities and remedial interventions. Annals of
Dyslexia, 41, 128-140.
France, A., Bendelow, G., & Williams, S. (2000). A ‘risky’ business: researching the health
beliefs of children and young people. In Ann Lewis & Geoff Lindsay Researching
Children’s Perspectives (pp. 150-161). Buckingham: Open University Press.
Fuchs, D., Fuchs, L. S., & Fernstrom, P. (1993). A Conservative approach to special
education reform: Mainstreaming through transenvironmental programming and
curriculum-based measurement. American Educational Research Journal, 30,
149-177.
Fuerst, K. B., Dool, C. B., & Rourke, B. P. (1995). Velocardiofacial syndrome. In B. P.
Rourke (Ed.), Syndrome of nonverbal learning disabilities: Neurodevelopmental
Manifestations (pp. 119-137). New York: Guilford Press.
Fuerst, K. B., & Rourke, B. P. (1995). White matter physiology and pathology. In B. P.
Rourke (Ed.) Syndrome of nonverbal learning disabilities: Neurodevelopmental
manifestations (pp. 27-44). New York: Guilford.

290
Giangreco, M. F. (1996). What do I do now? A teacher’s guide to including students with
disabilities. Educational Leadership, 53 (5), 56-59. USA: Association for
Supervision & Curriculum Development.
Gioia, G.A., Isquith, P.K., & Kenworthy, L. (2000). Behaviour rating inventory of
executive function. Odessa, Florida: Psychological Assessment Resources, Inc.
Gioia, G.A., Isquith, P.K., Guy, S., & Kenworthy, L. (2005). Behaviour rating inventory of
executive function. Retrieved October 15, 2005, from http://www3.parinc.com
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory: Strategies of
qualitative research. New York: Aldine.
Glesne, C. (1999). Becoming qualitative researchers: An introduction (2nd ed.).
New York: Longman.
Goldberg, E., & Costa, L. D. (1981). Hemisphere differences in the acquisition and use of
descriptive systems. Brain and Language, 14, 144-174.
Goldstein, S. (1997). Managing attention and learning disorders in late adolescence &
adulthood: A guide to practitioners. New York: Wiley.
Green, P. (2002). Slices of life: Qualitative research snapshots. Australia: RMIT.
Greene, J. C., & Caracelli, V. J. (2003). Making Paradigmatic sense of mixed methods
practice. In A. Tashakkori & C. Teddlie, Handbook of mixed methods in social and
behavioural research (pp. 91-110). Thousand Oaks, California: Sage.
Guba, E. G. & Lincoln, Y. S. (1981). Effective evaluation. London: Jossey-Bass.
Guba, E. G., & Lincoln, Y. S. (1983). Effective evaluation: Improving the usefulness of
evaluation results through responsive and naturalistic approaches. USA: Jossey.
Guba, E. G., & Lincoln, Y. S. (1989). Fourth generation evaluation. California: Sage.
Guba, E. G., & Lincoln, Y. S. (1999). Naturalistic and rationalistic enquiry. In J. P. Keeves
& Gabriele Lakomski, Issues in Educational Research (pp. 141-150). New York:
Pergamon.
Hallahan, D., Kauffman, J., & Lloyd, J. (1999). Introduction to learning disabilities,
(2nd ed.) London: Allyn and Bacon.
Hargreaves, D. (2004). E-magine Newsletter, 4. Retrieved December 15, 2004, from
http://www.e-magine.education.tas.gov.au/documents/iNETConference.doc
Harnadek, M., & Rourke, B. P. (1994). Principle identifying features of the syndrome of
nonverbal learning disabilities in children. Journal of Learning Disabilities, 27 (3),
144-160.
Harrison, P., & Oakland, T. (2003). Adaptive behavior assessment system (ABAS) (2nd ed.).
The Psychological Corporation, Harcourt Assessment Company.
Retrieved August 30, 2004 from http://www.harcourt-uk.com

291
Held, Richard. (1965). Plasticity in sensory-motor systems. Scientific American, 213 (5),
84-94.
Holler, K. A., Fennell, E. B., Crosson, B., Boggs, S. R., & Parker, M. (1995).
Neuropsychological and adaptive functioning in younger versus older children
shunted for early hydrocephalus. Child Neuropsychology, 1, 63-73.
Hommet, C., Billard, C., Barthez, M., Lourmiere, J. M., Santini, J. J., de Toffol,B., Corcia,
P., & Autret, A. (1999). Neuropsychologic and adaptive functioning in adolescents
and young adults shunted for congenital hydrocephalus. Journal of Child Neurology
14, 144-150.
Horn, D. G., Lorch, E. P., Lorch, R., & Culatta, B. (1985). Distractibility and vocabulary
deficits in children with spina bifida and hydrocephalus. Journal of Developmental
Medicine and Child Neurology, 27, 713-720.
Hunt, G. M., & Holmes, A. E. (1975). Factors relating to intelligence in treated cases of
spina bifida cystica. American Journal of Diseases in Children, 130, 823-827.
Hurley, Anne DesNoyers. (1993). Conducting psychological assessments. In Fern L.
Rowley-Kelly & Donald H. Reigel, Teaching the student with spina bifida (pp. 107-
123. Baltimore: Brookes.
Hurley, Anne DesNoyers, Dorman, Casey, Laatsch, L, Bell, S, & D’Avignon, J. (1990).
Cognitive functioning in Patients with spina bifida, hydrocephalus, and the “Cocktail
Party Syndrome”. Developmental Neuropsychology, 6, 151-172.
James, A., & Prout, A. (1990). Constructing and reconstructing childhoods: Contemporary
issues in the sociological study of childhood. New York: Falmer Press.
Kaufman, A. S. (1979). Intelligent testing with the WISC-R. New York: Wiley.
Kaufman, A. S. (1994). Intelligent Testing with the WISC-III. New York: Wiley.
Kauffman, J. M. (1989). The regular education initiative as Reagan-Bush education policy:
A trickle-down theory of education of the hard to teach. The Journal of Special
Education, 23, 256-278.
Keeves, J. P., & Lakomski, G. (1999). Issues in Educational Research. New York:
Permagon.
Kempster, E. A., Stringfield, S., & Teddlie, C. (2003). Mixed methods sampling strategies
in social science research. In A. Tashakkori & C. Teddlie (Eds.), Handbook of mixed
methods in Social and Behavioural Research (pp. 273-296). Thousand Oaks,
California: Sage.
Kozbelt-Culatta, B. (1975). The relationship among knowledge of concepts, sensory
integration, and relevance of language in spina bifida children. Unpublished doctoral
dissertation, University of Pittsburgh, Pennsylvania.
292
Levine, Melvin D. (1994). Educational care: A system for understanding and helping
children with learning problems at home and in school. Cambridge, Massachusetts:
Educators Publishing Service, Inc.
Levine, Melvin D. (1999). Developmental variation and learning disorders (2nd ed.).
Cambridge and Toronto: Educators Publishing Service, Inc.
Lezak, M. D. (1983). Neuropsychological Assessment. New York: Oxford University Press.
Lezak, M. D. (1995). Neuropsychological Assessment (3rd ed.). New York: Oxford
University Press.
Lightfoot, S. L. (1983). The good high school: Portraits of character and culture. New
York: Basic Books.
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. London: Sage.
Lincoln, Y. S. & Guba, E. G. (1999). Naturalistic and rationalistic enquiry. In J. P. Keeves
& Gabriele Lakomski, Issues in educational research (pp. 141-150). New
York: Pergamon.
Lindsay, A. R. (1997). Nonverbal learning disabilities and adult with spina bifida:
Differentiating subgroups based on higher order cognitive skills and family
environment. Dissertation abstracts international: Section B: The sciences &
engineering, 57, (9-B), 5923.
Llewellyn, G., & Green, L. (1987). Living with spina bifida. Sydney: Redfern Legal Centre.
Lloyd-Smith, M., & Tarr, J. (2000). A sociological dimension. In Ann Lewis & Geoff
Lindsay, Researching children’s perspectives (pp. 59-69). Buckingham: Open
University Press.
Loeser, J. D. (2001). Lipomyelomeningocele. Retrieved August 8, 2005, from
http://author.emedicine.com/PED/TOPIC2805.HTM
Lofland, J. (1971). Analyzing social settings. USA: Wadsworth.
Lofland, J., & Lofland, L. (1995). Analyzing social settings: A guide to qualitative
observation and analysis (3rd ed.). USA: Wadsworth.
Lonton, A. (1976). Hand preference in children with myelomeningocele and hydrocephalus.
Developmental medicine and child neurology, 18, 143-149.
Loomis, J. (2003). Spina bifida and nonverbal learning disabilities. Retrieved April 28,
2003, from http://www.drdeanmooney.com/spina.html
Lorber, J. (1973). Your child with hydrocephalus: A practical guide to parents. England:
Stane.
Lorber, J. (1974). Your child with spina bifida: A practical guide to parents. England: Stane.
Lutkenhoff, E. & Oppenheimer, S. (1997). Spinabilities: A young person’s guide to spina
bifida. USA: Woodbine House Inc.

293
Masson, J. (2000). Legal issues. In Ann Lewis & Geoff Lindsay, Researching children’s
perspectives (pp. 34-45). Buckingham: Open University Press.
Mayall, B. (1996). Children, health and the social order. Buckingham: Open University
Press.
Mattson, B. (1982). Learning problems of children with spina bifida. Clinical proceedings –
Children’s hospital national medical center, 38, 225-230.
Mayo Foundation for Medical Education and Research MFMER. (2003). Neural tube
closure. Retrieved March 16, 2003, from www.mayoclinic.com
Mayo Foundation for Medical Education and Research MFMER. (2003). Myelomeningocele.
Retrieved March 16, 2003, from www.mayoclinic.com
McDowell, M. (2001). Medical Causes of Developmental Disorders. Retrieved June 16,
2003, from http://www.childdreams.com.au/health/medicalcause.html
McDowell, M. (2003). Nonverbal Learning Disability: Psychological tests used in the
diagnosis of NLD. Retrieved November 23, 2004, from
http://www.childdevelopmentnet.com/clinical/disorder/nld.html
McLone, D., Czyzewski, D., Raimondi, A., & Sommers, R. (1982). Central nervous system
infections as a limiting factor in the intelligence of children with myelomeningocele.
Pediatrics, 70, 338-342.
Measor, L. (1985). Interviewing: A strategy in qualitative research. In R. Burgess, Strategies
of educational research: Qualitative method. (pp. 55-77). London: Falmer Press.
Menkes, J. H. (1995). Textbook of child neurology (5th ed.). London: Williams & Wilkins.
Miles, M. B., & Huberman, A. M. (1994). Qualitative data analysis: An expanded
sourcebook (2nd ed.). Thousand Oaks, California: Sage.
Mitrushina, M., Boone, K. B., & D’Elia, L. F. (1999). Handbook of normative data for
neuropsychological assessment. New York: Oxford University Press.
Molenaar-Klumper, M. (2002). Non-verbal learning disabilities: Characteristics, diagnosis
and treatment within an educational setting. London: Jessica Kingsley.
Mooney, Dean. (2003). NLD Assessment Protocols. Retrieved November 12, 2004, from
http://www.drdeanmooney.com/rourkepro.pdf
Murray-Seegert, C. (1989). Nasty girls, thugs and humans like us: Social relations between
severely disabled and nondisabled students in high school. Baltimore: Brookes.
Myers, G. J., Cerone, S. B., & Olson, A. L. (1981). A guide for helping the child with spina
bifida. USA: Charles C. Thomas.
Myklebust, H. R. (1968). Learning disabilities: Definition and overview. In H.R. Myklebust
(Ed.), Progress in Learning Disabilities, 1 (pp. 1-15). New York: Grune & Stratton.
Myklebust, H. R. (1978). Nonverbal learning disabilities: Assessment and intervention. In
H.R. Myklebust (Ed.), Progress in learning disabilities, 3 (pp. 85-121).

294
Nagel, P. (1988). The Adams women. In Extraordinary lives: The art and craft of American
biography. Edited by W. Zinsser (pp. 91-120). Boston: Houghton Mifflin.
National Institute of Neurological Disorders and Stroke. (2001). Hydrocephalus fact sheet:
What is hydrocephalus? Retrieved April 22, 2003, from
http://www.ninds.nih.gov/health_and_medical/pubs/hydrocephalus_fs.htm
National Institute of Neurological Disorders and Stroke. (2003). Brain basics: Know your
brain. Retrieved April 22, 2003, from
http://www.ninds.nih.gov/health_and_medical/pubs/brain_basics_know_your_brain.ht
m
National Institute of neurological disorders and stroke. (2003). NINDS. Encephaloceles
Information Page. Retrieved April 22, 2003, from
http://www.ninds.nih.gov/health_and_medical/disorders/encephaloceles.htmNINDSEn
cephaloceles
Nesbitt, E. (2000). Researching 8 – 13 yr olds’ perspectives on their experience of religion.
In Ann Lewis and Geoff Lindsay, Researching children’s perspectives (pp. 135-148).
Buckingham: Open University Press.
Nolte, J. (1993). The human brain: An introduction to its functional anatomy (3rd ed.).
Missouri: Mosby.
Nonaka, I., & Takeuchi, H. (1995). The knowledge creating company. New York: Oxford
University Press.
Obrzut, J. E., & Hynd, G. W. (1991). Neuropsychological foundations and learning
disabilities: A handbook of issues, methods & practice. San Diego: Academic Press.
Osterreith, P. A. (1944). Le test de copie d’une figure complexe. Archives de Psyichologie,
30, 206-356; translated by J. Corwin and F.W.Bylsma (1993), The Clinical
Neuropsychologist, 7, 9-15.
Ozols, E. J., & Rourke, B. P. (1988). Characteristics of young learning-disabled children
classified according to patterns of academic assessment: Auditory-perceptual and
visual-perceptual abilities. Journal of Clinical Child Psychology 17, 44-52.
Parlett, M., & Hamilton, D. (1972). Evaluation as illumination: A new approach to the study
of innovatory programs. Occasional paper. Centre for research in the educational
sciences.
Patton, M. (1990). Qualitative evaluation research methods (2nd ed.). London: Sage.
Patton, M. (2002). Qualitative research and evaluation methods (3rd ed.). USA: Sage.
Pelletier, P. M., Ahmad, S., & Rourke, B. P. (2001). Classification rules for basic
phonological processing disabilities and nonverbal learning disabilities: Formulation
and external validity. Child Neuropsychology, 7, 108-118.

295
Putman, J. W., Spiegel, A. N., Bruininks, R. H. (1995). Future directions in education and
inclusion of students with disabilities. Exceptional Children, 6 (6), 553-576.
Rapaport, D., Gill, M., & Shaffer, R. (1946). Diagnostic psychological testing: The theory,
statistical evaluation, and diagnostic application of a battery of tests. Chicago: Year
Book Publishers.
Reigel, D. H. (1989) Spina bifida. Pediatric neurosurgery (2nd ed.). Philadelphia: W.B.
Saunders.
Reitan, R. M. & Wolfson, D. (1993). The Halstead-Reitan Neuropsychological Test Battery:
Theory and clinical interpretation. Tueson, AZ: Neuropsychology Press.
Rogosky-Grassi, M. A. (1993). Working with perceptual-motor skills. In F. L. Rowley-Kelly
& D. H. Reigel (Eds.), Teaching the student with spina bifida. (pp. 193-209).
Baltimore: Brookes.
Roman, M. (1998). The syndrome of nonverbal learning disabilities: Clinical description and
applied aspects. Current Issues in Education, 1, 1-16.
Rourke, B. P. (Ed.). (1985). Neuropsychology of learning disabilities: Essentials of subtype
Analysis. New York: Guilford Press.
Rourke, B. P. (1989). Nonverbal learning disabilities: The syndrome and the model. New
York: Guilford.
Rourke, B. P. (Ed.). (1991). Neuropsychological validation of learning disability subtypes.
New York: Guilford.
Rourke, B. P. (Ed.). (1995). Syndrome of nonverbal learning disabilities. Neuro-
developmental manifestations. New York: Guilford.
Rourke, B. P., & Casey, J. (1989). Syndrome of nonverbal learning disabilities: Age
difference in personality/behavioural functioning. In B. P. Rourke, Nonverbal learning
disabilities: The syndrome and the model (pp. 100-110). New York: Guilford.
Rourke, B. P., & Conway, J. A. (1997). Disabilities of arithmetic and mathematical
reasoning: Perspective from neurology and neuropsychology. Journal of Learning
Disabilities, 30, 34-46.
Rourke, B. P. & Del Dotto, J. E. (1994). Learning disabilities: A neuropsychological
perspective. Thousand Oaks, California: Sage.
Rourke, B. P. & Tsatsanis, K. D. (1996). Syndrome of nonverbal learning disabilities:
Psycholinguistic assets and deficits. Topics in Language Disorders, 16 (2), 30-44.
Rourke, B. P., & Tsatsanis, K. D. (2000). Syndrome of nonverbal learning disabilities and
asperger syndrome. In A. Klin, F. Volkmar, & S. S. Sparrow (Eds.), Asperger
syndrome (pp. 231-253). New York: Guilford.
Rourke, B. P., Bakker, D.J., Fisk, J. L., & Strang, J. D. (1983). Child neuropsychology: An
introduction to theory research and clinical practice. New York: Guilford.

296
Rourke, B. P., Del Dotto, J. E., & Jerel E. (1994). Learning disabilities: A
neuropsychological perspective. Developmental clinical psychology & psychiatry, v. 30.
Thousand Oaks, California: Sage.
Rourke, B. P., Dietrich, D. M., & Young. G. C. (1973). Significance of WISC verbal-
performance discrepancies for younger children with learning disabilities. Perceptual
and motor skills, 36, 275-282.
Rourke, B. P., Fisk, J. L., & Strang, J.D. (1986). Neuropsychological assessments of
children: A treatment oriented approach. New York: Guilford.
Rourke, B. P., Fisk, J. L., Bakker, Dirk J., & Strang, J. D. (1983). Child neuropsychology:
An introduction to theory, research and clinical practice. New York: Guilford.
Rourke, B. P., van der Vlugt, H., & Rourke, S. B. (2002). Practice of child-clinical
neuropsychology: An introduction. The Netherlands: Swets & Zeitlinger.
Rourke, B. P., Young, G. C., & Flewelling, R. W. (1971). The relationships between WISC
verbal performance discrepancies and selected verbal, auditory-perceptual, and
problem-solving abilities in children with learning disabilities. Journal of Clinical
Psychology, 17, 475-479.
Rourke, B. P., Young, G. C., Strang, J. D., & Russell, D. L. (1986). Adult outcomes of
central processing deficiencies in childhood. In I. Grant & K. M. Adams (Eds.),
Neuropsychological assessment of neuropsychiatric disorders (pp. 244-267). New
York: Oxford University Press.
Rovet, J. F. (1995b). Turner syndrome. In B. P. Rourke (Ed.), Syndrome of nonverbal
learning disabilities: Neurodevelopmental manifestations (pp. 351-371). New York:
Guilford.
Rowley-Kelly, F. L. (1993). Social acceptance and disability awareness. In Teaching the
student with spina bifida (pp. 245-280). Baltimore: Brookes.
Rowley-Kelly, F. L., & Reigel, D. (1993). Teaching the student with spina bifida. Baltimore:
Brookes.
Ruddock, J., Chaplain, R., & Wallace, G. (1996). School improvement: What can pupils tell
us? New York: Falmer Press.
Russell, C. (2004). Understanding nonverbal learning disorders in children with spina bifida.
Teaching Exceptional Children, 36, 8-13.
Salomon, G. (1991). Transcending the qualitative-quantitative debate: The analytic and
systemic approaches to educational research. Educational Researcher, 20, 10-18.
Sandler, A. (1997). Living with spina bifida: A guide for families and professionals. London:
University of North Carolina Press.

297
Sattler, J. M. (1974). Assessment of children’s intelligence (Rev. ed.). Philadelphia:
Saunders.
Schmidt, Michael. (2005). Rey auditory verbal learning test: A handbook (RAVLT).
Psychological assessment resources. Inc. Retrieved December 2, 2005, from
http://www3.parinc.com
Semel, E., Wiig, E., Secord, W. (1980). Clinical Evaluation of Language Fundamentals (3rd
ed.) (CELF-3). Retrieved June 14, 2004, from
http://marketplace.psychcorp.com/PsychCorp.com
Semrud-Clikeman, M. & Hynd, G. (1990). Right hemispheric dysfunction in nonverbal
learning disabilities: Social, academic and adaptive functioning in adults and children.
Psychological Bulletin, 107, 196-207.
Shaffer, J., Friedrich, W., Shurtleff, D., & Wolf, L. (1985). Cognitive and achievement
status of children with myelomeningocele. Journal of Pediatric Psychology, 10, 325-
336.
Smith, K. L. (1997). Mixing and matching: Methods and models. In J. C. Green & V. J.
Caracelli (Eds.) Sociological Quarterly, (16), 415-428.
Smith, L. A., & Rourke, B. P. (1995). Callosal agenesis. In B. P. Rourke (Ed.), Syndrome of
nonverbal learning disabilities: Neurodevelopmental manifestations (pp.45-95). New
York: Guilford Press.
Soare, P. L., & Raimondi, A. J. (1977). Intellectual and perceptual-motor characteristics of
treated myelomeningocele Children. American Journal of Disabled Children, 131,
199-204.
Spina Bifida Association of South Australia. (2005). General facts: How does it occur?
Retrieved May 4, 2006, from http://www.spinabifida.asn.au
Spradley, J. P. (1979). The ethnographic interview. New York: Holt, Rinehart & Winston.
Spreen, O., & Strauss, E. (1998). A compendium of neuropsychological tests. Administration,
norms, and commentary (2nd ed.). New York: Oxford University Press.
Stake, R. E. (1994). Case Studies. In N. K. Denzin & Y. S. Lincoln (Eds.). Handbook of
qualitative research (pp. 435-454). Thousand Oaks, California: Sage.
Stake, R. E. (1995). The Art of Case Study Research. Thousand Oaks, California: Sage.
Staub, D. & Peck, C. A. (1995). What are the outcomes for nondisabled students?
Educational Leadership, 52 (4), 36-40.
Stewart, K. (2002). Helping a child with nonverbal learning disorder or asperger syndrome.
USA: New Harbinger.

298
Strang, J. D., & Rourke, B. P. (1985). Adaptive behavior of children who exhibit specific
arithmetic disabilities and associated neuropsychological abilities and deficits. In B. P.
Rourke (Ed.), Neuropsychology of learning disabilities: Essentials of subtype analysis
(pp. 303-328). New York: Guilford Press.
Sturman, A. (1999). Issues in educational research: Qualitative Data Analysis. New York:
Permagon.
Tanguay, P. (2002). Nonverbal learning disabilities at school. UK: Jessica Kingsley.
Tanguay, P. (1999). NLD = VIQ > PIQ …It ain’t necessarily so. Retrieved September 1,
2004, from http://www.nldontario.org/articles/viqvspiq.html
Tashakkori, A., & Teddlie, C. (2003). Handbook of mixed methods in social and behavioural
research. Thousand Oaks, California: Sage.
Telzrow, C., & Bonar, A. (2002). Responding to students with nonverbal learning
disabilities. Teaching Exceptional Children, 34, 8-13.
Tew, B. (1978). The psychology and educational consequences of spina bifida and its
complications. Developmental Medicine and Child Neurology, 20, 240.
Tew, B., & Laurence, K. M. (1979). The clinical and psychological characteristics of
children with the “Cocktail Party Syndrome”. Zeitschrift fur Kinderchirurgie, 28
(Suppl.1), 360-367.
Tew, B., & Laurence, K. M. (1984). The Relationship between intelligence and academic
achievements in spina bifida adolescents. Zeitschrift fur Kinderchivurgie, 39 (Suppl.2),
122-124.
Thompson, S. (1997). The sources for nonverbal learning disorders. USA: Lingui.
Tranel, D., Hall, L. E., Olson, S., & Tranel, N. (1987). Evidence for a right hemisphere
developmental learning disability. Developmental Neuropsychology 3, 113-127.
Tsatsanis, K. D., & Rourke, B. P. (1995). Conclusions and future directions. In B. P. Rourke
(Ed.) Syndrome of nonverbal learning disabilities: Neurodevelopmental
manifestations (pp. 476-496). New York: Guilford Press.
Tsatsanis, K. D., & Rourke, B. P. (1995b). de Lange syndrome. In B. P. Rourke (Ed.),
Syndrome of nonverbal learning disabilities: Neurodevelopmental manifestations
(pp. 171-205). New York: Guilford Press.
Turner, A. (1986). Upper-limb function of children with myelomeningocele. Journal of
Medicine and Child Neurology, 28, 790-798.
Vacca, D. M. (2001). Confronting the puzzle of nonverbal learning disabilities. Journal of
Educational Leadership, 59, 26-31.
Vaughn, S. & Schumm, J. S. (1995). Responsible inclusion for students with learning
disabilities. Journal of Learning Disabilities, 18 (5), 264-70.

299
Volden, J. (2002). Nonverbal learning disability: What the SLP needs to know. ASHA
Leader, 7, 4-15.
Voeller, K. K. S. (1986). Right-hemisphere deficit syndrome in children. American Journal
of Psychiatry, 143, 1004-1009.
Warner-Rogers, J. (1996) Congenital disorders: Structural disorders. In J. G. Beaumont, P.
Kenealy & M. Rogers (Eds.). The Blackwell dictionary of neuropsychology, (pp. 232-
240). USA: Blackwell Publishers.
Webb, Sidney, & Webb, Beatrice. (1975). Methods of social study. London: Cambridge
Press.
Wechsler, D. (1989). Wechsler intelligence scale for children (WISC III) (3rd ed.). Retrieved
July 17, 2004, from http://www.marketplace.psychcorp.com
Wechsler, D. (2001). Wechsler Individual Achievement Test (WIAT II) (2nd ed). Retrieved
June 23, 2004, from http://www.marketplace.psychcorp.com
Weintraub, S., & Mesulam, M. (1983). Developmental learning disabilities of the right
hemisphere: Emotional, interpersonal and cognitive components. Archives of
Neurology 40, 463-469.
Well, A. D., Lorch, E. P., & Anderson, D. R. (1980). Developmental trends in distractibility:
Is absolute or proportional decrement the appropriate measure of interference? Journal
of Experimental Child Psychology, 30, 109-124.
Westwood, P. S. (1997). Commonsense methods for children with special needs: Strategies
for the regular classroom. New York: Routledge.
Whitney, R. (2002). Bridging the gap: Raising a child with nonverbal learning disorder.
New York: Berkeley Publishing Group.
Williamson, G. G. (Ed.). (1987). Children with spina bifida: Early intervention and
preschool programming. Baltimore: Brookes.
Wills, K. E. (1993). Neuropsychological functioning in children with spina and/or
hydrocephalus. Journal of Clinical Child Psychology, 22, 247-26.
Wills, K. E., Holmbeck, G. N., & McLone, K. D. (1990) Intelligence and achievement in
children with myelomeningocele. Journal of Pediatric Psychology, 15, 161-176.
Wolf, R., & Tymitz, B. (1977). Toward More Natural Inquiry in Education. CEDR
Quarterly, 10, 7-9.
Woods, G. E. (1979). Visual problems in the handicapped child. Child: Care, Health and
Development, 5, 303-322.

300
APPENDIX A
CHAPTER TWO: PART II
NLD associated with shunted hydrocephalus and spina bifida
The focus here is on the unique profile that characterises children with NLD associated
with hydrocephalus and spina bifida. The following discussion about hydrocephalus and its
association with various forms of spina bifida will conclude by explaining the “final
common pathway” that links residual damage from a hydrocephalic condition to an NLD
(Rourke & Del Dotto 1994, p.37).
Part II of this review looks at:
• How an NLD is linked to hydrocephalus
• White Matter
• What is hydrocephalus?
• Hydrocephalus and spina bifida
• Hydrocephalus and IQ
• How hydrocephalus damages White Matter and causes NLD
How NLD is linked to Hydrocephalus
In 1987-1988, Rourke developed the “White Matter” model which sought to account
for the neuropsychological development within the domains believed to characterise all
children who exhibit the NLD syndrome (p.113).
Rourke expresses the White Matter NLD model in terms of three principle dimensions:
1. Amount of white matter destroyed or dysfunctional. The more white matter relative
to total brain mass that is lesioned, removed or dysfunctional, the greater the
likelihood of the NLD syndrome.
2. Type and Developmental Stage of Destruction/Dysfunction. The stage of a child’s
development and the white matter lesioned has important bearing on the
manifestations of NLD characteristics.
3. Development and Maintenance of Learned Behaviours. Right hemisphere white
matter is crucial for development and maintenance of specific functions. Damage
will significantly impair learning that requires integration of information (Rourke,
1989, p.113).
301
Rourke’s three principles indicate that a significant insult to the right hemisphere is
“sufficient” to cause the NLD syndrome, the “necessary” condition being damage or
destruction of the neuronal white matter which facilitates the transmission of information
between hemispheres (Rourke, 1989, p.114).
White Matter
The Brain has three principle types of white matter fibres, commissural, association and
projection:
1. Commissural nerve fibres join right and left (↔) hemispheres. These cross the
midline and interconnect similar regions in both cerebral hemispheres. There are
three sets of commissural fibres: (i) corpus collosum, (ii) anterior, posterior and
habenular commissures and (iii) hippocampal commissure fibres. The corpus
collosum comprises the largest set of these fibres (Rourke, 1989);
2. Association nerve fibres interconnect cortical (outer layer of tissue) regions within
the same hemisphere, back-front. These may be short when connecting
neighbouring cells or long when connecting remote groups of cells (Rourke, Bakker,
Fisk & Strang, 1983);
3. Projection nerve fibres project down-up (↑) from the diencephalon to the cerebral
hemispheres and from the hemispheres to the diencephalon, brain stem and spinal
cord (Rourke 1989, p.115). Diencephalon means “in-between-brain” which means
that this part of the central nervous system is situated between the cerebral
hemispheres and the brain stem (Nolte, 1993. p.3).
Conditions such as hydrocephalus are expected to principally affect the right-left
commissural fibres and down-up projection fibres, leaving association fibres relatively
undamaged (Rourke, 1989). It is here that a link between hydrocephalus and NLD is made.
Commissural fibres link the same areas of opposite hemispheres and projection fibres
transmit information from the diencephalon to hemispheres and from hemispheres to the
diencephalon, brain stem and spinal cord. Damage to right hemisphere white matter which
significantly interferes with these intercommunications between “systems” would be
expected to result in development of the NLD syndrome (p.116).
What is Hydrocephalus?
Hydrocephalus is a condition characterised by excessive cerebrospinal fluid (CSF)
within the ventricles or “caves of the brain”. It is caused by an obstruction that disrupts
normal circulation pathways (Rowley-Kelly & Reigel, 1993, p.10). Cerebrospinal fluid is a
clear colourless fluid that bathes the brain and spinal cord tissues and it is continuously

302
reabsorbed (Llewellyn & Green, 1987). About 600 ml of cerebrospinal fluid is produced
each day. Because there is continuous secretion of CSF by three brain ventricles, a specific
amount must be absorbed by the body to maintain a proper balance. Absorption occurs as
CSF exits the 4th ventricle to the outer surface of the brain and spinal cord and finally enters
the blood stream. This CSF production and absorption process “ensures a stable fluid
pressure” (Williamson, 1987, p.82).
Cerebrospinal fluid has three important life-sustaining functions. It
1. Keeps the brain tissue buoyant and acts as a cushion or “shock absorber”;
2. Acts as a vehicle for delivering nutrients to the brain and removes waste;
3. Flows between the head and spine to compensate for changes in the amount of blood
within the brain (National Institute of Neurological Disorders and Stroke, 2001).
Extra cell space, capillaries, lipids (organic compounds that are insoluble in water) and
proteins found in white matter allow a normal brain to be bioelastic, with normal CSF
pressure being lower than the brain’s bioelastic limits “so stress is distributed within the
brain tissue” (Dennis, 1996, p.407). Hydrocephalus upsets this natural compensatory
process, increases pressure within the ventricles thus raising effective CSF pressure. The
region around the ventricles receives the greatest stress and as it yields, the “ventricles
enlarge which increases the pressure” on brain tissue (p.407). Enlargement of the ventricular
system is expected to occur very close to the site of obstruction (Barron, Fennell & Voeller,
1995). Brain damage occurs within 12 hours of CSF obstruction (Dennis, 1996).
Hydrocephalus results from a number of congenital conditions which include spina
bifida. In the case of spina bifida, hydrocephalus is secondary to a structural malformation
therefore it does not represent a definitive entity or clinical syndrome (Fletcher & Levin,
1988). In young children, cerebral sutures are not fully fused and the skull expands to
accommodate ventricular swelling which leads to an enlarged head whereas in older children
where sutures are fused, an enlarged head does not always accompany hydrocephalus
(p.264).
Hydrocephalus can be classified according to whether the cause is congenital or
postnatal, the condition is communicating or non-communicating or the condition is
uncomplicated (hydrocephalus only) or complicated (associated with other clinical
problems).

303
Most congenital forms of hydrocephalus are non-communicating with obstruction
usually occurring within the 4th ventricle (Fletcher & Levin, 1988). Perhaps the largest
group of non-communicating hydrocephalic conditions stem from conditions of the spine or
skull (spina bifida or cranium bifidum) known as myelodysplasias. This term is used to
describe defective development of any part of the spinal cord (Eynon et al., 2002).
Hydrocephalus and Spina Bifida
Spina Bifida is a defect in the neural tube closure that may cause a complex congenital
disability (Fletcher et al., 1992). The term congenital presupposes the anomaly developed
during the prenatal phase and was evident at birth (Warner-Rogers, 1996). Fusion of
vertebrae arches is an important step in embryonic development (2 weeks after conception
until the end of the 7th or 8th week) when the two sides of the spinal canal in the back grow
together “to form the cavity for the spinal cord” (Andrews & Elkin, 1981, p.6) (Figure A1).
Figure A1.
Neural tube closure
Used with permission from Mayo Foundation for Medical Education and Research MFMER, 2003.
At 21 days, folds of tissue on the back of a developing embryo are rapidly growing
together (see arrows). At 22 days, the growth is almost complete. By 28 days, if the tissue
fails to close completely, development of the spine, muscle, and skin in this region is
affected and the baby will be born with spina bifida.
Incidence varies among countries and races (Rowley-Kelly and Reigal, 1993). Spina
bifida occurs in 4-5 births per 1,000 in Northern Ireland, is lower among African Americans
than among Anglo-Americans, very low in Japan but high in China (Wills, 1993).
According to the Spina Bifida Association of South Australia (2005), the incidence of spina
bifida in Australia is 2 in 1,000 (http://www.spinabifida.asn.au/). The cause of neural tube

304
anomalies is unknown but it is likely that genetic defects, “probably at more than one locus,
interact with environmental factors” (Menkes, 1995, p.250).
There is a slightly higher occurrence of spina bifida among females than males (Reigel,
1989) with the ratio of 1.3:1 girls born with spina bifida to boys (Anderson & Spain, 1977).
This slight difference may be due to a higher rate of spontaneous abortion of non-viable
foetuses among males (Wills, 1993). The fact that open spina bifida has been reported to be
13 times more common in spontaneously aborted foetuses than in full-term infants leads one
to question the true risk of neural tube defects for any given parent (Reigel, 1989). When
investigating IQ levels and sex differences, Wills (1993) found the lower average IQ scores
with girls was possibly because more survive, resulting in a higher population of girls with
shunts than boys.
Neural tube malformations categorised as cranium bifidum, such as encephalocele and
anencephalocele, are included in the term spina bifida (Andrews & Elkin 1981, Year Book
Australia, 2001). These defects occur “when there is a failure to fuse at the head end of the
nerve cord” (Anderson & Spain, 1977, p.14). Spina Bifida and cranium bifidum all share
failure of the bone to fuse along the vertebral column or bones of the skull (Menkes, 1995).
Protrusion of spinal tissue and CSF is often visible as a bulging sac. The physical and
cognitive outcomes of spina bifida depend on lesion level and paralysis may be experienced
below the level of lesion.
Figure A2.
The normal bony spine
Myers, Cerone and Olson, 1981, p.147.

305
Spina Bifida Cystica refers to meningocele and myelomeningocele lesions. It is the
second most common birth defect after cerebral palsy and the most common cause of
congenital hydrocephalus, the primary cause being failure of the neural tube to close. This is
because some of the spinal bones which normally protect and cover the delicate nerves of the
spinal cord fail to develop properly and the normal bony projections are split or “bifid”.
Through this gap, either membranes that surround the spinal cord called meninges or spinal
cord itself protrude, depending on the type of spina bifida (Anderson & Spain, 1977). Spina
Bifida presents with several degrees of severity.
Spina Bifida Occulta is the most common, innocent and hidden form which is
characterised by absence of a small portion of the vertebrae. This can occur in any vertebra
but is most common at the base of the back or lower spine (Mayo Foundation for Medical
Education and Research MFMER, 2003) (Figure A5). The only visible sign of defect may be
a discolouration of the skin, a dimple in the skin or a tuft of hair known as a faun’s tail
(Dunning, 1992). The occulta type does not involve herniation of meninges or contents of
spinal cord and rarely requires treatment (Eynon et al., 2002). The defect is not detectable
by physical examination and is usually discovered on an x-ray. While there may be minor
underlying nerve damage, it is usually of little or no consequence to the person (Rowley-
Kelly & Reigel, 1993).
Figure A3.
Spina bifida occulta
Myers, Cerone and Olson, 1981, p.116.
Spina Bifida Meningocele is an abnormality present at birth which is identified by a
smooth cystic sac protruding from a defect in the skull or the vertebral column. The
herniated cyst is filled with cerebrospinal fluid and either cerebral or spinal meninges but
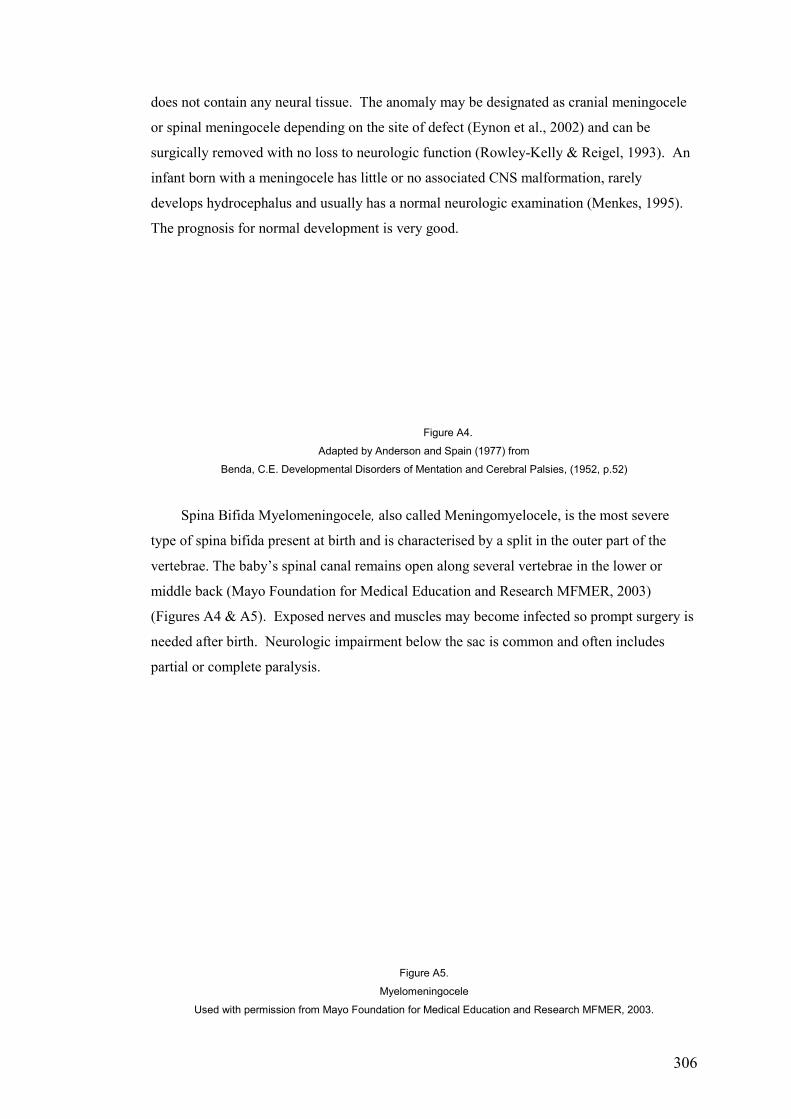
306
does not contain any neural tissue. The anomaly may be designated as cranial meningocele
or spinal meningocele depending on the site of defect (Eynon et al., 2002) and can be
surgically removed with no loss to neurologic function (Rowley-Kelly & Reigel, 1993). An
infant born with a meningocele has little or no associated CNS malformation, rarely
develops hydrocephalus and usually has a normal neurologic examination (Menkes, 1995).
The prognosis for normal development is very good.
Figure A4.
Adapted by Anderson and Spain (1977) from
Benda, C.E. Developmental Disorders of Mentation and Cerebral Palsies, (1952, p.52)
Spina Bifida Myelomeningocele, also called Meningomyelocele, is the most severe
type of spina bifida present at birth and is characterised by a split in the outer part of the
vertebrae. The baby’s spinal canal remains open along several vertebrae in the lower or
middle back (Mayo Foundation for Medical Education and Research MFMER, 2003)
(Figures A4 & A5). Exposed nerves and muscles may become infected so prompt surgery is
needed after birth. Neurologic impairment below the sac is common and often includes
partial or complete paralysis.
Figure A5.
Myelomeningocele
Used with permission from Mayo Foundation for Medical Education and Research MFMER, 2003.

307
The CSF which baths the brain and spinal cord distends the sac and leaks from the
surface (Dunning, 1992). If not treated, the sac will eventually scar over and heal but will
leave a weak and vulnerable swelling. Myelomeningocele involves the lining or meninges
of the spinal canal, the spinal cord and nerves and almost all children are treated with an
operation to remove the cyst and close the opening in the spine to reduce the risk of infection
(Rowley-Kelly & Reigel, 1993). Myelomeningocele affects about 95% of spina bifida cases
(Menkes, 1995).
The spinal cord not only protrudes into the sac but is itself “abnormal” resulting in
permanent unrepairable neurological disability (Anderson & Spain 1977, p.14). There is
always partial or complete paralysis and loss of sensation in the lower part of the body with
level and severity determined by the site and nature of the defect (Dunning, 1992). In
approximately 95% of cases, the most common anomalies associated with
myelomeningoceles in the lumbar-sacral region are the Arnold Chiari 2 malformation and
80-90% will develop progressive hydrocephalus that requires shunting (Bohan, Dominguez,
Fenstermacher, Kramer, Fletcher et al., 1994). A striking feature of the Arnold-Chiari 2
malformation is that a “tongue of tissue” usually derived from the lower lobes of the
cerebellum extends downwards into the upper spinal canal which may frequently cause
gagging and difficult swallowing for the child (Anderson & Spain, 1977, p.40).
Encephalocele describes lesions associated with cranium bifidum where bones of the
skull fail to fuse. Seventy-five percent of encephaloceles extend from the back of the head
and 25% extend from regions around the eyes, nose or forehead. This failure of bone fusion
results in a bony cleft through which meninges and varying amounts of brain or spinal cord
tissue herniate (Menkes, 1995) (Figures A6 & A7). Neural complications of an
encephalocele over the cervical area may involve protrusion of cerebellum through the bony
defect known as the Arnold-Chiari Malformation Type 3 and associated hydrocephalus.
Other complications include developmental delay, mental retardation, seizures and visual
problems. Incidence is about 1/10th that of spinal neural tube defects (Menkes, 1995) and “is
commoner in girls – in a proportion of about 7 to 3” (Lorber 1974, p.5).

308
Figure A6. Figure A7.
Encephalocele Encephalocele
Lorber, 1974, p.4 Used with permission from eMedicine.com.Inc. 2004
If the encephalocele is quite small and covered with skin, the prognosis is good.
However, if the swelling is large and covered by thin membrane only, the outlook is very
poor (Anderson & Spain, 1977). Long term prognosis for a child born with an encephalocele
depends largely upon the presence of brain tissue in the sac, the size of the sac and
associated hydrocephalus following surgical repair of the lesion (Date, 1993).
Approximately 60% of patients require placement of a shunt after removal of their
encephalocele (http://author.e.medicine.com, 2003). Herniation of cerebral tissue through
the skull defect is expected to be associated with sensory, motor and cognitive deficits
(Barron et al., 1995).
The images below illustrate two different children each born with a
lipomyelomeningocele or closed neural tube defect in the lumbar region. Although motor or
sensory impairments may not be evident at birth, “subtle, progressive neurologic
deterioration” may become evident in later childhood or adulthood (Sandler, 1997).
Figure A8.
Lipomyelomeningocele
Used with permission from Professor John D. Loeser, M.D.
Anencephaly is the most common major central nervous system malformation in the
West (Menkes, 1995) and is seen 3-7 times more frequently in female than male newborns.

309
Anencephaly results from a “virtual lack of development of the brain, only the brain stem
being present” and is incompatible with life (Andrews & Elkin 1981, p.7).
The occulta and meningocele types of spina bifida have a greater survival rate and
present fewer problems for educators but since encephalocele and myelomeningocele
together cause over 95% of all children born with manifested spina bifida (Menkes, 1995),
educators are mainly concerned with these children (Andrews & Elkin, 1981). Before shunt
systems were used on a large scale in the late 1950’s to relieve the abnormally high pressure
of the CSF to a normal level, few children with encephalocele and myelomeningocele
survived long enough to create interest and concern among educators for their educational
and psychological needs (Anderson & Spain, 1977).
Shunting
Hydrocephalus is a major complication in 95% of spina bifida cases. Sometimes the
raised pressure in and around the brain is temporary and the hydrocephalus becomes
naturally arrested but usually the process is progressive. When fluid continues to collect, the
pressure rises and must be relieved promptly to minimise brain damage (Dunning, 1992). To
relieve the excessive pressure, a shunt system made of silastic tubing is inserted surgically
into one of the ventricles of the brain through a burr-hole in the skull (Figure 9). With the
shunt’s tubing threaded beneath the skin, the spinal fluid drains continuously to a place
where it can be disposed of, usually the abdomen or heart (Figure 9).
Figure A9.
The Holter shunting system
Lorber, 1973, pp.11, 12.
To ensure a one-way flow, a valve which includes a pumping chamber is incorporated
into the system. Pressing the pumping chamber allows a medical practitioner to gauge shunt
functionality. A valve that fails to fill after depressing the pumping chamber may indicate a
malfunction between the catheter and valve. The shunt does not cure hydrocephalus but

310
rather controls it. It prevents excessive head growth and allows the brain to grow normally.
A well-placed shunt “serves to increase the functional capabilities of the child’s brain and
eventuates in a generally better prognostic picture” (Rourke et al., 1983, p.179). Even after
treatment, ventricles may not return to normal size due to continuing force on ventricle
walls, this force “directly proportional to the ventricular area” and pressure within the
ventricle. While shunting lowers CSF pressure, the surface area of the ventricles may
remain enlarged causing abnormal stress on the brain. Shunt treatment in children therefore
may only partially reverse neuropathological changes and may not fully “restore cognitive
function” (Dennis 1996, p.409).
Figure A10.
Shunt system to the abdominal cavity
Dunning, 1992, p.7.
Blockage or obstruction of CSF through the shunt tubing is common and unavoidable
due to normal growth and development. Onset of symptoms may be very sudden with
vomiting, recurring headache or seizure and if not relieved within hours, can be fatal
(Dunning, 1992, p.7). Headaches typically begin in early morning and intensify. They may
be accompanied by clumsiness, tremor, incontinence and affect upper and lower limbs.
Rourke et al. (1986) stress the need to monitor the neurological and neuropsychological
status of such children.

311
Hydrocephalus and IQ
In individuals with hydrocephalus and spina bifida, IQ tends to correlate with level of
spinal cord lesion, the higher the lesion the lower the IQ (Hunt & Holmes, 1975; Shaffer et
al., 1985; Rourke, 1989; Holler, 1995). Children with spina bifida in the 6 – 13 age range
whose hydrocephalus was severe enough to require surgical intervention were found to have
significantly lower performance than verbal scores than children with a history of arrested
unshunted hydrocephalus (Fletcher et al., 1996). Most studies report lower IQ scores in
children with spina bifida than in other aetiological groups which Anderson et al. (2001)
contend would be expected “given the major cerebral anomalies associated with the
condition” (p.194). McLone, Czyzewski, Raimondi and Sommers (1982) examined IQ
results of 167 children with myelomeningocele. Results associated IQ scores with shunt
complications and found those who were shunted but had no shunt complications had an
average IQ of 95 but those who had shunt complications had an average IQ of only 73.
Severity of hydrocephalus at birth was not found to be indicative of future intelligence and
the mental retardation often associated with myelomeningocele was reported to be an
“acquired deficit primarily related to ventriculitis and/or meningitis” (McLone et al. 1982,
p.341).
Fletcher and Levin (1988) report studies of children with myelomeningoceles,
meningoceles and encephaloceles which found “the occurrence of hydrocephalus reduces
intellectual skills” (p.266). Soare and Raimondi (1977) discovered a significant link
between lesion level, performance and IQ especially in subjects with myelomeningocele and
hydrocephalus. Individuals with higher lesion levels were found to experience greater
perceptual-motor difficulties and those with lower lesion levels “tended to have higher IQs”
(p.296). Wills et al. (1990) study of intelligence and achievement in children with
myelomeningocele found children with myelomeningocele, shunted hydrocephalus and
higher level lesions performed more poorly on visuomotor tasks than children with lower
lesions. Dennis et al. (1981) examined relationships of visual, motor and seizures problems
with psychometric intelligence and found ocular abnormalities, any form of motor
disturbance, and seizures lower performance and full scale intelligence scores. As a group,
Fletcher and Levin (1988) say individuals with hydrocephalus associated with a neural tube
defect have intelligence quotients that approximate one standard deviation below the mean
but in the absence of complications, individuals may function within the normal level of
intelligence (Fletcher et al., 1995; Wills, 1993).
Hunt and Holmes (1975) discuss effects of a number of shunt revisions and subsequent
intelligence in 66 children. Evidence indicated the proportion of “normal” to “subnormal”

312
children in their clinical population was not influenced by number of shunt revisions but
rather age at which shunt revisions occurred was more important, generally the earlier the
better. Although cognizant of studies unable to identify a relationship between numbers of
shunt revisions and reduction in cognitive skills, Fletcher et al. (1995) suggest shunting and
possibly shunt revisions have varying effects on cognitive abilities. Hydrocephalus in
conjunction with spina bifida may cause attention problems, language deficits especially
comprehension of abstract language, and the production of irrelevant speech (Warner-
Rogers, 1996).
How hydrocephalus damages white matter and causes and NLD
The left hemisphere’s “pattern of connectivity” is predominantly intra-regional whereas
the right hemisphere’s is predominantly inter-regional (Rourke, 1989, p.63). The right
hemisphere’s salience for inter-modal integration of novel and complex information, notably
deficient in individuals with NLD, highlights the importance of white matter integrity for
normal childhood development.
The brain and nervous system comprise many different types of cells and the primary
functional unit is a cell called a neuron. All sensations, movements, thoughts, memories, and
feelings result from signals that pass through neurons. Neurons consist of three parts, a cell
body, dendrites and axon (Figure A11). The cell body (purple) contains the nucleus.
Dendrites resemble branches that extend out from the cell body to receive messages from
other nerve cells. Signals that pass from dendrites and through the cell body may travel
away from the cell body down the long slender axon cable. The “terminal” at the other end
of the axon cable carries a message to another neuron (Eynon et al., 2002).
A fatty molecule called myelin forms around the axon to provide insulation and helps
“nerve signals travel faster and farther” (National Institute of Neurological Disorders and
Stroke, 2003). This light-coloured fatty substance is often called “white matter” which
Tanguay (2002) defines as the brain’s “wiring system” (p.24). The layered tissue or myelin
sheath surrounding nerve fibres acts like an insulator in an electrical system to ensure that
messages sent by nerve fibres are not lost enroute.

313
Figure A11.
Neuron and myelin sheath
Used with permission from Adam Inc.
White matter covers axons connect the layer of grey matter on the surface of a cerebral
hemisphere with other centres of the brain and spinal cord. It plays a critical role in the
accurate and rapid transmission of messages within the brain and damage to right
hemisphere white matter will impair or “short circuit” this process (p.25) which means a
signal may not be sent accurately or it may not reach its destination.
The myelination process begins prenatally and involves a gradual increase in the
thickness of myelin sheaths that surround axons. It begins in the spinal cord by the third
month of gestation and myelination of the human brain begins during the 5th foetal month
and “proceeds rapidly during the first 2 years of postnatal life” (Fuerst & Rourke, 1995,
p.29). Of particular interest is that once fibre tracts are covered with myelin, they begin to
function maturely which may account for foetal reflexes (Rourke et al., 1983). Tracts are
neuronal axons that group together to form a pathway (Eynon et al., 2002). Only a few areas
and tracts are completely myelinated at birth (Rourke et al., 1983). Myelination continues
through adolescence and is not complete until early adulthood during which time white
matter is particularly vulnerable to disruption or damage (Anderson et al., 2001).
Rourke and associates found a group afflicted from their earliest developmental stages
with a hydrocephalic condition and who manifested the NLD syndrome did sustain
significant damage or destruction of right hemisphere white matter from lesions caused by
the hydrocephalic condition. Over time, Fletcher (1998) believes hydrocephalus may be
associated with disruption of the myelination process and may result in overall reduction in
brain size.

314
Neurobehavioral characteristics that result from disturbance of the normal myelination
process are reported to be impaired information processing capacity, slowed response speed
and reduced attention (Anderson et al., 2001). For accurate and rapid transmission of
messages, such capacities demand inter-modal integration of information from various
sources and intact connections between hemispheres. This complex process therefore relies
heavily upon integrity of right hemisphere white matter.
Summary
This review has looked at the relationship between hydrocephalus, spina bifida and a
Nonverbal Learning Disability. Damage or destruction of white matter is expected to short
circuit the message transmission process which Rourke (1989) says is “sufficient” to cause
the NLD syndrome (p.114). Given the significant damage to large portions of neuronal
white matter principally in the right hemisphere expected from excessive accumulation of
CSF, individuals with hydrocephalus are a Level 1 risk for manifestation of the NLD
syndrome (Fletcher et al., 1995; Tsatsanis & Rourke, 1995).
This provides a biological link between hydrocephalus and a Nonverbal Learning
Disability. Damaged commissural fibres and projection fibres cause inter-communication
problems which characterise a student with NLD. Such damage highlights the importance of
white matter integrity for integration of new and complex information between hemispheres.
Under these circumstances, where deterioration of white matter interferes with right more
than left hemisphere functioning due to the grey-white ratios, the NLD syndrome would be
expected to develop. Rourke and Del Dotto (1994) reaffirm when they hypothesise that
“disordered myelinization and/or myelin functioning” is considered to be the “final common
pathway” that eventuates in the NLD syndrome (p.37).

315
APPENDIX B
SUMMARY OF STUDIES
Intelligence and achievement in children with myelomeningocele
(Wills, Holmbeck & McLone, 1990)
NOTE: To protect accuracy and integrity of study findings, direct author extracts have
been used in some instances.
Purpose: To explore the frequency with which particular score discrepancies such as
verbal-performance split, differences between reading and arithmetic achievement scores
and age effects on test performance appear among myelomeningocele children.
Total sample: 89 children 4-14 years with myelomeningocele
71 children had spina bifida and shunted hydrocephalus
Children whose verbal and performance tests fell below 70 were excluded. No subject had a
known seizure disorder.
Measures used to assess global IQ corresponded to:
• WISC-R or WPPSI Full Scale IQ, Stanford-Binet IQ score or MSCA General
Cognitive Index;
• WRAT-R (reading, spelling, arithmetic);
• VMI (Visual Motor Integration – to copy increasingly complex geometric designs).
All tests were administered by staff psychologists or interns during routine outpatient
hospital appointments.
Results: Children scored below population average but within normal range on most
tests. Negative correlations emerged between age and performance. The study focused on
difficulties involving visuomotor functioning and arithmetic calculation and spared other
abilities. Greatest deficits (12 points or more) were found on PIQ, arithmetic achievement,
visual-motor integration. With increasing age, children fell further behind age-peers on
arithmetic and visual-motor performance but reading spelling and VIQ scores “improved
with age at the same rate as the general population” (p.171). Shunted children with higher

316
level lesions that may affect hand-arm function and reduce speed and dexterity had poorer
visuomotor performance, which may widen V-P discrepancy as age increases.
V-P discrepancies occurred more than twice as often among the myelomeningocele children
as among the general population and almost all discrepancies were due to marked deficits in
PIQ relative to VIQ.

317
Early Hydrocephalus
(Fletcher, Brookshire, Bohan & Timothy, 1995)
Purpose: To investigate neurobehavioural characteristics of hydrocephalus in relation
to the NLD syndrome.
Total sample: 145 children 5-14 years with spina bifida and hydrocephalus
40 children had spina bifida and shunted hydrocephalus
Children whose scores on both verbal and performance tests fell below 70 on WISC-R were
excluded.
Measures:
• Grooved Pegboard Test Performance: Motor and Psychomotor Skills
• VMI (Beery)
• Judgment of Line Orientation (JLO – motor-free)
• McCarthy Scales of Children’s Abilities (for children with spina bifida) Verbal and
Perceptual performance
• WISC-R (for children with spina bifida)
• Tests of Visual-Perceptual Skills for children with shunted hydrocephalus
• Auditory Analysis Test:: Language tests, phonological awareness
• Rapid Automatised Naming Test: Word retrieval tasks
• WRAML: Attention, memory and problem solving
• Tower of London, Wisconsin Card Sorting Test: problem solving
• Sorting Test:
o Stroop Test: Selective attention
o Verbal and nonverbal cancellation tests: Focused attention
• Woodcock-Johnson Psychological Education Test: Academic achievement (basic
reading and passage comprehension)
• WRAT-R: Spelling and Arithmetic
Tactile-perceptual skills were not assessed. Fletcher et al. (1995) acknowledge that
neurologically, sensory function problems are common with spina bifida and children with
hydrocephalus.
Parents: Vineland Adaptive Behaviour Scales were completed during interview.
These scales took 20-30 minutes approximately to complete. Parents also provided history.

318
Results: Tests that assessed phonological awareness, word fluency, verbal fluency and
automaticity under timed conditions scored well below normal children. Language was
better developed but not fully preserved in children with hydrocephalus. The group with
spina bifida and hydrocephalus showed lower performance on the Story Recall subtest of
WRAM with deficits largely on immediate not delayed recall which may reflect language
discourse problems discussed by Dennis, Hendrick, Hoffman and Humphreys (1987).
Problem solving: The major finding was that spina bifida and hydrocephalic children
solved fewer problems correctly that may be relative to attention systems “mediated” by
white matter regions of the brain. The focused attention task showed the largest group
discrepancies. Problems with automaticity in the Stroop Test were possibly due to
interhemispheric difficulties. Children were less likely to solve a problem the first time on
the Tower of London test which may indicate difficulty focusing and orienting to task. They
also achieved fewer categories on the Wisconsin Card Sorting Test (WCST). Children with
hydrocephalus have motor and cognitive characteristics that are consistent with Rourke’s
1989 predictions of the NLD model. As well, children with hydrocephalus were found to
have cerebral abnormalities that clearly involve white matter tracts.

319
The intelligence of hydrocephalic children
(Dennis, Fitz, Netley, Sugar, Harwood-Hash, Hendrick, Hoffman &
Humphreys, 1981)
Purpose: To analyse how the level and pattern of intelligence in hydrocephalic
children is related to various parameters and symptoms of their condition.
Total sample: 78 children 5-15 years. Mean age at IQ testing 8.58 years.
33 children had spina bifida (myelomeningocele or encephalocele) and
shunted hydrocephalus, with shunt inserted before 12 months of age. Children whose scores
on both verbal and performance tests fell below 70 on WISC-R were excluded.
Measures:
• WISC or WISC-R.
Tests were individually administered to each child with scoring performed in strict
accordance with manual with no allowance for any handicap. Four scores were obtained for
each child – VIQ, PIQ, FSIQ. V-P discrepancy was derived from formula (verbal IQ – perf
IQ/x (verbal IQ + perf IQ) (100), when x indicated the mean. This formula allows the IQ
pattern of two children to be directly compared even when scores come from different ends
of IQ distribution. “As a measure of the patterning of intelligence, the V-P discrepancy
score is more interpretable than the arithmetic difference between VIQ and PIQ, a score that
considers the absolute rather than relative difference between VIQ and PIQ” (p.608).
Results: A common outcome of hydrocephalus in the first months of life is uneven
cognitive growth during childhood, with nonverbal intelligence developing less fully than
verbal intelligence. Intelligence was not found to be affected by type or number of shunts,
but seizures, even a single early seizure, was found to impair nonverbal intelligence. The
effects of disturbed visual function common in hydrocephalic children extending from loss
of visual acuity and visually guided behaviour to impaired nonverbal intelligence, was
discussed and a relationship between visual abnormalities and behavioural deficit is yet to be
analysed. The degree of motor problems was not considered critical to the nonverbal skills
deficit found in hydrocephalic children. Dennis et al. (1981) concluded that the origin of
poor development of nonverbal intelligence found in hydrocephalic children is considered
due to neither the hydrocephalic condition itself nor its treatment, but rather to the
“developmental brain anomalies of hydrocephalus and the symptoms to which the
hydrocephalic is prone” (p.607).

320
Cognitive functioning in patients with spina bifida, hydrocephalus and the
“Cocktail Party Syndrome”
(Hurley, Dorman, Bell & D’Avignon, 1990)
Purpose: To determine relationships among spina bifida, hydrocephalus and cocktail
party syndrome (CPS) on cognitive measures of intelligence, reasoning ability, academic,
social achievement and deeper comprehension of language.
Total sample: 50 subjects with spina bifida and hydrocephalus
26 subjects aged 10-32 years had shunted hydrocephalus. Average
mean age 15.88 years.
Measures:
• WAIS-R for subjects over 16 years
• WISC-R for subjects younger than 16 years
• WRAT for all subjects (reading, spelling, arithmetic scores recorded in standard
scores)
Standardised intelligence tests were chosen because (1) WAIS-R or WISC-R was
appropriate to ages, (2) WRAT tests are routinely used clinically due to reliability over time
and good predictive ability and are widely used in research on cognitive functioning and (3)
offer the best comparison with previous and future research results.
To categorise subjects into groups, all subjects were rated on five criteria to judge if the
child showed characteristics of CPS:
• Fluent, well-articulated speech;
• Verbal perseveration;
• Excessive use of social phrases;
• Irrelevant verbosity;
• Over-familiarity of manner.
A 6th criterion was developed and added to gather data about daily performance:
• Activities of Daily Living (ADL) to gather data about daily performance. Each rater
was asked to judge if subject had ability to handle daily responsibilities as would
peers of similar age and developmental level, excluding medical care issues unique
to spina bifida patients.

321
41 subjects agreed to undertake:
• WCST (Wisconsin Card Sorting Test). Chelune and Baer (1986) advise not to use
WCST in 8-12 age range due to immaturity of frontal lobe functions.
• MLT (Metaphoric Language Test).
WCST was given and scored according to percent perseverative errors and number of
categories completed. These scores were considered to be most indicative of brain damage
and level of daily functioning. WCST was chosen because it assesses ability to (1) use
environmental feedback to develop problem solving strategies (2) capacity to shift set and
suppress inappropriate responding and (3) ability to selectively attend to relevant stimulus
dimensions without distraction. Number of shunt revisions was also studied.
According to Burns, Halper and Mogil (1985), the MLT (Metaphoric Language Test) is
sensitive to the discernment of underlying meanings in language and has been used
previously to study patients with right hemisphere lesions observed to have CPS or to
display similar language deficits.
All tests were administered by doctoral level or master’s level psychologist with two or
more years experience in administering the tests. Each subject was judged by two
independent raters on the basis of who knew the subject the best and was acquainted with the
subject for more than two years.
Results: All 50 subjects had significant impairment of cognitive functioning.
Independent raters judged 15 subjects (12 shunted) to have CPS, 25 subjects (4 shunted) to
be normal functioning with “fluent and well-articulated speech” and 10 who met at least 2
CPS criteria (all shunted) considered dysfunctional in many significant areas. The 15 CPS
subjects met four out of five CPS criteria and were characterised as having poor abstract
reasoning skills, poor visual perceptual skills, low IQ and poor academic skills, with no
particular pattern associated with CPS that distinguished them from the low IQ subjects (15
drawn from normal and dysfunctional groups with IQ >82), except poor academic
achievement. Many CPS subjects were mentally retarded and additionally, these subjects
had trouble interpreting the deeper meaning of language as measured by the MLT. Ten
individuals in the Dysfunctional Group were characterised by a large V-P split and poor
ADL skills although not different in overall IQ scores to normal functioning subjects. These
individuals may need verbal cues throughout life with “expectations for independent
functioning” readjusted to “reasonable levels” (p.169).

322
Distractibility and vocabulary deficits in children with spina bifida and
hydrocephalus
(Horn, Lorch, Lorch & Culatta, 1985).
Purpose: To confirm hypothesis of a relationship between distractibility and language
deficits in spina bifida and hydrocephalic children. If distractibility affects language
comprehension of spina bifida and hydrocephalic children, they should perform relatively
poorly on vocabulary items presented with irrelevant information. In the absence of
irrelevant information, they should perform similarly to matched controls.
Total sample: 15 children with spina bifida and hydrocephalus, mean mental age 6.7
years, mean chronological age 7.8 years. Fifteen normal children, mean mental 6.7 years,
mean chronological age 5.9 years. Mental age based on nonverbal intelligence. Each child
had lower spinal lesion and shunt inserted soon after birth. Two tasks, Part 1 and Part 2,
were tested in a single session lasting approximately 45 minutes.
Part 1 Objective was to measure size of interference effect by comparing degree to
which spina bifida and hydrocephalic children and normal controls were distracted from
non-linguistic task by presence of irrelevant material.
Measure:
• A Speeded Classification Task to study development of selective attention (Well,
Lorch and Anderson 1980)
This card-sorting task was chosen because it minimises the role of language, learning
and memory and includes a clear base-line condition for comparison i.e. performance in the
absence of irrelevant information.
Part 2 Objective was to test for comprehension of selected relational words.
Measure:
• Boehm Test of Basic Concepts (Boehm 1971)
This test was chosen because it (1) presents distinctive examples of concepts without
irrelevant information and spina bifida and hydrocephalic children score well on it (2)
permits choice of items varying in difficulty (3) requires an unambiguous response and (4) is
easily adapted for presentation with irrelevant information.

323
Results: Parts 1 and 2 support hypothesis that spina bifida and hydrocephalic children
are more distractible than control children and this greater distractibility is partly responsible
for deficiencies in vocabulary comprehension. The Speeded Classification Test showed
larger and more persistent interference from irrelevant stimuli. Part II vocabulary
comprehension was very similar to normal children in the absence of irrelevant information
but they showed substantial decrements when there was a presence of irrelevant background.
Advice: Be cautious of inflating estimates of child’s language abilities if testing for
vocabulary deficits if presented with minimal irrelevant information. If vocabulary tests
reveal discrepant scores, there may be need for further testing that includes distractibility.

324
Cognitive and achievement status of children with myelomeningocele
(Shaffer, Friedrich, Shurtleff & Wolf, 1985).
Purpose: To accentuate need for comprehensive evaluation of strengths and
weaknesses in this population rather than create a profile typical for individuals with
myelomeningocele with/without shunted hydrocephalus. This would facilitate (1) planning
of programs to remediate weaknesses in young children and (2) in adolescence,
comprehensive evaluation data could be used to enhance effective vocational habilitation.
Total Sample: 60 children with spina bifida aged 6-15 years 8 months
25 children had myelomeningocele and shunted hydrocephalus
35 children had myelomeningocele and unshunted hydrocephalus (either
minimal evidence or no hydrocephalus)
Measures:
• WISC administered to all subjects
• WRAT administered to 43 subjects
Two-way t-test used to assess verbal-performance IQ differences.
Results: For the total sample, VIQ significantly exceeded PIQ. The presence of
myelomeningocele was associated with lowered cognitive abilities and academic
achievement and these findings were mediated by functional motor level.
Myelomeningocele children scored significantly lower than norms on PIQ and FSIQ and 24
or 40% had a difference greater than or equal to 12 points. In 6 cases, PIQ was greater than
VIQ. The mediating influence of motor level was not seen in the 25 individuals with shunts
and this group had significantly lower PIQ and VIQ. Intellectual functioning was found to
range with lesion level, lower lesions associated with higher levels of intelligence. Between
group differences revealed no significant differences between shunted and non-shunted on
FSIQ, VIQ, PIQ, WISC subtests or WRAT scores although Shaffer et al. (1985) report
previous studies finding lower cognitive abilities with a shunt than without.
Advice: A potentially more useful and empirically more relevant method of analysing
WISC scores may be to examine the three WISC factors outlined by Kaufman (1979):
• Verbal Comprehension Abilities (VCA)
• Perceptual Organisation Abilities (POA)
• Freedom From Distractibility (FFD)

325
This sample differed significantly from norms on POA and FFD but not on VCA. Do
not use verbal interaction as informal method of estimating scholastic and vocational
abilities with myelomeningocele and hydrocephalic subjects because it is likely to result in
expectations of a higher level of overall functioning “than could be realised” (p.333). For
example, this group was not different to established norms on Picture Completion,
Similarities and Vocabulary. Similarities and Vocabulary reflect expressive skills and
because myelomeningocele and hydrocephalic children have a relatively high level of verbal
expressive skills with other areas of intellectual functioning below norms, informal
assessment is likely to produce an unreliable and misguided result. Shaffer et al. (1985)
report Willner (1971) as finding WAIS Similarities score often indicates a “facade of
abstraction rather than actual abstraction ability” while Rapaport, Gill and Schafer (1968)
describe the test as a measure of concept formation requiring definitions based on everyday
verbal coherences that can become so over-learned that a good score may not require an
abstractive component. Psychologists be aware that Similarities scores may not reflect
abstract abilities and verbal expression does not reflect overall intelligence in this population.

326
The clinical and psychological characteristics of children with the “Cocktail
Party Syndrome”
(Tew & Laurence, 1979).
Purpose: To determine the level of intelligence and physical disability associated with
Cocktail Party Syndrome.
Sample: 49 subjects with spina bifida, aged 5-16 years
45 had myelomeningocele, 2 with encephalocele, 2 with congenital
hydrocephalus, 30 with shunted hydrocephalus
Measures:
Two examinations were conducted at ages 5 and 10 years. At 5 years:
• Wechsler administered to assess VIQ, PIQ, FSIQ
• Reynell Language Scale to assess expressive language and verbal comprehension
were used
Between ages 5 and 10 years, three children with CPS and two with meaningful
conversation died. Re-assessment at 10 years of IQ, Attainments, Perceptual-motor skills,
Personality, School Adjustment.
Five criteria were used to judge if child showed characteristics of CPS:
• Fluent, well-articulated speech;
• Verbal perseveration;
• Excessive use of social phrases;
• Irrelevant verbosity;
• Over-familiarity of manner.
Results: Findings revealed that CPS was closely associated with subnormal intelligence.
Tew and Laurence report Khan and Soare (1975) as finding that CPS appears to “decay with
time”, which obviously makes age distribution relevant. CPS seems to accompany severe
multiple physical disability and tended to be present in shunted cases where hydrocephalus
was rated as having a severe onset. Possible cause of CPS: They cite Brocklehurst (1976)
and Start (1977) as suggesting disruption of association fibres at cerebral cortex (layer of
neurons and grey matter on the surface of cerebral hemisphere), while Hagberg and Sjorgen
(1966) tentatively suggest “a special frontal lobe” syndrome as the cause (p.198).

327
Neuropsychological and adaptive functioning in younger versus older children
shunted for early hydrocephalus
(Holler, Fennell, Crosson, Boggs, Mickle & Parker, 1995).
Purpose: To describe psychological functioning in children with early onset
hydrocephalus and spina bifida and describe differences in neuropsychological and adaptive
functioning of younger and older children.
Total sample: 28 children with spina bifida and shunted hydrocephalus aged 5-12½
years
14 Young: 5-7 years
14 Old: 9-12 ½ years
Measures:
• Abbreviated WPPSI-R, Wechsler,1989, or WISC (111 Edition) Wechsler, 1991
using Object Assembly, Block Design, Vocabulary, Information
• VMI (Berry 1989) - Visuomotor skills
• Buschke-Morgan Selective Reminding Test (Morgan 1982) or Buschke-Levin
Selective Reminding Test (CLTR) (Levin 1989)
• Controlled Oral Word Association (Benton and Hamsher, 1989) (Fluency, verbal
intentional/organisational abilities)
• Naming as many “foods” or “animals” in line (Halperin, Zeitchik, Healy, Weinstein
and Ludman, 1989)
• Repetitive Finger Taps - fine motor speed
• Successive Finger Taps
Parents: Vineland Adaptive Behaviour Scales (Sparrow, Balla and Circhetti, 1984) to
assess competency in socialisation, communication, motor and daily living skills. Answers
range from “yes” to “I don’t know”.
Procedures: Researcher and trained assistant collected history, demographic and medical
information at parental interview. Second examiner tested each child individually during
one session lasting approximately 2 hours. To reduce examiner bias, detailed information
from medical records and parent reports were not shared until after children were tested and
scores recorded.

328
Results: V-P split was observed in this sample with intelligence scores comparable
between both age groups. Neuropsychological functioning for total sample was impaired
compared to age-based norms. Pattern of neuropsychological functioning was quite stable in
both age groups but the level of neuropsychological and adaptive functioning was more
difficult for older than younger children. More shunt revisions correlated with lower PIQ,
and lower spinal lesions with higher IQ. Lower spinal lesions were related to better daily
living and communication skills and fewer learning problems. Later shunt age was
associated with worse socialisation scores indicating that shunting before the age of one
week may be related to improved social skills and higher incidence of hyperactive
behaviours. Results indicated that children with shunted spina bifida and hydrocephalus may
be conceptualised as exhibiting a nonverbal learning disability.

329
Syndrome of Nonverbal Learning disabilities: Age difference in
personality/behavioural functioning
(Rourke & Casey, 1989)
Purpose: To determine age-related changes in the presentation of NLD in the 7-15 year
age range. Rourke and Casey hypothesised (a) WISC VIQ and PPVT IQ would not differ
between older and younger children (b) PIQ for younger children would exceed that of older
children and (c) difference between WISC VIQ and PIQ (favouring VIQ) would be larger for
older than younger children.
Total sample: 29 subjects referred for assessment due to learning disability (LD) for
which brain impairment was thought to be contributing factor. Two had well-documented
brain lesions.
Young 7-8 years
Old 9-15 years
All subjects were selected in accordance with neuropsychological, academic and
socioemotional criteria of the NLD syndrome.
Measures:
• WISC (Wechsler, 1949) – VIQ, PIQ and 11 subtests
• WRAT (Jastak and Jastak, 1965) – Reading, spelling, arithmetic
• PPVT (Dunn, 1965) – IQ
• Reitan and Davison, 1974 – Finger tapping and Name Writing Speed
• Klove-Matthews Motor Steadiness Battery (Klove, 1963) – Pegboard Tests
• Underlining Test (Rourke and Gates, 1980) – 1 control and 13 critical subtests
• PIC (Wirt et al., 1977) – validity, adjustment, academic achievement, intellectual
screen and 8 clinical scales
Procedure: All tests were administered in a standardised manner by extensively trained
technicians in the field of neuropsychological assessment.
Results: All results coincided with hypothesis expectations. The VIQs for younger and
older subjects were almost identical. PIQ for older subjects was lower than for younger
subjects and VIQ-PIQ discrepancies were greater for older than younger subjects. Four
WISC verbal subtest scaled scores were higher and two lower for older versus younger
subjects. All WISC performance subtest scaled scores were lower for older than for younger
subjects.

330
APPENDIX C
Background to verbal-performance discrepancies in individuals with
hydrocephalus related to spina bifida
Early gestational anomalies from a defect in the neural tube closure causing spina bifida
indicate a “prolonged rather than brief disruption” in the developing embryo (Fletcher et al.,
1992, p.595). Severity of hydrocephalus may also be related to discrepancies in skill
development due to damaged or destroyed right hemisphere white matter or limited access to
its functions (Fletcher et al., 1992). A common outcome of early hydrocephalus is uneven
development of different areas of cognitive development during childhood with nonverbal
intelligence developing less fully than verbal intelligence which is often confusing for
teachers (Dunning, 1992). A split in verbal-performance abilities with a tendency for verbal
abilities to be significantly higher than nonverbal abilities was a recognised research finding
(Badell-Ribera, Shulman & Paddock, 1966; Dennis et al., 1981; Wills et al., 1993; Fletcher
et al., 1995) until more recent literature shed new light.
A study by Pelletier et al. (2001) to revise criteria for selecting children 9 – 15 years
with NLD or a language disorder found that, for those classified with NLD, a V-P
discrepancy of at least 10 points was evident only 27.3% of the time. If this criterion was
used in isolation from other criteria for selecting persons with NLD, “it would be likely to
miss 72.7% of the Definite and Probable NLD population in the 9 – 15 age range”. “It
would appear that dropping a V-P discrepancy of at least 10 points as a criterion would, in
all likelihood, have no appreciable effect on ‘diagnostic’ accuracy” ( p.95). Twelve children
who met the criteria for Definite or Probable classification for both a language disorder and
NLD had a VIP < PIQ by at least 10 points (p.89). Roman (1998) also found some children
with an NLD “demonstrate other cognitive deficits, including severe language disorders”
which does not necessarily rule out NLD diagnosis but it must be “carefully demonstrated
that the pattern is not simply one of global cognitive dysfunction” (p.16).
Students with spina bifida and hydrocephalus usually have a number of disabilities that
affect performance on standardised test measures (Rowley-Kelly & Reigel, 1993). Strong
auditory perceptual skills and difficulties in the areas of fine motor, visual-motor, visual-
spatial perception and problem solving are characteristics consistently reported to contribute
to a discrepancy between verbal and performance abilities in individuals with hydrocephalus
and spina bifida. Hydrocephalus has major influences on cognitive, motor, visual and social

331
development with management of the hydrocephalic condition being the major determinant
of how well mental and social abilities develop (Fletcher & Levin, 1988). Tactile,
perceptual, visual-spatial and psychomotor deficits assumed present from their earliest
developmental stages are predicted to substantially alter the normal course of sensory and
motor skill development which contributes to impairment of cognitive skills (Rourke, 1989).
As well as cognitive, motor, visual and social developmental problems caused by
abnormal brain development in the child with hydrocephalus, seizures further reduce the
chance that nonverbal intelligence will develop normally. For children who have shunt
complications, McLone et al. (1982) found that the “onset of seizures correlates well with a
negative ultimate outcome for intellectual development” (p.342). Seizures damage both
overall and relative levels of nonverbal intelligence particularly when seizure focus involves
the right hemisphere (Dennis et al., 1981). Nonverbal intelligence therefore may be “more
vulnerable than verbal intelligence, even to a single early seizure” (p.614). The incidence of
seizures in spina bifida students is approximately 40% and according to Hurley (1993),
active seizures and anti-seizure medications alter concentration and active performance
levels. Physical symptoms of early onset hydrocephalus such as abnormal eye movement
and poor fine motor coordination are associated with poorer nonverbal performance on tasks
involving visual and tactile perception and psychomotor tasks which may link symptoms of
hydrocephalus to a nonverbal deficit.
Verbal-performance discrepancies in previous studies
Fletcher et al.’s (1992) study into discrepancies between verbal and nonverbal skills
demonstrated that “hydrocephalus per se is associated with discrepancies in verbal and
nonverbal cognitive skills with nonverbal skills being lower” (p.604). Wills et al. (1990)
compared small and large verbal-performance IQ differences in myelomeningocele children
with the general population. Of a total sample of 89 children aged 4-14 years, clinically
important discrepancies of 12 points or more (Kaufman, 1979) occurred more than twice as
often among myelomeningocele children as in the general population. Almost all
discrepancies were due to marked deficits in PIQ relative to VIQ. The sample scored lower
on almost all tests administered with PIQ subtests, Visual-Motor Integration (VMI) and
arithmetic calculation presenting particular difficulty. Deficits on these tests were found to
increase with age while tests of reading and spelling improved “at the same rate as in the
general population” (Wills et al., 1990, p.172). Whenever interpretation of V-P intelligence
discrepancies is necessary, Kaufman (1979) believes any difference of 11 or more points
should be treated as statistically important.
332
The cognitive and achievement status of children with myelomeningocele was also
studied by Shaffer et al. (1985) with a total sample of 60 children aged 6-15 years of whom
25 were shunted. Within the shunted group, 40% (vs. 5% of the general population) had a
V-P difference of 12 points or more while in 6 shunted cases, PIQ exceeded VIQ. Relative
verbal strengths compared to weaker cognitive skills such as visual memory, speed, acquired
knowledge, integrated functioning and coordination cause the expectations of professionals
to vary widely and this should be considered in education and vocational settings. With
respect to future prognosis, Tew (1978) reports that since one third of the spina bifida and
hydrocephalic population had deficits in speed and manipulative skills, they were “unlikely
to obtain competitive employment and should perhaps be educated to occupy their leisure
time fully” (p.240).
Fletcher and Levin’s (1988) review on the neuropsychological and behavioural
characteristics of children with hydrocephalus reveal characteristics consistent with Rourke’s
(1989) description of the NLD syndrome. Test scores revealed from Dennis et al. (1981) and
Fletcher et al. (1992) show lower performance-based measures than verbal-based measures.
Fletcher et al. (1995) recruited 189 subjects aged 5-14 years to address neurobehavioral
characteristics of hydrocephalus in relation to the NLD syndrome. Forty individuals had
shunted hydrocephalus and spina bifida. Hydrocephalus was found to be clearly associated
with lower performance than verbal-based tests, consistent with hydrocephalus-related
changes in ventricles and white matter tracts described in Rourke’s (1989) NLD model.
Rourke (1989) studied age-related changes in children who fitted the NLD criteria in
two groups aged 7-8 years and 9-15 years. He found V-P discrepancies were greater for
older than younger subjects, VIQ was almost identical for both groups and PIQ for older
subjects was lower than for younger subjects. Holler et al. (1995) studied the
neuropsychological and adaptive functioning in younger (5-7 years) versus older children (9-
12 ½ years) with shunted hydrocephalus and spina bifida. A V-P split was observed in the
total sample with intelligence scores comparable between age groups. Verbal IQ was in the
average range and PIQ in the borderline range, although exploring V-P differences was not a
focus of this study. Neuropsychological functioning for the total sample was impaired
compared to age-based norms. As well, adaptive functioning was more difficult for older
than younger children. Findings appeared to uphold that dynamics and neuropsychological
characteristics of an NLD proposed by Rourke (1989) were present in this sample of children
with hydrocephalus and spina bifida.

333
Studies reviewed have recruited children in the 5-16 year age-range. Dennis et al.
(1981) found that in children with treated and controlled hydrocephalus, intelligence remains
constant in this age-range and Tew and Laurence (1984) report IQ scores have an extremely
high level of reliability between the ages of 5 and 16. Wills et al.’s (1993) review of
neuropsychological functioning in children with spina bifida and hydrocephalus observed
that within the school years, IQ test scores of spina bifida children tended to be quite stable
and relative ranking remained consistent where “high-scoring” children continued to score
highly (p.254).
A child with white matter dysfunction may display a range of behaviours and abilities
evidenced by dependence on left hemisphere verbal and reading skills and difficulty with
tasks subserved by right hemisphere functions (Thompson, 1997). Impressive and relatively
well-structured speech and language have traditionally been considered a strength for
persons with spina bifida and hydrocephalus (Tew & Laurence, 1979) but they have
potential to cause confusion and frustration for those working with these individuals. Fluent
language is quite often impoverished in content. Approximately 30% of spina bifida and
hydrocephalic children exhibit hyperverbal speech, often referred to as Cocktail Party
Syndrome (CPS) (Culatta, 1993; Horn, Lorch, Lorch & Culatta, 1985; Hurley et al., 1990;
Rourke, 1987; Tew & Laurence, 1979).

334
APPENDIX D
Definitions
Nonverbal Learning Disability (NLD)
Rourke et al. (2002) define a Nonverbal Learning Disability as follows:
The NLD syndrome is a specific pattern of neuropsychological assets and deficits that
eventuates in the following: a specific pattern of relative assets and deficits in academic
(well developed single-word reading and spelling relative to mechanical arithmetic) and
social (e.g., more efficient use of verbal than nonverbal information in social situations)
learning; specific, developmentally dependent pattern of psychosocial functioning.
Typically, in children below the age of four years, psychosocial functioning is relatively
normal or reflective of mild deficits. Following this period, emerging manifestations of
externalized psychopathology are frequent; the child may be characterised as
“hyperactive” and “inattentive” during this period. The usual course with respect to
activity level is one of perceived “hyperactivity” through evident normoactivity to
hypoactivity with advancing years. By older childhood and early adolescence, the
typical pattern of psychopathology in evidence is of the internalised variety,
characterised by withdrawal, anxiety, depression, atypical behaviours, and social skill
deficits (p.153).
Executive Function (EF)
Baron (2004) defines Executive Function disorder as follows:
The metacognitive capacity that allows an individual to perceive stimuli from his or her
environment, respond adaptively, flexibly change direction, anticipate future goals,
consider consequences and respond in an integrated or common-sense way, utilising all
these capacities to serve a common purposive goal.
Executive function subdomains include: set shifting, hypothesis generation, problem
solving, concept formation, abstract reasoning, planning and organisation, goal setting,
fluency, estimation, common sense, working memory, inhibition, self-monitoring,
initiative, self-control, mental flexibility, attentional control, anticipation, behavioural
regulation, creativity (p.134).

335
Mild Intellectual Impairment (II)
The American Psychiatric Association (2004) defines a Mild Intellectual Impairment and
Borderline Intellectual Impairment as follows:
As a group, people with this level of intellectual impairment typically develop social
and communication skills during the preschool years (ages 0-5 years), have minimal
impairment in sensorimotor areas and often are not distinguishable from children
without Mild Intellectual Impairment until a later age. By their late teens, they can
acquire academic skills up to approximately the sixth-grade level. During their adult
years, they usually achieve social and vocational skills adequate for minimum self-
support, but may need supervision, guidance and assistance, especially when under
unusual social or economic stress. With appropriate supports, individuals with Mild
Intellectual Impairment can usually live successfully in the community, either
independently or in supervised settings (p.43).
Borderline Intellectual Functioning
This category can be used when the focus of clinical attention is associated with
borderline intellectual functioning, that is, an IQ in the 71-84 range. Differential
diagnosis between Borderline Intellectual Functioning and Intellectual Impairment (an
IQ of 70 or below) is especially difficult when the coexistence of certain mental
disorders is involved (p.740).

336
APPENDIX E
Glossary
abstract thinking: The ability to think in terms of ideas or concepts rather than facts.
aetiology: The source or origin of a syndrome or disease.
Anencephaly: A severe birth defect involving congenital absence of major portions of the
brain and malformation of the brain stem. The cranium does not close and the vertebral canal
remains a groove. Anencephaly is not compatible with life.
Asperger’s syndrome: A developmental disability characterised by normal intelligence,
motor clumsiness, eccentric interests and a limited ability to appreciate social nuances.
Attention deficit disorder (ADD): A neurologically based condition that is characterised by
distractibility, short attention span, and impulsiveness.
Autism: A developmental disability, with onset in infancy or early childhood, characterised
by severe deficits in social responsiveness and interpersonal relationships, abnormal speech
and language development, and repetitive or stereotyped behaviours.
axon: Part of the nerve cell that carries outgoing messages from the cell body to other cells.
brain: The part of the central nervous system inside the skull. Its functions include muscle
control and coordination, sensory reception and integration, speech production, memory
storage and the elaboration of thought and emotion.
brain plasticity: Theories based on the idea that the brain may have the ability to use
surviving brain cells in a different way to make up for those brain cells that are damaged.
brain stem: The portion of the brain that connects the brain with the spinal cord.
central nervous system: The brain and spinal cord.
cerebellum: The portion of the brain mainly responsible for balance and coordination.
cerebral cortex: The surface or outer layer of the brain or, the layer of tissue on the outer
surface of the cerebrum, commonly called grey matter.
cerebral hemisphere: One side of the cerebrum, which is the largest part of the brain. For
most people, the left cerebral hemisphere deals with language and the right side with spatial
relations.
cognition: Thinking skills such as knowing, awareness, perceiving objects, remembering
ideas, understanding and reasoning.
coordination: The harmonious working together of muscle groups in performing complex
movements.

337
corpus callosum: A thick band of nerve fibres that connects the two hemispheres of the
brain.
cranium: The portion of the skull that houses the brain.
crystallised intelligence: Storehouse of general information/knowledge; over-learned
skills; rote “old” learning; information based on past learning.
deficit: A deficiency relating to a lack of skill or ability
dendrite: A branch of a nerve cell that receives incoming messages from other nerve cells.
development: The interaction between maturational processes and environmental
influences.
developmental disability: Severe or chronic disability attributable to mental, social
and/or physical impairment manifested before the person attains age 22.
discrimination: The ability to differentiate between two or more sensory stimuli.
dysgraphia: A disability in the physical act of printing or cursive handwriting.
dyslexia: A developmental reading disability, which may vary in degree from mild to
severe. Children born to parents with dyslexia may be eight times as likely to have the
condition.
embryonic stage: Stage of prenatal development from time of implantation of fertilized
ovum about 2 weeks after conception until the end of the 7th or 8th week.
executive functions: Refer to higher-order cognitive processes such as initiation, planning,
hypothesis generation, cognitive flexibility, decision making, regulation, judgment, feedback
utilisation and self-perception.
eye-hand coordination: The integration of visual and tactile systems that enables the
hand to be used as a tool of the visual processes.
foetal stage: The interval from the end of the embryonic state (at the end of the 7th or 8th
week of gestation), to birth.
fine motor: The use of small muscle groups for specific tasks such as handwriting.
fine-motor skills: Enable arm/hand movements and ability to reach, grasp, manipulate and
release objects in a coordinated manner.
fluid intelligence: Practical, hands-on intelligence; how well a person “thinks on his or her
feet”; how quickly and competently a person processes and utilises the information at his or
her disposal.
frontal cortex: The portion of the brain that's involved with reasoning, planning, abstract
thought and other complex cognitive functions in addition to motor function.
338
frontal lobe: The largest portion of the cerebral cortex that lies in the front of the brain and
is important for cognitive functions and control of voluntary movement or activity.
frontal cortex: The portion of the brain that's involved with reasoning, planning, abstract
thought and other complex cognitive functions in addition to motor function.
frontal lobe: The largest portion of the cerebral cortex that lies in the front of the brain and
is important for cognitive functions and control of voluntary movement or activity.
gestalt perception: Deriving meaning from the “whole picture”, without breaking it down
into parts; “putting it all together”; a holistic view.
grey matter: Short non-myelinated nerve fibres. Those regions of the brain and spinal
cord where neuronal cell bodies and dendrites are abundant.
hemisphere: Half of the cerebral cortex. The two cortical hemispheres are each subdivided
into four lobes.
horizontal nystagmus: Spasmodic movement of the eyeballs in a left-right direction.
hydrocephalus: A condition in which excess cerebrospinal fluid accumulates in the brain,
often treated with the surgical placement of a shunt system to divert the fluid from the brain
to another part of the body.
impairment: A neurological blockage or barrier to expected development.
inference: Going beyond available evidence to form a conclusion.
intervention: The therapeutic and/or educational methods employed to aid a child once a
disability has been diagnosed.
IQ: The abbreviation for “intelligence quotient”, which is a person’s purported mental
capacity.
left hemisphere: The area of the brain which is specialised for processing verbal or
language-based information. This includes the rote memory, linguistic, symbolic, linear, and
analytical functions of an individual.
lipids: Organic compounds that are insoluble in water.
lumbar area: The lower part of the back between the hip bones.
meninges: The membranes that cover the spinal cord and brain.
midline: The imaginary line from the tip of the head to the feet, which separates the body
into halves.
myelin: A white, fat-like substance that forms a sheath around nerve fibres.
myelodysplasia: This term is used to describe defective development of any part of the
spinal cord

339
nerve: A bundle of fibres that connects the brain and spinal cord with various parts of the
body and through which impulses pass.
neural tube: A structure in early foetal life that develops into the brain, spinal cord, spinal
nerves and spine.
neural tube defect: A birth defect resulting in improper development of the brain or spinal
cord.
neuron: Cells in the brain involved in the reception, integration, and transmission of
signals. Neurons have specialised extensions called dendrites and axons. Dendrites bring
information to the cell body and axons take information away from the cell body.
neurosurgeon: A surgical doctor who specialises in operations which involve the nervous
system.
Nonverbal Learning Disorder (NLD): A neurological condition believed to result from
damage to the white matter connections in the right-hemisphere, which is important for
intermodal integration. Three major categories of dysfunction present themselves:
1. Motoric (lack of coordination, severe balance problems, and difficulties with fine
graphomotor skills.
2. Visual-spatial-organisational (lack of image, poor visual recall, faulty spatial
perceptions, and difficulties with spatial relations).
3. Social (lack of ability to comprehend nonverbal communication, difficulties
adjusting to transitions and novel situations, and deficits in social judgment and
social interaction).
occipital: Pertaining to the back of the head.
occipital lobe: An area at the back of the brain that receives and processes visual
information.
organisational skills: Facilitate ability to follow and execute verbal directions of more
than one step. A deficit in this area combined with poor time concept will likely impede task
completion within a time limit.
parietal lobe: An area of the brain that lies in front of the occipital lobe. Important in
processing information from the sense of touch and bringing together sensory information.
pathognomonic signs: Characteristics of a particular disease.
perception: The mental interpretation of sensations received from stimuli.
perceptual-motor: The functioning of the perceptual and motor processes together.
perseveration: The continued repetition of words or motions after the point where they no
longer serve a useful purpose.

340
pragmatics: The relationship between signs or linguistic expressions and their users; the
functional use of language.
prosody: The variations of emphasis and intonation in speech.
psychomotor: Pertaining to voluntary physical movement.
right hemisphere: The area of the brain which is specialised for processing nonverbal or
performance-based information. This includes the visual-spatial, intuitive, organisational,
evaluative, and gestalt (holistic) processing functions of an individual.
sacral area: The area of the spine which lies between the buttocks and below the small of
the back.
seizure: A sudden attack, often including convulsions. If recurrent, often referred to as a
seizure disorder or epilepsy.
spatial perception: Aids understanding of in/out, under/over, right/left concepts, the
ability to judge distances or directions.
spina bifida: A birth defect in the spinal column through which the spinal cord may
protrude.
spinal canal: The channel in the spinal column that contains the spinal cord.
spinal column: The bony assemblage of vertebrae; spine.
spinal cord: A lengthy, cord-like bundle of nerves that links nerves in the trunk and
extremities with the brain.
strabismus: A visual defect caused by a muscle imbalance that causes the two eyes to be
directed to different points when looking at an object in space. The eyes may turn inward or
outward.
syndrome: A set of symptoms occurring together.
tactile: Having to do with touch.
tactile perception: How an individual interprets the things he/she feels or touches.
temporal lobes: Areas located on each side of the brain that are important in processing
memory.
thoracic area: Chest area.
tract: Neuronal axons that group together to form a pathway.
ventricles: The fluid-filled cavities within the brain. Also, the two main pumping chambers
of the heart.
vertebra: Any one of the 33 bones that make up the spine.
vesicle: A small sac containing liquid.
visual-motor: The relationship between visual input and motoric output, as in copying text.

341
visual-motor skills: Facilitate eye-hand coordination and efficiency to visually direct,
reach, grasp and use manipulating movements (Williamson, 1987).
visual discrimination: Visual adeptness at perceiving likenesses and differences in
geometrical figures, symbols, pictures, and words.
visual-motor integration: The coordination of visual information with motor processes.
visual perception: Visual-perception skills facilitate ability to recognise what is seen,
discern salient features and integrate with existing information.
visual-spatial: The spatial relationships of the things one sees.
voluntary: Movement or action done in accordance with will.
white matter: Long myelinated nerve fibres in the brain.

342
APPENDIX F
Students with NLD and inclusive education
Background
Equal opportunity and anti-discrimination legislation makes it illegal to discriminate
against individuals on characteristics such as impairment, age, sex, race, marital and parental
status or religious beliefs (Delahaye, 2000). In terms of education, this means that design
and implementation of learning experiences “must be free of individual or systematic bias
that could directly or inadvertently discriminate against a person or group” (p.65).
Legislation of the Human Rights and Equal Opportunity Commission Act of 1986 and the
Disability Discrimination Act of 1992 boosted a move that began in the 1970s to include
children with special learning needs in regular classes. Full-time placement of children with
mild, moderate or severe disabilities in regular classes is now termed “inclusion”
(Westwood, 1997, p.2), the underpinning values of belonging, caring and community
considered relevant to the needs of all children (Staub & Peck, 1995). This focus on
inclusive education drew attention to the predicament of children with special learning needs
“as an oppressed minority group within a larger group” (Lloyd-Smith & Tarr, 2000, p.68).
Inclusive education is an emotionally-laden issue in education and a complex and
perplexing matter for educators. It is one that raises convincing arguments for and against
when addressed by the parents of a child with a disability. While some educators advocate
that placement in a general classroom is not necessarily the least restrictive learning
environment for all students regardless of disability (Putman, Spiegel & Bruininks, 1995),
others promote a full range of placement options that include special classes and retention of
special schools to allow choice of the most appropriate and responsible educational setting
for the student with a disability (Vaughn & Schumm, 1995). Although the least restrictive
environment is defined as a setting that is most like the norm which still meets the student’s
special educational needs (Vaughn & Schumm, 1995), evidence from empirical studies on
the effects of full inclusion, particularly for students with high-incidence disabilities and
their families, suggests these students do not fare well academically in the general education
classroom (Fuchs, Fuchs & Fernstrom, 1993).
In keeping with the Equal Opportunity and Disability Discrimination Acts, all
definitions of inclusion focus on the rights of students with disabilities to be educated in

343
regular schools (Westwood, 1997). Placement of children with intellectual, physical and
sensory disabilities and those with emotional or behavioural problems in regular classes
assumes this to be a relevant option for all children. However, inclusion in a regular class
does not preclude “pull-out services” or individualized instruction for the student with
special learning needs in a self-contained setting when necessary (Staub & Peck, 1995, p.36).
Inclusive practice presents practical and implementation changes in terms of class
organisation and subject matter for the teacher in order to cater for a much wider range of
ability and disability (Westwood, 1997). In terms of school practices, development of a
whole-school policy that supports inclusion, positive attitudes towards students with
disabilities, a competent and collaborative support network among staff, links to outside
services and support and adequate resource materials constitute a basic framework
(Giangreco, 1996). By becoming “informed consumers of support services”, teachers can
become better advocates for their students and themselves (p.59). In terms of teacher
preparedness to handle a diverse range of needs presented by students with disabilities,
exposure to a range of disability characteristics, a range of intervention strategies,
sufficiently trained support staff, in-service teacher and teacher-aide training and close
liaison with parents articulate some of the complementary training needed to equip teachers.
Benefits of inclusive schooling for all students
Inclusive schooling and a well-developed inclusion program argue well for the student
with NLD as well as other mainstreamed students (Thompson, 1997) because:
1. Inclusive education helps create a society in which individual similarities,
differences, diversity, individuality and caring are “better tolerated, accepted and
accommodated” and fear of human difference is accompanied by increased
comfort and awareness (Staub & Peck, 1995, p.74).
2. Programs designed to integrate students with and without disabilities provide
opportunities to shape attitudes towards difference by developing understanding
and acceptance by peers.
3. After helping students with disabilities, non-disabled students have previously
found unexpected strength of character in themselves as they “overcame the fear
of disabilities”, developed more positive feelings about themselves in the
knowledge that they had helped someone and have become more committed to
moral and ethical values (Murray-Seegert, 1989, p.86).
4. Warm and caring friendships that progress beyond school may develop into long-
term friendships.

344
5. Positive attitudes and acceptance by peers can minimise the impact of negative
school experiences on emotional status post-school.
An ecological approach
Since the child with a disability is the receiver and consumer of whatever inclusive
practice is implemented at school, a close working relationship between teacher and parent is
imperative. There can be problems affecting the student with a disability which may be
hidden from school staff but known to family which, if not addressed can easily lead to
educational failure, loneliness and isolation for the student rather than educational
achievement and inclusion. When communities fail to invest in educational care, they are
likely to incur far more draining of their resources as they pay for the later-life damage
caused by their neglect” says Levine (1994, p.277). Examination of factors such as peer
interaction, interpersonal dynamics within the class or social group, teacher expectations,
relevance of class work and homework set, classroom environment and rapport with the
teacher defines an ecological perspective towards identifying and addressing a learning
problem (Hallahan & Kauffman, 1994).
When advocating for additional help for a student, an ecological approach considers
that a number of interacting factors may constitute a learning problem and all merit attention
and consideration. For a child who exhibits clearly articulated speech, good vocabulary and
might show no sign of a disability but experiences more serious academic, functional and
social problems with age, open communication between teacher and parent allow
observations and concerns that may indicate an NLD to be expressed. Shared parent-teacher
observations and understandings encourage mutual discourse, supports an ecological
approach towards identification of learning needs and collective embrace of a culture of care.
For a child with NLD, an inclusive education program should involve the core group of
people directly involved with the child - the parents, classroom teacher/s, teacher aide and
special education teachers, whom Rourke (1995) calls the child’s principal caregivers. An
Individual Education Plan (IEP) “provides key information to assist educators in meeting a
student’s individual educational needs resulting from a disability”. The planning process
brings parents, professionals and sometimes the student together to consider the student’s
present level of performance and “determine needs and learning priorities for the next six
months”. This procedure encourages shared responsibility for decision making and
programming, agreement about educational goals for the student, shared accountability for
outcomes and a forum for communication (Education Queensland, 2006). Developing an
inclusion plan that addresses the educational and social integration needs of a student with

345
NLD requires regular and special education personnel to plan together and communicate
openly with parents (Thompson, 1997).
Strategies for a student with an NLD
If teachers are prepared to implement appropriate strategies to accommodate the unique
learning needs of the student with NLD, there is no sound reason why the majority of
students cannot be placed in regular classes (Thompson, 1997). Effective teaching
intervention strategies for the student with an NLD need to be differentiated from those used
for other learning disability subtypes. They need to be slow and proceed in a step-by-step
logical and repetitive manner at a level geared to the child’s information processing capacity.
The main impediment to engaging in this “painstaking” approach, says Rourke (1995), is the
“caregivers (faulty) impression that the child is much more adept and adaptable than is
actually the case” (p.499). Rourke et al. (1986) report that educators particularly were
convinced that students with “well-developed language” and an excellent vocabulary were
not often considered “at risk” for educational or socio-emotional difficulties during early and
mid-childhood (p.252). Even after neuropsychological assessment was completed, Rourke et
al. (1986) report some professionals and parents “held quite fervently to the notion that the
child in question was simply immature” and he or she only required more educational and
social experience (p.252).
The following broad guidelines are compatible with an ecological approach towards
identifying the student’s learning needs and are designed to ease inclusion of a student with
an NLD into a regular classroom. They involve the student’s principal caregivers, parents,
teachers, teacher aides and therapists and focus primarily on development of life skills. “A
child’s mastery of the academic curriculum is insignificant if the individual cannot cope with
the social and adaptive demands of independent living”, says Rourke (1995, p.507).
1. Use direct observation in new or complex situations to observe what the student
does as opposed to what he or she says. Observations will help teacher or parent
to appreciate the child’s potential inability to adapt to changing circumstances thus
indicating a need for systematic, structured, step-by-step interventions (Rourke,
1995).
2. Reduce the number of adults assigned to work with the student with an NLD. The
student with an NLD will have difficulty adapting to multiple classrooms and
adjusting to diverse staff whose styles and philosophies and expectations differ. In
high school context where this may be unavoidable, communication and

346
collaboration between parents and teachers are principal determinants of a
successful intervention program.
3. Maximise verbal strengths to bypass areas of incompetency. Skills developed
through the student’s auditory channels, strong reading verbal and rote memory
skills, must be capitalised on to acquire compensatory and develop daily living
skills (Thompson, 1997). Oral presentation, practice and review of new
information and instructions are of great benefit to a student with NLD. Steps
must be presented in the correct sequence, explicitly stated and accompanied by
logical explanation to compensate for inability to “read between the lines”. One-
on-one or small group discussion that provides opportunity to ask questions to
clarify meaning addresses problems with identifying underlying meanings and
making inferences. Students with NLD are part-to-whole learners therefore each
step must be clearly defined before a whole concept is grasped (Stewart, 2002).
Any new task or situation will induce repeated questioning to gather information
though in a social context where nonverbal behaviours are used to provide
feedback and direction, constant talking and questioning may be quite
inappropriate (Rourke, 1995).
4. Monitor the student’s organisational skills. A diary that records daily homework
and reminders of due dates should be kept as an aid to planning, organisation and
time management. Thompson (1997) suggests the teacher assume responsibility
for updating the diary, not the student with an NLD. Slowness transitioning from
one task to another, following directions, copying from the blackboard and tedious
handwriting may render the diary task futile. A peer or buddy may check that a
full complement of daily take-home workbooks is complete. Alternatively, a
second set of books at home will eliminate the problem of forgotten books.
5. Assignment writing. The child with NLD has rigid thinking due to impaired
executive function skills that control planning and organisation (Stewart, 2002).
To reduce rigidity and increase flexibility, they survive by relying on practiced
behaviours and clearly-defined rules. Assignment writing may be described as a
written work in 3 sections:
a. Introduction;
b. Explanatory section: each paragraph should have five sentences: an
opening sentence, three supporting sentences and a concluding
sentence;
c. Conclusion that brings together the main points from the explanatory
paragraphs (Thompson, 1997).

347
As a model before commencing an assignment, students may be shown the
finished product. Another accommodation which exploits strong verbal, rote
memory and clear articulation skills and eliminates the handwriting task is to
allow an oral presentation of an assignment.
6. Maintaining attention and concentration. Interacting factors influence the
learning issues faced by the student with an NLD. Slower processing of
information that is primarily presented through the visual modality causes loss of
attention and subsequent distractibility affects task completion (Stewart, 2002).
Attention, concentration and processing speed in turn affect general organisational
skills. As a general rule, the student with an NLD should be:
a. seated at the front of the classroom with minimal distractions, clutter
and noise;
b. given a workspace that is clean and tidy and away from visual and
auditory stimulus (Stewart, 2002);
c. allowed to use headphones to help focus during work time and
diminish distraction;
d. in a class where the teacher student ratio for core academic subjects is
no more than 12:1 (Stewart, 2002);
e. placed in a classroom where schedules are clean, consistent and
predictable;
f. given access to a computer to limit handwriting tasks;
g. given copies of overhead transparencies.
7. Monitor and adjust assignments on a daily basis. Slow mental processing,
deficient planning and organisational skills, difficulty “shifting set” to transition
from one task to another and a poor concept of time dictate that a student with
NLD work on one assignment at a time until completed. This will reduce anxiety
and confusion. To experience success and closure, teacher willingness to adjust
expectations and provide enough support to help plan the assignment framework,
conducting data searches, navigating the library, locating library books on shelves
and using a photocopier should be provided. These “taken-for-granted” skills may
not have yet been achieved by a high school student with an NLD.
8. Grading system should not discriminate against the student with an NLD.
Quantitative assessment based merely on the number of assignments completed
will greatly disadvantage the student with visual-spatial-planning and
organisational deficits who may in fact be working much harder than classmates to
produce much less (Thompson, 1997). To experience some measure of success,
alternative means of assessment that engage strengths need to be employed.

348
9. Teach appropriate strategies for dealing with troublesome situations that
frequently occur. The most common error made by caretakers is they
overestimate the capacity of the student with an NLD to generate adaptive
problem solving solutions to cope with difficult situations. Because the student is
not quick to discern the relevant aspects of a social situation, he or she must be
taught step-by-step responses and behaviours, similar to those employed for young
children (Rourke, 1995). For this reason, a student with an NLD must be
encouraged to describe events in which he has experienced interpersonal difficulty
and have not understood the behaviour of others. Problems understanding the
nonverbal aspects of behaviour and making inferences regarding cause-and-effect
relationships may result in large portions of emotional meaning being absent from
the child’s perception of a situation. Discussion may help the student become
aware of discrepancies between his or her perceptions and the perceptions of
others (Rourke, 1995). In this regard, role plays may help greatly. However,
ability to generalise is problematic and the child with an NLD tends not to be
flexible and adaptive in the application of learned behaviours and when to use
them.
10. Compensatory aids. A hand calculator will assist mathematical operations and a
digital watch will help learning to tell the time. After working mechanical
arithmetic with pencil and paper, the younger student can check the accuracy of
the answer with a hand calculator. If incorrect, the student may be encouraged to
rework the question using pencil and paper. To help the child understand the
passage of time, a traditional clock with a minute and second hand that moves
around the clock face is a better learning tool than the flashing numbers on a
digital watch (Stewart, 2002).
Selected hints from this study for teachers and aides
The following strategies were offered by teachers and aides which may prove useful for
others:
1. One teacher believed the secret of having a child with hydrocephalus and spina
bifida in the class was to get the class to help by developing a class culture of
support and understanding;
2. Provide a culture around them in the classroom that enlists the support of
classmates;
3. Teacher and student do not have to do it alone. Provide support that the child
knows they can rely on;
4. To promote a culture of acceptance and understanding, another teacher wove a

349
lesson on the Walking Miracles in our Class into a Science lesson. This provided
opportunity for every class member to speak about any significant illness or
operation;
5. There is a need for teachers and aides to adapt and protect a student with
hydrocephalus and spina bifida and be willing to accept “that is as much as she can
do and that’s great and that’s fine”;
6. There is a need for continual check on students with hydrocephalus and spina
bifida. “You can’t assume that because they’re not disrupting your lesson that they
are performing at their optimum level because the chances are that they’re not”;
7. Finding some talk time before or after a lesson was considered important to get to
know the student, build rapport and over time, observe what the student is capable
of;
8. A Pain Scale was found useful to gauge severity of headaches, aches and pains;
9. Colour-coding on the blackboard helped the student to locate work to be copied;
10. To reduce the amount of writing, one teacher underlined/circled key words on the
board for the child to copy as dot points;
11. To ease the writing task, student can read from the board while teacher aide does
the writing;
12. To help the child start a writing task, one teacher wrote sentence starters on
laminated card;
13. Teacher can manage the child’s difficulty with task completion beforehand by
reducing the amount of work;
14. Better application and writing fluidity with cursive writing than with printing was
observed which may have been due to continuous pencil-paper contact and more
focused attention;
15. When grouping in class, the teacher needs to be very aware of where the student is
supported … “there’s a natural barrier that she’s got to overcome with the other
students … it would be up to the peers to let her in” but once accepted, she would
get in and try her very best;
16. A daily checklist on student’s desktop helped organisational skills;
17. With any new situation, staff at one school ensured there was base of familiarity,
whether that is a person or an environment;
18. If the student is reluctant to ask for help, the teacher or aide may draw a
consequence tree that outlines the advantages and disadvantages of asking for
help.

350
19. For high school students:
a. “Lemonade Stand” was a maths computer game that offered experience
with buying, selling and profit;
b. Calligraphy was reported to be an enjoyable and manageable practical art
subject.
For older students, a talk to the class about the child’s medical condition in Years 1 or 2
is insufficient on two counts, changing class compositions and student regroupings. “I don’t
think that her classmates probably understand very much about her at all … if they did then
the dynamics that she’s had in the past couple of years probably wouldn’t have ever
happened” and “there’s some kids in her grade who have no idea what’s wrong with …” said
teachers and parents. Teachers have a particular responsibility here and should be
encouraged to engage the help of the class by building a class culture that emphasises:
1. care, consideration and support for classmates;
2. an understanding that some students have special requirements;
3. “no” there will be no teasing and “yes” there are special requirements for a student
with a shunt just like anyone else with broken leg or physical problem;
4. no bumping the student who has a shunt;
5. help for every child to do what they need to do;
6. discussion about the student’s back, shunt and the effects of the medical
conditions.
One teacher had regular open class discussions about student differences while another
wove such discussion/s into a Science lesson. This allowed the teacher to talk about
individual differences and it provided opportunity for each child to speak about any
significant illness, injury or operation. Alternatively, the school nurse may be invited to
conduct session/s with the class.

351
APPENDIX G
Information Packs
Letter of Introduction (Parents)
17 November, 2004 Dear Parent or Caregiver
Letter of Introduction
My name is Barbara Rissman and I am a PhD student from the Centre for Innovation in
Learning, Faculty of Education, Queensland University of Technology (QUT), Kelvin
Grove, Brisbane.
I am undertaking postgraduate research to explore how parents and teachers involved
with students who have shunted hydrocephalus and spina bifida perceive the educational
experiences of these young people.
Initially, I am looking for children and adolescents:
• aged 9-16 years in mainstream schooling
• with shunted hydrocephalus associated with spina bifida (including encephalocele)
• who speak and read well
• who have trouble with maths and handwriting
• who live in south-east Queensland
The project has been granted ethical approval by the University Human Research Ethics
Committee and the Royal Children’s Hospital Human Research Ethics Committee. This
approval requires me to ensure that informed consent and confidentiality issues are
safeguarded and that all information gathered is treated with the utmost respect.

352
I would ask you to read the attached Information Sheet. If you have any complaints
about the ethical conduct of the research or you wish to raise any concerns please contact:
QUT Research Ethics Officer Exec Support Officer RCH Ethics Committee
Tel 07 3864 2340 Tel 07 3636 9167
Fax 07 3864 1304 Fax 07 3365 5455
Email [email protected] Email [email protected]
If you would like more information about this project, please do not hesitate to contact
me on:
QUT 07 3864 3074
Home 07 3883 3757
Mobile 0421 826 401
Email [email protected]
If you and your child would like to share your experiences and take part in the
recruitment process for this study, it would help me a great deal if you could sign the consent
form and return to me by 24th November, 2004. This will allow me a short time to arrange
an interview with your child’s teacher/s before the end of the current school year.
Yours sincerely
Barbara Rissman
PhD student

353
Study Description (Parents)
Study Title: Learning experiences of young people with shunted Hydrocephalus and
Spina Bifida
This study is being conducted by Barbara Rissman who is a postgraduate research
student from the Centre for Innovation in Education, Faculty of Education at Queensland
University of Technology (QUT), Kelvin Grove, Brisbane.
The researcher proposes to recruit students with shunted hydrocephalus associated with
spina bifida (including encephalocele) who are in primary and secondary school classes.
Participation in this research is voluntary. If you decide to participate and then wish to
discontinue at any time, your decision will be respected without comment.
The study aims to “give voice” to parents, teachers and students by giving them
opportunity to share experience and insight gained from working with these young people.
Findings may lead to new understanding of the learning needs of individuals with shunted
hydrocephalus and spina bifida. The researcher will provide feedback to participants
involved in the study when this is requested and is practicable.
The project will involve:
• sharing information from previously conducted psychological testing with the
research team in order to determine what additional testing will be required for this
study;
• 1 assessment session with your child conducted by a person qualified to administer
psychological tests. The assessment session will be held at Kelvin Grove QUT
campus and parking will be arranged. The session is expected to last approximately
1 hour and there will be no cost to families for this assessment session;
• 2 informal interviews to explore how parents, teachers and students perceive the
learning experiences of these young people. If convenient, interviews with parents
and students will be conducted in the student’s home. Each interview will last
approximately 1 hour.

354
Participation in this study does not involve any known risks and assessment tasks do not
present any known safety hazards to participating children and adolescents. Parents and
caregivers are invited to accompany their child or adolescent to campus for the assessment
session. During assessments, young people will not be left unattended at any time.
With permission, informal interviews will be tape recorded to assist the researcher with
data analysis and coding. Information gathered will be checked with the person providing
that information. This information will later be used in the study’s final report in a de-
identified form.
The University Human Resource Ethics Committee and the Royal Children’s Hospital
Human Resource Ethics Committee require me to ensure that all personal names and names
of schools are substituted with false names and to exercise all reasonable precautions to
protect confidentiality of interview data. If you have any questions, please contact me by
using the contact details below.
If you have any complaints about the ethical conduct of the research or you wish to
raise any concerns please contact:
QUT Research Ethics Officer Exec Support Officer RCH Ethics Committee
Tel 07 3864 2340 Tel 07 3636 9167
Fax 07 3864 1304 Fax 07 3365 5455
Email [email protected] Email [email protected]
If you and your child or adolescent would like to participate in the recruitment process
for this study, please complete the attached consent form and return to me by 24th November,
2004.
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mob 0421 826 401
Email [email protected]

355
Consent Form (Parents)
Study Title: Learning experiences of young people with shunted Hydrocephalus and
Spina Bifida
By signing below, I indicate that I have:
• Read and understand the information sheet about this project
• Had any questions answered to my satisfaction
• Been assured that if I have any additional questions I may contact the researcher
• Understood that participation is voluntary and that my child or I are free to withdraw
at any time without comment
• Agreed to share information from previously conducted psychological testing with
the researcher and research team in order to determine what additional testing will be
required for this project
• Given consent for my child to take part in:
a. 1 assessment session to be conducted at QUT Kelvin Grove campus that will
last approximately 1 hour. I understand that parking will be arranged for
me;
b. 2 informal interviews and each interview will last approximately 1 hour.
• Agreed to participate in the project
• As parent, agreed to 2 informal interviews being tape recorded
• Agreed to 2 informal interviews with my child being tape recorded
• Been informed that the confidentiality of the information will be maintained and
safeguarded

356
Parent name ……………………………………………
Parent signature ……………………………………….
Date ………………………………………
Contact number ………………………....
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mob 0421 826 401
Email [email protected]

357
Letter of Introduction (Students)
17th November, 2004
Dear Student
Letter of Introduction
My name is Barbara Rissman and I am a postgraduate student at the Queensland
University of Technology (QUT), Kelvin Grove, Brisbane.
I am conducting a study to investigate how students, teachers and parents
involved with students who have shunted hydrocephalus and spina bifida understand
the educational experiences of these young people.
I am looking for children and adolescents aged 9-16 years who speak and read
well but have trouble with maths and handwriting.
I would ask you to read the Information Sheet for more information. If you
have any concerns or complaints about the way this study will be conducted, you
may contact:
QUT Research Ethics Officer Exec Support Officer RCH Ethics Committee
Tel 07 3864 2340 Tel 07 3636 9167
Fax 07 3864 1304 Fax 07 3365 5455
Email [email protected] Email [email protected]
If you would like to share your experiences and take part in the selection process
for this study, I would be very pleased if you could sign the Statement of Assent and
post it back to me by 24th November, 2004. This will allow me a short time to
arrange an interview with your teacher/s before the end of this school year. I am also
writing to invite your parents to take part in this project.

358
If you would like more information, please do not hesitate to contact me by
using the contact details below:
QUT 07 3864 3074
Home 07 3883 3757
Mobile 0421 826 401
Email [email protected]
Yours sincerely
Barbara Rissman PhD student

359
Study Description (Students 9-16 years)
Study Title: Learning experiences of young people with shunted Hydrocephalus and
Spina Bifida
This study will be conducted by Barbara Rissman who is a postgraduate student
at the Queensland University of Technology (QUT), Kelvin Grove, Brisbane. The
study will involve children and adolescents with shunted hydrocephalus and spina
bifida (including encephalocele) who are in primary and secondary school classes.
You are free to choose whether or not you would like to take part in this
research. If you decide to take part and then you wish to stop taking part at any time,
your decision will be respected without any comment.
The study aims to give students, parents and teachers an opportunity to talk
about the educational experiences of students. Findings may lead to new
understanding of the learning needs of students who have shunted hydrocephalus and
spina bifida. The researcher will give you feedback on the overall outcomes of the
study if you request this.
Firstly, we would like to use well-used tests to assess some of your skills.
Testing will be conducted at the Kelvin Grove QUT campus by a person who is
qualified to administer these tests. The test session will last about 1 hour.
Secondly, the researcher would like to talk with you, your teacher and your
parents about how they understand your learning experiences. This will involve 2
informal interviews and each interview will last about 1 hour.
With permission from you and your parents, I would like to tape record
interviews because this will make the coding and analysis of information easier for
me. All information that you provide will be treated with respect and trust. This
information will be checked with you and later used in the study’s final report.

360
If you would like more information, you or your parents may contact me by
using the contact details below. If you have any concerns or complaints about the
way this study will be conducted, please contact:
QUT Research Ethics Officer Exec Support Officer RCH Ethics Committee
Tel 07 3864 2340 Tel 07 3636 9167
Fax 07 3864 1304 Fax 07 3365 5455
Email [email protected] Email [email protected]
If you would like to share your experiences and take part in the selection process
for this study, please sign the enclosed Statement of Assent and return it to me by
24th November, 2004.
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mob 0421 826 401
Email [email protected]

361
Statement of Assent (Students 9 - 16 years)
Study Title: Learning experiences of young people with shunted Hydrocephalus and
Spina Bifida
By signing below, I indicate that I have:
• Read and understand the information sheet about this project
• Had any questions answered to my satisfaction
• Been told that if you have any more questions I may contact the researcher
• Understood that I am free to choose to take part in the research and that if I
wish to withdraw at any time, my decision will be respected without any
comment
• Agreed to take part in this project
• Agreed to take part in:
a. 1 test session to be conducted at QUT Kelvin Grove campus that will
last about 1 hour;
b. 2 informal interviews to discuss my learning experiences.
• Understood that all information will be treated with respect and trust
Student name ……………………………………………
Student signature ………………………… Date ……………
Parent signature ………………………….. Date ……………
Contact number ………………………....

362
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mob 0421 826 401
Email [email protected]

363
Letter of Introduction (Principals, teachers and teacher aides)
4 February, 2005 Principal ……… Dear
Letter of Introduction
My name is Barbara Rissman and I am a PhD student from the Centre for Innovation in
Learning, Faculty of Education, Queensland University of Technology (QUT), Kelvin
Grove, Brisbane.
I am undertaking postgraduate research to explore how teachers and teacher aides
involved with students who have shunted hydrocephalus and spina bifida perceive the
educational experiences of these young people. I propose to recruit a group of students aged
9-16 years who are in primary and secondary mainstream schooling. These children will be
recruited through Spina Bifida and Hydrocephalus Queensland, Mater Spina Bifida clinic
and the Royal Children’s Hospital Spina Bifida clinic.
I am writing to ask your permission to interview the teachers and teacher aides in your
school who currently teach and assist … If you agree, I would like to conduct interviews at
the beginning of Term 2, 2005. Each interview is expected to last approximately 1 hour.
The study aims to provide opportunity for teachers and teacher aides to share valuable
insight and experience gained from working with these young people. Every endeavour will
be made not to encroach upon busy teaching and classroom schedules and the researcher will
at all times be happy to accommodate whatever interview day and time is nominated by the
teacher. As part of the research, parent and student perceptions will also be explored and
these interviews will be conducted in the family home. Participation does not involve any
known risks.

364
With permission, informal interviews will be tape recorded to assist with data analysis
and coding. Information gathered will be checked with the person providing that
information. This information will be later used in the study’s final report in a de-identified
form. The researcher will provide an executive summary of research findings to
participating schools and to Education Queensland.
Ethical approval for this study has been granted by QUT Human Resource Ethics
Committee, Education Queensland, the Mater Hospital and the Royal Children’s Hospital.
These approvals require me to ensure that (1) all personal names and names of schools are
substituted with pseudonyms and (2) the researcher exercises all reasonable precautions to
protect confidentiality of interview data. If you have any concerns or complaints about the
ethical conduct of the project you may contact:
QUT Research Ethics Officer Education Queensland
Tel 07 3864 2340 Tel 07 3237 1700
Fax 07 3864 1304 Fax 07 3237 1175
Email [email protected] Email Denise Coulter
If you would like more information about the study, please do not hesitate to contact me
by using the contact details below. For your information, I attach a copy of the proposed
Letter of Introduction, Study Description and Consent Form for teachers and teacher aides.
Thank you for taking the time to read this letter. It would help me very much if you
could respond by Friday, 18th February and if you agree, return the attached consent form so
that I may forward information packs to teachers and teacher aides.
Yours sincerely
Barbara Rissman
PhD student
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mobile 0421 826 401
Email [email protected]

365
Consent Form (Principal)
Study Title: Learning experiences of young people with shunted Hydrocephalus and
Spina Bifida
By signing below, I indicate that I have:
• Read and understood the researcher’s Letter of Introduction which provided
information about this project
• Had any questions answered to my satisfaction
• Been assured that if I have any additional questions I may contact the researcher
• Understood that participation by the school of which I am principal is voluntary
• Understood that participation by teachers in the school of which I am principal is
voluntary
• Agreed to allow specified teachers to participate in the project subject to the consent
of the individual teacher or teacher aide
• Been informed that the confidentiality of the information will be maintained and
safeguarded
• Understood that an executive summary of the study will be provided to participating
schools
Principal’s name ………………………………..
Signature ………………………………………...
Date …………………………………….
Contact number …………………… …

366
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mobile 0421 826 401
Email [email protected]

367
Letter of Introduction (Teachers and teacher aides)
……… 2005 Dear
Letter of Introduction
My name is Barbara Rissman and I am a PhD student in the Centre for Innovation in
Education, Faculty of Education, at Queensland University of Technology (QUT), Kelvin
Grove, Brisbane. I am undertaking research to explore how teachers, teacher aides, parents
and students perceive the learning experiences of young people with shunted hydrocephalus
and spina bifida.
I propose to recruit students aged 9-16 years who are in primary and secondary school
classes. This age-range will incorporate transitional periods in a young person’s life. These
children will be recruited through Spina Bifida and Hydrocephalus Queensland, Mater Spina
Bifida clinic and the Royal Children’s Hospital Spina Bifida clinic. The student selected to
participate from your school is …
I expect that teachers and teacher aides will have information-rich understanding and
insights and based on this premise, I would like to invite you to participate. Participation is
voluntary and if you decide to participate and then wish to discontinue at any time, your
decision will be respected. If you agree to participate, I would like to conduct interviews at
the beginning of Term 2, 2005. Each interview is expected to take approximately 1 hour.
Every endeavour will be made not to encroach upon busy teaching/classroom schedules and
I will at all times be happy to accommodate whatever interview day and time you nominate.
This study has been granted ethical approval by QUT Human Resource Ethics
Committee, Education Queensland, the Mater Hospital and the Royal Children’s Hospital.
These approvals require me to ensure that (1) all personal names and names of schools will
be substituted with pseudonyms (2) the researcher will exercise all reasonable precautions to
protect confidentiality of interview data.

368
I would ask you to read the attached Study Description for more information. If you
have any concerns or complaints about the ethical conduct of the project you may contact:
QUT Research Ethics Officer Education Queensland
Tel 07 3864 2340 Tel 07 3237 1700
Fax 07 3864 1304 Fax 07 3237 1175
Email [email protected] Email Denise Coulter
If you would like more information about the study, please do not hesitate to contact me by
using the following contact details:
QUT 07 3864 3074
Home 07 3883 3757
Mobile 0421 826 401
Email [email protected]
If you would like to share your experience and insights and participate in this study, I
would be very pleased to hear from you by …
Yours sincerely
Barbara Rissman
PhD Student

369
Study description (Teachers and teacher aides)
Study: Learning experiences of young people with shunted Hydrocephalus and Spina
Bifida
This study is being conducted by Barbara Rissman, a postgraduate research student
from the Centre for Innovation in Education, Faculty of Education at QUT, Kelvin Grove,
Brisbane. The researcher proposes to recruit young people with shunted hydrocephalus
associated with spina bifida who are in primary and secondary school classes.
I propose to conduct one informal interview with teachers and teacher aides to explore
how they perceive the learning experiences of these students. Interviews are expected to last
approximately 1 hour each. The study aims to provide opportunity for teachers to share
valuable insight and experience gained from working with these young people. The student
selected to participate from your school is …
Every endeavour will be made not to encroach upon busy teaching/classroom schedules
and the researcher will at all times be happy to accommodate whatever interview day and
time is nominated by the teacher. As part of the research, parent and student perceptions will
be explored and these interviews will be conducted in the family home. Participation does
not involve any known risks.
With permission, informal interviews will be tape recorded to assist the researcher with
data analysis and coding. Information gathered will be checked with the person providing
that information. This information will be later used in the study’s final report in a de-
identified form. The researcher will provide an executive summary of research findings to
participating schools and to Education Queensland.
Ethical approvals from QUT, Education Queensland, the Mater Hospital and the Royal
Children’s Hospital require me to ensure that (1) all personal names and names of schools
are substituted with pseudonyms (2) the researcher exercises all reasonable precautions to
protect confidentiality of interview data. If you would like more information about this
study, please do not hesitate to contact me by using the contact details below.

370
If you have any concerns or complaints about the ethical conduct of the project, please
contact:
QUT Research Ethics Officer Education Queensland
Tel 07 3864 2340 Tel 07 3237 1700
Fax 07 3864 1304 Fax 07 3237 1175
Email [email protected] Email Denise Coulter
If you would like to share your experience and insights and participate in this study,
please complete the attached consent form and return to me by …
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mobile 0421 826 401
Email [email protected]

371
Statement of Consent (Teachers and teacher aides)
Study: Learning experiences of young people with shunted Hydrocephalus and Spina
Bifida
By signing below, I indicate that I have:
• Read and understand the information sheet about this project
• Had any questions answered to my satisfaction
• Been assured that if I have any additional questions I may contact the researcher
• Understood that participation is voluntary and that I may withdraw from the study at
any time and that my decision will be respected
• Agreed to participate in 1 informal interview
• Agreed to 1 informal interview being tape recorded for the purpose of data coding
and analysis
• Been informed that the confidentiality of the information will be maintained and
safeguarded
• Agreed to participate in the project
Teacher’s name ………………………………..
Signature ………………………………………...
Date …………………………………….
Contact number …………………… …

372
Barbara Rissman Research Team Supervisors
QUT 07 3864 3074 Assoc Prof J Lidstone Tel 07 3864 3289
Home 07 3883 3757 Assoc Prof M McDowell, M.D. Tel 07 3010 3366
Mobile 0421 826 401
Email [email protected]





























