Embed Size (px)
DESCRIPTION
paediatrics lecture notes on bronchial asthma from college of medicine, university of ibadan, Nigeria
Citation preview

Bronchial Asthma
Outline of the Lecture(s)
Bronchial Asthma IIntroductionDefinitionsEpidemiologyPathogenesis/ Pathophysiology
Bronchial Asthma IIClinical Features & InvestigationsDifferential Diagnoses

Introduction
• Bronchial asthma is one of the most common chronic illnesses and prevalence is increasing.
• Asthma is probably not one illness, but a syndrome.
• The disease has different phenotypes with respect to its course and prognosis and its association with atopy.
• The diagnosis, assessment of severity and monitoring of the effects of therapy are more difficult in young children because it may not be possible to obtain reliable objective measurement of airway obstruction.

Definitions
Bronchial Asthma: Asthma is a chronic inflammatory disorder of
the airway in which many cellular elements play a role.
The chronic inflammation causes associated increase in airways hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness and coughing particularly at night or early in the morning.
These episodes are usually associated with
widespread or variable airflow obstruction that is often reversible either spontaneously or with treatments.

Definitions (contd.)
• Airway responsiveness:
The response of the airways to provoking stimuli, usually expressed as the provoking dose (concentration causing a 20 per cent fall in FEV1) or the slope of a dose-response curve.
Definitions (contd.)
• Hyperresponsiveness (Hyperreactivity): The propensity of the airway to constrict too easily and too much to allergens.
• Atopy: The ability to develop IgE to innocuous and ubiquitous environmental agents such as pollens, mites and molds.

Definitions (contd.)
• Vital capacity: largest volume a subject can expire after a single maximal inspiration.
• Forced vital capacity : The vital capacity when the expiration is performed as rapidly as possible.
Definitions (contd.)
• Forced expiratory volume in one second (FEV1): Volume expired during first second of Forced Vital Capacity.
FEV1/FVC=75%
This ratio is reduced in obstructive airway diseases like asthma, emphysema and bronchitis.
• Peak expiratory flow rate (PEFR): Maximum expiratory flow rate achieved during a forced expiration.
PEFR is more convenient to measure than FEV1


Epidemiology
Geographical distribution• Worldwide• Prevalence
*Aderele reported 200 hospitalised children in two and a half years (Archives of disease in childhood
1980…..)*Sofowora and Clark: 2.4 per cent.*Okoromah reported 3.0 per cent among 6-13 year old children in Enugu.*Oviawe reported 0.7 per cent among children in a rural community.

Trend in the Prevalence of Bronchial Asthma in Ibadan,
NigeriaFalade et al using International Study of Asthma and Allergies in Childhood (ISAAC) Questionnaire
• ISAAC Phase One(1995) 6-7 year olds : 4.8%
13 -14 year olds:10.7%
• ISAAC Phase Three(2001/2002)6-7 year olds :5.6%13-14 year olds:13%

Epidemiology(contd.)
*Highest prevalence in the UK, Australia and New Zealand (ISAAC, 1998): 20% - 36.8%.
Epidemiology (contd.)
• Gender distribution
M:F=1.3:1
Risk Factors
• Host
• Environmental factors

Risk Factors (contd.)
• Host factorTwins study: effect of genetic factors about 35 to 70%
No gene or genes involved in the heritability of atopy or asthma has been identified with any certainty.
Results suggest involvement of multiple genes and chromosomal regions likely to harbour asthma susceptibility genes identified.
Environmental Factors
• Allergens
• Air pollution
• Viral respiratory infections

Environmental Factors (contd.)
• Allergens
Outdoor: Pollen (tree, grass and flower), moulds (Aspergillus fumigatus and others)
Indoor: Mites (Dermatophagoides pteronyssinus, D. farina), Animals (cats, dogs,birds), cockroaches.

Environmental Factors (contd.)
• Air pollution
Outdoor: Ozone (High ozone level where cars are many), SO2(High SO2 level in industrialized areas due to oil and coal combustion)
Indoor: Tobacco smoke, moulds, contaminants from indoor gas combustion(NO2), fumes, perfumes, wood smoke.
Environmental Factors (contd.)
Viral respiratory infections
• Mainly RSV
• Others are: Rhinovirus, Parainfluenza virus

• Inducers (Precipitating factors)
• Inciters (Triggers)
Pathogenesis
• Chronic Eosinophilic Inflammation
• CD4+ TH2 Lymphocytes
• Interleukins• IgE antibodies (Allergen specific)• Mast Cell (and other effector cells)• Sensitization• Early response• Late response

Pathogenesis (contd.)
The Allergic Cascade
Sensitization• CD4+ Th2 cells and B cells interact and produce allergen
specific IgE
• Interactions between CD4+ T Cells and B Cells are important in IgE synthesis.
• IgE antibodies synthesized bind to high-affinity IgE receptors on the surface of mast cells in tissue or peripheral-blood basophils, and low-affinity IgE receptors on the surface of lymphocytes, eosinophils, platelets, and macrophages.
• This process is known as sensitization.

Pathogenesis (contd.)

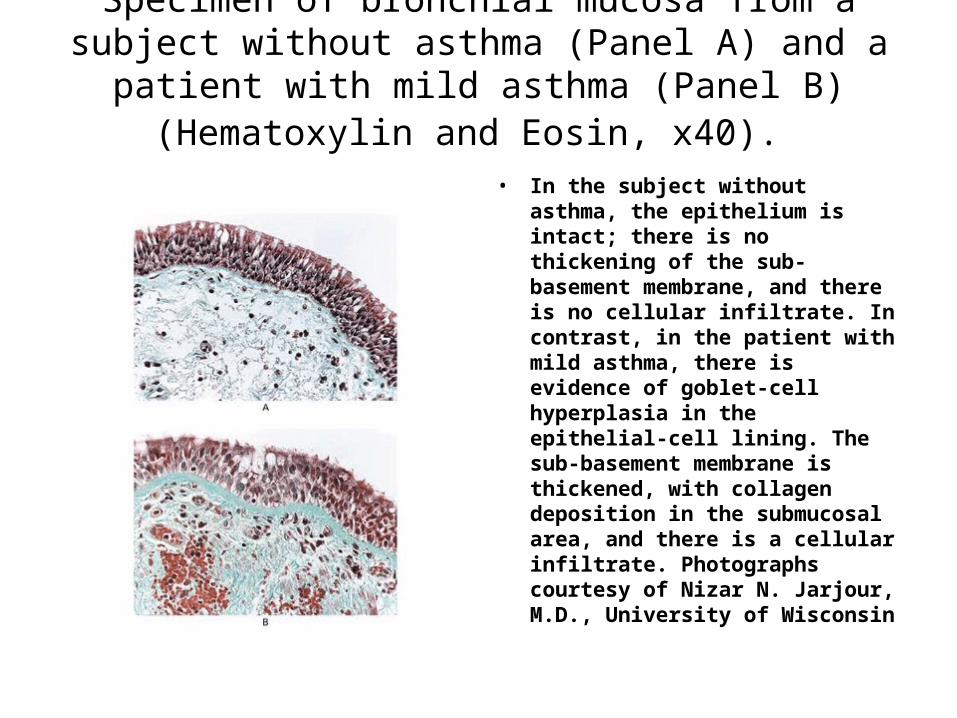
Specimen of bronchial mucosa from a subject without asthma (Panel A) and a patient with mild asthma (Panel B) (Hematoxylin and Eosin, x40).
• In the subject without asthma, the epithelium is intact; there is no thickening of the sub-basement membrane, and there is no cellular infiltrate. In contrast, in the patient with mild asthma, there is evidence of goblet-cell hyperplasia in the epithelial-cell lining. The sub-basement membrane is thickened, with collagen deposition in the submucosal area, and there is a cellular infiltrate. Photographs courtesy of Nizar N. Jarjour, M.D., University of Wisconsin
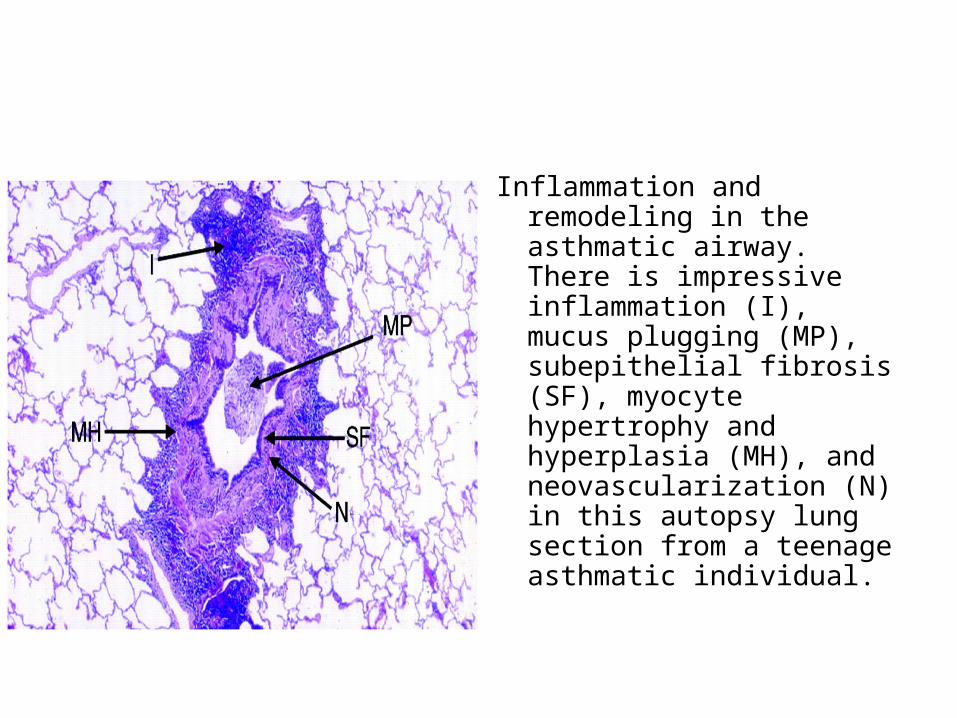
Inflammation and remodeling in the asthmatic airway. There is impressive inflammation (I), mucus plugging (MP), subepithelial fibrosis (SF), myocyte hypertrophy and hyperplasia (MH), and neovascularization (N) in this autopsy lung section from a teenage asthmatic individual.

Allergic Cascade (contd.)
Early Phase Response
When a sensitized individual comes in contact with the same allergen again, there is molecular bridging of the receptors.
• This occurs when allergen interacts with receptor-bound IgE molecules, causes activation of the cell and the release of preformed and newly generated mediators including histamine, prostaglandins, leukotrienes, and cytokines among others.
Early Phase Response (contd.)
• Once present in various tissues, mediators may produce various physiological effects, depending on the target organ.
• The early response involves mucosa oedema and bronchospasm producing the airway obstruction.

Late Phase Response
If no intervention, there is an influx of inflammatory cells mainly eosinophils and neutrophils,
• Further worsening the airway narrowing and consequently the airflow obstruction.
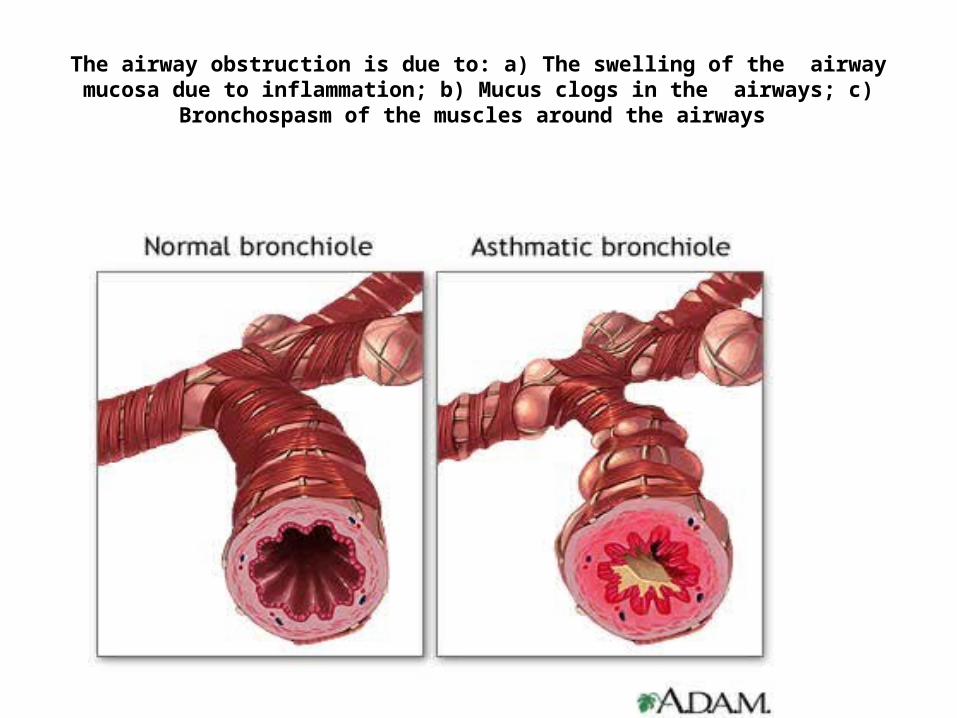
The airway obstruction is due to: a) The swelling of the airway mucosa due to inflammation; b) Mucus clogs in the airways; c) Bronchospasm of the muscles
around the airways

Airway Remodeling in Asthma
• Remodeling entails thickening of the airway walls, with increases in submucosal tissue, the adventitia, and smooth muscle.
• Preventing the progressive loss of lung function in childhood may require recognition and treatment of the disease during the first five years of life.
Bronchial Asthma II
Clinical Features
Investigations
Differential Diagnoses
Clinical Features
Symptoms
• One or more of the following three:
Cough
Attacks of wheeze, and
Breathlessness

Clinical Features (contd.)
• Repeated wheeze
• Recurrent or persistent cough
• Night time disturbance by wheeze or cough
• Symptoms precipitated by viral URTI; exercise or excitement; family emotional disturbances; potential allergens such as those associated with pets, pollens, dust, or feathers; cigarette smoke.
• Presence of collateral allergy e.g., allergic rhinitis and atopic dermatitis
Clinical Features (contd.)
• Past medical history of infantile eczema (atopic dermatitis)
• Family history of atopy
• Also therapeutic response to a bronchodilator makes the diagnosis more likely.
Investigations
• Demonstration of reversible airway obstruction
Pulmonary function test: FEV1 or PEFR before and after β2-agonist administration
An improvement of greater than 12% after 10 minutes


Other Tests
a) Bronchial provocation test,
b) Laboratory evaluation*Full blood count and absolute eosinophil count, *Specific IgE antibody measurements:-In vivo i.e., skin prick tests, -In vitro i.e., radioallergosorbent test (RAST)
c) Chest radiography.
Differential diagnoses
Differential diagnosis of wheezing during early life
Very commonAsthmaViral bronchiolitis
CommonForeign body in trachea or bronchusEndobronchial tuberculosis(TB)Enlarged TB nodes
Differential diagnoses contd.
UncommonVascular ringsBronchiectasisLaryngotracheomalaciaChlamydia trachomatis infectionObliterative bronchiolitisBronchopulmonary dysplasiaAspiration from swallowing mechanism dysfunction
or cardioesophageal reflux

Differential Diagnoses contd.
Rare
Tumour
Laryngeal webs
Tracheostenosis or bronchiostenosis
Alpha-1-antitrypsin deficiency
Cystic fibrosis

Bronchial Asthma (III)
• ManagementManagement
Therapy
• Acute therapy
• Long term management

Acute Therapy
Exacerbation:
• Usually reflects exposure to inciters (triggers)
• May reflect failure of long–term management/poor compliance with outpatient treatment

Goals of Therapy
• To reduce wheeze and cough
Relieve airflow obstruction and hypoxaemia as rapidly as possible
• Reduce the risk and number of acute exacerbations
Plan prevention of future relapses

Goals of Therapy (contd.)
• Minimize adverse effects of treatments, sleep disturbances, and absences from schoolClose monitoring of patients condition and response to treatments crucial for successful treatment
• Treatment is tailored to the severity of asthma

Management of Acute Exacerbations of Asthma
• Short History
• Assess severity
Acute exacerbations of asthma may be classified as mild, moderate or severe /life threatening
• Follow flow chart (algorithm) for acute therapy

Short history
Assessment of Severity
• Table 1: Classification of Acute exacerbation of Bronchial Asthma

Classification of Acute Exacerbation of Bronchial Asthma (contd.)
Recognition of acute severe asthma• Too breathless to talk
• Too breathless to feed
• Tachypnoea
• Tachycardia

Classification of Acute exacerbation of Bronchial Asthma (contd.)
Life threatening features
• Cyanosis, a silent chest, or poor respiratory effort
• Fatigue or exhaustion
• Agitation or reduced level of consciousness

Pharmacotherapy
Beta2 Agonists
• Short acting β2-agonists e.g., salbutamol (rather than theophylline)
• Bronchodilators used intermittently for the relief of symptoms rather than as regular maintenance therapy
• No oral or intravenous beta2 agonists in the treatment of acute asthma
• The inhaled method is the route of choice

Bronchodilators
• Oral steroids given early during an acute asthma exacerbation (i.e., within 45 minutes of the onset of symptoms)
• Oral corticosteroids more effective than inhaled or nebulized corticosteroids
• Children on oral steroids: extra care should be taken during episodes of increased stress e.g. surgery
• Subcutaneous adrenaline (0.01 ml/kg), 1:1000, a maximum of 0.3 ml
• Repeated maximum of 2 times after 20 minutes, i.e., 3 doses in 1 hour

Management at Home
• Mild acute exacerbation
Inhaled or nebulised beta2 agonist (3ce in 1 hour)

Management at Emergency Room
• Mild/Moderate/Severe
Moderate acute exacerbation
*Inhaled or nebulized beta2 agonist(3ce in 1 hr, and every hr after)
*Oxygen to achieve SaO2 95% or more
*If no immediate response or patient recently took oral steroid – oral prednisolone 1-2 mg/kg

Severe acute exacerbation
• Humidified O2
• Short-acting β2 agonist via oxygen driven
nebuliser(3ce in 1 hr.)
• Oral prednisolone 1-2 mg/kg
Severe acute exacerbation bronchial asthma (contd.)
If no response after 15 – 30 minutes
• Oxygen
• Oral prednisolone
• Nebulized salbutamol every 30 mins./continuously
• Add Ipratropium bromide

Severe acute exacerbation bronchial asthma (contd.)
If no response
• Aminophylline drip
If no response
• Admit ICU

The very severe asthma attack
• Children who present in extremis with a very severe attack of asthma should immediately be given 100% oxygen and adrenaline 0.3 ml subcutaneously, followed by intravenous salbutamol if they are unable to use a nebuliser. They should be admitted immediately to a high-care facility or ICU for intensive treatment
The very severe asthma attack (contd.)
• Humidified oxygen
• Short-acting β2 agonist nebulisation
• IV aminophylline 5mg/kg stat and aminophylline drip 1mg/kg/hr
• IV Hydrocortisone sodium succinate
• Ipratropium bromide 0.25 mg to nebulised beta2 agonist

The very severe asthma attack (contd.)
If no response
• Intubation and mechanical ventilation
Flowchart I

Flowchart II
Unnecessary therapy
• Antibiotics, cough syrups, mucolytics, antihistamines, mist tents, lung lavage, ionisers and physiotherapy (breathing
exercises)

Supplemental Oxygen
• 100% Oxygen for hypoxaemia(SaO2 < 90 %)
• Face mask or nasal prongs at 3-4 liters/min, or with
• Nasopharyngeal catheter at 1-2 liters/min.
• This will supply about 40% oxygen
Anticholinergics
• Ipratropium bromide
CORTICOSTEROIDS
• Oral vs. IV/Inhaled
THEOPHYLLINE
• It is not recommended for routine use
Radiographs
• Should be individualized
Follow-up
• Observed for at least 24 hours before discharge. • Discharged with sufficient medication for at least 3 days. • Instructed on the use of the Metered Dose Inhaler
(MDI), spacer or nebuliser.• PEFR measurements should be made at least 3 times a
day until they are reassessed within 3 days of discharge to assess PEFR deterioration.
• It is important that trigger factors (inciting agents) of the acute attack should be identified
• A written plan of action should be given to the patient.

Immunotherapy
• Immunotherapy can be used as an adjunct to standard drug therapy in allergic asthmatic children.
Long Term Management
• Long term management focuses on controlling asthma by treating the underlying airway inflammation.
CORTICOSTEROIDS
• Inhaled corticosteroids are the agent of choice in preventive care

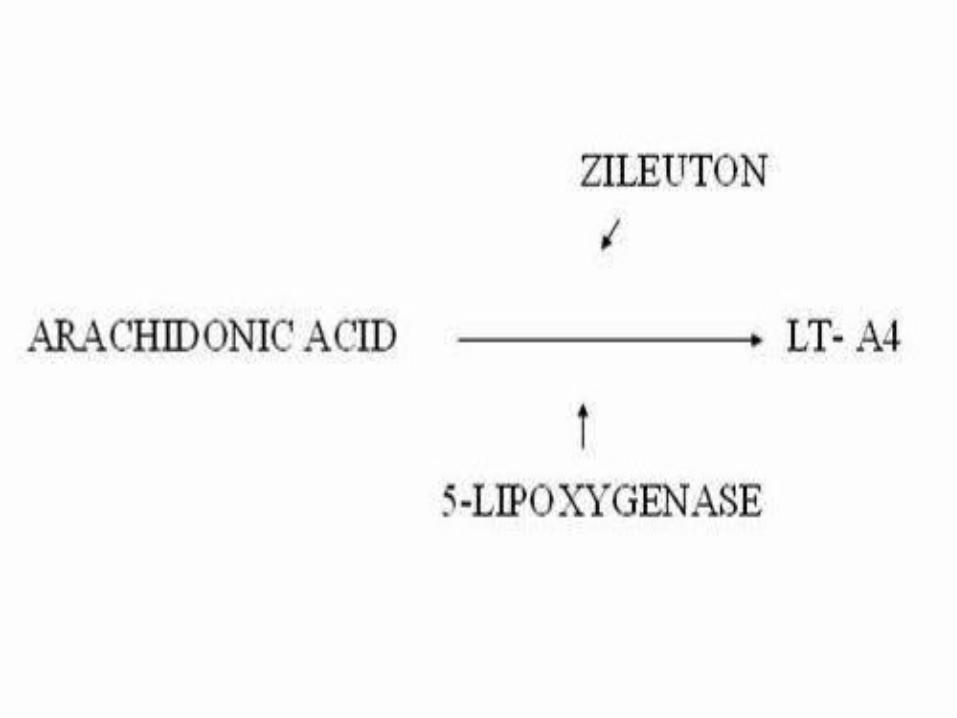
LEUKOTRIENE MODIFIERS
• Very useful

NEDOCROMIL AND CROMOLYN
• Not as useful as corticosteroid

LONG-ACTING BETA2 AGONIST
• Useful

ORAL THEOPHYLLINE
• In summary, its use in children cannot be recommended because of the potential for serious side effects, such as cardiac arrhythmias or convulsions, if therapeutic blood levels are exceeded

Classification of Severity for Long Term Management
• Intermittent
• Mild persistent
• Moderate persistent
• Severe persistent

Table: Classification of Severity for Long Term Management
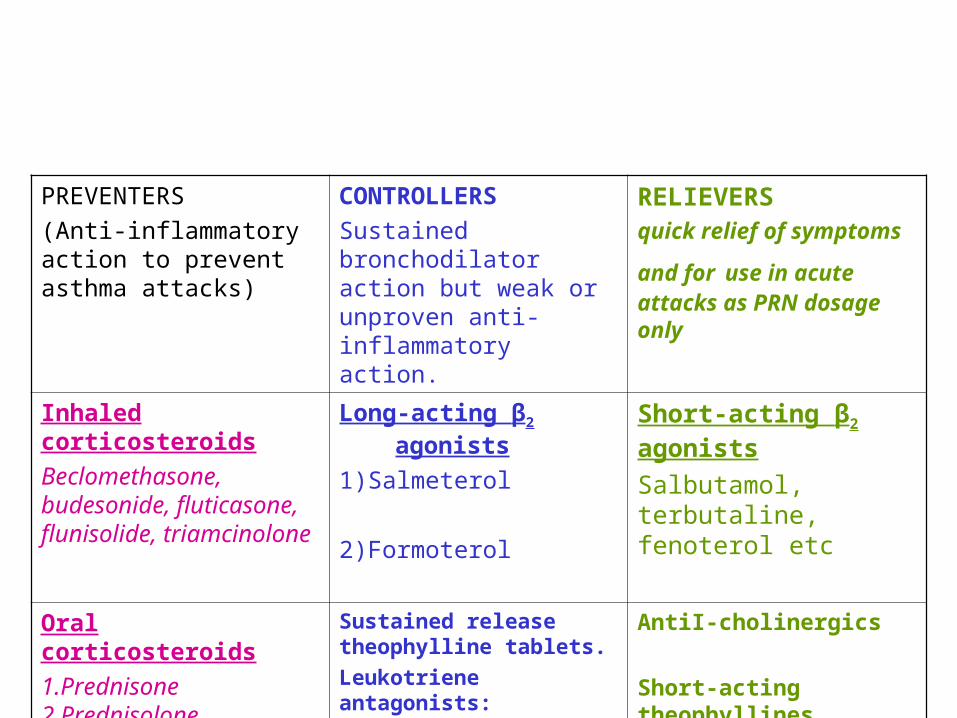
PREVENTERS
(Anti-inflammatory action to prevent asthma attacks)
CONTROLLERS
Sustained bronchodilator action but weak or unproven anti-inflammatory action.
RELIEVERS quick relief of symptoms
and for use in acute attacks as PRN dosage only
Inhaled corticosteroids
Beclomethasone, budesonide, fluticasone, flunisolide, triamcinolone
Long-acting β2 agonists
1)Salmeterol
2)Formoterol
Short-acting β2 agonists
Salbutamol, terbutaline, fenoterol etc
Oral corticosteroids
1.Prednisone2.Prednisolone 3.Methylprednisone
4.Methylprednisolone
Sustained release theophylline tablets.
Leukotriene antagonists:
1) Montelukast
2) Zarfirlukast
AntiI-cholinergics
Short-acting theophyllines


Long term management
IMMUNOTHERAPY
• Immunotherapy can be used as an adjunct to standard drug therapy in allergic asthmatic children
• Sublingual (allergy drops) and injectable (allergy shots) therapies have been shown to reduce the presence of asthma and the overall use of asthma medication

Other Interventions
• EDUCATION
• Reducing asthma triggers
The control of allergens has not been demonstrated to work as monotherapy. A recent study showed that house dust mite allergen avoidance and dietary fatty acid modification in the
first few years of life do not prevent asthma, eczema, or atopy in children with a family
history of asthma [Guy et al Allergy,2006]

Early Interventions Don't Prevent Asthma in High-Risk Children
• House dust mite allergen (HDM) avoidance and dietary fatty acid modification in the first few years of life do not prevent asthma, eczema, or atopy in children with a family history of asthma, new research shows.
• Sensitization to HDM and consumption of diets with a low omega-3 to -6 fatty acid ratio have been linked to asthma. Guy et al studied 616 children who were randomized to receive HDM avoidance, a diet with an increased omega-3 to -6 fatty acid ratio, both interventions, or no intervention during the first 5 years of life. Of these children, 516 were available for evaluation at 5 years.
• The HDM avoidance measure involved the use of allergen-impermeable linens and regular washing with an anti-HDM detergent. With the diet intervention, parents were encouraged to prepare their child's meals using canola-based oils and tuna oil capsules to achieve a high omega-3 to -6 fatty acid ratio.
• Although HDM avoidance measure reduced bedding allergen levels by 61%, it had no effect on the occurrence of asthma, wheeze, or atopy. In fact, eczema was actually more common in the HDM avoidance group than in controls: 26% vs. 19%.
• Similarly, while the diet intervention did succeed in increasing the omega-3 to -6 fatty acid ratio, it did not prevent asthma, wheezing, eczema, or atopy.
• Despite the null findings of the present study, previous reports support the view that, under certain circumstances, asthma can be prevented. However, the most effective, practical forms of early life environmental modification and the circumstances under which it will be appropriate to implement them remain to be established.
.

Newer therapy of chronic asthma
• Omalizumab and Sublingual Immunotherapy

Omalizumab
• Omalizumab is a recombinant DNA-derived humanized IgG monoclonal antibody that selectively binds to human immunoglobulin E (IgE).
• It inhibits the binding of IgE to the high-affinity IgE receptor on the surface of mast cells and basophils, limiting release of allergic mediators.
• Omalizumab is approved for use in children 12 years and older with moderate to severe persistent asthma who have a positive skin test or in vitro reactivity to a perennial aeroallergen and whose symptoms are inadequately controlled with inhaled corticosteroids .
Sublingual Immunotherapy
• Sublingual immunotherapy is a newer, more convenient option than injectable immunotherapy
The Take Home Message
• Don't call recurrent viral induced lower airway obstruction "bronchitis" or "pneumonia," or RAD, and just give antibiotics or just bronchodilators

The Take Home Message (contd.)
• Recognition that the viral URIs cause acute exacerbations, they are not responsive to antibiotics.
The Take Home Message (contd.)
• Limit maintenance medication to chronic or prolonged seasonal allergic symptoms choose the simplest effective and safe measures.

The Take Home Message (contd.)
• Recognize and instruct that maintenance medication won't prevent viral respiratory infection-induced exacerbations, and there needs to be consistency in instructions. This is a problem for large groups, because you may do things one way, your partner who is on call the next weekend may have very different instructions, for a chronic problem, that makes it very difficult to provide any kind of consistency, and just causes confusion for the patient.

The Take Home Message (contd.)
• Eliminate tobacco smoke exposure, continuing on timely intervention for acute exacerbations.
• Simplest age-appropriate method for inhaled bronchodilator delivery on hand and instructed

The Take Home Message (contd.)
• Early recognition of bronchodilator subresponsiveness.

The Take Home Message (contd.)
• Oral corticosteroids on hand, and started the day prior to the need for urgent care.

The Take Home Message (contd.)
• And we've got to develop a mentality of having zero tolerance for poor control. There is no such thing as successful treatment of asthma in the hospital - they are all failures. It's damage control, that's all it is. Successful treatment is preventing that from happening again.