Embed Size (px)
DESCRIPTION
Bronze Level Electrocardiography. Aims. Brief summary of relevant clinical electrophysiology Indications for taking an electrocardiogram (ECG) How to obtain a diagnostic ECG Basic ECG interpretation. Section 1 – electrophysiology for clinicians. Unique properties of cardiomyocytes. - PowerPoint PPT Presentation
Citation preview

www.ve
ts-now
.com
Bronze Level Electrocardiography

www.ve
ts-now
.com
Aims
1. Brief summary of relevant clinical electrophysiology
2. Indications for taking an electrocardiogram (ECG)
3. How to obtain a diagnostic ECG4. Basic ECG interpretation

www.ve
ts-now
.com
Section 1 – electrophysiology for clinicians

www.ve
ts-now
.com
Unique properties of cardiomyocytes
1. Electrical syncytiumThis means that the cells are coupled together in a way that permits rapid conduction of electrical impulses
2. Automaticity This describes the ability of cardiomyocytes to spontaneously depolarise. Under normal conditions the cells of the sinoatrial node have the fastest rate of spontaneous depolarisation and therefore are the dominant pacemaker cells.

www.ve
ts-now
.com
What is the ECG measuring?
• Electrical activity detected at the body surface– Cardiac tissue– Neuromuscular tissue (= movement)
• Movement artefact such as trembling results in irregular baseline movement as shown below:

www.ve
ts-now
.com
Einthoven’s triangle• Dr Einthoven invented the first practical ECG in
1903• Einthoven’s triangle refers to the imaginary
equilateral triangle formed by the 3 standard limb leads
+ Lead I - - L
ead
II
+
The dots demonstrate the standard electrode positions
Left forelimb Left hindlimb - Lead III +

www.ve
ts-now
.com
Anatomy of the intracardiac conduction system
Sinoatrial node (SAN)
Atrioventricular node (AVN)
Bundle of His
Left bundle branchRight bundle branch
Right Left

www.ve
ts-now
.com
Origin of -QRS-T
+VE(Left hindlimb in lead II)
-VE(Right forelimb in lead II)
Wave of depolarisation moves from sinoatrial node across atria from right to left thereby creating a flow in current towards the positive electrode
ECG:
P
Right Left
P

www.ve
ts-now
.com
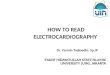
Origin of P- RS-T
Small delay as impulse traverses AVN hence trace returns to baseline. Depolarisation of the proximal interventricular septum then creates a small negative deflection – the Q wave.
ECG:
P Q
-VE(Right forelimb in lead II)
+VE(Left hindlimb in lead II)
Right Left
Q

www.ve
ts-now
.com
Origin of P- Q S-T
Wave of depolarisation moves rapidly through the conduction system to the heart apex thereby creating a flow in current towards the positive electrode – the R wave
ECG:
P QR
-VE(Right forelimb in lead II)
+VE(Left hindlimb in lead II)
Right Left
R

www.ve
ts-now
.com
Origin of P- QR -T
Wave of depolarisation moves from the cardiac apex towards the heart base
ECG:
P Q R S
-VE(Right forelimb in lead II)
+VE(Left hindlimb in lead II)
Right Left
S

www.ve
ts-now
.com
Origin of P- QRS-
Wave of depolarisation moves from sinoatrial node across atria from right to left thereby creating a flow in current towards the positive electrode
ECG:
P QRS T
-VE(Right forelimb in lead II)
+VE(Left hindlimb in lead II)
Right Left
T

www.ve
ts-now
.com
Section 2 - Indications for obtaining an ECG
• Common indications:– Document heart rate and rhythm– Dysrhythmia on auscultation
• Less common indications:– Electrolyte abnormalities– Suspected drug toxicity– Suspected cardiac chamber enlargement

www.ve
ts-now
.com
Section 3 - Obtaining a diagnostic ECG

www.ve
ts-now
.com
Patient set up for conscious ECG
• Patient calm and still• Good electrical contact• Clips over bony areas to reduce muscle
artefact• 50mm/s in leads I, II, III, aVL, aVR and aVF• 25mm/s rhythm strip for 1-5 minutes

www.ve
ts-now
.com
Machine set up for conscious ECG

www.ve
ts-now
.com
Set up for monitoring ECG
• Multi-parameter monitors• Tape ensures good contact between
electrode and pad

www.ve
ts-now
.com
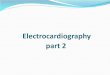
Muscle movement artefact
A common artefact seen on ECG is movement artefact caused by electrical activity present in moving muscles being detected by the ECG This results in rapidly undulating baseline movement which does not disrupt the superimposed heart rhythm.

www.ve
ts-now
.com
Now move onto the second slide show