-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
1/8
1www.eurosurveillance.org
Surveillance and outbreak reports
Description o measles D4-Hamburg outbreak inHamburg, Germany,
December 2008 to June 2009,which disproportionally afected a local
Roma
communityG Hy ([email protected].)1, K Kz2, M H3, A Mz4, S Bm5, A W6, G
F1
1. Centre or Inectious Disease Epidemiology, Institute or
Hygiene and Environment, Hamburg, Germany2. Public Health
Department o Hamburg-Mitte, Hamburg, Germany3. Public Health
Department o Hamburg-Harburg, Hamburg, Germany4. National Reerence
Centre Measles, Mumps, Rubella, Robert Koch-Institute, Berlin,
Germany5. Department o Microbiological Consumer Protection,
Institute or Hygiene and Environment, Hamburg, Germany6. Department
o Medical Microbiology, Institute or Hygiene and Environment,
Hamburg, Germany
C y f h :Hegasy G, Ktzner K, Helle M, Mankertz A, Baumgarte S,
Wille A, Fell G. Description o measles D4-Hamburg outbreak in
Hamburg, Germany, December 2008 toJune 2009, which
disproportionally afected a local Roma community. Euro Surveill.
2012;17(24):pii=20194. Available online:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20194
Article submitted on 27 October 2011 / published on 14 June
2012
From December 2008 to June 2009 a measles outbreakoccurred in
the Federal State of Hamburg, Germany.The outbreak affected 216
persons and was caused bya new measles strain termed D4-Hamburg
which led toconsecutive outbreaks between 2009 and 2011 in atleast
12 European countries. Here, we describe epide-miological
characteristics of the outbreak and evalu-ate the control measures
taken in Hamburg. In one of
the seven boroughs of Hamburg a local Roma commu-nity comprised
more than 50% of the notified cases.We compared in a stratified
analysis the age distribu-tion of these cases with cases of fellow
citizens whodid not belong to the Roma community. The age groupof
infants (0-11 months) comprised 33% among thenon-Roma measles
cases, while in the Roma commu-nity only 4% belonged to this
stratum. In the stratumof 5-17 year-olds only 8% were affected
among thenon-Roma cases, whereas in the Roma community50% belonged
to this age group. We discuss the influ-encing factors that might
have led to this difference inage distribution between the two
groups.
BackgroundIn December 2008 a measles outbreak started in thecity
o Hamburg, reached its peak during Februaryand March 2009 and ended
in June 2009 [1]. As dem-onstrated later by molecular typing, this
outbreak wasthe origin o European-wide spread o a measles
strainclosely related to D4-Enield, but later classiied asa
separate strain on the basis o sequence analysis.Consequently this
strain was named D4 Hamburg. Thespread o this D4-Hamburg virus
continued in Europein the ollowing three years and led to
consecutive out-
breaks in Bulgaria, Poland, Ireland, Northern Ireland,Austria,
Greece, Romania, Turkey, Macedonia, Serbia,Switzerland and Belgium
with over 25,000 personsinected [2].
The ollowing surveillance data on the D4-Hamburgoutbreak
concerning age, vaccination status and hos-pitalisation rate o
cases have been published earlier[1,2] and are only briely
summarised here: The agerange o cases was 1 day to 54 years; the
mean agewas 14.6 years and the median age was 13.5 years.
Avaccination card was available or 196 o 216 cases(91%). O these,
157 cases had no record o immunisa-
tion with measles-containing vaccine (MCV), including28 cases
below the recommended vaccination age o11 months. O 39 cases with a
record o MCV immuni-sation, one dose was documented or 33 cases,
twodoses or three cases, and or three cases the recordwas
ambiguous. O the 33 cases with one documenteddose, 26 were contacts
who had received a combinedmeasles-mumps-rubella vaccine (MMR) as
post-expo-sure prophylaxis, but still developed the disease. Nocase
ulilled the criteria or application o passive pro-tection using
antiserum according to guidelines o theGerman Standing Committee on
Vaccination (StndigeImpkommission, STIKO) [3]. The hospitalisation
ratewas 40%, with pneumonia and otitis media as the mostrequent
complications. No atality was reported in thisoutbreak.
Measles virus inection has been a notiiable diseasein Germany
since 2001 according to the CommunicableDisease Law Reorm Act
(Inektionsschutzgesetz,ISG). Vaccination guidelines are provided by
theSTIKO, which is ailiated to the Robert Koch Institute(RKI)
representing the ederal institution or diseaseprevention and
control in Germany. According to STIKOguidelines, a irst dose o MCV
should be given at the
age o 11 to 14 months and a second dose at the age o15 to 23
months, preerably using combined MMR vac-cine [3]. For individuals
missed in the regular sched-ule, catch-up vaccination is
recommended. Since 2010,
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
2/8
2 www.eurosurveillance.org
the STIKO has additionally recommended a single doseo MCV to be
given to any person born ater 1970 whohas not received two doses o
MCV or does not havea medical record o a subsided measles inection
[4].This decision to extend MCV immunisation to adultswas taken as
a result o continuing measles outbreaksin Germany, including the
outbreak described here [5].
To meet the WHO European Region measles eliminationtarget by
2015, a vaccination coverage o 95% or twodoses o MCV is necessary
[6]. According to assess-ment at school entry, adequate vaccination
status hasincreased in Germany over the last 10 years, but
cov-erage is still below this threshold (Germany 90.2%,Hamburg
90.5%) [7]. Furthermore, underserved minori-ties have repeatedly
been involved in large outbreaks inGermany [8,9]. Here, we describe
the measles outbreakin the Federal State o Hamburg in 2008-09,
which dis-proportionally aected a local Roma community.
MethodsFor the D4-Hamburg outbreak description, data romthe
electronical surveillance system were re-evaluatedaccording to ISG
using SurvNet sotware o RKI. Thesenotiication data include case
inormation on age, sex,onset and duration o disease, clinical
symptoms, lab-oratory conirmation, epidemiological links
betweencases and vaccination status i available. In
addition,semi-structured records on contact tracing and out-break
containment measures o the seven public healthdepartments o Hamburg
were evaluated.
Cases were deined as persons with a) a generalisedmaculopapular
rash or more than three days ANDever AND at least one o the
ollowing symptoms:cough, coryza, conjunctivitis or Koplik spots, OR
b) ageneralised maculopapular rash or more than threedays AND/OR
ever, AND laboratory diagnosis o mea-sles inection. Persons with
laboratory diagnosis o ameasles vaccine strain were excluded.
Measles virus RNA in nasopharyngeal swabs or oralluid was
detected by real-time RT-PCR perormed atthe municipal Institute or
Hygiene and Environmentas described earlier [10]. Genotyping was
perormedat the National Reerence Centre (NRC) or Measles,Mumps, and
Rubella as described earlier [11].
Analysis o the cases areas o residence by post-code and
cartography was perormed employingthe Geographical Inormation
System sotware ESRIArcGIS.
Outbreak description
Epidemic curve and geographical distributionThe outbreak started
in 2008 with a case in week 49
and a second case in week 52. It continued in 2009rom week 2 to
week 25 with 214 cases (Figure 1). Thecase in week 52 o 2008 was
initially termed as theindex case or Hamburg, although the patient
alling ill
Figure 1
Epidemic curve of measles D4-Hamburg outbreak,Hamburg, 1
December 200817 June 2009 (n=216)
Cases were assigned to the corresponding week according
toappearance o irst measles symptoms.
0
2
4
6
8
10
12
14
16
18
20
22
24
48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 1 1 12 1 3 14 1 5 16 1 7 18
19 20 21 2 223 24 25 26
2008
2009
Numberofcases
Week
Schleswig-
Holstein
Hamburg
Lower
Saxony
Figure 2
Outbreak location in the Federal State of Hamburg,Germany,
bordering Lower Saxony and Schleswig-Holstein, 1 December 200817
June 2009 (n=216)
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
3/8
3www.eurosurveillance.org
in week 49 o 2008 was retrospectively counted in asbelonging to
the outbreak as well. The outbreak lastedor 29 weeks with highest
case numbers between week6 and week 10 o 2009 (Figure 1).
Between week 3 and week 18 o 2009 the outbreakexpanded to Lower
Saxony, a bordering ederal state
south o Hamburg (Figure 2). Here, 53 cases were noti-ied. Within
the city limits o Hamburg the outbreakwas mainly localised in the
boroughs south o the riverElbe with a ocus on the boroughs o
Hamburg-Mitteand Harburg (Figure 3). To analyse the spatial
distribu-tion o the outbreak in more detail, postcodes o thecases
place o residence were mapped using geoinor-mation sotware at the
Centre or Inectious DiseaseEpidemiology. As demonstrated by this
approach, eighto 21 postcode areas were aected in this borough.
Thehighest incidences were restricted to the two postcodeareas in
the district o Wilhelmsburg (Figure 4).
Clinical and laboratory-confirmed casesFor 207 o the 216 cases
the diagnosis was based onthe clinical presentation and 190 o the
216 cases werelinked to another case epidemiologically. For 149 o
the216 cases a laboratory conirmation was notiied rep-resenting
69%. For 100 o them laboratory diagnosiswas based on PCR, o which
78 were conirmed by PCRalone, 20 by PCR in conjunction with IgM
detection,and one each by PCR in combination with rising IgGtitre
or virus isolation. A urther 44 o the 149 labora-tory-conirmed
diagnoses were based on IgM detectionalone, while our cases were
based solely on rising IgG
titre. One case was conirmed by virus isolation in con-junction
with IgM detection.
In addition to patients who received laboratory con-irmation o
measles inection by their amily doctor,physicians o the public
health departments oeredimmediate laboratory diagnostics during
contact trac-ing to potentially inected individuals. To this
endnasopharyngeal swabs or oral luid were taken andanalysed or
measles virus RNA by real-time RT PCR.Laboratory analyses were
oered ree o charge to thepublic health departments o Hamburg by the
munici-pal Institute or Hygiene and Environment. O 174 per-sons rom
whom nasopharyngeal swabs or oral luidwere taken during contact
tracing, 100 were ound pos-itive. This represents 67% o all
laboratory-conirmedcases o the outbreak. For sequencing and
geneticstrain analysis, 23 swabs were sent to the NRC. Twelveo them
were identiied as the virus strain later termedD4-Hamburg [2]. Ten
samples that were ound positivein diagnostic PCR could not be
sequenced successully.For one sample sequencing revealed an
inection withthe vaccine virus, and consequently this patient
wasnot counted as a case.
Index caseOn 27 and 28 December 2008, a patient in their
20spresented to the outpatient department (OPD) o a
hospital in Hamburg. The patient had suered rom asore throat
since 24 December 2008 and had devel-oped a rash ater taking
acetylsalicylic acid. Underthe assumption o streptococcal
pharyngitis and drugeruption ambulatory treatment with amoxicillin,
par-acetamol and an anti-histamine was given. Because
the patients condition deteriorated, they presentedon 29
December 2008 to the OPD o a second hospi-tal where inection with
measles virus was suspectedand the patient was hospitalised. As any
case o
Figure 3
Measles cases in the seven boroughs of Hamburg, 1December 200817
June 2009 (n=216)
Wandsbek19(4.1)Nord
11(3.8)
Eims-bttel
5(1.9)
Altona12
(4.8)RiverElbe
Bergedorf6
(5.0)
Mitte107(43.7)Harburg
56(29.6)
Number of Cases
0
1 - 5
6 - 20
21 - 100> 100
Incidence per 100,000 is given in parentheses.
3 (0.13)
3(n.d.)
1 (n.d.)
0
0
00 0 0
00
0
0
0 0
2(0.08)1 (0.06)
6 (0.45)
16(0.60)
75(3.05)
Number of Cases
0
1 - 5
6 - 20
21 - 100
> 100
Figure 4
Measles cases in the borough of Hamburg-Mitte bypostcode areas
of residence, 1 December 200825 May2009 (n=107)
Incidence per 100,000 is given in parentheses. For two
postcodeareas extending outside the borough borders o
Hamburg-Mitte,the incidence was not determined (n.d.).
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
4/8
4 www.eurosurveillance.org
clinically suspected measles has to be notiied accord-ing to the
ISG, the responsible public health depart-ment received a report on
this case on 31 December2008. Laboratory diagnosis later conirmed
the inec-tion by demonstrating positive IgM titre against mea-sles
virus and increasing IgG titres.
First and following generations of casesThe OPD visited irst by
the index patient was highlyrequented between Christmas and New
Year. The wait-ing area was overcrowded and patients had to wait
orseveral hours. Potentially inectious patients were notseparated.
Between 8 and 11 January 2009, ive per-sons that had been present
in this OPD on 27 or 28December 2008 ell ill with measles. These
comprisedtwo patients present in the waiting area or accidentand
emergency consultation, our persons accompany-ing patients to the
OPD or medical advice in internalmedicine or accident and
emergency, and one hospitalsta. All ive cases were notiied by their
physicians
according to the ISG. Further spread rom these ivecases to
household contacts was traced by the pub-lic health departments. In
the entire outbreak, one ormore, transmission chains were identiied
at each othe aected publicly accessible sites such as
kinder-gartens, primary and secondary schools, shoppingcentres, and
waiting areas o medical practices. Exactnumbers cannot be given
because not all records ontransmission sites were accessible or
retrospectiveevaluation.
Spread in a Roma community
On 26 January 2009, the public health department oHamburg-Mitte
received a report on a measles casein a woman in her 20s who was in
her 16th week opregnancy when she was diagnosed with measles on16
January 2009. As part o the contact tracing activi-ties, a home
visit was paid to this patient. She declaredunquestioned that she
belonged to a settled Romacommunity that traditionally lives in
this borougho Hamburg. She urther stated that all contact per-sons
named by her also belonged to that community.Consequently, she was
regarded as the index case orthe Roma community. In the ollowing
nine weeks, 60persons who indicated that they belonged to the
samecommunity ell ill with measles. O those, 56 caseslived in
Hamburg-Mitte which represents 52% o the107 cases reported in this
borough. The last case othe community ell ill on 19 March 2009.
Additionally,in Lower Saxony seven cases stated that they
belongedto the ethnic group o Roma.
On subsequent home visits paid to the community, twomore cases
were identiied who had occurred earlierthan the case regarded
initially as the Roma commu-nity index: On 2 December 2008, an
adolescent romthe community was diagnosed with measles. The
patient had been visited by relatives rom London inthe month o
November 2008. This case was notiied,but notiication reached the
responsible public healthdepartment with a delay o several weeks.
Although no
link could be ound to the patient who later presentedto the OPD,
this adolescent was most likely the trueindex case o the measles
D4-Hamburg outbreak. On17 December 2008 the patients older sibling
ell illwith measles. No notiication o this case was
receivedalthough the patient had been seen by a physician. Theolder
sibling was acquainted with the pregnant woman
ormerly regarded as the Roma community index case,but stated no
personal contact to her. Even assuming amaximal length o inectious
and incubation period (9and 21 days, respectively), disease onset
in the oldersibling occurred at least ive days too early to allowa
direct virus transmission rom them to the preg-nant woman. Thus, it
is highly probable that at leastone more connecting case occurred
in the communitythat was not seen by a physician, misdiagnosed or
notnotiied.
Control measuresIn all boroughs o Hamburg control measures
were
taken, but actions were ocused on those boroughssouth o the
river Elbe where most cases were reported.Visits were paid to 34
community acilities such as kin-dergartens, primary schools and
secondary schools.A community acility was selected or a visit i a
casehad occurred there, i a contact o a case attended thatacility,
or i it was located in a district highly aectedby the outbreak. On
these occasions, 364 doses oMCV were given on site to children as
well as teach-ers and sta. Another 497 children who could not
pro-duce parental consent to vaccination were advised toreceive MCV
rom their amily doctor. A total o 701
persons attending or working at the community acili-ties could
not provide proo o MCV immunisation or amedical record o a subsided
measles inection, andwere, based on ISG, suspended or two weeks
romtheir last potential contact to an inectious person.
In the context o enhanced measles surveillance,the requency o
case notiications rom local healthdepartments to RKI was increased
rom weekly to daily.In parallel, surveillance data were evaluated
and com-piled by the Centre or Inectious Disease Epidemiologyor
brieings o the State Health Department o Hamburgand or press
releases targeting either the general pub-lic or speciically local
physicians.
To provide inormation on measles to residents oaected districts
and to oer low-threshold accessto vaccination, a promotional bus
was borrowed romthe German Organisation or the Protection o
Children(Deutscher Kinderschutzbund Hamburg, DKSB) andallocated or
medical advice on measles prevention.Sta included two physicians,
two assistants, and atleast two interpreters. Interpreters were
health media-tors o the programme With Migrants or Migrants
(MitMigranten r Migranten, MiMi) which is described in
detail elsewhere [12]. The promotional bus was openedon six
occasions or our hours at central public placesin the borough o
Hamburg-Mitte. On these occasions
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
5/8
5www.eurosurveillance.org
964 consultations were requested and 18 MMR vacci-nations were
given.
To speciically reach the Roma community, 10 homevisits were paid
by the Public Health Departmento Hamburg-Mitte to Roma patients and
their con-tacts between 19 January and 5 February 2009. Sta
included a physician and at least one assistant. Onthese
occasions, vaccination cards were controlled andMMR immunisation
was oered as well as laboratorydiagnostics by nasopharyngeal swabs
or oral luid. Nodata were recorded separately or the Roma
communityconcerning the number o persons seen, contact per-sons
traced or vaccinations given, but on these occa-sions 19
PCR-positive measles cases were identiied inthe community.
Age distribution of cases in Hamburg-MitteO 107 cases notiied in
the borough o Hamburg-Mitte,56 belonged to the Roma community. We
considered
these surveillance data as suitable or urther analy-sis with
respect to the aected Roma and non-Romacommunity in Hamburg-Mitte.
No signiicant dier-ence in sex distribution o inected individuals
wasseen between both groups (non-Roma: 28 male and23 emale, Roma:
29 male and 27 emale, chi-squaredtest, two-tailed p value: 0.747).
As shown in Figure5A the mean age o the cases was 10.1 years or
theRoma group and 11.8 years or the non Roma group,while their
median age was one year or the non-Romaand nine years or the Roma
group. As the dierencebetween mean and median in the non-Roma
group
pointed to a non-Gaussian distribution, we wanted tostudy the
age distribution in both groups in more detailand thereore deined
ive age groups or a stratiiedanalysis. Stratiication was chosen as
ollows accord-ing to the standard vaccination schedule as
recom-mended by STIKO guidelines [3]: (i) inants under theage or
receiving MCV (11 months), (ii) age range orscheduled
administration o two doses o MCV (1223months), (iii) age range
without scheduled vaccina-tions (24 years), (iv) age range or
urther scheduledand catch-up vaccinations (517 years), (v) adults
(18years). As shown in Figure 5B, the age distribution inthe strata
(i) and (iv) diered between the groups.
DiscussionFor outbreak surveillance to be suicient, 80% o
clini-cally diagnosed measles cases should according to theWorld
Health Organizations guidelines, be laboratory-conirmed [6]. In the
outbreak described here, 149 o216 cases (69%) were conirmed by
laboratory analy-ses. O these 100 were identiied by PCR rom
naso-pharyngeal swabs or oral luid, representing 67% othe tests.
These PCR diagnostics were oered duringcontact tracing and home
visits by the public healthdepartments and perormed at the
municipal Institute
or Hygiene and Environment. In contrast to serologicalanalyses
as a standard tool or laboratory diagnosiso measles inection,
taking o nasopharyngeal swabsor oral luid or PCR is non-invasive
and was easily
A
0
5
10
15
20
25
30
35
40
45
50
Non-Roma community(n=51)
Roma community
Non-Roma community Roma community
(n=56)
B
9(18%)
17(33%)
9(16%)
7(12%)
1 (2%)
2 (4%)
4(8%)
28(50%)
20(39%)
10(18%)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
18 y
5-17 y
2-4 y
12-23 m
0-11 m
Age(years)
(n=51) (n=56)
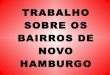
Figure 5
Age distribution of affected Roma and non-Roma inthe borough of
Hamburg-Mitte measles D4-Hamburgoutbreak, 1 December 200825 May
2009 (n=216)
A. Boxplot showing mean, median and quartiles o disease onsetage
o aected Roma and non-Roma community. Figures aregiven in table
below.
B. Stratiied age analysis. Cases were assigned to groups
asindicated based on age at disease onset.
Mean MedianM Q1 Q3 Max
Non-Roma community 11,8 1 0 0 24 44
Roma community 10,1 9 0 3,8 15 31
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
6/8
6 www.eurosurveillance.org
perormed by medical assistants. Ater arrival o thematerial at
the Institute or Hygiene and Environment,PCR results were available
within our to 24 hours andthus proved to be a ast and useul tool or
laboratoryconirmation o suspected cases ound during contacttracing.
The Institute or Hygiene and Environmentoered PCR analyses ree o
charge to the public
health departments in Hamburg which do not have abudget or
laboratory analyses. Furthermore, availabil-ity o nasopharyngeal or
oral luid swab material wasa prerequisite or genetic comparison o
the strainsby the NRC and identiication o the epidemiologicallinks
o the D4-Hamburg virus in Europe [2]. In sum-mary, ree-o-charge PCR
analyses provided a useultool or rapid case identiication,
laboratory conirma-tion and genetic analysis o the measles strain
in theD4-Hamburg outbreak.
Healthcare acilities can play an important role inmeasles
outbreaks [13,14]. This was also true or the
outbreak in Hamburg, where an early ocus o virustransmission was
a waiting area in a hospital, and atleast one urther transmission
site was the waitingarea at a doctors practice. Among the irst
generationo notiied cases a member o hospital sta was identi-ied.
Later, a second case o measles in a nurse wasnotiied. Both cases
had never received a dose o MCVaccording to their vaccination
cards. The STIKO hassince 2007 recommended a single dose o MCV to
begiven to non-immune healthcare sta, preerably as acombined MMR
vaccination [15]. Still there is no obliga-tion to comply with this
recommendation and control
o adequate vaccination status o their employees isthe
responsibility o the healthcare acility. Suboptimalimmunisation
coverage o healthcare proession-als in Germany has been described
beore [16]. TheD4-Hamburg outbreak demonstrates again that
pre-vention o disease transmission in healthcare acilitiesneeds to
be addressed.
One o the measures to contain the outbreak was apromotional bus
positioned in public places on sixoccasions, providing inormation
and vaccinations.Counselling was requested by 964 visitors who,
accord-ing to the physicians present, were almost exclusivelyadults
on their way to the nearby shopping centres.Only 18 persons (less
than 2% o visitors) acceptedon-site MMR vaccination. No data were
recorded onage, sex or immunisation status, but it is likely
thatmore visitors with inadequate measles protection didnot want to
receive a vaccination on this occasion. Weconclude that the
promotional bus as used in this out-break was appropriate or
providing inormation onmeasles to the local public, but it was not
eicient inpromptly raising vaccination numbers. We would there-ore
recommend this approach in an outbreak situationwhere the main
intent is increasing public awareness.
Furthermore, any outbreak containment measureshould record all
accessible data in order to allow alater evaluation o the measures
eiciency.
To speciically reach the Roma community, home vis-its were paid
to Roma patients and their householdcontacts. This approach was
chosen because otherattempts to establish contact with cases in the
com-munity were unsuccessul. As reported by the
outbreakinvestigation teams, initial visits to a household
werereceived with apprehension. On subsequent visits,
members o the community stated that this may havebeen caused by
an uncertainty to which public author-ity the team belonged and
what their actual intentionwas. When a team member identiied
themselves asa physician they were met with more trust on
urthervisits, and contact tracing and outbreak investiga-tions
became possible. During the home visits PCRdiagnostics could be
oered without delay, whichallowed identiication o a total o 19
cases that oth-erwise might not have been notiied. Based on
inor-mation gained during the visits the likely index patiento the
outbreak was identiied retrospectively andthe initial transmission
chain in the Roma community
could be partially reconstructed. Furthermore, pres-ence o a
physician allowed on-site vaccinations in theRoma community. It is
a shortcoming that no data wererecorded on the number o
vaccinations given on thesevisits, but this measure might have
contributed to theact that virus transmission stopped nine weeks
ear-lier in the Roma community than in the non Roma com-munity o
Hamburg-Mitte. In our experience, repeatedhome visits by a
physician are an advisable approachto establish contact to this
minority and to take imme-diate outbreak containment measures.
In a retrospective analysis we compared the age distri-bution o
cases in the Roma community and the non-Roma community in the
borough o Hamburg-Mitte.We considered the outbreak parameters as
suitable orthis comparison or two reasons: (i) number o casesand
sex distribution were similar in both groups, (ii)both groups were
citizens o the same borough, with85% living in the same district as
demonstrated bypostcode analysis. No reliable igures exist on the
sizeo this settled Roma community in Wilhelmsburg, butas an
estimate, the community may comprise severalhundred persons. It is
a shortcoming o our analysisthat no statistical reerence igures are
available tocompare age-related incidences in the two
subpopula-tions. Thus, our data only describe case numbers asthey
were recorded.
The most prominent dierences occurred in the stratao 011 month-
and 517 year-olds. In the non-Romacommunity, 33% o 011 month-olds
were inected withmeasles, compared with only 4% o the Roma
com-munity. This age group consists o inants too youngor MCV
immunisation according to STIKO guidelines.Their immune protection
correlates with the level andpersistence o transerred maternal
antibodies and
may depend on whether the mothers immunity wasacquired by
natural inection or by vaccination [17].Other actors modiy this
passive immunity, e.g. expo-sure to wildtype measles virus as a
natural booster or
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
7/8
7www.eurosurveillance.org
age o the mother during pregnancy [18]. It is temptingto
speculate that early protection in the Roma commu-nity described
here may have been higher because themothers were exposed to
wildtype measles inection,but this hypothesis could only be veriied
i data ontheir measles immune status were available.
Only 8% o 517 year-olds were aected among thenon-Roma citizens,
compared with 50% in the Romacommunity. For this age group standard
and catch-upvaccinations including MCV are recommended accord-ing
to STIKO guidelines. There are two mandatorycheckpoints in Hamburg
or control o a childs vac-cination status by a physician, the irst
on entry tokindergarten, the second on entry to school. The
irstcheckpoint is unlikely to reach children o a Roma com-munity as
they are usually parented by communitymembers. At school entry the
main ocus is on control-ling the vaccination record, and in case o
undervac-cination the parents are usually reerred to their
amily
doctor. This reerral might be ineective with memberso a Roma
community as they tend to make less useo standard healthcare and
preventive services [19-21]. Thus, it is conceivable that the
current approachto ensure adequate immunisation status o children
inHamburg is more eective in the non-Roma than theRoma population,
in which undervaccinated childrenand adolescents may
accumulate.
In other measles outbreaks in Europe involvingRoma communities,
the age distribution o cases di-ered between Roma and non-Roma
citizens [22,23],
although the results o these analyses are divergent.This might
be explained by dierences in the subpopu-lation analysed (e.g. Roma
or Sinti), the living condi-tions o the subpopulation (e.g. settled
or travelling),diversity in national vaccination schemes, and
dier-ent approaches to implement vaccination programmesor
underserved minorities.
The group o Roma has suered extensively rom thisoutbreak in
Hamburg and in other European countries[24]. The D4-Hamburg
outbreak demonstrates againthat strategies to raise measles
vaccination coverageshould be speciically devised to target
underservedpopulations. Furthermore, innovative outbreak
con-tainment measures and vaccination programmes areneeded. In a
review o the literature concerning theinteraction between Roma
communities and healthservice providers, Hajio and McKee came to
theconclusion that published research is sparse [25]. Wesuggest
that studies are needed to better understandthe view o Roma
community members towards thehealthcare sector in order to be able
to create vaccina-tion programmes that are acceptable to this
neglectedminority.
Acknowledgments
We would like to thank Jrg Thyro, Sabine Richtberg,Veronika
Hellmund, Susanne Steinberg rom the PublicHealth Department
Hamburg-Mitte and Katharina Traudt,Joachim Kanschik rom the Public
Health DepartmentHamburg-Harburg or outbreak investigations.
Furthermorewe would like to thank Markus Kirchner rom the
NLGA,Hannover, or inormation on measles outbreak in LowerSaxony.
Finally, we would like to thank Klaus Baumgardt
rom the Division or Environmental Monitoring, Hamburg,or
instruction on geographic inormation system sotware.Cartography was
based on standard maps rom the StateOice Geoinormation and Geodetic
Survey, Hamburg.
-
7/30/2019 Brote Sar Hamburgo Eurosurv 2012 Art20194
8/8
8 www.eurosurveillance.org
References
1. Fell G. Meldeplichtige Inektionskrankheiten in Hamburg2009.
Epidemiologischer Bericht. [Notiiable inectiousdiseases in Hamburg
2009. Epidemioloical report]. Hamburg:Institut r Hygiene und
Umwelt; Jul 2010. Available
rom:http://www.hamburg.de/contentblob/2463562/data/jahresbericht-2009-inektionsepidemiologie.pd
2. Mankertz A, Mihneva Z, Gold H, Baumgarte S, Baillot A,
HelbleR, et al. Spread o measles virus D4-Hamburg, Europe,
2008-2011. Emerg Inect Dis. 2011;17(8):1396-401.
3. Robert Koch Institute. Empehlungen der StndigenImpkommission
(STIKO) am Robert-Koch-Institut/ Stand:Juli 2011. [Recommendations
o the Standing Committee onVaccination (STIKO) at the Robert Koch
Institute: July 2011].Epidemiologisches Bulletin No 30; 1 Aug 2011.
Availablerom:
http://edoc.rki.de/documents/rki_v/rep5YpW0YJOrw/PDF/28CKjOWgLiRzg.pd
4. Robert Koch Institute. Empehlungen der StndigenImpkommission
(STIKO) am Robert-Koch-Institut/Stand:Juli 2010. [Recommendations o
the Standing Committee onVaccination (STIKO) at the Robert Koch
Institute: July 2010].Epidemiologisches Bulletin No 30; 2 Aug 2010.
Availablerom:
http://edoc.rki.de/documents/rki_v/reLMSiAJvAFI6/PDF/25vQaMWNX2EXrE.pd
5. Robert Koch Institute. nderung der Empehlung zur Impunggegen
Masern. [Change in the recommendation or vaccinationagainst measles
]. Epidemiologisches Bulletin No 32. 16 Aug2010. Available rom:
http://edoc.rki.de/documents/rki_v/
reJeAanavg8r/PDF/2392OVQG5cQlAA.pd6. World Health Organization
(WHO). Eliminating Measles and
Rubella. Framework or the Veriication Process in the WHOEuropean
Region. Copenhagen: WHO Regional Oice orEurope; 2012. Available
rom:
http://www.euro.who.int/__data/assets/pd_ile/0005/156776/E96153.PDF
7. Reiter S. Impquoten bei den Schuleingangsuntersuchungenin
Deutschland 2009. [Immunisation coverage at schoolentry
examinations in Germany 2009]. EpidemiologischesBulletin No 16; 26
Apr 2011. Available rom:
http://edoc.rki.de/documents/rki_v/rermiABI3LoaA/PDF/24hM4nPQ2U.pd
8. Btzing-Feigenbaum J, Pruckner U, Beyer A, Sinn G, DinterA,
Mankertz A, et al. Spotlight on measles 2010: Preliminaryreport o
an ongoing measles outbreak in a subpopulationwith low vaccination
coverage in Berlin, Germany, January-March 2010. Euro Surveill.
2010;15(13):pii=19527. Availablerom:
http://www.eurosurveillance.org/ViewArticle.
aspx?ArticleId=195279. Gold H. Zu einem Masernausbruch bei
Migranten in Mnchen.[On a measles outbreak among migrants in
Munich].Epidemiologisches Bulletin No 50; 20 Dec 2011.
Availablerom:
http://edoc.rki.de/documents/rki_v/reu8y56vT4KNk/PDF/22deQTGmzUXbY.pd
10. Hummel KB, Lowe L, Bellini WJ, Rota PA. Development
oquantitative gene-speciic real-time RT-PCR assays or thedetection
o measles virus in clinical specimens. J VirolMethods.
2006;132(1-2):166-73.
11. World Health Organization. New genotype o measles virusand
update on global distribution o measles genotypes. WklyEpidemiol
Rec. 2005;80(40):34751.
12. Salman R, Weyers S. Germany: MiMi Project - With Migrantsor
Migrants. In: Poverty and social exclusion in the WHOEuropean
Region: health systems respond. Koller T, editor.Copenhagen: WHO
Regional Oice or Europe; 2010. p. 52-63.Available rom:
http://www.euro.who.int/__data/assets/pd_ile/0006/115485/E94018.pd
13. Follin P, Dotevall L, Jertborn M, Khalid Y, Liljeqvist JA,
Muntz S,et al. Eective control measures limited measles outbreak
aterextensive nosocomial exposures in January-February 2008
inGothenburg, Sweden. Euro Surveill.
2008;13(30):pii=18937.Available rom:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18937
14. Botelho-Nevers E, Cassir N, Minodier P, Laporte R, GautretP,
Badiaga S, et al. Measles among healthcare workers:a potential or
nosocomial outbreaks. Euro Surveill.2011;16(2):pii=19764. Available
rom:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19764
15. Robert Koch Institute. Empehlungen der StndigenImpkommission
(STIKO) am Robert-Koch-Institut/Stand:Juli 2007. [Recommendations o
the Standing Committee onVaccination (STIKO) at the Robert Koch
Institute: July 2007].Epidemiologisches Bulletin No 30; 27 Jul
2007. Available
rom:
http://edoc.rki.de/documents/rki_v/re3BNEVpkzVE/PDF/27Rqk0xJi3JThw.pd
16. Voigt K, Khne F, Twork S, Gbel A, Kugler J, BergmannA.
[Current vaccination status o health-care personnel inBrandenburg,
Saxony And Saxony-Anhalt]. Gesundheitswesen.2008;70(7):408-14.
German.
17. Leuridan E, Hens N, Hutse V, Ieven M, Aerts M, Van Damme
P.Early waning o maternal measles antibodies in era o
measleselimination: longitudinal study. BMJ. 2010;340:c1626.
18. Leuridan E, Van Damme P. Passive transmission andpersistence
o naturally acquired or vaccine-induced maternalantibodies against
measles in newborns. Vaccine. 200721;25(34):6296-304.
19. Muscat M. Who gets measles in Europe? J Inect Dis.
2011;204Suppl 1:S353-365.
20. Feder GS, Vaclavik T, Streetly A. Traveller Gypsies
andchildhood immunization: a study in east London. Br J GenPract.
1993;43(372):281-4.
21. Kraigher A, Vidovic M, Kustec T, Skaza A. Vaccination
coveragein hard to reach Roma children in Slovenia. Coll
Antropol.2006;30(4):789-94.
22. Curtale F, Perrelli F, Mantovani J, Cioi degli Atti M, Filia
A,Nicoletti L, et al. Description o two measles outbreaks in
theLazio Region, Italy (2006-2007). Importance o pockets o
lowvaccine coverage in sustaining the inection. BMC Inect
Dis.2010;10:62.
23. Pervanidou D, Horeti E, Patrinos S, Lyt ras T,
TriantaillouE, Mentis A, et al. Spotlight on measles 2010:
ongoingmeasles outbreak in Greece, January-July 2010. EuroSurveill.
2010;15(30):pii=19629. Available rom:
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19629
24. European Centre or Disease Prevention and Control
(ECDC).Measles disproportionately aects Roma. European
monthlymeasles monitoring (EMMO). Issue 6. Stockholm: ECDC; Nov
2011 Available rom:
http://ecdc.europa.eu/en/publications/Publications/1112_European_monthly_measles_monitoring_Nov_2011.pd
25. Hajio S, McKee M. The health o the Roma people: a reviewo
the published literature. J Epidemiol Community
Health.2000;54(11):864-9.