Embed Size (px)
Citation preview

BRUCELLOSIS

MICROBIOLOGY
• 6 SPECIES, 4 CAN BE TRANSMITTED TO MAN.
• GRAM NEGATIVE, NON-MOTILE, NON-SPORE FORMING.
• THE ORGANISM IS FACULATIVE.• CULTURE CAN TAKE LONG TIME.• SURVIVAL CAN BE VERY LONG.• OPTIMUM TEMPERATRE IS 37 °C (20-
40 °C)

ANTIGEN STRUCTURE OF BRUCELLA
Outer Membrane
(OM)
(Cytoplasmic Membrane) NH = native hapten
Poly B = B poly-saccharide
OM = Phospholipides Lipopolysaccharides
Proteins = (outer membrane; proteins; OMP )

PMN T Suppresser
Ant. Pr. Cell
T. helper
B cell
Macrophage
Elimination
OR

AFTER ENTERING THE BODY Leukocyte
ORRegional Lymph node
OR Blood Stream
Liver Spleen Bone Marrow Lymph Node
OR
Microgranuloma Micro abscess formationOR OR
Blood Stream
BLOOD STREAM
BLOOD STREAM
BLOOD STREAM
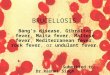
FREQUENCY OF COMMON SYMPTOMS IN STUDIES FROM SAUDI ARABIA
STUDYRMHAL-KUHER TEACHING HOSPITAL
KFNGH
SYPMTOMFREQUINCE OF SYMPTOM
FEVER100&90%56%
BODY ACHES100%N/D32%
LETHARGY100%N/D24%
BACK PAIN64%34%35%
JOINT PAIN64%34%21%
SWEATING56%33%27%
ANOREXIA33%17%28%
IRRITABILITY10%N/D7%
HEADACHE25%30%20%
WEIGHT LOSS26%N/D15%

CLINICAL FINDINGS
SPLENOMEGALLY29 %
JOINT TENDERNESS28 %
HEPATOMEGALLY20 %
SPINAL TENDERNESS13 %
SACRO ILEITIS13 %
LYMPHADENOPATHY10 %
IMPAIRED STRAIGHT LEG RAISING
6 %
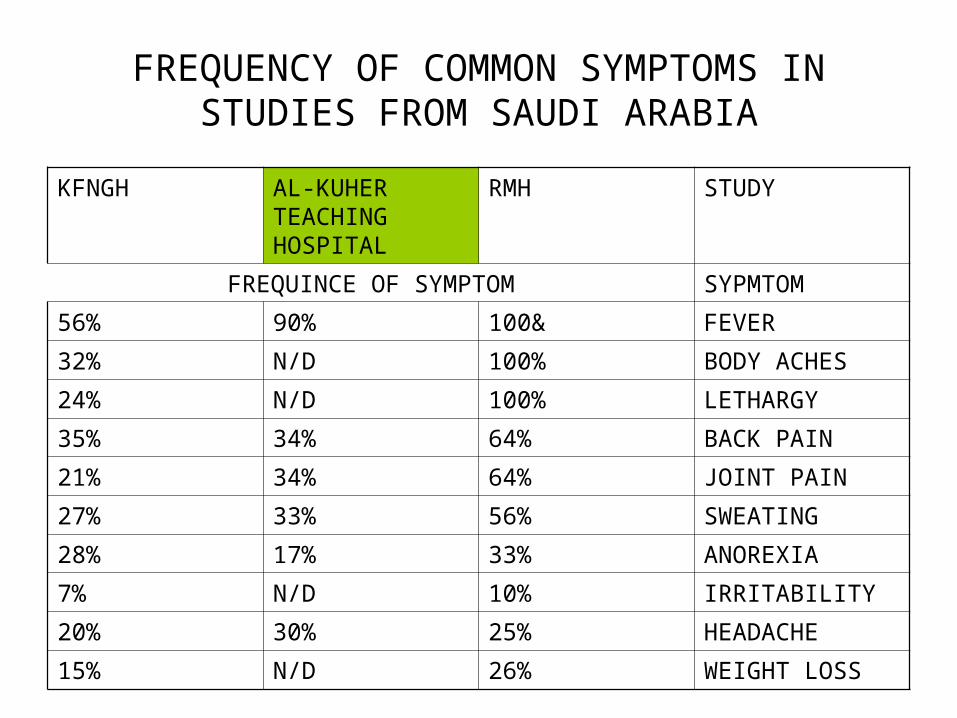
REGIONAL DISTRIBUTION OF SEROPOSITIVITY ACCORDING TO THE MICROPLATE AGGLUTINATION TEST
REGIONTOTAL SAMPLE
POSITIVEPERCENTAGE
EASTRERN2939119340.6
WESTERN7131383953.8
NORTHERN3152132041.9
SOUTHERN4794242150.5
CENTRAL5597271848.5
TOTAL236131149148.9

SEROLOGCAL TESTS
• STANDARD TUBE AGGLUTINATION TEST• MICROPLATE AGGLUTINATION TEST• 2-MERCAPTOETHANOL AGGLUTINATION
TEST• COOMBS TEST• COMPLEMENT FIXATION TEST• ROSE BENGAL TEST• ENZYME-LINKED IMMUNOSORBENT
ASSAY• GEL PRECIPITAITON TEST

POSITIVE BLOOD CULTURES FOR BRUCELLA
TIME IN WEEKSNUMBER OF POSITIVE CULTURES
12
25
34
41
91
101
TOTAL14

ACTIVE DISEASE
• Clinical evidence (symptoms & signs) of brucellosis plus:
Positivity at > 1:160 by STAT Positivity at > 1:140 by 2-ME test Positivity by ELISA (high IgG & low IgM)

TREATMENT FOR HUMAN BRUCELLOSIS
CategoryTreatmentDoseDuration
Bone & JointSTM +
Rif.
Doxy
1.0 g bid
900 mg/d
100 mg bid
3
12
12
Meningio-
Enceph.
Rif. +
TMP-SMZ
?Doxy
900 mg/d
300 mg(T)/kg-d
12
2
12
EndocarditisSTM +
Rif. +
TMP-SMZ+
Doxy
1.0 g bid
900 mg/d
30 mg(T) kg-d
100 mg bid
13
13
3
12

TREATMENT FOR HUMAN BRUCELLOSIS
CategoryTreatmentDoseDuration
Adult & children (>8 years)
Doxy + STM100 mg bid
1.0 g bid
6
2 – 3
Children
< 8 years
Rif + TMP – SMZ
15 g (kg-d)
30-60 mg (T*)/kg-d
2 or 8
3 or 8
Preg. Women
1st Trim.
2nd & 3rd Trim.
[Doxy +
[Rif. TMP-SMZ
100 mg bid
900 mg bid
6 w
3 w

COMPARATIVE STUDY OF 3 DRUGS REGIMENS
RegimenDrug(s)DoseDuration
(Days)
Cure Rate
AOral Rif. +
Doxycycline
900 mg/d
200 mg/d
45
45
95%
“
BStreptomycin
Doxycycline
1.0 g/d
200 mg/d
14
45
96%
“
CStreptomycin1.0 g/d1459%
(WHO)Tetracycline2.0 g/d2159%
(Accole et al. 1989)

PREVENTION
• “ELIMINATION OF THE DISEASE IN ANIMALS”• PERSONAL HYGIENE (WASHING EXPOSED
CLOTHES)• ENVIRONMENTAL SANITATION (DISPOSAL
OF CONTAMINATED SUBSTANCES)• PASTURIZATION OF DIARY PRODUCTS• HEALTH EDUCATION• IMMUNIZATION

VACCINES
• B. abortus strain 19
• B. melitensis strain Rev I
• B. suis strain 2s
• B. abortus strain 45/20
• B. melitensis strain H38

CLASSIFICATION OF SALMONELLA
• According to their ecologic niches
• Serotyping [kanfmann white]– O antigen A-I– H antigen (subtypes)
* Over 2000 serotypes

• Spectrum of clinical manifestations of salmonella
• Gastroenteritis
• Enteric fever
• Bacteremia– With metastatic disease– Without metastatic disease
• Asymptomatic carrier state

TYPHOID FEVER(Enteric Fever)
Definition:A disease characterized by prolonged fever, abdominal pain, diarrhea, delirium, rash (rose spots) & splenomegaly.
Etiology:Salmonella Typhi & paratyphi A & B-A motile gram-negative bacilli, which possess:
• H-Antigen (associated with flagella)• O-Antigen (a LPS associated with cell wall)• VI-Antigen (a PS associated with cell capsule)

EPIDEMIOLOGY OF TYPHOID FEVER
It affects all age groups. No sex difference. Common in developing countries. Infecting dose 7x10(6) in Africa, Asia & Latin
America. Transmission is through Oral-fecal route. Affected individuals may become asymptomatic
carriers particularly females & older males (Underlying cholecystitis).
S-Typhi is resistant to drying & cooling.

SYMPTOMS & SIGNS
SymptomsSignsPathology
1st wk.Fever, Chills headache
Abdominal tenderness
Bacteremia
2nd wk.Rash, abdominal pain,
Rose spotsMononuclear vasculitis of skin, hyperplasia of peyer’s batches typhoid nodules

SIGNS & SYMPTOMS(cont,)
______________________________________
Symptoms Signs Pathology
_____________________________________________________________
3rd wk Intestinal Melena Ulcerations, perforation
bleeding, per- rigid abdomen with peritonitis.
foration & shock ileus, coma
____________________________________________________________
4th week Resolution Recurrence Cholecystitis, chronic
& later relapse of acute fecal carriage of bacteria
weight loss disease,
cachexia.

ANTIBIOTIC USED FOR SALMONELLA TYPHI
- Chloramphenicol
- Ampicillin, Amoxil
- Co-trimoxazole
- 3rd generation cephalosporins
- Quinolones

PROGNOSIS
Case fatality dropped 12% to 4% It is still +\- 10% in developing countries Perforation +\- 5% Chronic fecal carriers 1-3%

VACCINATION FOR S.TYPHI
- Inactivated S.typhi:- 2 SC injections:- 55-88% protection for 3-5yr.
- Attenuated S.typhi:- Liquid 3 doses- Enteric coated capsules- Protection 60-70%
PREVENTION

PREVALENCE OF SCHISTOSOMIASIS AS REPORTED BY THE STATIONS
StationNo. of Persons Examined
Prevalence(%)
S.HaematobiumS.ManSoni
Ovwrall Prevalence
AL-Baha20.412---13.013.0
Jizan30.8837.01.28.2
Taif39.5990.27.77.9
Abha23.0131.74.96.6
Madinah17.5911.93.65.5
Bisha16.7660.48.58.9
Najran8.8201.69.911.5
Mahael5.7837.6---7.6
Hayil4.335---14.212.2
Riyadh15.129---5.65.6
Makah25.8942.53.05.5
Al-Jouf12.5771.31.62.9

KATAYAMA FEVER(KATAYAMA River, Japan)
1. SEVERAL DAYS – 2-3 WEEKS
2. FEVER, CHILLS, HEADACHE, MALAISE, EDEMA, CONFUSION
3. HEPATOSPLENOMEGALLY
4. LYMPHADENOPATHY
5. EOSINOPHILIA
6. CEREBRAL EDEMA (CT)

S. MANSONI (SYMPTOMS)
SYMPTOMCASES
Abdominal Pain258
Fatigue221
Blood in Stool205
Mucous in Stool191
Tenesmus121
Depression108
Diarrhea54
Constipation1

BOTH (MANSONI & Haema.)
SYMPTOMS
Haematuria11
Abdominal Pain7
Tiredness7
Frequency6
Depression4
Tenesmus4
Blood in Stool3
Mucous in Stool3

SIDE EFFECTS OF ANTISCHISTOSOMAL DRUGS (%)
SYMPTOMSPRAZIQUANTELOXAMNIQUINEMETRIFONATE
NONE563040
DIZZINESS203610
ABDOMINAL PAIN
122512
JOINT PAIN101210
NAUSIA8106
RASH642
VOMITING6108
ITCHING610-
FATIGUE2128
HAIRFALL2--
CHANGE IN TASTE
122
DIARRHEA124
CONVULSION-1-

S. HAEMATOBIUM
SYMPTOMS
Haematuria89
Dysuria77
Abdominal Pain43
Frequency40
Tiredness33
Blood in Stool23
Mucous in Stool22
Depression8

PREVALENCE OF SCHISTOSOMIASIS AS REPORTED BY THE STATION*
/PREVALENCE (%)
STATIONNo. of Persons Examined
S. Haematobium
S. MansoniOverall Prevallence +
AL-BAHA20.412---13.013.0
JIZAN30.8837.01.28.2
TAIF39.5990.27.77.9
ABHA23.0131.74.96.6
MADINAH17.5911.93.65.5
BISHA16.7660.48.58.9
NAJRAN8.8201.69.911.5
MAHAEL5.7837.6---7.6
HAYIL4.335---14.212.2
RIYADH15.129---5.65.6
MAKAH25.8942.53.05.5
AL-JOUF12.5771.31.62.9•MODIFIED FROM ARFAA.
+ Appropriate, Since a small percentage has double Infection.

An Immunoblotting Study of Serologic Response in Patients with Acute Brucellosis
- Specific & Sensitive only in patients with Chronic Brucellosis
Leiva-Leon et al,. 1991
Diagon. Microbiol. Inf. Dis

DITRIBUTUTION OF BRUCELLA BY LEVEL OF EDUCATION
Level of Education
TotalPositive(%)Odds Ratio
Higher11622(0.2)1.0
Secondary249822(0.9)5.1
Primary468434(0.7)4.2
Read & Write
437779(1.8)10.7
Illiterate9723271(2.9)16.6 There is an Inverse relationship between the rate of positivity & the level of education

MEAN BRUCELLA TITERS/INITIAL4 WEEKS8 WEEKS
ABORTUS2560
(N-98)
1280
(N-56)
640
(N-25)
MELITENSIS1280
(N-82)
640
(N-53)
640
(N-21)

DISTRIBUTION OF BRUCELLA ACCORDING TO THE TYPE OF HOUSING
Type of Housing
TotalPositive(%)Odds Ratio
Palace/ Villa
7209122(1.7)1.0
Flat/ Small House
12442144(1.2)0.7
Low grade Housing*
3510146(4.2)2.5
*The rate of Positivity is Significantly Higher

BRUCELLOSIS IN THE KINGDOM OF SAUDI ARABIA
/NegativePositiveTotalRelative Risk
-95%CI
MILKING ANIMALS
(Significant)
Yes226015724175.5(4.4,6.7)
No2024125720498
1.0
No Data
6962

Modulation of the Intracellular Survival of B. abortus by Tufsin & Muramyl dipeptide
• Tufsin (T), physiologically bioactive peptide (animal origin).
• Muramyl dipeptide (MD). Synthetic bioactive glyco-peptide (microbial Origin)
• T & MD both enhance Ø Functions & increase non specific resistance against various pathogens.
• Addition of MD significantly (P<0.03) enhanced macrophage (Ø) to control intracellular replication of B. abortus.
• Cause conversion of permissive macrophage to restrictive macrophage.
• No additive effect of T & MD Together.
Price et al,.1993
Vet. Immunol Imuno Pathol.

Specific Antibody Profile in Human Brucellosis
• Comparison of STAT,MAT,RB & Coomb’s tests with Elisa I 761 Sera of patients.
• ELISA found to be more specific & sensitive (OM; or NH antigens)
• Chronic Brucellosis IgG persists.
• Relapsing brucellosis IgG peaks up
Ariza J et al, 1992
Clin. Infect. Dis.

Prevelance of Brucellosis in Al-Qaseem Area
Tube Agg. B. abortusNo.%
40402.6
801231.5
160660.8
320253200.3
640160.2
128060.1
256060.1
>512020.01
Negative766494.4%
Total8120
Active Dis.1.51%
Al-Balla S.R. Unpublished data

Antibody Prevalence of B. Abortus in Al-Qaseem Area
Micro. B. AbortusNo.%
101561.9
206307.8
407379.1
805817.1
1604295.3
3202903.6
6401511.9
1280630.8
2560410.5
5210210.3
1024070.1
>10240180.2
Negative500261.6

Immunotherapy in Chronic Brucellosis-Effect of Levamisole & Interferon
A. Interferon Alpha 2B
B.Levamisole
C.Conventional therapy
- A & B gave Quick Response + Quick Eradication of the organism
- A + B no Additive Effects
Printzis S et al,. 1994
Immunopharmacol – Immunotoxicol.

THE IMMUNE RESPONSE MAGNITUDE & DURATION IS AFFECTED BY:
1. Virulence of infecting strain
2. Size of inoculum
3. Age
4. Immune status

VACCINES FOR USE IN MAN
Live Vaccines
[USSR (Exposed Worker)]
• B. abortus 19-BA
• Intradermal injection, scarification
• Dose10(9) cells
• Repeated after 9-10 months if skin test and serologic are negative

VACCINES FOR USE IN MAN
Contd…
Live Vaccine Man
• China
• 104 M B. abortus
• Dose 7-10 x 10 cells (Scarifying)
S. PATHOGENESIS
- ID 10ˆ6 – 10ˆ9
- Penetration of the distal ileum mucosa
- Multiplication in the payer patches
- Diarrhea is caused by: - Prostaglandin Induced ˆ (c-AMP)
a. Local Inflammatory response
b. S. enterotoxin

SYMPTOMS & SIGNS

PREVENTION

ANTI-R IMMUNOGLOBULIN ISOTYPES
• IgM - early & the only Ig in a few days• IgG – later predominant• IgM + IgG = SAT – IgG = CF, 2 ME• Nonagglut. IgA = Coombs/ELISSA,
radioimmunoassay• IgE appear after IgM ad before IgG

BRUCELLOSIS & OTHER RISK FACTORS
Risk factorOdds ratioP value
Caring for delivering animal20.40.00001
Placental membrane12.90.00001
Consumption of raw milk products
4.20.001
EARLY LESION
Process starts ios Superior end-plate Erosion & sclerosis (bone repairs) may
simultaneously occur Sclerosis may extend further (Parrot
beak)

BRUCELLOSIS IN THE KINGDOM OF SAUDI ARABIA
NegativePositiveTotalRelative Risk95%CI
Breed Internally
(Significant)
YES
NO
No data
2944
19532
721
186
228
2
3130
19760
5.4
1.0
4.4,6.6)

●Leukocyte










![Review on Bovine, Small ruminant and Human Brucellosis in ... · intracellular, coccobacilli, non-motile and non- spore-forming bacteria [45]. Currently, there are eleven species](https://img.pdfslide.net/doc/110x75/5f04af767e708231d40f32b2/review-on-bovine-small-ruminant-and-human-brucellosis-in-intracellular-coccobacilli.jpg)