Embed Size (px)
Citation preview
3M Health Care AcademySM
BSI: Addressing Clinical Challenges with Catheter Maintenance
March 15, 2018
Marc J. Molitor, MSN. RN. VA-BC, CIC
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 2
Disclosure
• Marc J. Molitor, MSN, RN, VA-BC, CIC
o Employed by 3M as a Clinical Specialist
• Presentation will mention brands as this is how it was presented in the literature

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 3
3M Health Care AcademySM
Learning Objectives
1. Identify sources of contamination that can lead to
bloodstream infection (BSI)
2. Describe recommended practices and evidence based
interventions for catheter maintenance to reduce BSI risk
3. Discuss clinical challenges associated with catheter
maintenance that can impact outcomes
4. Identify solutions to address these challenges and clinical
studies that support these solutions
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 4
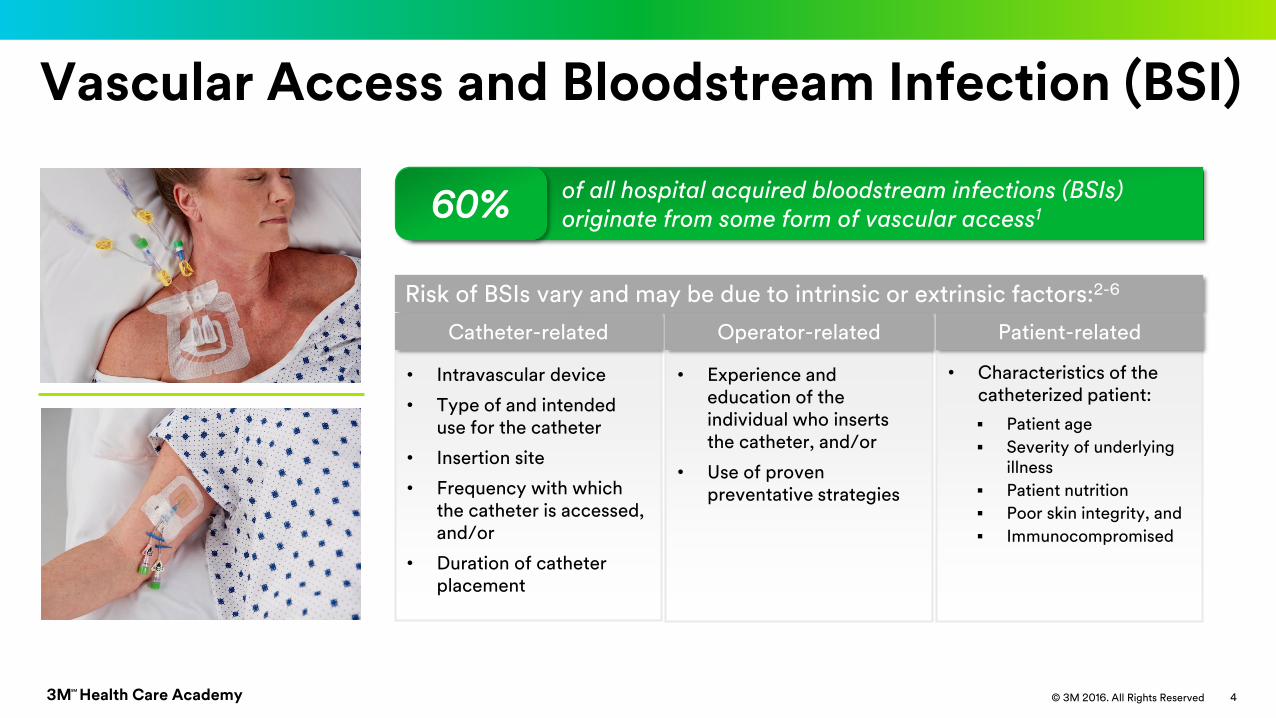
Vascular Access and Bloodstream Infection (BSI)
• Intravascular device
• Type of and intended use for the catheter
• Insertion site
• Frequency with which the catheter is accessed, and/or
• Duration of catheter placement
Risk of BSIs vary and may be due to intrinsic or extrinsic factors:2-6
• Experience and education of the individual who inserts the catheter, and/or
• Use of proven preventative strategies
• Characteristics of the catheterized patient:
▪ Patient age
▪ Severity of underlying illness
▪ Patient nutrition
▪ Poor skin integrity, and
▪ Immunocompromised
Catheter-related Operator-related Patient-related
of all hospital acquired bloodstream infections (BSIs) originate from some form of vascular access160%
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 5
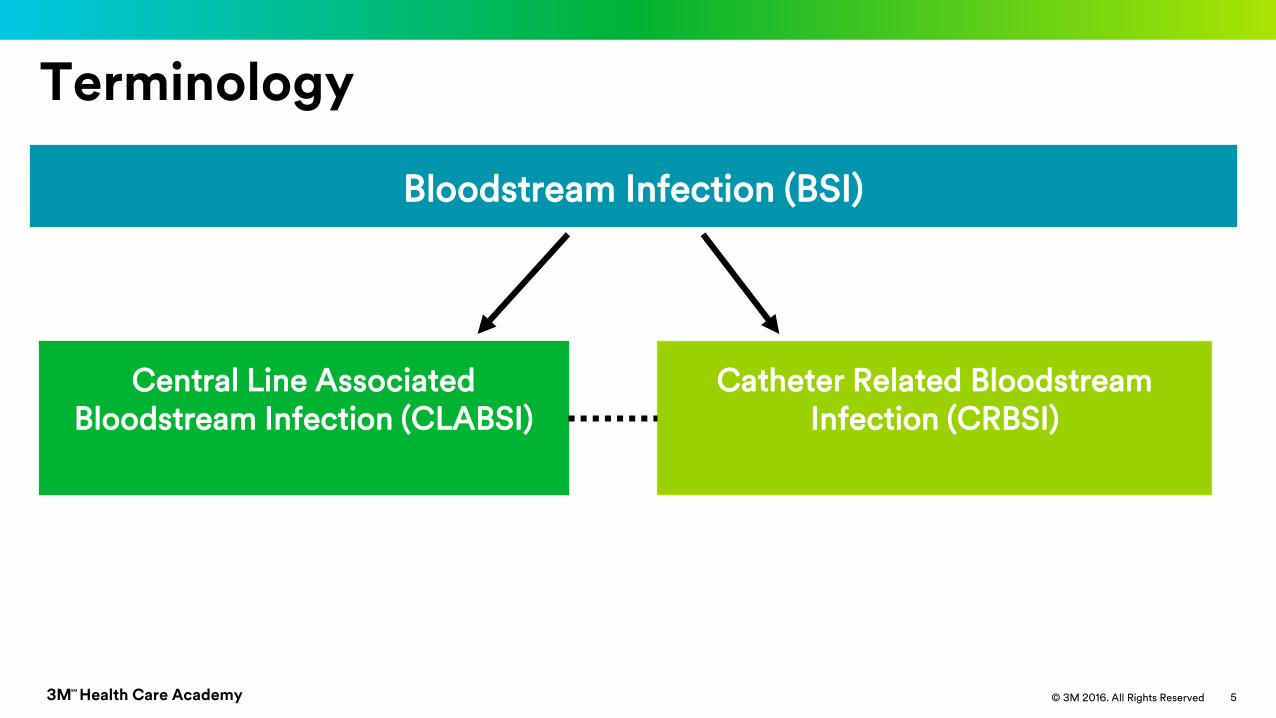
Terminology
Central Line Associated Bloodstream Infection (CLABSI)
Bloodstream Infection (BSI)
Catheter Related Bloodstream Infection (CRBSI)
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 6
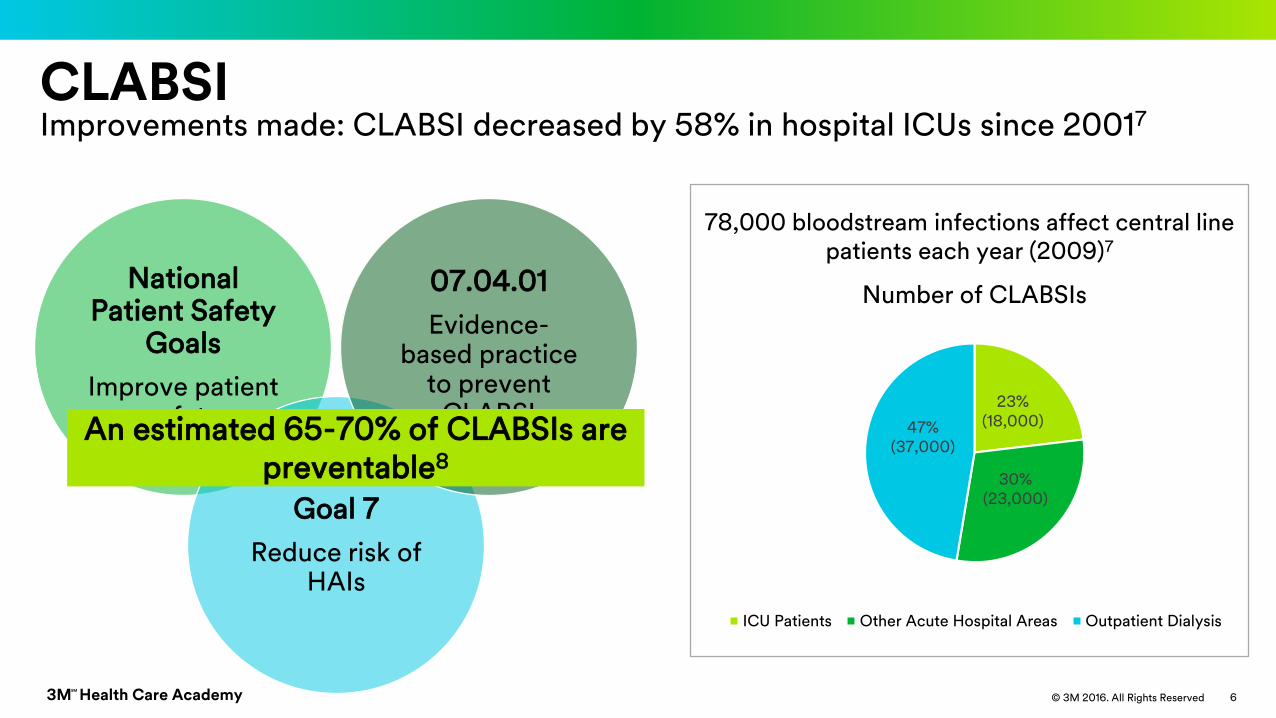
CLABSIImprovements made: CLABSI decreased by 58% in hospital ICUs since 20017
23%(18,000)
30%(23,000)
47%(37,000)
Number of CLABSIs
ICU Patients Other Acute Hospital Areas Outpatient Dialysis
78,000 bloodstream infections affect central line patients each year (2009)7
National Patient Safety
Goals
Improve patient safety
Goal 7
Reduce risk of HAIs
07.04.01
Evidence-based practice
to prevent CLABSI
An estimated 65-70% of CLABSIs are preventable8
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 7
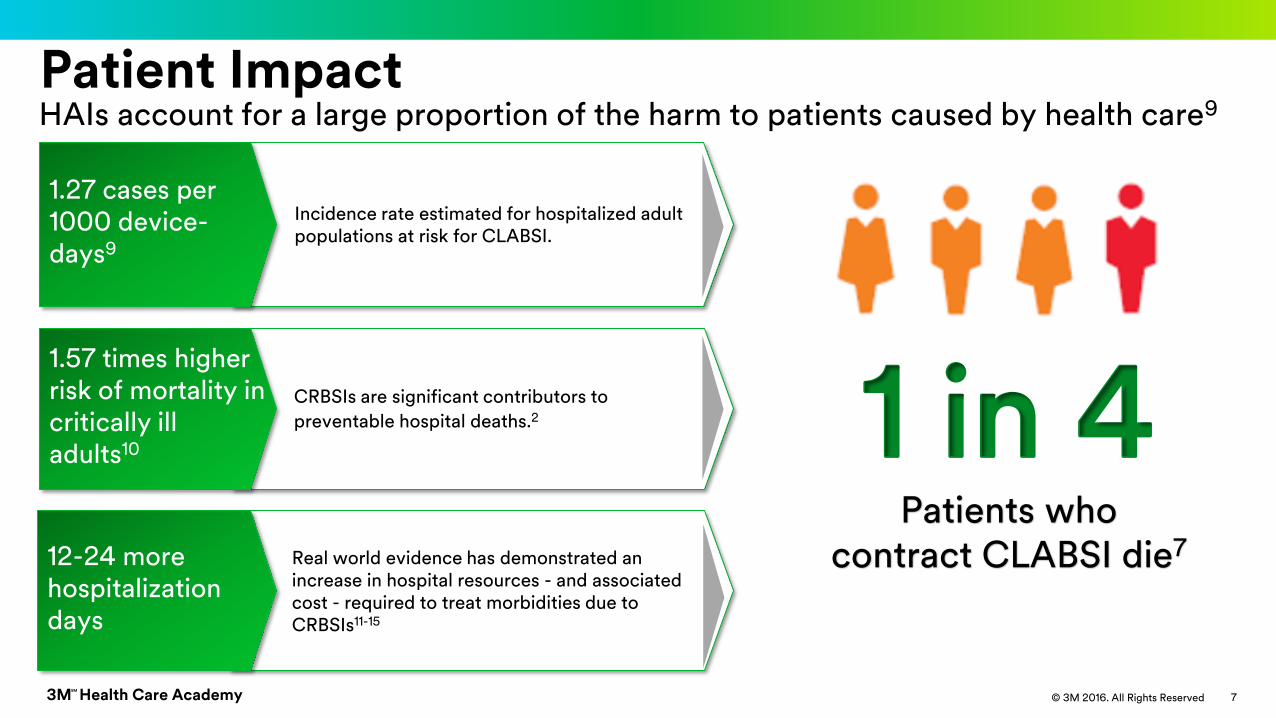
Patient ImpactHAIs account for a large proportion of the harm to patients caused by health care9
CRBSIs are significant contributors to
preventable hospital deaths.2
Incidence rate estimated for hospitalized adult populations at risk for CLABSI.
1 in 4Patients who
contract CLABSI die7
1.57 times higher risk of mortality in critically ill adults10
1.27 cases per 1000 device-days9
Real world evidence has demonstrated an increase in hospital resources - and associated cost - required to treat morbidities due to CRBSIs11-15
12-24 more hospitalization days
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 8
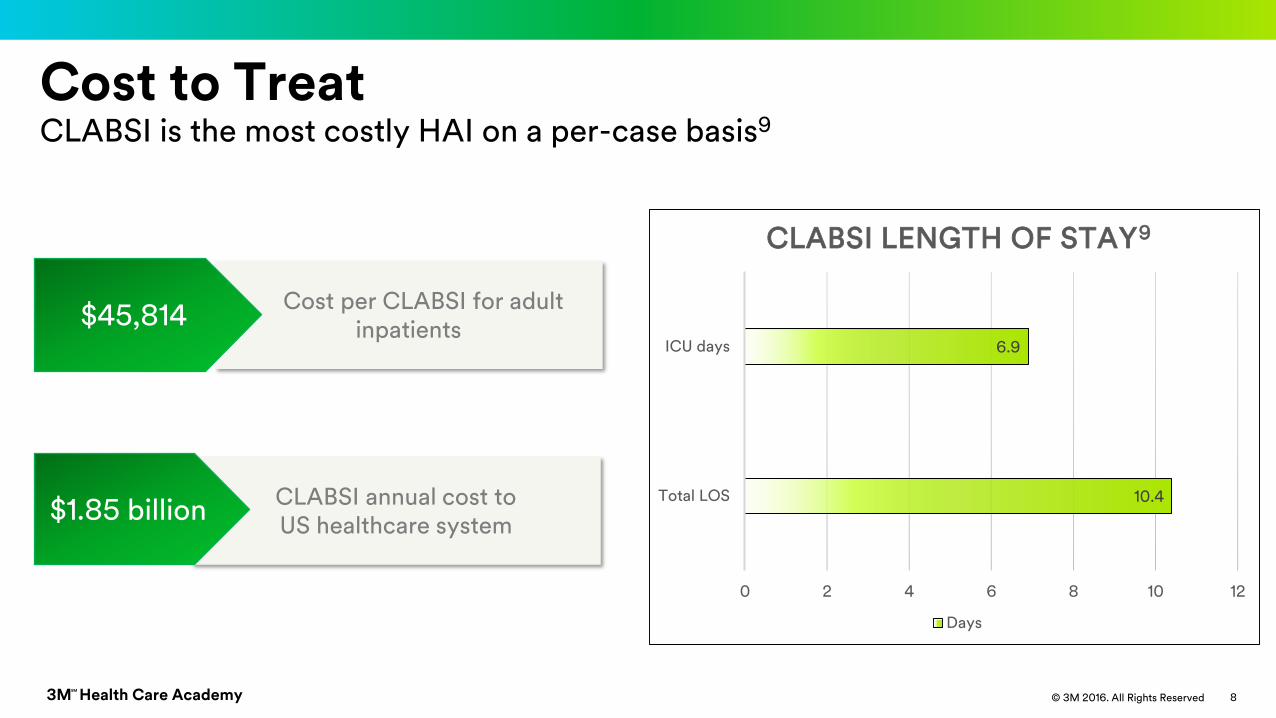
Cost per CLABSI for adult inpatients
Cost to Treat CLABSI is the most costly HAI on a per-case basis9
CLABSI annual cost to US healthcare system
$1.85 billion10.4
6.9
0 2 4 6 8 10 12
Total LOS
ICU days
CLABSI LENGTH OF STAY9
Days
$45,814
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 9
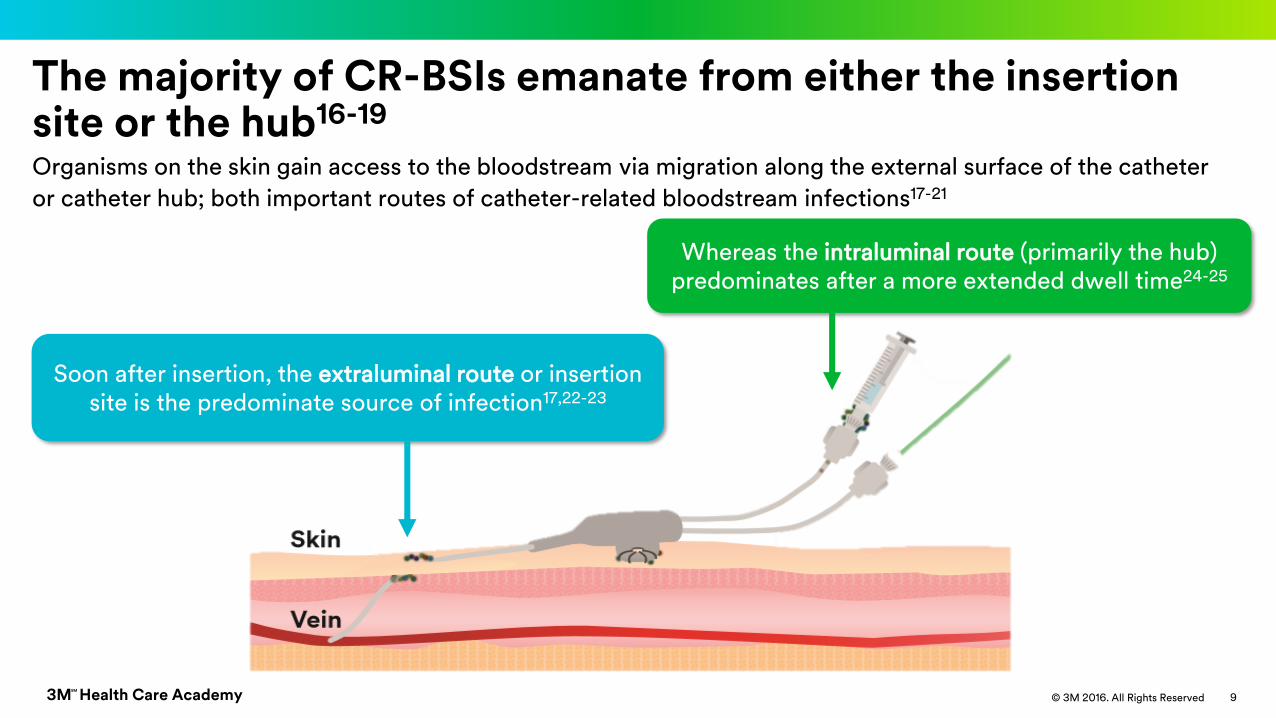
The majority of CR-BSIs emanate from either the insertion site or the hub16-19
Organisms on the skin gain access to the bloodstream via migration along the external surface of the catheter
or catheter hub; both important routes of catheter-related bloodstream infections17-21
Whereas the intraluminal route (primarily the hub) predominates after a more extended dwell time24-25
Soon after insertion, the extraluminal route or insertion site is the predominate source of infection17,22-23
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 10
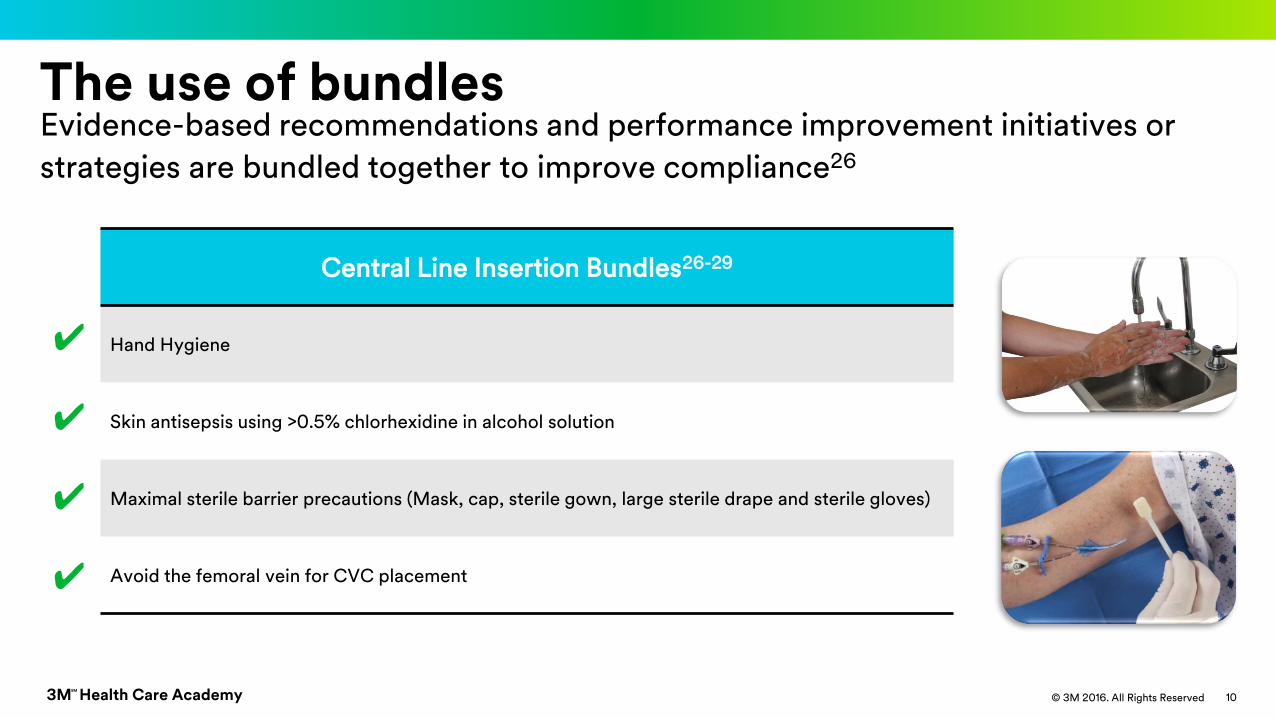
The use of bundlesEvidence-based recommendations and performance improvement initiatives or
strategies are bundled together to improve compliance26
Central Line Insertion Bundles26-29
Hand Hygiene
Skin antisepsis using >0.5% chlorhexidine in alcohol solution
Maximal sterile barrier precautions (Mask, cap, sterile gown, large sterile drape and sterile gloves)
Avoid the femoral vein for CVC placement
✔
✔
✔
✔
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 11
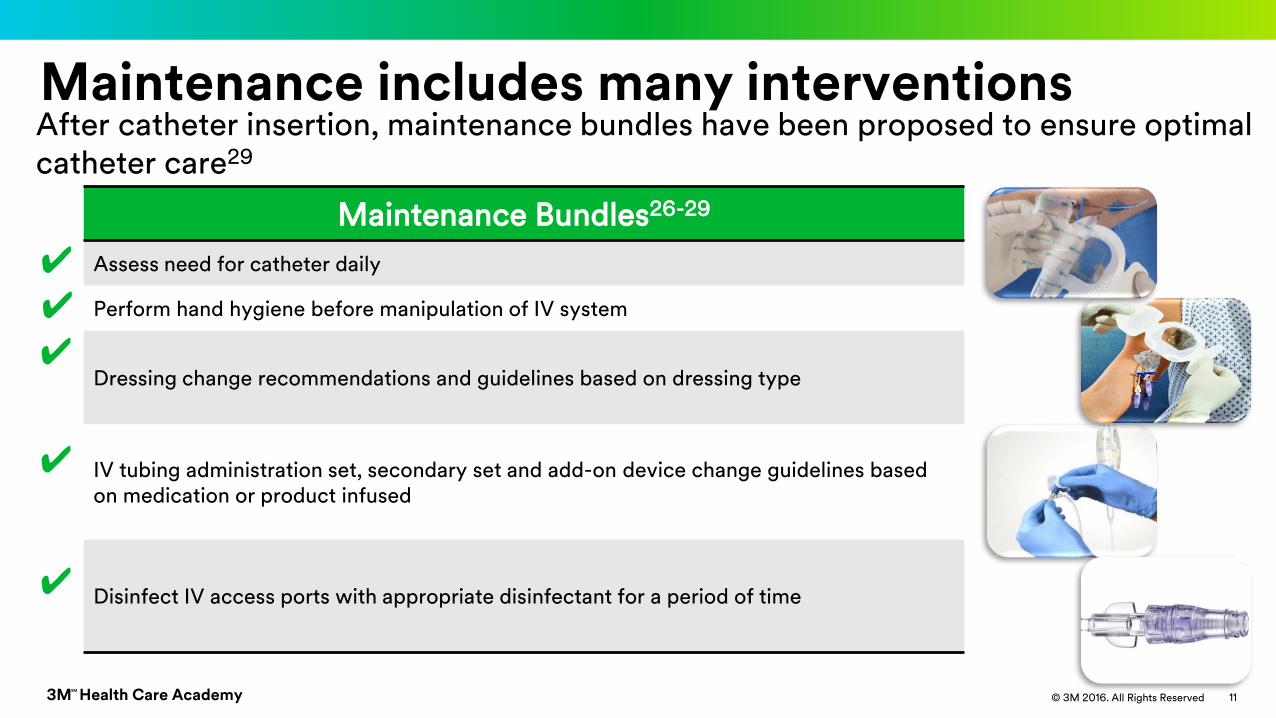
Maintenance includes many interventions
✔✔
✔
✔
✔
Maintenance Bundles26-29
Assess need for catheter daily
Perform hand hygiene before manipulation of IV system
Dressing change recommendations and guidelines based on dressing type
IV tubing administration set, secondary set and add-on device change guidelines based on medication or product infused
Disinfect IV access ports with appropriate disinfectant for a period of time
After catheter insertion, maintenance bundles have been proposed to ensure optimal catheter care29
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 12
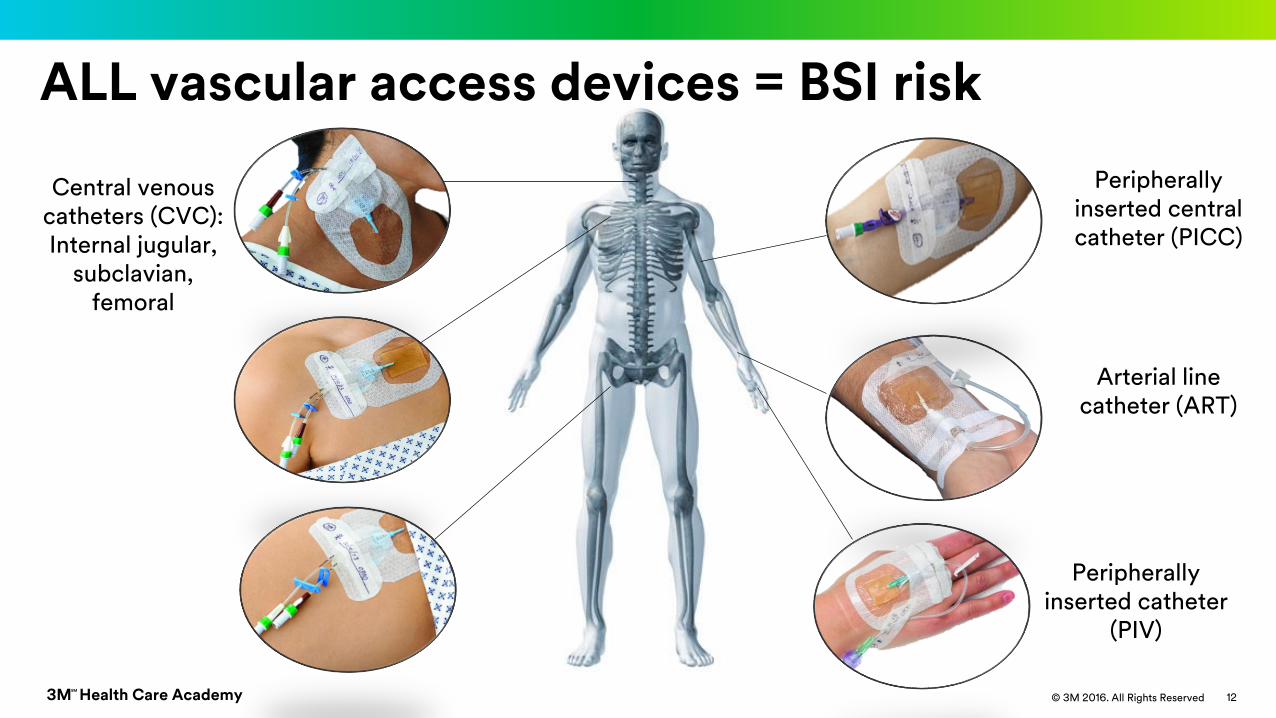
ALL vascular access devices = BSI risk
Peripherally inserted central catheter (PICC)
Arterial line catheter (ART)
Central venous catheters (CVC):Internal jugular,
subclavian, femoral
Peripherally inserted catheter
(PIV)
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 13
References1. Scheithauer S, Lewalter K, Schröder J, Koch A, Häfner H, Krizanovic V, Nowicki K, Hilgers RD, Lemmen SW. Reduction of central venous line-associated bloodstream infection rates by using a
chlorhexidine-containing dressing. Infection. 2014; 42(1): 155-159.
2. Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc.
2006; 81(9): 1159-1171.
3. O'Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter–related infections. Clin Infect Dis. 2002; 35(11): 1281-1307.
4. Safdar N, Mermel LA, Maki DG. The epidemiology of catheter-related infection in the critically ill. In: O’Grady NP, Pittet D, eds. Catheter-Related Infections in the Critically Ill. New York, NY:
Kluwer Academic; 2004: 1-22.
5. Karchmer TB, Cook E, Palavecino E, Ohl C, Sherertz R. Needleless valve ports may be associated with a high rate of catheter-related bloodstream infection. In: Program and abstracts of the
15th Annual Scientific Meeting of the Society for Healthcare Epidemiologists of America. April 9, 2005.
6. Jarvis WR, Murphy C, Hall KK, Fogle PJ, Karchmer TB, Harrington G, Salgado C, Giannetta ET, Cameron C, Sherertz RJ. Health care-associated bloodstream infections associated with
negative-or positive-pressure or displacement mechanical valve needleless connectors. Clin Infect Dis. 2009; 49(12): 1821-1827.
7. CDC Vitalsigns making health care safer: Reducing bloodstream infections. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/vitalsigns/pdf/2011-03-vitalsigns.pdf
Published March, 2011. Accessed June 18, 2017.
8. Septimus EJ, Moody J. Prevention of device-related healthcare-associated infections [version 1; referees: 2 approved]. F1000Research. 2016; 5(F1000 Faculty Rev):65. doi:
10.12688/f1000research.7493.1
9. Zimlichman E, Henderson D, Tamir O, et al. Health care-associated infections: A meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med. 2013;1 73(22):
2039-2046.
10. Siempos II, Kopterides P, Tsangaris I, Dimopoulou I, Armaganidis AE. Impact of catheter-related bloodstream infections on the mortality of critically ill patients: A meta-analysis*. Crit Care
Med. 2009; 37(7): 2283-2289.
11. Blot SI, Depuydt P, Annemans L, Benoit D, Hoste E, De Waele JJ, Decruyenaere J, Vogelaers D, Colardyn F, Vandewoude KH. Clinical and economic outcomes in critically ill patients with
nosocomial catheter-related bloodstream infections. Clin Infect Dis. 2005; 41(11): 1591-1598.
12. Renaud B, Brun-Buisson C. Outcomes of primary and catheter-related bacteremia: a cohort and case-control study in critically ill patients. Am J Respir Crit Care Med. 2001; 163: 1584–1590.
13. Dimick JB, Pelz RK, Consunji R, Swoboda SM, Hendrix CW, Lipsett PA. Increased resource use associated with catheter-related bloodstream infection in the surgical intensive care unit. Arch
Surg. 2001; 136: 229–234.
14. Warren DK, Quadir WW, Hollenbeak CS, Elward AM, Cox MJ, Fraser VJ. Attributable cost of catheter-associated bloodstream infections among intensive care patients in a nonteaching
hospital. Crit Care Med. 2006; 34: 2084–2089.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 14
References cont.
15. Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1994; 271: 1598–1601.
16. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of
America. Clin Infect Dis. 2009; 49(1): 1-45.
17. Safdar N, Maki DG. The pathogenesis of catheter-related bloodstream infection with noncuffed short-term central venous catheters. Intensive Care Med. 2004; 30(1): 62-67.
18. Mermel LA. What is the predominant source of intravascular catheter infections? Clin Infect Dis. 2011; 52(2): 211-212.
19. Maki DG, Stolz SM, Wheeler S, Mermel LA. Prevention of central venous catheter-related bloodstream infection by use of an antiseptic-impregnated catheter: A randomized, controlled trial.
Ann Intern Med. 1997; 127(4): 257-266.
20. Douard MC, Clementi E, Arlet G, et al. Negative catheter-tip culture and diagnosis of catheter-related bacteremia. Nutrition. 1994; 10(5): 397-404.
21. Dittmer ID, Sharp D, McNulty CA, Williams AJ, Banks RA. A prospective study of central venous hemodialysis catheter colonization and peripheral bacteremia. Clin Nephrol. 1999; 51(1): 34-39.
22. Mermel LA, McCormick RD, Springman SR, Maki DG. The pathogenesis and epidemiology of catheter related infection with pulmonary artery Swan-Ganz catheters: A prospective study
utilizing molecular subtyping. Am J Med. 1991; 91(36):197S–205S.
23. Maki DG, Weise CE, Sarafin HW. A semiquantitative culture method for identifying intravenous-catheter-related infection. N Engl J Med. 1977; 296(23): 1305-1309.
24. Segura M, Lladó L, Guirao X, Piracés M, Herms R, Alia C, Sitges-Serra A. A prospective study of a new protocol for ‘in situ’diagnosis of central venous catheter related bacteraemia. Clin Nutr.
1993; 12(2): 103-107.
25. Raad I, Costerton W, Sabharwal U, Sadlowski M, Anaissie E, Bodey GP. Ultrastructural analysis of indwelling vascular catheters: a quantitative relationship between luminal colonization and
duration of placement. J Infect Dis. 1993; 168(2): 400-407.
26. O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011; 52(9): e162-e193.
27. The Joint Commission. Preventing central line–associated bloodstream infections: A global challenge, a global perspective. Oak Brook, IL: Joint Commission Resources; Mat 12, 2012.
https://www.jointcommission.org/assets/1/18/CLABSI_Monograph.pdf
28. Gorski L, Hadaway L, Hagle ME, McGoldrick M, Orr M, Doellman D. Infusion Therapy Standards of Practice. J Infus Nurs. 2016; 39(suppl 1): S1-S59.
29. Marschall J, Mermel LA, Fakih M, et al. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014; 35(7):
753-771.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
15
Extraluminal Contamination
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 16
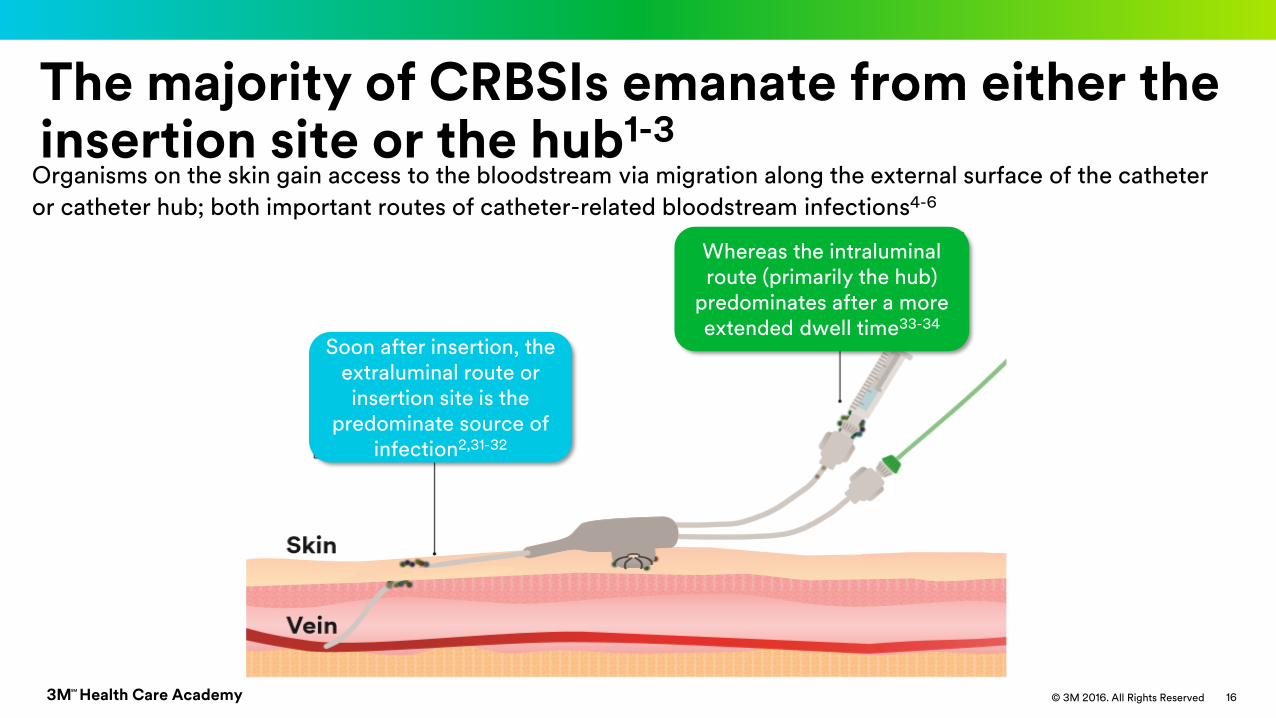
The majority of CRBSIs emanate from either the insertion site or the hub1-3
Organisms on the skin gain access to the bloodstream via migration along the external surface of the catheter
or catheter hub; both important routes of catheter-related bloodstream infections4-6
Soon after insertion, the extraluminal route or insertion site is the
predominate source of infection2,31-32
Whereas the intraluminal route (primarily the hub)
predominates after a more extended dwell time33-34
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
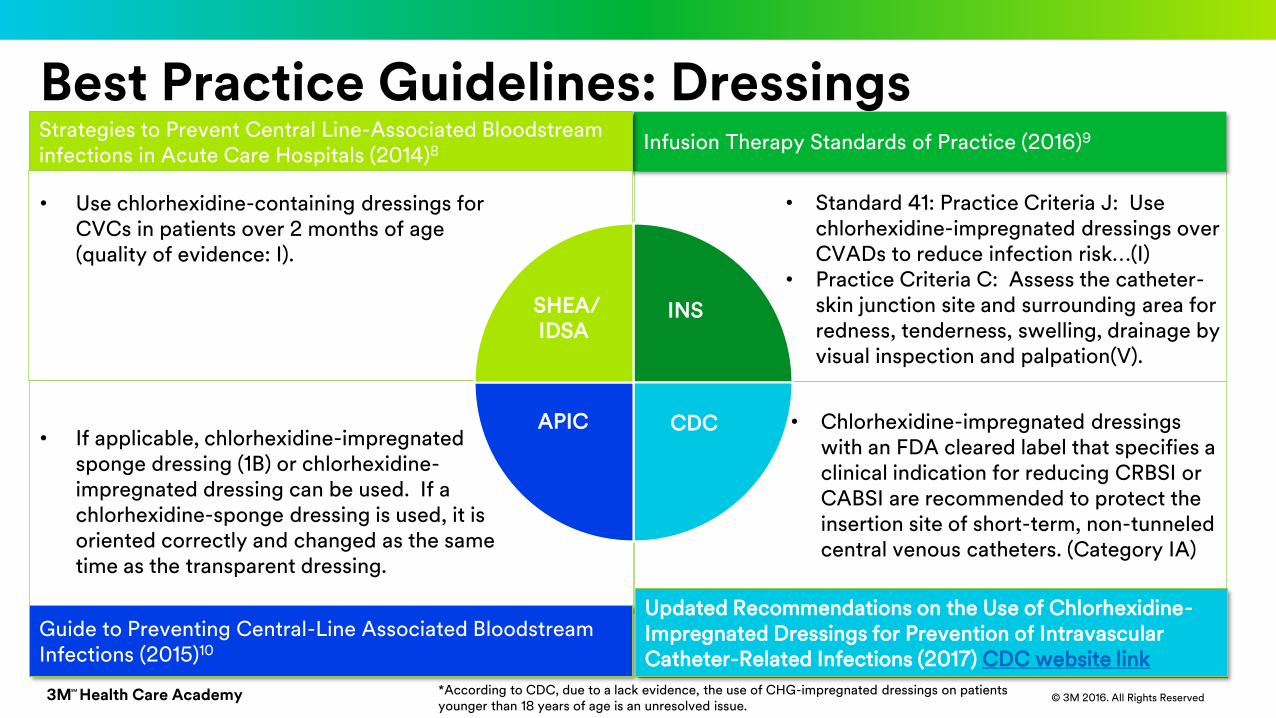
Infusion Therapy Standards of Practice (2016)9Strategies to Prevent Central Line-Associated Bloodstream infections in Acute Care Hospitals (2014)8
Guide to Preventing Central-Line Associated Bloodstream Infections (2015)10
Best Practice Guidelines: Dressings
Updated Recommendations on the Use of Chlorhexidine-Impregnated Dressings for Prevention of Intravascular Catheter-Related Infections (2017) CDC website link
SHEA/IDSA
APIC CDC
INS
• Standard 41: Practice Criteria J: Use chlorhexidine-impregnated dressings over CVADs to reduce infection risk…(I)
• Practice Criteria C: Assess the catheter-skin junction site and surrounding area for redness, tenderness, swelling, drainage by visual inspection and palpation(V).
• Chlorhexidine-impregnated dressings with an FDA cleared label that specifies a clinical indication for reducing CRBSI or CABSI are recommended to protect the insertion site of short-term, non-tunneled central venous catheters. (Category IA)
• Use chlorhexidine-containing dressings for CVCs in patients over 2 months of age (quality of evidence: I).
• If applicable, chlorhexidine-impregnated sponge dressing (1B) or chlorhexidine-impregnated dressing can be used. If a chlorhexidine-sponge dressing is used, it is oriented correctly and changed as the same time as the transparent dressing.
*According to CDC, due to a lack evidence, the use of CHG-impregnated dressings on patients younger than 18 years of age is an unresolved issue.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 18
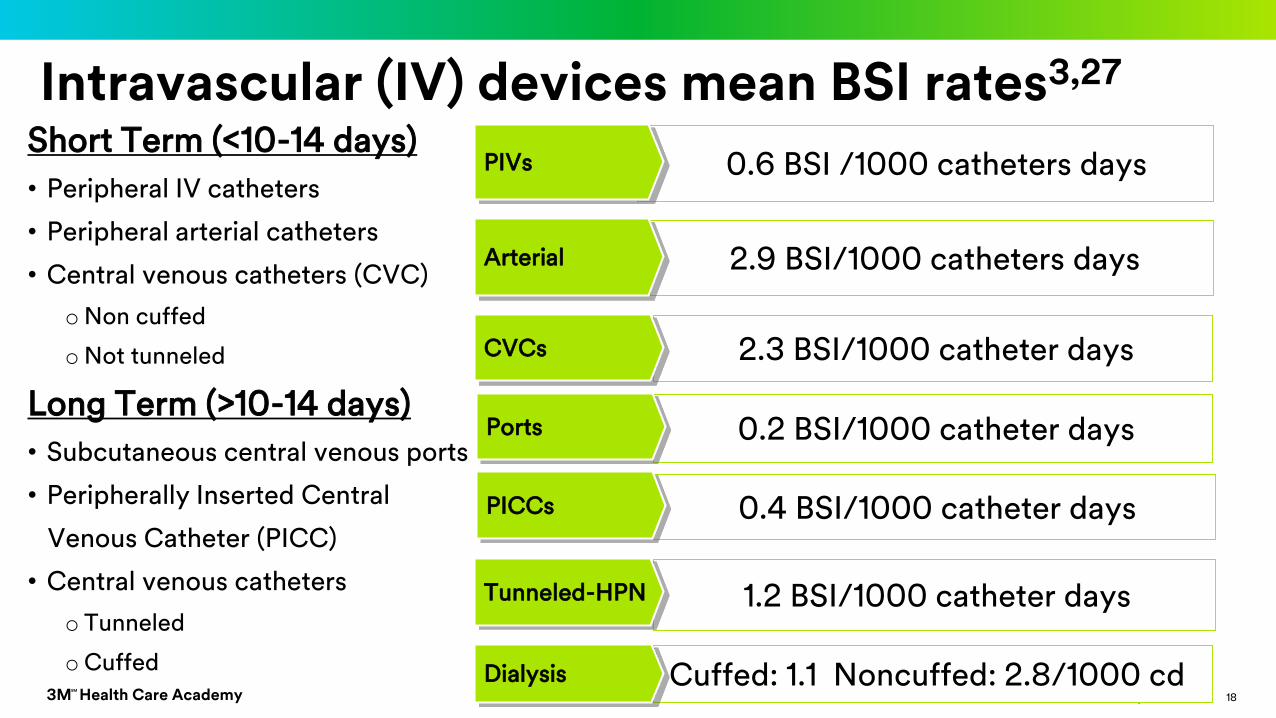
Intravascular (IV) devices mean BSI rates3,27
Short Term (<10-14 days)
• Peripheral IV catheters
• Peripheral arterial catheters
• Central venous catheters (CVC)
oNon cuffed
oNot tunneled
Long Term (>10-14 days)
• Subcutaneous central venous ports
• Peripherally Inserted Central
Venous Catheter (PICC)
• Central venous catheters
o Tunneled
oCuffed
0.6 BSI /1000 catheters days PIVs
2.9 BSI/1000 catheters days
0.2 BSI/1000 catheter days
1.2 BSI/1000 catheter days
Cuffed: 1.1 Noncuffed: 2.8/1000 cd
0.4 BSI/1000 catheter days
2.3 BSI/1000 catheter days
Arterial
CVCs
Ports
PICCs
Tunneled-HPN
Dialysis
3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
19
Beyond the guidelines: Clinical considerations for VAD site maintenance

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 20
Maintenance is for the life of the line
Insertion- the procedure represents only one aspect of the risk for CRBSI8
Maintenance- the risk of CRBSI extends to all aspects of nursing care and maintenance during the CVC dwell time8
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 21
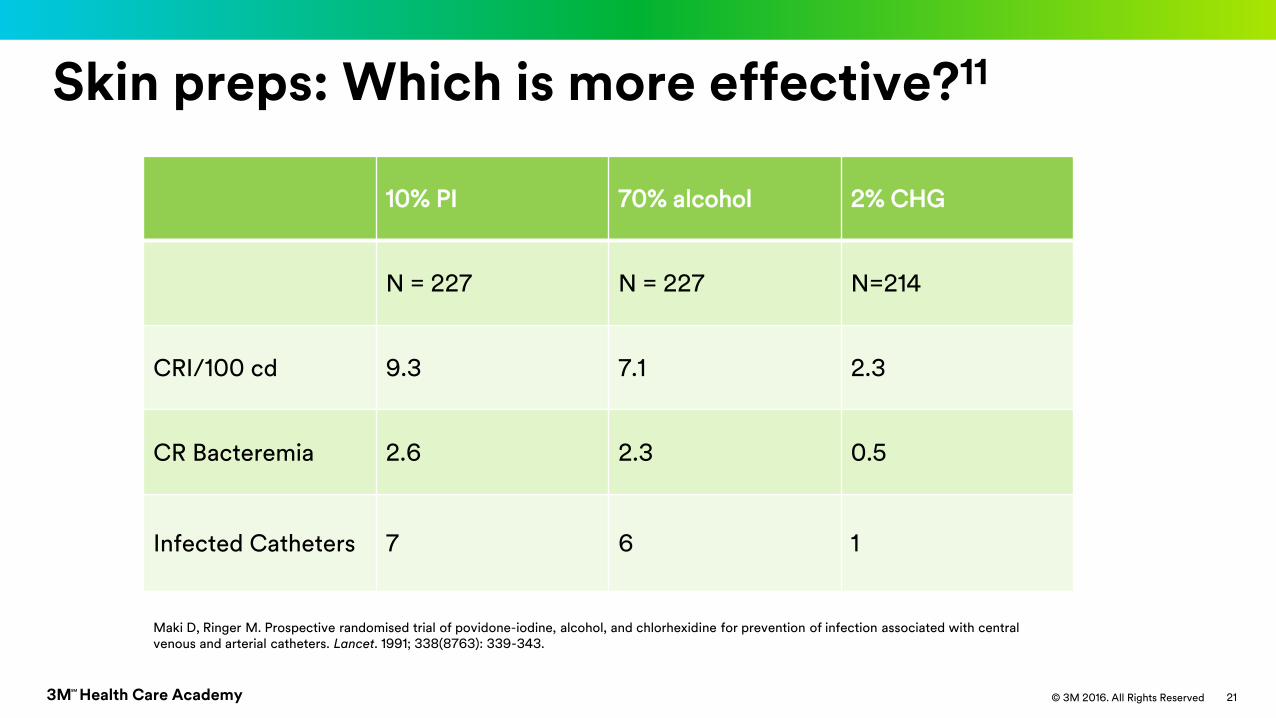
Maki D, Ringer M. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991; 338(8763): 339-343.
10% PI 70% alcohol 2% CHG
N = 227 N = 227 N=214
CRI/100 cd 9.3 7.1 2.3
CR Bacteremia 2.6 2.3 0.5
Infected Catheters 7 6 1
Skin preps: Which is more effective?11
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
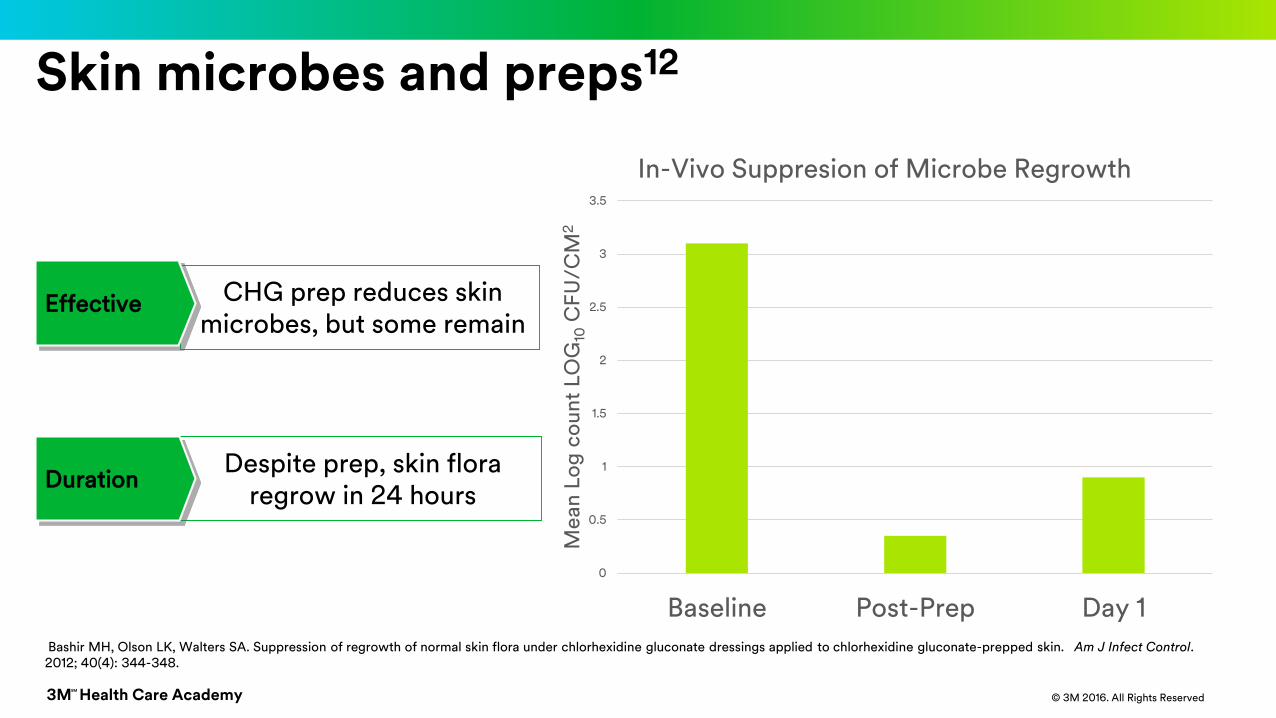
Skin microbes and preps12
0
0.5
1
1.5
2
2.5
3
3.5
Baseline Post-Prep Day 1
Me
an
Lo
g c
ou
nt
LO
G10
CF
U/C
M2
In-Vivo Suppresion of Microbe Regrowth
CHG prep reduces skin microbes, but some remain
Effective
Despite prep, skin flora regrow in 24 hours
Duration
Bashir MH, Olson LK, Walters SA. Suppression of regrowth of normal skin flora under chlorhexidine gluconate dressings applied to chlorhexidine gluconate-prepped skin. Am J Infect Control. 2012; 40(4): 344-348.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 23
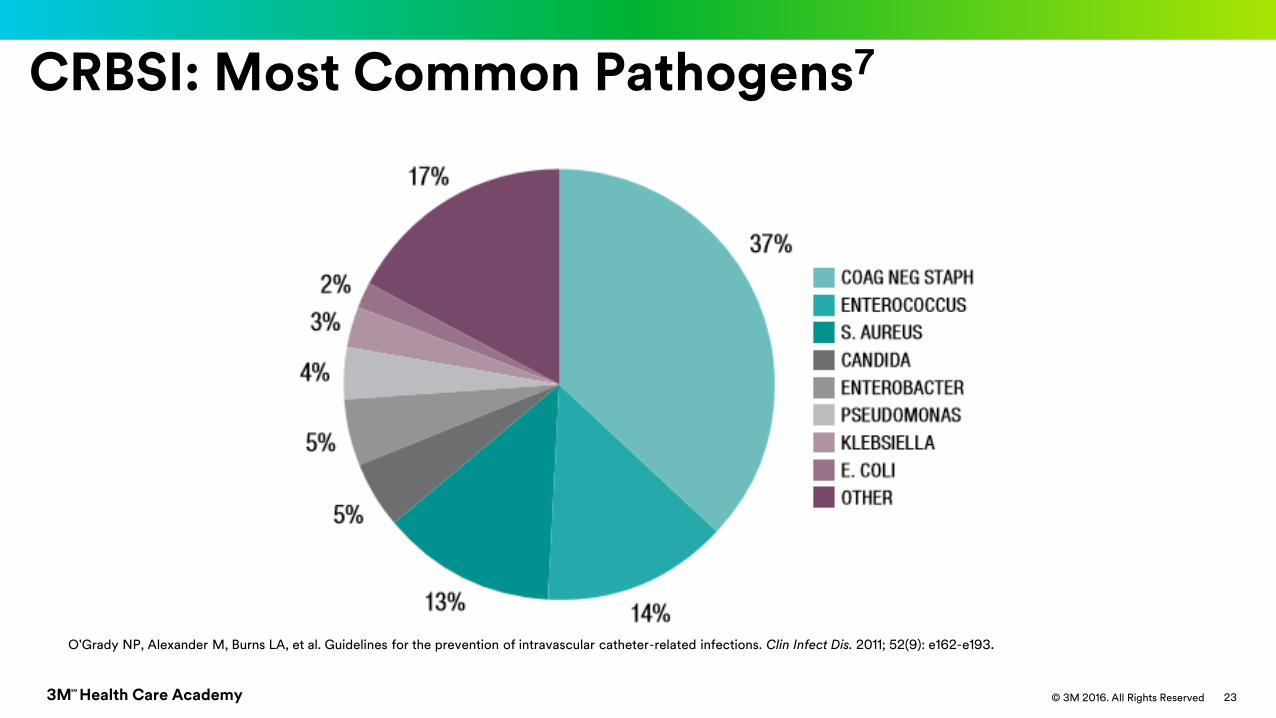
CRBSI: Most Common Pathogens7
O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011; 52(9): e162-e193.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 24
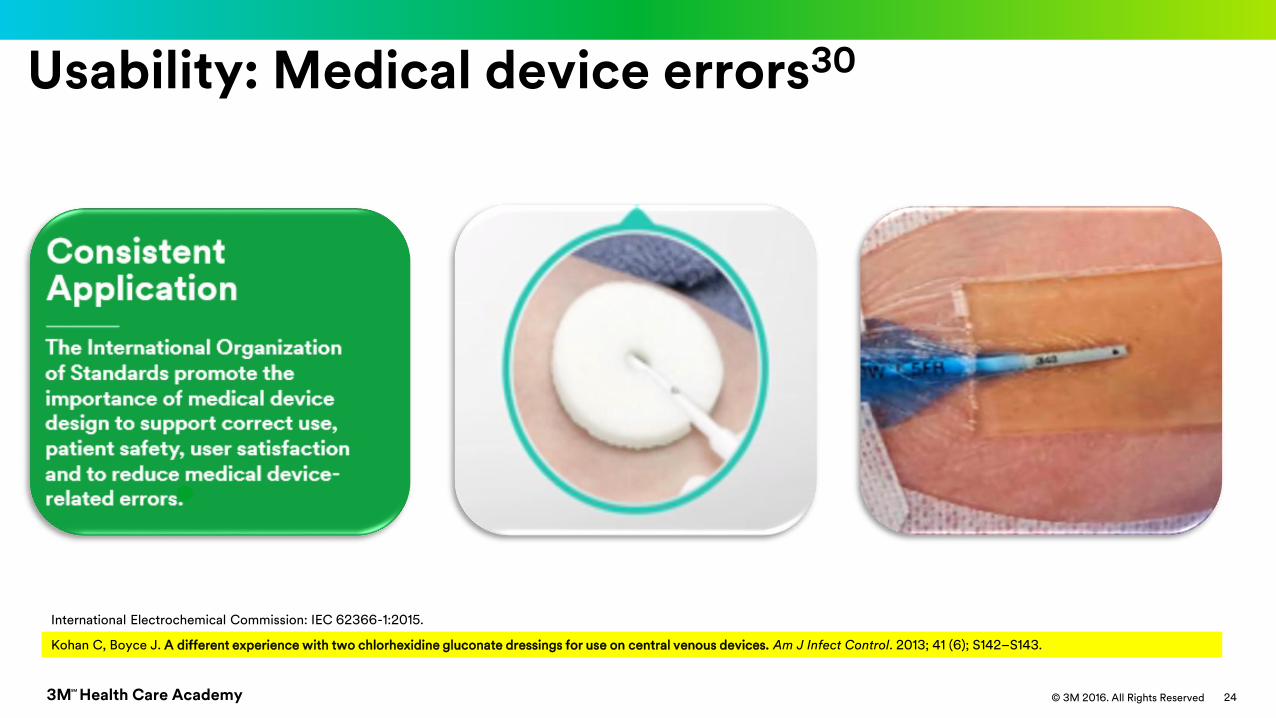
Usability: Medical device errors30
Kohan C, Boyce J. A different experience with two chlorhexidine gluconate dressings for use on central venous devices. Am J Infect Control. 2013; 41 (6); S142–S143.
International Electrochemical Commission: IEC 62366-1:2015.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 25
Site assessment
Recommends the use of transparent dressings because they permit continuous visual inspection of the catheter site.
Some dressing materials may obstruct site visibility and reduce securement.
CDC7
Gauze or sponges9
INS 2016 Standard 41 recommends assessment of the VAD catheter-skin junction site and surrounding area for redness, tenderness,
swelling, and drainage by visual inspection and palpation.
INS9
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 26
Phlebitis is related to bloodstream infection15
Mestre G, Berbel C, Tortajada P, et al, Successful multifaceted intervention aimed to reduced short peripheral venous catheter related adverse events: A quasi experimental study. Am J Infect Control. 2013; 41: 520-526.
Related to the incidence of peripheral catheter bloodstream infection (ratio 1 catheter related bloodstream infection for every 320 episodes of peripheral vein phlebitis)
Peripheral Vein Phlebitis
• The most used catheter CVC to PVC = 1:90• Peripheral catheters cause 19% of all CRBSIs• Peripheral catheters are the leading source of S. aureus BSI
Peripheral Catheters

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 27
Dressing Disruption
Do not rely on standard (non-bordered) VAD dressings as a means of stabilization… (I). 9
INS 2016
>10x risk of infection with 2+ unscheduled dressing changes16CRBSI Risk
Timsit JF, Bouadma L, Ruckly S, Schwebel C, Garrouste-Orgeas M, Bronchard R. Dressing disruption is a major risk factor for catheter-related infections. Crit Care Med. 2012; 40(6): 1707-1714.
0.1
1
10
100
1st 2nd final
Hazard ratio
# Dressing disruptions
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 28
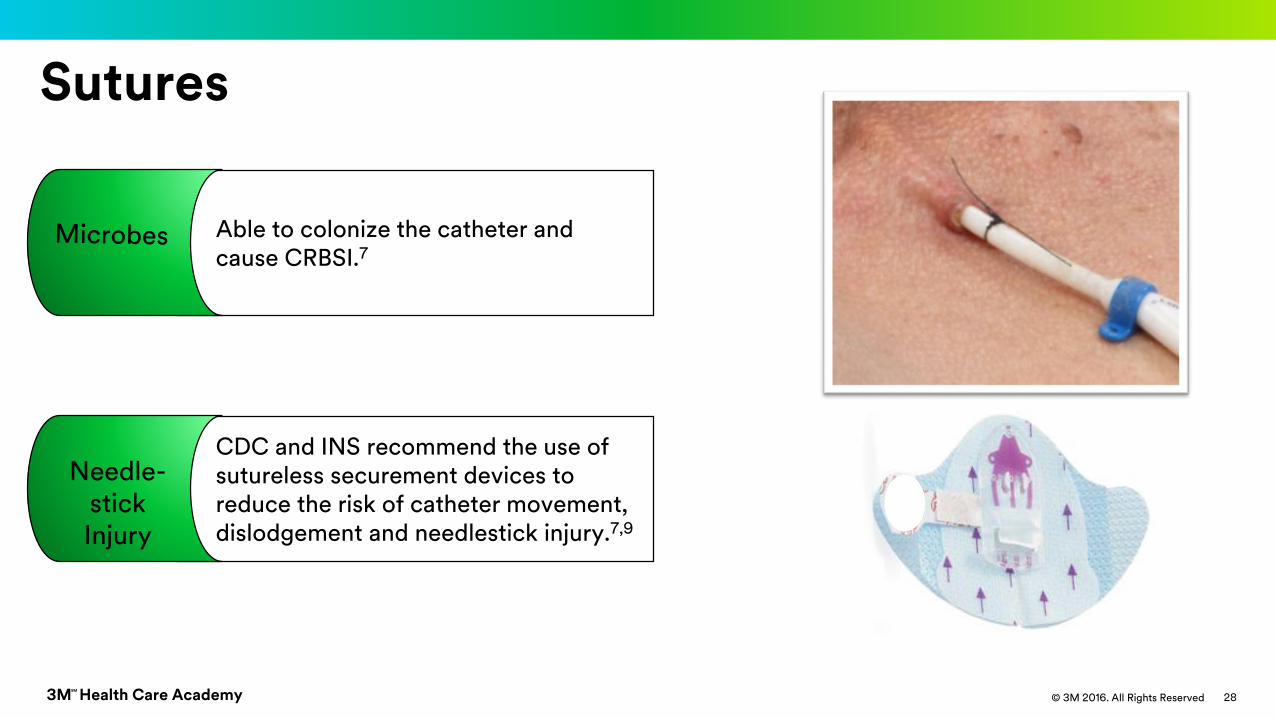
Sutures
CDC and INS recommend the use of sutureless securement devices to reduce the risk of catheter movement, dislodgement and needlestick injury.7,9
Needle-stick Injury
Able to colonize the catheter and cause CRBSI.7
3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
29
The difference is clear:Solving the site maintenance challenge
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 30
▪ 1st Synthesized & Marketed in 1950s– Over 55 years of efficacy and safety experience by chlorhexidine as a topical
antimicrobial
▪ Efficacy– Broad-spectrum activity against gram-positive and gram-negative bacteria,
anaerobes and aerobes, yeasts, and some lipid-envelope viruses. Not sporicidal. Demonstrated effectiveness against S. epidermidis, MRSA, VRE, K. pneumoniae, C. albicans
– Bacterial Susceptibility• After 50 years of research and experience, still no development of bacterial resistance
against CHG• A large multitude of genes will need to evolve to fend off CHG attack on bacteria
CHG Effectiveness

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 31
CHG Gel: Tested against 37 microbial strains17
Hensler JP, Schwab DL, Olson LK, Palka-Santini M. Growth inhibition of microorganisms involved in catheter-related infections by an antimicrobial transparent iv dressing containing chlorhexidine gluconate (CHG). Presented at: 19th Annual Conference of the European Society of Clinical Microbiology and Infectious Diseases; May 16-19, 2009: Helsinki, Finland.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 32
Bashir (2012) Am J Infect Control12
CHG Gel Securement Dressing Results
DESIGN: Randomized controlled trial comparing
suppression of microbe regrowth chlorhexidine prep vs.
CHG gel vs CHG disk dressings.
METHODS:
o All patients treated with CHG skin prep
o Randomized to either:
• Transparent film dressing (control)
• CHG gel dressing
• CHG disk + transparent film dressing
RESULTS:
o n = 32 healthy subjects
o The CHG gel dressing demonstrated significantly greater microbial suppression than CHG disk on day 7 (p = 0.01).
Bashir MH, Olson LK, Walters SA. Suppression of regrowth of normal skin flora under chlorhexidine gluconate dressings applied to chlorhexidine gluconate-prepped skin. Am J Infect Control. 2012; 40(4): 344-348.
CHG Gel Dressing
CHG Disk Transparent Film Dressing

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 33
Kohan (2013) Am J Infect Control14
A Different Experience with Two Different Chlorhexidine Gluconate Dressings for use on Central Venous Devices
CHG Gel Securement Dressing Results
DESIGN: Clinical audit: correct application
METHODS:
o Staff re-educated on both products
o Evaluated application of CHG gel dressing in 2012, and CHG disk in 2009
RESULTS:
o n = 248 dressing applications
o CHG disk placed incorrectly 64%
o CHG gel pad of the CHG dressings placed correctly 100%
Kohan C, Boyce J. A different experience with two chlorhexidine gluconate dressings for use on central venous devices. Am J Infect Control. 2013; 41 (6); S142–S143.
CHG Gel Pad CHG Disk

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 34
CHG Gel: Site visibility to assess complications9
Erythema Extravasation
Catheter Damage
Catheter movement
Infiltration
Phlebitis
Bleeding
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 35
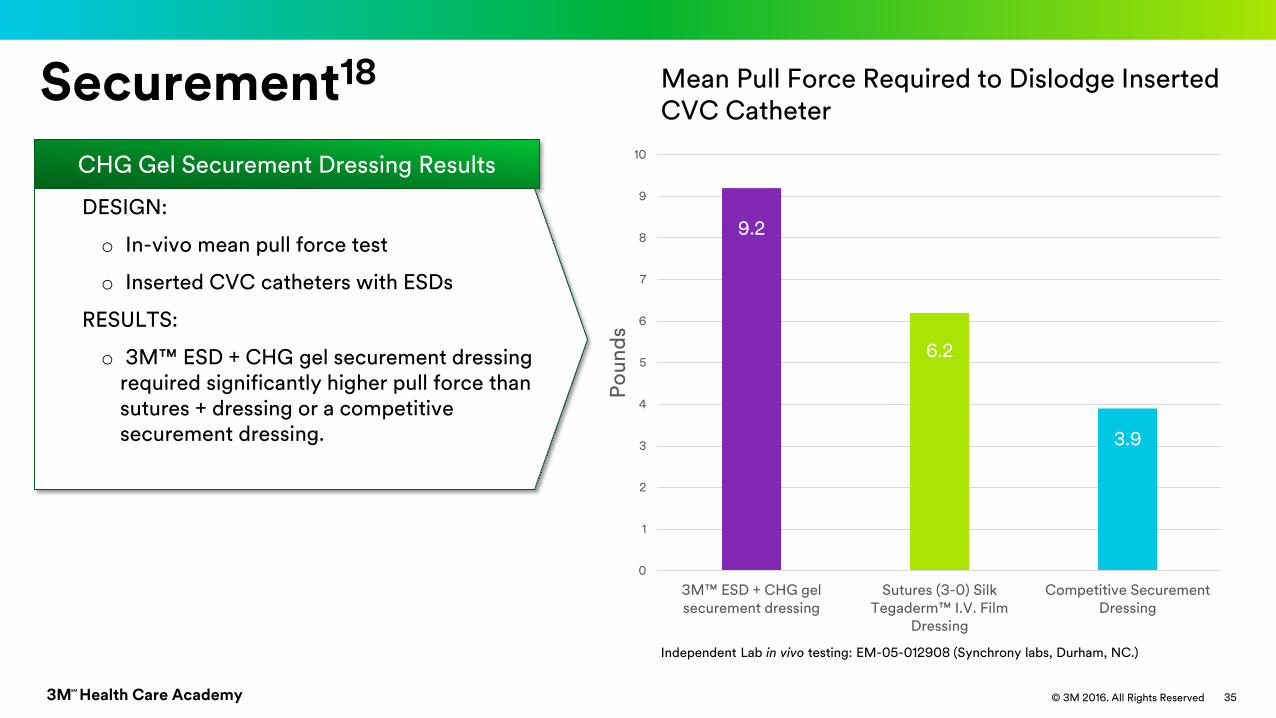
Securement18
9.2
6.2
3.9
0
1
2
3
4
5
6
7
8
9
10
3M™ ESD + CHG gel securement dressing
Sutures (3-0) Silk Tegaderm™ I.V. Film
Dressing
Competitive SecurementDressing
Po
un
ds
Mean Pull Force Required to Dislodge Inserted CVC Catheter
CHG Gel Securement Dressing Results
DESIGN:
o In-vivo mean pull force test
o Inserted CVC catheters with ESDs
RESULTS:
o 3M™ ESD + CHG gel securement dressing required significantly higher pull force than sutures + dressing or a competitive securement dressing.
Independent Lab in vivo testing: EM-05-012908 (Synchrony labs, Durham, NC.)
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 36
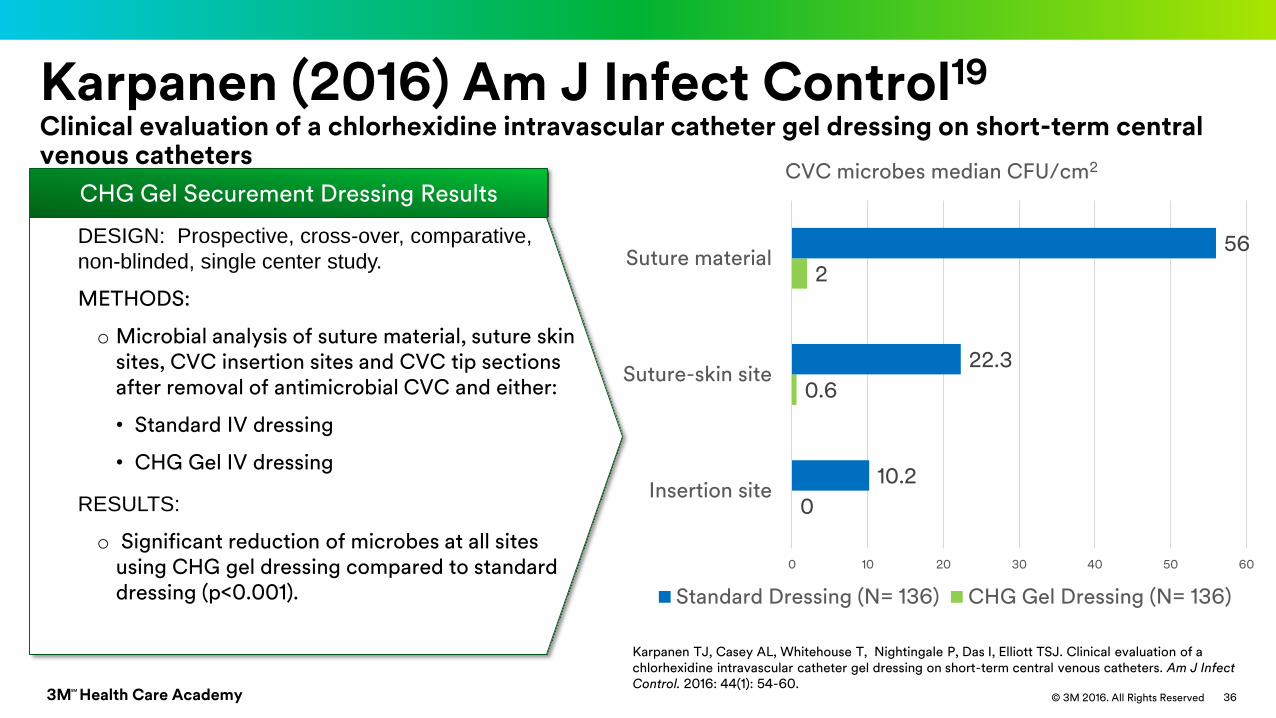
Karpanen (2016) Am J Infect Control19
Clinical evaluation of a chlorhexidine intravascular catheter gel dressing on short-term central venous catheters
CHG Gel Securement Dressing Results
DESIGN: Prospective, cross-over, comparative,
non-blinded, single center study.
METHODS:
o Microbial analysis of suture material, suture skin sites, CVC insertion sites and CVC tip sections after removal of antimicrobial CVC and either:
• Standard IV dressing
• CHG Gel IV dressing
RESULTS:
o Significant reduction of microbes at all sites using CHG gel dressing compared to standard dressing (p<0.001).
0
0.6
2
10.2
22.3
56
0 10 20 30 40 50 60
Insertion site
Suture-skin site
Suture material
CVC microbes median CFU/cm2
Standard Dressing (N= 136) CHG Gel Dressing (N= 136)
Karpanen TJ, Casey AL, Whitehouse T, Nightingale P, Das I, Elliott TSJ. Clinical evaluation of a chlorhexidine intravascular catheter gel dressing on short-term central venous catheters. Am J Infect Control. 2016: 44(1): 54-60.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
37
CRBSI Clinical Studies
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
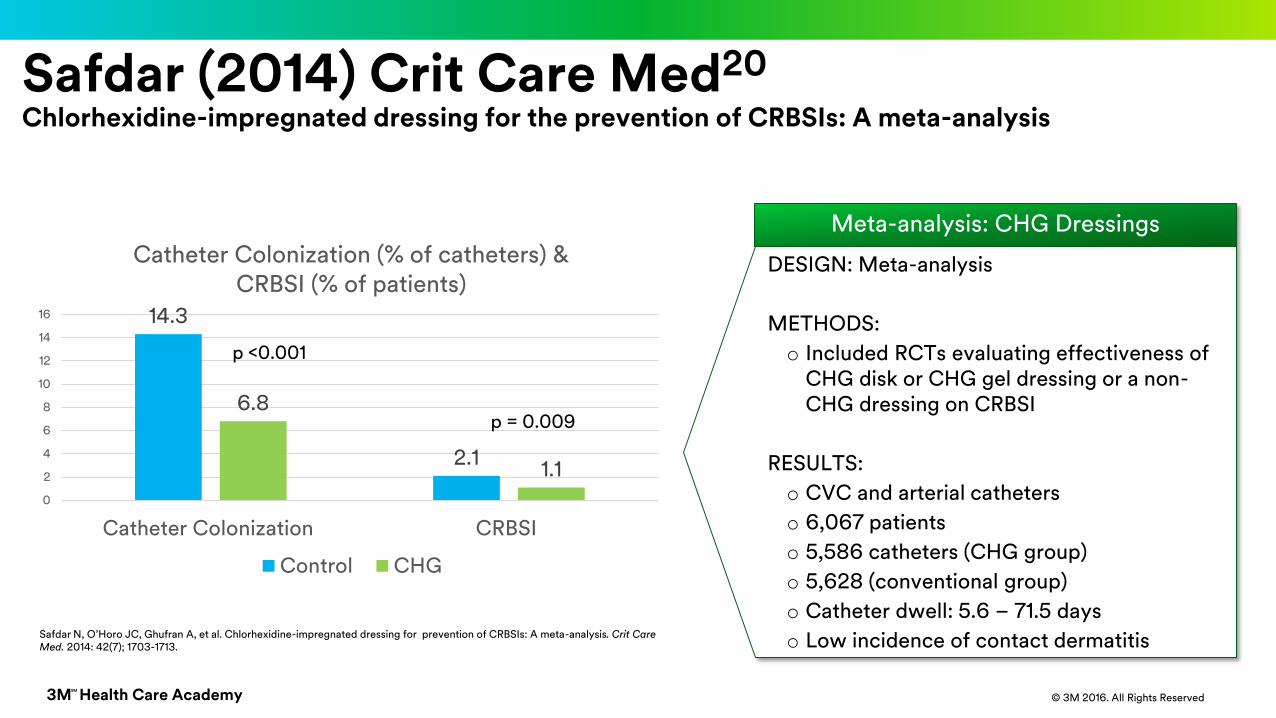
Safdar (2014) Crit Care Med20
Chlorhexidine-impregnated dressing for the prevention of CRBSIs: A meta-analysis
Safdar N, O’Horo JC, Ghufran A, et al. Chlorhexidine-impregnated dressing for prevention of CRBSIs: A meta-analysis. Crit Care Med. 2014: 42(7); 1703-1713.
Meta-analysis: CHG Dressings
DESIGN: Meta-analysis
METHODS:
o Included RCTs evaluating effectiveness of CHG disk or CHG gel dressing or a non-CHG dressing on CRBSI
RESULTS:
o CVC and arterial catheters
o 6,067 patients
o 5,586 catheters (CHG group)
o 5,628 (conventional group)
o Catheter dwell: 5.6 – 71.5 days
o Low incidence of contact dermatitis
14.3
2.1
6.8
1.1
0
2
4
6
8
10
12
14
16
Catheter Colonization CRBSI
Catheter Colonization (% of catheters) & CRBSI (% of patients)
Control CHG
p <0.001
p = 0.009
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 39
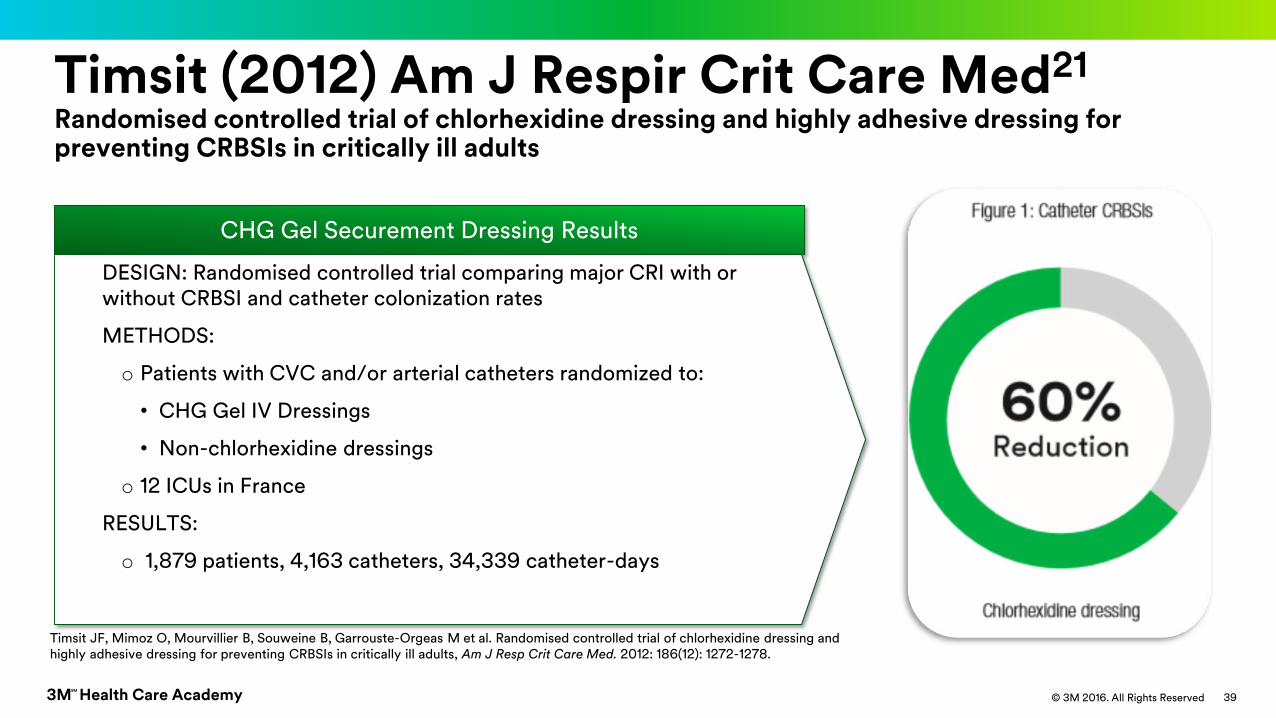
Timsit (2012) Am J Respir Crit Care Med21
Randomised controlled trial of chlorhexidine dressing and highly adhesive dressing for preventing CRBSIs in critically ill adults
CHG Gel Securement Dressing Results
DESIGN: Randomised controlled trial comparing major CRI with or without CRBSI and catheter colonization rates
METHODS:
o Patients with CVC and/or arterial catheters randomized to:
• CHG Gel IV Dressings
• Non-chlorhexidine dressings
o 12 ICUs in France
RESULTS:
o 1,879 patients, 4,163 catheters, 34,339 catheter-days
Timsit JF, Mimoz O, Mourvillier B, Souweine B, Garrouste-Orgeas M et al. Randomised controlled trial of chlorhexidine dressing and highly adhesive dressing for preventing CRBSIs in critically ill adults, Am J Resp Crit Care Med. 2012: 186(12): 1272-1278.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 40
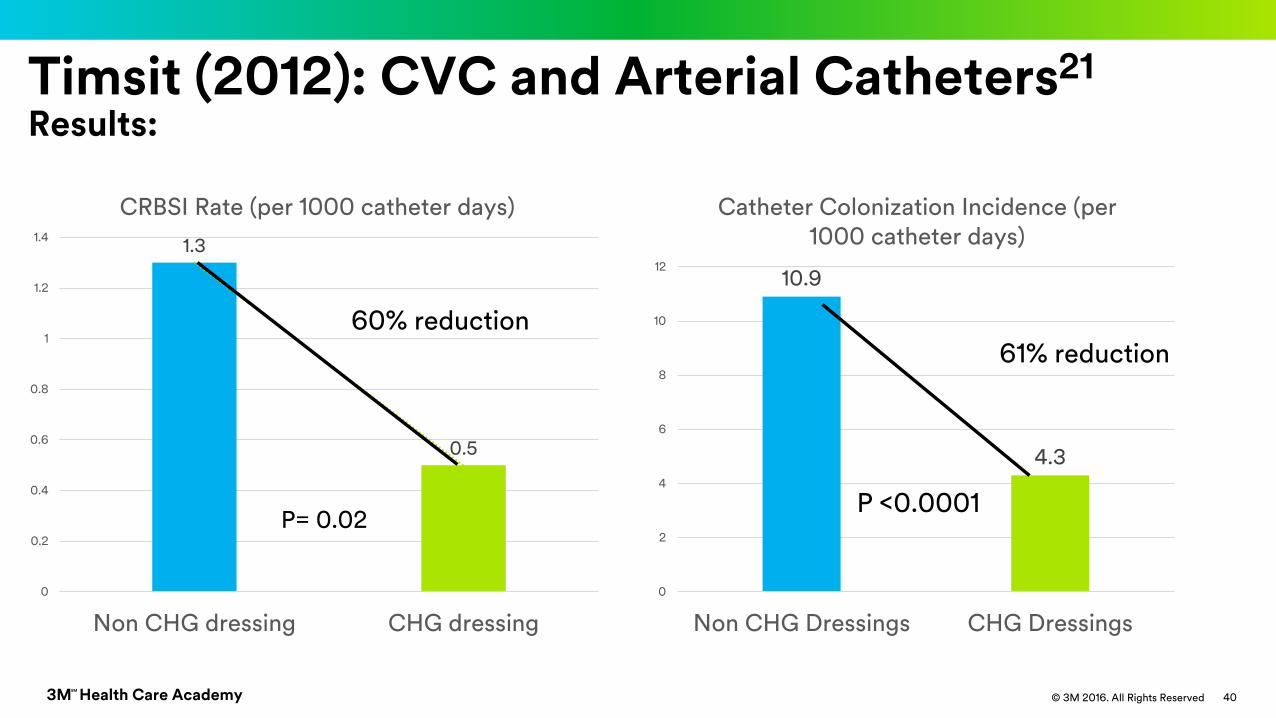
Timsit (2012): CVC and Arterial Catheters21
Results:
P= 0.02
1.3
0.5
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Non CHG dressing CHG dressing
CRBSI Rate (per 1000 catheter days)
60% reduction
10.9
4.3
0
2
4
6
8
10
12
Non CHG Dressings CHG Dressings
Catheter Colonization Incidence (per 1000 catheter days)
61% reduction
P <0.0001
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
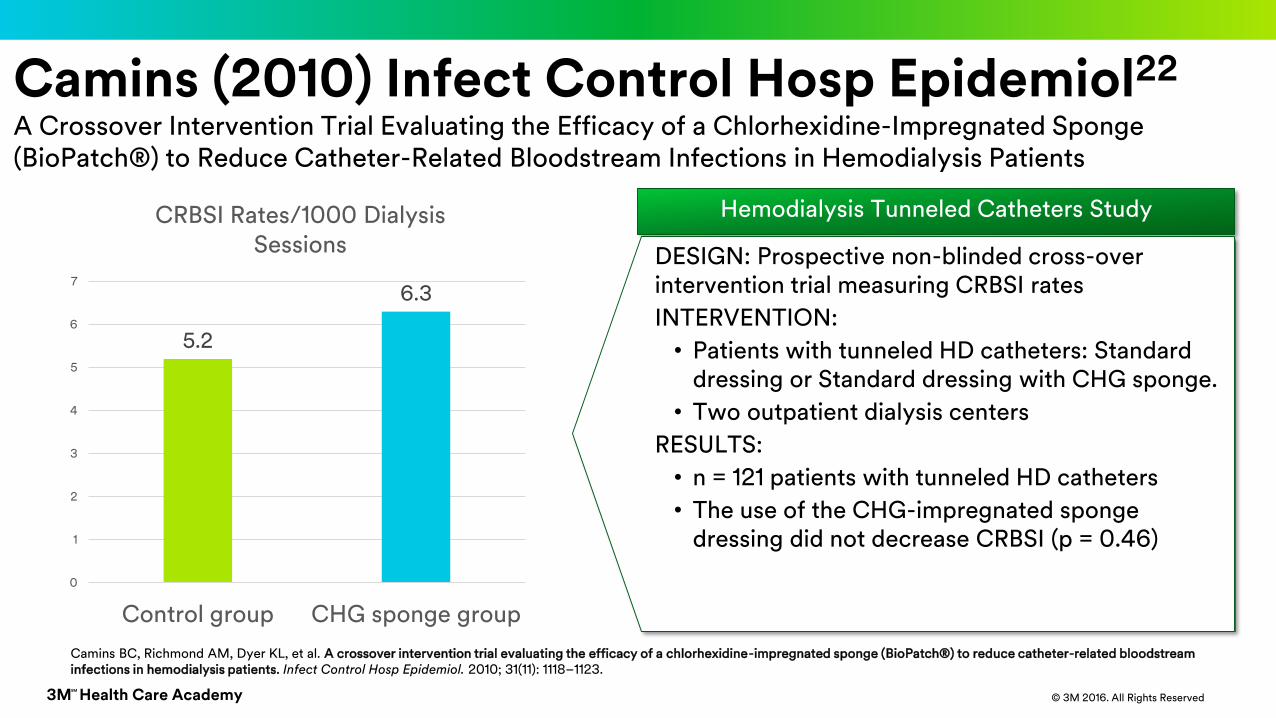
Camins (2010) Infect Control Hosp Epidemiol22
A Crossover Intervention Trial Evaluating the Efficacy of a Chlorhexidine-Impregnated Sponge (BioPatch®) to Reduce Catheter-Related Bloodstream Infections in Hemodialysis Patients
Hemodialysis Tunneled Catheters Study
DESIGN: Prospective non-blinded cross-over intervention trial measuring CRBSI rates
INTERVENTION:
• Patients with tunneled HD catheters: Standard dressing or Standard dressing with CHG sponge.
• Two outpatient dialysis centers
RESULTS:
• n = 121 patients with tunneled HD catheters
• The use of the CHG-impregnated sponge dressing did not decrease CRBSI (p = 0.46)
5.2
6.3
0
1
2
3
4
5
6
7
Control group CHG sponge group
CRBSI Rates/1000 Dialysis Sessions
Camins BC, Richmond AM, Dyer KL, et al. A crossover intervention trial evaluating the efficacy of a chlorhexidine-impregnated sponge (BioPatch®) to reduce catheter-related bloodstream infections in hemodialysis patients. Infect Control Hosp Epidemiol. 2010; 31(11): 1118–1123.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
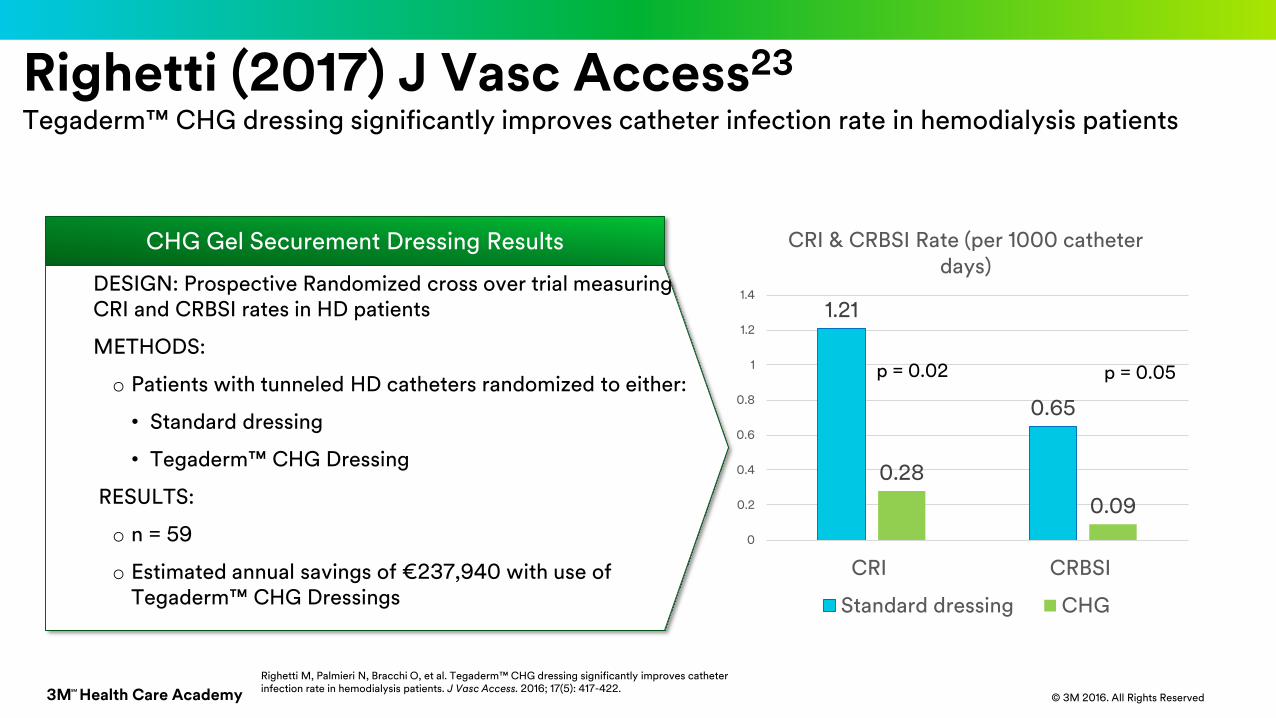
Righetti M, Palmieri N, Bracchi O, et al. Tegaderm™ CHG dressing significantly improves catheter infection rate in hemodialysis patients. J Vasc Access. 2016; 17(5): 417-422.
Righetti (2017) J Vasc Access23
Tegaderm™ CHG dressing significantly improves catheter infection rate in hemodialysis patients
CHG Gel Securement Dressing Results
DESIGN: Prospective Randomized cross over trial measuring CRI and CRBSI rates in HD patients
METHODS:
o Patients with tunneled HD catheters randomized to either:
• Standard dressing
• Tegaderm™ CHG Dressing
RESULTS:
o n = 59
o Estimated annual savings of €237,940 with use of Tegaderm™ CHG Dressings
1.21
0.65
0.28
0.09
0
0.2
0.4
0.6
0.8
1
1.2
1.4
CRI CRBSI
CRI & CRBSI Rate (per 1000 catheter days)
Standard dressing CHG
p = 0.02 p = 0.05
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
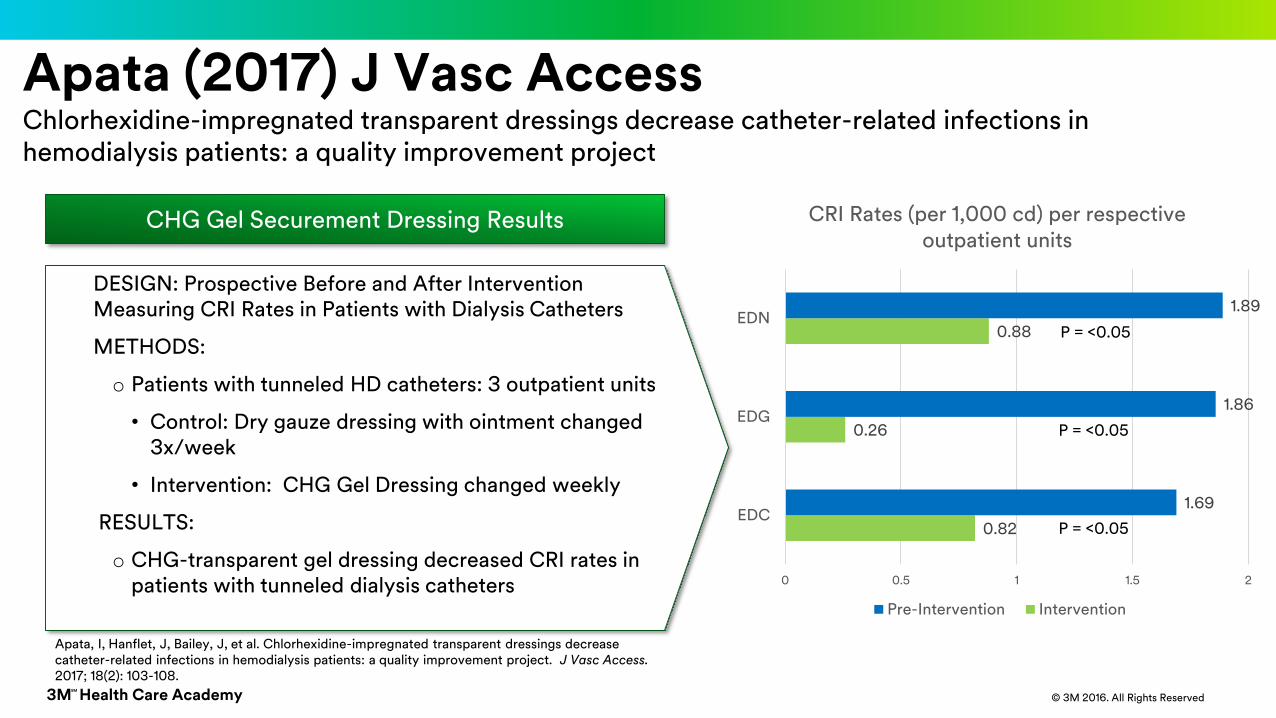
Apata, I, Hanflet, J, Bailey, J, et al. Chlorhexidine-impregnated transparent dressings decrease catheter-related infections in hemodialysis patients: a quality improvement project. J Vasc Access. 2017; 18(2): 103-108.
Apata (2017) J Vasc AccessChlorhexidine-impregnated transparent dressings decrease catheter-related infections in hemodialysis patients: a quality improvement project
CHG Gel Securement Dressing Results
DESIGN: Prospective Before and After Intervention Measuring CRI Rates in Patients with Dialysis Catheters
METHODS:
o Patients with tunneled HD catheters: 3 outpatient units
• Control: Dry gauze dressing with ointment changed 3x/week
• Intervention: CHG Gel Dressing changed weekly
RESULTS:
o CHG-transparent gel dressing decreased CRI rates in patients with tunneled dialysis catheters
0.82
0.26
0.88
1.69
1.86
1.89
0 0.5 1 1.5 2
EDC
EDG
EDN
CRI Rates (per 1,000 cd) per respective outpatient units
Pre-Intervention Intervention
P = <0.05
P = <0.05
P = <0.05
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
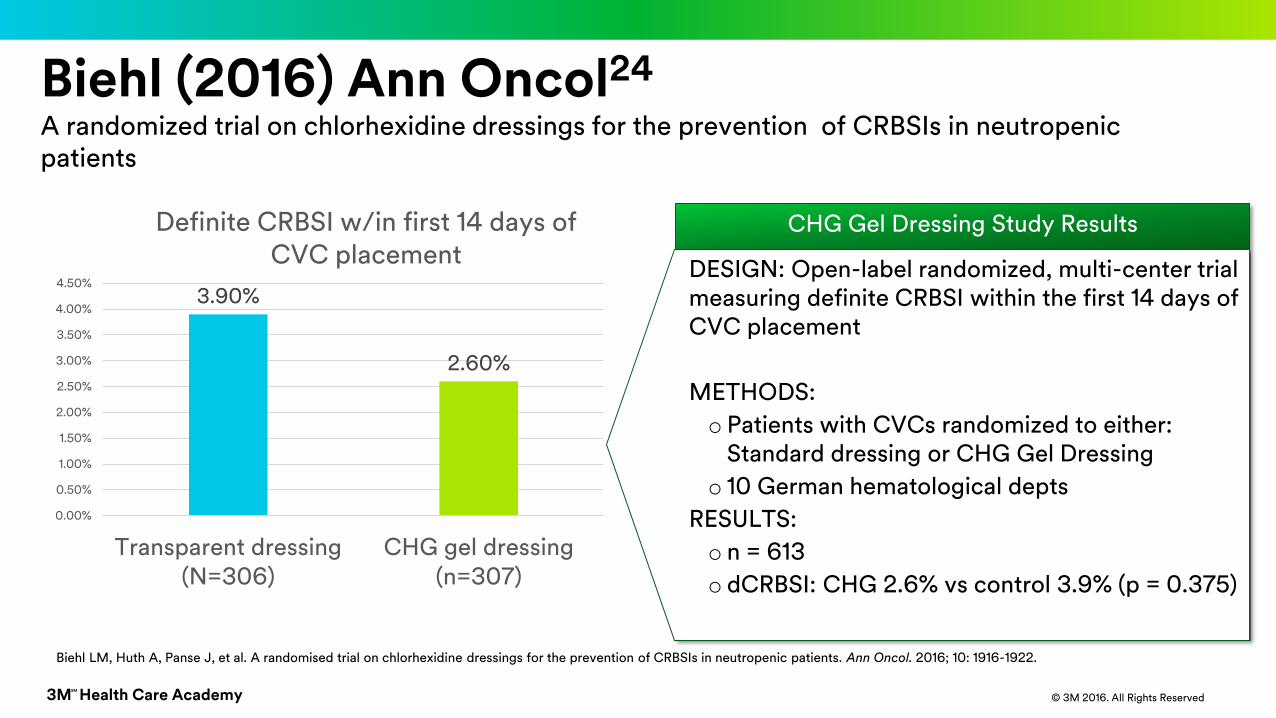
Biehl (2016) Ann Oncol24
A randomized trial on chlorhexidine dressings for the prevention of CRBSIs in neutropenic patients
CHG Gel Dressing Study Results
DESIGN: Open-label randomized, multi-center trial measuring definite CRBSI within the first 14 days of CVC placement
METHODS:
o Patients with CVCs randomized to either: Standard dressing or CHG Gel Dressing
o 10 German hematological depts
RESULTS:
o n = 613
o dCRBSI: CHG 2.6% vs control 3.9% (p = 0.375)
3.90%
2.60%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
4.50%
Transparent dressing(N=306)
CHG gel dressing(n=307)
Definite CRBSI w/in first 14 days of CVC placement
Biehl LM, Huth A, Panse J, et al. A randomised trial on chlorhexidine dressings for the prevention of CRBSIs in neutropenic patients. Ann Oncol. 2016; 10: 1916-1922.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
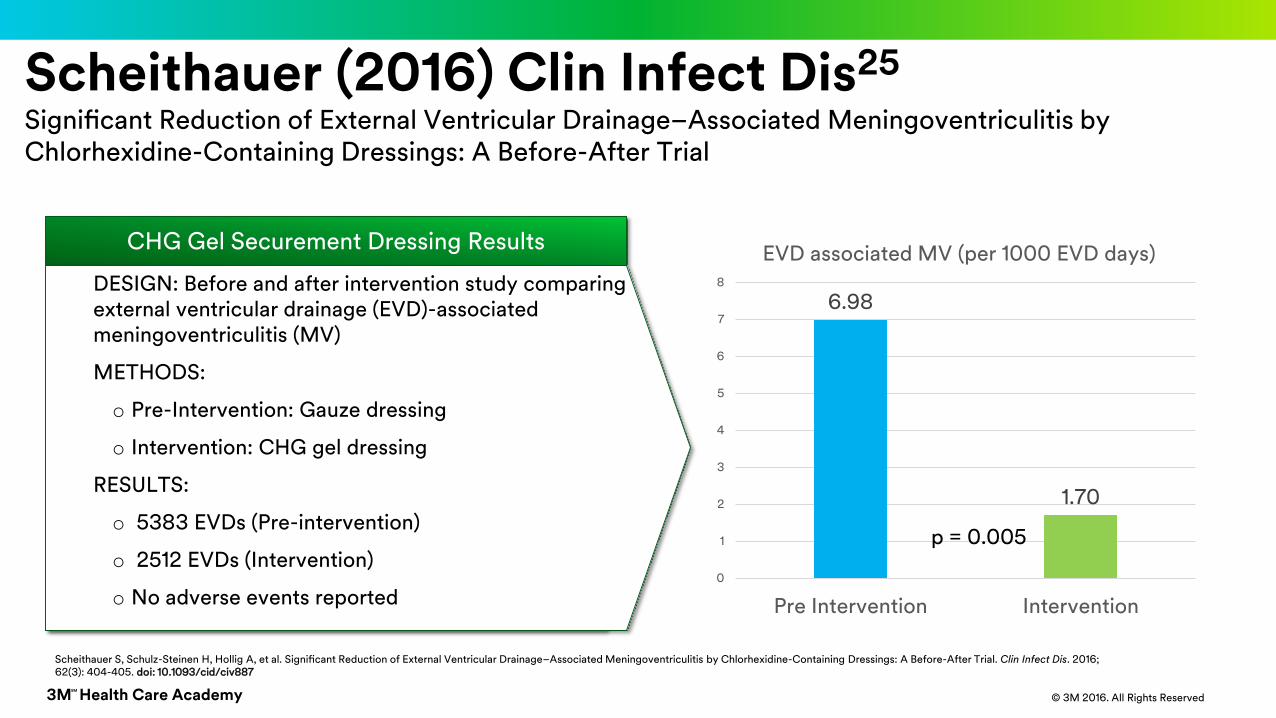
Scheithauer (2016) Clin Infect Dis25
Significant Reduction of External Ventricular Drainage–Associated Meningoventriculitis by Chlorhexidine-Containing Dressings: A Before-After Trial
Scheithauer S, Schulz-Steinen H, Hollig A, et al. Significant Reduction of External Ventricular Drainage–Associated Meningoventriculitis by Chlorhexidine-Containing Dressings: A Before-After Trial. Clin Infect Dis. 2016; 62(3): 404-405. doi: 10.1093/cid/civ887
CHG Gel Securement Dressing Results
• DESIGN
• RESULTS
o
DESIGN: Before and after intervention study comparing external ventricular drainage (EVD)-associated meningoventriculitis (MV)
METHODS:
o Pre-Intervention: Gauze dressing
o Intervention: CHG gel dressing
RESULTS:
o 5383 EVDs (Pre-intervention)
o 2512 EVDs (Intervention)
o No adverse events reported
6.98
1.70
0
1
2
3
4
5
6
7
8
Pre Intervention Intervention
EVD associated MV (per 1000 EVD days)
p = 0.005
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 46
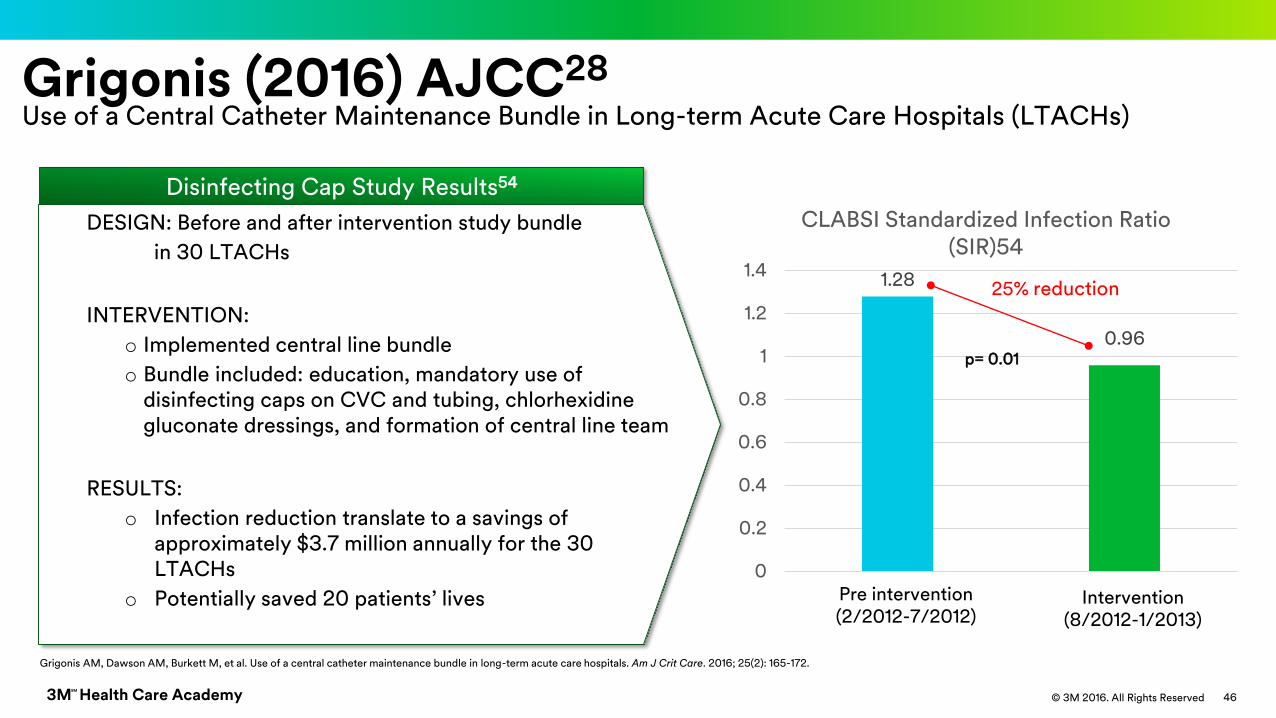
Grigonis (2016) AJCC28
Use of a Central Catheter Maintenance Bundle in Long-term Acute Care Hospitals (LTACHs)
Disinfecting Cap Study Results54
DESIGN: Before and after intervention study bundle
in 30 LTACHs
INTERVENTION:
o Implemented central line bundle
o Bundle included: education, mandatory use of disinfecting caps on CVC and tubing, chlorhexidine gluconate dressings, and formation of central line team
RESULTS:
o Infection reduction translate to a savings of approximately $3.7 million annually for the 30 LTACHs
o Potentially saved 20 patients’ lives
Grigonis AM, Dawson AM, Burkett M, et al. Use of a central catheter maintenance bundle in long-term acute care hospitals. Am J Crit Care. 2016; 25(2): 165-172.
1.28
0.96
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Pre intervention Intervention
CLABSI Standardized Infection Ratio (SIR)54
p= 0.01
25% reduction
Pre intervention(2/2012-7/2012)
Intervention(8/2012-1/2013)

3M Health Care AcademySM
© 3M 2016. All Rights Reserved
Thokala P, (2016) J Infec Prev29
Thokala P, Arrowsmith M, Poku E, et al. Economic impact of Tegaderm™ CHG chlorhexidine gluconate IV securement dressing in critically ill patients. J Infect Prev. September 17, 2016; (5): 216-223.
Economic impact of Tegaderm™ CHG IV securement dressing in critically ill patients
3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
48
Medical Adhesive-Related Skin Injury (MARSI)

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 49
McNichol L, Lund C, Rosen T, Gray M. Medical Adhesives and Patient Safety: State of the Science: Consensus Statements for the Assessment, Prevention, and Treatment of Adhesive-Related Skin Injuries. J Wound Ostomy Continence Nurs. 2013; 40(4):365-380.
Central Vascular Access Device (CVAD) Stabilization Standard 37, page S72-74
• Apply barrier solutions to skin exposed to adhesive dressing to reduce risk of Medical Adhesive-Related Skin Injury (MARSI). (Level I)
Skin preparation Best Practice: protect skin with an alcohol-free barrier film
Gorski L, Hadaway L, Hagle ME, McGoldrick M, Orr M, Doellman D. Infusion Therapy Standards of Practice. J Infus Nurs. 2016; 39(suppl 1): S1-S59.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 50
• Forms a protective interface between the adhesive and skin
• Adhesive removal removes barrier film, not epidermal cells
This
Not this
Best Practice: protect skin with an alcohol-free barrier film

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 51
So how do we prevent MARSI? Address causal factors
Type of adhesive Skin Preparation Application Technique Removal Technique

3M Health Care AcademySM
© 3M 2016. All Rights Reserved
What Does Some of the Evidence Tell Us?A recent study evaluated skin condition in 100 patients with peripherally inserted central catheters36
-
10
20
30
40
50
60
70
Without Cavilon NSBF With Cavilon NSBF
% o
f p
ati
en
ts
n=100*rash/redness, peeling, maceration, adhesive transfer
% Patients with skin complications* (PICC lines)
A significant decrease in local skin
complications with use of Cavilon™ NSBF was
demonstrated
Skin damage is a local complication that can lead to increased risk of colonization and infection37-38
Skin protectant plays an important role in reducing the local complications in PICC linesGeorge M. Use of a barrier film (3M™Cavilon™ No Sting Barrier Film) to reduce local skin complications around PICC lines: A randomized prospective controlled study. WCET Journal. 2016; 36(4): 8-13.
Roth RR, James WD. Microbial Ecology of the Skin. Annu Rev Microbiol. 1988; 42: 441-464.
Abad CL, Safdar N. Catheter-related Bloodstream Infections. Infect Dis. (Special Edition) 2011; 84-98. McMahon Publishing.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 53
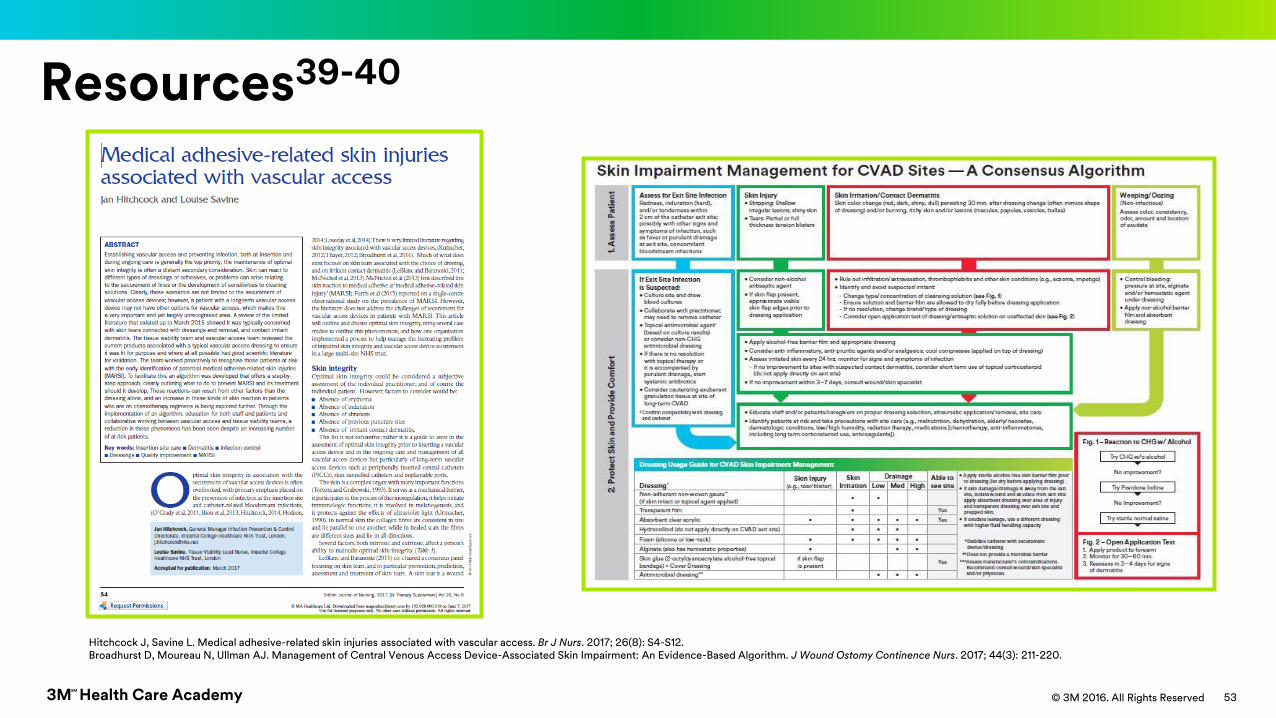
Resources39-40
Hitchcock J, Savine L. Medical adhesive-related skin injuries associated with vascular access. Br J Nurs. 2017; 26(8): S4-S12.Broadhurst D, Moureau N, Ullman AJ. Management of Central Venous Access Device-Associated Skin Impairment: An Evidence-Based Algorithm. J Wound Ostomy Continence Nurs. 2017; 44(3): 211-220.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
54
CHG Clinical Study Summary Slide
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 55
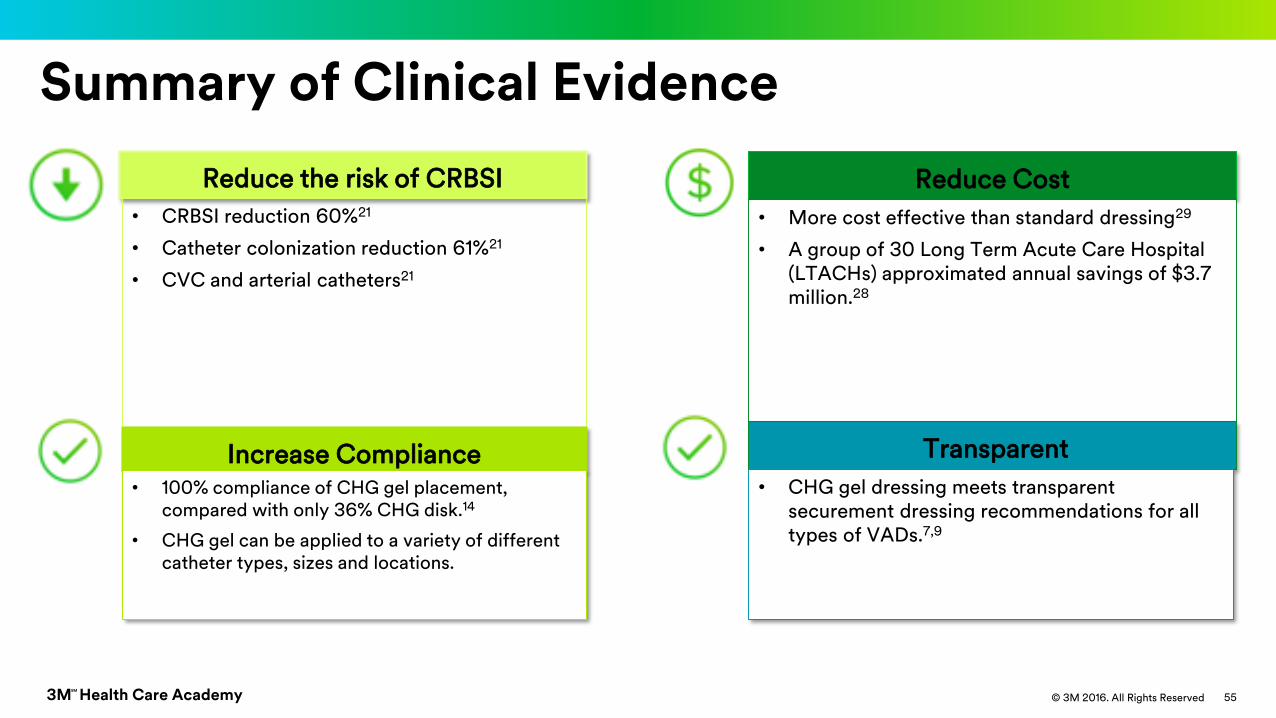
Summary of Clinical Evidence
Reduce the risk of CRBSI
• CRBSI reduction 60%21
• Catheter colonization reduction 61%21
• CVC and arterial catheters21
Reduce Cost
• More cost effective than standard dressing29
• A group of 30 Long Term Acute Care Hospital (LTACHs) approximated annual savings of $3.7 million.28
Transparent
• CHG gel dressing meets transparent securement dressing recommendations for all types of VADs.7,9
Increase Compliance• 100% compliance of CHG gel placement,
compared with only 36% CHG disk.14
• CHG gel can be applied to a variety of different catheter types, sizes and locations.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved 56
BSI
• ALL vascular access devices increase the risk of BSI
• Contamination can be introduced into bloodstream via:
• Extraluminal route
• Intraluminal route
• Clinical considerations are important when implementing
evidence based interventions to address catheter
maintenance challenges

3M Health Care AcademySM
© 3M 2016. All Rights Reserved 57
Reducing the risk of BSI A comprehensive approach to maintenance is critical to reduce risk at
all access points.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved© 3M 2016. All Rights Reserved3M Health Care AcademySM
58
Thank you
Questions?

3M Health Care AcademySM
© 3M 2016. All Rights Reserved
References1. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by
the Infectious Diseases Society of America. Clin Infect Dis. 2009; 49(1): 1-45.
2. Safdar N, Maki DG. The pathogenesis of catheter-related bloodstream infection with noncuffed short-term central venous catheters. Intensive Care Med. 2004;
30(1): 62-67.
3. Mermel LA. What is the predominant source of intravascular catheter infections? Clin Infect Dis. 2011; 52(2): 211-212.
4. Maki DG, Stolz SM, Wheeler S, Mermel LA. Prevention of central venous catheter-related bloodstream infection by use of an antiseptic-impregnated catheter:
A randomized, controlled trial. Ann Intern Med. 1997; 127(4): 257-266.
5. Douard MC, Clementi E, Arlet G, et al. Negative catheter-tip culture and diagnosis of catheter-related bacteremia. Nutrition. 1994; 10(5): 397-404.
6. Dittmer ID, Sharp D, McNulty CA, Williams AJ, Banks RA. A prospective study of central venous hemodialysis catheter colonization and peripheral bacteremia.
Clin Nephrol. 1999; 51(1): 34-39.
7. O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011; 52(9): e162-e193.
8. Marschall J, Mermel LA, Fakih M, et al. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control
Hosp Epidemiol. 2014; 35(7): 753-771.
9. Gorski L, Hadaway L, Hagle ME, McGoldrick M, Orr M, Doellman D. Infusion Therapy Standards of Practice. J Infus Nurs. 2016; 39(suppl 1): S1-S59.
10. Association for Professionals in Infection Control and Epidemiology. APIC Implementation Guide: Guide to Preventing Central Line-Associated Bloodstream
Infections. 2015. https://apic.org/Resource_/TinyMceFileManager/2015/APIC_CLABSI_WEB.pdf. Accessed September 2017.
11. Maki D, Ringer M. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and
arterial catheters. Lancet. 1991; 338(8763): 339-343.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved
References cont.12. Bashir MH, Olson LK, Walters SA. Suppression of regrowth of normal skin flora under chlorhexidine gluconate dressings applied to chlorhexidine gluconate-
prepped skin. Am J Infect Control. 2012; 40(4): 344-8.
13. Aslam, S, Effect of antibacterials on biofilms. Am J Infect Contr. 2008; 36:S175.e9-S175.e11.i
14. Kohan C, Boyce J. A different experience with two chlorhexidine gluconate dressings for use on central venous devices. Am J Infect Contr. 2013; 41 (6); S142–
S143.
15. Mestre G, Berbel C, Tortajada P, et al, Successful multifaceted intervention aimed to reduced short peripheral venous catheter related adverse events: A quasi
experimental study. Am J Infect Control. 2013; 41: 520-526.
16. Timsit JF, Bouadma L, Ruckly S, Schwebel C, Garrouste-Orgeas M, Bronchard R. Dressing disruption is a major risk factor for catheter-related infections. Crit
Care Med. 2012; 40(6): 1707-1714.
17. Hensler JP, Schwab DL, Olson LK, Palka-Santini M. Growth inhibition of microorganisms involved in catheter-related infections by an antimicrobial transparent
IV dressing containing chlorhexidine gluconate (CHG). Presented at: 19th Annual Conference of the European Society of Clinical Microbiology and Infectious
Diseases; May 16-19, 2009: Helsinki, Finland.
18. Independent Lab in vivo testing: EM-05-012908 (Synchrony labs, Durham, NC.)
19. Karpanen TJ, Casey AL, Whitehouse T, Nightingale P, Das I, Elliott TSJ. Clinical evaluation of a chlorhexidine intravascular catheter gel dressing on short-term
central venous catheters. Am J Infect Control. 2016: 44(1): 54-60.
20. Safdar N, O’Horo JC, Ghufran A, et al. Chlorhexidine-impregnated dressing for prevention of CRBSIs: A meta-analysis. Crit Care Med. 2014: 42(7); 1703-1713.
21. Timsit JF, Mimoz O, Mourvillier B, Souweine B, Garrouste-Orgeas M et al. Randomised controlled trial of chlorhexidine dressing and highly adhesive dressing
for preventing CRBSIs in critically ill adults, Am J Resp Crit Care Med. 2012: 186(12): 1272-1278.
3M Health Care AcademySM
© 3M 2016. All Rights Reserved
References cont.22.Camins BC, Richmond AM, Dyer KL, et al. A crossover intervention trial evaluating the efficacy of a chlorhexidine-impregnated sponge (BioPatch®) to reduce
catheter-related bloodstream infections in hemodialysis patients. Infect Control Hosp Epidemiol. 2010; 31(11): 1118–1123.
23.Righetti M, Palmieri N, Bracchi O, et al. Tegaderm™ CHG dressing significantly improves catheter infection rate in hemodialysis patients. J Vasc Access. 2016;
17(5): 417-422.
24.Biehl LM, Huth A, Panse J, et al. A randomised trial on chlorhexidine dressings for the prevention of CRBSIs in neutropenic patients. Ann Oncol. 2016; 10: 1916-
1922.
25. Scheithauer S, et. al., Significant reduction of external ventricular drainage–associated meningoventriculitis by chlorhexidine-containing dressings: A before-
after trial, Clin Infect Dis. 2016, 62 (3): 404-405. doi: 10.1093/cid/civ887
26. Mermel, et. al., Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infection: 2009 Update by the Infectious
Diseases Society of America, Clinical Infectious Diseases, 2009; 49:1-45
27. Maki, Catheter BSI rates: Clinical Infectious Diseases, 2002; 34:1232-1262
28. Grigonis AM, Dawson AM, Burkett M, et al. Use of a central catheter maintenance bundle in long-term acute care hospitals. Am J Crit Care. 2016; 25(2): 165-
172.
29. Thokala P, Arrowsmith M, Poku E, et al. Economic impact of Tegaderm™ CHG chlorhexidine gluconate IV securement dressing in critically ill patients. J Infect
Prev. September 17, 2016; (5): 216-223.
30. International Electrochemical Commission: IEC 62366-1:2015 IEC 201
31. Mermel LA, McCormick RD, Springman SR, Maki DG. The pathogenesis and epidemiology of catheter related infection with pulmonary artery Swan-Ganz
catheters: A prospective study utilizing molecular subtyping. Am J Med. 1991; 91(36):197S–205S.
32. Maki DG, Weise CE, Sarafin HW. A semiquantitative culture method for identifying intravenous-catheter-related infection. N Engl J Med. 1977; 296(23): 1305-
1309.

3M Health Care AcademySM
© 3M 2016. All Rights Reserved
References cont.33. Segura M, Lladó L, Guirao X, Piracés M, Herms R, Alia C, Sitges-Serra A. A prospective study of a new protocol for ‘in situ’diagnosis of central venous catheter
related bacteraemia. Clin Nutr. 1993; 12(2): 103-107.
34. Raad I, Costerton W, Sabharwal U, Sadlowski M, Anaissie E, Bodey GP. Ultrastructural analysis of indwelling vascular catheters: a quantitative relationship
between luminal colonization and duration of placement. J Infect Dis. 1993; 168(2): 400-407.
35. McNichol L, Lund C, Rosen T, Gray M. Medical Adhesives and Patient Safety: State of the Science: Consensus Statements for the Assessment, Prevention, and
Treatment of Adhesive-Related Skin Injuries. J Wound Ostomy Continence Nurs. 2013; 40(4):365-380.
36. George M. Role of skin protectant in reducing the local complications in PICC lines. Poster presentation at the 2013 meeting of the Infusion Nursing Society
37. Roth RR, James WD. Microbial Ecology of the Skin. Annu. Rev. Microbiol. 1988; 42: 441-464
38. Abad CL, Safdar N. Catheter-related Bloodstream Infections. Infect Dis. (Special Edition) 2011. McMahon Publishing
39.Hitchcock J, Savine L. Medical adhesive-related skin injuries associated with vascular access. Br J Nurs. 2017; 26(8): S4-S12.
40.Broadhurst D, Moureau N, Ullman AJ. Management of Central Venous Access Device-Associated Skin Impairment: An Evidence-Based Algorithm. J Wound
Ostomy Continence Nurs. 2017; 44(3): 211-220.




























