Embed Size (px)
Citation preview

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101068Z01SA2019. www.ijcasereportsandimages.com
Aida et al. 1
CASE REPORT PEER REVIEWED | OPEN ACCESS
Budd–Chiari syndrome complicating hepatic sarcoidosis: A rare association
Saoud Aida, Bellamlih Habib, Laamrani Fatima Zahra
ABSTRACT
Introduction: The Budd–Chiari syndrome is an obstruction of the hepatic venous drainage. It is not common as a complication of hepatic sarcoidosis but the association is possible. We report a case of Budd–Chiari syndrome complicating a hepatic sarcoidosis. Case Report: A 32-year-old female patient with a history of mediastino-pulmonary, hepatic, and splenic sarcoidosis since her young age, that stopped her medication, was readmitted at our Emergency Department for recurrent threatening hematemesis. The oeso-gastroduodenal fibroscopy found esophageal varices. Biological assessment found a cytolysis and cholestasis. Hepatic Doppler ultrasound showed nodular bumpy hepatomegaly, with outflow obstruction of the hepatic veins, and a laminated aspect of the inferior vena cava that remains permeable. Abdominal computed tomography (CT) showed multinodular liver and spleen, multiple lymphadenopathies, and a lack of individualization of hepatic veins. Chest CT showed an interstitial syndrome associated with bilateral mediastinal and hilar adenopathies. Viral serologies B and C, and the search for thrombophilia were negative. Hepatic sarcoidosis was previously confirmed by liver biopsy, with a negative tuberculosis testing and a high level of angiotensin-converting enzyme. All these assessments led to the diagnosis of Budd–Chiari syndrome complicating hepatic sarcoidosis. Conclusion: Budd–Chiari syndrome is thus an exceptional complication, but possible in case of hepatic sarcoidosis. Therefore, it is
Saoud Aida1, Bellamlih Habib1, Laamrani Fatima Zahra1
Affiliation: 1Emergency Radiology Department, Ibn Sina Hos-pital, CHU of Rabat, Morocco.Corresponding Author: Saoud Aida, Secteur 15, bloc D n°19, Hay Riad, Rabat, Morocco; Email: [email protected]
Received: 29 July 2019Accepted: 16 September 2019Published: 07 November 2019
worthwhile to look for it in case of any worsening of hepatic sarcoidosis, and to suggest possible sarcoidosis in case of Budd–Chiari syndrome.
Keywords: Budd–Chiari syndrome, Hepatic sar-coidosis, Liver, Sarcoidosis
How to cite this article
Aida S, Habib B, Zahra LF. Budd–Chiari syndrome complicating hepatic sarcoidosis: A rare association. Int J Case Rep Images 2019;10:101068Z01SA2019.
Article ID: 101068Z01SA2019
*********
doi: 10.5348/101068Z01SA2019CR
INTRODUCTION
Sarcoidosis is an inflammatory disorder categorized by the presence of noncaseating granulomas, which has the ability to affect multiple organs of the body [1, 2]. The pulmonary system is the most common site of involvement (90% of cases) [1]. The liver is the third most commonly affected organ system after the lungs and lymph nodes. It has been found that 50–65% of sarcoid patients have hepatic involvement as per liver biopsy [2].
Budd–Chiari syndrome is a heterogeneous group of clinical conditions presenting with hepatic venous outflow obstruction, which can be located at any level from the small hepatic veins to the junction of the inferior vena cava with the right atrium [3]. It is classified as being primary if flow is obstructed due to an endoluminal aberration, or secondary if the flow is obstructed by compression or invasion of a lesion outside the hepatic venous outflow track [3].
The Budd–Chiari syndrome is not common as a complication of hepatic sarcoidosis but the association is possible. A dozen cases are reported in the literature, to which we add our case of Budd–Chiari syndrome in the context of a sarcoidosis with liver injury.

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101068Z01SA2019. www.ijcasereportsandimages.com
Aida et al. 2
CASE REPORT
We report the case of a 32-year-old female patient with a history of mediastino-pulmonary, hepatic, and splenic sarcoidosis since her young age, under corticotherapy. The patient was lost to follow-up for two years and she willingly stopped her medication. She was readmitted at our Emergency Department for recurrent threatening high digestive bleeding. The oeso-gastroduodenal fibroscopy found esophageal varices. Biological assessment found a cytolysis and cholestasis with elevated alkaline phosphatase (289 IU/L), gamma-glutamyltransferase (GGT) (147 IU/L), total bilirubin (5.4 mg/dL) mostly conjugated, alanine aminotransferases (ALATs) (36 IU/L), and serum alanine aminotranspeptidases (ASAT) (47 IU/L).
Hepatic Doppler ultrasound showed nodular bumpy hepatomegaly, with outflow obstruction of the hepatic veins on pulse wave and color flow Doppler, and a laminated aspect of the inferior vena cava that remains permeable.
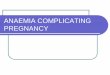
Abdominal CT showed multiple hepatic and splenic nodules enhanced after contrast injection, multiple peritoneal and retroperitoneal lymphadenopathies, and a lack of individualization of hepatic veins. The portal vein and its branches were permeable (Figures 1–3).
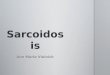
Chest CT showed an interstitial syndrome with diffuse parenchymal reticulomicronodular infiltrate associated with bilateral mediastinal and hilar adenopathies (Figure 4A and B). Viral serologies B and C were negative.
The search for thrombophilia, namely dosage of protein C, protein S, antithrombin III, nocturnal paroxysmal hemoglobinuria, antiphospholipid syndrome, Leiden’s factor V mutation, and the prothrombin gene mutation, was negative.
Figure 1: Abdominal CT with injection of contrast medium at venous time showing multinodular liver and spleen, with no visualization of the hepatic veins and a laminated inferior vena cava (red arrow).
Figure 2: Abdominal CT showing inter-aortico-cava and latero-aortic adenopathies (red arrows).
Figure 3: Abdominal enhanced CT at venous time showing heterogeneous nodular hepatomegaly with mass effect on the inferior vena cava which is laminated (red arrow).

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101068Z01SA2019. www.ijcasereportsandimages.com
Aida et al. 3
Hepatic sarcoidosis was previously confirmed by liver biopsy, which objectified noncaseating granulomas, with a negative tuberculosis testing (IDR, BK in sputum, and GeneXpert) and a high level of angiotensin-converting enzyme (97 UECA).
All these assessments led to the diagnosis of Budd–Chiari syndrome complicating hepatic sarcoidosis.
DISCUSSION
Cholestasis and portal hypertension represent the most common complications of hepatic sarcoidosis. Budd–Chiari syndrome is actually an exceptional complication of sarcoidosis. It has been reported in a dozen cases in literature [4–13]. The pathophysiology is not clearly elucidated; however, two hypotheses are proposed to explain this causality. On the one hand, the extrinsic compression of the hepatic veins by the adjacent nodules, which would lead to venous stasis with endoluminal thrombus formation [13], causing a secondary Budd–Chiari syndrome [14]. On the other hand, granulomatous infiltration of the vascular wall [11] by contiguity, without formation of vascular thrombi, could lead to a primary Budd–Chiari syndrome [14].
Clinically, depending on the number of occluded veins and the speed of occlusion, Budd–Chiari syndrome may remain asymptomatic, or manifest as hepatomegaly, abdominal pain, hepatocellular insufficiency, or ascites.
The imaging will find portal hypertension signs with suprahepatic obstacle, manifested by disorders of the flow on the Doppler ultrasound and of a lack of enhancement of hepatic veins and/or inferior vena cava, with development of collateral venous circulation. We can also find a dysmorphic liver with multiple hepatic nodules (related to hepatic parenchymal involvement of sarcoidosis), perfusion disorders, or ascites.
Treatment of Budd–Chiari syndrome will be based on the management of its etiology, in this case sarcoidosis (corticosteroids, immunosuppressants, synthetic antimalarials), the prevention of venous thrombosis and the restoration of hepatic venous drainage [15] (surgical or endovascular). Liver transplantation may be considered in patients with rapidly worsening hepatocellular insufficiency, which was the case of our patient.
CONCLUSION
Budd–Chiari syndrome is thus an exceptional complication, but possible in case of hepatic sarcoidosis. Therefore, it is worthwhile to look for it in case of any worsening of hepatic sarcoidosis, and to suggest possible sarcoidosis in case of Budd–Chiari syndrome.
REFERENCES
1. Syed U, Alkhawam H, Bakhit M, Companioni RA, Walfish A. Hepatic sarcoidosis: Pathogenesis, clinical context, and treatment options. Scand J Gastroenterol 2016;51(9):1025–30.
2. Tadros M, Forouhar F, Wu GY. Hepatic sarcoidosis. J Clin Transl Hepatol 2013;1(2):87–93.
3. Martens P, Nevens F. Budd-Chiari syndrome. United European Gastroenterol J 2015;3(6):489–500.
4. Ennaifer R, Bacha D, Romdhane H, Cheikh M, Nejma HB, BelHadj N. Budd-Chiari syndrome: An unusual presentation of multisystemic sarcoidosis. Clin Pract 2015;5(3):768.
5. Van Brusselen D, Janssen CE, Scott C, et al. Budd-Chiari syndrome as presenting symptom of hepatic sarcoidosis in a child, with recurrence after liver transplantation. Pediatr Transplant 2012;16(2):E58–62.
6. Efe C, Shorbagi A, Ozseker B, et al. Budd-Chiari syndrome as a rare complication of sarcoidosis. Rheumatol Int 2012;32(10):3319–20.
7. Sghier IA, Billah NM. Budd-Chiari syndrome: A rare complication of hepatic sarcoidosis (about one case). [Article in French]. Pan Afr Med J 2016;23:4.
8. Krishnamoorthy G, Ray G, Agarwal I, Kumar S. Unusual presentation of sarcoidosis in a child. Rheumatol Int 2012;32(5):1453–5.
9. Delfosse V, de Leval L, De Roover A, et al. Budd-Chiari syndrome complicating hepatic sarcoidosis: Definitive treatment by liver transplantation: A case report. Transplant Proc 2009;41(8):3432–4.
10. Maàmouri N, Ketari S, Habessi H, et al. Budd-Chiari syndrome in sarcoidosis. [Article in French]. Gastroenterol Clin Biol 2009;33(2):147–8.
11. Deniz K, Ward SC, Rosen A, Grewal P, Xu R. Budd-Chiari syndrome in sarcoidosis involving liver. Liver Int 2008;28(4):580–1.
12. Russi EW, Bansky G, Pfaltz M, Spinas G, Hammer B, Senning A. Budd-Chiari syndrome in sarcoidosis. Am J Gastroenterol 1986;81(1):71–5.
13. Natalino MR, Goyette RE, Owensby LC, Rubin RN. The Budd-Chiari syndrome in sarcoidosis. JAMA 1978;239(25):2657–8.
14. Valeyne D, Soler P, Tazi A, et al. Sarcoïdose. In: Kahn MF, Paltier AP, Meyer O, Piette JC, editors. Maladies et Syndromes Systémiques. Paris: Flammarion Médecine-Science; 2000. p. 1207–36.
15. Plessier A. Budd Chiari syndrome. [Article in French]. Gastroenterol Clin Biol 2006;30(10):1162–9.
*********
Figure 4 (A) and (B): Chest CT showing reticulomicronodular pulmonary parenchymal infiltration (red circle).

International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101068Z01SA2019. www.ijcasereportsandimages.com
Aida et al. 4
Author ContributionsSaoud Aida – Conception of the work, Design of the work, Acquisition of data, Analysis of data, Interpretation of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Bellamlih Habib – Analysis of data, Interpretation of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Laamrani Fatima Zahra – Analysis of data, Interpretation of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone.
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Conflict of InterestAuthors declare no conflict of interest.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Copyright© 2019 Saoud Aida et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.
Access full text article onother devices
Access PDF of article onother devices