Embed Size (px)
Citation preview

BUILDING TEAMS AND PROGRAMS FOREFFECTIVE REHABILITATION
Patrick W. Corrigan, Psy.D.
Carefully controlled, clinical research has shown psychiatric rehabilitation tosignificantly help persons with severe mental illness address their disabilitiesand obtain a higher quality of life. For psychiatric rehabilitation to yield itsgreatest effect, discrete principles and skills that are part of the rehabilitationparadigm must be disseminated to staff working in real-world settings. Stafftraining strategies that help the rehabilitation team develop effective programsare especially important. This paper reviews Interactive Staff Training (1ST),an approach to team building and program development that combines educa-tional and organizational strategies. 1ST comprises four stages—introduction tothe system, program development, program implementation, and program main-tenance—with each stage defined by behavioral tasks that engage the teamand corresponding products that serve as markers of progress. Testing treat-ment dissemination strategies poses interesting problems for the researcher,some which are reviewed here. Outcome studies completed on 1ST are summa-rized in light of these problems. The paper ends with a consideration of somefuture directions for research in this area.
Think about the immensity of the task. Develop a psychiatricrehabilitation program that brings together state-of-the-artassessments and technologies to meet the diverse goals of personsdisabled by a variety of psychiatric disorders. Make sure theteam charged with operating this program is suitably skilled tocarry out these assessments and technologies. Moreover, make
Address correspondence to Patrick Corrigan, Psy.D., University of ChicagoCenter for Psychiatric Rehabilitation, 7230 Arbor Drive, Tinley Park, IL 60477;e-mail: [email protected].
PSYCHIATRIC QUARTERLY, Vol. 69, No. 3, Fall 19980033-2720/98/0900-0193$16.00/0 © 1998 Human Sciences Press, Inc. 193
sure the team is sufficiently organized to implement the programin a timely and consumer-responsive manner. Finally, equip staffand consumers with feedback mechanisms with which the pro-gram can be regularly adjusted to meet the continually evolvingneeds of participants. Efforts to train staff, build teams, and fa-cilitate program development rest on sound clinical and dissemi-nation research.
Clinical researchers have used considerable energy to uncoverthe psychological variables that describe psychiatric disabilityand services to rehabilitate these disabilities. The fruits of clini-cal research form the basis of practice guidelines for severe men-tal illness (1, 2). In this paper, we turn to a different body ofliterature to understand strategies that facilitate the dissemina-tion of best practices. The object of study in this kind of researchis not the consumer, but rather service providers who come to-gether in teams to develop and implement rehabilitation pro-grams. Although the ultimate goal of this research is consumeroutcome—is the person better able to deal with his or her dis-ability as a result of the rehabilitation program?—examiningquestions about teams and programs includes goals about thefeasibility and user-friendliness of program components.
Research conducted by organizational psychologists is espe-cially useful for this enterprise. Organizational researchers haveidentified and tested best practices for building teams and pro-grams. In the process, they have considered various research as-sessments and strategies for measuring the effects of thesepractices. The purpose of this paper is to present Interactive StaffTraining (1ST) as a specific method for facilitating the dissemi-nation of rehabilitation strategies. 1ST blends organizational andeducational strategies and has been effectively used to dissemi-nate rehabilitation programs in Illinois and the Midwest (3,4).Specific tasks that comprise 1ST are reviewed in this paper. Inaddition, research on its outcome is summarized.
INTERACTIVE STAFF TRAINING
The assumptions that guide 1ST rest on research that has ex-amined barriers to the incorporation of innovative strategies.
194 PSYCHIATRIC QUARTERLY

This research was conducted by asking staff why they do notupdate their existing programs with newly-developed innovationsin rehabilitation. Emerson and Emerson (5) identified 15 impedi-ments to rehabilitation innovations by questioning more than 100staff at a Canadian hospital. Our group followed up this studyby asking more than 300 staff at a California agency to rate theimportance of these 15 impediments (6). A factor analysis of theirresponses yielded five constructs that describe why staff fail touse treatment innovations: (1) institutional constraints: adminis-trative practices and budgetary limitations result in insufficientresources to carry out satisfactory rehabilitation programs; (2)insufficient collegial support: the perception that other staff arenot interested in, and will not support, innovative rehabilitationprograms; (3) philosophical opposition: staff do not believe reha-bilitation practices are effective or appropriate for persons withsevere mental illness; (4) client dissatisfaction: clients and theirfamilies do not approve of many rehabilitation skills; and (5) col-lateral interference: clients, family members, and others obstructeffective rehabilitation programs.
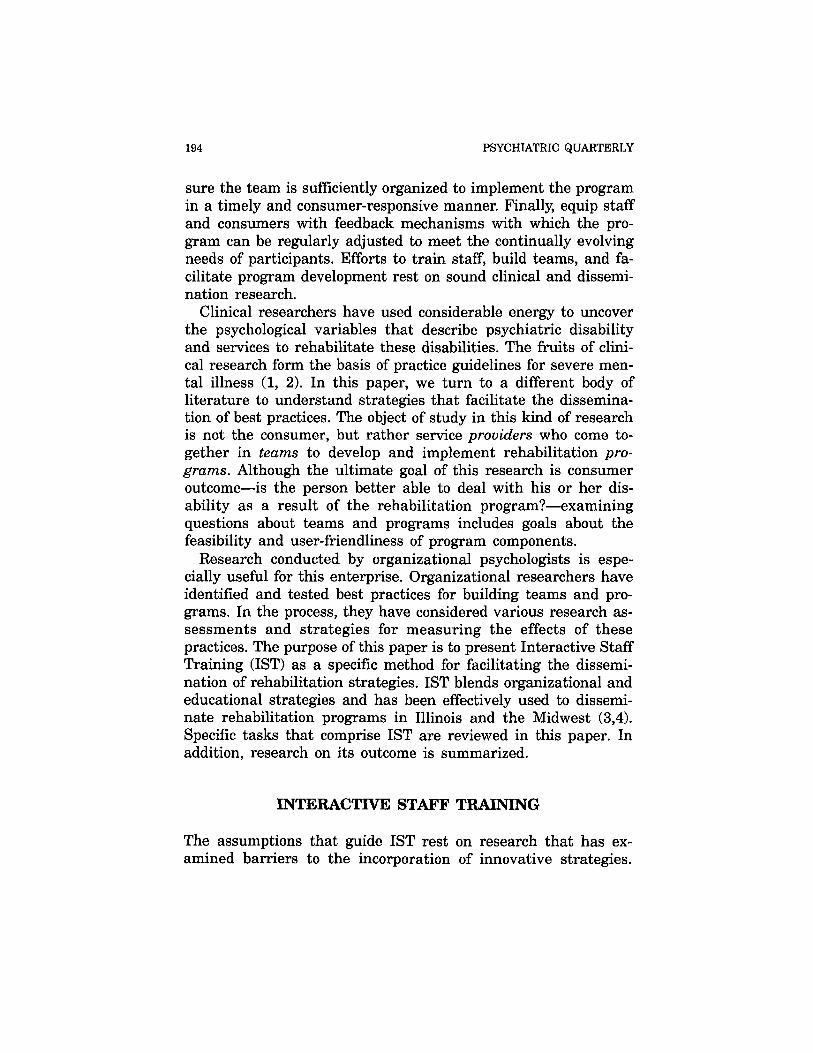
At first glance, it seems that organizational barriers—institu-tional constraints and lack of collegial support—in large part, in-terfere with the introduction of innovations into rehabilitationsettings. This assertion moves the focus of training away frommore traditional targets; namely, staff need to be educated aboutthe principles and skills with which they are unfamiliar. How-ever, additional analyses showed that the last three factors weresignificantly associated with education (5). Staff who knew moreabout rehabilitation therapies were less likely to be philosophi-cally opposed to them and were less likely to think consumersand family members were dissatisfied or interfered with reha-bilitation programs. We wondered, therefore, whether organiza-tional and educational factors independently affectedimplementation of rehabilitation innovations. To test this hy-pothesis, an analysis was conducted to determine the path be-tween two independent variables—an organizational factor(measured by indices of collegial support and burnout) and aneducational factor (measured as years of experience with specificrehabilitation therapies)—and the dependent factor (attitudesabout rehabilitation innovation). The resulting path, summarized
CORRIGAN 195
196 PSYCHIATRIC QUARTERLY
in Figure 1, suggests that organizational and educational factorsindependently affect openness about developing innovative reha-bilitation programs (7). Hence, training programs which seek tobuild teams that will develop effective rehabilitation programsmust address both the organizational and educational needs ofthese teams. Interactive staff training gets its name from an in-teraction of educational and organizational models.
Educational and Organizational Models
There has been substantial effort to develop educational pro-grams to improve the skills and knowledge of staff who provideservices for persons with severe mental illness (8, 9, 10, 11, 12,3). These programs educate staff on three types of informationnecessary to implement effective programs. (1) Team memberslearn attitudes that reflect a community-focus to treatment, con-sumer empowerment, and the optimism of recovery (13, 14, 15).For some, these attitudes replace old-school, custodial viewswhere consumers were considered to be incompetent patientsthat need to be cared for. (2) Staff learn basic knowledge aboutpsychiatric illness, especially learning to appreciate the disabili-
FIGURE 1. Findings from a path analysisshowing how organizational and educationalfactors independently affect attitudes aboutrehabilitation programs.

ties that result from psychiatric symptoms (16). They also needbasic knowledge about the range of medication and psychosocialtreatments that comprise state-of-the-art rehabilitation (17). (3)Staff master a variety of skills that comprise the actual practiceof rehabilitation. These skills are the tools with which the reha-bilitation team helps consumers meet their life goals (18).
Educational trainers have combined classroom experience withon-the-job training to help staff learn attitudes, basic knowledge,and skills. In classroom settings, staff members are provided di-dactic presentations that outline the attitudes, knowledge andskills; these lectures are frequently augmented by discussion androle plays. On-the-job training provides hands-on opportunitiesto try out newly learned skills. Staff members receive correctivefeedback from supervisors as they try out newly-learned skillswith their clientele. Staff fine tune these skills based on reactionsof clients and supervisors.
As our earlier research suggests, educational strategies are notenough to change actual practices of rehabilitation staff. Organ-izational barriers also impede the implementation of innovativerehabilitation programs. Industrial and organizational psycholo-gists have developed several training and development strategieswhich are useful for improving the coordinated functioning of therehabilitation team. Total quality management (TQM), developedby W. Edwards Deming, provides an excellent paradigm for themental health team (3, 19, 20). According to proponents of TQM,training and development must reflect the needs of stakeholdersassociated with the program. A rehabilitation program is ulti-mately judged by the consumer's perception of its quality. Con-sumers of rehabilitation programs include the persons whoparticipate in the program to address psychosocial goals as wellas family members and others who are concerned about the per-son's disabilities. Hence, consumer perceptions of program rele-vance and efficacy are essential for setting up staff trainingprograms.
The other relevant group in the TQM needs assessment is thestaff. They are viewed as internal consumers in a TQM model(21). They have needs (in addition to a steady income) which arealso satisfied by participating in the rehabilitation program; feel-ings of personal accomplishment and collegiality at work, abilities
CORRIGAN 197
to adequately meet clients' goals, and coping with job stress aresome examples. Hence, staff opinion about the focus of trainingand development efforts is also essential.
Beyond assessing consumer and staff perceptions, TQM es-pouses two other principles that are important for training anddevelopment: participative decision making and data-driven feed-back. According to TQM, all decisions about the development ofinnovative programs need to be made by the stakeholders whoimplement them. This may require educating stakeholders aboutthe range of options from which they might select a specific strat-egy to further design a program. For example, when developinga vocational rehabilitation program, the team may select fromsupported employment, job training, limited job coaching, andsheltered employment strategies. Once knowledgeable aboutthese options, the decision about which option to develop, andways to actually implement them, needs to rest with the teamof professionals who carry them out. Teams that actively partici-pate in decisions about their program are more committed to thatprogram and more likely to carry it out.
Once the team has made decisions about changing the pro-gram, they need to collect data to regularly assess the impact ofthat program on various stakeholders. This includes evaluatingwhether a program has a positive effect on the consumer's dis-abilities and whether the program is user-friendly to staff car-rying it out (22). Information from this kind of continuous qualityassessment leads to ongoing improvements in the program.
1ST has a double meaning. Conceptually, 1ST rests on an in-teraction of educational and organizational training models thataddress both team and system issues that underlie the develop-ment of innovative rehabilitation programs. 1ST also refers tothe quality of interactions between trainers and team members.Traditional training is often dominated by an expert trainer whoprovides information in classroom situations. The goal of thiskind of training is to teach state-of-the-art principles which needto be absorbed by the rehabilitation team. Experts are trying tobestow upon students the one way which research shows practiceshould best occur.
The quality of interactions in 1ST is markedly different. The1ST facilitator is expert in a set of rehabilitation principles and
198 PSYCHIATRIC QUARTERLY

CORRIGAN 199
skills. The facilitator is also knowledgeable about various insti-tutional forces that affect the presentation of these principles andskills. Members of the rehabilitation team, however, are expertin the organizational dynamics of their setting. They know bestthe goals of their consumers. They know best the strengths andlimitations of the current team. The 1ST facilitator needs to bevigilant to the perceptions of these local experts to make surethat best practices fit into the real needs of their program.
The Steps That Comprise Interactive Staff Training
Interactive staff training was developed as a behavior packagewhich trainers might adopt to help rehabilitation teams developand implement effective programs. A brief summary of 1ST isprovided here; readers should consult Corrigan and McCracken(4) for a more thorough discussion. As outlined in Figure 2, In-teractive Staff Training (1ST) comprises four stages: Introductionto the System, Program Development, Program Implementation,and Program Maintenance. Each stage is defined by two or threetasks and corresponding products. The tasks are discrete behav-ioral steps which the 1ST facilitator completes with the team or
FIGURE 2. The four stages and corresponding tasks that make upInteractive Staff Training.

other key stakeholders. The products are indices of the team'sprogress towards development of a more enriched program.
During the first stage of 1ST—Introduction to the System—1STfacilitators try to be accepted by the rehabilitation team so thatstaff members are willing to work with them in developing, andeventually implementing, various rehabilitation programs. Al-though the focus of 1ST is the line-level rehabilitation team, fa-cilitators' efforts will only be successful with the explicit supportof institutional administrators. Hence, the consultant begins withthe executive director by educating him or her to the componentsof 1ST and getting his/her public support to proceed.
Team members are then engaged through a staff and consum-ers' needs assessment. Team members are most likely to imple-ment intervention programs that reflect their perceptions ofimportant consumer care and milieu management issues. A pro-file of programmatic needs may be obtained through various sur-vey methods (22). Team members and consumers could be askedto complete a written questionnaire about their views of the pro-gram. Alternatively, they might participate in focus groups wherethey can share views about current interventions (23). The re-sults of the needs assessment are then summarized for teammembers. Subsequent discussion of survey results leads to agree-ment on a direction for program development. Selecting the di-rection for program development is facilitated by presenting theteam with a menu of rehabilitation strategies from which teammembers select appropriate intervention protocols to address pro-gram development goals.
Next, individuals from within the existing team, who will de-velop and operate the rehabilitation program, are assembled asa program committee charged with developing provisional pro-gram changes which will then be considered by the team as awhole. The efforts of the program committee are greatly facili-tated when at least one staff member is identified as a programchampion (24, 25, 26). This tends to be an energetic and opti-mistic individual who wants responsibility for convening the pro-gram committee and keeping the group focused on developmenttasks. Facilitators know they have successfully introduced them-selves to the system when the executive director has publicly en-dorsed 1ST; teams have identified their program development
200 PSYCHIATRIC QUARTERLY

needs; they have picked a direction from the menu of programoptions that addresses these needs; and they have selected achampion, a colleague who will lead the team in framing out thisoption.
Efforts to frame out the selected option—the Program Devel-opment Stage of 1ST—begin after the program committee andchampion are seated. The 1ST consultant introduces the programcommittee to the principles and services described in the researchliterature that are relevant to the option selected as a result ofthe needs assessment. This information provides a useful outlineof the ideal rehabilitation program. The program committee isthen engaged in making decisions about how the ideal programwill be adapted to meet the needs of its consumers and staff.This process is participative decision making (27, 28, 29).
The 1ST consultant uses his or her expertise to help the com-mittee evaluate the outlined program after they make initial de-cisions about the targeted rehabilitation program. Socraticquestioning is a useful means for accomplishing this goal (30,31). Rather than asserting a weakness or limitation of a program,the purpose of Socratic questions is to help the champion andprogram committee evaluate the cost and benefits of specific pro-gram choices. Sometimes a certain line of Socratic questions leadsthe committee to realize that they do not have enough informa-tion about a component of the rehabilitation strategy. The 1STfacilitator takes advantage of these learning opportunities byteaching curious team members about the specific component.Traditional education strategies are used for this purpose.Clearly, however, classroom-based training, grounded in 1ST, hasa different quality from more traditional approaches. Now teammembers are studying rehabilitation strategies that they identi-fied as important and relevant to their plan of care. Moreover,their current need to transpose the particular strategy into auser-friendly program makes them significantly more attentiveto the classroom-based training sessions.
A date is set to implement the drafted program after severalmonths of planning. This is the Program Implementation Stageof 1ST. The program committee and rehabilitation team need topilot the program before a full-fledged trial occurs. Testing adrafted program during a pilot uncovers weaknesses in the
CORRIGAN 201

newly-developed program. Pilots are only conducted by a sub-group of team members with a subset of consumers; the programcommittee should not attempt to implement a new program withall staff and consumers until some of the more obvious pitfallshave been worked out.
The program committee needs to adopt a revisionist approachto changing components of the newly designed program that havebeen found deficient during the pilot. D'Zurilla (32, 33) developeda multi-step strategy for evaluating interpersonal problems; thisstrategy has been used to revise drafted programs. Through thisprocess, program committees and treatment teams are taughtthat limitations in a rehabilitation program are problems thatcan be fixed, rather than overwhelming difficulties which indicatethat the program should be abandoned.
The last stage of 1ST is Program Maintenance; the team setsup structures that support the newly developed program over thelong term. Continuous quality improvement (CQI) is an institu-tional effort that has been shown to help maintain efficient pro-grams over time (20). In many ways, CQI activities parallel theproblem solving steps that occur during the pilot. Staff membersare encouraged to brain storm questions about the efficacy of aprogram which then lead to plans of correction. The 1ST facili-tator might share various resources that provide strategies rele-vant to the plan of correction. The committee then sifts throughthis information to decide on the best solutions.
The success of a CQI program depends on the data that testthe plan of correction. Unfortunately, without 1ST consultationteam members engaged in CQI are frequently seduced by state-of-the-art psychological assessments rather than meaningfuldata gathering instruments. As a result, measures are selectedwhich cannot be reliably gathered by busy staff. Ironically, someof the data necessary for CQI is already collected during thecourse of a rehabilitation program. Information about the effectsof the entire program, and about plans of correction to fix theseprograms, can be obtained easily from these sources. For exam-ple, the effects of social skills training can be determined byrating the quality of interactions in role plays held during train-ing classes.
202 PSYCHIATRIC QUARTERLY
Efforts from the previous nine steps of 1ST help the rehabili-tation team become a united body that has learned strategies fordeveloping programs that meet consumer and staff needs. Thecontinued success of 1ST rests, in part, on the efforts of the fa-cilitator. To assure that these accomplishments do not fade whenthe facilitator leaves, an organizational champion needs to beidentified and educated to assume the functions of the 1ST con-sultant. The organizational champion is typically selected fromteam members at the rehabilitation agency. Organizationalchampions might be central administrators or could be drawnfrom the ranks of the line-level staff. Regardless of background,their task is clear; organizational champions master the othernine steps of 1ST and assume responsibility for continuing or-ganizational development and support activities with the treat-ment team.
CONDUCTING RESEARCH ON TRAINING ANDDEVELOPMENT
The definition of careful research broadens when consideringtreatment dissemination strategies like 1ST. This is evident inThomas and Rothman's (34) distinction of the three types of re-search needed to investigate the effects of a staff training anddevelopment package: basic psychological research, which in re-habilitation domains, seeks to understand the course and impli-cations of psychopathology; clinical research, which uses theresults of basic psychological research to develop and evaluatetherapies which modify psychopathology; and dissemination re-search, which evaluates strategies for transferring clinical strate-gies into real-world settings. The rules and values that describegood methodology vary across intervention research enterprises(35, 36, 37). Research that addresses questions of basic psychol-ogy and clinical practice is dominated by internal validity issueswhile dissemination investigators concern themselves with exter-nal validity. Dissemination researchers are especially interestedin the generalizability of an intervention; is Intervention A rele-vant for a large number of consumers suffering a particular prob-lem and for the professionals charged with providing care for
CORRIGAN 203

these consumers? In addition, dissemination research is con-cerned with the utilizability of an intervention. Effective inter-ventions are valuable when they are user-friendly to theconsumers and clinicians who must partake them. Because in-ternal and external validity are inversely related, disseminationresearch focusing on external validity is often judged harshly byclinical investigators (38). This judgement neither promoteshealthy doses of research on dissemination strategies nor encour-ages discussion of alternative research designs which might ad-dress dissemination questions (35, 39).
Dissemination research also targets a broader set of dependentvariables when assessing the impact of training and developmentstrategies; these levels of measurement are hierarchically listedin Table 1. Many training and development programs begin as-sessment by considering staff satisfaction with the training proc-ess. Are staff more interested in and satisfied with a specific setof rehabilitation principles and strategies after training? Interestin and satisfaction with rehabilitation principles and practiceswould seem to precede staff knowledge. Assessing the knowledgedomain addresses questions like, as the result of training, havestaff learned more information about severe mental illness anda specific set of rehabilitation principles and strategies? More
TABLE 1
Levels of Measurement in DisseminationResearch
Level 1: Staff Interest and Satisfaction
Level 2: Staff Knowledge
Level 3: Staff Treatment Behavior
Level 4: Consumer Interest and Satisfaction
Level 5: Consumer Treatment Behavior
Level 6: Consumer Disabilities
204 PSYCHIATRIC QUARTERLY

knowledge about mental illness and effective rehabilitationshould lead to actual change in rehabilitation practices, Level 3measurement. Hence, the next level of measurement in dissemi-nation research is staff treatment behavior: do staff actuallychange the way in which they conduct the rehabilitation programafter training? This includes whether staff-consumer interactionsimprove and whether the range of activities that are therapeuticbroaden.
Changes in staff behavior are ultimately valued if they lead tochange in consumer behavior. Three levels of consumer behaviorare assessed to determine the impact of training and develop-ment. Consumer interest and satisfaction: as a result of staffchange, do consumers perceive the program as more relevant totheir needs? Greater interest in the program should lead tochanges in consumer participation in the program. Level 5 as-sessment examines whether consumers are "acting" differentlyat the rehabilitation program, actions which are likely to helpresolve their disabilities. Perhaps the ultimate arbiter of success-ful program change is measuring improvement in consumer dis-abilities. Do consumers show diminished disabilities andimproved quality of life as the result of participating in the re-habilitation program?
Units of analysis also vary in dissemination research. Units ofanalysis are the object of study and might include individual staffmembers or the team of service providers. Successful staff train-ing and program development may have their effects on individ-ual staff members; they may report less burnout and moremotivation to learn new interventions. Individual staff membersmay show greater knowledge about rehabilitation and a greaterrate of using specific rehabilitation skills. Individual consumersmay show greater satisfaction in the program and greater reha-bilitation of their disabilities. Individual units of analysis wouldthen be incorporated into the research design; these are com-monly the object of clinical research.
Contrast the individual level of analysis to system or grouplevels of analysis which are more commonly used in industrial/or-ganizational research. This kind of research views the impact oftraining and development strategies on the team, not on the in-dividual staff member. It parallels the rationale of family therapy
CORRIGAN 205

and research; namely, activity of the family is best understoodby considering the gestalt of interactions among all members.Similarly, the impact of a training and development program isbest understood by considering the attitudes and activity of theteam as a whole. Hence, the goal of research might be to deter-mine whether the entire team is implementing different strate-gies after training.
Studies using the team as the unit of analysis enlarges theresearch enterprise tremendously. Examining questions using in-dividual staff as units of analysis can be done with about 60staff in one or two settings. For example, staff could be randomlyassigned to education versus 1ST conditions and determine itseffect on burnout and collegial support. Using teams as the unitof analysis in a randomized experimental design requires a muchlarger sample to achieve equal power. For example, a study cur-rently conducted by our group involves fifty teams made up ofmore than 1000 staff serving more than 10,000 consumers (40).Investigators have used quasi-experimental research strategieslike the time series design to examine questions involving teamunits of analysis (41).
Research on 1ST
Three studies have examined the impact of 1ST on the six levelsof measurement using both units of analysis. The first study in-corporated an individual unit of analysis and focused on staffburnout and attitudes. The impact of nine months of 1ST on 35staff members was examined in this investigation (42). Resultsshowed significant reductions in burnout, improvements in col-legial support, and increments in attitudes about program devel-opment. Interestingly, these effects interacted with staff roles.Namely, nursing staff charged with more face-to-face interactionswith the client showed greater reductions in burnout than clinicalstaff like psychiatrists, psychologists, and social workers whoseactivities were restricted to infrequent therapy sessions.
A second study used a team level of analysis to examinewhether 1ST led to actual change in the behavior of staff con-ducting a rehabilitation program in a residential setting (43). Re-sults showed increases in staff participation from zero to more
206 PSYCHIATRIC QUARTERLY
than 75% of the team. Moreover, consumers increased participa-tion in the targeted rehabilitation strategies from less than 10%to more than 85% of the population attending that rehabilitationcenter. Finally, results suggested a 40% reduction in aggressionas a result of changes in the rehabilitation program. This studyshowed improvements in three levels of measurement: staff treat-ment behavior, consumer participation in treatment, and con-sumer outcome.
A third study had similar results using a time-series designmeasuring changes in staff behavior related to the rehabilitationprogram, and consumer response to that program (43). This studyused a team level of analysis and examined staff and consumervariables. Results showed burnout diminished across the team.Staff attitudes about rehabilitation innovations, and the actualimplementation of these innovations, improved significantly. Con-sumer satisfaction with the rehabilitation program improved andoverall consumer outcome showed significant change.
Like most interventions, 1ST is a work in progress, a programdevelopment package with a good base of empirical support. Fu-ture research needs to continue to examine the effects of 1ST onprogram change, on the team who is charged with carrying outthis program, and on the consumers who benefit from its imple-mentation. Combinations of educational and organizationalstrategies offer the greatest promise for assisting rehabilitationteams in the development of programs that meet consumer needseffectively.
REFERENCES
1. Crits-Christoph P: The dissemination of efficacious psychological treatments.Clinical Psychology: Science and Practice 3:260-263, 1996.
2. Havik OE, VandenBos GR: Limitations of manualized psychotherapy foreveryday clinical practice. Clinical Psychology: Science and Practice 3:264-267, 1996.
3. Corrigan PW, McCracken S: Refocusing the training of psychiatric rehabili-tation staff. Psychiatric Services 46:1172-1177, 1995.
4. Corrigan PW, McCracken SG: Interactive staff training: Rehabilitationteams that work. New York, Plenum Press, 1997a.
5. Emerson E, Emerson C: Barriers to the effective implementation of habili-tative behavioral programs in an institutional setting. Mental Retardation25:101-106, 1987.
CORRIGAN 207

6. Corrigan PW, Kwartarini WY, Pramana, W: Barriers to the implementationof behavior therapy. Behavior Modification 16:132-144, 1992.
7. Corrigan PW, Williams OB, McCracken SG, et al: Staff attitudes that im-pede the implementation of behavioral treatment programs. Behavior Modi-fication, In Press.
8. Cook JA, Yamaguchi J, Solomon ML: Field-testing a post-secondary facultyin-service training for working with students who have psychiatric disabili-ties. Psychosocial Rehabilitation Journal 17:157-170, 1993.
9. Kuehnel TG, Liberman RP: Competency-based training of psychiatric prac-titioners in the rehabilitation of the chronic mental patient. Edited byJohnson DL. Service needs for the seriously mentally ill: Training implica-tions for psychology. Washington, American Psychological Association, 1990.
10. Paul GL, Mclnnis T: Attitudinal changes associated with two approachesto training mental health technicians in milieu and social learning pro-grams. Journal of Consulting and Clinical Psychology 42:21-33, 1974.
11. Rogers ES, Cohen BF, Danley KS, et al: Training mental health workersin psychiatric rehabilitation. Schizophrenia Bulletin 12:709-719, 1986.
12. Wallace C, Liberman RP, MacKain SJ, et al. Effectiveness and replicabilityof modules for teaching social and instrumental skills to the severely men-tally ill. American Journal of Psychiatry 149:654-658, 1992.
13. Anthony WA: Recovery from mental illness: The guiding vision of the mentalhealth service system in the 1990s. Psychosocial Rehabilitation Journal16:11-23, 1993.
14. Deegan PE: Recovery as a journey of the heart. Psychiatric RehabilitationJournal 19:91-97, 1996.
15. McLean A: Empowerment and psychiatric consumer/ex-patient movementin the United States: Contradictions, crisis and change. Social Science andMedicine 40:1053-1071, 1995.
16. Spaulding W, Sullivan M: From laboratory to clinic: Psychological methodsand principles in psychiatric rehabilitation, in Handbook of psychiatric re-habilitation. Edited by Liberman RP. Boston, Allyn and Bacon, 1992.
17. Liberman RP: Handbook of psychiatric rehabilitation. New York, PergamonPress, 1992.
18. Corrigan PW, Rao D, Lam C: Psychiatric rehabilitation, in Case Manage-ment Desk Reference. Edited by Chan F, Leahy ML, In Press.
19. Sluyter GV, Barnette JE: Application of total quality management to mentalhealth: A benchmark case study. Journal of Mental Health Administration22:278-285, 1995.
20. Sluyter GV, Mukherjee AK: Total quality management for mental healthand mental retardation services: A paradigm for the 90's. Annandale, VA,National Association of Private Residential Resources, 1993.
21. Leebov W, Ersoz CJ: The health care manager's guide to continuous qualityimprovement. Chicago, American Hospital Publishing, 1991.
22. Corrigan PW, Luchins DJ, Malan RD, et al: User-friendly continuous qualityimprovement for the mental health team. Medical Interface 7:89-95, 1994.
23. Krueger RA: Focus groups: A practical guide for applied research. ThousandOaks CA, Sage Publications, 1994.
24. Backer T, Liberman R, Kuehnel T: Dissemination and adoption of innovativepsychosocial interventions. Journal of Consulting and Clinical Psychology54:111-118, 1986.
208 PSYCHIATRIC QUARTERLY
25. Corrigan PW: Wanted: Champions of rehabilitation for psychiatric hospitals.American Psychologist 40:514-521, 1995.
26. Corrigan PW, Holmes EP, Luchins D: Identifying staff advocates of behav-ioral treatment innovations in state psychiatric hospitals. Journal of Behav-ior Therapy and Experimental Psychiatry 24:219-225, 1993.
27. Bowditch JL, Buono AF: A primer on organizational behavior, 2nd ed. NewYork, Wiley, 1994.
28. Hackman RJ, Wageman, R: Total quality management: Empirical, concep-tual, and practical issues. Administrative Science Quarterly 40:309-342,1995.
29. Spector PE: Perceived control by employees: A meta-analysis of studies con-cerning autonomy and participation at work. Human Relations 39:1005-1016, 1986.
30. Overholser JC: The Socratic method as a technique in psychotherapy su-pervision. Professional Psychology: Research and Practice 22:68-74, 1993a.
31. Overholser JC: Elements of the Socratic method: II. Inductive reasoning.Psychotherapy 30:75-85, 1993b.
32. D'Zurilla TJ: Problem solving therapy: A social competence approach to clini-cal intervention. New York, Springer Press, 1996.
33. D'Zurilla TJ, Goldfried MR: Problem solving and behavior modification.Journal of Abnormal Psychology, 78:107-126, 1971.
34. Thomas EJ, Rothman J: Intervention research: Design and development forhuman service. New York, Haworth Press, 1994.
35. Corrigan PW, McCracken SG. Intervention research: Integrating practiceguidelines with dissemination strategies. Applied and Preventive Psychol-ogy, 6:205-209, 1997.
36. Martinez-Brawley EE: Knowledge diffusion and transfer of technology: Con-ceptual premises and concrete steps for human services innovators. SocialWork 40:670-682, 1995.
37. Rothman J: Intervention research: Application torunaway and homelessyouths. Social Work Research and Abstracts 25:13-18, 1989.
38. Paul GL, Stuve P, Cross JV: Real-world inpatient programs: Shedding somelight. Applied and Preventive Psychology, 6:193-204, 1997.
39. Rooney RH: Disseminating intervention research in academic settings—Aview from social work, in Intervention research: Design and developmentfor human service. Edited by Rothman J, Thomas EJ. New York, HaworthPress, 1994.
40. Corrigan PW, Garman AN, Lam C, Leary M: Factors in effective teamworkand team leadership in mental health settings. Administration and PolicyIn Mental Health, In Press.
41. Kratochwill TR: Single subject research: Strategies for evaluating change.New York, Academic Press, 1978.
42. Corrigan PW, Holmes EP, Luchins D, et al: The effects of interactive stafftraining on staff programming and patient aggression in a psychiatric in-patient unit. Behavioral Interventions 10:17-32, 1995.
43. Corrigan PW, McCracken SG, Kommana S, et al: Changing staff attitudesabout behavioral rehabilitation programs. Psychiatric Services 48:1336-1338,1997.
CORRIGAN 209






















![Occupational Rehabilitation Programs Presented by: [name]](https://img.pdfslide.net/doc/110x75/5a4d1af77f8b9ab059982005/occupational-rehabilitation-programs-presented-by-name.jpg)