Embed Size (px)
Citation preview

Buprenorphine
in
Primary CareEric Olson, MD, FAAFP
Board-Certified Family Medicine and Addiction Medicine
March 26, 2021

Disclosures
No financial disclosures
I am addicted to fishing. I have no desire to Cut down, I do get Annoyed
when criticized for this, I do not feel Guilty for this, I frequently have an Eye-
opener fishing trip.

Acknowledgements
I appreciate assistance from:
PCSS-MAT for borrowed slides (from Half-and Half Buprenorphine waiver
course)
James Walsh at Swedish Addiction Recovery Services in Ballard for slides and
expert knowledge
Steve Aguilu for assistance with PowerPoint and Zoom

Objectives
Understand buprenorphine pharmacology
Understand how buprenorphine can be useful in chronic pain
Review legal issues in prescribing buprenorphine
Brief review of recent trends in Addiction Medicine
Medications for alcohol use disorder (if time allows)

Buprenorphine Pharmacotherapy
Partial agonist at mu opioid receptor
High affinity at mu receptor
Antagonist at kappa opioid receptor
Poor oral availability (first pass metabolism)

Major Features of Buprenorphine
Partial agonist at mu receptor
▪ Comparatively minimal respiratory
suppression and no respiratory arrest
when used as prescribed
Long acting
▪ Half-life ~ 24-36 Hours
High affinity for mu receptor
▪ Blocks other opioids
▪ Displaces other opioids
• Can precipitate withdrawal
Slow dissociation from mu receptor
▪ Stays on receptor for a long time
SAMHSA, 2018
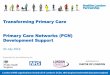
Orman & Keating, 2009
full agonist(e.g. morphine,
methadone)
partial agonist(buprenorphine)
antagonist(naloxone,
naltrexone)
dose
mu o
pio
id e
ffects

Major Features of Naltrexone
Full Antagonist at mu receptor
▪ Competitive binding at mu receptor
Long acting
▪ Half-life:
• Oral ~ 4 Hours
• IM ~ 5-10 days
High affinity for mu receptor
▪ Blocks other opioids
▪ Displaces other opioids
• Can precipitate withdrawal
Formulations
▪ Tablets: Revia®: FDA approved in 1984
▪ Extended-Release intramuscular
injection: Vivitrol®: FDA approved in
2010
SAMHSA, 2018
full agonist(e.g. morphine,
methadone)
partial agonist(buprenorphine)
antagonist(naloxone,
naltrexone)
dose
mu o
pio
id e
ffects

Buprenorphine
▪ Semi-synthetic analogue of thebaine
▪ Approved by the FDA in 2002 as a Schedule III
medication for the treatment of opioid use disorder
▪ Metabolized in the liver, mainly by cytochrome
P450 3A4 (CYP3A4), and has a less-active
metabolite, norbuprenorphine
▪ Most buprenorphine is ultimately excreted into the biliary tract,
but small fractions enter the urine and are detectable in urine
drug tests
▪ Because of extensive first-pass metabolism, buprenorphine has
poor oral bioavailability when swallowed (<5%), and all therapeutic
formulations use other routes
▪ Sublingual administration bypasses first-pass metabolism and
allows bioavailability around 30%Mendelson et al., 1997
SAMHSA, 2016, 2016
SAMHSA, 2018

How Does Buprenorphine Work?
AFFINITY is the strength with which a drug physically binds to a receptor
Buprenorphine has strong affinity; will displace full mu receptor agonists like heroin and methadone
Receptor binding strength, is NOT the same asreceptor activation
DISSOCIATION is the speed (slow or fast) of disengagement or uncoupling of a drug from the receptor
Buprenorphine dissociates slowly
Buprenorphine stays on the receptor a long timeand blocks heroin, methadone and other opioidsfrom binding to those receptors
NOTE: It is unlikely to block all effects from an opioid taken after initiation of buprenorphine treatment. Because binding to mu receptors is a dynamic process; while effects may be less, they are not likely to be completely eliminated.

Common Adverse Effects
of Buprenorphine
▪ Headaches
Management: aspirin, ibuprofen, acetaminophen (if there are no contra-indications)
▪ Nausea
Management: Consider spitting the saliva out after adequate absorption instead of swallowing.
▪ Constipation
Management: Stay well-hydrated, Consume high-fiber diet, Consider stool softeners, laxatives, naloxegol
▪ Xerostomia (Dry mouth) – side effect of ALL opioids
Complications: Gingivitis, Periodontitis
Management: Stay well-hydrated, Maintain good oral hygiene
SAMHSA, 2018
Wald, 2016

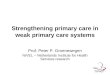
Buprenorphine Dosing: Safety
▪ Nearly all fatal poisonings involve multiple substances
Buprenorphine dose (mg)
Resp
irato
ry r
ate
(bre
ath
s/m
in)
Buprenorphine dose (mg)
Oxygen s
atu
rati
on (
%)
Hakkinen et al., 2012
Walsh et al., 1994
▪ Cognitive and psychomotor effects appear to be negligible.
▪ Respiratory rate slowed but has as a plateau effect in adults.

Buprenorphine and Benzodiazepines
▪ Benzodiazepines are present in most fatal poisonings involving buprenorphine
▪ Used as prescribed benzodiazepines in combination with buprenorphine have
been associated with more accidental injuries, but not with other safety or
treatment outcomes
Bardy et al., 2015
Jones et al., 2012
Nielsen & Taylor, 2005
Schuman-Olivier et al., 2013


Buprenorphine for Opiate Dependence
Beyond the Scope of this lecture, but briefly:
MOUD (Medication for Opiate Use Disorder) is life-saving and life-changing
I strongly encourage ALL PCPs to take a buprenorphine waiver course
Using medication to treat substance use disorders is a critical part of primary
care.
You must complete a buprenorphine training course and receive a new DEA#
before prescribing buprenorphine FOR OPIOID DEPENDENCE

Poll Question
Do you have your Buprenorphine Prescribing Waiver?
A. Yes, and I am prescribing buprenorphine.
B. Yes, but I am not yet prescribing buprenorphine.
C. No, but I am thinking about taking the training.
D. What is a buprenorphine waiver?

Buprenorphine in Chronic pain
Only patches and liquid are approved for pain management
Use of other formulations is Off-Label
Keep in mind how pharmacology impacts medication effects
All forms may relieve pain
Buprenorphine Waiver is required to prescribe buprenorphine if OUD is
present

Buprenorphine Formulations
▪ Choice of formulations is based on: Insurance/Third party payer considerations
Patient preferences
Safety
Decreased Diversion potential
▪ Formulations: Buccal film; Sublingual films
Tablets
Subdermal implants
Depot formulation given as a subcutaneous injection
▪ All of the approved forms have demonstrated similar efficacy for
treating opioid use disorder
▪ Buprenorphine for transdermal (via patch) and intravenous (via
injection) use are available for analgesic use. They were tested but
not approved for treating opioid use disorder
SAMHSA, 2016, 2016

Buprenorphine Formulations for
Opioid Use Disorder

Acute Pain Management in
Buprenorphine Maintained Patients▪ Different Approaches:
• Initially try non-opioid
analgesics (ketorolac or
NSAIDs)
• Continue Same buprenorphine maintenance dose but add non-opioid analgesics
• Use split dose for concurrent pain and dependence
• Buprenorphine’s analgesic duration is only a few
hours
• Stop buprenorphine and initiate full agonist therapy

Perioperative Management
▪ General:
Patients fear mistreatment,
Providers fear deception
Lack of consensus in the field
– often based on the preference of the
surgical/anesthesia teams
▪ Pre-Op:
Confirm Multi-Party Consent and Coordination of care with
providers
If patient is already on Partial Agonist:
Take last Buprenorphine maintenance dose 24-hours prior to surgery
Higher dosing of short-acting opioids may be required post-surgical
Merrill et al., 2002
Wenzel et al., 2016

Post Op Options for Patients already on
Buprenorphine
Merrill et al., 2002
Wenzel et al., 2016

Chronic Pain Patients
▪ Consider consulting a
pain medicine
specialist
▪ Consider Multidisciplinary
Team Approach
▪ Try non-opioid and
adjuvant analgesics
▪ Consider non-pharmacologic therapies


Legal Aspects of Prescribing
Buprenorphine
FDA has approved only patches and injectable liquid for treating pain
Use of other formulations for pain is considered Off-Label
If prescribing for a patient with Opioid Use Disorder then waiver is required
When in doubt, do not prescribe without the waiver

DSM V Criteria Loss of Control
Larger amounts, longer time
Inability to cutback
More time spent, getting, using,
recovering
Activities given up to use.
Craving
Physiologic
Tolerance
Withdrawal
Consequences
Hazardous use
Social or interpersonal problems related
to use
Neglected major roles to use
Continued use after significant problems.
• A substance use disorder is
defined as having 2 or
more of these symptoms in
the past year
• Tolerance and withdrawal
alone don’t necessarily
imply a disorder.
• Severity is related by the
number of symptoms.
2-3 = mild
4-5 = moderate
6+ = severe

Pivotal Milestones in Treatment

DATA 2000 – Practitioners Requirements
▪ Licensed provider with DEA Registration
▪ Subspecialty training in addictions or completion
of an 8-hour course
▪ Registration with SAMHSA and DEA
▪ Must affirm the capacity to refer patients for appropriate counseling and
ancillary services
▪ Must adhere to patient panel size limits
30 during the first year
Eligible to apply for increase to 100 after the first year
May apply to increase to 275 after being at 100 for a year and meeting specific
criteria.

Drug Addiction Treatment Act
(DATA 2000)Permitted physicians who met certain
qualifications to treat opioid addiction
with:
Schedule III, IV, and V narcotic medications that had
been specifically approved by the FDA or combination
of such drugs for the treatment of opioid dependence
In treatment settings other than the traditional Opioid
Treatment Program ("methadone clinic") settings
DATA, 2000

Urine Drug Testing
Rapid Testing
Convenient
Inexpensive
Less Accurate
Gas Chromatography (Reference Lab)
Delayed Results
Expensive
More Accurate

General Goals of Drug Testing in
Office-Based Treatment
Important and routine component of treatment
Urine testing can be viewed as
a means for helping the provider
to help the patient
Testing is not meant to "catch" the
patient, and a positive test result should
not simply lead to discharge from treatment, but an opportunity for reviewing the
patient’s Recovery Management

Screening and Confirmatory Tests
▪ A common clinical approach:
Test for a panel of commonly-used substances using screening
tests
Then to perform confirmatory tests for:
Positive results whose accuracy is important for treatment planning
Periodic general screening assessing commonly used substances that are not evident
on POCT
Identification of prescribed medications or metabolites
▪ Confirmatory testing is not necessary at every visit
DuPont et al., 2013
Moeller et al., 2017
SAMHSA, 2012

Common Tests
▪ Some commonly-used screening tests include:
Benzodiazepines
Cannabinoids
Amphetamines
Cocaine metabolite (benzoylecgonine)
Opiates (detects morphine, codeine, and metabolites)
Less commonly-used screening tests include:
Alcohol metabolite (ethyl glucuronide or ethyl sulfite)
Buprenorphine
Fentanyl
Oxycodone
Methadone
Moeller et al., 2017
these and other synthetic opioids
require specific tests—they are not
detected by the test for opiates

Testing for Buprenorphine
▪ Confirmatory testing will distinguish buprenorphine and its metabolite,
norbuprenorphine, which is usually present in greater concentrations
▪ Individuals vary in the ratio of buprenorphine to norbuprenorphine due to
individual metabolism and co-administered inducers or inhibitors of CYP3A4
▪ Buprenorphine with little or no metabolite (i.e. a ratio of
norbuprenorphine:buprenorphine: < 0.02) suggests that buprenorphine was
added to the urine
▪ Testing for buprenorphine during MAT can be useful to monitor adherence and
detect possible diversion
Sethi & Petrakis, 2013
Hull et al., 2008


Recent Trends in Substance Misuse
Methamphetamine overdose deaths are up 400%
Counterfeit oxycodone tablets (M 30) contain no oxycodone
(100% contain fentanyl)

Recent Trends in Addiction Treatment
We don’t call it “Addiction” anymore
DSM-5 identifies Substance Use Disorder
Our words matter
Instead of “dirty urine” try ..
Positive urine drug screen.
Instead of “drug addict” try …
Person struggling with substance disorder

Recent Trends in Addiction Treatment
MAT is giving way to MOUD
MAT = Medication Assisted Treatment
MOUD = Medication for Opioid Use Disorder
MOUD recognizes that medication is the primary treatment for OUD
Very high risk of death when patients discontinue MOUD or when they are
released or discharged from structured environment.

MAT⇒ MOUD
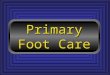
Impact of treatment for opioid dependence on fatal drug related poisoning: a national cohort study in England
Matthias Pierce et al. Addiction 2015, 111, 298–308


Audience Response
True or False:
Fentanyl has a shorter half-life than morphine
True
False
Pharmacokinetics of fentanyl after subcutaneous administration in volunteers
Capper, Sarah Ja et al European Journal of Anaesthesiology: March 2010 - Volume 27 - Issue 3 - p 241-246

Audience Response
True or False:
Fentanyl has a shorter half-life than morphine
False
Pharmacokinetics of fentanyl after subcutaneous administration in volunteers
Capper, Sarah Ja et al European Journal of Anaesthesiology: March 2010 - Volume 27 - Issue 3 - p 241-246

Audience Response Answer
Which drug has the shorter half life?
A. Fentanyl –
10 hours, 13.5 h, 7.9 h
B. Morphine –
2.1 hours, 1.6h
Pharmacokinetics of fentanyl after subcutaneous administration in volunteers
Capper, Sarah Ja et al European Journal of Anaesthesiology: March 2010 - Volume 27 - Issue 3 - p 241-246

Recent Trends in Addiction Treatment
Buprenorphine Microdosing

Buprenorphine Microdosing
Buprenorphine given concurrently
with full opioid agonists.
Initial very low dose with titration upward
over 5-10 days.
Full opioid agonists tapered after patient is on effective doses of
buprenorphine.

Buprenorphine Microdosing
Buprenex
0.15 mg SL QID x 1 day
0.3 mg SL QID x 1 day
0.6 mg SL QID x 1 day
then Suboxone
2 mg QID x 2 days
4 mg QID x 2 days
8 mg TID
Suboxone
0.5 mg qD x 1 day
0.5 mg BID x 1 day
1 mg BID x 1 day
2 mg BID x 1 day
4 mg BID x 1 day
4 mg TID
Transitioning Hospitalized Patients with Opioid Use Disorder from Methadone to Buprenorphine without a Period of Opioid
Abstinence Using a Microdosing Protocol. Terasaki D et al Pharmacotherapy. 2019 Oct;39(10):1023-1029
Case report: Successful induction of buprenorphine/naloxone using a microdosing schedule and assertive outreach.
Rozylo J et al. Addict Sci Clin Pract. 2020 Jan 15;15(1):2


Would you prescribe or encourage him to take:
A. Disulfiram
B. Acamprosate
C. Naltrexone
D. Gabapentin
Audi Poll Question
▪ A 48 year old man was just completed a home alcohol detox with a 3 day
prescription of chlordiazepoxide after he was brought to his PCP by his wife.
▪ He was drinking 1 bottle of wine nightly.
▪ Still a little anxious and not sleeping great.
▪ He is confident that he won’t drink again.

Medications for Alcohol Use Disorder
Three FDA-Approved Medicines:
Disulfiram (Antabuse)
Acamprosate (Campral)
Naltrexone (Revia, Vivitrol)
Additional Medicines showing Promise:
Gabapentin
Topiramate
Ondansetron

Medications for Alcohol Use Disorder
Three FDA-Approved Medicines:
Disulfiram (Antabuse)
Acamprosate (Campral)
Naltrexone (Revia, Vivitrol)

Disulfiram (Antabuse)
Aversive therapy
Blocks the Enzyme Aldehyde dehydrogenase (ALDH1A1)
Leads to rapid rise of acetaldehyde
Symptoms include flushing of the face, headache, nausea, vomiting, chest
pain, weakness, blurred vision, mental confusion, sweating, choking,
breathing difficulty, and anxiety.
Risk of liver toxicity
Mixed data on effectiveness, no longer commonly used

Acamprosate (Campral)
Inhibits Negative Reinforcement from alcohol
(Patient does not miss the alcohol as much)
333 mg, 2 tablets TID, do the math …..
666 mg three times daily
Really??
Decreases glutamate, increases beta-endorphins
Probably decreases craving for alcohol
NNT = 12 (abstinence), NNT = 9 (decreased drinking)

Naltrexone (Revia, Vivitrol)
Inhibits positive reinforcement from alcohol
Opiate Antagonist (risk of precipitated withdrawal if using opiates)
50-100 mg po daily (compliance is often poor)
“Sinclair Method” (Take only on drinking days)
380 mg IM monthly ($$, improved compliance)

Medications for Alcohol Use Disorder
Additional Medicines showing Promise:
Gabapentin
Topiramate
Ondansetron
In patients with concurrent depression and AUD, sertraline and fluoxetine
have led to decreased alcohol use

Gabapentin
300 mg BID starting dose
May titrate up to 1800 mg daily
Be aware of abuse potential

Gabapentin
Abstinence 4.1% placebo, 11.1% 300 mg TID, 17% 600 mg TID
(NNT = 8 for 1800 mg).
No heavy drinking rate 22.5% placebo, 29.6% 900 mg, and 44.7% 1800 mg
(NNT = 5 for 1800 mg).
-----------------
No heavy drinking days 27% gabapentin vs 9% placebo NNT 5.4
Abstinence 18% gabapentin vs 4% placebo NNT 6.2
Worked mainly in pts who had withdrawal symptoms
Gabapentin Treatment for Alcohol Dependence: A Randomized Controlled Trial Barbara J. Mason et al JAMA Intern Med. 2014 Jan 1; 174(1): 70–77
Efficacy of Gabapentin for the Treatment of Alcohol Use Disorder in Patients With Alcohol Withdrawal Symptoms A Randomized Clinical Trial
Raymond F. Anton et al JAMA Intern Med. 2020;180(5):728-736.

Topiramate
Start at 25 mg daily
Titrate up to 300 mg BID
Decrease by 50% for creatinine clearance <60

Ondansetron
4 mcg/kg BID
May go to higher doses
Available in 4, 8, 16 and 24 mg doses

Thank You

Questions?