Embed Size (px)
Citation preview
Burn Priorities of Care: Triage/Treatment/Transfer
Via Christi Regional Burn Center
Sarah Fischer, MSN, RN
Disclosure
I have nothing to disclose…
Objectives
➢ Identify American Burn Association referral criteria
➢ Explain the difference between partial and full
thickness burns
➢ Calculate TBSA using Rule of Nines
➢ Explore the priorities of initial assessment and
management of the burn patient
➢ Describe best practice for patient transport
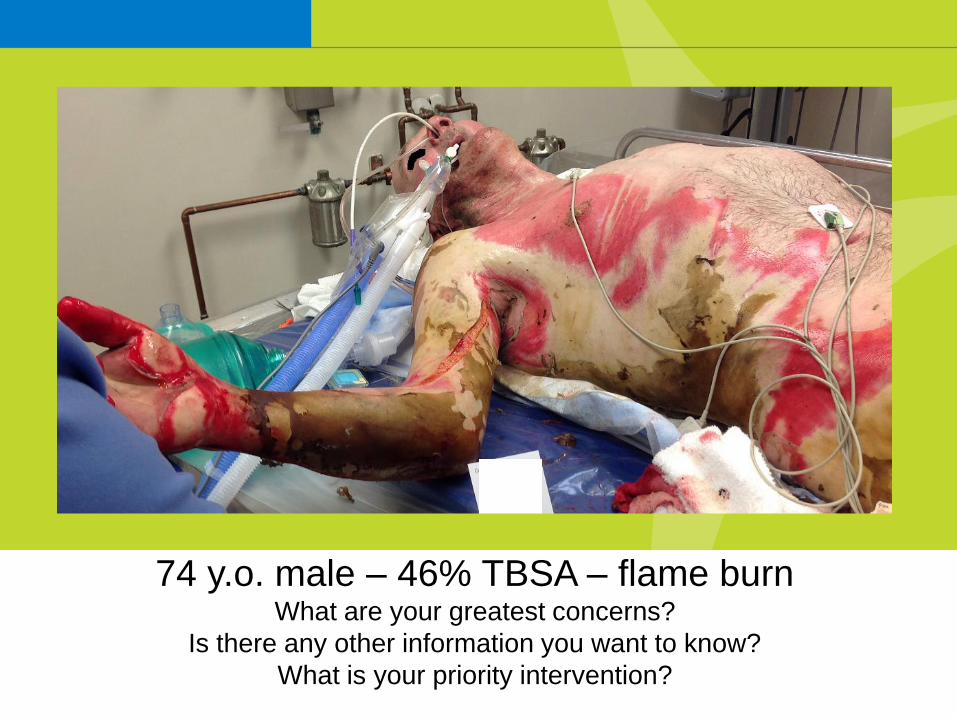
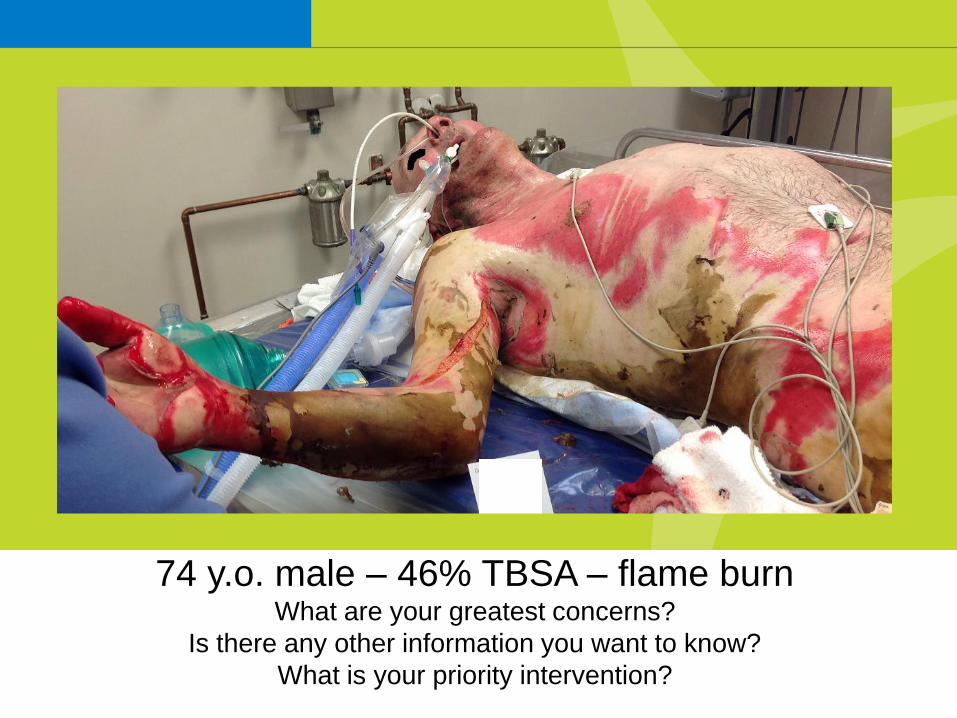
74 y.o. male – 46% TBSA – flame burnWhat are your greatest concerns?
Is there any other information you want to know?
What is your priority intervention?
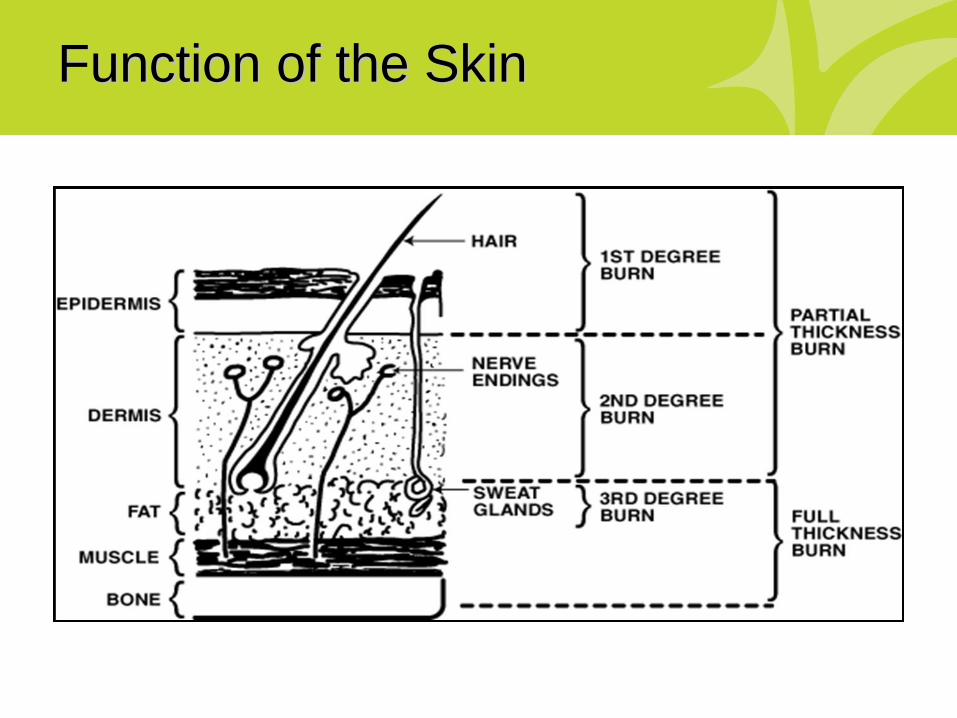
Function of the Skin
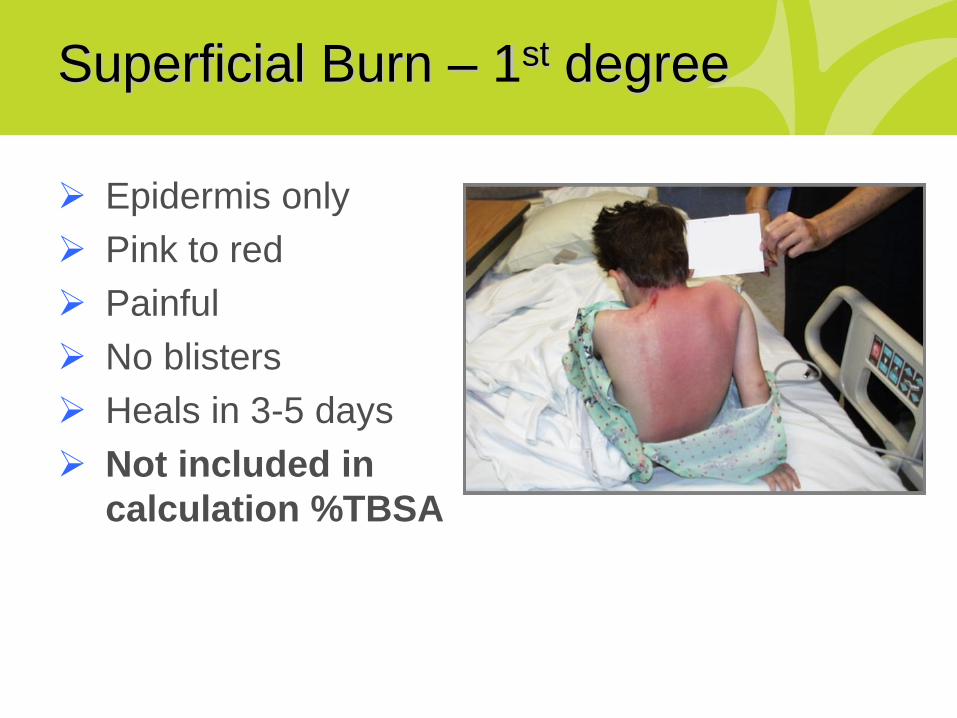
Superficial Burn – 1st degree
➢ Epidermis only
➢ Pink to red
➢ Painful
➢ No blisters
➢ Heals in 3-5 days
➢ Not included in
calculation %TBSA
Partial Thickness Burn – 2nd degree
➢ Epidermis and part of dermis
➢ Heal without surgical intervention
➢ Blisters• Large or small
• May not appear initially
• Continue to develop
➢ Wet and weepy
➢ Very painful
➢ Blanches
➢ Heals in 7-21 days
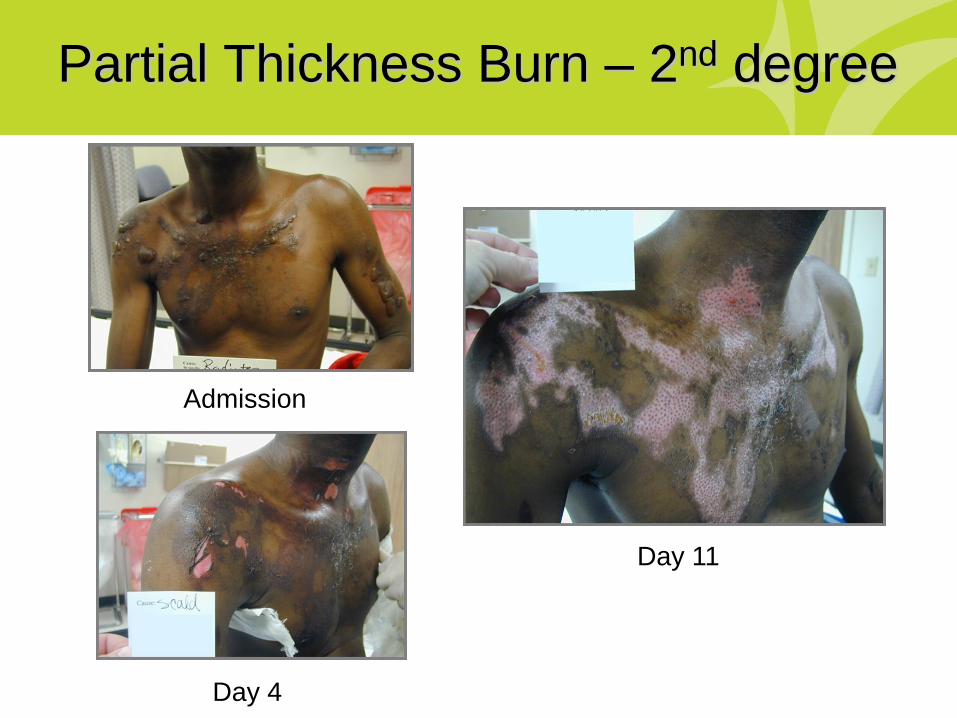
Partial Thickness Burn – 2nd degree
Admission
Day 4
Day 11
Full Thickness Burn – 3rd degree
➢ Epidermis, dermis, subcutaneous tissue
➢ Surgical intervention
➢ Insensate
➢ No blanching or capillary refill
➢ Charred, bright red, marbled, leathery,
tan, waxy, or pearly white
➢ Tight, non-elastic

Full Thickness Burn – 3rd degree
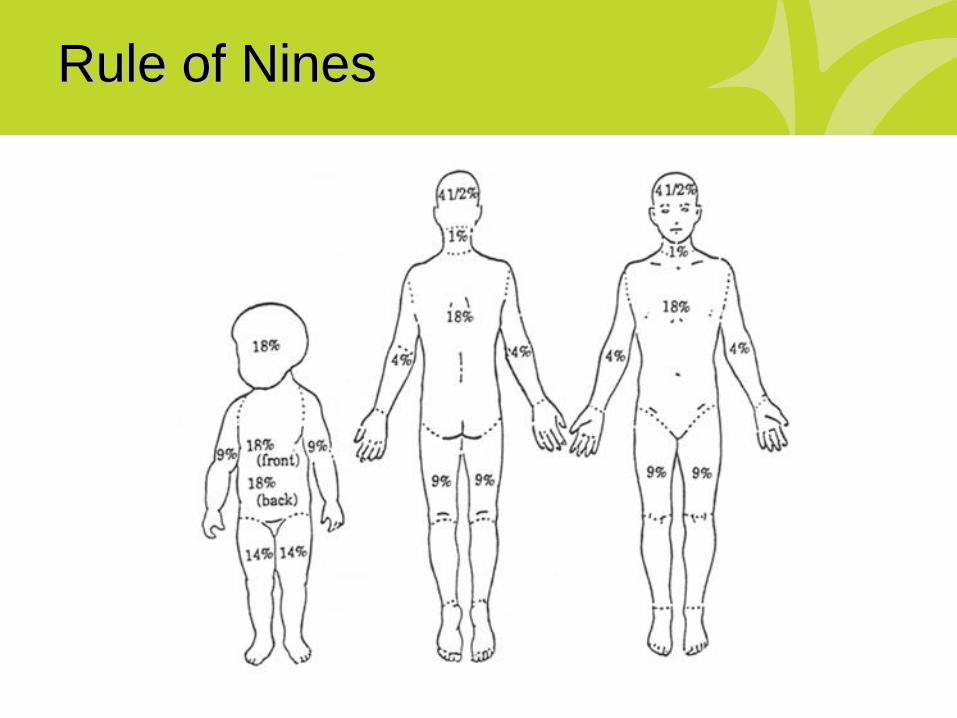
Rule of Nines

Primary Assessment: Life and Limb
➢ Airway
• Maintain c-spine precautions
➢ Breathing
➢ Circulation, cardiac status, CPR
➢ Disability, Deformity, Neurological Deficit
➢ Expose, Examine, Environment
• Stop the burning process
• Keep warm and dry
➢ Secondary assessment does not start until all of
these elements are accounted for…
• Including calculated fluid resuscitation
Precedence Over Burns
➢ Airway obstruction
➢ Cardiac arrest
➢ Spinal or head injury
➢ Open chest wounds
➢ Severe abdominal trauma
▪ Burn Center works closely with trauma for
multisystem injuries
▪ Consult with Burn Center physician to
ensure concurrent trauma activation
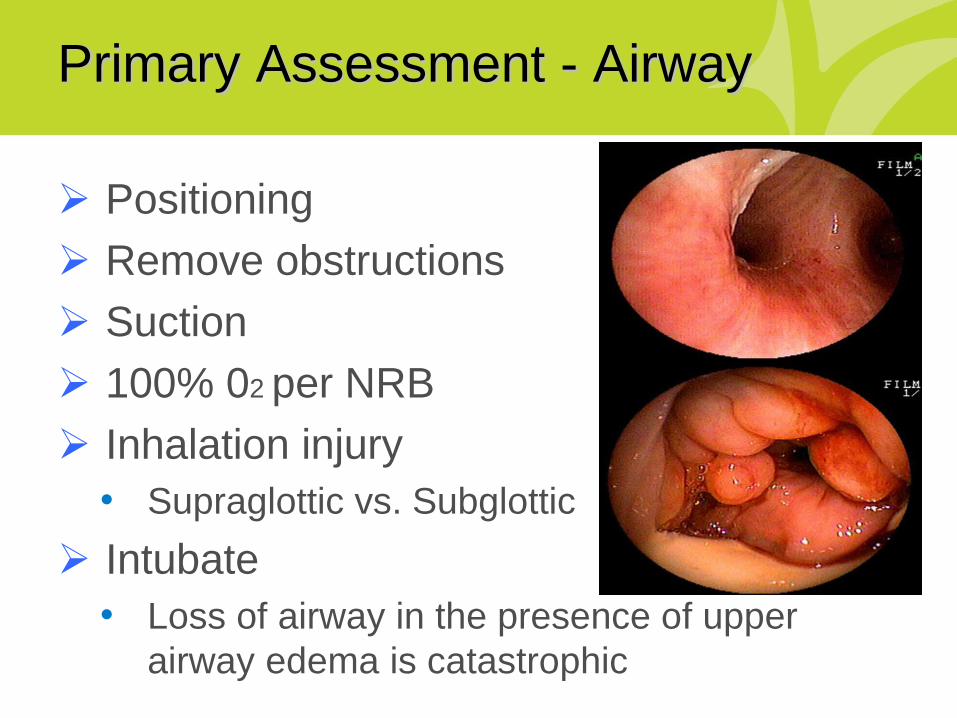
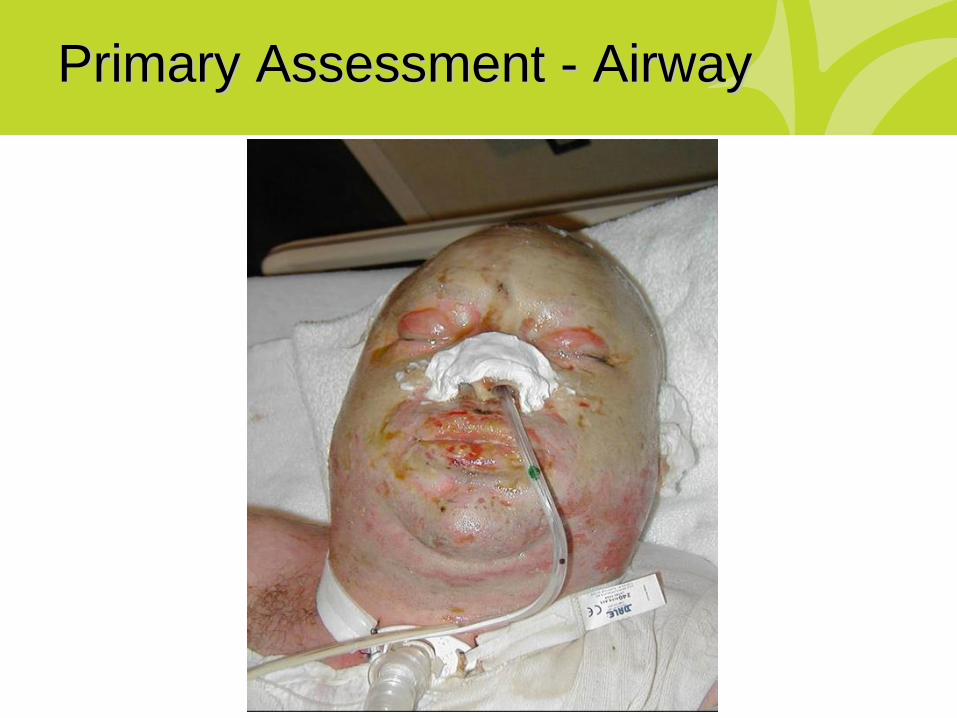
Primary Assessment - Airway
➢ Positioning
➢ Remove obstructions
➢ Suction
➢ 100% 02 per NRB
➢ Inhalation injury
• Supraglottic vs. Subglottic
➢ Intubate
• Loss of airway in the presence of upper
airway edema is catastrophic
Intubation
➢ Clinical judgment
• Feel free to discuss with Burn Center
➢ Weigh the risks and benefits
• Laryngeal injury, tube misplacement,
stenosis, fistula, swallowing impairment
➢ Err on the side of safety
• Loss of airway in the presence of upper
airway edema is catastrophic
➢ Special considerations for end of life
Intubation
➢ Rapid Sequence Intubation
• By the most experienced person
➢ Route
• Orotracheal vs. nasotracheal
➢ Size of endotracheal tube
• Use standard sizes for age/body type
• Place the largest recommended size possible
➢ Secure the tube
➢ Place NG/OG

Primary Assessment - Airway
Primary Assessment - Airway
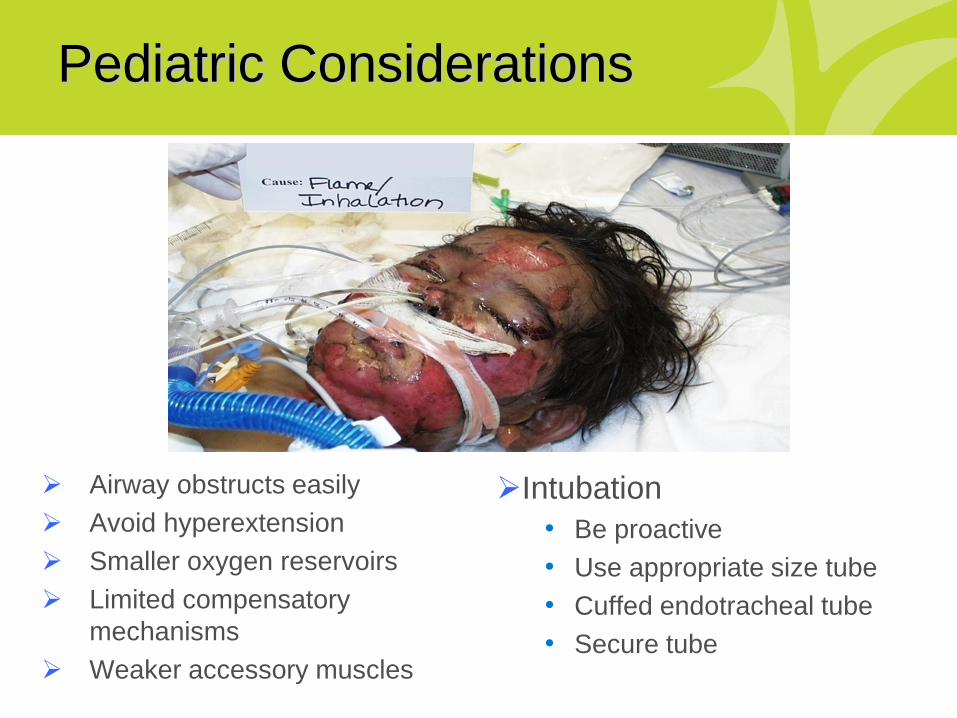
Pediatric Considerations
➢ Airway obstructs easily
➢ Avoid hyperextension
➢ Smaller oxygen reservoirs
➢ Limited compensatory
mechanisms
➢ Weaker accessory muscles
➢Intubation
• Be proactive
• Use appropriate size tube
• Cuffed endotracheal tube
• Secure tube

Primary Assessment – Breathing
➢ Assess rate, depth,
lung sounds
➢ Monitor for
circumferential
chest/torso burns
➢ Compromise of chest
wall excursion and
ventilation

Chest Escharotomies
Primary Assessment - Circulation
➢ CPR if indicated
➢ Control hemorrhage
➢ BP and pulse
• Normal pulse: 110-120bpm
• Hypotension: late sign of hypovolemia
• Edema can affect readings
➢ Circumferential burns
➢ Cardiac monitor
Fluid Resuscitation
➢ Two large bore IVs
• Adults > 20% TBSA
• Children > 15% TBSA
➢ Site selection
• Burned vs. unburned
• Peripheral vs. central
• Intraosseous
➢ Lactated Ringers
• D5LR for children < 30kg
Fluid Resuscitation
➢ Initial fluid resuscitation for major burns
• < 5 years old: 125 ml/hour
• 5-14 years old: 250 ml/hour
• > 14 years old: 500 ml/hour
➢ Consider an increased need with
associated trauma and inhalation injury
➢ No boluses or diuretics
➢ Consult with burn physician
• Consensus Formula
• Fluid rates for minor burns
Consensus Formula
➢ Adult thermal and chemical
• 2 ml/kg/TBSA
➢ Pediatric (< 14 years old)
• 3 ml/kg/TBSA
• D5LR for children < 30kg
➢ High voltage injury (any age)
• 4 ml/kg/TBSA
Primary Assessment - Disability
➢ Glascow Coma Scale
➢ Level of consciousness
• Carbon monoxide
• Head injury
• Hypoxia
• Drugs & alcohol
➢ AVPU
➢ Deformity
➢ Disability
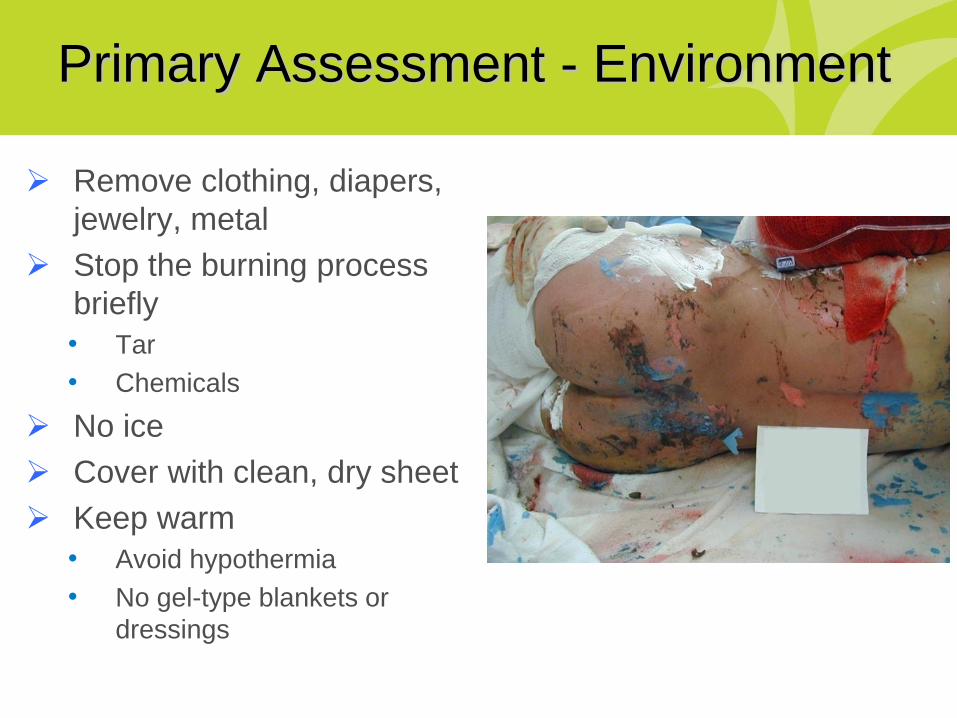
Primary Assessment - Environment
➢ Remove clothing, diapers,
jewelry, metal
➢ Stop the burning process
briefly
• Tar
• Chemicals
➢ No ice
➢ Cover with clean, dry sheet
➢ Keep warm
• Avoid hypothermia
• No gel-type blankets or
dressings

History
➢ Mechanism of injury
➢ Associated injuries
➢ Chemical exposure
➢ Substance abuse
➢ Abuse or neglect
➢ Intentional injuries
➢ AMPLET
• Allergies
• Medications
• Past medical history
• Last meal or drink
• Events and
environment
• Tetanus
ABA Referral Criteria
➢ Partial thickness burns > 10%
➢ Face, hands, feet, genitalia, perineum, joints
➢ Full thickness burns, any size
➢ Electrical injury, including lightning
➢ Chemical burns
➢ Inhalation injury
➢ Preexisting medical disorders that could complicate
recovery
➢ Burns with concomitant trauma
➢ Children
➢ Social, emotional, rehab needs
Transport
➢ Monitor vital signs
➢ Assess extremity perfusion
➢ Administer pain medication
➢ Cover burns with clean linens
• Do not apply special dressings
• Saran Wrap
➢ Maintain body temperature
• Hypothermia can be lethal
➢ Documentation
Transport
➢ Physician to physician communication
➢ Referring physician provides:
• Demographic and historical data
• Result of primary and secondary surveys
➢ Receiving physician will give
recommendations for transport
➢ Nurse to nurse communication
➢ Transport by trained personnel
74 y.o. male – 46% TBSA – flame burnWhat are your greatest concerns?
Is there any other information you want to know?
What is your priority intervention?
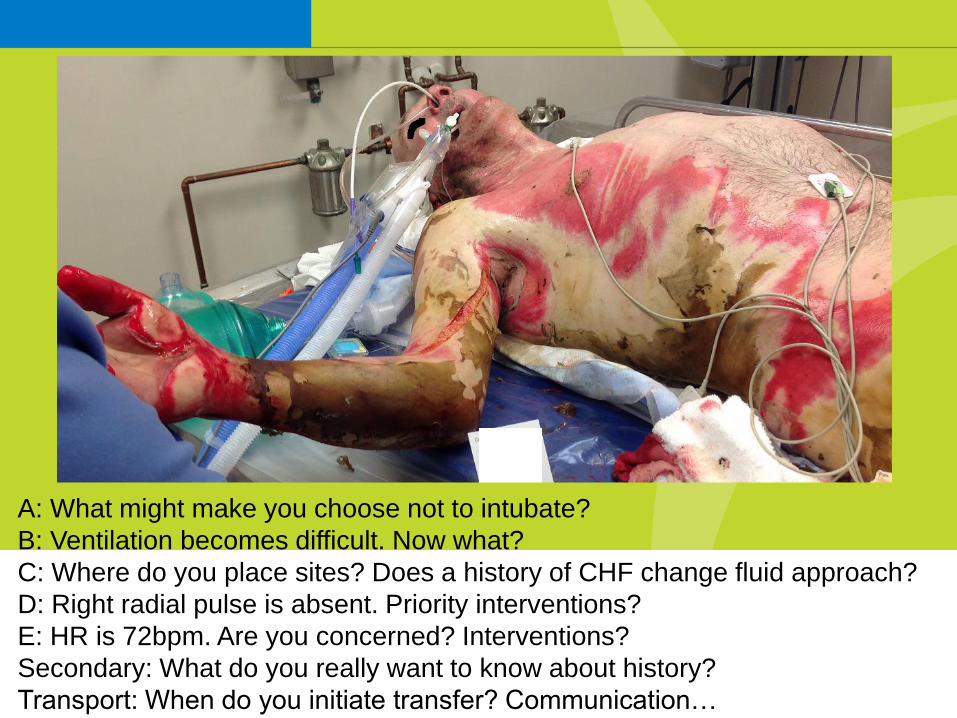
A: What might make you choose not to intubate?
B: Ventilation becomes difficult. Now what?
C: Where do you place sites? Does a history of CHF change fluid approach?
D: Right radial pulse is absent. Priority interventions?
E: HR is 72bpm. Are you concerned? Interventions?
Secondary: What do you really want to know about history?
Transport: When do you initiate transfer? Communication…
References
➢ American Burn Association. (2016).
Advanced burn life support.
➢ Herndon, D. (2012). Total burn care (4th
ed.). Edinburgh: Saunders Elsevier.
Thank You!
➢ Sarah Fischer, Burn Program Coordinator
• 316-268-5875
➢ Via Christi Regional Burn Center
• 316-268-5388
➢ Via Christi Dispatch
• 1-800-353-3111





























