Embed Size (px)
Citation preview
© 2002 Nature Publishing Group
PERSPECTIVES
them. The overwhelming majority of patientsusing CAM approaches do so to comple-ment conventional care, rather than as analternative to it5.
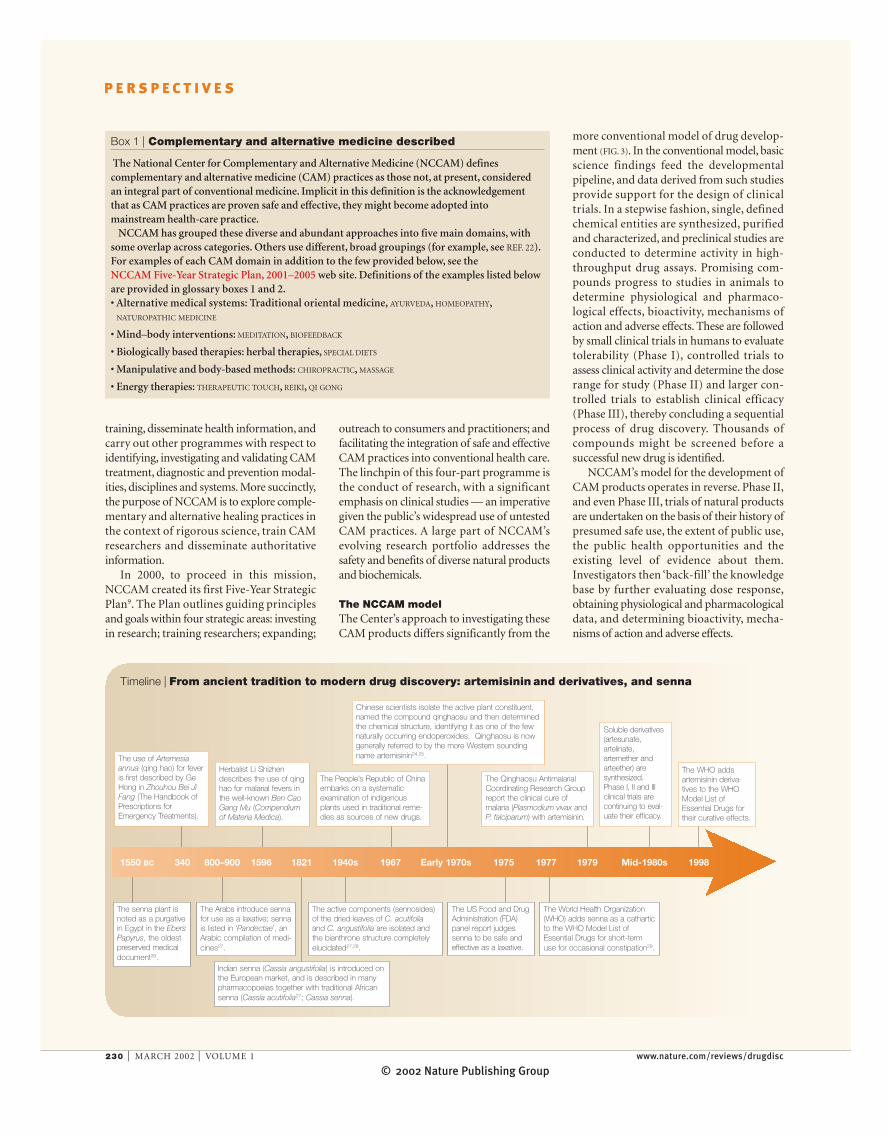
Expanding the health-care repertoireHistorical precedent predicts the potential ofCAM to expand the health-care repertoire,either as single-chemical entities or as com-plex botanical drugs. Among the first drugsfor the treatment of high blood pressure wasreserpine from the herb Rauwolfia serpentina,which was described many centuries ago inIndian Ayurvedic monographs. Indeed, someof our most important drugs, although theydid not originate as CAM therapies, are deriv-atives of the active ingredients identified inherbal remedies6. Such drugs of botanicalorigin include quinine (cinchona bark),digitalis (foxglove leaf), morphine (poppyherb) and vincristine (rosy periwinkle)7,8.More recently, the use of the leaves ofArtemisia annua for fevers by practitioners ofTRADITIONAL ORIENTAL MEDICINE, led to the devel-opment of artemisinin as the basis for amajor new class of single-chemical-entityantimalarial drugs (TIMELINE; FIG. 2). Otherimportant drugs that have their roots inindigenous medical practices are complexmixtures of natural products. For example,the observed use of the senna plant as apurgative by the Egyptians as early as 1550 BC
led, ultimately, to the development of laxa-tives that are now available as over-the-counter (OTC) medicines (TIMELINE; FIG. 2).
There are indications that herbal remediesand other CAM practices might prove effec-tive in preventing and treating chronic dis-eases, possibly reducing the costs of healthcare. At present, however, few of theseapproaches have been tested rigorously forsafety and effectiveness. Still others awaitdiscovery and validation of their worth.
NCCAM investigates CAM treatmentsIn 1998, responding to public demand forbetter guidance regarding the myriad ofCAM options, the United States Congressauthorized the creation of the NationalCenter for Complementary and AlternativeMedicine (NCCAM) at the NationalInstitutes of Health (NIH). The establish-ment of the Center represented an expansionin scope and authority of the Office ofAlternative Medicine (OAM), which was firstestablished in 1992. The authorizing languagecharged NCCAM to conduct and supportbasic and applied research and research
Whereas other components of theNational Institutes of Health support thediscovery and subsequent development ofnovel chemical entities into drugs, theNational Center for Complementary andAlternative Medicine (NCCAM) studiescomplex natural products that are marketedas dietary supplements. This articlecontrasts the regulatory framework fordietary supplements and drugs, outlinesthe challenges of evaluating dietarysupplements for safety and clinicaleffectiveness, and describes the evolvingdrug model for botanicals.
The popularity of CAMAn increasing number of individuals in theUnited States — as many as 42% of themaccording to one estimate — are adoptingcomplementary and alternative medicine(CAM) approaches to help meet their per-sonal health needs1,2 (FIG. 1). The attractivenessof CAM extends far beyond the UnitedStates3. In the United Kingdom, for example,the House of Lords Select Committee onScience and Technology undertook a compre-hensive inquiry into CAM. Its use is increas-ing not only in the United Kingdom, but alsoacross the whole of the developed world4.Generally, patients who choose CAMapproaches (defined and described in BOX 1)are seeking ways to improve their health andwell-being, and to relieve symptoms associ-ated with chronic, even terminal, illnesses orthe side effects of conventional treatments for
NATURE REVIEWS | DRUG DISCOVERY VOLUME 1 | MARCH 2002 | 229
Development of therapeutics:opportunities within complementaryand alternative medicine
Linda W. Engel and Stephen E. Straus
B U S I N E S S O U T LO O K
Milli
ons
of v
isits
MDs
388 M 386 M427 M
629 M700
600
500
400
300
200
100
0CAM
1990 1997
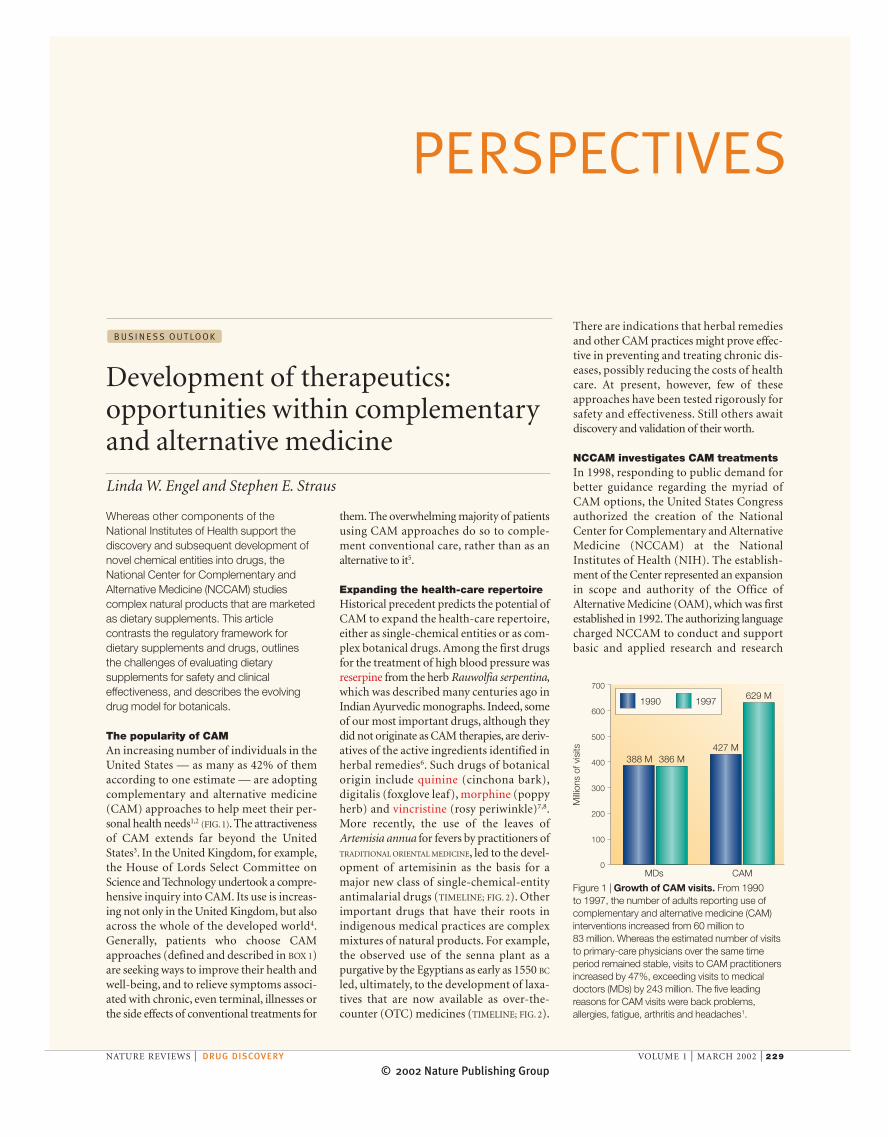
Figure 1 | Growth of CAM visits. From 1990 to 1997, the number of adults reporting use ofcomplementary and alternative medicine (CAM)interventions increased from 60 million to 83 million. Whereas the estimated number of visitsto primary-care physicians over the same timeperiod remained stable, visits to CAM practitionersincreased by 47%, exceeding visits to medicaldoctors (MDs) by 243 million. The five leadingreasons for CAM visits were back problems,allergies, fatigue, arthritis and headaches1.
© 2002 Nature Publishing Group230 | MARCH 2002 | VOLUME 1 www.nature.com/reviews/drugdisc
P E R S P E C T I V E S
more conventional model of drug develop-ment (FIG. 3). In the conventional model, basicscience findings feed the developmentalpipeline, and data derived from such studiesprovide support for the design of clinicaltrials. In a stepwise fashion, single, definedchemical entities are synthesized, purifiedand characterized, and preclinical studies areconducted to determine activity in high-throughput drug assays. Promising com-pounds progress to studies in animals todetermine physiological and pharmaco-logical effects, bioactivity, mechanisms ofaction and adverse effects. These are followedby small clinical trials in humans to evaluatetolerability (Phase I), controlled trials toassess clinical activity and determine the doserange for study (Phase II) and larger con-trolled trials to establish clinical efficacy(Phase III), thereby concluding a sequentialprocess of drug discovery. Thousands ofcompounds might be screened before asuccessful new drug is identified.
NCCAM’s model for the development ofCAM products operates in reverse. Phase II,and even Phase III, trials of natural productsare undertaken on the basis of their history ofpresumed safe use, the extent of public use,the public health opportunities and theexisting level of evidence about them.Investigators then ‘back-fill’ the knowledgebase by further evaluating dose response,obtaining physiological and pharmacologicaldata, and determining bioactivity, mecha-nisms of action and adverse effects.
outreach to consumers and practitioners; andfacilitating the integration of safe and effectiveCAM practices into conventional health care.The linchpin of this four-part programme isthe conduct of research, with a significantemphasis on clinical studies — an imperativegiven the public’s widespread use of untestedCAM practices. A large part of NCCAM’sevolving research portfolio addresses thesafety and benefits of diverse natural productsand biochemicals.
The NCCAM modelThe Center’s approach to investigating theseCAM products differs significantly from the
training, disseminate health information, andcarry out other programmes with respect toidentifying, investigating and validating CAMtreatment, diagnostic and prevention modal-ities, disciplines and systems. More succinctly,the purpose of NCCAM is to explore comple-mentary and alternative healing practices inthe context of rigorous science, train CAMresearchers and disseminate authoritativeinformation.
In 2000, to proceed in this mission,NCCAM created its first Five-Year StrategicPlan9. The Plan outlines guiding principlesand goals within four strategic areas: investingin research; training researchers; expanding;
Box 1 | Complementary and alternative medicine described
The National Center for Complementary and Alternative Medicine (NCCAM) definescomplementary and alternative medicine (CAM) practices as those not, at present, consideredan integral part of conventional medicine. Implicit in this definition is the acknowledgementthat as CAM practices are proven safe and effective, they might become adopted intomainstream health-care practice.
NCCAM has grouped these diverse and abundant approaches into five main domains, withsome overlap across categories. Others use different, broad groupings (for example, see REF. 22).For examples of each CAM domain in addition to the few provided below, see theNCCAM Five-Year Strategic Plan, 2001–2005 web site. Definitions of the examples listed beloware provided in glossary boxes 1 and 2.• Alternative medical systems: Traditional oriental medicine, AYURVEDA, HOMEOPATHY,
NATUROPATHIC MEDICINE
• Mind–body interventions: MEDITATION, BIOFEEDBACK
• Biologically based therapies: herbal therapies, SPECIAL DIETS
• Manipulative and body-based methods: CHIROPRACTIC, MASSAGE
• Energy therapies: THERAPEUTIC TOUCH, REIKI, QI GONG
The use of Artemesiaannua (qing hao) for feveris first described by GeHong in Zhouhou Bei JiFang (The Handbook ofPrescriptions forEmergency Treatments).
The senna plant isnoted as a purgativein Egypt in the EbersPapyrus, the oldestpreserved medicaldocument26.
The Arabs introduce sennafor use as a laxative; sennais listed in ‘Pandectae’, anArabic compilation of medi-cines27.
Herbalist Li Shizhendescribes the use of qinghao for malarial fevers inthe well-known Ben CaoGang Mu (Compendiumof Materia Medica).
The People’s Republic of Chinaembarks on a systematic examination of indigenousplants used in traditional reme-dies as sources of new drugs.
Indian senna (Cassia angustifolia) is introduced onthe European market, and is described in manypharmacopoeias together with traditional Africansenna (Cassia acutifolia27; Cassia senna).
Chinese scientists isolate the active plant constituent,named the compound qinghaosu and then determinedthe chemical structure, identifying it as one of the fewnaturally occurring endoperoxides. Qinghaosu is nowgenerally referred to by the more Western soundingname artemisinin24,25.
The Qinghaosu AntimalarialCoordinating Research Groupreport the clinical cure ofmalaria (Plasmodium vivax and P. falciparum) with artemisinin.
Soluble derivatives(artesunate,artelinate,artemether andarteether) are synthesized.Phase I, II and IIIclinical trials arecontinuing to eval-uate their efficacy.
The WHO addsartemisinin deriva-tives to the WHOModel List ofEssential Drugs fortheir curative effects.
The US Food and DrugAdministration (FDA)panel report judgessenna to be safe andeffective as a laxative.
The World Health Organization(WHO) adds senna as a catharticto the WHO Model List ofEssential Drugs for short-termuse for occasional constipation29.
The active components (sennosides)of the dried leaves of C. acutifoliaand C. angustifolia are isolated andthe bianthrone structure completelyelucidated27,28.
1550 BC 340 800–900 1596 1821 1940s 1967 Early 1970s 1975 1977 1979 Mid-1980s 1998
Timeline | From ancient tradition to modern drug discovery: artemisinin and derivatives, and senna
© 2002 Nature Publishing Group
P E R S P E C T I V E S
those for which the claim resembled that of adrug were regulated as unapproved — that is,illegal, new drugs. However, in 1994, theUnited States Congress passed the DietarySupplement Health and Education Act(DSHEA)12 to promote consumer access todietary supplements. This law defined a newcategory of food for regulatory purposes —the dietary supplement13 — which wouldinclude herbs and other botanicals, vitaminsand minerals, and other substances.
Under the DSHEA, manufacturers ofdietary supplements might claim that anutrient or dietary ingredient has effects onthe body. Such claims might describe: thebenefits ‘‘related to a classical nutrient defic-iency disease…’’; ‘‘…the role of a nutrientor dietary ingredient intended to affect thestructure or function in humans’’; ‘‘…thedocumented mechanism by which a nutrientor dietary ingredient acts to maintain suchstructure or function,’’; or the attainment of‘‘…general well-being from consumption of anutrient or dietary ingredient’’. Collectively— in regulatory parlance in the UnitedStates — these are referred to asstructure/function claims. For example,addressing some mild symptoms ofmenopause — a physiological not a patho-logical process — would represent a struc-ture/function claim. The DSHEA requiresthat the product must not be intended todiagnose, treat, cure or prevent any disease.Although dietary ingredients that werelegally on the market before the enactmentof the DSHEA do not need pre-marketapproval or review by the FDA, a pre-marketsafety notification is required for newingredients.
Under Federal law, drugs and dietary sup-plements are subject to different requirementsconcerning their manufacture and theirstandards for safety and efficacy. First, drugsare subject to specific GMP requirements.Whereas the law permits the FDA to developspecific GMPs for dietary supplements, so farsuch GMPs have not been issued. At a mini-mum, therefore, companies must follow exist-ing manufacturing requirements for foods.Second, drug products must be approved bythe FDA as being safe and efficacious beforemarketing. By contrast, manufacturers ofdietary supplements are responsible for ensur-ing that their products are safe. Whereas theFDA monitors adverse effects after dietary-supplement products are on the market, newlymarketed dietary supplements are not sub-jected to pre-market approval or a specificpost-market surveillance period. Moreover,the resources that are available to the Agencyfor monitoring dietary supplements are not
Regulatory law drives the model An overview of the legal framework underwhich conventional drugs and diverse naturalproducts are regulated in the United Statesreveals one explanation for this differencebetween CAM products and conventionaldrug development. At present, there are eightproduct categories within the regulatoryframework of the United States. Classificationwithin these categories is based on intendeduse, as indicated by the hypothetical exampleof garlic in FIG. 4. Of particular relevance tothis discussion is the distinction betweendrugs (that is, prescription and OTC medi-cines) and dietary supplements and theirrespective regulatory routes.
The Federal Food, Drug and Cosmetic Act— enacted in 1938 (REF. 10) — established thatdrugs, which are products that are claimed to
treat, cure, mitigate or prevent a disease, are tobe regulated by the US Food and DrugAdministration (FDA) as drugs. Since 1938,drugs have had to be proven safe for theirintended use to gain FDA pre-marketapproval (unless they had been ‘grand-fathered’ as old drugs). Since 1962, approvalhas also required that efficacy can be shownin adequate and well-controlled studies.Furthermore, all drug manufacturers mustfollow GOOD MANUFACTURING PRACTICES (GMPs)to assure quality and standardization of theirdrugs, and must list their facilities andproducts with the FDA11.
Herbal products are regulated either asfoods or drugs, depending on their intendeduse. Until 1994, HERBS that were labelled oradvertised with no indication of intended usewere usually considered to be foods, whereas
NATURE REVIEWS | DRUG DISCOVERY VOLUME 1 | MARCH 2002 | 231
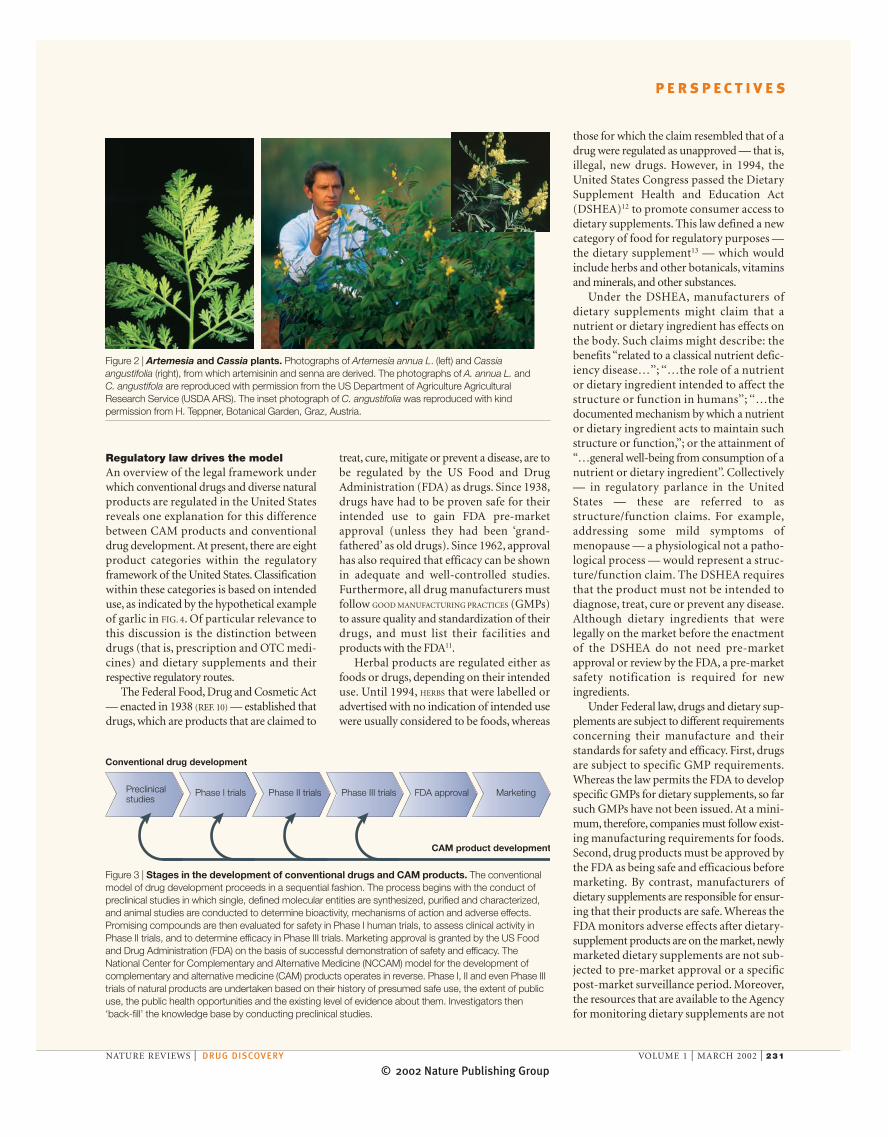
Figure 2 | Artemesia and Cassia plants. Photographs of Artemesia annua L. (left) and Cassiaangustifolia (right), from which artemisinin and senna are derived. The photographs of A. annua L. and C. angustifola are reproduced with permission from the US Department of Agriculture AgriculturalResearch Service (USDA ARS). The inset photograph of C. angustifolia was reproduced with kindpermission from H. Teppner, Botanical Garden, Graz, Austria.
Preclinicalstudies
Phase I trials Phase II trials Phase III trials FDA approval Marketing
CAM product development
Conventional drug development
Figure 3 | Stages in the development of conventional drugs and CAM products. The conventionalmodel of drug development proceeds in a sequential fashion. The process begins with the conduct ofpreclinical studies in which single, defined molecular entities are synthesized, purified and characterized,and animal studies are conducted to determine bioactivity, mechanisms of action and adverse effects.Promising compounds are then evaluated for safety in Phase I human trials, to assess clinical activity inPhase II trials, and to determine efficacy in Phase III trials. Marketing approval is granted by the US Foodand Drug Administration (FDA) on the basis of successful demonstration of safety and efficacy. TheNational Center for Complementary and Alternative Medicine (NCCAM) model for the development ofcomplementary and alternative medicine (CAM) products operates in reverse. Phase I, II and even Phase IIItrials of natural products are undertaken based on their history of presumed safe use, the extent of publicuse, the public health opportunities and the existing level of evidence about them. Investigators then‘back-fill’ the knowledge base by conducting preclinical studies.

© 2002 Nature Publishing Group232 | MARCH 2002 | VOLUME 1 www.nature.com/reviews/drugdisc
P E R S P E C T I V E S
and in defining the pharmacology, toxicologyand biological activity of dietary supplementsin animal models.
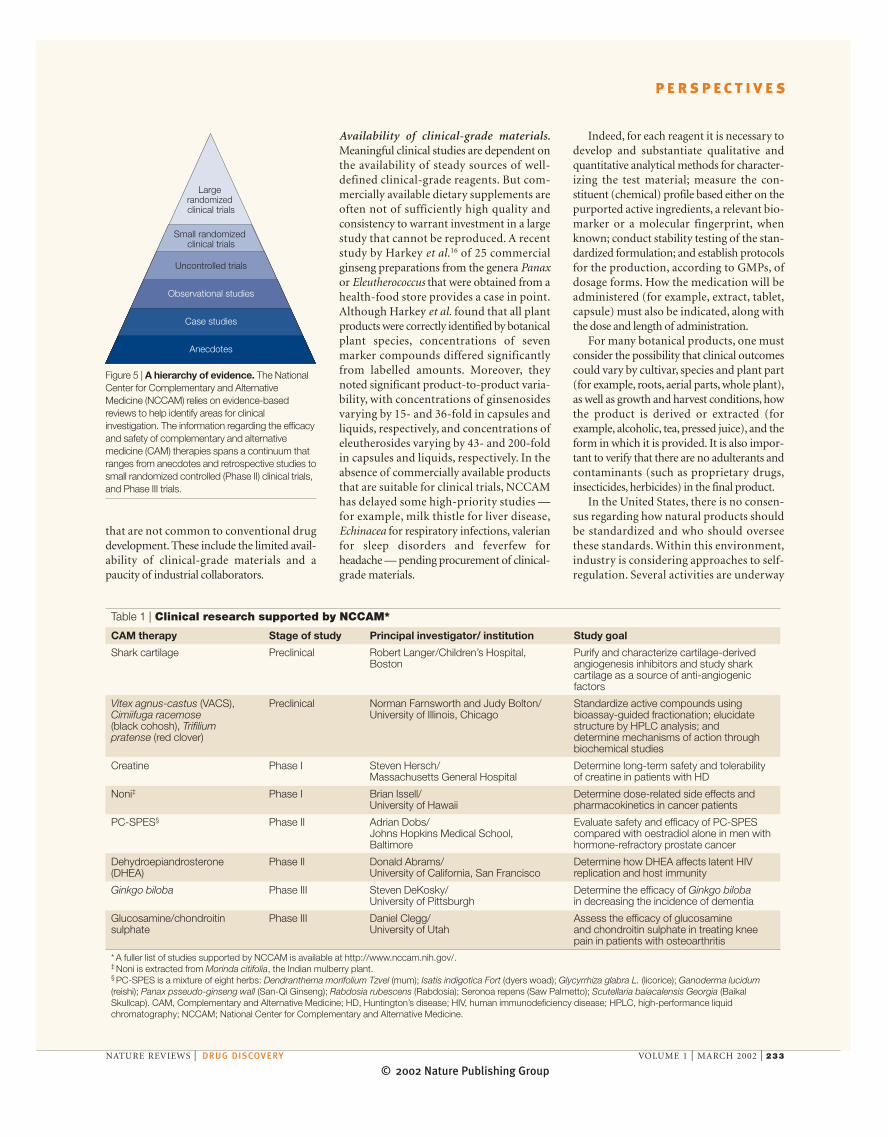
Determining safety and efficacy. To helpidentify fertile areas for clinical investigationand the appropriate level of investment inthese areas, the Center relies on evidence-based reviews. These analyses indicate thatinformation regarding the efficacy and safetyof CAM therapies spans a continuum, rang-ing from anecdotes and retrospective studiesto small randomized controlled (Phase II)clinical trials, and should culminate as it doesin the conventional model — in Phase IIItrials (FIG. 5). The National Advisory Councilon Complementary and AlternativeMedicine, and many key groups of stake-holders, help NCCAM assign priority to itsresearch initiatives by considering howextensively products are being used by con-sumers, the potential for public healthimpact, the opportunity to expand the sciencebase, the feasibility of any particular studyand, of course, cost.
Complicating the development of a CAMresearch portfolio is a patient/consumer dual-ism in how natural products are used in theUnited States. Whereas many consumers usethem for non-pathological conditions forwhich they are marketed, such as dietaryapproaches to menopause and its symptoms,others use natural products to treat or preventspecific diseases. NCCAM is obliged to studythese products as the public uses them, butplaces a higher priority on studies that wouldaddress the most important public healthissues that surround CAM product use. So,whereas NCCAM does fund research relatedto the use of botanical products forstructure/function indications, the Centerinvests far more in studies of CAM approachesto serious, debilitating and/or life-threateningillnesses for which conventional medicaloptions afford incomplete remedies. TABLE 1
lists a number of NCCAM-supported studies,ranging from basic research to Phase III clini-cal trials. (A more detailed list of studies thatNCCAM supports can be viewed by visitingThe NIH NCCAM web site.)
Obstacles to CAM research The use of many CAM products by indige-nous cultures for centuries, and the belief thatthey are safe and beneficial, represent theopportunities for further improving healthand well-being and for preventing and treat-ing disease. However, drug development andclinical research are complex endeavours ingeneral, and, in fulfilling its research agenda,NCCAM faces a number of extra obstacles
adequate to fulfil this duty14. Third, whereasthe DSHEA requires companies to substan-tiate claims of benefit, it is believed thatcitation of existing literature, such as it is, issufficient to validate such claims. In addition,manufacturers are not required, as they arefor drugs, to submit such substantiation datato the FDA. Instead, it is the Federal TradeCommission that has primary responsibilityfor monitoring dietary supplements for truthin advertising.
In Europe, intended use of dietary supple-ments also determines the regulatory route,which varies from country to country. Forexample, herbals are considered to be drugs inGermany, France and Italy, whereas in GreatBritain and the Netherlands they are regardedas food supplements for which medicinalclaims are prohibited15. Accordingly, garlic (tolower cholesterol) and St. John’s wort (to treatdepression) would be available in Germany asboth drugs and OTC medicines, but sold asfood supplements in the Netherlands. Thissituation will change if the European Uniondevelops a uniform set of laws to be followedby its member states.
US patent law and the CAM modelsAn understanding of patent law in theUnited States also helps to explain some
crucial differences in how conventional drugsand CAM products are being developed.Many people in the natural-products indus-try perceive few opportunities to obtaindefensible patents for natural products thathave been used in the public domain formany years. So, with little chance to achievemarket exclusivity and without a requirementfor pre-market approval, companies have littleincentive to conduct expensive clinical trialsof dietary supplements.
A large role for NCCAM/NIHAs a result of the use patterns of CAM prod-ucts and the current regulatory climate in theUnited States, there is a relatively larger rolefor NCCAM and its sister institutes at NIH inthe research arena than in the development ofconventional drugs.
Basic research. As is also true in the conven-tional model of drug development, the task ofconducting basic, preclinical research oftenfalls to NIH-supported investigators. There isa particularly appropriate role for govern-ment in the case of research that does notprovide immediate financial gain for corpo-rate sponsors. Hence, NCCAM can have animportant role in supporting preclinicalstudies to delineate mechanisms of action,
12
3
6
9
CosmeticGarlic spray and body lotion "to rejuvenate the skin and prevent the appearance of wrinkles"
Dietary supplementOdourless garlic capsule "boosts the immune system"
Biologic"Injected garlic vaccine prevents garlic allergies"
Foods for special dietary usesEnteral formula "for management of patients with heart disease"
Food additive (GRAS*)Garlic powder added to microwavable pizza "to impart flavour"
Conventional food"Fresh garlic!" or health claim: "taken with a complete diet, it might reduce your risk to heart disease"
Drug"Garlic cures cancer and prevents hypertension"
Medical deviceGarlic clove earplugs "prevent swimmer's ear"
Garlic
Figure 4 | Intended use defines the US regulatory classification (example: claims for garlicproducts). Depending on the use intended by the manufacturer, garlic products are classified forregulatory purposes in one of eight categories: conventional food; dietary supplement; food for specialdietary uses; biologic; drug; medical device; cosmetic; or food additive. Note: garlic is GenerallyRecognized as Safe (GRAS) based on its common use in food before 1 January, 1958. Adapted withpermission from REF. 23.
© 2002 Nature Publishing Group
P E R S P E C T I V E S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 1 | MARCH 2002 | 233
Indeed, for each reagent it is necessary todevelop and substantiate qualitative andquantitative analytical methods for character-izing the test material; measure the con-stituent (chemical) profile based either on thepurported active ingredients, a relevant bio-marker or a molecular fingerprint, whenknown; conduct stability testing of the stan-dardized formulation; and establish protocolsfor the production, according to GMPs, ofdosage forms. How the medication will beadministered (for example, extract, tablet,capsule) must also be indicated, along withthe dose and length of administration.
For many botanical products, one mustconsider the possibility that clinical outcomescould vary by cultivar, species and plant part(for example, roots, aerial parts, whole plant),as well as growth and harvest conditions, howthe product is derived or extracted (forexample, alcoholic, tea, pressed juice), and theform in which it is provided. It is also impor-tant to verify that there are no adulterants andcontaminants (such as proprietary drugs,insecticides, herbicides) in the final product.
In the United States, there is no consen-sus regarding how natural products shouldbe standardized and who should overseethese standards. Within this environment,industry is considering approaches to self-regulation. Several activities are underway
Availability of clinical-grade materials.Meaningful clinical studies are dependent onthe availability of steady sources of well-defined clinical-grade reagents. But com-mercially available dietary supplements areoften not of sufficiently high quality andconsistency to warrant investment in a largestudy that cannot be reproduced. A recentstudy by Harkey et al.16 of 25 commercialginseng preparations from the genera Panaxor Eleutherococcus that were obtained from ahealth-food store provides a case in point.Although Harkey et al. found that all plantproducts were correctly identified by botanicalplant species, concentrations of sevenmarker compounds differed significantlyfrom labelled amounts. Moreover, theynoted significant product-to-product varia-bility, with concentrations of ginsenosidesvarying by 15- and 36-fold in capsules andliquids, respectively, and concentrations ofeleutherosides varying by 43- and 200-foldin capsules and liquids, respectively. In theabsence of commercially available productsthat are suitable for clinical trials, NCCAMhas delayed some high-priority studies —for example, milk thistle for liver disease,Echinacea for respiratory infections, valerianfor sleep disorders and feverfew forheadache — pending procurement of clinical-grade materials.
that are not common to conventional drugdevelopment. These include the limited avail-ability of clinical-grade materials and apaucity of industrial collaborators.
Observational studies
Large randomized clinical trials
Small randomized clinical trials
Uncontrolled trials
Case studies
Anecdotes
Figure 5 | A hierarchy of evidence. The NationalCenter for Complementary and AlternativeMedicine (NCCAM) relies on evidence-basedreviews to help identify areas for clinicalinvestigation. The information regarding the efficacyand safety of complementary and alternativemedicine (CAM) therapies spans a continuum thatranges from anecdotes and retrospective studies tosmall randomized controlled (Phase II) clinical trials,and Phase III trials.
Table 1 | Clinical research supported by NCCAM*
CAM therapy Stage of study Principal investigator/ institution Study goal
Shark cartilage Preclinical Robert Langer/Children’s Hospital, Purify and characterize cartilage-derivedBoston angiogenesis inhibitors and study shark
cartilage as a source of anti-angiogenicfactors
Vitex agnus-castus (VACS), Preclinical Norman Farnsworth and Judy Bolton/ Standardize active compounds usingCimiifuga racemose University of Illinois, Chicago bioassay-guided fractionation; elucidate(black cohosh), Trifilium structure by HPLC analysis; andpratense (red clover) determine mechanisms of action through
biochemical studies
Creatine Phase I Steven Hersch/ Determine long-term safety and tolerability Massachusetts General Hospital of creatine in patients with HD
Noni‡ Phase I Brian Issell/ Determine dose-related side effects andUniversity of Hawaii pharmacokinetics in cancer patients
PC-SPES§ Phase II Adrian Dobs/ Evaluate safety and efficacy of PC-SPESJohns Hopkins Medical School, compared with oestradiol alone in men withBaltimore hormone-refractory prostate cancer
Dehydroepiandrosterone Phase II Donald Abrams/ Determine how DHEA affects latent HIV(DHEA) University of California, San Francisco replication and host immunity
Ginkgo biloba Phase III Steven DeKosky/ Determine the efficacy of Ginkgo bilobaUniversity of Pittsburgh in decreasing the incidence of dementia
Glucosamine/chondroitin Phase III Daniel Clegg/ Assess the efficacy of glucosamine sulphate University of Utah and chondroitin sulphate in treating knee
pain in patients with osteoarthritis
* A fuller list of studies supported by NCCAM is available at http://www.nccam.nih.gov/.‡ Noni is extracted from Morinda citifolia, the Indian mulberry plant.§ PC-SPES is a mixture of eight herbs: Dendranthema morifolium Tzvel (mum); Isatis indigotica Fort (dyers woad); Glycyrrhiza glabra L. (licorice); Ganoderma lucidum(reishi); Panax psseudo-ginseng wall (San-Qi Ginseng); Rabdosia rubescens (Rabdosia); Seronoa repens (Saw Palmetto); Scutellaria baiacalensis Georgia (BaikalSkullcap). CAM, Complementary and Alternative Medicine; HD, Huntington’s disease; HIV, human immunodeficiency disease; HPLC, high-performance liquidchromatography; NCCAM; National Center for Complementary and Alternative Medicine.
© 2002 Nature Publishing Group234 | MARCH 2002 | VOLUME 1 www.nature.com/reviews/drugdisc
P E R S P E C T I V E S
predecessor, the OAM,to the US $104.6 millionthat is NCCAM’s 2002 fiscal year appropria-tion. However, its resources are insufficient topursue all available scientific opportunities.Similarly, whereas the knowledge and experi-ence of NCCAM staff is extensive anddiverse, it is not exhaustive. So, NCCAMmust not only make its investments a priority,but it must also seek to leverage its intellec-tual and financial resources through collabo-rations.
in which key trade associations and theirindividual member companies, jointly orindividually, are involved in developing andimplementing quality assurance pro-grammes for natural products. Still otherorganizations are involved in developingthird-party certification programmes thatwill use a yet to be determined set of stan-dards, or are providing a seal of approvalassuring that the product contains no adulter-ants or contaminants, meets label specifica-
tions and/or is manufactured in compliancewith GMPs. NCCAM is eager for theseefforts to proceed to ensure a more reliablesource of materials for research and publicpurchase.
Availability of industrial collaborators.NCCAM has enjoyed generous Federal fund-ing. Appropriations for NIH-supported CAMresearch have risen from the US $2 millionthat was provided in 1992 to NCCAM’s
Botanicalproduct
What is theintended use?
Consumed forits taste, aromaor nutritive value
Food
Ingested to affectstructure or
function of body
Ingested to supplement diet
Dietarysupplement
Applied to body forcleansing, beautifyingor altering appearance
Cosmetic
Used to diagnose,cure, mitigate, treator prevent disease
Drug Is it intended foruse as a drug?
Yes No
Has it been marketedin the United States for a specific
OTC indication for a materialtime and to a material extent?
Does available evidenceof safety and effectiveness
warrant inclusion in anOTC monograph?
Is marketingexclusively desired?
OTC monograph
Is the proposedindication appropriate
for non-prescription use?
Is there sufficient evidenceof safety and effectiveness
and adequate CMC informationto support an NDA?
Yes
Yes
Yes
No
No
No
No
INDNDA application
Yes
NoYes
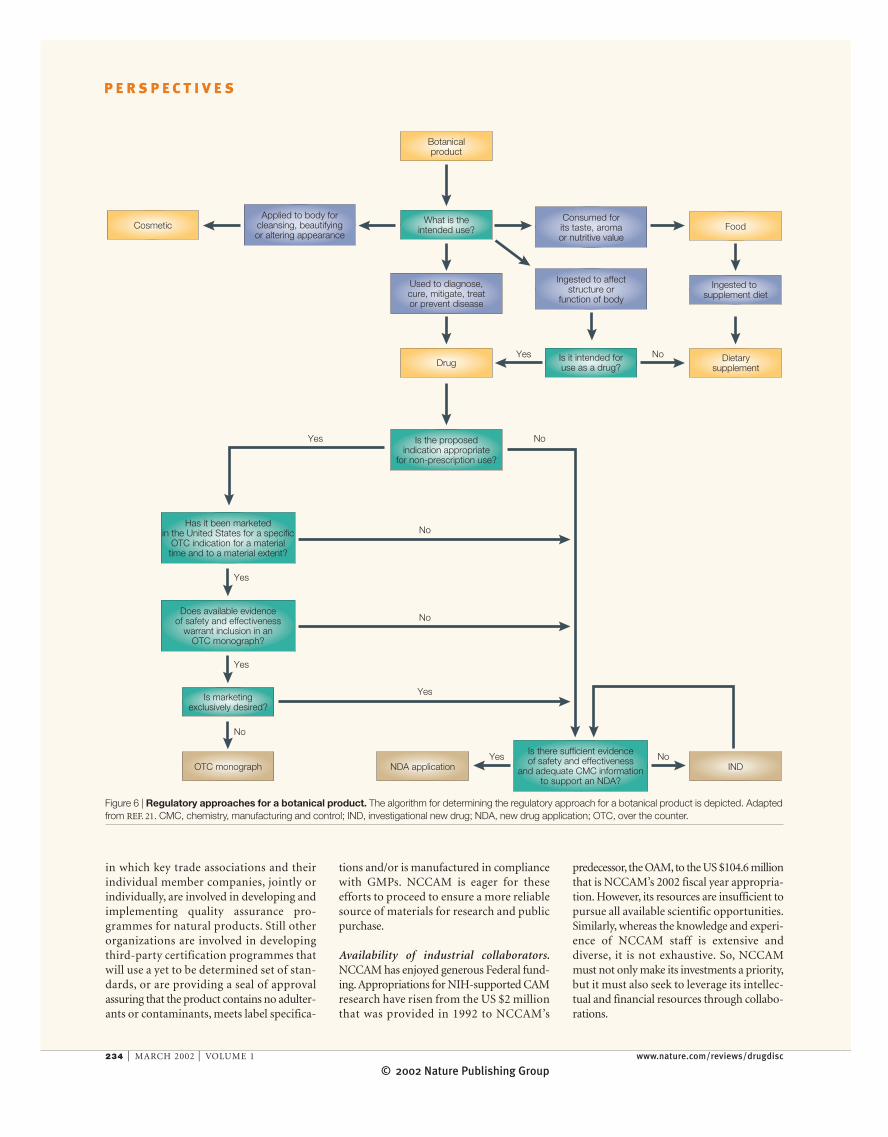
Figure 6 | Regulatory approaches for a botanical product. The algorithm for determining the regulatory approach for a botanical product is depicted. Adaptedfrom REF. 21. CMC, chemistry, manufacturing and control; IND, investigational new drug; NDA, new drug application; OTC, over the counter.
© 2002 Nature Publishing Group
P E R S P E C T I V E S
NATURE REVIEWS | DRUG DISCOVERY VOLUME 1 | MARCH 2002 | 235
NCCAM sees opportunities for collabora-tion in CAM product development withindustry through sharing of proprietaryproducts, preliminary data, technologies andcosts; exploiting complementary interests indefining basic mechanisms and pursuingparticular treatment indications; providingoptimal study design management and over-sight; comparing products from differentcompanies; and providing an imprimatur ofobjectivity to CAM studies.
Industry members at the meeting articu-lated their perception of advantages for theircollaboration with NCCAM, including thepossibility to acquire: exclusive results on acompany’s formulated product; research datato permit exclusive product claims, some ofwhich might result in product licensure andapproval by the FDA; expert input fromskilled academicians on trial design; andpublic credibility. Moreover, they cited theopportunity for suppliers to create thedemand for a specific ingredient through newresearch, and for health professional groups tocontribute input in the design and manage-ment of multicentre trials.
Some, however, saw industry–NCCAMcollaborations as being of limited impact.Without market exclusivity, companies can-not capture a return on their investment,especially if the results of the research on awidely available product are made public.
The drug model for botanicalsHowever, this view is not universally held.Encouraged by regulatory policies underdevelopment by the Center for DrugEvaluation and Research (CDER) of theFDA21 that are different from those that areapplied to synthetic or highly purified drugs,some members of industry believe that CAMproducts have an advantage relative to con-ventional drugs in feeding the drug develop-ment pipeline. CAM products have alreadyaccrued extensive human experience, indicat-ing safety and effectiveness by virtue of theirwidespread use over long periods of time.Therefore, the draft guidance for industryrelated to the development of botanical drugproducts states that applicants might submitreduced documentation of preclinical safetyand of CHEMISTRY, MANUFACTURING, AND CONTROLS
(CMCs) to support an INVESTIGATIONAL NEW DRUG
(IND) for initial clinical studies of botanicalsthat have been legally marketed in the UnitedStates as DIETARY SUPPLEMENTS or cosmeticswithout any known safety concerns. Inpractical terms, this means that approvalscould be earned several years more quicklyand at much less cost than for conventional,single-chemical-entity drugs (see FIG. 6 for a
commitment to work together to improvepublic health, while protecting intellectualproperty and the commercial needs ofinvestors.
To extend this model to the CAM arena,NCCAM convened a colloquium to exploreopportunities to collaborate with companiesthat supply raw materials and manufactureand market CAM therapeutics (for example,HERBAL THERAPIES and other biologically basedtreatments), and organizations that developand apply standards to determine the qualityand safety of these products19,20.
The colloquium was successful in initiat-ing a productive dialogue between NCCAMand its stakeholders in the CAM therapeuticsindustry. The industry sees the results ofNCCAM-funded clinical research that poten-tially would confirm the safety and efficacy ofa commodity as a genuine boon, because thehigh costs of research would be borne by thegovernment. This is especially true for prod-ucts that could have a significant impact ifused to cure, treat or mitigate disease (that is,for use as drugs rather than supplements).However, the extent to which productivecollaborations will be established with thissegment of industry remains unclear.
NCCAM’s success in enlisting other com-ponents of the NIH as partners and co-sponsors of large Phase III trials has beengratifying. For example, Phase III trials areunderway to evaluate: St John’s wort fordepression in collaboration with the NationalInstitute of Mental Health and the Office ofDietary Supplements; Ginkgo biloba to preventdementia in collaboration with the NationalInstitute on Aging, the National Heart, Lung,and Blood Institute, and the NationalInstitute of Neurological Disorders andStroke; and glucosamine and chondroitinsulphate for osteoarthritis, in collaborationwith the National Institute of Arthritis andMusculoskeletal and Skin Diseases.
In addition, the NIH Institutes andCenters have a rich tradition of collaborationwith industry related to conventional drugdiscovery and development. Such collabora-tion includes informal sharing of informa-tion, and developing letters of understanding,materials transfer agreements, confidentialdisclosures, clinical trial agreements,COOPERATIVE RESEARCH AND DEVELOPMENT AGREEMENTS
(CRADAs)17 and license agreements. Thesecooperative efforts are encouraged by US law(BAYH–DOLE ACT)18, and are founded on a genuine
Glossary box 1
AYURVEDA
Ayurveda is India’s traditional system of medicine.Ayurvedic medicine (meaning “science of life”) is acomprehensive system of medicine that places equalemphasis on the body, mind and spirit, and strives torestore the innate harmony of the individual. Some ofthe primary Ayurvedic treatments include diet, exercise,meditation, herbs, massage, exposure to sunlight andcontrolled breathing.
BAYH–DOLE ACT OF 1980
The Bayh–Dole Act of 1980 guaranteesorganizations/investigators the right to patent and retaintitle to their inventions from research sponsored withgovernment funds. The law was enacted to promote thetransfer, commercialization and utilization of federallyfunded technologies.
BIOFEEDBACK
A process for monitoring a body function (such asbreathing, heart rate and blood pressure), and alteringthe function through relaxation or imagery.
CHEMISTRY, MANUFACTURING AND CONTROLS
(CMCs). Extensive, detailed documentation of the drugunder study, including its structural formula, animal-testing results and manufacturing information, all ofwhich are required for an investigational new drug(IND) application.
CHIROPRACTIC
A system of treatment that is based on the relationshipbetween structure (primarily the spine) and function,and how that relationship affects the preservation andrestoration of health.
COOPERATIVE RESEARCH AND DEVELOPMENT
AGREEMENT
(CRADA). A provision of the Federal TechnologyTransfer Act of 1986 that permits the directors of gov-ernment-operated Federal laboratories to enter intocooperative research and development agreements onbehalf of such agencies with other Federal agencies,units of state or local government, industrial organiza-tions, public and private foundations, and nonprofitorganizations (including universities).
DIETARY SUPPLEMENT
A dietary supplement is a product that: contains one ormore ingredients (such as vitamins and minerals, andherbs or botanicals) that is intended to supplement thediet; is intended for human use; is a tablet, capsule, pow-der or some other form that is “not represented as con-ventional food [or] for use as a sole item of a meal ordiet,”; passes through the alimentary canal; and was not anew drug or biological product before being marketed asa dietary supplement or food in this country.
GOOD MANUFACTURING PRACTICES
(GMPs). Systems, processes and controls that are usedin the manufacture of consumer products, particularlyFDA-regulated products, that help to ensure the qualityof finished goods.
HERBS
Plants or plant products that produce or contain chemi-cals that act on the body.
HERBAL THERAPIES
Individual herbs or mixtures of herbs that are used fortherapeutic value.
© 2002 Nature Publishing Group236 | MARCH 2002 | VOLUME 1 www.nature.com/reviews/drugdisc
P E R S P E C T I V E S
repertoire, either as dietary supplements —the use of which is found to be safe andeffective — or as botanical drugs. In doing so,NCCAM will continue to make the most ofits resources through collaborations withboth public and private partners.
Linda W. Engel and Stephen E. Straus are at theNational Center for Complementary and
Alternative Medicine (NCCAM), NationalInstitutes of Health, 31 Center Drive, Bethesda,
Maryland 20892, USA. Correspondence to: L.W.E.email: [email protected]
DOI: 10.1038/nrd750
1. Eisenberg, D. M. et al. Trends in alternative medicine usein the United States, 1990–1997. J. Am. Med. Assoc.280, 1569—1575 (1998).
2. Kessler, R. C. et al. Long-term trends in the use ofcomplementary and alternative medical therapies inthe United States. Ann. Intern. Med. 135, 262—268(2001).
3. Goldbeck-Wood, S. et al. Complementary medicine isbooming worldwide. Br. Med. J. 313, 131–133 (1996).
4. House of Lords Session 1999–2000, Select Committeeon Science and Technology, Sixth Report,Complementary and Alternative Medicine, 21 November2000.
5. Astin, J. A. Why patients use alternative medicine: resultsof a national study. J. Am. Med. Assoc. 279, 1548—1553 (1998).
6. Clark, A. M. Natural products as a resource for newdrugs. Pharm. Res. 13, 1133—1141 (1996).
7. Tyler, V. E., Brady, L. R. & Robbers, J. E. Pharmacognosy9th edn (Lea & Febiger, Philidelphia, 1988).
8. Schultz, V., Hansel, R. & Tyler, V. E. RationalPhytotherapy: A Physician’s Guide to Herbal Medicine4th edn (Springer, Berlin, 2001).
9. Expanding Horizons of Healthcare: Five-Year StrategicPlan, 2001–2005, National Center for Complementaryand Alternative Medicine, National Institutes of Health.
10. Pub L no. 75–717, 52 Stat 1040 (1938) 21 USC 9 (FoodDrug and Cosmetic Act 1938).
11. Pub L no. 87–781, § 102(c), 76 Stat 780 (1962) (codifiedat 21 USC § 355(d)(5)) (Kefauver Harris Amendment of1962).
12. Pub L no. 103–417, 108 Stat 4325 (1994) 21 USC 231(The Dietary Supplement Health and Education Act of1994).
13. Bass, I. S. & Raubicheck, C. J. Marketing DietarySupplements (Food and Drug Law Institute, WashingtonDC, 2000).
14. Federal Register. House Government Reform Committee.Six Years After the Enactment of DSHEA: The Status ofNational and International Dietary Supplement Regulation(March 20, 2001).
15. Blumenthal, M. in The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines(eds Blumenthal, M. et al.) 17 (American BotanicalCouncil, Austin, Texas, 1998).
16. Harkey, M. R., Henderson, G. L., Gershwin, M. E.,Stern, J. S. & Hackman, R. M. Variability in commercialginseng products: an analysis of 25 preparations. Am. J. Clin. Nutr. 73, 1101—1106 (2001).
17. Pub L no. 96–517, 94 Stat 3018 (1980) (codified at 35 USC 200 et seq) (The Bayh–Dole Act of 1980).
18. Pub L no. 99–502, 100 Stat 1785 (1986) (codified at 15USC § 3710 (a)) (Amendment to the Stevenson–WydlerTechnology Innovation Act of 1980, commonly known asthe Federal Technology Transfer Act of 1986).
19. Exploring Opportunities for Collaboration with Industry.National Center for Complementary and AlternativeMedicine, National Institutes of Health, 2001.
20. Engel, L. W., Weinberg, M. S., Coates, P. M. and theColloquium Planning Group. NCCAM-IndustryColloquium: exploring opportunities for collaboration. J. Altern. Complement. Med. 7, 579—582 (2001).
21. Guidance for Industry: Botanical Drug Products. DraftGuidance, Center for Drug Evaluation and Research, USFood and Drug Administration, 2000.
22. Kaptchuk, T. J. & Eisenberg, D. M. Varieties of healing. 2: A taxonomy of unconventional healing practices. Ann.Intern. Med. 135, 196–204 (2001).
23. Hoffman, F. A. & Rheinstein, P. in Legal Medicine 5th edn(eds Sanbar, S. S. et al.) 560–584 (Mosby, St Louis,2001).
schematic representation of the regulatoryapproaches that can be taken for marketingbotanical drug products in the UnitedStates).
Some pharmaceutical companies believethere is a very large market for multicompo-nent prescription botanical drugs that arederived from herbal products that would beeligible for reimbursement by third-partypayers. Their interest in developing thesedrugs arises not only because of the potentialfor faster development, especially if toxicol-ogy data are already available, but alsobecause of their assessment that botanicaldrugs will fill unmet market needs for safer,first-line therapies in cases in which no safesynthetic drugs are available, and as naturalalternatives to synthetics.
Furthermore, the proposed policy wouldallow companies to capture administrativemarket protection in the absence of patentprotection. The draft guidance provides thatwhen a product is approved under a new drugapplication (NDA), the approval is specific tothe applicant’s drug product, and the appli-cant might be eligible for marketing exclu-sivity. In the case of new chemical entities, for
which botanical drugs are considered, com-panies are afforded a five-year period ofexclusivity. During this time, generic drugcompanies are blocked from gaining approvalfor a generic botanical drug unless they tooconduct all studies that are necessary to provethe safety and effectiveness of their products.
ConclusionThe opportunities presented by safe and effec-tive CAM therapeutics are many, andNCCAM is committed to exploring them inthe context of rigorous science, in spite of thechallenges in conducting such research.NCCAM-supported basic and clinical studiesmight identify important single-chemicalentities as promising lead compounds forpotential drug development sponsored byother Institutes and Centers. They might alsolead to the development of botanical drugsunder the aegis of NCCAM. Importantly,NCCAM looks to clinical studies to determinethe safety and efficacy of dietary supplements,as they are used at present by individuals inthe United States. Throughout, NCCAM willmaintain its focus on realizing the potential ofnatural products to expand the health-care
Glossary box 2
HOMEOPATHY
A Western system of medicine that is based on the prin-ciple that ‘like cures like’, — that is, the same substancethat in large doses produces the symptoms of an illness,in very minute doses cures it. Homeopathic physiciansbelieve that the more dilute the remedy, the greater itspotency. Therefore, homeopaths use small doses of spe-cially prepared plant extracts and minerals to stimulatethe body’s defence mechanisms and healing processes inorder to treat illness.
INVESTIGATIONAL NEW DRUG (IND) APPLICATION
A request for authorization from the US Food and DrugAdministration (FDA) to administer an investigationaldrug or biological product to humans.
MASSAGE
The manipulation of the soft tissues of the body to normalize those tissues.
MEDITATION
A self-directed practice for relaxing the body and calm-ing the mind in which the meditator makes a concen-trated effort to focus on a single thought in order to stillthe mind’s inclination to mull over the thousands ofdemands and details of daily life.
NATUROPATHIC MEDICINE
A system of treatment that views disease as a manifesta-tion of alterations in the processes by which the bodynaturally heals itself. It emphasizes health restoration aswell as disease treatment. Naturopathic physicians usean array of healing practices, including diet and clinicalnutrition; homeopathy; acupuncture; herbal medicine;hydrotherapy (the use of water in a range of tempera-tures and methods of applications); spinal and soft-tissue
manipulation; physical therapies involving electric cur-rents, ultrasound and light therapy; therapeutic coun-selling; and pharmacology.
QI GONG
Qi (pronounced chi) gong is a component of traditionaloriental medicine that combines movement, meditationand the regulation of breathing to enhance the flow ofvital energy (qi) in the body, to improve blood circula-tion and to enhance immune function.
REIKI
Meaning Universal Life Energy, Reiki is based on thebelief that by channelling spiritual energy through thepractitioner the spirit is healed, and it in turn heals thephysical body.
SPECIAL DIET
A special diet therapy that is believed to prevent and/orcontrol illness and/or promote health, such as thoseproposed by Drs Atkins, Ornish and Pritikin.
THERAPEUTIC TOUCH
Therapeutic touch is derived from the ancient techniqueof ‘laying-on of hands’, and is based on the premise thatit is the healing force of the therapist that affects thepatient’s recovery and that healing is promoted whenthe body’s energies are in balance.
TRADITIONAL ORIENTAL MEDICINE
Traditional oriental medicine emphasizes the properbalance or disturbances of qi — or vital energy — inhealth and disease, respectively. Traditional orientalmedicine consists of a group of techniques and meth-ods, including acupuncture, herbal medicine, orientalmassage and qi gong (a form of energy therapy).

© 2002 Nature Publishing Group
P E R S P E C T I V E S
therefore intrinsically reductionist; it aims tofind underlying principles, not only to collateisolated facts.
The pharmacologist can chose to study theinteractions between living organisms anddrugs or medicines at any level of integrationand using any methodology available.Nevertheless, the understanding of interac-tions between medicines and the most com-plex of systems — the intact being — is theultimate goal. Of course, this also perfectlydescribes the process of drug discovery.
Many pharmacologists (and indeed manyscientists who do not describe themselves aspharmacologists) study biological processes atdifferent levels of integration to define thepathways involved. The aim here is to under-stand not only the physiology, but also thepathophysiology, of the system studied. As wecome to understand which malfunction ofwhich components in a signalling cascadeleads to disease or a symptom of disease, wealso identify specific sub-processes that, ifmodified, might relieve the disease or symp-toms of disease. By this process, we have iden-tified a potential drug target. It must beemphasized that this drug target is not neces-sarily the protein(s) that is specifically affectedin the disease, but could equally well be acomponent of a parallel pathway that, whenacted on, will result in a normalized function.
Experience tells us that any potential drugtarget can be part of many physiological andpathophysiological signal cascades in manycells. So, although specificity of action isalways the goal, such specificity is rarely, ifever, absolute, and relative selectivity is gen-erally the best we can obtain. The all-important issue of specificity or selectivityis related to what can be called target vali-dation. We need to know that when weinterfere with the proposed drug target, notonly do we achieve the effect we aim for,but we also do not see secondary effects, or
The International Union of Pharmacology(IUPHAR) enthusiastically welcomes thedecision by the Nature Publishing Group tolaunch its new journal, Nature ReviewsDrug Discovery. The title of the new journalposes interesting questions forpharmacologists. Why ‘Drug Discovery’?Would we have preferred ‘Pharmacology’?And do these distinctions even matter, asaren’t all pharmacologists involvedsomehow in drug discovery?
Within the International Union of Pharma-cology (IUPHAR), several answers to thequestion “What is pharmacology?” have beengiven1. The subject of pharmacology has beengiven various definitions in dictionaries andtextbooks, as the few examples given in BOX 1
will illustrate. Each of these one-sentencedefinitions seems to leave out somethingimportant, and it is probable that similarattempts to define such a rich subject in a fewwords would be equally inadequate. However,these definitions emphasize different andcrucially important aspects, which togetherdefine the subject.
Pharmacology is concerned with drugs, bywhich we mean any biologically active sub-stance (compare with the original Greek wordpharmakon, which means poison). It hascome to be deeply involved with the idea ofspecificity or selectivity of drugs, as this is the
basis for medical use — therapeutic effectsshould be maximized and side effects mini-mized. It therefore requires quantitativemethodology. Pharmacology is particularlyconcerned with medicines — drugs that areused clinically in either man or animals —and especially with the interactions betweenliving systems and medicines or drugs. Theseinteractions are reciprocal: the living organ-ism affects the drug or medicine, and the drugor medicine affects the organism. In someinstances, notably antimicrobial drugs, morethan one biological organism is affected.Pharmacology aims to elucidate the mecha-nisms that underlie these interactions, and is
24. Klayman, D. L. Qinghaosu (artemisinin): an antimalarialdrug from China. Science 228, 1049–1055 (1985).
25. Meshnick, S. R., Taylor, T. E. & Kamchonwongpaisan, S.Artemisinin and the antimalarial endoperoxides: fromherbal remedy to targeted chemotherapy. Microbiol. Rev.60, 301–315 (1996).
26. Porter, R. The Greatest Benefit to Mankind: a MedicalHistory of Humanity from Antiquity to the Present (HarperCollins, London, 1997).
27. Lemli, J. Senna — an old drug in modern research.Pharmacology 36, 3–6 (1988).
28. Franz, G. The senna drug and its chemistry.Pharmacology 47, 2–6 (1993).
29. World Health Organization (WHO). WHO Monographs onSelected Medicinal Plants Vol. 1 (WHO, Geneva, 1999).
AcknowledgementsThe authors thank I. Scott–Bass, J. Betz, R. Temple, J. Thompsonand R. Upton for their critical reading of the manuscript and helpfulinput. We are especially grateful to J. Tisch for meticulouslyresearching background materials.
Online links
DATABASESThe following terms in this article are linked online to:Medscape DrugInfo:http://promini.medscape.com/drugdb/search.aspmorphine | quinine | reserpine | vincristine
FURTHER INFORMATIONComplementary and Alternative Medicine, House of LordsSession 1999–2000: http://www.parliament.the-stationery-office.co.uk/pa/ld/ldselinf.htmExploring Opportunities for Collaboration with Industry:http://nccam.nih.gov/colloquium Guidance for Industry: Botanical Drug Products:http://www.fda.gov/cder/guidance/1221dft.htmThe NCCAM Five-Year Strategic Plan, 2001–2005:http://nccam.nih.gov/strategicThe NIH NCCAM web site: http://nccam.nih.govAccess to this interactive links box is free online.
NATURE REVIEWS | DRUG DISCOVERY VOLUME 1 | MARCH 2002 | 237
The role of pharmacology in drug discoveryBertil B. Fredholm, William W. Fleming, Paul M. Vanhoutte andThéophile Godfraind
O P I N I O N
Box 1 | Various attempts to define Pharmacology
• The scientific study of medicines and drugs.
• The branch of science relating to drugs and medicines.
• The study of substances that interact with living systemsthrough chemical processes, especially by binding toregulatory molecules and activating or inhibiting normal body processes.
• The science studying the interactions between chemicals and living beings directed to prevent,ameliorate or cure the deleterious consequences of their diseases.
• The study of the manner in which the function of living systems is affected by chemical agents.
• The science that deals with the mechanism of action, uses and adverse effects of drugs.
• The scientific discipline that deals with the interaction between chemical agents and the livingorganism.
• Pharmacology is what pharmacologists do.





























