Embed Size (px)
Citation preview
BY DR. ABIDEMI J. AKINDELE
Department of Pharmacology, Therapeutics & Toxicology Faculty of Basic Medical Sciences
College of Medicine, University of Lagos, Lagos, Nigeria
AJAKINDELE2016/17
ADRENOCEPTORS Adrenoceptors mediate central and peripheral actions of
NA (NT) & Adr. (hormone & NT).
Found in nearly all peripheral tissues & on many neuronal
populations within the CNS.
NA & Adr. play important roles in BP control, myocardial
contractile rate & force, airway reactivity and variety of
metabolic & CNS functions.
AJAKINDELE2016/17
ADRENOCEPTORS CONT’D
Agonists & antagonists have proved useful in treatment of
variety of diseases including hypertension, angina pectoris,
CHF, asthma, depression, BPH & glaucoma.
Also useful in therapeutic situations e.g. shock, premature
labour, opioid withdrawal & as adjuncts to general
anaesthesia.
AJAKINDELE2016/17
HISTORICAL PERSPECTIVE
Oliver & Schafer (1896)
Demonstrated that injection of extracts of adrenal gland
caused rise in arterial pressure.
Adrenaline was subsequently isolated as the active
compound in the adrenal gland extracts.
Dale (1913)
Demonstrated that Adr. Caused 2 distinct effects:
vasoconstriction in certain vascular beds and vasodilation
in others.
AJAKINDELE2016/17
HISTORICAL PERSPECTIVE
Vasoconstriction component was observed to be abolished
by pre-treatment of animal with an ergot derivative
[selective α- adrenoceptor antagonist(s)].
Adr. then caused fall in arterial pressure [α-blockade
resulted in transition to β-adrenoceptor agonist effect(s)].
Ahlquist (1948)
Proposed existence of more than one adrenergic receptor
based on abilities of Adr., NA & other agonists to regulate
various physiological processes.
AJAKINDELE2016/17
These drugs were found to cause either contraction or
relaxation of smooth muscles depending on site, dose and
agent.
Ahlquist proposed designations α & β: αRs on smooth
muscles where catecholamines produce excitatory
responses & βRs where inhibitory responses are produced.
GIT presents an exception as it is relaxed by either α or β
agonist action.
AJAKINDELE2016/17
Rank order of potency: β → Isoprenaline > Adr. ≥ NA; α →
Adr. ≥ NA ≥ Isoprenaline.
1955
Selective β-adrenoceptor antagonists were developed,
Ahlquist’s original classification was confirmed & further
subdivisions of α & β adrenoceptors were suggested.
AJAKINDELE2016/17
Initial classification corroborated by finding that certain
antagonists produce selective blockade of effects of
adrenergic nerve impulses & sympathomimetic agents @ α-
adrenoceptors (e.g. phenoxybenzamine) & others produce
selective β-adrenoceptor blockade (e.g. propranolol).
Lands et al. (1967)
Compared rank order of potency in a way similar to work
of Ahlquist and concluded that there are two subtypes of β-
adrenoceptor (β1 & β2).
AJAKINDELE2016/17
β1-ADR (dominant receptor in heart and adipose tissue)
was equally sensitive to NA & Adr.
β2-ADR (responsible for relaxation of vascular, uterine &
airway smooth muscles) was much less sensitive to NA vis-
à-vis Adr.
Subsequent studies with agonists & antagonists have
confirmed existence of α1, α2, β1, β2 & β3 – ADRs, all being
GPCRs with distinct 2nd messenger systems.
Pharmacological & molecular evidences have throw-up
subtypes of ADRs.
AJAKINDELE2016/17
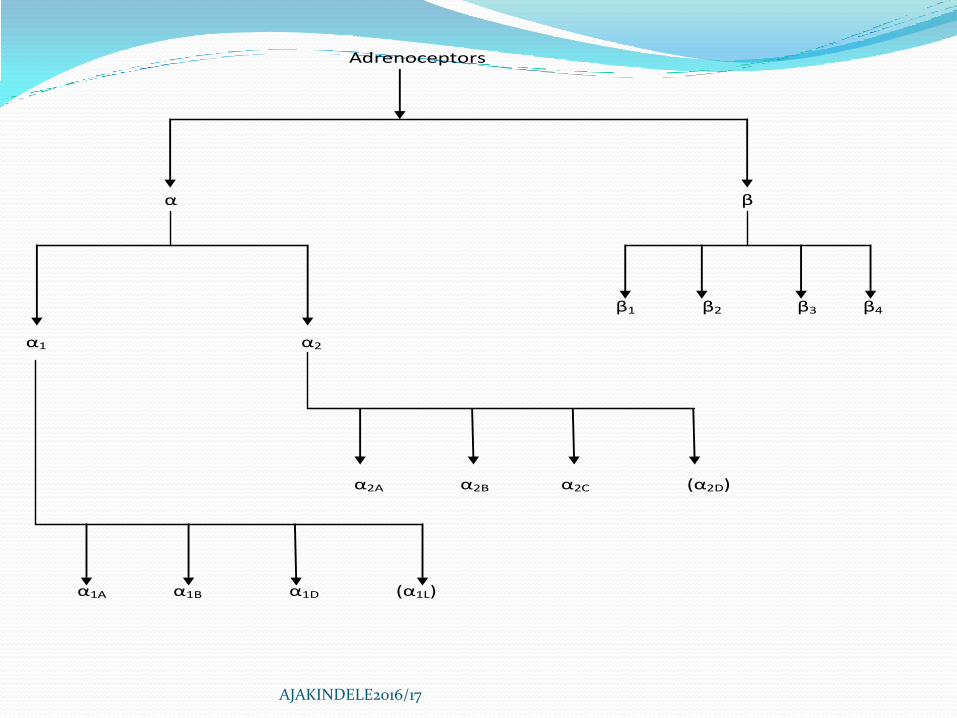
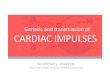
Adrenoceptors
α β
β1 β2 β3 β4
α1 α2
α2A α2B α2C (α2D)
α1A α1B α1D (α1L)
AJAKINDELE2016/17
α1L may represent a particular conformational state of the
α1A-ADR.
α2D is a species orthologue of the human α2A subtype hence
it is not considered to be a separate subtype.
AJAKINDELE2016/17
AJAKINDELE2016/17
AJAKINDELE2016/17
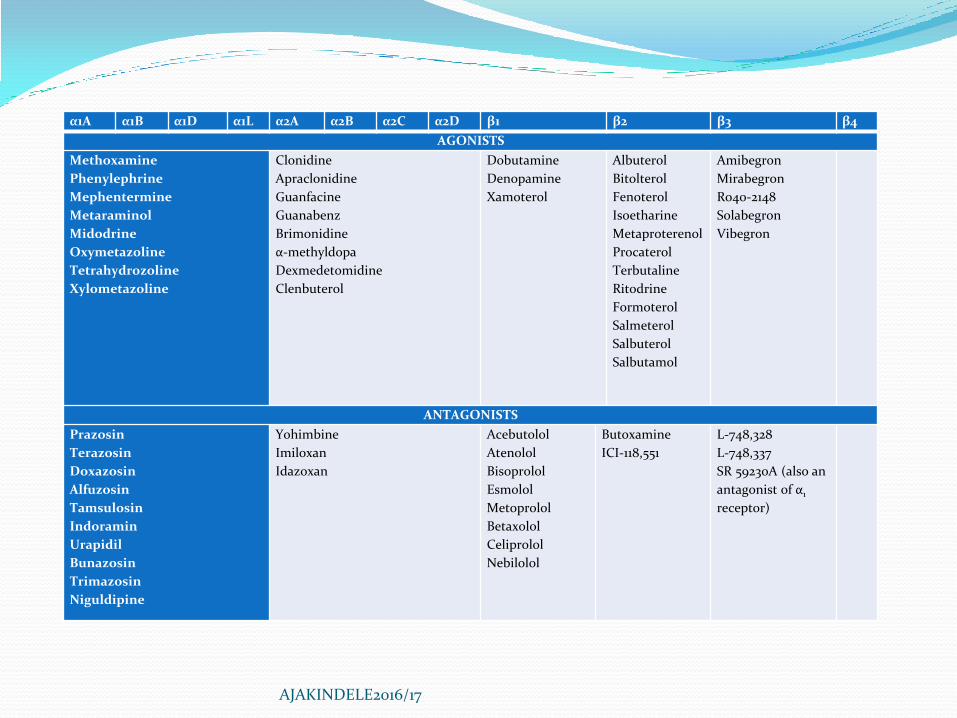
α1A α1B α1D α1L α2A α2B α2C α2D β1 β2 β3 β4
AGONISTS
Methoxamine
Phenylephrine
Mephentermine
Metaraminol
Midodrine
Oxymetazoline
Tetrahydrozoline
Xylometazoline
Clonidine
Apraclonidine
Guanfacine
Guanabenz
Brimonidine
α-methyldopa
Dexmedetomidine
Clenbuterol
Dobutamine
Denopamine
Xamoterol
Albuterol
Bitolterol
Fenoterol
Isoetharine
Metaproterenol
Procaterol
Terbutaline
Ritodrine
Formoterol
Salmeterol
Salbuterol
Salbutamol
Amibegron
Mirabegron
Ro40-2148
Solabegron
Vibegron
ANTAGONISTS
Prazosin
Terazosin
Doxazosin
Alfuzosin
Tamsulosin
Indoramin
Urapidil
Bunazosin
Trimazosin
Niguldipine
Yohimbine
Imiloxan
Idazoxan
Acebutolol
Atenolol
Bisoprolol
Esmolol
Metoprolol
Betaxolol
Celiprolol
Nebilolol
Butoxamine
ICI-118,551
L-748,328
L-748,337
SR 59230A (also an
antagonist of α1
receptor)
AGONISTS
Non-selective agonists: Adr. (α1, α2, β1 , β2 , β3); NA (α1, α2, β1
>> β2 ); Isoprenalol (β1 + β2).
α1 agonists: Methoxamine, Phenylephrine,
Mephentermine, Metaraminol, Midodrine,
Oxymetazoline, Tetrahydrozoline and Xylometazoline.
Mephentermine & Metaraminol also act indirectly to
release NA.
Midodrine is a pro-drug.
AJAKINDELE2016/17
AGONISTS (α1 agonists)
Prominent Pharmacological Action (PPA): Vasoconstriction
Principal Therapeutic Uses (PTUs): Pressor agents (Rx of
hypotension & shock – methoxamine & phenylephrine), nasal
decongestants (oxymetazoline, tetrahydrozoline, xylometazoline
& some preparations of phenylephrine).
Adverse Effects (AEs): Hypertension, headache, reflex
bradycardia, excitability, restlessness, dry mouth, sedation &
rebound hypertension ff. abrupt withdrawal.
AJAKINDELE2016/17
AGONISTS
α2 agonists: Clonidine, Apraclonidine, Guanfacine, Guanabenz,
Brimonidine, α-methyldopa, dexmedetomidine and Clenbuterol.
Apraclonidine & Brimonidine are used topically for glaucoma
and ocular hypertension.
Methyldopa is converted in CNS to α-methylNA (α2 agonist).
Used very occasionally as centrally-acting sympatholytic
vasodilators for the Rx of hypertension.
AJAKINDELE2016/17

AGONISTS (α2 agonists)
PPAs: ↓ sympathetic outflow resulting in ↓ peripheral
vascular resistance and ↓ production of aqueous humour.
PTUs: Adjunct therapy in shock; hypertension; to ↓
sympathetic response to withdrawal from narcotics,
alcohol & tobacco; glaucoma.
AEs: Sedation, dry mouth & nasal mucosa, bradycardia,
orthostatic hypotension, impotence, constipation, nausea
& gastric upset, bradyarrythmia, ↓ CO, hypotension etc.
AJAKINDELE2016/17
β1 agonists: Dobutamine, Denopamine and Xamoterol.
Use with caution in patients with hypertension or cardiac
arrhythmias; used only IV.
PPAs: ↑ in cardiac contractility; some ↑ in HR; ↑ AV
conduction.
PTUs: short term Rx of cardiac decompensation after
surgery or in patients with CHF or myocardial infarction.
AEs: ↑ BP and HR.
AJAKINDELE2016/17
β2 agonists: Albuterol, Bitolterol, Fenoterol, Isoetharine,
Metaproterenol, Procaterol, Terbutaline, Ritodrine (all
intermediate acting), Formoterol, Salmeterol (long acting)
& Salbutamol.
Use with caution in patients with CV disease (reduced by
inhalational administration); minimal side effects →
intermediate acting.
AJAKINDELE2016/17
Agonists (β2 agonists)
PPAs: Relaxation of bronchial smooth muscle; relaxation of
uterine SM; activation of other β2Rs after systemic
administration.
PTUs: Asthma & chronic obstructive pulmonary disease; acute
bronchospasm (short & intermediate acting drugs); premature
labour (Ritodrine); prophylaxis (long acting agents).
AEs: Headache, anxiety, nausea, muscle tremors, nervousness,
palpitations etc.
AJAKINDELE2016/17
β3 agonists: BRL 37344, CGP 12177 and CL 316243.
β4 agonists: ?
AJAKINDELE2016/17
ANTAGONISTS
α-non selective antagonists: Phenoxybenzamine,
Phentolamine and Tolazoline.
α1-selective antagonists: Prazosin, Terazosin, Doxazosin,
Alfuzosin, Tamsulosin, Indoramin, Urapidil, Bunazosin,
Trimazosin and Niguldipine.
PPAs: ↓peripheral vascular resistance; relax smooth
muscles in neck of bladder & in prostate.
PTUs: Primary hypertension; ↑ urine flow in BPH.
AEs: Postural hypotension when therapy is instituted.
AJAKINDELE2016/17
ANTAGONISTS CONT’D
α2-selective antagonists: Yohimbine, Imiloxan and
Idazoxan.
Blockade ↑ sympathetic outflow & potentiate release of NA
from nerve endings.
Results in activation of α1 & β1 Rs in the heart & peripheral
vasculature → ↑ BP.
AJAKINDELE2016/17
ANTAGONISTS CONT’D
β-non selective antagonists: Nadolol, Penbutolol, Pindolol,
Propranolol, Timolol, Carteolol, Carvedilol, Bucindolol
and Labetalol.
Carvedilol & Labetalol also block α1Rs.
β 1-selective antagonists: Acebutolol, Atenolol, Bisoprolol,
Esmolol, Metoprolol, Betaxolol, Celiprolol and Nebivolol.
β 2-selective antagonists: Butoxamine
AJAKINDELE2016/17
β-BLOCKERS
PPAs: ↓ HR; ↓ contractility; ↓ CO; slow conduction in atria & AV
node; ↑ refractory period, AV node; bronchoconstriction;
prolonged hypoglycaemia; ↓ plasma free fatty acids; ↓ HDLc; ↑
LDLc & triglycerides; hypokalemia.
PTUs: Angina pectoris; hypertension; cardiac arrhythmias; CHF;
pheochromocytoma; glaucoma; hypertropic obstructive
cardiomyopathy; hyperthyroidism; migraine prophylaxis; acute
panic symptoms; substance withdrawal; variceal bleeding in
portal hypertension.
AJAKINDELE2016/17

β-BLOCKERS CONT’D
AEs: Bradycardia; -ve ionotropic effect; ↓ CO;
bradyarrythmias; ↓ AV conduction; bronchoconstriction;
fatigue; sleep disturbances (insomnia, nightmares);
prolongation of hypoglycemia; sexual dysfunction in men;
drug interactions.
NB: Pharmacological effects depend largely on degree of
sympathoadrenal tone.
Bronchoconstriction is of concern in asthmatics & COPD.
AJAKINDELE2016/17
β-BLOCKERS CONT’D
Hypoglycemia is of concern in hypoglycemics and
diabetics.
Membrane stabilization effect associated with propranolol,
acebutolol, carvedilol & betaxolol only.
Intrinsic sympathomimetic activity (ISA) strong for
pindolol & weak for penbutolol, carteolol, labetalol &
betaxolol.
AJAKINDELE2016/17
β-BLOCKERS CONT’D
3rd generation non-selective agents (carteolol, carvedilol,
bucindolol & labetalol) have as their PPAs – membrane
stabilizing effect; ISA; vasodilation.
Their multiple mechanism of action includes – α1
antagonism; β2 agonism; release of NO; Ca2+ channel
blockade; opening of K+ channels.
AJAKINDELE2016/17