Embed Size (px)
Citation preview
Menorrhagia – An overview
By Dr Rukhsana Hussain ST117th November 2009
ObjectivesTo increase awareness of menorrhagia, its
causes and impact on individuals and societyTo cover key points in history-taking and
examinationTo increase awareness of medical and
surgical treatments available as outlined by the NICE guidelines
Menorrhagia - Definition“Excessive menstrual blood loss which interferes with a woman’s physical, emotional, social and material quality of life and which can occur alone or in combination with other symptoms” (NICE guidelines 2007)
Objective blood loss >80ml no longer important in defining menorrhagia
Impact of menorrhagia1 in 20 women aged 30-49 years consults GP
each year with menorrhagiaMany women will have days off work due to
menorrhagia1 in 5 women in UK will have hysterectomy
before age of 60 years50% of all women who have a hysterectomy
for menorrhagia will have a normal uterus removed
Causes of menorrhagia4 main subtypes
1) Ovulatory2) Anovulatory3) Anatomic4) Other causes
Ovulatory menorrhagia“Primary” or “idiopathic” menorrhagia –
treatments guided by probable causesCharacterized by heavy bleeding during
regular cycles. Usually associated dysmenorrhoea and premenstrual symptoms
Probable causes Abnormal prostaglandin synthesisIncreased intrauterine fibrinolysisAcquired /congenital clotting disorders eg
VWD
Anovulatory menorrhagiaUsually irregular periods, often heavy and
frequently separated by long intervals. Usually minimal pain
Menorrhagia in adolescents usually anovulatory
Anovulatory cycles less common in 20-40 age group
Anovulatory menorrhagiaCommon in perimenopausal women Intermittent ovulation and ovarian
queiscence results in variability in LH/FSH and oestrogen causing erratic cycles
During this period follicles remaining in ovary are quite resistant to FSH – sometimes ovulation occurs after long follicular phase, other times it fails.
Anovulatory menorrhagia In delayed ovulation/anovulation
endometrium is thickened by prolonged stimulation by proliferative levels of oestrogen and is eventually shed in a long and heavy period
Long term anovulation increases risk of endometrial hyperplasia
Anovulatory menorrhagiaCauses include
HyperprolactinaemiaThyroid diseaseAdrenal diseaseAnorexia/BulimiaPituitary adenomaChronic illnessStressDrugs – eg. tricyclic antidepressants, steroids
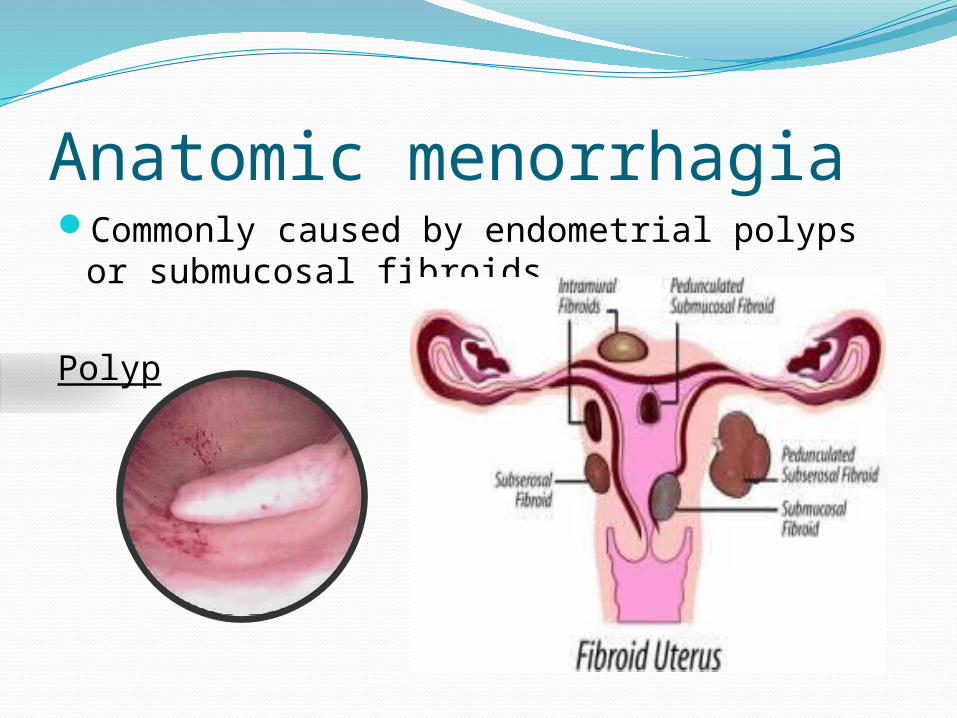
Anatomic menorrhagiaCommonly caused by endometrial polyps or
submucosal fibroids
Polyp
Other causes menorrhagiaCervicitis/endometritisIUDHyperoestrogenismEndometrial cancerCoagulopathy
History – key pointsAge at menarcheOnset and duration of periodCycle – regular or irregular? Length?Amount blood loss – clots? Flooding? Number
sanitary towels? Social impactChanges from previous bleeding patternsIntermenstrual bleedingPostcoital bleedingPelvic painDyspareunia
HistorySymptoms related to anaemia
- SOB/fatigue/dizzinessSymptoms of thyroid disease/systemic illnessPMH – Obstetric Hx, Fertility wishesDH- Warfarin? Aspirin? AllergiesSH – Stress? Smoking? Alcohol intake?FH – Bleeding disorders? Malignancies?
HistoryCover risk factors for Endometrial Cancer
ObesityAge > 45NulliparityPCOSTamoxifen1st degree relative with breast, colon or
endometrial cancerPersonal hx breast/colon cancerUnopposed oestrogen treatment
ExaminationGeneral – pallor? Bruising? Signs of thyroid
disease? BMI?Abdominal examination – fibroid uterus? Pelvic examination
InvestigationsFBC – exclude anaemiaCervical smear if dueIf IMB/PCB vaginal swab for chlamydia screenUSS pelvis if indicatedReferral for hysteroscopy and endometrial biopsy –
Persistent IMB, >45 years, treatment failure, ineffective treatment , risk factors endometrial cancer
NO value of TFT unless signs thyroid disease. NO value of hormone levels according to NICE guidelines
Medical treatments – First LineLevonorgestrel-releasing intrauterine
system(MIRENA)
- Slowly releases progestogen, prevents proliferation of endometrium
- Reduces menstrual loss by 86% in 3 months, and by 97% at 12 months
- Effective contraceptive- Return to fertility after removal
Medical treatments – First LineSide effects Mirena coil
- progestagenic effects – breast tenderness, acne, headaches
- irregular bleeding at start may last for 6 mths- functional ovarian cystsAlso, risk of uterine perforation at time of insertion
Medical treatments – Second line Tranexamic acidMefenamic acid/NSAIDsCOCP
Can be used first line if Mirena not acceptable to patient
Tranexamic acidAntifibrinolytic agentMean reduction blood loss nearly 50%Dose 1-1.5g tds during menstruation onlyMay be combined with mefenamic acid esp if
dysmenorrhoea prominentTheoretically increased risk DVT but little
evidence in studiesSuitable if patient wanting to conceiveUse for 3 cycles to determine effectiveness
Mefenamic acidReduces prostaglandin productionIndicated for menorrhagia and
dysmenorrhoeaMean reduction blood loss around 30%Dose 500mg tds – taken during menstruation
Side effects – indigestion, diarrhoea, worsening asthma, peptic ulceration
COCPPrevents proliferation of endometrium
therefore reducing blood loss Contraceptive Side effects - headache, mood change, fluid
retention, risk of DVT, stroke
Medical treatments – Third lineOral progestogen – norethisterone
Effective when given in high doses between day 5- 26 of cycle
Dose 5mg tdsInjected progestogen (Depo-provera)
Given every 3/12After 1 year 50% women amenorrhoeicDisadvantage of delayed return to fertility
Medical treatmentsGn-RH analogue injections Stop production of oestrogen and
progesterone inducing amenorrhoeaSide effects include menopausal- like
symptomsRisk of osteoporosis with longer than 6
month use
Surgical/radiological treatments Endometrial ablationUterine artery embolisationMyomectomyHysterectomy
Endometrial ablationIndication – severe impact on quality of life +
no desire to conceive + normal uterus (or small fibroids <3cm diameter)
Destroys womb lining Risk of perforation during procedurePossible side effects – vaginal discharge,
increased period pain
Uterine artery embolisationIndication – fibroids >3cm diameter, pressure
symptoms, not wanting surgery, wants to remain fertile
Small particles injected into blood vessels supplying uterus , block supply to fibroids causing shrinkage
Short hospital stay – usually overnightSide effects – persistent PV discharge, post
embolisation syndrome – pain, nausea, vomiting, fever. Risk of haemorrhage

MyomectomyIndication – fibroids > 3cm, severe impact on
quality of life
Risks associated with surgery – adhesions, infection, perforation, haemorrhage
Recurrence of fibroids possible

HysterectomyIndication – other treatments failed, no wish
to remain fertile, patient request after fully informed, desire for amenorrhoea
Vaginal /abdominal as indicatedMajor surgery – 4-5 days inpatient stay, risks
of surgeryLonger recovery time- months although
permanent solution for menorrhagia!

SummaryMenorrhagia is a common problemMirena coil is offered as first line treatment
and has reduced need for hysterectomies significantly
For women wanting to conceive in short term – tranexamic acid and mefenamic acid appropriate
For others COCP, norethisterone, Depo-provera can be effective
Surgical and radiological interventions available in secondary care setting

Referenceswww.nice.org.uk – Heavy menstrual bleeding
NICE 2007www.doctors.net.ukOxford Handbook of Obstetrics and
Gynaecology