Embed Size (px)
Citation preview

USAARL Report No. 90-3
IILaser Protection with Image Intensifier¢Q t Night Vision Devices
~By
O David J. Walsh
0
Sensory Research Division
S EECTEIAP261l9g03
February 1990 U
Approved fer publio release; distribution unlimited.
United States Army Aeromedical Research LaboratoryFort Rucker, Alabama 36362-5292

Notice
Oualified reauesters
Qualified requesters may obtain copies from the DefenseTechnical Information Center (DTIC), Cameron Station, Alexandria,Virginia 22314. Orders will be expedited if placed through thelibrarian or other person designated to request documents fromDTIC.
Change of address
Organizations receiving reports from the U.S. ArmyAeromedical Research Laboratory on automatic mailing lists shouldconfirm correct address when corresponding about laboratoryreports.
Disposition
Destroy this report when it is no longer needed. Do not returnto the originator.
Disclaimer
The views, opinions, and/or findings contained in this reportare those of the author(s) and should not be construed as anofficial Department of the Army position, policy, or decision,unless so designated by other official documentation. Citationof trade names in this report does not constitute an officialDepartment of the Army endorsement or approval of the use of suchcommercial items.
Reviewed:
THOMAS L. FREZELLP'C, MSDirector, Senso earch
Division Re sed for publication:
J.0. LaMOT$E, Ph.D. DAVID H. KARNVY yCOL, MS Colonel, MCChairman, Scientific CommandingReview Committee

UnclassifiedSECURITY CLASSIFICATION OF THIS PAGE
Form Approved
REPORT DOCUMENTATION PAGE OMB No. 0704-0188Ia. REPORT SECURITY CLASSIFICATION lb. RESTRICTIVE MARKINGSUnclassified2a. SECURITY CLASSIFICATION AUTHORITY 3. DISTRIBUTION /AVAILABILITY OF REPORT
2b. DECLASSIFICATION / DOWNGRADING SCHEDULE Approved for public release; distributionunlimited
4. PERFORMING ORGANIZATION REPORT NUMBER(S) S. MONITORING ORGANIZATION REPORT NUMBER(S)
USAARL Report No. 90-3* 6a. NAME OF PERFORMING ORGANIZATION 6b. OFFICE SYMBOL 7a. NAME OF MONITORING ORGANIZATIONU.S. Army Aeromedical Research (If applicable) U.S. Army Medical Research and Development
Laboratory JSGRD-UAS-VS Command6C. ADDRESS (City, State, and ZIP Code) 7b. ADDRESS (City, State, and ZIP Code)
Fort DetrickFort Rucker, AL 36362-5292 Frederick, MD 21701-5012Ba. NAME OF FUNDING I SPONSORING I8b. OFFICE SYMBOL 9. PROCUREMENT INSTRUMENT IDENTIFICATION NUMBER
ORGANIZATION | (If applicable)
Sc. ADDRESS (City, State, and ZIp Code) 10. SOURCE OF FUNDING NUMBERS
PROGRAM PROJECT TASK WORK UNITELEMENT NO. NO. NO. ACCESSION NO.
62787A 3M162787A8 BG 16411. TITLE (Include Security Classfication)
Laser Protection with Image Intensifier Night Vision Devices12. PERSONAL AUTHOR(S)
Walsh, David J.13a. TYPE OF REPORT I13b. TIME COVERED 114. DATE OF REPORT (Year, Month,Day) 115. PAGE COUNTFinalI FROM TO 1990 February 2216. SUPPLEMENTARY NOTATION
17. COSATI CODES 18. SUBJECT TERMS (Continue on reverse if necessary and identify by block number)FIELD GROUP SUB-GROUP20 06 laser, injury, protection, ANVIS, aviator, night vision
19. ABSTRACT (Continue on reverse if necessary and identify by block number)Current military ranging and targeting techriology employs high power laser systems.Since coherent (laser) energy with wavelengths in the visible and near infrared canseriously damage the retina if the eye, laser retinal injury has been the subject of manystudies. The results of these investigations are used by various agencies to recommendlaser eye protection. In the aviation community, since laser protective helmet visors are
not compatible with most common night vision devices (NVDs), i.e., AN/PVS-5 Night VisionGoggle (NVG) and Aviator's Night Vision Imaging System (ANVIS), the only laser protectioncurrently afforded the NVD aviator is a barrier-type protection provided by the device. -- •
(Continued)
20. DISTRIBUTION /AVAILABILITY OF ABSTRACT 21. ABSTRACT SECURITY CLASSIFICATIONrZUNCLASSIFIED/UNLIMITED 0 SAME AS RPT. 0 "TIC USERS Unclassified
22a. NAME OF RESPONSIBLE INDIVIDUAL 22b. T"%.EPHONE (Include Area Code) 22c. OFFICE SYMBOLChief, Scientific Tnformator, Center (205) 255-6907 SGRD-UAX-SI
D0 Form 1473, JUN 86 Previous edItIons are obsolete. SECURITY CLASSIFICATION OF THIS PAGE
Unclassified

19. ABSTRACT (Continued)
-' Based on eye anatomy and function, three retinal regions have been identified ascritical to protect - fovea, macula and peripapillary zone (1 to 2 degree annulussurrounding the optic disc). When full-coverage laser protection is not possible,minimum acceptable coverage must include these regions. A circular area whichincludes the critical regions would cover the central retina, i.e., area out to25 degrees from the visual axis.
During ANVIS use, coverage exceeds the recommended 25 degree minimum, but onlywhen the eyes are in the primary (straight ahead) position. With normal scanningeye movement, critical areas of the retina become exposed to laser damage. Contin-uous laser protection for the central retina, out to 25 degrees, will require eithera mechanical obstruction or a laser protective spectacle or visor which covers atleast 90 degrees. The mechanical laser protection provided by NVD wear alone is notadequate to protect the aviator.

Table of contents
Page
Background ............................... 3Retinal features ....... ........ . . ..... . . ......... 4Retinal damage from medical laser use ..................... 6Retinal damage mechanisms .................................. 7
Papillomacular bundle .................................... 7Optic nerve .............................................. 8Retinal sensitivity of laser damage ...................... 8
Retinal geometry and NVD protection ........................ 10NVD usage factors ................... ........ ........... 12Computer model of NVD protection ........................... 14Discussion ................................................. 16Conclusions ................................................ 18
References .................... .................... 20Appendix A................... o. ........... .. . o........ 21
List of fitures
Figure
1. Schematic of the right eye............ ......... 52. Papillomacular bundle. . ...... ................... 63. Thermal emission ...... o ....... ............... 94. Sensitivity of retina to laser energy damage.......... 105. Extended binocular vsual field ...................... 116. Laser protection provided by helmet ................... 127. ANVIS field-of-view (FOV) versus vertex distance...... 138. ANVIS mechanical laser protection..................... 169. Effect of eye rotation on 18mm ANVIS protection ....... 1710. Effect of eye rotation on 25mm ANVIS protection ....... 17
List 21 tables
Table
1. Size of binocular visual field ....................... 112. Values used in the laser protection model ............. 143. Lateral laser protection provided by ANVIS ............ 154. Effect of vertex distance on protection provided
by A IS. . . . . . . . . . . . . . . . . . . . . . 18 For
IU'IC TABUnannouncedJustification
Distribution/
Availability Codes1 Avail and/or
Dist Special
I'-

This page intentionally left blank.
2

Background
Current military ranging and targeting technology employshigh power laser systems. Since coherent (laser) light withwavelengths in the visible and near infrared can seriously damagethe retina of the eye, laser retinal injury has been the subjectof many studies (e.g., Wolfe, 1985). The results of theseinvestigations are used by various agencies to recommend lasereye protection.
The fovea of the eye, the region of the retina whichprovides maximum spatial resolution, i.e., visual acuity, is mostsensitive to the effects of high energy photic stimulation.Since loss of function can be devastating to aviators requiringfine resolution, most studies recommend limiting direct exposureto this region. Based on a review of accidental laser exposures,one investigator states that exposure outside the fovea wouldhave an insignificant effect on visual acuity unless secondaryphenomena, i.e., vitreal hemorrhage or retinal edema, eitherblocked light from reaching the fovea or distorted vision bydisrupting the organization of photoreceptors (Wolfe, 1985).
Since Army aviation missions place aviators in anenvironment prone to laser exposure, the development of laserprotection is a compelling concern. Current aviation developmentand procurement efforts are expected to provide at least twolevels of laser protection -- three-wavelength protection for dayuse, and two wavelength protection for night flying. Therestricted level of protection provided in the night device is atrade-off to achieve the minimum level of transmissivityrecommended for unaided night flight (Wiley, 1989).
The two vehicles presently used for laser protection arespectacles and helmet visors. As an interim measure, protectionin the form of laser spectacles has been provided for specificapplications, e.g., AH-64 aviators. The goal of the aviationcommunity, however, is to incorporate laser protection intohelmet visors. When laser protection needs are identified, ornew visors are developed to meet emergent laser threats, a simpleexchange of helmet visors can be made. As a helmet mounteddevice, the same visor provides protection for both spectacle(ametropic) and nonspectacle wearer. With laser protectivespectacles, ametropic aviators require laser spectaclesincorporating their vision correction.
The use of laser protective visors does have a majordisadvantage. Helmet visors are not compatible with the most
3

common night vision devices (NVDs)'. When the NVDs are movedfar enough forward (away from the eyes) to allow visordeployment, the NVD field-of-view (FOV) is reduced tounacceptable dimensions. During NVD-aided night flight, the NVDswill provide some barrier-type laser protection, i.e., physicallyblock the laser light. The NVDs protect only the central area ofthe retina while the user views the environment through thedevice. This leads to the perception that foveal exposure todamaging laser sources can occur only during infrequent "looks"under or around the NVD to view the environment unaided. In viewof this and reports stating extrafoveal laser-iAduced damage isnot as devastating as foveal damage (e.g., Wolfe), the use ofNVDs as the sole laser protective device for aided night flighthas been hesitantly accepted.
In response to a request from the U.S. Army Aviation SystemsCommand (AVSCOM) (Appendix A) to evaluate laser spectacles, theissue of laser protection for use with NVDs is being readdressed.This report presents the results of the evaluation.
Retinal features
Anatomically, the macula lies near the posterior pole of theeye (Figure 1). Within this area lies the fovea and thevascular-free foveola. When viewing an object directly, theimage is focused on the fovea. The dimensions of the macula andfovea vary depending on the metric used, e.g., density of cones,rod-free area, or vascular-free region, and on whether theanatomical or clinical designation is used (L'Esperance, 1989).For this report, diameters of 5 degrees and 12 degrees will beused for the fovea and macula, respectively (MIL-HDBK-141, 1962).
The central retina covers an area which extends 25 degreesfrom the center of the fovea, and the peripheral retina coversthe remainder of the field (Harrington, 1971). The most notablelandmark in the central retina is the optic disc, or the opticnerve head (Figure 1). At this location nerve fibers from theretina converge to form the optic nerve which carries visualinformation out of the eye. The high density of photoreceptorsin the macula area produces a large bundle of nerve fibers(papillomacular bundle) which courses nasally from the macula tothe temporal side of the optic disc (Figure 2). The papillo-macular bundle of nerve fibers is important because it carriesvisual information from the macula. Damage at any point alongthe nerve fibers carrying foveal information will result in a
'For this discussion, NVDs will include only the AN/AVS-6Aviator's Night Vision Imaging System (ANVIS).
4

M C pticdiscLine of sight
etina
Posterior hemisphere of eye
MTemporal F-@ Optic Nasal
disc
M = Macula F = Fovea
Figure 1. Schematic of the right eye. Two views show thelocations of critical regions - fovea, macula andoptic disc.
5

Macul ---- optic
disc
pigure 2. PapillOacUlar bundle. N~erve fibers course from
the
macula to the optic disc.
scotma ad dgradd aCitY Thus# while military
related laser
injr stuies primarily address the efecs
n et cental
j u ry studm a g t o t h e f o e a e x t r a fo v e a l d am ag e a
f e c e t a
Retinal damage from medical laser use
n fteee ~-
w~ith medi~cally indicated laser treat,*enton ther eye eth.
us o lser to treat retina
ceOrtcuari threa are
secif i pr tions rgarding~ treatment Of cetinaea Of
the
re ina Thesex areas include the papillomacular
bunde fth
necvefie laeteotCds an the peripapillary area,
t
ri. Theeio ~ oun the optic disc (Goldberg and Hierb~t
th~Pkpe retian., 1976a and b).
ie.# ept to usa asrelrytocaglt vessels either on
or73 above th enetiC dis eoa~~a~~andaroun
the optic disc
(p~i~aillrhe havc esule in central scotomas
and visionl
los. llr) oesuy(lderg and Herbst# 93,priail~
trae n r sudy in ld a eta toma with acuity reduced to
l0/20. i ailt te enta resute in a central scotoma,
with an acuity decreae frm 20/20 t figra~ tig(os
than 20/10 00). in a more recen 0eot ae uno h

peripapillary zone resulted in a central scotoma with acuity at20/200 (Swartz, Apple, and Creel, 1983).
One might argue that the medical use literature containscase studies of complications arising from laser damage topathological eyes, and such damage is less likely to occur inhealthy eyes. However, investigations of laser induced retinallesions on human eyes and animal models provide histologicalevidence of damage mechanisms consistent with laser energyabsorption by pigmentation (Apple, Goldberg, and Wyhinny, 1973;Apple et al., 1976a and b).
Retinal damage mechanisms
The primary damaging effects of laser on the eye areclassified into three major categories -- photochemical, thermaland ionizing (L'Esperance, 1989). The potential for immediatereduction in visual acuity associated with thermal and ionizingdamage makes these mechanisms militarily relevant.
Photocoagulation is the only important thermal effect whenconsidering retinal damage. This can be produced by laser lighthaving transmission spectra matching absorption properties ofavailable retinal pigmentation, e.g., melanin, hemoglobin, andxanthophyll. Light absorption by retinal pigment and subsequentemission of energy in the form of heat coagulates surroundingtissue. Among the group of lasers capable of photocoagulationare argon, krypton, dye, ruby, frequency-doubled neodymium, andneodymium/YAG lasers.
Photodisruption is a term used to describe the ionizingeffect produced by neodymium/YAG lasers. The extremely highenergy flux disintegrates the tissue into plasma at the focuspoint. Secondarily, shock and acoustic waves producedmechanically disrupt adjacent tissue (LIEsperance, 1989). Thiseffect is not limited to pigmented retinal tissue as is thethermal effect.
These two damage mechanisms form a basis for exploringdamage effects on two extramacular retinal areas, thepapillomacular bundle and optic nerve.
Papillomacular bundle
The nerve fibers which form the inner layer of the retinaare transparent to light. These fibers allow laser energy topass through to the outermost layers of the retina, e.g.,pigmented epithelium. The nerve fiber layer (NFL), including thepapillomacular bundle, is located a relatively safe distance fromthe pigmented epithelium, the site of most energy absorption.
7

Therefore, the thermal effect to the nerve fibers is minimal formost locations. However, damage to the NFL has been reportedwhen photocoagulation of arterioles and venules has beenattempted (Apple, Goldberg, and Wyhinny, 1973; Apple et al.,1976a). Since these vessels are located within the NFL, thedamage follows laser energy absorption by hemoglobin. The heatemission from a vessel nccurs in a radial pattern (Figure 3A)with consequent nerve "iber damage adjacent to the vessels(perivascular). This eff:ct can occur in the absence ofdestruction to the blood vessel. While the likelihood of adirect vascular irradiation may seem remote, in a group ofaccidental laser exposures from nonionizing lasers (N=12), 50percent resulted in sufficient vascular damage to cause a retinalhemorrhage (Wolfe, 1985).
The papillomacular bundle nerve fibers are at greatest riskat the optic disc. As the nerve fibers turn to enter the opticdisc, the distance between the fibers and the pigmentedepithelium is reduced (Figure 3B). Laser irradiation of theperipapillary pigmented epithelium has been shown to producecentral vision losses (Apple et al., 1976b; Swartz, Apple, andCreel, 1983).
With the photodisruption effect, from a neodymium/YAG laser,for example, there is the potential for NFL damage and centralvision loss. The severity of vision loss would depend on thelocation and extent of the damage to the papillomacular bundle.
Optic nerve
Optic nerve damage can occur in four ways. First, thermaldamage can result from light absorption and heat emission byvasculature of the nerve head margin. Second, ischemic damagecan occur when choroidal vessels adjacent to the optic disc arecoagulated. Third, direct coagulation of nerve tissue will occurin the presence of an extremely high power flux density, i.e.,resulting from a high power and a small spot size (L'Esperance,1989). Finally, photodisruption at the optic disc willdisintegrate never fibers. In any of these cases, a subsequentoptic neuritis (inflammation of the optic nerve) would beaccompanied by central vision loss.
Retinal sensitivit to laser daMage
Based on the anatomy of the eye and complications associatedwith medical laser use, one author (L'Esperance, 1989) classifiesretinal sensitivity to photocoagulation with a scale of 1 to 5.The fovea is the most sensitive retinal region. The second mostsensitive regions include the macula and a 1 to 2 degreeperipapillary zone (Figure 4).
Ia

A. Thermal emission from blood vessels
B. Thermal emission from pigmented epithelium
Nerve fiber layerSensory retinaPigmented epithelium
Choroid
Nerve fibers sparedOpticnerve Nerve fibers damaged
Figure 3. Thermal emission. Laser light absorbed by retinalpigment is emitted as thermal energy (arrows). A.Thermal energy is emitted radially from blood vessels.B. Thermal emission adjacent to optic disc candestroy nerve fibers.
9

Fovea Peripapillary zone
Macula 1 2~Optic
disc
Figure 4. Sensitivity of retina to laser energy damage. Thefovea is the most sensitive (1) area. The next mostsensitive (2) areas include the macula andperipapillary zone.
When there is an operational/performance trade-off whichprecludes full coverage laser protection for the eye, the minimumcoverage acceptable must include the two most sensitive areas ofthe retina. A circular area which includes the most sensitiveregions of the eye would cover the central retina, i.e., an areaextending out to 25 degrees from the visual axis.
Retn aeometrv and NVD rotetion
The normal binocular visual field covers an oval area withlimits listed in Table 1. Visual field measurements usually aretaken with the eyes fixed in the primary, or straight ahead,position. When the eyes move, the extents of the visual fieldincrease by an amount equal to the ocular excursion. Undernormal conditions, the eyes will move a limited amount before thehead turns. Standard human factors reference sources, e.g., MIL-HDBK-759A, suggest a preferred limit of 15 degrees and a maximumlimit of 20 degrees when designing visual displays. The maximumarea of potential retinal exposure used in this report expandsthe binocular visual field oval by 15 degrees in four directions.Figure 5 portrays the extended visual field. The two small blackovals in the figure represent the location of optic discs whilethe eyes are in the primary position.
10

Table 1.
Size of binocular visual field*
Angular ExtentDirection (degrees)
Temporal 100Nasal 100Superior 60Inferior 75
* Harrington, 1971
Figure 5. Extended binocular visual field. The large ovalrepresents the binocular visual field extended by 15degrees in each direction to account for eyemovements. The small dark ovals show the positions ofthe optic discs.
11

Figure 6 shows the protection provided by the SPH-4 helmet.This represents only a rough estimate since the area of pro-tection will vary depending on anatomic features of the wearer,helmet type, helmet size, helmet fit, etc. Anthropometric datalocating the position of the eyes relative to the helmet shell,although not available, could provide valuable information forfuture laser protection modelling.
NVD usage factors
While helmet visors protect most of the exposed visualfield, the protection provided by NVDs is limited by theirphysical dimensions and their positioning in front of the eyes.
Helmet-mounted NVDs are usually adjusted by the aviator asfar away from the eyes as possible while retaining the maximum
Figure 6. Laser protection provided by helmet (shaded area).Limited lateral and superior laser protection isachieved by flight helmet wear.
12

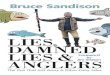
field-of-view (FOV) of approximately 40 degrees. As the NVDs aremoved further from the eyes, less head tilt is required to lookunder the device to view the cockpit instruments. The maximumFOV can only be achieved when the NVD is positioned withinapproximately 20 - 30 mm of the cornea of the eye (Figure 7).These distances are dependent on the type of eyepiece the deviceuses, i.e., 18 mm versus 25 mm ANVIS.
To compensate for the limited FOV, head movements must besubstituted for eye movements when scanning the environment. Dueto the increased head-supported weight, any increase in headmovements will increase the aviator's overall workload. To avoidexcessive head movements, aviators are taught (TC 1-204) to usescanning techniques to view the imaged scene. With a 40 degreeFOV, the eyes would theoretically turn 20 degrees before a headmovement would be initiated.
Based on the above considerations, two NVD configurationswere selected for detailed evaluation: 18 mm ANVIS worn at a
- 45
0--@ 18 mmA-A25 mm
S40-
#4- 35-o 0
004'-4 30 •
25 , , , , ,
15 20 25 30 35 40 45
Vertex distance (mm)
Figure 7. ANVIS field-of-view (FOV) versus vertex distance.FOV decrements for 18mm and 25mm ANVIS begin atapproximately 20mm and 30mm, respectively.
13

vertex distance of 20 mm and 25 mm ANVIS worn at a vertex
distance of 30 mm.
Computer model of NVD protection
A simple computer model was developed to determine retinalcoverage/exposure expected during normal NVD use. The majorvariables, Table 2, include eye relief of the ANVIS eyepieces (18mm vs. 25 mm), expected vertex distances, outside Oiameter of theeyepiece, ideal and maximum eye excursions prior to head turn,and the locations of specific reference points of a standard eye.
Table 2.
Values used in the laser protection model
Parameter Value/range
Eye relief 18 or 25 mm
Eyepiece diameters (measured):18 mm eyepiece 30.90 mm25 mm eyepiece 39.12 mm
Eye lens inset (measured):18 mm eyepiece 1.5 mm25 mm eyepiece 0.5 mm
Vertex distances:18 mm eyepiece 20 mm25 mm eyepiece 30 mm
Eye movements (MIL-HDBK-759A):Preferred 15 degreesMaximum 20 degrees
Standard eye (MIL-HDBK-141):Cornea-lst nodal point 7.30 mmCornea-center of rotation 13.0-15.5 mm
Optic disc (Harrington):Horizontal dimension 5.5 degreesVertical dimension 7.5 degreesLocation of center:
From fovea 15.5 degreesBelow horizontal 1.5 degrees
14

Key values estimated by the computer model appear in Table3, which describes the protection provided for two ANVISconfigurations as they are expected to be worn, i.e., 18mm ANVISat 20 mm vertex distance and 25 mm ANVIS at 30 mm vertexdistance. When the eyes move from center, critical areas of theretina become exposed to laser damage. The areas exposed areindicated in Table 3.
Table 3.
Lateral laser protection provided by ANVIS
Eye Lateral protectionrotation (degrees)(degrees) 18mm ANVIS 25mm ANVIS
0 31.00 27.9910 19.12 16.61 *15 13.11 ** 10.88 **20 7.56 ** 5.59 ***
* Partial optic disc exposure•* Optic disc exposed
•** Optic disc exposed + partialmacula exposure
Vertical eye movement is not considered in this reportbecause its impact on exposure is minimal. The central retina isprotected by the helmet and the NVD mount during upwardmovements. When looking down, the partially exposed optic diskis protected by the structure of the aircraft, i.e., instrumentpanel.
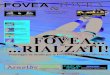
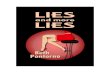
Figure 8 illustrates the additional laser protection with an18 mm ANVIS positioned 20 mm in front of the eyes. The coverageexceeds the recommended 25 degree minimum, but only when the eyesare in the primary position. Figures 9 and 10 (18 mm and 25 mmANVIS, respectively) illustrate exposure of a critical retinalfeature, the optic disc, as the eyes turn to the right 15 and 20degrees.
Table 4 contains data which demonstrate the vertex distanceeffect on ANVIS as laser protection. At any vertex distance, the25 mm ANVIS provides greater protection because of the width ofits eyepiece assembly. However, the 25-mm eyepiece was designedto be worn further away from the eye. When worn at optimumvertex distances, 30 mm for 25 mm ANVIS and 20 mm for the 18 mmANVIS, the 18 mm ANVIS has a slight protection advantage (Table3). As the NVDs are moved further from the eyes, the portion ofthe visual field protected decreases.
i5

Figure 8. ANVIS mechanical laser protection. The circularshaded area (62 degrees diameter) represents theprotection provided by 18mm ANVIS, with eyes inthe primary position.
Discussion
Under most viewing conditions and helmet/NVD configurations,the NVDs protect the macular area of the retina. Also, they willprotect the critical areas of the central retina, for at leastone of the eyes, at all times. For example, when the eyes rotateto the right during scanning, the optic disc and papillomacularbundle of the right eye are exposed, while the disc and bundle ofthe left eye are protected. This points to the main disadvantageassociated with relying on NVDs to provide laser protection,namely, the lack of continuous protection for the central retinaof both eyes.
As shown in Table 4, the area of protection decreases as theNVDs are moved further from the eyes. Variations in individualanthropometry and use of multiple optical surfaces, e.g.,protective mask with outserts, can move the NVDs far enough fromthe eyes to expose both the optic disc and part of the macula.
26

18mm ANVIS - Vertex distance = 20 mm
No eye rotation 15 degree eye rotation 20 degree eye rotation
Figure 9. Effect of eye rotation on 18mm ANVIS protection.The optic disc is unprotected during both 15- and20-degree eye rotations.
25mm ANVIS - Vertex distance = 30 mm
No eye rotation 15 degree eye rotation 20 degree eye rotation
Figure 10. Effect of eye rotation on 25mm ANVIS protection.The optic disc is unprotected during both 15- and20-degree eye rotations.
17

Table 4.
Effect of vertex distance on protectionprovided by ANVIS
Eye Vertex Lateral protectionrotation distance (degrees)(degrees) (mm) 18mm ANVIS 25mm ANVIS
15 36.59 41.9020 31.00 36.12
0 25 26.71 31.6030 23.41 27.9935 20.80 25.08
15 18.48 24.2120 13.11 18.61
15 25 9.14 14.2930 6.10 10.8835 3.72 5.90
15 12.29 18.1820 7.56 13.01
20* 25 4.82 8.7630 3.71 5.5935 3.32 3.42
* As vertex distance increases, there is a loss ofdisplay field-of-view (FOV). The lateral protec-tion listed is based on the maximum FOV for thevertex distance.
Aviators routinely use the look-under and look-aroundcapability of NVDs to view outside the aircraft. Unaided viewingis recommended to obtain chromatic cues or to judge distancesaccurately (TC 1-204, 1988). For lasers with visible outputs,peripheral retina detection/damage could result in the aviatordirecting an unprotected central retinal toward the source.
Laser damage to the NVD will require immediate transition toan unaided flight mode. This will leave the eyes unprotecteduntil a laser visor can be deployed.
Conclusions
Continuous laser protection for the central retina, out to25 degrees, will require either a mechanical obstruction or alaser protective spectacle or visor which covers at least 90degrees. The mechanical laser protection provided by NVD wear is
18

not adequate to protect the aviator. It must be understood bythe operational community that the provision of laser protectionby mechanical blockage using NVDs only protects the user fromincapacitating macular injury. The peripheral retina would beunprotected and susceptible to injury.
19

References
Apple, D. J., Goldberg, M. F., and Wyhinny G. 1973.Histopathology and ultrastructure of the argon laser lesionin human retinal and choroidal vasculatures. Americanjournal of ophthalmology, 75, 4:595-609.
Apple D. J., Wyhinny G. J., Goldberg M. F., Polley E. H., andBizzell, J. W. 1976a. Experimental argon laser photo-coagulation, I. Effects on retinal nerve fiber layer.Archives of ophthalmology, 94:137-144.
Apple D. J., Wyhinny G. J., Goldberg M. F., and Polley E. H.1976b. Experimental argon laser photocoagulation, II.Effects on the optic disc. Archives of ophthalmolov,94:296-304.
Department of the Army. 1962. Optical design, MIL-HDBK-141,dated 5 October 1962. Washington, DC.
Department of the Army. 1981. Human factors engineering designfor Army materiel (metric), MIL-HDBK-759A (MI), dated 30June 1981. Washington, DC.
Department of the Army. 1988. Night flight. techniques andprocedures, TC-I-204, dated 27 December 1988. Washington,DC.
Goldberg, M. F. and Herbst, R. W. 1973. Acute complications ofargon laser photocoagulation. Archives of ophthalmology,89:311-304.
Harrington, D. 0. 1971. The visual fields. 3rd ed. St. Louis:The C. V. Mosby Company.
L'Esperance, F. A., ed. 1989. Ophthalmic lasers. 3rd ed.St. Louis: The C. V. Mosby Company.
Swartz M., Apple D. J., and Creel D. 1983. Sudden severe visualloss associated with peripapillary burns during panretinalargon photocoagulation. British journal of ophthalmology,67:517-519.
Wiley, R. W. 1989. Visual acuity as a function of mean ambientluminance and target contrast (Abstract). Aviation, space.and environmental medicine. 59:466.
Wolfe, J. A. 1985. Laser retinal injury. Military medicine,150:177-185.
20

Appendix A
Tasking document.
21

DEPARTMENT OF THE ARMYPRODUCT MANAGER AVIATION UFE SUPPORT EQUIPMENT
4300 GOODFELLOW BOULEVARD. ST. LOUIS. MD 63120-1798
REPLY TO) TTENTION OP
AMCP-ALSE (70) APR I 1988
MEMORANDUM FOR COMMANDER, U.S. ARMY AEROMEDICAL RESEARCH LABORATORY, ATTN:SGRD-UAS-VS (DR. WILEY), P.O. BOX 577, FORT RUCKER, AL 36362-5000
SUBJECT: Field of View (FOV) Laser Eye Protection
1. Request an FOV evaluation be made with an SPH-4 Helmet and the followingoptical devices: ANVIS, HGU-4P Spectacles, and HGU-56/P Laser Glasses.
2. The purpose is to determine the FOV l -'-r eye protection these devices willprovide.
3. Point of contact for this action is Hr. Herbert Lee, AMCPM-ALSE, AUTOVON693-1933 or Commercial (314) 263-3513.
RAYMD J.CONNOLLY
LTC, AVProduct ManagerAviation Life Support Equipment
22

Initial distribution
Commander CommanderU.S. Army Natick Research U.S. Army Research Institute
and Development Center of Environmental MedicineATTN: Documents Librarian Natick, MA 01760Natick, MA 01760
Naval Submarine Medical U.S. Army Avionics ResearchResearch Laboratory and Development Activity
Medical Library, Naval Sub Base ATTN: SAVAA-P-TPBox 900 Fort Monmouth, NJ 07703-5401Groton, CT 06340
Commander/Director U.S. Army Research and DevelopmentU.S. Army Combat Surveillance Support Activity
& Target Acquisition Lab Fort Monmouth, NJ 07703ATTN: DELCS-DFort Monmouth, NJ 07703-5304
Commander Chief, Benet Weapons Laboratory10th Medical Laboratory LCWSL, USA ARRADCOMATTN: Audiologist ATTN: DRDAR-LCB-TLAPO New York 09180 Watervliet Arsenal, NY 12189
Commander CommanderNaval Air Development Center Man-Machine Integration SystemBiophysics Lab Code 602ATTN: G. Kydd Naval Air Development CenterCode 60BI Warminster, PA 18974Warminster, PA 18974
Naval Air Development Center CommanderTechnical Information Division Naval Air Development CenterTechnical Support Detachment ATTN: Code 6021 (Mr. Brindle)Warminster, PA 18974 Warminster, PA 18974
Commanding Officer Commanding OfficerNaval Medical Research Harry G. Armstrong Aerospace
and Development Command Medical Research LaboratoryNational Naval Medical Center Wright-PattersonBethesda, MD 20014 Air Force Base, OH 45433
Under Secretary of Defense Directorfor Research and Engineering Army Audiology and Speech Center
ATTN: Military Assistant Walter Reed Army Medical Centerfor Medical and Life Sciences Washington, DC 20307-5001
Washington, DC 20301
23

Director CommanderWalter Reed Army Institute U.S. Army Institute
of Research of Dental ResearchWashington, DC 20307-5100 Walter Reed Army Medical Center
Washington, DC 20307-5300
HQ DA (DASG-PSP-O) Naval Air Systems Command5109 Leesburg Pike Technical Air Library 950DFalls Church, VA 22041-3258 Rm 278, Jefferson Plaza II
Department of the NavyWashington, DC 20361
Naval Research Naval Research Laboratory LibraryLaboratory Library Shock and Vibration Infor-
Code 1433 mation Center, Code 5804Washington, DC 20375 Washington, DC 20375
Harry Diamond Laboratories DirectorATTN: Technical Infor- U.S. Army Human Engineer-
mation Branch ing Laboratory2800 Powder Mill Road ATTN: Technical LibraryAdelphi, MD 20783-1197 Aberdeen Proving Ground,
MD 21005-5001
U.S. Army Materiel Systems CommanderAnalysis Agency U.S. Army Test
ATTN: Reports Processing and Evaluation CommandAberdeen proving Ground ATTN: AMSTE-AD-HMD 21005-5017 Aberdeen Proving Ground,
MD 21005-5055
U.S. Army Ordnance Center Directorand School Library U.S. Army Ballistic
Building 3071 Research LaboratoryAberdeen Proving Ground, ATTN: DRXBR-OD-ST Tech ReportsMD 21005-5201 Aberdeen Proving Ground,
MD 21005-5066
U.S. Army Environmental Hygiene CommanderAgency U.S. Army Medical Research
Building E2100 Institute of Chemical DefenseAberdeen Proving Ground, ATTN: SGRD-UV-AOMD 21010 Aberdeen Proving Ground,
MD 21010-5425
Technical Library CommanderChemical Research U.S. Army Medical Research
and Development Center and Development CommandAberdeen Proving Ground, ATTN: SGRD-RMS (Ms. Madigan)MD 21010-5423 Fort Detrick, Frederick,
MD 21701
24

Commander CommanderU.S. Army Medical Research U.S. Army Biomedical Research
Institute of Infectious Diseases and Development LaboratoryFort Detrick, Frederick, ATTN: SGRD-UBZ-IMD 21701 Fort Detrick, Frederick,
MD 21701
Director, Biological Defense TechnicalSciences Division Information Center
Office of Naval Research Cameron Station600 North Quincy Street Alexandria, VA 22313Arlington, VA 22217
Commander U.S. Army Foreign ScienceU.S. Army Materiel Command and Technology CenterATTN: AMCDE-XS ATTN: MTZ5001 Eisenhower Avenue 220 7th Street, NEAlexandria, VA 22333 Charlottesville, VA 22901-5396
Commandant Director,U.S. Army Aviation Applied Technology Laboratory
Logistics School USARTL-AVSCOMATTN: ATSQ-TDN ATTN: Library, Building 401Fort Eustis, VA 23604 Fort Eustis, VA 23604
U.S. Army Training U.S. Army Trainingand Doctrine Command and Doctrine Command
ATTN: ATCD-ZX ATTN: SurgeonFort Monroe, VA 23651 Fort Monroe, VA 23651-5000
Structures Laboratory Library Aviation Medicine ClinicUSARTL-AVSCOM TMC #22, SAAFNASA Langley Research Center Fort Bragg, NC 28305Mail Stop 266Hampton, VA 23665
Naval Aerospace Medical U.S. Air Force ArmamentInstitute Library Development and Test Center
Bldg 1953, Code 102 Eglin Air Force Base, FL 32542Pensacola, FL 32508
Command Surgeon U.S. Army Missile CommandU.S. Central Command Redstone ScientificMacDill Air Force Base Information CenterFL 33608 ATTN: Documents Section
Redstone Arsenal, AL 35898-5241
Air University Library U.S. Army Research and Technology(AUL/LSE) Labortories (AVSCOM)Maxwell AFB, AL 36112 Propulsion Laboratory MS 302-2
NASA Lewis Research CenterCleveland, OH 44135
25

AFAMRL/HEX U.S. Air Force InstituteWright-Patterson AFB, OH 45433 of Technology (AFIT/LDEE)
Building 640, Area BWright-Patterson AFB, OH 45433
University of Michigan Henry L. TaylorNASA Center of Excellence Director, Institute of Aviation
in Man-Systems Research University of Illinois-ATTN: R. G. Snyder, Director Willard AirportAnn Arbor, MI 48109 Savoy, IL 61874
John A. Dellinger, COL Craig L. Urbauer, ChiefSouthwest Research Institute Office of Army Surgeon GeneralP. 0. Box 28510 National Guard BureauSan Antonio, TX 78284 Washington, DC 50310-2500
Product Manager CommanderAviation Life Support Equipment U.S. Army AviationATTN: AMCPM-ALSE Systems Command4300 Goodfellow Blvd. ATTN: SGRD-UAX-AL (MAJ Lacy)St. Louis, MO 63120-1798 4300 Goodfellow Blvd., Bldg 105
St. Louis, MO 63120
Commander U.S. Army Aviation Systems CommandU.S. Army Aviation Library and Information
Systems Command Center BranchATTN: AMSAV-ED ATTN: AMSAV-DIL4300 Goodfellow Blvd 4300 Goodfellow BlvdSt. Louis, MO 63120 St. Louis, MO 63120
Commanding Officer Federal Aviation AdministrationNaval Biodynamics Laboratory Civil Aeromedical InstituteP.O. Box 24907 CAMI Library AAC 64D1New Orleans, LA 70189 P.O. Box 25082
Oklahoma City, OK 73125
U.S. Army Field Artillery School CommanderATTN: Library U.S. Army AcademySnow Hall, Room 14 of Health SciencesFort Sill, OK 73503 ATTN: Library
Fort Sam Houston, TX 78234
Commander CommanderU.S. Army Health Services Command U.S. Army InstituteATTN: HSOP-SO of Surgical ResearchFort Sam Houston, TX 78234-6000 ATTN: SGRD-USM (Jan Duke)
Fort Sam Houston, TX 78234-6200
26

Director of Professional Services U.S. Air Force SchoolAFMSC/GSP of Aerospace MedicineBrooks Air Force Base, TX 78235 Strughold Aeromedical Library
Documents Section, USAFSAM/TSK-4Brooks Air Force Base, TX 78235
U.S. Army Dugway Proving Ground Dr. Diane DamosTechnical Library Department of Human FactorsBldg 5330 ISSM, USCDugw.y, UT 64022 Los Angeles, CA 90089-0021
U.S. Army Yuma Proving Ground U.S. Army White SandsTechnical Library Missile RangeYuma, AZ 85364 Technical Library Division
White Sands Missile Range,NM 88002
AFFTC Technical Library U.S. Army Aviation Engineering6520 TESTG/ENXL Flight ActivityEdwards Air Force Base, ATTN: SAVTE-M (Tech Lib)CAL 93523-5000 Stop 217
Edwards Air Force Base,CA 93523-5000
Commander Ms. Sandra G. HartCode 3431 Ames Research CenterNaval Weapons Center MS 239-5China Lake, CA 93555 Moffett Field, CA 94035
Aeromechanics Laboratory CommanderU.S. Army Research Letterman Army Institute
and Technical Labs of ResearchAmes Research Center, ATTN: Medical Research Library
M/S 215-1 Presidio of San Francisco,Moffett Field, CA 94035 CA 94129
Sixth U.S. Army '*Mr. Frank J. Stagnaro, MEATTN: SMA Rush Franklin PublishingPresidio of San Francisco, 300 Orchard City DriveCA 94129 Campbell, CA 95008
Commander CommanderU.S. Army Aeromedical Center U.S. Army Medical MaterielFort Rucker, AL 36362 Development Activity
Fort Detrick, Frederick,MD 21701-5009
27

Commander, U.S. ArmyAviation Center
Directorate Directorateof Combat Developments of Training Development
Bldg 507 Bldg 502Fort Rucker, AL 36362 Fort Rucker, AL 36362
Chief ChiefArmy Research Institute Human Engineering Laboratory
Field Unit Field UnitFort Rucker, AL 36362 Fort Rucker, AL 36362
Commander CommanderU.S. Army Safety Center U.S. Army Aviation CenterFort Rucker, AL 36362 and Fort Rucker
ATTN: ATZQ-T-ATLFort Rucker, AL 36362
U.S. Army Aircraft Development PresidentTest Activity U.S. Army Aviation Board
ATTN: STEBG-MP-QA Cairns AAFCairns AAF Fort Rucker, AL 36362Fort Rucker, AL 36362
Commander Dr. William E. McLeanU.S. Army Medical Research Human Engineering Laboratory
and Development Command ATTN: SLCHE-BRATTN: SGRD-PLC (COL Sedge) Aberdeen Proving Ground,Fort Detrick, Frederick MD 21005-5001MD 21701
MAJ John Wilson Canadian Army Liaison OfficeTRADOC Aviation LO Building 602Embassy of the United States Fort Rucker, AL 36362APO New York 09777
Netherlands Army Liaison Office German Army Liaison OfficeBuilding 602 Building 602Fort Rucker, AL 36362 Fort Rucker, AL 36362
British Army Liaison Office French Army Liaison OfficeBuilding 602 Building 602Fort Rucker, AL 36362 Fort Rucker, AL 36362
Italian Army Liaison Office Brazilian Army Liaison OfficeBuilding 602 Building 602Fort Rucker, AL 36362 Fort Rucker, AL 36362
28

Australian Army Liaison Office CommandantBuilding 602 Royal Air Force InstituteFort Rucker, AL 36362 of Aviation Medicine
Farnborough Hants UK GU14 6SZ
Dr. Garrison Rapmund Dr. A. Kornfield, President6 Burning Tree Court Biosearch CompanyBethesda, MD 20817 3016 Revere Road
Drexel Hill, PA 29026
29