Embed Size (px)
Citation preview
By Kim Harbal and Marcus Williamson

Taxonomy• CLASS: SECERNENTEA
• SUBCLASS: RHABDITIA
• ORDER: RHABDITIDA
• SUBORDER: RHABDITINA
• SUPERFAMILY: RHABDITOIDEA
• FAMILY: STRONGYLOIDIDAE

Where is this Parasite Found?
• Tropical and Sub-tropcial regions
• Temperate regions• Rural areas,
institutional settings, and in lower socioeconomic groups
• Mostly found in warm moist areas that favor the survival of the juvenile stages
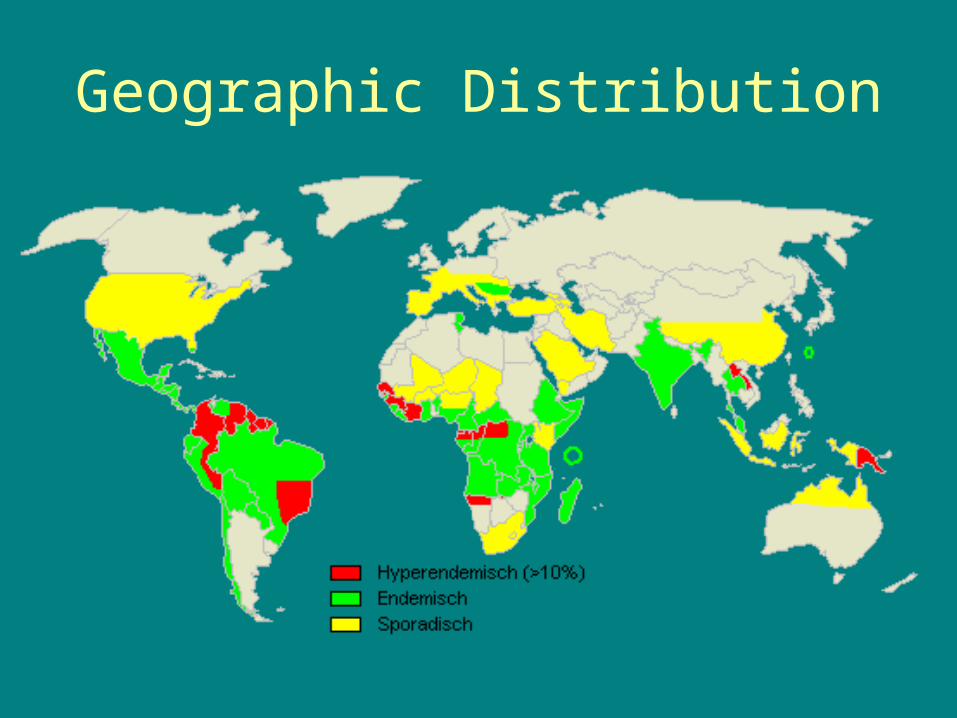
Geographic Distribution
• Currently, an estimated 100-200 million people are infected worldwide in 70 countries
• In the US: Appalachians, especially in eastern Tennessee, Kentucky, and West Virginia.
• Internationally: Sub-Saharan Africa, South and Southeast Asia, Central America, and South America, and parts of Eastern Europe

Question #1
• Name a state that has Strongyloides stercoralis?
Geographic Distribution

General Things to Know• Commonly called a Threadworm• The smallest nematode parasites of humans• Most Strongyloides and their eggs are found in the
soil • Infections are initiated when exposed skin contacts
contaminated soil • Autoinfection commonly occurs allowing infection to
persist for decades • More common in people who suffer from alcholism,
who are caucasion, males, or have an occupation that involves soil contact
• Not likely to be transmitted through water

HostsDefinitive
• Humans• Dogs• Cats• Other mammals
Intermediate Hosts• None
There are 38 species of threadworms found in sheep, swine,
goat, ox, deer, camel, rabbit, primates, dogs, and cats

Question #2
• How many species of Strongyloides are there?
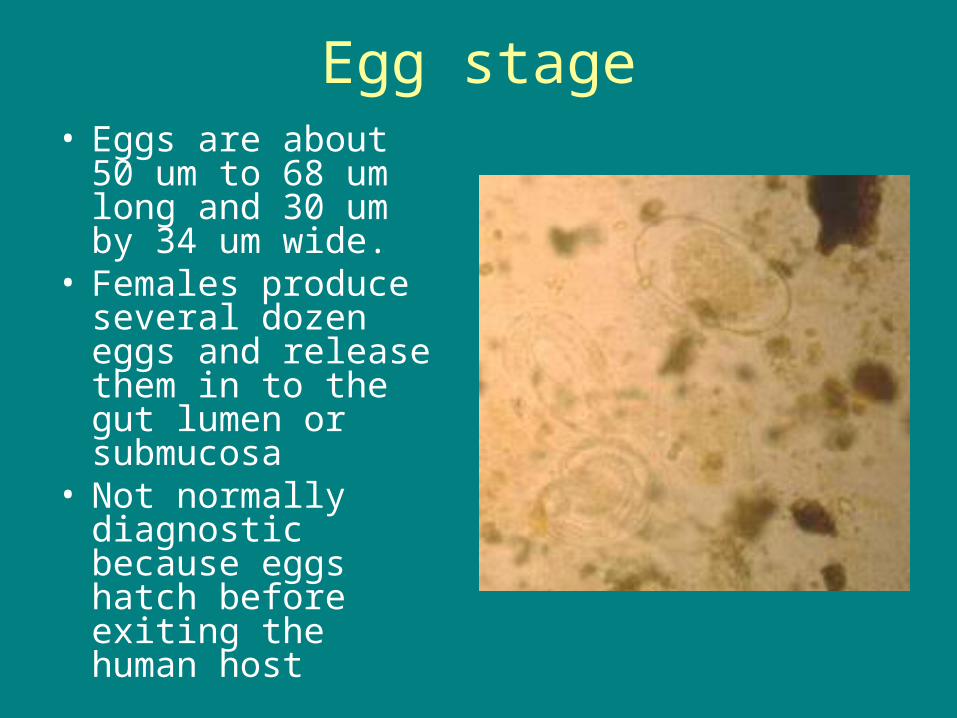
Egg stage• Eggs are about 50
um to 68 um long and 30 um by 34 um wide.
• Females produce several dozen eggs and release them in to the gut lumen or submucosa
• Not normally diagnostic because eggs hatch before exiting the human host

Rhabditiform larvae stage (L1)
• Non infective stage• Size ranges from 250-
300 microns in length and 60 microns in diameter
• Passed with feces
Rhabditiform larvae stage (L1)
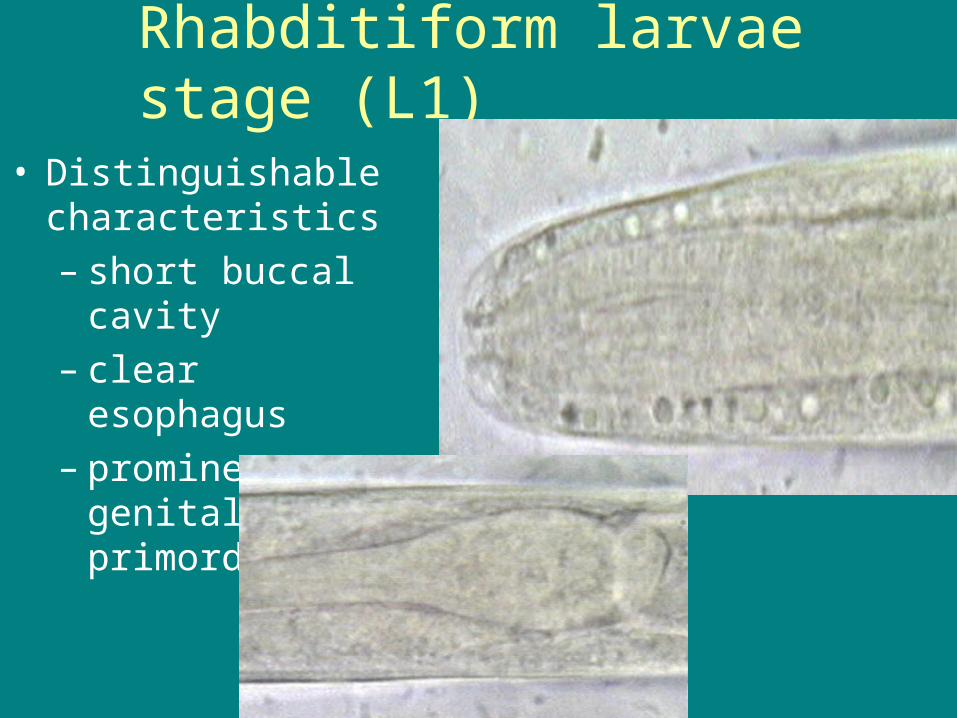
• Distinguishable characteristics– short buccal cavity – clear esophagus– prominent genital
primordium

Rhabditiform Stage (cont’d)

Filariform Stage (L3)
• Reside in the small intestine of the host
• They are about 650 microns long and 50 microns in length
• Have a long esophagus
• This is the infective stage of Strongyloidiasis
Filariform Stage (cont’d)
• Have a long non bulbous esophagus of about 2/5 of the length of the body
• Female filariform larvae are slender and faster moving than the rhabditiform stage
• Male filariform larvae are not parasitic, only the females are
• Filariform larvae penetrate the skin by releasing hydrolitic enzymes

Question #3
• Name one of the three distinguishable characteristics of rhabditiform larvae from other species of nematodes?

Question #4
• What larvae form is the infective stage?

Free living Females• Have a rhabditiform
esophagus• Females are about 1
mm in length by 50-75 um wide
• Contain embryonated eggs
• Females have a vulva that is about equatorial
• Females uteri contains more eggs than most parasitic females

Free living Males• Have a rhabditiform
esophagus
• Males are up to 0.9 mm long and 40um to 50 um wide
• Have two simple spicules and a gubernaculum
• Their pointed tail is a curved ventrad
Parthenogenetic females
• Parthenogenetic females reach a length of 2.0-3.0 mm
• 1/3 of the worm is the esophagus
• Inhabit crypts of the small intestines
• Female is stout and has a vulva that is about equatorial
• Vulva is in the posterior third of the body
• The uteri carries only a few eggs at a time

Question #5
• T/F The adult male is found in the definitive host.
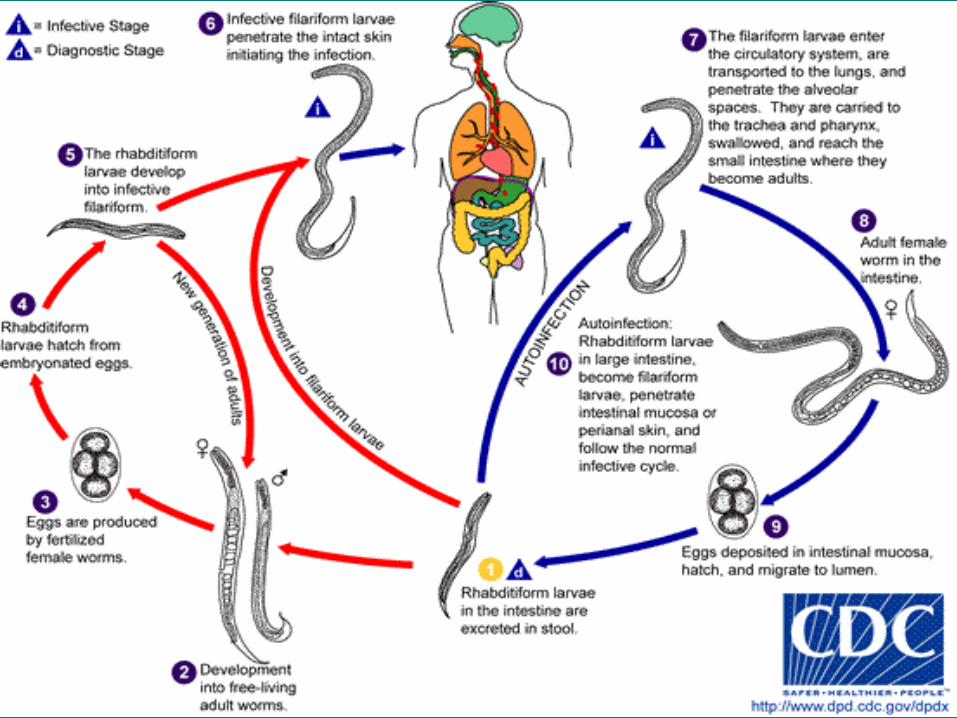

Life Cycle
• Adults lay eggs in the intestines within the definitive host
• Rhabditiform larvae hatch from the eggs in the intestines
• Three possibilities from here– Free living adult worms (Heterogonic)– Filariform larvae (Homogenic - Parasitic
Generation) – Autoinfection
Free living adult worms (Heterogonic)
• Rhabditiform larvae will be excreted in the stool• In this developmental option, the rhabditiform will
molt four times and will either become a female or male adult worm
• The free-living adults then mate and produce eggs
• The rhabditiform larvae then hatch from the eggs• The larvae then can either produce a new
generation of adults or become filariform larvae

Homogenic Life Cycle
• Rhaabditiform larvae will be excreted in the stool
• The rhabditiform larvae molt twice and develop into filariform larvae
• No adult stages outside of host with this life cycle

Autoinfection
• In this, the rhabditiform larvae develop into filariform larvae before they leave the hosts intestines
• The filariform larvae then penetrate the intestinal mucosa or perianal skin
• They then follow the life cycle in the host…to be explained next…
Parasite in the host• Now, the filariform larvae from each cycle enter
the circulatory system and travel to the heart • They come out of the pulmonary artery and
enter into the lungs• Penetrate the alveolar spaces and are carried to
the trachea and pharynx, swallowed, and make there way to the small intestines
• In the small intestines they molt twice and become adult female worms
• By parthenogenesis they produce eggs, yielding rhabditiform larvae
• The prepatent period lasts about 1 month • Possible cycles start over again
Question #6
• Name 1 of the 3 cycles that occurs with Strongyloides stercoralis?
Question #7
• What larvae stage is excreted in the stool?
Transmission
• Through contaminated soil– Ingestion– Skin contact
• Autoinfection• Transmammary
infection (with dogs)– Presumably it can
occur in humans

Symptoms• Most Strongyloides infections are asymptomatic
and can survive decades undiagnosed– The longest documented asymptomatic infection was
more than 65 years• Symptomatic infections typically manifest in
gastrointestinal, pulmonary, and dermatologic systems
• In immunocompromised persons, symptomatic infections can be devastating and carry a 60-85% mortality rate
• Acute Infection• Chronic infection• Hyperinfection• Disseminated Infection
Types of Infections• Acute Infection
• Symptoms occur after a few weeks whether it is a cough, abdominal pain, diarrhea, and/or anorexia.
• Most likely detection of hundreds of larvae
• Chronic infection– manifested by epigastric pain, recurrent hives (urticaria) and transient
red lines on the skin that appear and move rapidly (larva currens) and sporadic diarrhea
• Hyperinfection– Most patients that experience this are immunocompromised– Most likely from accelerated autoinfection– Large number of parasites present– Large numbers of larvae in stool and/or sputum
• Disseminated Infection– Migration of larvae to organs beyond the range of the pulmonary
autoinfective cycle
Gastrointestinal Symptoms
• Bloating, distension • Diffuse abdominal
pain • Diarrhea, typically
nonbloody • Anorexia, weight loss,
nausea • Malabsorption
syndromes may occur in chronic infections

Question #8
• T/F It can be transmitted by breast milk

Dermatologic Symptoms
• Ground itch - Papulovesicular pruritic rash, usually on the feet
• Cutaneous infection: Dermatitis is produced by migration of the infective juveniles through the skin
• Petechial/purpuric rash (with disseminated disease)
• Inflammation• Slight hemorrhage and swelling• Larva currens – Skin lesions,
hives, or rash often on the trunk and buttocks (allergic response due to migrating larvae

Cardiopulmonary Symptoms
• Wheezing or coughing• Mild to severe symptoms
of pneumonia when worms are present in the lungs
• Hyperinfection syndrome– massive proliferation of
larval forms
• Pulpatations• Atriofibrillations• Choking sensation

Diagnosis
• Examination of feces and duodenal contents• Finding rhabdiform or filariform larvae in a fresh
stool – If not in a fresh stool, may be misdiagnosed as
hookworm
• Finding larvae in the sputum• Culture techniques• ELISA• Immunodiagnosis by indirect immunofluorescence
– Antigen: whole Strongyloides ratti larvae

Question #9
• Name a way the parasite can be diagnosed?

Culture Technique
• Fairly new technique• Movement of the larval
forms can be seen• Bacterial colonies of
normal oral flora are formed along the moving trail
• Performed using a chocolate agar sputum culture

Treatment and Prevention
• Thiamendazole– Keeps nematode larvae from growing into
adult forms
• Cambendazole
• Ivermection – 100% effective for clearing Strongyloides infection with no side effects
Control• Proper hygiene• Do not allow
infected hosts to breast feed
• Do not walk barefoot in soil
• In Hospitals– Make sure you
wear clean masks, gloves, and aprons
– Wash hands frequently
Question #10
• What drug is 100% effective against Strongyloidiasis?
Question #11
• Are you more likely to get Strongyloidiasis by swimming in a lake or walking barefoot in the woods?
Works cited
• Schmidt, G., & Roberts, L. (2005). Foundations of Parasitology (7th ed.). New York, NY: McGraw-Hill
• Schmidt, G.S., and L.S. Roberts. 1989. Chapter 25. Order Rhabditata: Pioneering Parasites. in Foundations of Parasitology. Times Mirror/Mosby
College Publishing. St. Louis. 750 pages. • http://www.dpd.cdc.gov/dpdx/HTML/Strongyloidiasis.htm• http://www.emedicine.com/emerg/topic843.htm• http://www.cdfound.to.it/HTML/str1.htm#ss1• http://www.wormtreatment.com/worm/strongyloides/• http://martin.parasitology.mcgill.ca/jimspage/biol/
strongyl.htm• http://cmr.asm.org/cgi/content/full/17/1/208?
ck=nck#Acute%20Strongyloidiasis
![Strongyloides myopotami (Secernentea: Strongyloididae) from … · 2017. 4. 7. · Schistosoma mansoni, Giardia lamblia, Taenia spp., and Fasciola hepatica [1]. Until now, no efforts](https://img.pdfslide.net/doc/110x75/6146adddf4263007b1355575/strongyloides-myopotami-secernentea-strongyloididae-from-2017-4-7-schistosoma.jpg)